Pain Management and JPS Presentation by: Brandt Oliver UTA Intern.
38
Pain Management and JPS Presentation by: Brandt Oliver UTA Intern
-
Upload
winifred-thomas -
Category
Documents
-
view
216 -
download
1
Transcript of Pain Management and JPS Presentation by: Brandt Oliver UTA Intern.

Pain Management and JPS
Presentation by:Brandt OliverUTA Intern

The Concerns
Chronic pain has become a leading healthcare issue in the nation.
Chronic pain has drastically increased the use of narcotic-only drug treatments nationally.
These two issues are increasingly affecting the JPS Healthcare System.

The Question
If JPS creates a dedicated Pain Management Center will it lead to better quality of life for CHC patients and will the number of prescriptions of pain controlling narcotics decrease also?

Chronic Pain Prevalence in the US An estimated 50 million to 75 million people live with
chronic pain, defined as constant pain lasting at least three months.
Among adults, 90% suffer pain at least once a month and 42% have daily pain; 22% of all primary care patients have chronic pain.
80% of Americans believe their aches and pains are "just part of getting older" and 28 percent believe there is no solution to their pain.
Less than half (42%) of people who visit their doctor for pain believe that their doctor completely understands how their pain makes them feel.
The Arthritis Foundation, "Pain In America: Highlights from a Gallup Survey," www.arthritis.org, 2000

Chronic Pain Prevalence in the US
Pain Facts & Figures: Incidence of Pain, as Compared to Major Conditions, www.painfoundation.org, January 2007
Chronic Pain’s cost to society
Persistent pain affects approximately 30% of the U.S. population annually1.
It has created substantial disability and societal costs related to decreased work productivity, absenteeism, and increased healthcare utilization.
Chronic pain costs the U.S. $100 billion a year in health care expenses, lost income and productivity2.
The average cost for chronic back pain for Worker’s Compensation is $7,000 – 8,0002.
1. Kerns, Thorn, and Dixon. Psychological Treatments for Persistent Pain: An Introduction. JOURNAL OF CLINICAL PSYCHOLOGY: IN SESSION, Vol. 62(11), 1327–1331 (2006)
2. Pain Facts & Figures: Incidence of Pain, as Compared to Major Conditions, www.painfoundation.org, January 2007 4.

Controlled Substance Abuse
Drug Abuse StatisticsThe DEA has reported a 40% rise in
prescriptions of Hydrocodone in the last five years.
Abuse of prescription drugs accounts for approximately 35% of the total drug abuse problem in the United States.
HAMMER, DAVID, Advocates Demand Funding for Pain Treatment, CBS Health Watch, Jul. 21, 2006

Opioid Abuse Case Study
Study revealed that there is significant abuse of opioids
Out of 100 patients, 24% of the patients abused opioids, and frequent abuse was seen in 50% of these patients, in spite of controlled substance contracts and additional interventional techniques.
L Manchikanti, V Pampati, K S Damron, B Fellows, R C Barnhill, C D Beyer, Prevalence of opioid abuse in interventional pain medicine practice settings: a randomized clinical evaluation., Pain Physician. 2001 Oct

Drug Diversion Sources

Non-medical use of Prescriptions
1. Laxmaiah Manchikanti, MD. Prescription Drug Abuse: What is Being Done to Add ress This New Drug Epidemic? Testimony Before the Subcommittee on Criminal Justice, DrugPolicy and Human Resources. Pain Physician. 2006;9,287-321

8 Year change in Prescription Narcotic sales

Payments for Prescription Drug Use

Federal Drug Control Spending
1. Laxmaiah Manchikanti, MD. Prescription Drug Abuse: What is Being Done to Add ress This New Drug Epidemic? Testimony Before the Subcommittee on Criminal Justice, DrugPolicy and Human Resources. Pain Physician. 2006;9,287-321

JCAHO
JCAHO believes that, “Unrelieved pain has enormous physiological and psychological effects on patients. Effective management of pain is a crucial component of good care.”
JCAHO also asserts that, “Research clearly shows that unrelieved pain can slow recovery, create burdens for patients and their families, and increase costs to the healthcare system.”
14th Annual Meeting of the American Society of Pain Management NursesMarch 18-21, 2004. Nurse Reporter. Vol. 1 Issue 3 June 2004

Provider Response to Pain Management “Would be great if it could happen.” “If the AMA came in and audited how I
prescribe narcotics I would be very worried.” “I sometimes feel like a drug dealer.” “The amount of pain management
education I received was very limited.” “I don’t want to lose my license.” “This population is hard to manage.”

Consequences of Mismanaged or Under-Managed Pain
Mismanaged or under treated pain can result in:Extensive, costly, unhelpful work-ups
and treatmentDysfunction in family, vocational, and
social lifeMental and physical sufferingIncreased disability costsIncreased yearly expenditures
Benefits of Appropriate Pain Treatment Saves lives - patients in severe pain who are
not treated have been known to commit suicide to end their suffering.
Reduces the chances of developing additional physical problems or making existing problems worse.
Reduces suffering for patients and families. Returns the patient to being in charge of his
or her life. Allows the patient to become more productive
in society - through work, family life, or social activities.
Reduces the cost of medical care.

Patient Referrals
Reasons for a pain center referral The mere mention of the patient’s name
strikes fear in the hearts of the office staff. You run late with the patient every time the
patient comes to see you. The patient is inconsistent or has poor
compliance with the treatment regimen. Multiple physicians are treating the same or
related conditions. The patient has multiple visits to the urgent
care center or to the emergency room or has multiple hospitalizations.

Comprehensive Pain Program (CPP)
Clinical Evaluation The current guidelines recommend that
chronic pain patients be evaluated by healthcare professionals with specialized training in chronic pain management.
The initial evaluation should be performed by a qualified physician and psychologist.
The evidence continues to accumulate that the most effective treatment for chronic pain patients is found within an integrated interdisciplinary pain rehabilitation program.
John D. Loeser, MD. Comprehensive Pain Programs Versus Other Treatments for Chronic Pain. The Journal of Pain, Vol 7, No 11 (November), 2006: pp 800-801

Clinical Evaluation of CPP
Clinical Team Make-up Pain Specialist MD Psychologist Neurologist Physical Therapist Occupational
Therapist Pain Specialist RN Dietician Social Worker

Patient’s Pain Care Plan of CPP Care Plan Process
Assess patient’s understanding of their disorder
Perform a psychological exam Prescribe pharmacological interventions Treat patient with physical and occupational
therapy Perform higher level interventional pain
management procedures Educate and empower patient to take active
role in their own recovery Involve family and community to help with
patients treatmentGatchel and Okifuji. Evidence-Based Scientific Data Documenting the Treatment and Cost-Effectiveness of Comprehensive Pain Programs for Chronic Nonmalignant Pain. The Journal of Pain, Vol 7, No 11 (November), 2006: pp 779-793

Success of CPP’s
Researchers found a more than 33% reduction in pain-related clinic visits in the HMO setting in the year following the completion of CPPs with a strong cognitive behavioral orientation.
Another study reported a substantial 50% decline in pain-related clinic visits following a comprehensive rehabilitative treatment.
60% to 90% of CPP patients do not seek any additional therapy for pain within 1 year following the treatment.
Gatchel and Okifuji. Evidence-Based Scientific Data Documenting the Treatment and Cost-Effectiveness of Comprehensive Pain Programs for Chronic Nonmalignant Pain. The Journal of Pain, Vol 7, No 11 (November), 2006: pp 779-793
Success of CPP’s
Almost half of conventionally treated patients require surgery or hospitalization compared to 16% -17% of CPP patients.
Annual medical costs following a CPP have been shown to be reduced by 68%
Evaluating the average return to work rate from 20 different clinical studies shows that on average 67% of CPP patients return to work compared to only 27% of non CPP patients
Gatchel and Okifuji. Evidence-Based Scientific Data Documenting the Treatment and Cost-Effectiveness of Comprehensive Pain Programs for Chronic Nonmalignant Pain. The Journal of Pain, Vol 7, No 11 (November), 2006: pp 779-793

Success of CPPs

Successful Pain Center
Massachusetts General Hospital (MGH) Pain Center
Don Cornuet, Director Interventional Pain Clinic
Diverse pain population Provide a true consult serviceRecently changed to a non-narcotic
treatment plan

MGH Pain Center (cont.)
Why MGH changed to a non-narcotic plan?Traditional Narcotic Management
• Clogs up capacity of Pain clinic• Few spaces available for new patients• Ongoing pain care with narcotics can go
on literally forever• Patients are kept in a medicated state• High E&M Levels for a cycling population
loses money for the clinic

MGH Pain Center (cont.)
MGH MantraTreat one episode at a time
• Separate script for each medical need
Increase functionality of patient• PT is extensively used • Alternative medicine
• i.e. Acupuncture
• Occupational Therapy

MGH Success Statistics
Visit mix Dec. 06 53% Follow ups Dec. 07 46% Follow ups
New Patients Dec. 06 18% Dec. 07 25%
Procedures Dec. 06 23% Dec. 07 29%
DNKA rate Dec. 07 22% Jan. 08 13%

Current Status of Pain Management at JPS In 2004, the Musculoskeletal Clinic opened
at the JPS Sports Medicine Clinic Within a year, majority of the 2000 patients
were taking CSNAs to control musculoskeletal pain.
At the time an initiative was undertaken to create a new pain management scheme for the Stop Six and FHC clinics.

Pain Management Initiative ID all patients receiving 60 doses of CSNAs
per month ID all CSNA patients with musculoskeletal
nocioceptive, neuropathic, and nocleceptive pain.
Develop a care plan using guidelines from the Federation of State Licensing Board of 2004
Removal of Oxycontin and Soma from formulary
Present care plan to P&T board for approval Opening of a large Sports Medicine and
Musculoskeletal clinic to perform a thorough evaluation of patients

Clinic Requirements of Initiative
The requirements will include: Full time Physical Therapy Case manager to monitor CSNA patients On-site psych evals for addiction screening
and co-morbid Condition Assessment Consulting for acupuncture, orthopedics,
and anesthetic procedures Consulting for PMR (Polymyalgia
rheumatica)

JPS Controlled Substance Agreement
Requirements: Patients can only receive narcotics from
one provider and one pharmacy Refills are only given at each office visit Urine tests are done monthly Patients must provide proof that they are
involved in other pain treatment modalities Patients cannot obtain any controlled
substances from any non-physician sources
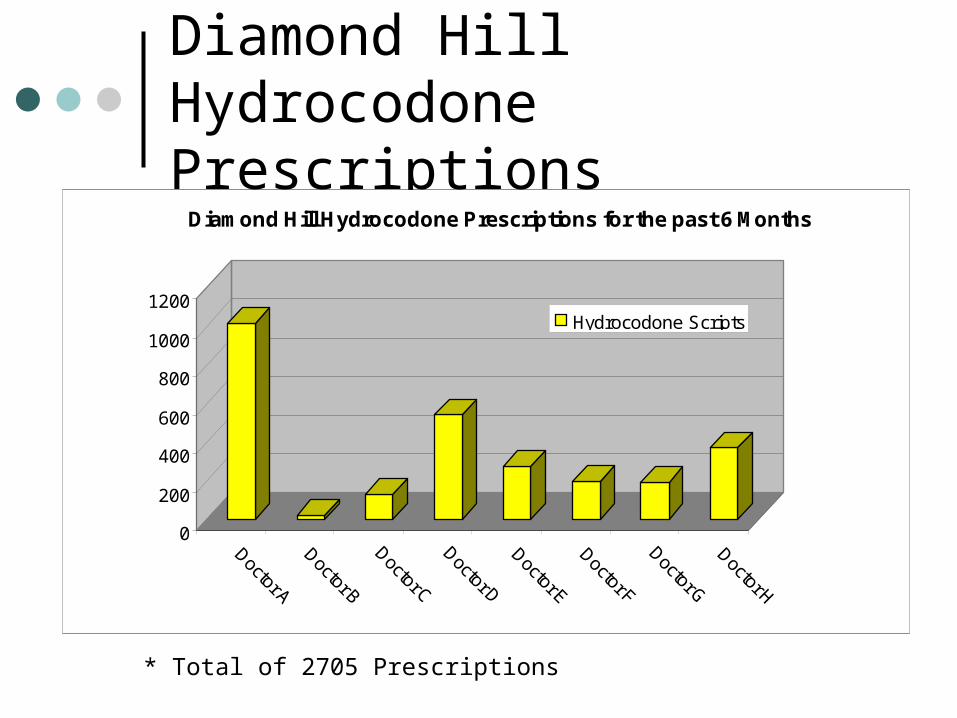
Diamond Hill Hydrocodone Prescriptions
* Total of 2705 Prescriptions
0
200
400
600
800
1000
1200
Doctor A
Doctor B
Doctor C
Doctor D
Doctor E
Doctor F
Doctor G
Doctor H
Diamond Hill Hydrocodone Prescriptions for the past 6 Months
Hydrocodone Scripts

CHC Hydrocodone Prescriptions
* Total of 13289 Prescriptions
0
500
1000
1500
2000
2500
3000
3500
Arlington HC
Diamond Hill
Northeast
FHCNorthwest
PolySouth Cam
pus
Stop 6
Viola Pitts
Arlington Central
CCH
CHC Total Prescriptions of Hydrocodone for the last 6 months
Scripts of Hydrocodone

Why should JPS have a dedicated Pain Center?
Patient Quality of Life Prescription abuse and the costs of
dispensing unneeded prescriptions JCAHO and Government
requirements Supporting providers Pain Patients clog Health Centers The image of JPS

Recommendations to coincide with a Pain Center Group Visits
Use the same model of the Diabetic Group Visits
Bring in pain patients under a strict CSNA regimen for group assessments
Larger numbers of patients can be seen and have their meds refilled quickly
Provides a cost efficient way of seeing a large population of people

Recommendations to coincide with a Pain Center Provide more institutional pain treatment education to
physicians 90% of physicians rate their education in pain
management as poor, and more than 70% rate their residency training as fair or poor.
75% of physicians believe a lack of familiarity with patient assessment for pain to be the major barrier to effective pain management, and 61% are reluctant to prescribe opioids.
In 2003, AMA created a free continuing education program for doctors to learn more about treating pain, and 84,000 doctors signed up in the first six months.
HAMMER, DAVID, Advocates Demand Funding for Pain Treatment, CBS Health Watch, Jul. 21, 2006

Conclusion
Bottomline Having a pain management center is
becoming the standard of care for the industry
Pain management centers and programs increase the quality of life for pain patients
A Comprehensive Pain Program can reduce aberrant drug behavior and increase patient quality life
Treating pain extensively can possibly reduce healthcare costs