
Palliative cancer care in Uganda Palliativ cancervård i...
30
Institutionen för Neurobiologi, Vårdvetenskap och Samhälle Sektionen för omvårdnad Sjuksköterskeprogrammet Examensarbete i omvårdnad 15 hp _____________________________________________________________ Palliative cancer care in Uganda The Nurse experience Palliativ cancervård i Uganda Sjuksköterskors erfarenheter Författare: Karoline Ekblad och Sara Dorrian Handledare: Lena Wettergren, Institutionen för Neurologi, Vårdvetenskap och Samhälle Examinator: Kristiina Heikkilä, Institutionen för Neurologi, Vårdvetenskap och Samhälle
Transcript of Palliative cancer care in Uganda Palliativ cancervård i...
Institutionen för Neurobiologi,
Vårdvetenskap och Samhälle
Sektionen för omvårdnad
Sjuksköterskeprogrammet
Examensarbete i omvårdnad 15 hp
_____________________________________________________________
Palliative cancer care in Uganda
The Nurse experience
Palliativ cancervård i Uganda
Sjuksköterskors erfarenheter
Författare: Karoline Ekblad och Sara Dorrian
Handledare: Lena Wettergren, Institutionen för Neurologi, Vårdvetenskap
och Samhälle
Examinator: Kristiina Heikkilä, Institutionen för Neurologi, Vårdvetenskap
och Samhälle
Sammanfattning
Bakgrund: Cancer ökar globalt och Uganda är ett av de länder som är beräknat att drabbas
påtagligt av ökningen. Cancervård i Uganda är underfinansierat och omkring 30 % av
cancerpatienter i låginkomstländer som till exempel Uganda får palliativvård. Sjuksköterskan
har en nyckelroll inom den givna cancervården.
Syfte: Syftet med studien var att beskriva palliativ cancervård i Uganda utifrån
sjuksköterskors erfarenheter.
Metod: En kvalitativ metod har använts. Data har samlats in genom semistrukturerade
intervjuer med sex sjuksköterskor anställda på Ugandas cancer institut. Ett bekvämlighets
urval användes och informerat samtycke erhölls. Intervjuerna transkriberades och data
analyserades med hjälp av så kallad kvalitativ innehållsanalys.
Resultat: Följande tre kategorier utgjorde resultatet: Utmaningar, Lindra lidande och
Betydande relationer.
Slutsats: Att ge cancervård i Uganda innebär ett flertal utmaningar. Underfinansiering leder
till att patienter avlider till följd av brist på nödvändiga resurser. Patienters lidande kan lindras
genom smärtlindring och interaktion. Sjuksköterskorna kommer patienterna nära och blir
beroende av anhöriga i omvårdnaden.
Abstract
Background: Cancer is increasing globally and Uganda is estimated to be particularly
effected. Cancer care in Uganda is underfunded and about 30 % of the cancer patients in low-
income countries such as Uganda are being given palliative care. Nurses play a core role in
providing the care to the patients.
Aim: The aim of the study was to describe palliative cancer care in Uganda as shown through
the nurse experience.
Method: A qualitative method was used and the data was collected by semi-structured
interviews with six nurses working at the UCI. The sample was selected using convenience
sampling and informed consent was obtained. The interviews were transcribed and the data
was analysed using content analysis.
Results: The three following categories constitute the result: The challenges, Easing suffering
and Significant relationships.
Conclusion: Cancer care in Uganda is seen to face major challenges. The financial
underfunding leads to lack of necessary resources, and it so happens patients die due to severe
shortages. Patient suffering is eased by pain control and interaction. The nurses become
attached to the cancer patients and the caregivers are needed to provide acceptable care.

Acknowledgements
We would like to thank Jackson Orem and Victoria Walunsansa at the Uganda Cancer
Institute (UCI) for generously allowing us to carry out our study and all the staff involved for
their valuable help. To our supervisors, Lena Wettergren, Rose Nabirye and Allen Naamala,
we would like to give a deep appreciation of the encouragement and guidance you gave us.
Also we would like to thank Tom Ngabirano for his appreciated assistance. We wish to
express our gratitude toward the Department of womens and childrens health at Uppsala
University and the Swedish International Development Cooperation Agency (SIDA) who
granted us minor field study (MFS) scholarships. Last but not least a special thanks to our
families and friends for their love and support.
Table of Contents
1. Introduction ............................................................................................................................ 1
2. Background ............................................................................................................................ 2
2.1 The cancer burden ........................................................................................................ 2
2.2 Health care in Uganda .................................................................................................. 2
2.3 Cancer care in Uganda ................................................................................................. 3
2.4 Palliative care ............................................................................................................... 3
2.5 Problem statement ........................................................................................................ 4
3. Aim ......................................................................................................................................... 5
4. Method ................................................................................................................................... 6
4.1 Data collection .............................................................................................................. 6
4.2 Data analysis ................................................................................................................ 6
4.3 Ethical considerations .................................................................................................. 7
5. Results .................................................................................................................................... 8
5.1 The challenges .................................................................................................................. 8
5.1.1 Poverty ...................................................................................................................... 8
5.1.2 Lack of resources ...................................................................................................... 9
5.1.3 Lack of staff .............................................................................................................. 9
5.1.4 Patients lack of knowledge regarding cancer .......................................................... 10
5.1.5 Wish for specialisation ............................................................................................ 10
5.2 Easing suffering .............................................................................................................. 10
5.2.1 Holistic perspective ................................................................................................. 10
5.2.2 Pain control ............................................................................................................. 10
5.2.3 Interaction ................................................................................................................ 11
5.3 Significant relationships ................................................................................................. 11
5.3.1 Attachment .............................................................................................................. 11
5.3.2 Depending on caregivers ......................................................................................... 11
6. Discussion ............................................................................................................................ 12
6.1 Method discussion ...................................................................................................... 12
6.2 Result discussion ........................................................................................................ 13
6.3 Relevance for nursing science and society ................................................................. 14
6.4 Conclusion .................................................................................................................. 15
References ................................................................................................................................ 16
Appendix 1 ............................................................................................................................... 19
Appendix 2 ............................................................................................................................... 21

1
1. Introduction The idea to conduct our bachelor thesis abroad developed during an exchange program we
participated in Sydney in the spring of 2012. We were both intrigued by practising health care
outside Sweden. Our curiosity and interest lead us to contact a teacher and professor at the
Nursing department at Karolinska Institutet who was conducting research in Uganda. This
resulted in the UCI agreeing to host our study project and with financial assistance from
MFS-scholarships we were enabled to spend a period of eight weeks in Uganda. The UCI is
one of the major cancer research and treatment centres in Uganda and it was a great
opportunity for us to conduct this study there. Once we started to read about cancer care in
Uganda we began to appreciate the complexities within this field of work, and we realised
that it should be interesting to study. We will soon be registered nurses and therefore it was
motivating to have nurses share their experiences of giving care.
2
2. Background 2.1 The cancer burden
Cancer is one of the leading causes of death worldwide and in 2008 it accounted for 7.6
million deaths (World Health Organization (WHO), 2010). About 70 % of these deaths
occurred in low- and middle-income countries. The numbers of people diagnosed with cancer
is increasing and by 2030 it is estimated that 13.1 million people will die of cancer (WHO,
2010). This increase will mostly be in low-income countries and Sub-Saharan Africa is
predicted to be particularly effected (Thun, DeLancey, Center, Jemal, A, Ward, 2009). In this
region 70% of diagnosed cancer patients died in 2007 (Harding et al., 2011). According to
Okuku et al. (2013) HIV is one major factor for the cancer increase in Sub-Saharan Africa
and it is estimated that 30% of the cancer cases are related to infections. Changing lifestyles
due to economic growth and increasing age of the population are other reasons for this
increase (Parkin et al., 2008).
Uganda is located on the east coast of Sub-Saharan Africa and is seen to have a high cancer
burden (Parkin, Nambooze, Wabwire-Mangen & Wabinga 2010). It has a population of 32
million people and each year approximately 22 000 people die in Uganda due to cancer
(Okuku et al., 2013). The most common cancer types among male adult patients in Kampala
(Uganda) is prostate cancer and Kaposi’s sarcoma, while cervix and breast cancer is most
common amongst females (Parkin et al., 2010). Cancer among children has increased rapidly
without known reason, the most common type being leukaemia in 2000. In general, cancer
patients in Uganda are diagnosed and treated in the later stages of their illness, which is
reflected in the high mortality rate. The fact that cancer treatment is expensive is a
contributing factor for this outcome (Orem & Wabinga, 2009).
2.2 Health care in Uganda
The health sector in Uganda consists of a private and a public part. The Ministry of Health
(MOH), a department of the Ugandan government, published the second National Health
Policy (NHP II) (2010) that describes the their strategies for health care. The focus of the
policy is health promotion, disease prevention, early diagnosis and treatment of disease. It
states that the government is obliged to provide all people with basic health care. However
Zikusooka, Kyomuhang, Orem and Tumwine (2009) claims that it is difficult to achieve due
to the sector being largely underfunded. According to Utrikesdepartementet (2010) only 9 %
of the national budget goes to the health care sector, pointing out that it is underfunded. Public
health services in Uganda are for free but are lacking in quality, accessibility and provision of
medicines (Zikusooka et al., 2009).
Nurses are one part of the health care system and there is a global shortage of them, especially
in Sub-Saharan Africa (WHO, 2006). In Uganda one reason for the shortage is that nursing
students prefer to work abroad due to low salaries in Uganda (Nguyen et al., 2008). Since
nurses and their services have been recognized by the WHO (2001) as the core of the health
care system the lack of them in countries such as Uganda is critical. To become a nurse in
Uganda you can either study to get a certificate, diploma or degree. To obtain the degree it is
required to attend the Bachelor of Nursing Science programme (BNSc) at university level.
The degree is a four-year education including one year of paid internship and a bachelor in
midwifery. The diploma requires three and a certificate two years of studies (P. Wampaalu,
personal communication, February 24, 2013).
3
2.3 Cancer care in Uganda
As in many African countries cancer care in Uganda is a low priority for governments (Parkin
et al., 2008). Orem and Wabinga (2009) discuss several barriers for cancer care in Uganda
and other African countries. Low political priority resulting in underfunding is one. Other
barriers are the large increase of cancer patients, low cancer awareness in the population and
lack of specialized health care workers. Additional limitations such as lacks of capacity for
diagnose and treatment as well as expensive medicines adds up to a challenging situation.
Cancer screening, treatment and management in Uganda is carried out mainly from two
centers, The Uganda Cancer Institute (UCI) and St Mary’s Hospital. The UCI started in 1967
and is funded by the Ministry of health. The institute consists of four departments:
Lymphoma treatment center (LTC), Solid tumor center (STC), Outpatient department (OPD)
and the Private department. The LTC and STC are the inpatient care departments. At the
moment there are 67 nurses working at the UCI, none of whom has a specialisation in
oncology. Furthermore there is no nursing oncology education in Uganda (A. Naamala,
personal communication, January 25, 2013). Approximately 2000 newly diagnosed cancer
patients get admitted to the UCI annually (Okuku et al., 2013). In order to treat cancer one or
any combination of chemotherapy, surgery and radiotherapy can be applied. Chemotherapy is
given to the patients at the UCI and it is normally administrated in cycles. A cycle may last
from one to several days and it can be one drug or a combination of several used in the same
cycle (Hansson, Henriksson & Petersson, 2008, p. 185). Chemotherapy has a negative effect
on the bone marrows production of platelets and leukocytes, which can lead to weeks of
leuko- and thrombocytopenia, and thus increase the risk of severe haemorrhage and infections
(Hansson et al., 2008, p. 211). Other acute side effects of chemotherapy include vomiting,
diarrhoea, fever, pain and fatigue (McGarvey, Baum, Pinkerton & Rogers, 2001). To perform
surgery and radiotherapy the UCI collaborate with Mulago Hospital. Much of the care at the
UCI is palliative and for advice and support the institute work together with the Hospice
Africa Uganda (HAU) (A. Naamala, personal communication, January 25, 2013). The HAU
is a centre that provides and facilitates palliative care in Uganda and other African countries.
2.4 Palliative care
According to the WHO (2013) the majority of cancer patients get in contact with health care
when they are in a late stage of their illness, making most of the care palliative in nature.
About 30% of the cancer patients in low-income countries are estimated to be managed
palliative (Okuku et al., 2013).
WHO (2013) define palliative care:
Palliative care is an approach that improves the quality of life of patients and their
families facing the problems associated with life threatening illness, through the
prevention and relief of suffering by means of early identification and impeccable
assessment and treatment of pain and other problems, physical, psychosocial and
spiritual. (WHO, 2013, http://www.who.int/cancer/palliative/definition/en/).
As presented in the definition easing suffering is one part of palliative care. Jakobsson,
Andersson & Öhlén (2009, p. 345) recognise reducing suffering as the overall purpose within
palliative care. Suffering is something that everyone has to face in their life and it is has to be
taken into consideration when providing care. The experience of suffering is affected by the
individual and the surrounding tradition and culture (Wiklund, 2009, p. 296). Pain and illness
can lead to suffering but it does not necessarily need to be so. It is rather the meaning of pain
and illness for the patient that decides the amount of suffering they experience (Seymour &

4
Ingelton, 2008). Easing patient suffering is one of the major responsibilities for a nurse
(International council of Nurses, 2007).
The HAU presented palliative medicine for the first time in 1993. Mwangi-Powell (2012)
means that even though Uganda can provide some excellent institutions for palliative care, it
is not sufficient to meet the needs. The care needs required for patients in Uganda are
presented by Harding et al. (2011) and it shows that the primary needs were pain control and
psychological support. Harding and Higginson (2005); Merriman (1996); Harding et al.
(2011) point out that control of pain is important within palliative care, but unfortunately they
describe a shortage of opioid availability. Except for control of pain the palliative care
patients in Uganda and other African countries need spiritual, emotional and financial support
(Harding & Higginson, 2005). Selman et al. (2011) describe that for patients receiving
palliative care in Uganda close relationships were highly important. However for patients in a
hospital family members might not be able to come and visit due to transportations costs
(Gysels, Pell, Straus & Pool, 2011).
For patients that get admitted to the UCI it is usually required that they have a caregiver with
them. A caregiver is often a family member or a friend. This is because the caregiver is
needed to be a part of the care, for example to feed and manage side-effects of chemotherapy
(A. Naamala, personal communication, February 25, 2013). It is well known that caregivers
of palliative patients are experiencing financial and psychological burdens (Gysels et al.,
2011) Providing the patients with food, medicine and water leads to impoverishment and the
emotional demands can sometimes lead to depression. The caregiver’s burden of palliative
care is mentioned to be worsened by the lack of hospital resources such as drugs, beds and
staff.
2.5 Problem statement
Cancer is increasing globally and Uganda is expected to be particularly effected. With an
increasing number of patients follows an increased need of cancer care. Uganda and other
African countries are facing challenges in providing cancer care due to health care being
underfunded. The patients usually get admitted for treatment in a late stage and one third of
the world’s cancer patients are being treated palliative. As a nurse you can work anywhere in
the world, and it also means that you can give care to patients from many different cultures. It
is therefore crucial as well as valuable to conduct studies like this one. Nurses play a key role
in providing care to the patients, making it important to present their experiences.

5
3. Aim The aim of the study was to describe palliative cancer care in Uganda as shown through the
experiences of nurses.
The specific research questions were:
1. What kinds of challenges are described?
2. How is patients suffering eased?
3. What do nurses think around giving care?

6
4. Method
In this study a qualitative method was suitable since the aim was based on individual
experiences (Holloway & Todres, 2006, p.193). The approach was inductive, which means
working from empirical data to theory (Polit & Beck, 2010, p. 13).
4.1 Data collection
Individual face-to-face interviews were conducted with nurses working at the UCI. The
method of using personal interviews is considered to lead to high quality data and the
possibility to get rich answers (Polit & Beck, 2010, p. 295).
The sample included six informants, they were chosen through convenience sampling, which
often is efficient. It was also chosen due to time limitation that occurred during the process.
The sample selection began at the UCI when the chief nurse asked who of the nurses were
willing to participate. A schedule for the interviews was arranged. The including criteria were
at least two years of working experience with cancer care and to be fluent in English. The
interviews were conducted during working hours and when it was possible within the daily
work schedule. The interviews were performed in two different settings at the institute. Four
interviews were held in the UCI boardroom and two were held in the counselling room at the
LTC department. The students performed three interviews each. During two of the interviews
both students were present, one acted as the interviewer and the other one as an observer. The
interviews lasted between 30-90 minutes and they were audio recorded. The interviews were
conducted with semi-structured questions, which according to Polit and Beck (2010, p. 341)
encourage the informants to talk without restraint. The questions were prepared in an
interview guide. See appendix 1.
4.2 Data analysis
The student who conducted the interview transcribed the audio recording. The transcriptions
were made the same day as the interview, since it is of importance that it reflects the totality
of the interview experience (Polit & Beck, 2010, p. 465). To be able to separate the interviews
and to preserve confidentiality they were coded. The data was analysed according to
qualitative content analysis, as described by Granheim and Lundman (2008). This method is
suitable for analysing transcribed data from interviews since it focuses on interpretations of
text material. To get a deep understanding for the material the students read all transcriptions
several times. Then meaning units were identified, which are parts of the transcripts that can
be connected together according to the content, for example through similar words or
sentences. Each meaning unit were condensed to make the material shorter and easier to
handle. The condensed meaning units were given codes, which briefly describe the content of
the meaning unit. By collecting the codes with similar content sub-categories were created.
These sub-categories could then come together and create major categories. It is pointed out
that the content within the categories should be similar but that the categories compared to
each other should differ.
7
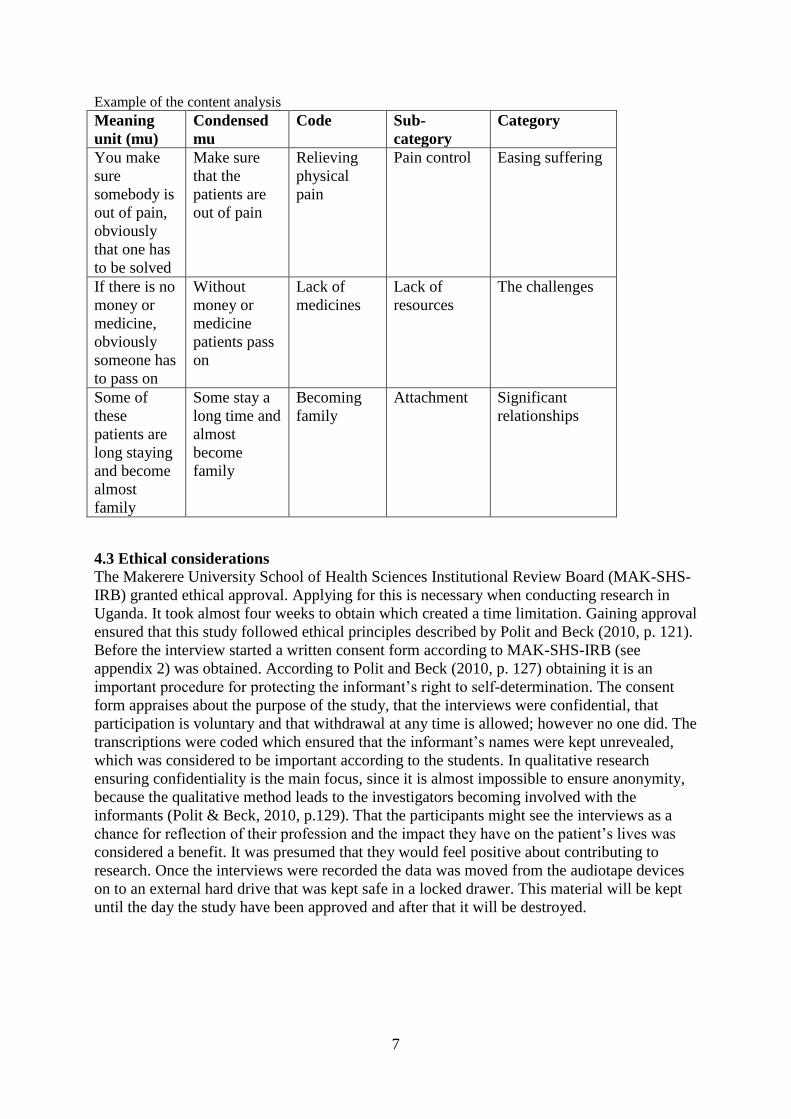
Example of the content analysis
Meaning
unit (mu)
Condensed
mu
Code Sub-
category
Category
You make
sure
somebody is
out of pain,
obviously
that one has
to be solved
Make sure
that the
patients are
out of pain
Relieving
physical
pain
Pain control Easing suffering
If there is no
money or
medicine,
obviously
someone has
to pass on
Without
money or
medicine
patients pass
on
Lack of
medicines
Lack of
resources
The challenges
Some of
these
patients are
long staying
and become
almost
family
Some stay a
long time and
almost
become
family
Becoming
family
Attachment Significant
relationships
4.3 Ethical considerations
The Makerere University School of Health Sciences Institutional Review Board (MAK-SHS-
IRB) granted ethical approval. Applying for this is necessary when conducting research in
Uganda. It took almost four weeks to obtain which created a time limitation. Gaining approval
ensured that this study followed ethical principles described by Polit and Beck (2010, p. 121).
Before the interview started a written consent form according to MAK-SHS-IRB (see
appendix 2) was obtained. According to Polit and Beck (2010, p. 127) obtaining it is an
important procedure for protecting the informant’s right to self-determination. The consent
form appraises about the purpose of the study, that the interviews were confidential, that
participation is voluntary and that withdrawal at any time is allowed; however no one did. The
transcriptions were coded which ensured that the informant’s names were kept unrevealed,
which was considered to be important according to the students. In qualitative research
ensuring confidentiality is the main focus, since it is almost impossible to ensure anonymity,
because the qualitative method leads to the investigators becoming involved with the
informants (Polit & Beck, 2010, p.129). That the participants might see the interviews as a
chance for reflection of their profession and the impact they have on the patient’s lives was
considered a benefit. It was presumed that they would feel positive about contributing to
research. Once the interviews were recorded the data was moved from the audiotape devices
on to an external hard drive that was kept safe in a locked drawer. This material will be kept
until the day the study have been approved and after that it will be destroyed.

8
5. Results
The sample consisted of six female informants with different educational levels and working
experience. Their working experience expressed in a median was four years.
The result will be presented below, in three categories. The first category is “The challenges”
and it contains five sub-categories: poverty, lack of resources, lack of staff, patients’ lack of
knowledge regarding cancer and wish for specialisation. The second category is “Easing
suffering” and it contains three sub-categories: holistic perspective, pain control and
interaction. The third and last category is “Significant relationships” and it contains two sub-
categories: attachment and depending on caregivers.
The main findings when interviewing the informants were the challenges they face when
working within palliative cancer care. Descriptions regarding patients’ poverty, lack of
resources, staff and knowledge are central in the result. Furthermore the informants shared
information on their thoughts about easing patient suffering. They also described how
significant relationships to patients and their caregivers are a part of the care.
5.1 The challenges The statements included that the poverty of the patients is a challenge within the palliative
cancer care. The informants describe how essential resources and staff are lacking.
Furthermore patients are lacking knowledge about cancer and specialized nursing education is
missing. “Challenges” is the major category in the result since it was the main issue brought
up by the informants themselves during the interviews. The category derived from the
following sub-categories: poverty, lack of resources, lack of staff, lack of knowledge and lack
of specialization.
5.1.1 Poverty
It is explained that the patients who seek care are very poor. To get treatment the patients may
have to pay for drugs themselves whenever it runs out of stock at the institute. Many patients
lack financial resources and it is difficult for them to afford the necessary drugs, in order to be
treated. Informant F tells that drugs are very expensive and because of poverty people die
premature. Sometimes patients and caregivers try to raise money by searching for funding but
it often fails due to poverty in the country. Informant D states: “Drugs drugs, the caregiver
could not raise money for the drugs…she had to pass on”. Informant B gives another example
A poor mother from a rural area with two children sick with Burkitt’s lymphoma. One
got treatment, had a relapse and then given palliative care. The other one has an
infection, resistant to the antibiotics free of charge at the hospital. Vancomycin would
help, but the mother could not afford it. It is very stressing due to the knowledge that the
boy could be fine (Informant B).
Informant C describes that when a child has cancer the parents can be forced to pay for
treatment, even though they cannot afford it. It is described that asking parents to pay for
drugs when they do not have money for food, or school fees can lead to depression and cause
trauma. If the patients get treatment there is another challenge because of poverty. Patients
might have difficulties to go back home from the hospital since transportation requires
money. Facing that dilemma informant E declares: “Once in a while you may have to give
from your own pocket for food, or to give them a little transport, if you can afford”. The
9
informants express a concern regarding the patients who need to come back to the hospital for
further treatment, saying that they might not be able to do so due to transportation costs.
5.1.2 Lack of resources
All of the informants describe lack in different resources such as medicine, materials,
equipment and space, as a challenge when giving care to the patients. Several informants
describe how everyday material such as gloves, swabs and cannulas are running out of stock,
one state: “When you do dressings, we don’t have materials, gloves and what, so we touch the
wounds by our own hands, it is disgusting”(Informant B). The supply of fluids and medicine
for the patients are not enough. Informant E means that when you do not have the right
material, you need to improvise to try and solve the problem the best you can. Furthermore
the lack of equipment is described as a challenge, and informant D explains that the ward only
has one blood pressure machine for all of the patients, so by the time you have taken the
blood pressure on the last patient the batteries are running low, and you end up with an invalid
result. It is mentioned that machines for taking electrocardiography is shared with Mulago
hospital, thus making the process for investigations slower. Several informants describe a
problem with providing oxygen because the cylinders are not enough and the concentrators
are depending on electricity, one state:
The boy was unconscious and he was put on oxygen for some days. So the oxygen was
provided through a concentrator were you have to use electricity. It happened that the
power went off…so this boy passed on there and then: So you ask yourself, if we had a
cylinder, maybe this wouldn’t happen (Informant A).
Lack of blood products to give to bleeding patients is also mentioned as a challenge and one
state: “It is difficult to get blood for those leukaemia patients. I think we lost a patient due to
that this weekend…”(Informant D). Several informants describe the confined working
environment as challenging since there are patients lying on mattresses on the floor and sitting
out on the veranda. Informant C exemplifies difficulties with putting in cannulas, when
someone is on the floor or, it might be difficult to find places to hang the fluid chemotherapy.
It is also described that with so few beds in relation to the number of patients, it can be
difficult to accommodate the patients through out the treatment.
The lack of resources lead to emotional distress amongst the informants, one state: “I get
reminded that this person dies because of these things missing, it makes you feel like you are
a part of the cause of death” (Informant A). Several informants also describe moral stress by
not being able to help the patients, due to lack of resources, and how this leads to frustration
since they cannot do the job as good as possible. It was mentioned that the lack in resources is
an economic issue on a political level, one state: “I can’t say it is the institution that is lacking
really but it is rather the country and the high officials…the institution actually does its best
“(Informant F).
5.1.3 Lack of staff
All the informants describe that there is a shortage of staff and one state: “The staff is limited,
we have very few nurses, you could say almost 1 nurse for 50 patients” (Informant E). Several
informants describe the situation as overwhelming due to few nurses working on the ward,
but also because of the increasing numbers of patients, one states: “Another challenge is the
shortage in staff…the number of patients’ increases, not that cancer is increasing now, but
more because people are starting to get aware of cancer, looking for treatment” (Informant
A).
10
Even though the numbers of patients are increasing, the informants describe that the number
of nurses is not. The work environment is described as hectic with a lot of things to be done
and the need to prioritize. Informant C points out that you sometimes are not able to do things
when they are urgent. The heavy workload and lack of staff leads to the informants working
overtime: “You may stay at work until 7 pm…it becomes voluntary work, but you have to do
it” (Informant B). It is mentioned, that working more hours is sometimes done, at the expense
of ones own family. Several informants describe, that the consequence of limited staff
resources, is that you do not have enough time for the patients.
5.1.4 Patients lack of knowledge regarding cancer
Several informants describe that various people in Uganda, believe cancer to be a curse. This
means a challenge when whenever giving care. Informant A says that some patients, do not
have the knowledge about what cancer is or what it means. It is described that many patients
do not understand reasons for developing cancer: “Some believe in myths, thinking they can
have been bewitched” (Informant B). Regarding knowledge about the cancer care and
treatment, some patients have unrealistic expectations of the help they seek: “Sometimes they
get here and they think one injection is enough, and that they later on can go back home”
(Informant A).
5.1.5 Wish for specialisation
The informants speak about a lack of knowledge within the cancer area they are working in. It
is stated that: “Cancer care is very big, I need to specialise in oncology. I am not doing it the
proper way” (Informant B). The informants state that lacking of oncology specialisation leads
to feeling inadequate and therefore making it challenging to provide care. Furthermore they
devotedly express a wish to improve their nursing skills, in order to be able to improve the
care they give to their patients by saying: “It is good to be a nurse, better to be an oncology
nurse”(Informant E).
5.2 Easing suffering It is described by the informants how patient suffering is eased. They describe different
aspects to consider, such as talking with patients and relieving them from pain. The category
derived from the following sub-categories: holistic perspective, pain control and interaction.
5.2.1 Holistic perspective
It is described that the patients are miserable and suffering and therefore many issues have to
be considered while giving care. One informant states following: “You must deal with them
medically, psychologically and emotionally…you have to apply all these aspects” (Informant
C). It is pointed out that there are a lot of aspects in easing suffering for the patients, such as
giving advice, hope and helping with anxiety. General nursing care is mentioned: “General
nursing care...the total care for the patient. The vitals, find out if your patient is eating well
and passing out, the input and output the weight. All those things we shall consider. The
comfort, everything” (Informant D).
5.2.2 Pain control Informant D describes pain as the major problem for the patients, and controlling the pain
should be addressed primarily. Several informants agree that the pain has to be managed
directly and one state: “You see our patients, they have that long time pain, that chronic pain.
Pain controllers are given, mainly morphine” (Informant A).
11
5.2.3 Interaction
Several informants describe that talking and interacting with the patients is an essential
intervention, when easing suffering, one state: “We have to talk to the patients, many of them
are too depressed, and they are too emotional, talking is necessary” (Informant C).
According to the informants, many patients are depressed and therefore talking with them, is
important in their care. Further they describe that the approach and the interaction ease
suffering and informant B claims counselling to be needed. Giving hope to the patients is an
additional intervention that is mentioned. It is described that this can be achieved by taking
the patients around the ward so they can meet other patients that are doing well.
5.3 Significant relationships In this category an attachment between the patients and the nurses, is described as a part of
the care. Further, it is explained how the nurses depend on caregivers to help them give care.
This category derived from following two sub-categories: attachment and depending on
caregivers.
5.3.1 Attachment
All informants describe how they get attached to the patients, since they take care of them for
a long time. Several informants describe the patients and the caregivers almost become
family: “Some of these patients are long staying and become almost family” (Informant C). A
devotion to the patients is expressed and informants describe, that they think about the
patients outside work. Since death is common within palliative cancer care, Informant E
describes feeling a strong sadness when someone passes on. When patients die, it is said to be
difficult since they have become friends. However the work continues and one thought about
how to cope is presented as following: “Their love for you keeps you going” (Informant C).
The informants also mention that you have to look forward, and think about the other patients
who need your help. That keeps you going.
5.3.2 Depending on caregivers
It is described how the informants involve for example mothers, of ill children in the care, in
order to manage the workload of the day: “You involve the patients and the caregiver…we tell
them everything. We teach them how to use things and for example to report fever and urine
output. They actually play some of our part” (Informant C). Therefore a mutual relationship
between the nurses and caregivers is established. To emphasise it further, Informant D
enlightens the following: “They are the ones who wash for the children, to bath them and
provide extra meals. They do most of the work”.

12
6. Discussion
6.1 Method discussion
In qualitative research, trustworthiness is essential when evaluating the study process. In 1985
Lincoln and Guaba identified the following criteria to obtain trustworthiness: credibility,
dependability, confirmability, transferability and authenticity. Credibility seeks the truth
within the data and interpretations. Dependability strive to achieve data that consist over time.
Confirmability seeks objectivity within the data and interpretations. Transferability refers to
the applicability of the findings. Authenticity refers to which extent the data conveys the
surrounding context (Polit & Beck, 2010, p. 192 & 193). To achieve trustworthiness it is
important that the students are experienced in interviewing. The quality of the data in this
study could lack because of the inexperience of the students, this can be seen as a weakness.
Regarding the choice of convenience sampling Procter and Allan (2006, p. 181) states that it
can increase the chance for a trustworthy relationship between the informants and researchers.
The chief nurses asked which of the nurses were willing to participate, something that could
lead to data bias and effect the credability. However the students felt the data was not
weakened by the used sampling method and it was clear that the informants sincerely wanted
to participate.
An including criteria was two years of working with cancer care. It was decided through a
discussion with one of the supervisors, thinking two years would be enough. Only English
talking informants were included since English was spoken by the students and the
informants. Since the students are not used to the English spoken in Uganda there was a risk
for misinterpretations. When something was unclear the students asked the informant to
clarify and also the audio recordings helped to explain uncertainties when transcribing.
Two of the interviews were performed in the counselling room at the LTC department,
allocated within the ward and therefore interruptions occurred several times. People
interrupted since they were looking for someone in the room, or had a question to the nurse
being interviewed. This could have affected the informants, however they stated it did not.
The interruption caused the students to become unfocused, for a short while. To strengthen
the data outcome, during two of the interviews both students participated, one acted as the
interviewer and the other one as an observer. This was done to ensure confirmability, but the
students did not feel as if this increased the understanding for the interview.
Semi-structured interviews were used, which according to Polit and Beck (2010, p. 341)
encourages the informants to talk without restraint, which is considered to strengthen the data.
The students appreciated if the informants spoke freely. This was pointed out before the
interview started, and it was written in the consent form. To make sure the content of the
interviews could be comparable, an interview guide was used. It was not possible to strictly
follow it since the students searched to achieve a good flow during the interview, and to make
the informants comfortable.
To ensure that the data would not be lost, it was recorded with two audio devices. To get a
wider understanding of the collected data, the students started the analysis by reading all
transcripts several times, to achieve credibility and confirmability. Constant discussions were
held to make sure no data of importance was neglected. Polit and Beck (2010, p. 107)
mentions that if there is more than one investigator, discussions between them can minimize
bias.
13
The students come from a high-income country and a western culture, which means they have
a different context. Granheim and Lundman, (2008) say it is of importance to understand the
informants cultural context in order to comprehend and analyse the data accurately.
Fortunately the students had some weeks to begin to appreciate Ugandan culture before the
data analysis started, this increased the authenticity and strengthened the study. To clarify the
analysis process, parts of the category-scheme is presented in the method section. Polit and
Beck (2010, p. 466) express that this helps the readers to critique. Since this is the first time
the investigators conduct a content analysis, the trustworthiness maybe somewhat weakened.
Obtaining ethical approval by MAK-SHS-IRB, ensured that the study followed ethical
principles such as, beneficence, respect for human dignity and justice. Furthermore, the
students offered to share the finished study with the informants, which according to Polit and
Beck (2010, p. 131) is a part of following ethical principles. The interviews were held during
working hours at the UCI, meaning colleagues may predict who the informants where. The
reason for conducting the interviews during working hours, was that it suited the informants.
A risk of exposing the informants occurred, and to keep confidentiality as far as possible
codes were used.
6.2 Result discussion
The aim of the study was to describe palliative cancer care in Uganda through the nurse
experience. The data collection resulted in interesting findings. Central in the result are the
challenges within cancer care. The challenges are patients’ poverty and lack of resources such
as medicine, material and equipment. Furthermore the shortage of staff, increasing number of
patients, and patients’ lack of knowledge is presented. Pain control and interaction, are
brought up as the most essential interventions for easing suffering. The minor, but yet relevant
part of the result are the significant relationships that develop between the nurses, patients and
caregivers.
One of the research questions, aimed to find information about the challenges cancer care is
facing and the result reveals that several challenges exist. This confirms the challenges Orem
and Wabinga (2009) bring up to discussion. Since the government underfund cancer care the
consequence is lack of resources for treatment and cure. Not only does the result show that
cancer medicines are missing, but also essential material and equipment for general nursing
care. The findings regarding patients’ financial difficulties, can be compared to a study
performed in a similar cancer care setting in Tanzania, conducted by Masika, Wettergren,
Kohi and von Essen (2012). That study was based on interviews with patients, and they
described lacking money for drugs and transportation to the hospital. The results from this
study were based on interviews with nurses, however they revealed similar financial
difficulties. Cancer patients are increasing in Uganda, and the results point out that higher
cancer awareness in the population could be one reason for the increase. An increasing
awareness could lead to more people seeking health care, and having a chance for treatment.
However Orem and Wabinga (2009) mean that the cancer awareness is low in Uganda, but
the result might indicate that this is about to change. The increased number of patients makes
it even more challenging for the nurses to manage in providing palliative care. Nevertheless
the increased awareness in the future might lead to patients seeking and receiving treatment in
earlier stages of their illness, and hopefully the care then does not have to be palliative to the
current extent.
It is claimed in the result that the number of staff is not increasing to cope with the increasing
number of patients. According to WHO (2006) there is a global shortage of nurses, so this
14
situation does not seem to be unique for Uganda. Nevertheless, the ratio of 1 nurse taking care
of 50 patients indicates a severe shortage. Caregivers become involved in providing care and
are mentioned to play a significant role. Orem and Wabinga (2009) state that close
relationships can be seen as a resource in providing cancer care. However, Gysels et al.
(2011) describe that caregivers have experienced emotional and financial burdens, from
giving palliative care. Caring for the relative means less time to get income, and therefore
sacrificing resources. Reasons for why the caregivers become so involved are indicated in the
result to be a consequence of staff limitations, however it might also be due to close family
relationships in Uganda.
Another research question aimed to describe how patients suffering can be eased. Since it is
known that the patients seek cancer care in a late stage of their illness palliative care is given.
According to Jakobsson et al. (2009) easing suffering is central within palliative care. It is
described that the patients are in pain, and pain control is stated as the primary intervention to
ease suffering. Masika et al., (2008) claim pain to be a major issue for the cancer patients in
Tanzania. This indicates that what the nurses identify as problems, agree with the patients’
descriptions. The result shows that interacting with the patients is another intervention for
easing suffering. Through Flensner, Öhlén (2009, p. 120) describe being present with the
patient, is essential to ease the suffering. Presence can be seen as a part of interaction, and
therefore the result describe relevant interventions. Talking with the patients does not require
material resources, and it should not be underestimated, however with the heavy workload
nurses find time is not enough.
The result shows that, working within cancer care in Uganda is demanding, for the nurses and
causes them emotional distress. Wanting to help a patient, but not being able to, because the
things you need are missing leads to frustration. The nurses often become close to the patients
so when they pass on it is painful. These findings answer the third research question,
regarding thoughts about giving care. The emotional experiences should raise a concern, and
is something that requires more research. The result has revealed that patients for various
reasons seek health care in a late stage of the cancer making the care palliative, a fact that is
concerning, since early detection of cancer is central for a successful treatment (WHO, 2010).
It is mentioned that, this might be due to patients believing in witchcraft, or thinking cancer is
a curse. These health care seeking behaviours amongst cancer patients in Uganda could also
be interesting for further research.
6.3 Relevance for nursing science and society
The fact that cancer is increasing, and that nurses play a core role within care, makes it
essential to recognize their experiences of palliative cancer care. This study shows that
working within cancer care in Uganda means working with limited resources. In order to get
more resources allocated to cancer care these limitations must be acknowledged. It is
something that the students hope this study can contribute to. The students are aware that the
solution to the challenging situation exists on a wider level, but nonetheless this study and
others like it do hope to contribute to the improvements so clearly desired by those providing
palliative cancer care in Uganda. The result will be shared with the UCI and therefore they
have the possibility to gain insight as to what nurses working there are thinking. Furthermore,
the study will be shared through Karolinska Institutet, making it available for both staff and
fellow nursing students. For Swedish nurses and nursing students this study gives the
opportunity to broaden the perspectives on health care in a low-income country, and this is
valuable since it stands in contrast to health care in Sweden and also because they someday
might want to go and work abroad. In practicing nursing this study could increase the nurses
understanding for patients from countries such as Uganda. The study will also be available
15
through SIDA on their website, so that students who have been granted minor field study
scholarships can read it, and might be inspired to undertake research within similar areas.
6.4 Conclusion
This study reveals that the cancer care in Uganda is being faced to deal with challenges. The
prevalence of cancer is on the increase in Uganda and the result indicates this to be partly due
to increased awareness of the illness among the Ugandan population. This new awareness
could lead to more cancer sufferers seeking health care and being treated at earlier stages, a
development in the right direction. However, the nursing staff patient ratio is currently under
pressure and perhaps does not have the possibility to provide sufficient care and treatment
with swelling cancer patient demand. Indeed caregivers are relied upon in the provision of
care for the patients and the nurses depend on them to make the care as acceptable as possible.
Although the contribution by the caregivers have become a resource for the nurses, previous
research shows that caregivers experience emotional and financial burdens which should be
considered.
The patients who receive cancer treatment are often admitted during the later stages of their
illness and therefore the care becomes palliative, and nursing interventions at this stage is
foremost to ease the patients suffering. Easing the suffering is primarily done by managing
the pain and patient interaction. These interventions can be seen as basic in the cancer care
setting, however the students reflect they are essential in general nursing care.
The government is underfunding cancer care and therefore necessary resources are missing. It
is stated in the NHP II (MOH, 2010) that the government is obliged to provide all people with
health care, but in reality this appears not to be happening. Patients are in many cases poor
and are not able to afford the cost of drugs, or hospital transport, while having to maintain a
household which is quite often the case. These financial difficulties are similar to those
presented in a study of cancer patients in Tanzania. Without drugs, blood products and
oxygen it becomes difficult to treat patients to the desired extent, and it so happens patients
die almost by default. The sense of helplessness experienced by not being able to administer
fully to the needs of patients due to lack of resources appears to be a burden to nurses and
presumably other health care staff. The students reflect that these emotional experiences are
concerning and should be researched further.
This study is an attempt to give insight into the field of cancer care in Uganda. Improvements
need to happen, this could be speeded up by a substantial financial injection to raise the
standard of cancer care, and to support nurses in providing qualitative cancer interventions.
Declaration of independence
Writer Karoline Ekblad and writer Sara Dorrian have equally contributed in all parts of this
bachelor thesis.
16
References
Flensner, G. Vem är patienten?. In E. Dahlborg-Lyckhage (Ed.), Att bli sjuksköterka: en
introduction till yrke och ämne (pp. 108-122). Lund: Studentlitteratur.
Granheim, U.H., & Lundman, B. (2004). Qualitative content analysis in nursing research:
concepts, procedures and measures to achieve trustworthiness. Nurse Education Today,
24(2), 105-112. doi:10.1016/j.nedt.2003.10.001
Gysels, M., Pell, C., Straus, L., & Pool, R. (2011). End of life care in sub-Saharan Africa: a
systematic review of the qualitative literature. BioMedCenter Palliative Care, 10(1).
doi:10.1186/1472-684X-10-6
Hansson, J., Henriksson, R., Petersson, C. (2008). Cytostatika och cytostatikabehandling. In
U. Ringborg, T. Dalianis, R. Henriksson, T. (Eds.), Onkologi. (2nd ed.) (pp. 184-217).
Stockholm: Liber.
Harding, R., & Higginson, I.J. (2005). Palliative care in sub-Saharan Africa. Lancet,
365(9475), 1971–77. Retrieved from
http://www.sciencedirect.com.proxy.kib.ki.se/science/article/pii/S0140673605666664
Harding, R., Selman, L., Agupio, G., Dinat, N., Downing, J., Gwyther, L., … Higginson, I.
(2011). The prevalence and burden of symptoms amongst cancer patients attending
palliative care in two African countries. European Journal Of Cancer, 47(1), 51-56.
doi:http://dx.doi.org.proxy.kib.ki.se/10.1016/j.ejca.2010.08.003
Holloway, I., Todres, L. (2006). Grounded theory. In K. Gerrish & A. Lacey (Eds.), The
research process in nursing. (5th ed.) (pp. 192-207) Oxford, UK: Blackwell Pub.
International Council of Nurses. (2007). ICN:s etiska kod för sjuksköterskor. Retrieved 24th
of March, 2013, from
http://www.swenurse.se/PageFiles/2582/SSF%20Etisk%20kod%20t%20webb2.pdf
Jakobsson, E., Andersson, M., & Öhlén, J. (2009) Livets slutskede - välbefinnande och död.
In I F. Friberg & J. Öhlén (Eds.), Omvårdnadens grunder: Perspektiv och förhållningssätt.
(1. ed.) (pp. 327-354). Lund: Studentlitteratur.
Masika G.M., Wettergren, L., Kohi, T.W., & von Essen, L. (2012). Health-related quality of
life and needs of care and support among adults Tanzanians with cancer. Health and
Quality of Life Outcomes, 10(1). doi:10.1186/1477-7525-10-133
McGarvey, E.L., Baum L.D., Pinkerton, R.C., Rogers L.M. (2001). Psychological sequelae
and alopecia among women with cancer. Cancer Practice, 9(6), 283-9.
doi:10.1111/j.1523-5394.2001.96007.pp.x
Merriman, A. (1996). Uganda: Status of cancer pain and palliative care. Journal of Pain &
Symptoms Management, 12(2), 141-143.
Ministry of Health (MOH). (2010). The second national health policy: promoting people´s
health to enhance socio-economic development. The Republic of Uganda. Retrieved 5th of
17
February, from http://apps.who.int/medicinedocs/documents/s18426en/s18426en.pdf.
Mwangi-Powell, F. (2012). APCA's role in the development of palliative care in Africa.
Progress In Palliative Care, 20(4), 230-233.
doi:http://dx.doi.org.proxy.kib.ki.se/10.1179/1743291X12Y.0000000014
Nguyen, L., Ropers, S., Nderiut, E., Zuyderduin, A., Luboga, S., & Hagopian, A. (2008).
Intent to migrate among nursing students in Uganda: Measures of the brain drain in the
next generation of health professionals. Human Resource for Health, 6(5).
doi:10.1186/1478-4491-6-5
Okuku, F., Omoding, A., Walunsansa, V., Origa, M., Mutungi, G., & Orem, J. (2013).
Infection-related cancers in sub-Saharan Africa: a paradigm for cancer prevention and
control. Oncology, 84(2), 75-80. doi: 10.1159/000343151
Orem, J., & Wabinga, H. (2009). The roles of national cancer research institutions in evolving
a comprehensive cancer control program in a developing country: experience from
Uganda. Oncology 77(5), 272-280. doi 10.1159/000259258
Parkin, D., Sitas, F., Chirenje, M., Stein, L., Abratt, R., Wabinga, H. (2008). Part I: Cancer in
Indigenous Africans: burden, distribution, and trends. Lancet Oncology, 9(7), 683-692.
doi:10.1016/S1470-2045(08)70175-X
Parkin, D.M., Nabooze, S., Wabwire-Mangen, F., Wabinga H.R. (2010). Changing cancer
incidence in Kampala, Uganda, 1991-2006. International Journal of Cancer, 126(5), 1187-
1195. doi:10.1002/ijc.24838
Polit, D.F,. & Beck, C.T. (2010). Essentials of nursing research: appraising evidence for
nursing practice. (7th ed.) Philadelphia PA: Wolters Kluwer Health/Lippincott Williams &
Wilkins.
Procter, S., & Allan, T. (2006). Sampling. In K. Gerrish & A. Lacey (Eds.), The research
process in nursing. (5th ed.) (pp. 173-191) Oxford, UK: Blackwell Pub.
Selman, L.E., Higginson, I.J., Agupio, G., Dinat, N., Downing, J., Gwyther, L., … Harding,
R. (2011). Quality of life among patients receiving palliative care in South Africa and
Uganda: A multi-centred study. Health and Quality of Life Outcomes, 9(1). doi:
10.1186/1477-7525-9-21
Thun, M.J., DeLancey, J.O., Center, M.M., Jemal, A., Ward, E.M. (2009). The global burden
of cancer: priorities for prevention. Carcinogenesis, 31(1), 100-110. doi
10.1093/carcin/bgp263
Utrikesdepartementet. (2010). Mänskliga rättigheter i Uganda 2010. Retrieved 26th of
March, 2013, from http://www.manskligarattigheter.se/sv/manskliga-rattigheter-i-
varlden/ud-s-rapporter-om-manskliga-rattigheter/afrika-och-soder-om-sahara?c=Uganda
Wiklund, L. (2009). Lidande: en del av människans liv. In F. Friberg & J. Öhlén (Eds.),
Omvårdnadens grunder: Perspektiv och förhållningssätt. (1 ed.) (pp. 295-325). Lund:
Studentlitteratur.
18
World Health Organization. (2001). Strengthening nursing and midwifery. Retrieved 26th of
March, 2013, from http://apps.who.int/gb/archive/pdf_files/EB107/eer2.pdf.
World Health Organization. (2006). Working together for health: the world health report
2006. Retrieved 26th of March, 2013, from http://www.who.int/whr/2006/whr06_en.pdf.
World Health Organization. (2010). Cancer: Fact Sheet no 297. Retrieved 5th of February,
2013, from http://www.who.int/mediacentre/factsheets/fs297/en/.
World Health Organization. (2013). Cancer: WHO definition of palliative care. Retrieved 5th
of February, 2013, from World health organization,
http://www.who.int/cancer/palliative/definition/en/).
Zikusooka, C.M., Kyomuhang, R., Orem, J.N., & Tumwine, M. (2009). Is health care
financing in Uganda equitable? African Health Sciences, 9(2), 52-58. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2877292/pdf/AFHS09S2-0S52.pdf.
19
Appendix 1

20
21
Appendix 2

22
23
24
25


















