Palliative enteroscopic stent placement for malignant mid-gut obstruction · the anatomy of the...
5
Review Article Palliative enteroscopic stent placement for malignant mid-gut obstruction Esha Baichoo, Louis M. Wong Kee Song * abstract Palliation of malignant small intestinal obstructions beyond the reach of conventional endoscopes for stent placement generally requires endoscopic decompression via a gastrostomy tube or a surgical bypass in patients who are operable candidates. With the advent of deep enteroscopy, palliative stent placement for mid-gut obstruction using currently available self-expandable metal stents may be feasible in selected cases. Proper patient selection and technical proficiency in deep enteroscopy and stent placement are key determinants for a successful outcome. Alternative means of stent delivery, including the percutaneous route, are also being developed, with the hope of expanding the use of stents in the mid small bowel beyond palliation. Copyright Ó 2014, Society of Gastrointestinal Intervention. Published by Elsevier. Keywords: deep enteroscopy, palliation, small intestinal carcinoma, small intestinal obstruction, stent Introduction Placement of a self-expandable metal stent (SEMS) is an accepted therapeutic option for palliation of malignant obstruction involving the esophagus, gastroduodenum, and colon, and dedi- cated SEMS are available for over-the-wire or through-the-scope (TTS) insertion across obstructive lesions at these locations. 1,2 Ma- lignant small bowel obstruction is a dire complication of intrinsic disease or extrinsic compression from abdominopelvic tumors. However, endoscopic stent placement in the mid small bowel, defined as the segment between the ampulla of Vater and the ileocecal valve, can be technically challenging or infeasible owing to the anatomy of the small intestine, limitations of conventional endoscopes, and lack of TTS SEMS designed specifically for use in the mid gut. 3 Palliation of malignant obstruction in the distal duodenum, and even the proximal jejunum, can generally be achieved using a therapeutic upper endoscope or an adult colonoscope whose large working channel can accommodate TTS placement of currently available enteral SEMS. 4 In some cases, however, significant looping in the stomach and duodenal sweep limits endoscope insertion to more distal areas of obstruction and palliative surgical intervention, such as a bypass or diverting ostomy, is necessary. In poor surgical candidates, placement of a venting percutaneous endoscopic gas- trostomy (PEG) or jejunostomy tube may be required. 5,6 The introduction of double balloon enteroscopy (DBE) and, subsequently, single balloon enteroscopy and spiral overtube- assisted enteroscopy (SE) have significantly impacted the diagnosis and therapy of diseases involving the small intestine. 7,8 These techniques, collectively referred to as deep enteroscopy, can overcome looping, such as in a J-shaped stomach, and enable access to deeper segments of the small intestine for palliative stent placement. Balloon-assisted enteroscopy involves sequential push– pull maneuvers, whereas SE uses rotation of a specialized overtube with raised spirals at its tip to pleat the small bowel onto the overtube and enable enteroscope insertion deep into the small bowel. 9 Although the working channel of deep enteroscopes (2.8 mm diameter) does not allow TTS passage of currently avail- able SEMS and there are no dedicated stents for enteroscopic use, the deep enteroscopy techniques provide a stable platform via a fixed overtube for the non-TTS delivery of stents to the mid gut, as outlined below. Indications and practical considerations Although the major indication for mid-gut stent placement is palliation of malignant extrinsic or intrinsic obstructions, other po- tential indications include preoperative decompression as a bridge to surgery, closure of malignant chronic fistulae, and sealing of anas- tomotic leaks for which surgical revision is deemed too risky. 3 Careful patient assessment remains an absolute prerequisite prior to considering stent placement for palliation of mid-gut ste- nosis. Radiological imaging, such as computed tomography of the abdomen and pelvis, is essential and may demonstrate multifocal sites of small bowel obstruction, which negate the benefit of placing a stent at a single point of obstruction (Fig. 1). This is Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN, USA Received 30 March 2014; Accepted 11 April 2014 * Corresponding author. Division of Gastroenterology and Hepatology, Mayo Clinic, 200 1st Street South West, Rochester, MN 55905, USA. E-mail address: [email protected] (L.M. Wong Kee Song). Contents lists available at ScienceDirect Gastrointestinal Intervention journal homepage: www.gi-intervention.org 2213-1795 Copyright Ó 2014, Society of Gastrointestinal Intervention. Published by Elsevier. http://dx.doi.org/10.1016/j.gii.2014.04.001 Gastrointest Interv 2014; 3:30–34 Open access under CC BY-NC-ND license. Open access under CC BY-NC-ND license.
Transcript of Palliative enteroscopic stent placement for malignant mid-gut obstruction · the anatomy of the...

lable at ScienceDirect
Gastrointest Interv 2014; 3:30–34
Contents lists avai
Gastrointestinal Intervention
journal homepage: www.gi - intervent ion.org
Review Article
Palliative enteroscopic stent placement for malignant mid-gutobstruction
Esha Baichoo, Louis M. Wong Kee Song*
a b s t r a c t
Palliation of malignant small intestinal obstructions beyond the reach of conventional endoscopes for stent placement generally requires endoscopicdecompression via a gastrostomy tube or a surgical bypass in patients who are operable candidates. With the advent of deep enteroscopy, palliative stentplacement for mid-gut obstruction using currently available self-expandable metal stents may be feasible in selected cases. Proper patient selection andtechnical proficiency in deep enteroscopy and stent placement are key determinants for a successful outcome. Alternative means of stent delivery,including the percutaneous route, are also being developed, with the hope of expanding the use of stents in the mid small bowel beyond palliation.
Copyright � 2014, Society of Gastrointestinal Intervention. Published by Elsevier.
Keywords: deep enteroscopy, palliation, small intestinal carcinoma, small intestinal obstruction, stent
Open access under CC BY-NC-ND license.
Introduction
Placement of a self-expandable metal stent (SEMS) is anaccepted therapeutic option for palliation of malignant obstructioninvolving the esophagus, gastroduodenum, and colon, and dedi-cated SEMS are available for over-the-wire or through-the-scope(TTS) insertion across obstructive lesions at these locations.1,2 Ma-lignant small bowel obstruction is a dire complication of intrinsicdisease or extrinsic compression from abdominopelvic tumors.However, endoscopic stent placement in the mid small bowel,defined as the segment between the ampulla of Vater and theileocecal valve, can be technically challenging or infeasible owing tothe anatomy of the small intestine, limitations of conventionalendoscopes, and lack of TTS SEMS designed specifically for use inthe mid gut.3
Palliation of malignant obstruction in the distal duodenum, andeven the proximal jejunum, can generally be achieved using atherapeutic upper endoscope or an adult colonoscope whose largeworking channel can accommodate TTS placement of currentlyavailable enteral SEMS.4 In some cases, however, significant loopingin the stomach and duodenal sweep limits endoscope insertion tomore distal areas of obstruction and palliative surgical intervention,such as a bypass or diverting ostomy, is necessary. In poor surgicalcandidates, placement of a venting percutaneous endoscopic gas-trostomy (PEG) or jejunostomy tube may be required.5,6
The introduction of double balloon enteroscopy (DBE) and,subsequently, single balloon enteroscopy and spiral overtube-assisted enteroscopy (SE) have significantly impacted the
Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN, USAReceived 30 March 2014; Accepted 11 April 2014* Corresponding author. Division of Gastroenterology and Hepatology, Mayo Clinic, 20
E-mail address: [email protected] (L.M. Wong Kee Song).
2213-1795 Copyright � 2014, Society of Gastrointestinal Intervention. Published by Elsehttp://dx.doi.org/10.1016/j.gii.2014.04.001
diagnosis and therapy of diseases involving the small intestine.7,8
These techniques, collectively referred to as deep enteroscopy,can overcome looping, such as in a J-shaped stomach, and enableaccess to deeper segments of the small intestine for palliative stentplacement. Balloon-assisted enteroscopy involves sequential push–pull maneuvers, whereas SE uses rotation of a specialized overtubewith raised spirals at its tip to pleat the small bowel onto theovertube and enable enteroscope insertion deep into the smallbowel.9 Although the working channel of deep enteroscopes(2.8 mm diameter) does not allow TTS passage of currently avail-able SEMS and there are no dedicated stents for enteroscopic use,the deep enteroscopy techniques provide a stable platform via afixed overtube for the non-TTS delivery of stents to the mid gut, asoutlined below.
Indications and practical considerations
Although the major indication for mid-gut stent placement ispalliation of malignant extrinsic or intrinsic obstructions, other po-tential indications includepreoperative decompression as a bridge tosurgery, closure of malignant chronic fistulae, and sealing of anas-tomotic leaks for which surgical revision is deemed too risky.3
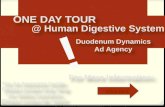
Careful patient assessment remains an absolute prerequisiteprior to considering stent placement for palliation of mid-gut ste-nosis. Radiological imaging, such as computed tomography of theabdomen and pelvis, is essential and may demonstrate multifocalsites of small bowel obstruction, which negate the benefit ofplacing a stent at a single point of obstruction (Fig. 1). This is
0 1st Street South West, Rochester, MN 55905, USA.
vier. Open access under CC BY-NC-ND license.

Esha Baichoo and Louis M. Wong Kee Song / Stenting mid-gut obstruction 31
particularly true in patients with extensive peritoneal carcinoma-tosis, where a venting PEG may be the best palliative option. Im-aging is not foolproof, however, and distal sites of obstruction maymanifest themselves only after stent placement for a radiographi-cally apparent isolated proximal stenotic segment has beenperformed.
The use of an adult colonoscope can be effective in deliveringenteral stents for malignant obstructions of the distal duodenumand proximal jejunum, and should be given primary considerationfor lesions at these locations. The technical success rate was 93% inone study of 16 patients with malignant distal duodenal or prox-imal jejunal obstruction.4 Of note, nine of the patients had under-gone prior unsuccessful attempts at stent placement using agastroscope.
Surgical bypass should be considered preferentially for patientswith a reasonable performance status and a longer life expectancy,as it is associated with better long-term outcomes, fewer adverseevents, and a lesser rate of intervention relative to stent place-ment.5,10 Although the data pertain primarily to gastric outletobstruction, the findings can likely be extrapolated to malignantmid-gut obstruction.
Deep enteroscopy for stent placement in the mid gut
Although the depth of insertion and rate of complete entero-scopy is greater with DBE, clinical comparative trials have shownsimilar diagnostic and therapeutic yields among the deep entero-scopy instruments.8,11 All three modalities appear to be equally safeand effective for the evaluation of the small intestine. Thus, theselection of a particular device is influenced primarily by deviceavailability and operator preference.
A deep enteroscopy approach for the palliative stenting of mid-gut obstructions represents an attractive option over surgical
Fig. 1. Multifocal areas of obstruction with dilation and fecalization of the small boweldue to extensive peritoneal carcinomatosis.
intervention because of its minimally invasive nature and expectedlower rate of procedure-related morbidity, particularly in termi-nally ill patients with a poor performance status. Deep enteroscopy,however, may not be suitable or feasible in patients with bowelencasement from widespread peritoneal carcinomatosis and inthose with severe small bowel fixation and angulation from sur-gical adhesions that hinder advancement of the enteroscope.Therefore, the decision to proceed with deep enteroscopy-assistedstent placement for palliating mid gut obstruction should be indi-vidualized. Two methods of mid-gut stent insertion using deepenteroscopy instruments and commercially available SEMS havebeen described: the withdrawal–reinsertion technique and thethrough-the-overtube technique.
Withdrawal–reinsertion technique
Lee et al12 described the use of the withdrawal–reinsertiontechnique that involves the advancement of DBE and balloon-assisted reduction maneuvers, as needed, to reach the site ofobstruction, the insertion of a long guide-wire through the stric-ture, and instrument removal while leaving the guide-wire in place.The guide-wire is then back-fed into the working channel of aconventional therapeutic endoscope, which is advanced as far astechnically feasible into the gut lumen. A TTS SEMS is subsequentlyinserted over the guide-wire and placed across the stricture, fol-lowed by stent deployment under both endoscopic and fluoro-scopic view. The length of the selected stent is based on theestimated length of the stricture at endoscopy or following fluo-roscopic contrast assessment.
In the series by Lee et al,12 19 patients underwent the with-drawal–reinsertion technique as a rescue procedure for failedconventional palliative stent placement for malignant small bowelobstruction. Small intestinal obstruction was due to metastaticgastric (n ¼ 15), colorectal (n ¼ 2), and primary small bowel cancer(n ¼ 2), and the obstruction sites were in the efferent jejunal limb(53%), proximal jejunum (32%), or third portion of the duodenum(15%). The technical success rate was 95%, and the clinical successrate, defined as relief of obstructive symptoms after stent place-ment, was 84%. No major procedure-related adverse eventsoccurred. Stent migration and restenosis occurred in 11% and 21% ofpatients, respectively, with median stent patency duration of 67days.12 Potential drawbacks of this technique include the risk oflosing the guide-wire with the unfolding of small bowel pleatsduring the removal of the deep enteroscope or during the insertionof the second endoscope, as well as looping of the conventionalendoscope in the stomach despite its advancement over the guide-wire. This technique may be more suited for proximally situatedsmall bowel lesions, but not likely to succeed for obstructing lesionslocated in the mid-distal jejunum and beyond.
Through-the-overtube technique
The through-the-overtube technique for placement of stents inthe mid gut has been described for all three deep enteroscopy in-struments. Data regarding this technique are currently limited tocase reports and small series (Table 1).13–20
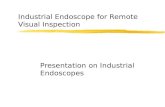
The technique involves the use of the dedicated balloon-assistedor spiral overtubes as conduits for placement of esophageal orenteral SEMS through malignant mid-gut obstruction under fluo-roscopic guidance (Fig. 2). The procedure is relatively similar for allthree enteroscopic systems, albeit with technical nuances tocompensate for length discordance between overtubes and stentdelivery catheters.
In brief, a deep enteroscope with balloon-assisted or spiralovertube is advanced to the stricture site. With the tip of the

Table 1 Deep Enteroscopy Overtube-Assisted Stent Placement for Malignant Small Bowel Obstruction
Study N Location of malignant obstruction Stent Endoscope Route of insertion Clinical success* AE
Yamamoto et al 200413 2 NR EsophagealUltraflex
DBE NR NR No
Ross et al 200615 1 Distal duodenum EsophagealUltraflex
DBE Oral Yes No
Kita et al 200714 6 NR NR DBE Oral/Anal NR NRPérez-Cuadrado et al 201318 1 Distal jejunum Enteral
Taewoong Niti-SDBE Oral Yes No
Popa et al 201417 1 Proximal jejunum EnteralWallflex
DBE Oral Yes No
Espinel and Pinedo 201119 1 Distal duodenum EnteralWallflex
SBE Oral Yes No
Lennon et al 201020 2 Proximal jejunum EnteralWallflex
SE Oral Yes No
AE, adverse events; DBE, double balloon enteroscope, NR, not reported; SBE, single balloon enteroscope; SE, spiral enteroscope.* Defined as ability to tolerate at least a liquid diet.
Gastrointestinal Intervention 2014 3(1), 30–3432
overtube anchored closely to the site of obstruction, pull maneu-vers are performed to reduce loop formation proximal to the ste-notic site and to maintain an overtube configuration in thestraightest and shortest path possible to facilitate passage of thestent’s delivery catheters, which are relatively stiff and inflexible.Although SE has a lower insertion depth than DBE, it may providebetter anchoring and a more stable platform than balloon over-tubes, which can slip.20
Once in position at the obstruction site, the length of the stric-ture can be assessed endoscopically or by fluoroscopic contrastinstillation if the enteroscope cannot traverse the stricture. Afluoroscopic marker (endoscopic clip or intramural contrast injec-tion) can be placed to identify the proximal and/or distal end (iftraversed) of the stricture. Thereafter, a long guide-wire isadvanced as far as feasible beyond the stricture, followed by
Fig. 2. Schematic layout of mid-gut stent placement using double balloon enteroscopy. (A)(B) Guide-wire advancement beyond the obstruction. (C) Enteroscope removal leaving overthe stent’s delivery system across the obstruction. (E) Stent deployment under fluoroscopic
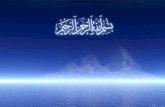
withdrawal of the enteroscope while leaving the guide-wire andovertube in place. For DBE, withdrawal of the enteroscope throughits overtube can be problematic and may result in loss of theovertube position owing to the traction force required to disruptthe manufacturer’s rubber band used to affix the enteroscope’sballoon at its tip. As an alternative, the enteroscope’s balloon can beaffixed with a suture instead of the rubber band, enabling theretraction of the enteroscope into the overtube while preservingthe double-balloon maneuvers unique to DBE (Fig. 3). Anothercaveat is that the stent’s delivery catheter (e.g., esophageal SEMS)may not be long enough to pass through the entire length of theovertube, in addition to the stricture site. One solution is tomake anincision with a scalpel through the lining of the overtube close tothe mouth and transfer the guide-wire so it exits through theincision site. Of note, caution is warranted to make the incision
Instrument advancement to the site of obstruction with balloon anchoring of overtube.tube and guide-wire in place. (D) Through-the-overtube and over-the-wire insertion ofview.

Fig. 3. Modification of balloon fixation at the tip of the endoscope. (A) Replacement of the standard rubber band with silk suture to affix the balloon at the tip of the endoscope. (B)This allows retraction of the balloon-loaded enteroscope through the overtube and (C) preserves the double balloon maneuvers unique to double balloon enteroscopy.
Esha Baichoo and Louis M. Wong Kee Song / Stenting mid-gut obstruction 33
away from the internal tubing that supplies air insufflation to theovertube balloon. This maneuver can significantly truncate thedistance from the mouth to the obstruction site and enable theselection of a shorter stent delivery system to reach its target(Fig. 4). Another alternative is to use the short DBE instrument, ifavailable, which has an overtube length of 105 cm as opposed to145 cm for the standard DBE overtube.18
Under fluoroscopic view, the selected stent’s delivery catheter isadvanced over the guide-wire and through the overtube forplacement across the stricture. To avoid inadvertent deployment ofthe proximal flange of the stent in the overtube, distal-releaseesophageal or enteral SEMS is used and partially deployed. Theovertube is subsequently retracted at a safe distance from theproximal aspect of the stricture and the stent is then completelyreleased.
After stent deployment, the enteroscope can be reintroducedthrough the overtube to confirm satisfactory positioning (Fig. 5).Contrast flush can also be administered to confirm free flow andpatency of the stent.
Alternative methods for stent placement in the mid gut
Oral or rectal routes of endoscopic stent delivery in the mid gutare not always feasible, particularly in the setting of altered gutanatomy. Percutaneous insertion of enteral SEMS in themid gut hasbeen described in such cases, usually after a failed endoscopicattempt at stent placement. Percutaneous routes utilized for enteralSEMS placement have included percutaneous endoscopic duode-nostomy, percutaneous tube enterostomy, and percutaneoustranshepatic cholangiostomy. In a review by Zhang et al,3 an esti-mated 10.5% and 9.3% of enteral stents were deployed usingpercutaneous endoscopic duodenostomy/percutaneous tube en-terostomy and percutaneous transhepatic cholangiostomy,respectively. The major indication for percutaneous placement of
Fig. 4. Technique for passage of shorter length stent’s delivery catheter through overtube oscalpel. (B) Transfer of the guide-wire (arrow) so it exits through the incision site. (C) Sho(rather than the proximal end of the overtube) to the obstruction site.
an enteral stent was for palliation of malignant obstructions inpatients with surgically altered gut anatomy, particularly at anafferent loop.
Other radiological interventions include percutaneous radio-logical jejunostomy long tube placement following jejunopexy todecompress the small bowel proximal to the obstruction and toprovide a route via the percutaneous radiological jejunostomy forsubsequent SEMS placement to palliate one or more small bowelobstructions. In one study, clinical success using this technique wasachieved in 18 of 21 patients (85.7%), although major (peritonitis)and minor procedure-related adverse events occurred in 4.8% and28.6% of patients, respectively.21
Percutaneous stent placement requires a matured fistulizedtract, a process that typically takes 1 month on average. This delayis not suitable for acutely ill patients. Furthermore, endoscopepassage through the percutaneous tract is limited by the diameterof the tract, greatly restricting the size of endoscopes that can beused. To circumvent the need for a matured tract and subsequentdelay in stenting, a percutaneous assisted transprosthetic endo-scopic therapy (PATENT) procedure has been proposed, whereby acovered SEMS is deployed through a freshly created enter-ocutaneous tract secured by T-tags.22 The secured expansion of thetract with the SEMS allows a one-step transprosthetic procedureand the possibility for repeated interventions using therapeuticendoscopes. The PATENT procedure has been described in proof-of-concept studies, including single-session antegrade endo-scopic retrograde cholangiopancreatography (ERCP) through afresh PEG tract in patients with a Roux-en-Y gastric bypass,23
drainage of the gallbladder through an SEMS-secured chol-ecystostomy tract,24 and transprosthetic access through a PEGtract to control a bleeding ulcer at a gastrojejunal anastomosisusing a standard upper endoscope.25 The PATENT technique maynot only be applicable for palliation of malignant mid-gutobstruction, but also for a variety of benign small intestinal
f double balloon endoscope. (A) Incision through overtube close to the mouth using artened over-the-wire travel distance for the stent’s delivery catheter from the mouth

Fig. 5. Mid gut stent placement via single balloon enteroscopy. (A) Malignant mid jejunal obstruction with proximal bowel dilation on computed tomography. (B) Advancement ofsingle balloon enteroscope to the site of obstruction. (C) Enteroscopic and fluoroscopic confirmation of satisfactory stent deployment across the obstruction.
Gastrointestinal Intervention 2014 3(1), 30–3434
conditions, including placement of biodegradable or drug-elutingstents to manage Crohn’s strictures not accessible by standardendoscopes.
Future directions
Deep enteroscopic stent placement for malignant mid-gutobstruction beyond the reach of conventional endoscopes is anappealing option in patients who are deemed poor surgical can-didates. Relative to surgery, stent placement allows for amore rapidreturn to functional bowel status, with shorter hospital stay and alower rate of early adverse events. However, stent insertion deep inthe mid gut is a technically challenging and complex procedure,requiring the inventive use of currently available deep enteroscopyinstruments and SEMS not specifically suited for that purpose. Stentplacement for deep small bowel obstruction represents the lastfrontier for gastrointestinal endoscopic stenting. The developmentof new enteroscopes that allow TTS stent placement and/or novelhighly flexible stent designs compatible with current enteroscopeswill facilitate endoscopic stenting of the mid gut, with the appli-cation extending beyond palliation in the foreseeable future.26
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Baron TH. Expandable metal stents for the treatment of cancerous obstructionof the gastrointestinal tract. N Engl J Med. 2001;344:1681–7.
2. ASGE Technology CommitteeVaradarajulu S, Banerjee S, Barth B, Desilets D,Kaul V, et al. Enteral stents. Gastrointest Endosc. 2011;74:455–64.
3. Zhang F, Amateau SK, Khashab MA, Okolo PI. Mid-gut stents. Curr Opin Gas-troenterol. 2012;28:451–60.
4. Jeurnink SM, Repici A, Luigiano C, Pagano N, Kuipers EJ, Siersema PD. Use of acolonoscope for distal duodenal stent placement in patients with malignantobstruction. Surg Endosc. 2009;23:562–7.
5. Jeurnink SM, Steyerberg EW, van Hooft JE, van Eijck CH, Schwartz MP,Vleggaar FP, et al. Surgical gastrojejunostomy or endoscopic stent placementfor the palliation of malignant gastric outlet obstruction (SUSTENT study): amulticenter randomized trial. Gastrointest Endosc. 2010;71:490–9.
6. Kawata N, Kakushima N, Tanaka M, Sawai H, Imai K, Hagiwara T, et al.Percutaneous endoscopic gastrostomy for decompression of malignant bowelobstruction. Dig Endosc. 2014;26:208–13.
7. Elena RM, Riccardo U, Rossella C, Bizzotto A, Domenico G, Guido C. Currentstatus of device-assisted enteroscopy: technical matters, indication, limits andcomplications. World J Gastrointest Endosc. 2012;4:453–61.
8. Jeon SR, Kim JO. Deep enteroscopy: which technique will survive? Clin Endosc.2013;46:480–5.
9. ASGE Technology CommitteeTierney WM, Adler DG, Conway JD, Diehl DL,Farraye FA, et al. Overtube use in gastrointestinal endoscopy. GastrointestEndosc. 2009;70:828–34.
10. Fiori E, Lamazza A, Demasi E, Decesare A, Schillaci A, Sterpetti AV. Endoscopicstenting for gastric outlet obstruction in patientswith unresectable antro pyloriccancer. Systematic review of the literature and final results of a prospectivestudy. The point of view of a surgical group. Am J Surg. 2013;206:210–7.
11. Park JJ, Cheon JH. Malignant small bowel obstruction: the last frontier forgastrointestinal stenting. J Gastroenterol Hepatol. 2012;27:1136–7.
12. Lee H, Park JC, Shin SK, Lee SK, Lee YC. Preliminary study of enteroscopy-guided, self-expandable metal stent placement for malignant small bowelobstruction. J Gastroenterol Hepatol. 2012;27:1181–6.
13. Yamamoto H, Kita H, Sunada K, Hayashi Y, Sato H, Yano T, et al. Clinical out-comes of double-balloon endoscopy for the diagnosis and treatment of small-intestinal diseases. Clin Gastroenterol Hepatol. 2004;2:1010–6.
14. Kita H, Yamamoto H, Yano T, Miyata T, Iwamoto M, Sunada K, et al. Doubleballoon endoscopy in two hundred fifty cases for the diagnosis and treatmentof small intestinal disorders. Inflammopharmacology. 2007;15:74–7.
15. Ross A, Semrad C, Waxman I, Dye C. Enteral stent placement by double balloonenteroscopy for palliation of malignant small bowel obstruction. GastrointestEndosc. 2006;64:835–6.
16. Ross AS, Dye C, Waxman I. Enteral stent placement and small bowel balloondilation using double balloon enteroscopy. Tech Gastrointest Endosc. 2008;10:119–23.
17. Popa D, Ramesh J, Peter S, Wilcox CM, Mönkemüller K. Small bowel stent-in-stent placement for malignant small bowel obstruction using a balloon-assisted overtube technique. Clin Endosc. 2014;47:108–11.
18. Pérez-Cuadrado E, Carballo F, Latorre R, Soria F, López-Albors O. An endoscopictechnique for treating symptomatic distal jejunum obstruction by leaving theovertube in place. Rev Esp Enferm Dig. 2013;105:107–9.
19. Espinel J, Pinedo E. A simplified method for stent placement in the distal du-odenum: enteroscopy overtube. World J Gastrointest Endosc. 2011;3:225–7.
20. Lennon AM, Chandrasekhara V, Shin EJ, Okolo PI. Spiral-enteroscopy–assistedenteral stent placement for palliation of malignant small-bowel obstruction(with video). Gastrointest Endosc. 2010;71:422–5.
21. Kim YJ, Yoon CJ, Seong NJ, Kang SG, An SW, Woo YN. Safety and efficacy ofradiological percutaneous jejunostomy for decompression of malignant smallbowel obstruction. Eur Radiol. 2013;23:2747–53.
22. Baron TH, Wong Kee Song LM. Percutaneous assisted transprosthetic endo-scopic therapy (PATENT): expanding gut access to infinity and beyond! (withvideo). Gastrointest Endosc. 2012;76:641–4.
23. Law R, Wong Kee Song LM, Petersen BT, Baron TH. Single-session ERCP inpatients with previous Roux-en-Y gastric bypass using percutaneous-assistedtransprosthetic endoscopic therapy: a case series. Endoscopy. 2013;45:671–5.
24. Abu Dayyeh BK, Baron TH. Development of a hybrid percutaneous–endoscopicapproach for the complete clearance of gallstones. Clin Gastroenterol Hepatol.2012;10:947–9.
25. Baron TH, Wong Kee Song LM. Placement of an esophageal self-expandablemetal stent through a percutaneous endoscopic gastrostomy tract, for endo-scopic therapy of upper gastrointestinal bleeding. Endoscopy. 2012;44(Suppl. 2UCTN):E319–20.
26. Rejchrt S, Kopacova M, Brozik J, Bures J. Biodegradable stents for the treatmentof benign stenoses of the small and large intestines. Endoscopy. 2011;43:911–7.