Paediatric Rehabilitation Analysis for PCMCH Data for ... · reduction in days occurred within CCC...
9
Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 1 Paediatric Rehabilitation Analysis for PCMCH Data for Fiscal Year 2014/15
Transcript of Paediatric Rehabilitation Analysis for PCMCH Data for ... · reduction in days occurred within CCC...

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 1
Paediatric Rehabilitation Analysis for PCMCH Data for Fiscal Year 2014/15

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 2

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 3

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 4

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 5
Activity Overview and History:
Acronym HBKRH Main patient catchment area Toronto, GTA, Ontario Primary Academic Affiliation University of Toronto Year founded 1899
Other descriptive section 150 Kilgour Road in Toronto Beds - Staffed and in Operation TOTAL Rehabilitation CCC Respite HOLLAND BLOORVIEW 64 36 21 7 Definition: The number of inpatient beds that are resourced and available for patient accommodation, whether or not they are actually occupied by a
patient at the time. The CCC beds include 1 budgeted bed for sleep studies
Specialty Services Include: Child Development Rehabilitation & Complex Continuing Care
o Autism (satellites included) o Acquired Brain Injury o Cleft Lip & Palate o Amputee o Dental/Oral Surgery/Maxillofacial o Concussion Care o Developmental Paediatrics o Chronic Pain Management o Feeding o Orthopaedics o Hypertonia o Respite o Lifespan Clinic o Sleep Studies o Neuromotor o Spinal Cord Injury o Neuromuscular o Neurology
o Psychopharmacology o Saliva Management o Specialized Seating Services o Spina Bifida
Participation and Inclusion o Communications & Writing Aids o Community Based Services o Life Skills o Nursery Schools
Diagnostic Services Include:
Cath Lab Radiology Image Guided Therapy
Other Notes
X

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 6
HB 7.0 Holland Bloorview Patient Volume Breakdown The indicator provides a breakdown of hospital inpatient volumes into Complex Continuing Care discharges, Day Patient discharges, Rehabilitation discharges which is compiled of Brain Injury Rehabilitation Team (BIRT) and Specialized Orthopaedic Developmental Rehabilitation (SODR), and Respite Service discharges categories. Fiscal Year Complex
Continuing Care
Rehabilitation Respite Service*
Total Inpatient
Day Patient
Grand Total
BIRT SODR FY 2014-15 37 132 156 253 578 53 631 Rehabilitation (BIRT and SODR): The child and adolescent rehabilitation service provides comprehensive rehabilitation care to clients from birth to age 18, with a variety of congenital, acquired and traumatic injuries. Diagnostic groups include but are not limited to clients with acquired brain injuries, arthritis, burns, cerebral palsy, complications of prematurity, complex epilepsy and seizure disorders, orthopedic conditions, respiratory conditions and spinal cord injuries. Respite*: The respite care service supports families by providing short-term, inpatient care for children with disabilities or complex medical needs. Families may access up to six weeks of respite care each year. This is a high volume, low length of stay service which displays peak periods of occupancy during the summer and holiday months. Complex Continuing Care: The complex continuing care service meets the needs of clients with unstable chronic illnesses and/or multi-system diseases. Many clients have tracheostomies or require mechanical ventilation. Although clients may be admitted to the respiratory/complex continuing care unit for extended periods, the goal is to facilitate discharge to the community. Transitioning children continues to be a ‘system’ challenge with Holland Bloorview engaged in multiple strategies:
• Internal transition strategy; • Provincial engagement in wait times information system (WTIS) Alternate Level of Care (ALC)
data collection • Toronto Central –Local Health Integration Network (TC-LHIN) Strategy for long stay ALC Rehab
patients • Toronto Central –Community Care Access Centre (TC-CCAC) partnership
While ALC remains a provincial strategy, Holland Bloorview continues to work with all stakeholders to ensure safe and appropriate transition of clients across the continuum of care. Day Patient: Day patients are clients who visit hospital daily for intensive therapy with a defined treatment period however do not occupy an inpatient bed. Note: Holland Bloorview Kids Rehabilitation Hospital serves a significantly large paediatric population through the outpatient programs and services. In 2014/15 a total of 6,982 clients were served, through more than 55,452 client encounters. An encounter is generated when a client is registered at the centre to receive one or more services. As per MIS guidelines, only one encounter is recorded per day, irrespective of the number of services received.

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 7
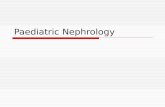
HB 7.1 Percent of Inpatient Discharges by Type Holland Bloorview has three key inpatient services, Specialized Orthopaedic Developmental Rehabilitation (SODR), Brain Injury Rehabilitation Team (BIRT), Complex Continuing Care (CCC) and Respite Services. The distribution of inpatients across both SODR and BIRT is similar in profile with CCC having the least amount of movement across the system. Respite services continue to be utilized significantly by families for the uniqueness of service and participation provided for children with complex needs (e.g. ventilator necessity, medical complexity). While Respite appears to be the largest number of discharges, it accounts for 5% of all inpatient days. Discharge patterns have not significantly shifted from last fiscal year across services. HB 7.2 Percent of Inpatient Days by Type Inpatient beds continue to be the key measure of resource utilization and a marker of shifting populations and access. The largest proportion of inpatient days continues to be attributed to Rehabilitation ‘designated beds’. While there has been relative stability in the total patient days for the last 2-3 fiscal years, in 2014/15 a significant shift was noted within our Rehabilitation service with an increase of 14.4% patient days. The reduction in days occurred within CCC and has been attributed to the focused and strategic partnering to transition our clients over the age of 19 into community housing or into adult residential homes.
HB 7.3 Inpatient Average Length of Stay The average length of stay (ALOS) is an industry standard measure to provide information as to ‘the average number of days’ a bed is occupied by a client in an inpatient setting. Length of Stay is calculated from the date of admission to the date of discharge. The ALOS for the organization over the last 5 years has been 50.0 days with a gradual trend downwards. This fiscal year the organizational ALOS within rehabilitation services was 49.3 days a marginal reduction. HB 7.4 Percent of Inpatient Clients Receiving Outpatient Services Ensuring the continuity of care for clients after discharge is of paramount importance in paediatric rehabilitation as recovery continues in a community setting. The graph demonstrates an increase of six percent of clients discharged from inpatients who continue receiving services on an outpatient basis since 2009/10 fiscal year. No further increases seen in the past 3 years. The high percentage of use is a reflection of the needs of client’s as they transition across the continuum of care.
FY 2013/14 FY 2014/15 Rehabilitation (SODR and BIRT) 12,573 14,382 Complex Continuing Care (include Sleep Studies) 6,561 5,443 Respite 1,265 1,021 Total 20,399 20,846
6%
23%
27%
44%
Inpatient Distribution for Fiscal Year 2014/15
CCC BIRT SODR Respite
75.873.8
76.8
81.7 81.6 81.9
40
50
60
70
80
90
100
Fiscal Year2009-10
Fiscal Year2010-11
Fiscal Year2011-12
Fiscal Year2012-13
Fiscal Year2013-14
Fiscal Year2014-15
Perc
enta
ge o
f Clie
nts
Disc
harg
ed
Percentage Clients Discharged Receiving Outpatient Services

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 8
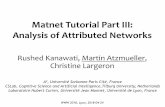
HB 7.5 Outpatient Patient Profile Annually, the organization provides services for 6,982 unique clients in our outpatient setting, totaling 71,510 attendances. The organization experienced more unique clients this fiscal year and totaled attendances. The outpatient age profile is different than inpatients with many children (49.6%) accessing services before the age of 9 to assist with external funding, school supports and early intervention. This distribution is quite different from inpatients as our regional programs and the legislative shifts necessitating ‘wellness’ visits have materialized with more children being seen younger. We continue to offer specialized programming for young adults where system gaps are evident or transitions are challenging. HB 7.6 Referral Pattern for Autism Services - Assessment (Outpatient) Access to autism assessment (“diagnosis”) continues to be a strategic focus for Holland Bloorview with active oversight of wait times. Our accountability is demonstrated through the Quality Improvement Plan (QIP) - ‘autism’ is a key indicator and linked to executive compensation. Since the ‘wellness visit’ legislation was introduced, referrals have continued to increase for Autism assessment. At a system level, the incidence and prevalence of autism continues to increase with rates as high as 1 in 68 children being reported. This is 120% higher than the estimate 10 years ago. From a system perspective a diagnosis on average will cost a family approximately $60,000 annually in services with scientific studies suggesting early assessment and intervention being beneficial for learning. Holland Bloorview is at a critical juncture with Autism with referrals for assessment services continuing to exceed our limited resources. HB 7.7 Holland Bloorview Leading the System Concussion Centre - The Holland Bloorview Concussion Centre is one of the first in the world dedicated exclusively to pediatric concussion. Youth brains are still developing and require a unique approach to concussion care. It is estimated that one in five sport-related injuries are concussions – yet Canadians may be surprised to learn that only about 200,000 concussions are reported each year. That number may reach much higher, as concussions are a largely under-addressed health issue and can occur in many ways – falling during a bike ride, playing a sport, or an everyday mishap. Children and youth live with the invisible injury and experience headaches, dizziness, and confusion among other symptoms, and if left unaddressed can lead to longer-term symptoms such as difficulty concentrating, sleep disturbances, sensitivity to light and noise, and irritability. Our centre includes clinicians specifically trained in pediatric brain injury and researchers who are leading experts in the field of youth concussion. Focused on the three key pillars of Education, Research and Clinical care this ensures fluidity in our model of service delivery and the ability to influence the system through immediate knowledge translation surrounding the paediatric brain. Chronic Pain Program - Chronic pain among Canadian children is a growing area of concern. A recent systematic review of prevalence studies found that that 11% to 38% of children and adolescents will suffer from chronic pain and approximately 5% to 8% of these children will develop significant pain--related disability (i.e., social isolation, poor attendance at school, limitations in physical functioning, sleep and mood/anxiety disorders). Childhood chronic pain also has a significant impact on the family such as missed time from work,
0
50
100
150
200
250
300
0
50
100
150
200
250
300
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Fiscal Year 2009-2010 Fiscal Year 2010-2011 Fiscal Year 2011-2012 Fiscal Year 2012-2013 Fiscal Year 2013-2014 Fiscal Year 2014-2015
Num
ber
of R
efer
rals
Num
ber
of A
tten
danc
es
Attendances and Referrals Autism - Fiscal Year 2009 through 2015
Attendances Referrals Poly. (Attendances) Poly. (Referrals)

Holland Bloorview Kids Rehabilitation Hospital PCMCH Report – Pediatric Rehabilitation November 2015 9
financial stress as well as an emotional impact on family relationships. The Ministry of Health has invested in provincial pain programs and funded the collaborative proposal with the Hospital for Sick Children and Holland Bloorview resulting in the ‘Get Up and Go’ initiative. ‘The Get Up and Go’ Persistent Pediatric Pain Service at Holland Bloorview Kids Rehabilitation Hospital provides a four-week intensive rehabilitation service for children with chronic pain. This service is structured into a two-phased approach to rehabilitation. This graduated approach is designed to facilitate the success of the patients in returning to their home and community. This newly innovative service will provide greater insight towards the needs of children with chronic pain and inform new models of service delivery to achieve better health outcomes.
Paediatric Rehabilitation Mapping - Rehabilitation continues to evolve across the Canadian landscape with recognition that many rehabilitation services are decanted from acute care into the community. A continued strategic focus on how to better provide care to children and youth that aligns with local, provincial and national mandates is required. The Canadian Network for Child and Youth Rehabilitation (CN-CYR) under the Canadian Association of Paediatric Health Centres (CAPHC) has strategically led work aimed to better understand rehabilitation services and the challenges and opportunities that exist. A key opportunity in 2015 was an initiative that explored the breadth and depth of publically funded agencies providing publically delivered pediatric rehabilitation services across Canada. Through a generous donation from the Holland Bloorview Kids Rehabilitation Foundation, a mapping initiative of rehabilitation centres and services was conducted to capture both quantitatively and qualitatively the key challenges within rehabilitation. This analysis of this work will inform the rehabilitation sector in next steps to advance paediatric services.
Paediatric Rehabilitation Reporting System (PRRS): Canada is at a significant cross-road in its healthcare reform efforts. The ability to implement service improvements related to access and quality at an individual and system level are needed to support a sustainable healthcare system. Improvements must always be anchored in data that is reliable, accurate and reproducible. Unequivocally, there is a paucity of information in the paediatric rehabilitation sector on the access, effectiveness, efficiency and overall quality of services. Historically, organizations have collected information locally in the hopes of guiding the planning of services as it related to community needs. While there have been significant advances in the adult sector, paediatrics and rehabilitation have only recently been a focus. Creating this standardize approach in the collection, analysis and dissemination of valid and reliable outcomes measurement related to the rehabilitation of children and youth with disabilities within Canada will allow the healthcare system at the macro, meso and micro levels to measure and compare the quality of paediatric rehabilitation care with a view to improving services and outcomes across the care continuum into adulthood. It is clear that decision-making across all levels of leadership (e.g. clinicians, administrators and policy makers) cannot be made in the absence of standardized data collection and reporting practices. The PRRS is a reporting system that captures and shares data from paediatric rehabilitation centres across the country. It is a vehicle to ensure pan-national rehabilitation data can inform an accountable, transformational service delivery system for children with disabilities or chronic conditions that balances the clients’ need and economic realities. This national barrier that had impacted rehabilitation has now been removed with PRRS and will go on to address critical gaps while creating a national climate for data sharing, benchmarking and information client outcomes. PRRS is now live to capture data nationally and will be reporting information in early 2016.