Paediatric Organ Donation in 2018
48
Organ Donation in Pediatrics – special aspects and considerations Prof. Luregn Sch la p b a ch , MD, Ph D, FCICM Head, Department of Intensive Care and Neonatology, University Children` s Hospital Zurich, Zurich, Switzerland Past Chair, ANZICS Paediatric Study Group
Transcript of Paediatric Organ Donation in 2018
Orga n Don a t ion in Pe d ia t r ics –sp e cia l a sp e ct s a n d con s id e ra t ion s
Prof. Luregn Schlapbach , MD, PhD, FCICMHead , Departm ent of In tensive Care and Neona tology, Unive rsity Child ren` s Hosp ita l Zurich , Zurich , Switze rlandPast Cha ir, ANZICS Paed ia tric Study Group
Con t e n t• Patte rns of dea th in ch ild ren• Pedia tric cha llenges and in fan t dona tion• Recognizing the poten tia l donor • Bra in dea th te sting in ch ild ren• Pedia tric dona tion a fte r ca rd iac dea th• The fam ily pe rspective and consen t
conside ra tions• Sum m ary
Con t e n t• Pa t t e rn s o f d e a t h in ch ild re n• Pedia tric cha llenges and in fan t dona tion• Recognizing the poten tia l donor • Bra in dea th te sting in ch ild ren• Pedia tric dona tion a fte r ca rd iac dea th• The fam ily pe rspective and consen t
conside ra tions• Sum m ary
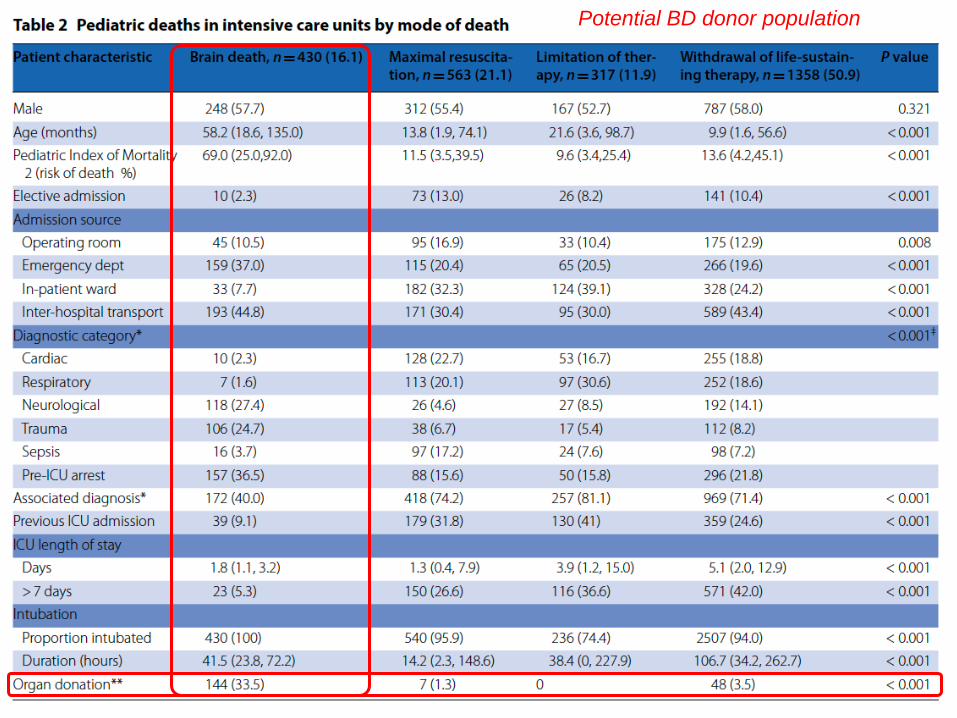
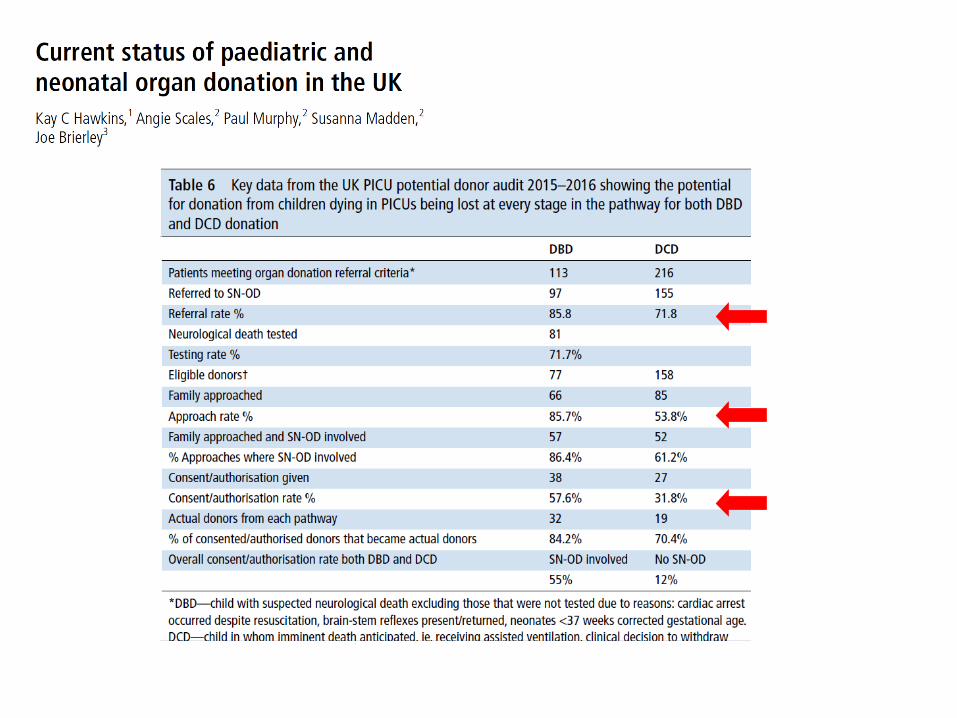
Potential BD donor population
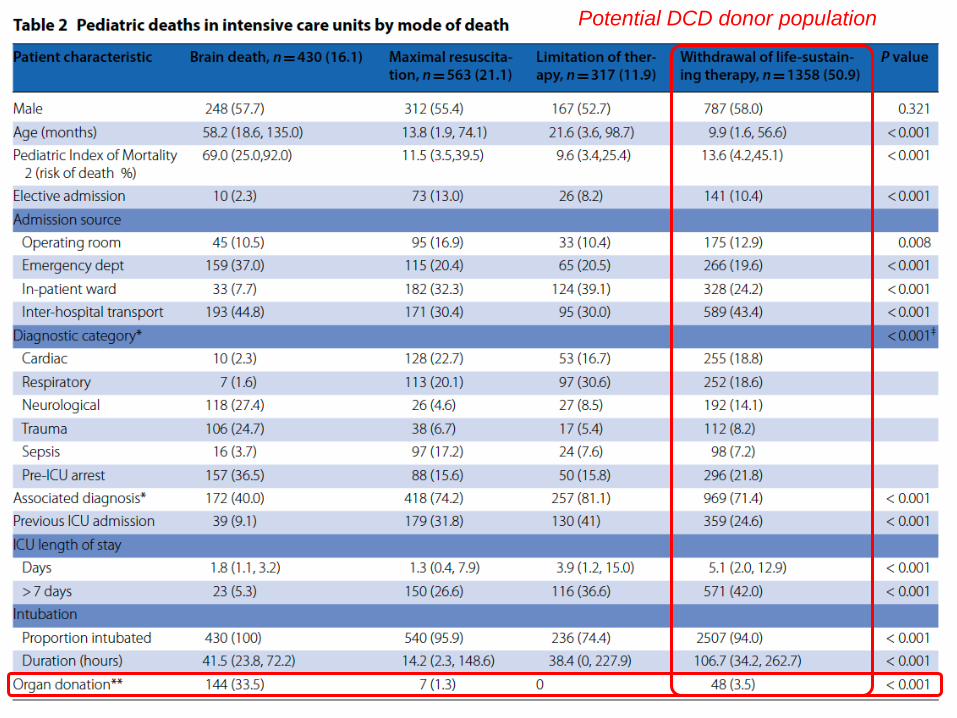
Potential DCD donor population
Con t e n t• Patte rns of dea th in ch ild ren• Pe d ia t r ic ch a lle n ge s a n d in fa n t d on a t ion• Recognizing the poten tia l donor • Bra in dea th te sting in ch ild ren• Pedia tric dona tion a fte r ca rd iac dea th• The fam ily pe rspective and consen t
conside ra tions• Sum m ary
Fir s t Pa e d ia t r ic Tra n sp la n t
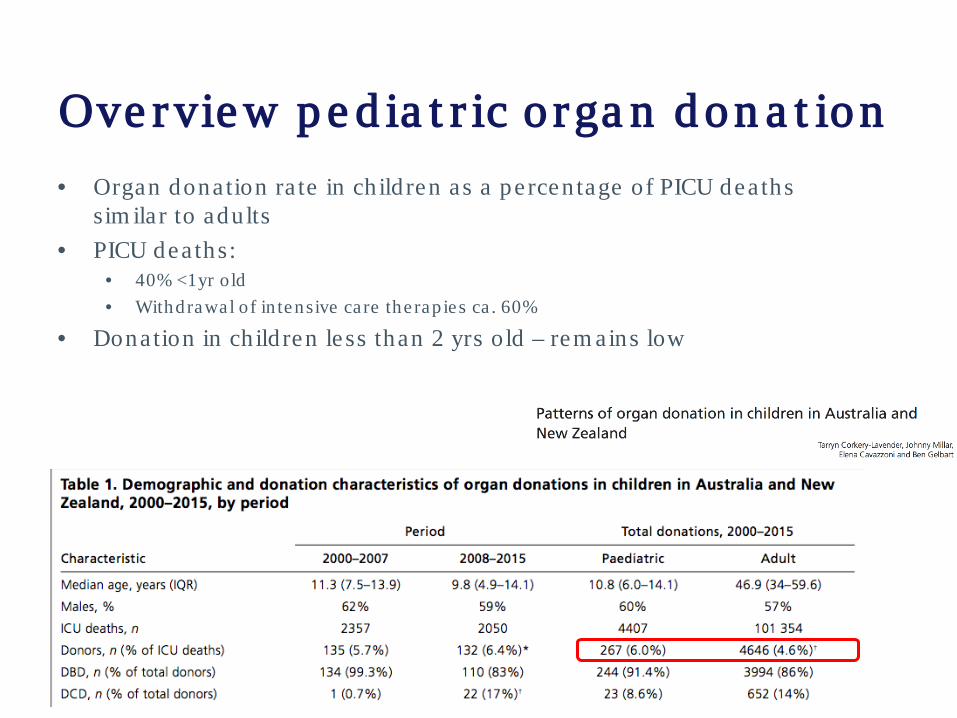
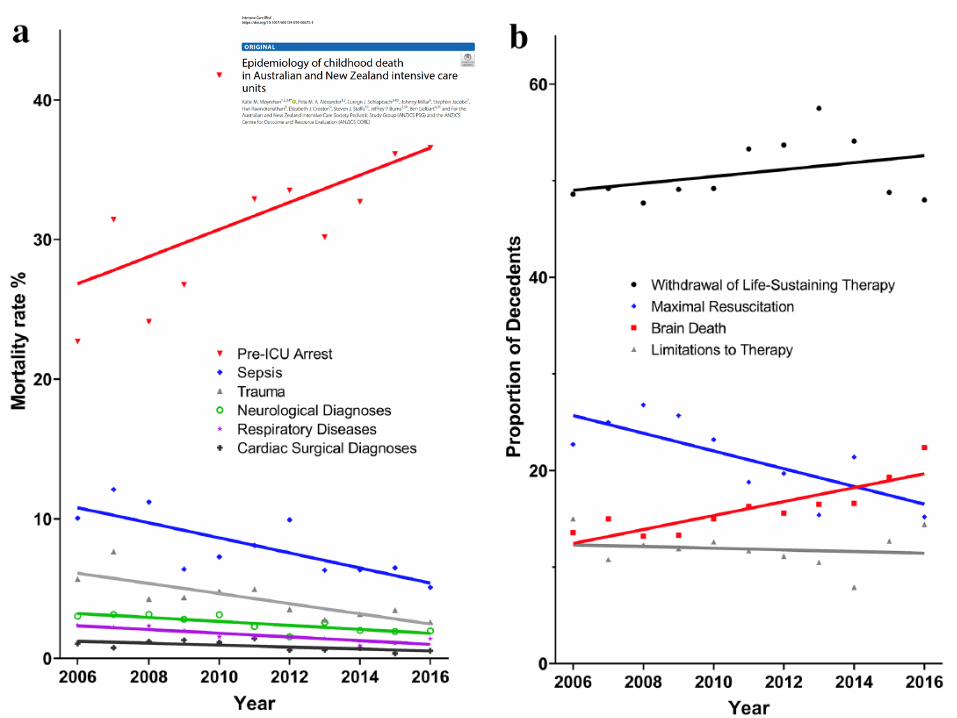
Ove rvie w p e d ia t r ic o rga n d on a t ion• Organ donation ra te in ch ild ren as a pe rcen tage of PICU dea ths
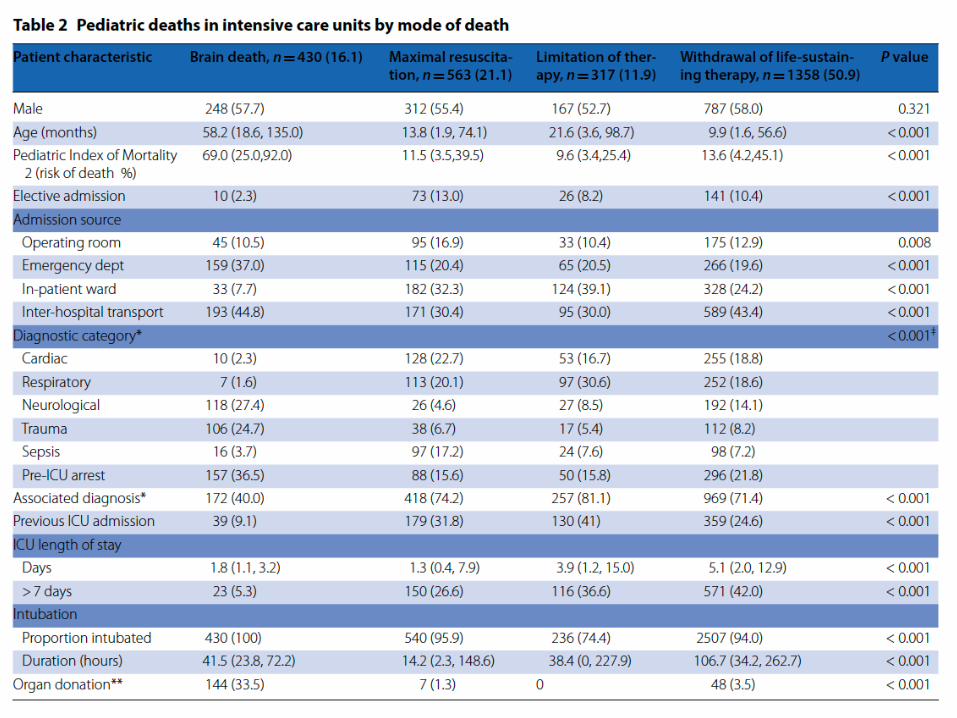
sim ila r to adu lts• PICU deaths:
• 40% <1yr o ld• Withdrawal of in tensive care the rap ie s ca . 60%
• Donation in ch ild ren le ss than 2 yrs old – rem ains low
Am e r ica n Aca d e m y o f Pe d ia t r ics• Paed ia tricians shou ld
p rom ote awareness• In tegra l part of end of
life care• Fam ilie s shou ld be given
the opportun ity• The process shou ld be
facilita ted by an organ p rocurem ent organ isa tion

Pe d ia t r ic ch a lle n ge s• Rate of pedia tric dona tion to to ta l dona tion re la tive ly
constan t in m ost countrie s• Variab le approaches to neona ta l and infan t dona tion
• poten tia lly under-u tilized• Lower age /we ight lim its
• Fam ilia rity with BD te sting in th is age group• Logistic/practica l issues with DCD in pedia tric hospita ls• Rules, p ractices, and conversa tions as for adult OD la rge ly
apply
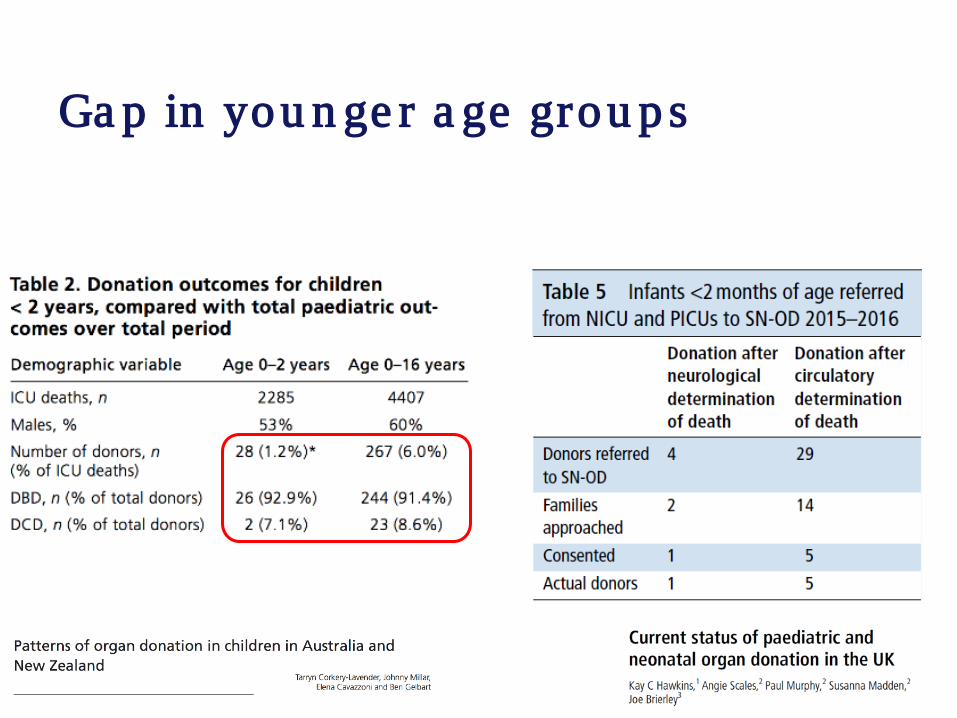
Ga p in you n ge r a ge grou p s
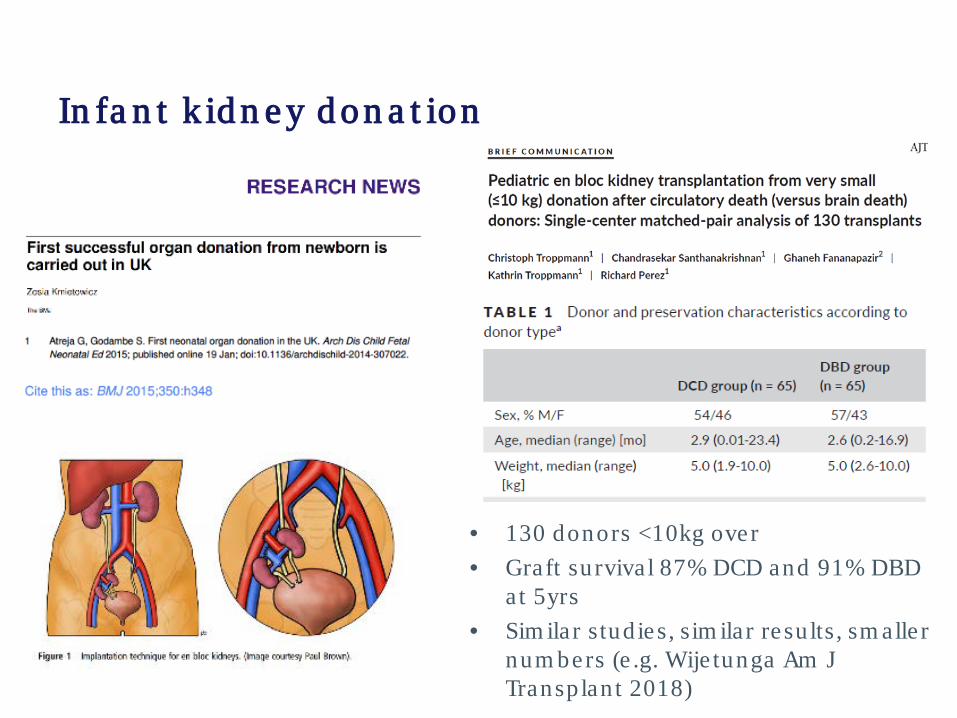
In fa n t k id n e y d on a t ion
• 130 donors <10kg over • Graft su rviva l 87% DCD and 91% DBD
at 5yrs• Sim ilar stud ies, sim ila r re su lts , sm alle r
num bers (e .g. Wije tunga Am J Transp lan t 2018)
In fa n t d on a t ion• Infan t dea ths represen t a lm ost ha lf of PICU dea ths• Feasib le and outcom es prom ising• Fam ilie s of in fan ts who d ie often ask about organ dona tion• Relie s on deve loping expertise and process• Expanding the upper age lim it of recip ien ts vs risk of lower
age lim it of donors• Procurem ent and transp lan t capability• Confidence in ou tcom es from sm all organs• ? h ighe r risk of gra ft loss and dysfunction• Reduced donor recognition
Ne on a t a l d on a t ion• Excluded in som e jurisd ictions, increasingly pe rform ed in
North Am erica• Most com m on causes neona ta l asphyxia , m ajor
m alform ations (i.e . usua lly occur in NICU, not PICU)• Neonata l b ra in dea th is ra re (flexib le su tures/fon tane ls)• Neonata l DCD is an option• Technica l cha llenges
• Donor organ size• En-bloc kidney rem oval m ay have sim ila r gra ft function &
surviva l• Vascula r anastom osis
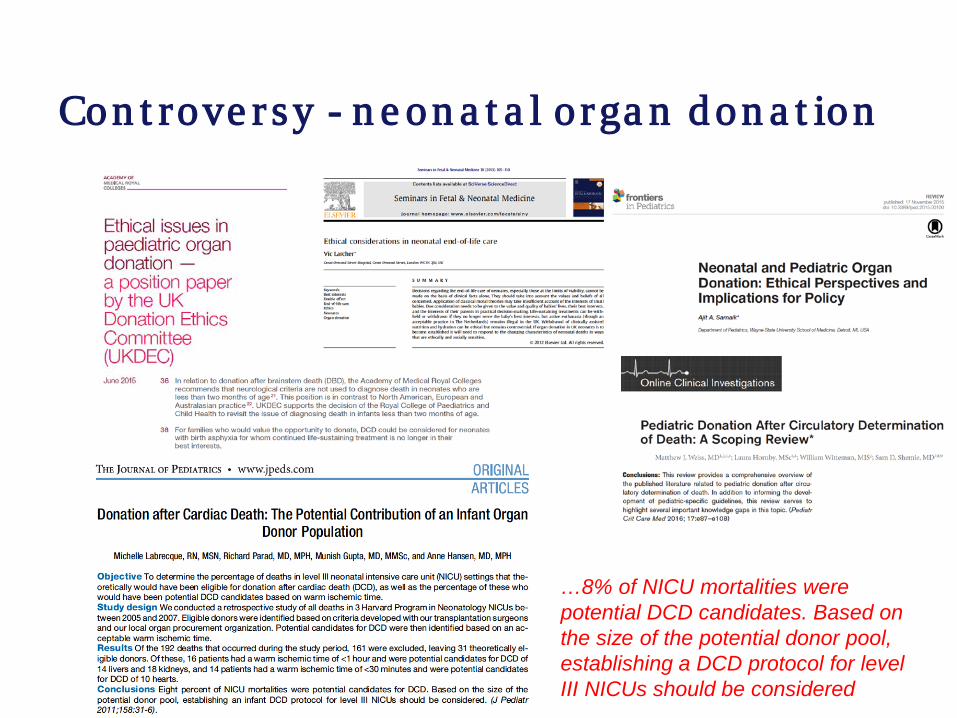
Con t rove r sy - n e on a t a l o rga n d on a t ion
…8% of NICU mortalities were potential DCD candidates. Based on the size of the potential donor pool, establishing a DCD protocol for level III NICUs should be considered
Profe ss ion a l b od y s t a t e m e n t – RCPCH (UK)
• Ability to d iagnose Bra in Death in neonates was questioned in the UK• British Paed ia tric Associa tion (BPA) in 1991
• “it is ra re ly possib le confiden tly to d iagnose bra in stem dea th a t th is age”
• 2015 a working group reviewed evidence to da te• The d iagnosis of “Death by Neurologica l
Crite ria” using the clin ica l exam ination crite ria used to estab lish dea th in adu lts, ch ild ren and o lde r in fan ts, ca n b e con fid e n t ly u se d in in fa n t s from 37 w e e ks co r re ct e d ge s t a t ion (p os t m e n s t ru a l) t o t w o m on t h s p os t t e rm
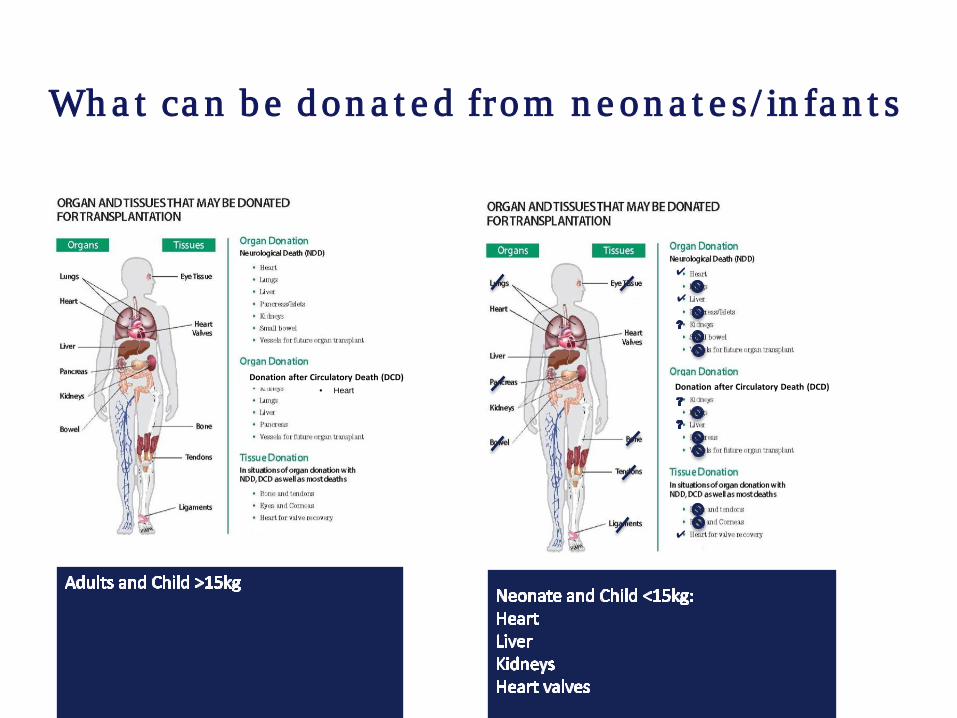
Wh a t ca n b e d on a t e d from n e on a t e s / in fa n t s
• Heart
✔
✔
✔
Donation after Circulatory Death (DCD)Donation after Circulatory Death (DCD)
Con t e n t• Patte rns of dea th in ch ild ren• Pedia tric cha llenges and in fan t dona tion• Re cogn izin g t h e p o t e n t ia l d on or • Bra in dea th te sting in ch ild ren• Pedia tric dona tion a fte r ca rd iac dea th• The fam ily pe rspective and consen t
conside ra tions• Sum m ary
Gu id e lin e s - e xa m p le s
Pe d ia t r ic con s id e ra t ion s• Requirem ents for neurologica l de te rm ination of dea th (BD) in
neonates, in fan ts, and adu lts a re sim ila r• Canada , RCPCH UK, US, ANZ• But:
• Increasingly cau tious with decreasing age , som e with first 24hours postna ta l (ANZICS)
• not re liab le in p re te rm s (im m ature re flexes)• Pupilla ry re flexes p resen t from 30-35 weeks• Response to hypercarb ia is im m ature un til la te p rem aturity
• Tim ing, severity, dura tion of insu lt lead ing to com a (such as pe rina ta l asphyxia) m ay be d ifficu lt to asce rta in
• In in fan ts >1m o <12m o, som e ju risd ictions (e .g. CH) requ ire 24hr obse rva tion pe riod
• In neonates, obse rva tion pe riod of 24 to 48 hours is usua lly recom m ended; in som e ju risd ictions neonata l donation is not a llowed
• Im aging m odalitie s can be used
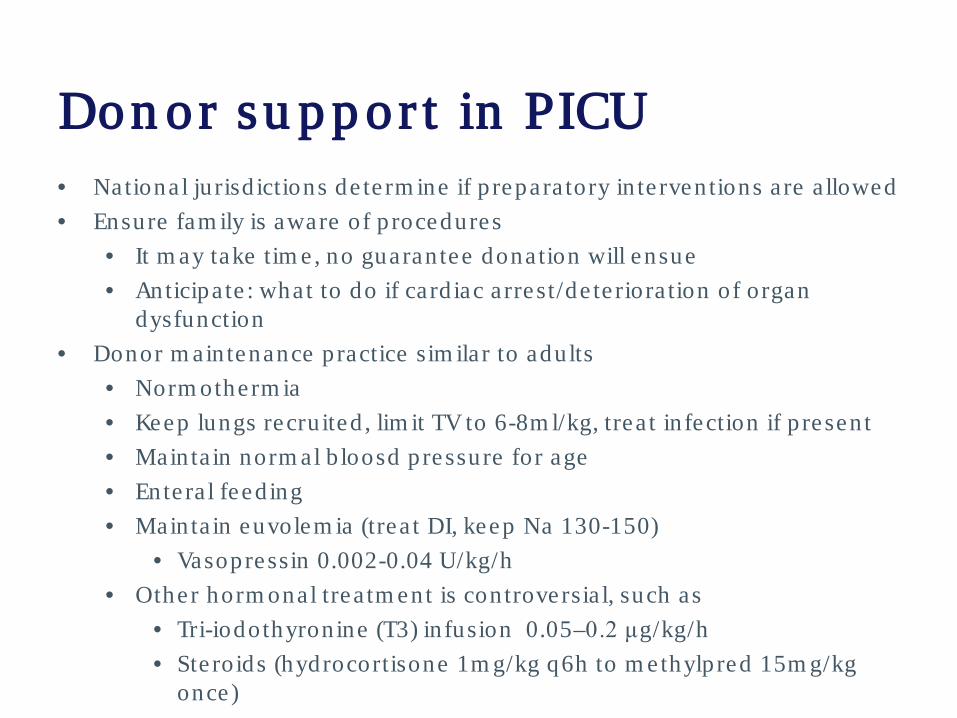
Don or su p p or t in PICU• National ju risd ictions de te rm ine if p repara tory in te rven tions a re a llowed• Ensure fam ily is aware of p rocedures
• It m ay take tim e , no guaran tee donation will ensue• Anticipa te : what to do if card iac a rrest/de te riora tion of organ
dysfunction• Donor m ain tenance practice sim ila r to adu lts
• Norm otherm ia• Keep lungs recru ited , lim it TV to 6-8m l/kg, trea t in fection if p resen t• Mainta in norm al b loosd pressure for age• Ente ra l feed ing• Mainta in euvolem ia (trea t DI, keep Na 130-150)
• Vasopressin 0.002-0.04 U/kg/h• Other horm onal trea tm ent is con troversia l, such as
• Tri-iodothyron ine (T3) in fusion 0.05–0.2 μg/kg/h• Ste roids (hydrocortisone 1m g/kg q6h to m ethylpred 15m g/kg
once)
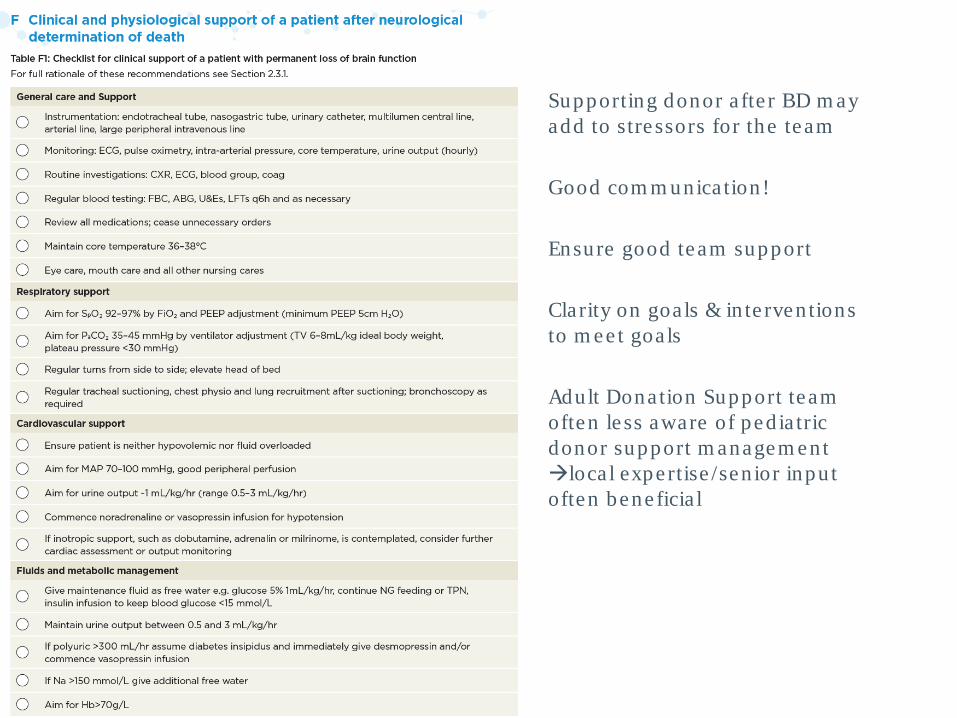
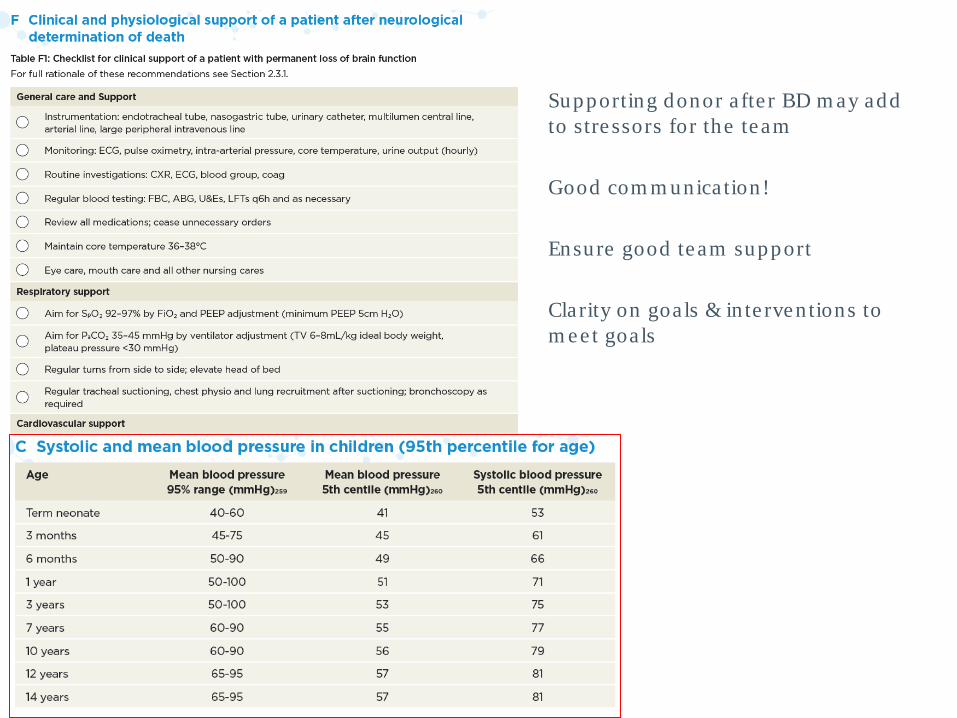
• Supporting donor a fte r BD m ay add to stre ssors for the team
• Good com m unica tion!
• Ensure good team support
• Clarity on goa ls & in te rven tions to m ee t goa ls
• Adult Donation Support team often le ss aware of ped ia tric donor support m anagem ent loca l expe rtise /sen ior inpu t often bene ficia l
• Supporting donor a fte r BD m ay add to stre ssors for the team
• Good com m unica tion!
• Ensure good team support
• Clarity on goa ls & in te rven tions to m ee t goa ls
Con t e n t• Patte rns of dea th in ch ild ren• Pedia tric cha llenges and in fan t dona tion• Recognizing the poten tia l donor • Bra in d e a t h t e s t in g in ch ild re n• Pedia tric dona tion a fte r ca rd iac dea th• The fam ily pe rspective and consen t
conside ra tions• Sum m ary
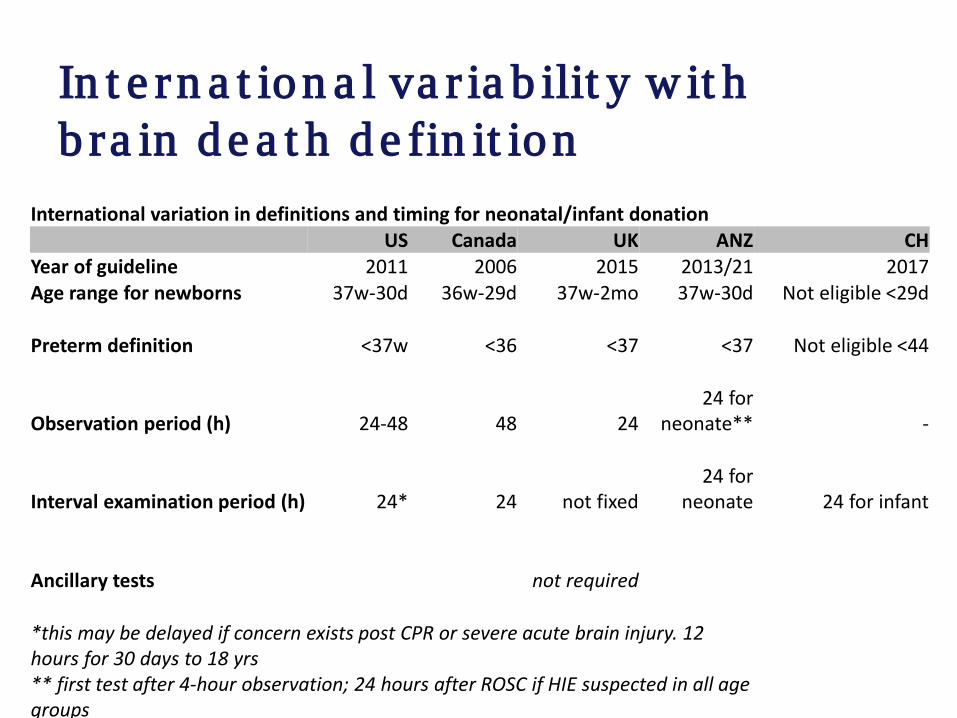
In t e rn a t ion a l va r ia b ilit y w it h b ra in d e a t h d e fin it ion
International variation in definitions and timing for neonatal/infant donationUS Canada UK ANZ CH
Year of guideline 2011 2006 2015 2013/21 2017Age range for newborns 37w-30d 36w-29d 37w-2mo 37w-30d Not eligible <29d
Preterm definition <37w <36 <37 <37 Not eligible <44
Observation period (h) 24-48 48 2424 for
neonate** -
Interval examination period (h) 24* 24 not fixed24 for
neonate 24 for infant
Ancillary tests not required
*this may be delayed if concern exists post CPR or severe acute brain injury. 12 hours for 30 days to 18 yrs** first test after 4-hour observation; 24 hours after ROSC if HIE suspected in all age groups

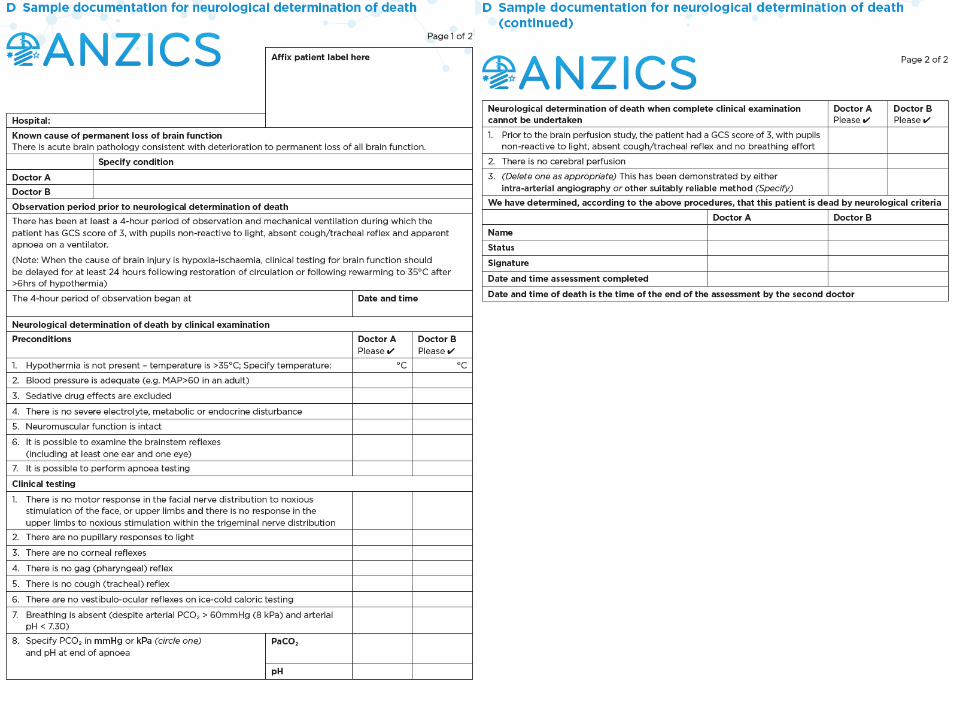
Pe d ia t r ic con s id e ra t ion s – e xa m p le ANZICS
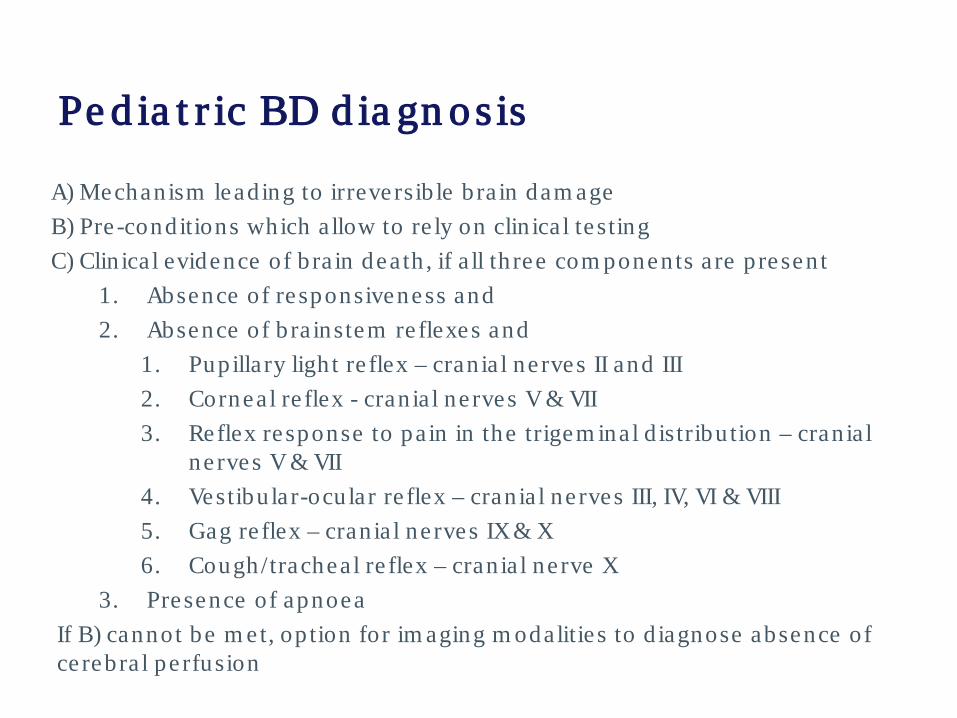
Pe d ia t r ic BD d ia gn os is
A) Mechanism lead ing to irreversib le b ra in dam ageB) Pre -conditions which a llow to re ly on clin ica l te stingC) Clin ica l evidence of b ra in dea th , if a ll th ree com ponents a re p resen t
1. Absence of re sponsiveness and2. Absence of b ra instem re flexes and
1. Pupilla ry ligh t re flex – cran ia l ne rves II and III2. Cornea l re flex - cran ia l ne rves V & VII3. Reflex response to pa in in the trigem inal d istribu tion – cran ia l
ne rves V & VII4. Vestibu lar-ocu lar re flex – cran ia l ne rves III, IV, VI & VIII5. Gag re flex – cran ia l ne rves IX & X6. Cough/trachea l re flex – cran ia l ne rve X
3. Presence of apnoeaIf B) cannot be m et, op tion for im aging m odalitie s to d iagnose absence of ce rebra l pe rfusion
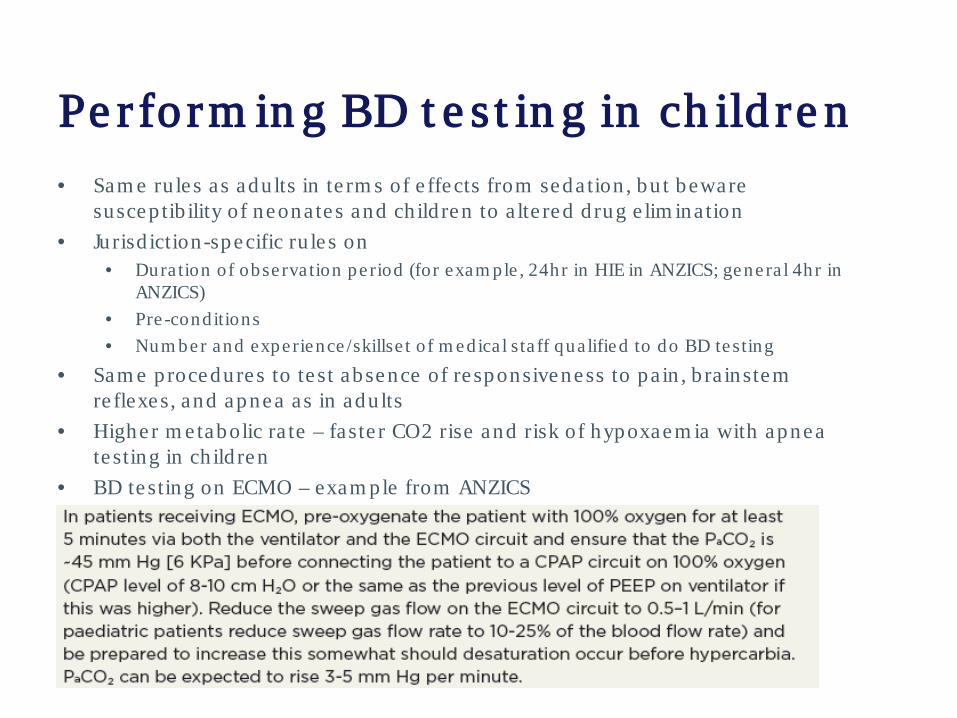
Pe r fo rm in g BD t e s t in g in ch ild re n• Sam e ru le s as adu lts in te rm s of e ffects from seda tion , bu t beware
suscep tib ility of neona te s and ch ild ren to a lte red d rug e lim ina tion• Jurisd iction-specific ru le s on
• Dura tion of obse rva tion pe riod (for exam ple , 24hr in HIE in ANZICS; gene ra l 4hr in ANZICS)
• Pre -conditions• Num ber and expe rience /skillse t of m edica l sta ff qua lified to do BD te sting
• Sam e procedures to te st absence of re sponsiveness to pa in , b ra instem re flexes, and apnea as in adu lts
• Higher m e tabolic ra te – faste r CO2 rise and risk of hypoxaem ia with apnea te sting in ch ild ren
• BD te sting on ECMO – exam ple from ANZICS
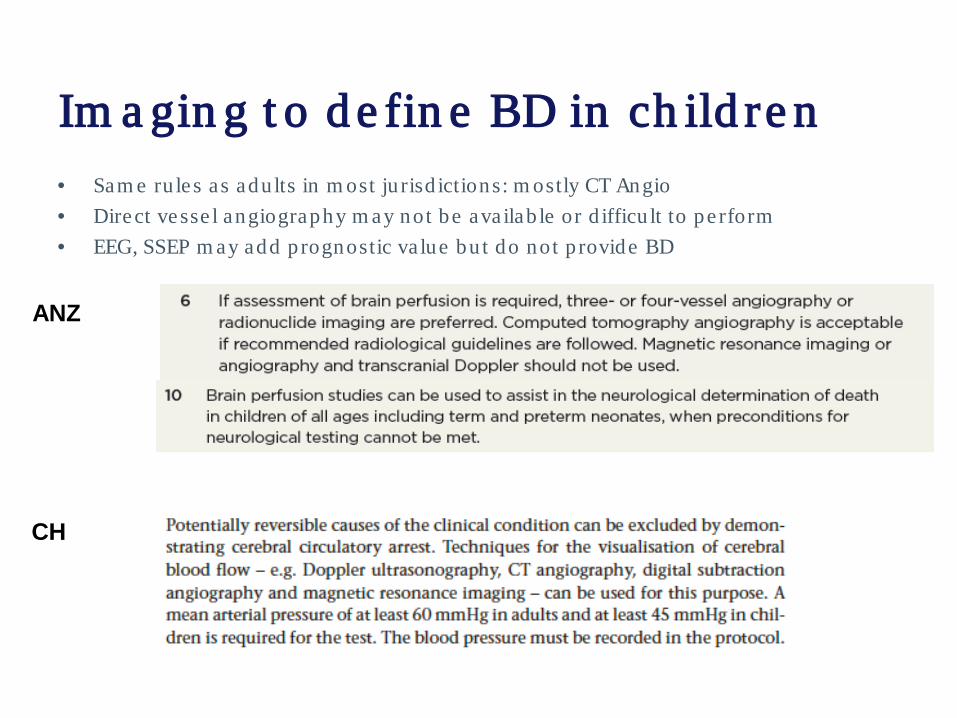
Im a gin g t o d e fin e BD in ch ild re n• Sam e ru le s as adu lts in m ost ju risd ictions: m ostly CT Angio• Direct vesse l angiography m ay not be ava ilab le or d ifficu lt to pe rform• EEG, SSEP m ay add p rognostic va lue bu t do not p rovide BD
CH
ANZ
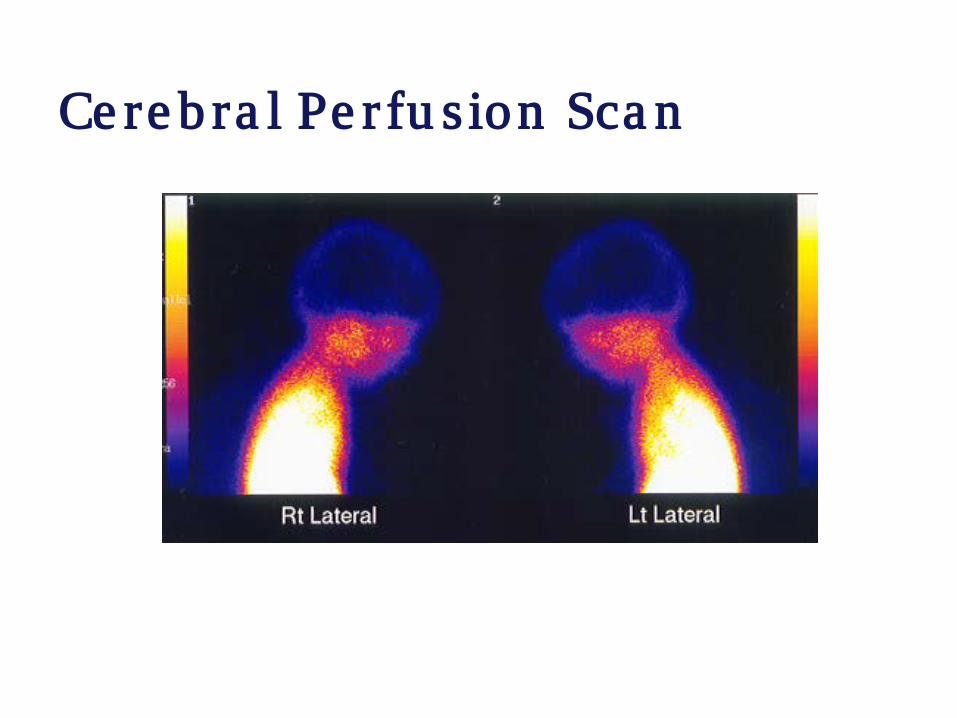
Ce re b ra l Pe r fu s ion Sca n
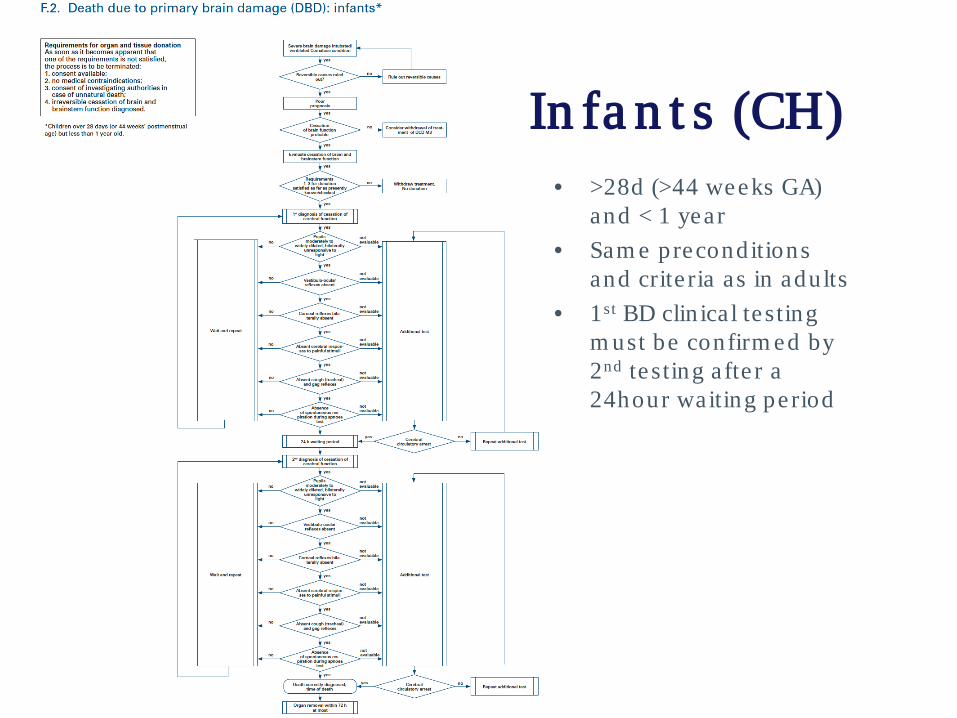
In fa n t s (CH)• >28d (>44 weeks GA)
and < 1 year• Sam e preconditions
and crite ria as in adu lts• 1st BD clin ica l te sting
m ust be confirm ed by 2nd te sting afte r a 24hour waiting pe riod
Con t e n t• Patte rns of dea th in ch ild ren• Pedia tric cha llenges and in fan t dona tion• Recognizing the poten tia l donor • Bra in dea th te sting in ch ild ren• Pe d ia t r ic d on a t ion a ft e r ca rd ia c d e a t h• The fam ily pe rspective and consen t
conside ra tions• Sum m ary
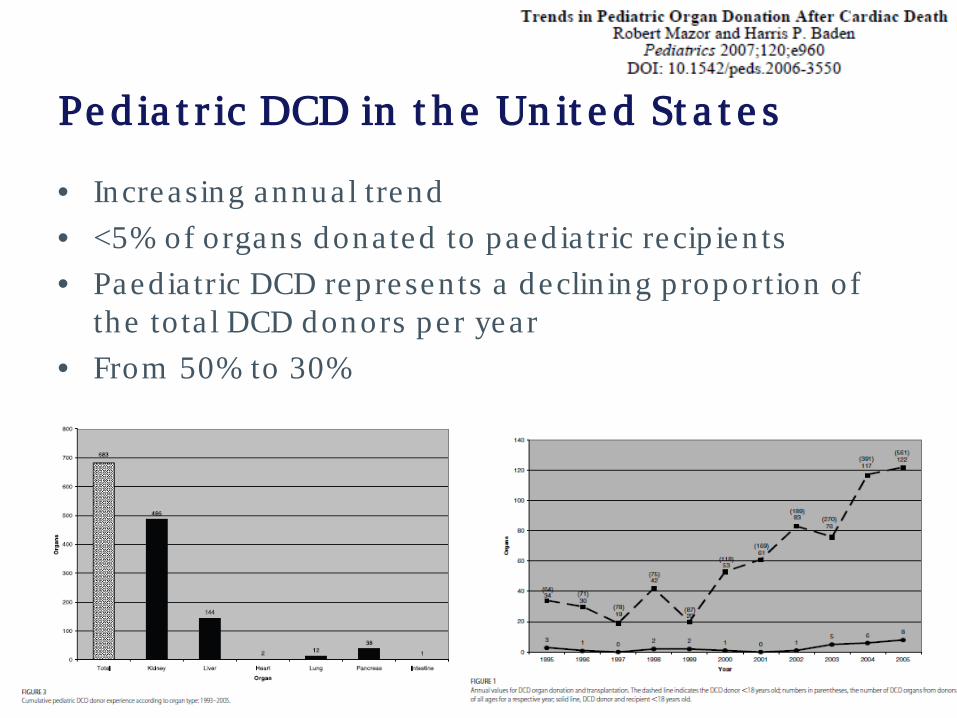
Pe d ia t r ic DCD in t h e Un it e d St a t e s
• Increasing annual trend • <5% of organs dona ted to paed ia tric recip ien ts• Paed ia tric DCD represen ts a declin ing p roportion of
the to ta l DCD donors pe r year• From 50% to 30%
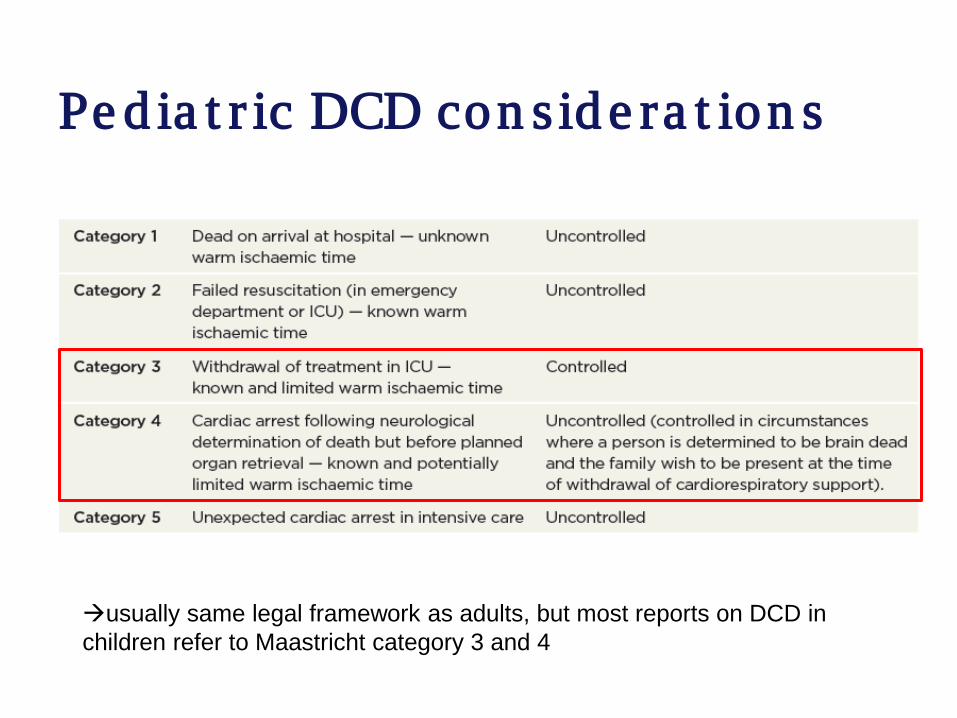
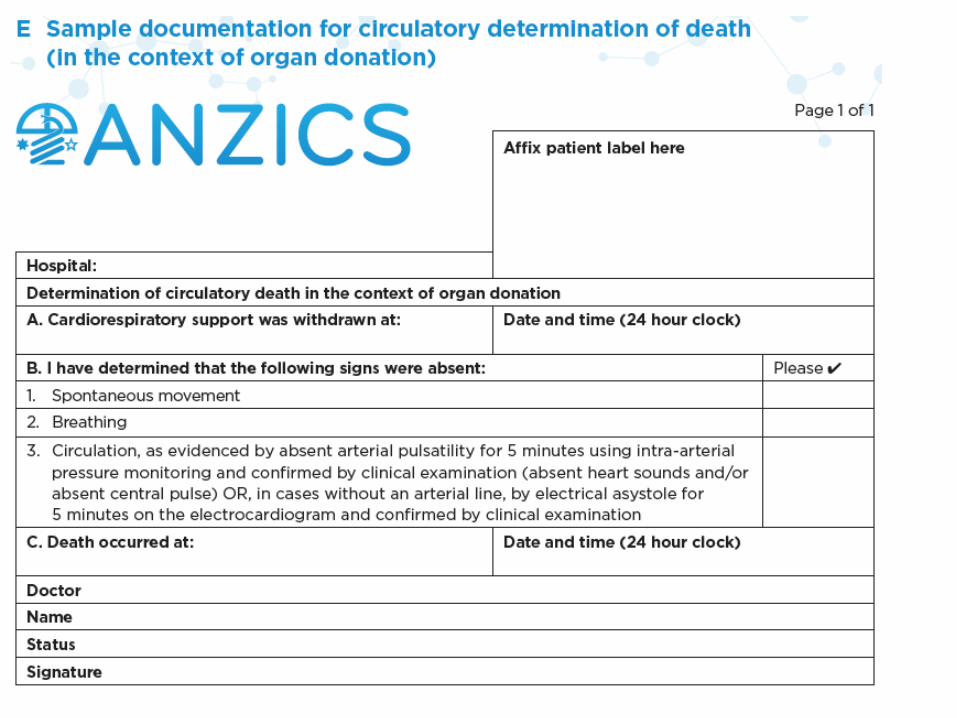
Pe d ia t r ic DCD con s id e ra t ion s
usually same legal framework as adults, but most reports on DCD in children refer to Maastricht category 3 and 4
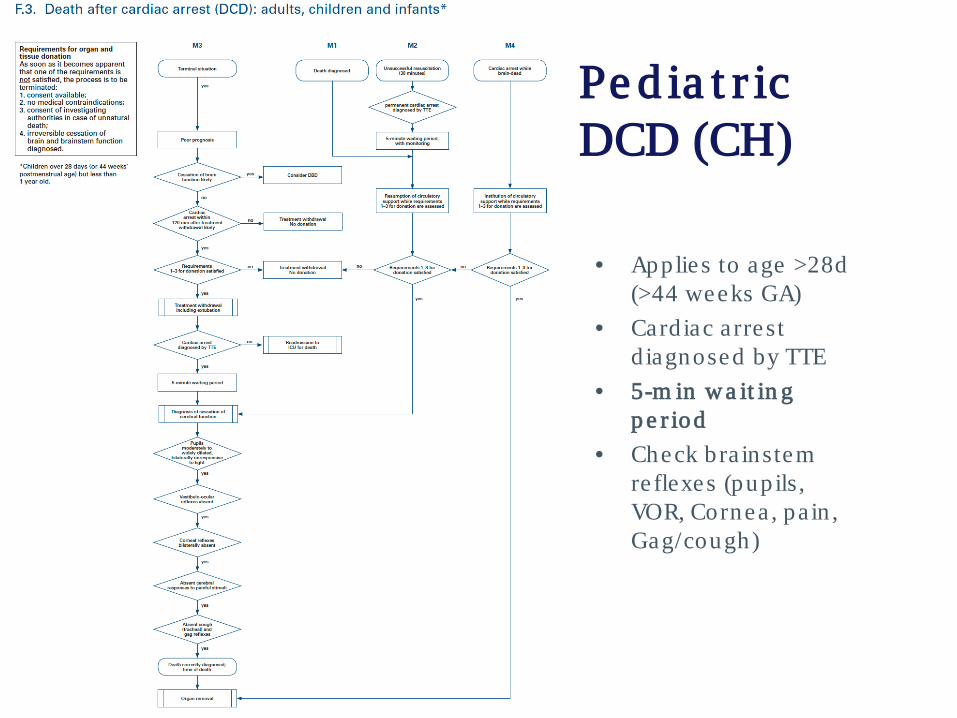
• Applies to age >28d (>44 weeks GA)
• Card iac a rrest d iagnosed by TTE
• 5-m in w a it in g p e r iod
• Check bra instem re flexes (pupils, VOR, Cornea , pa in , Gag/cough)
Pe d ia t r ic DCD (CH)
Con t e n t• Patte rns of dea th in ch ild ren• Pedia tric cha llenges and in fan t dona tion• Recognizing the poten tia l donor • Bra in dea th te sting in ch ild ren• Pedia tric dona tion a fte r ca rd iac dea th• Th e fa m ily p e r sp e ct ive a n d con se n t
con s id e ra t ion s• Sum m ary
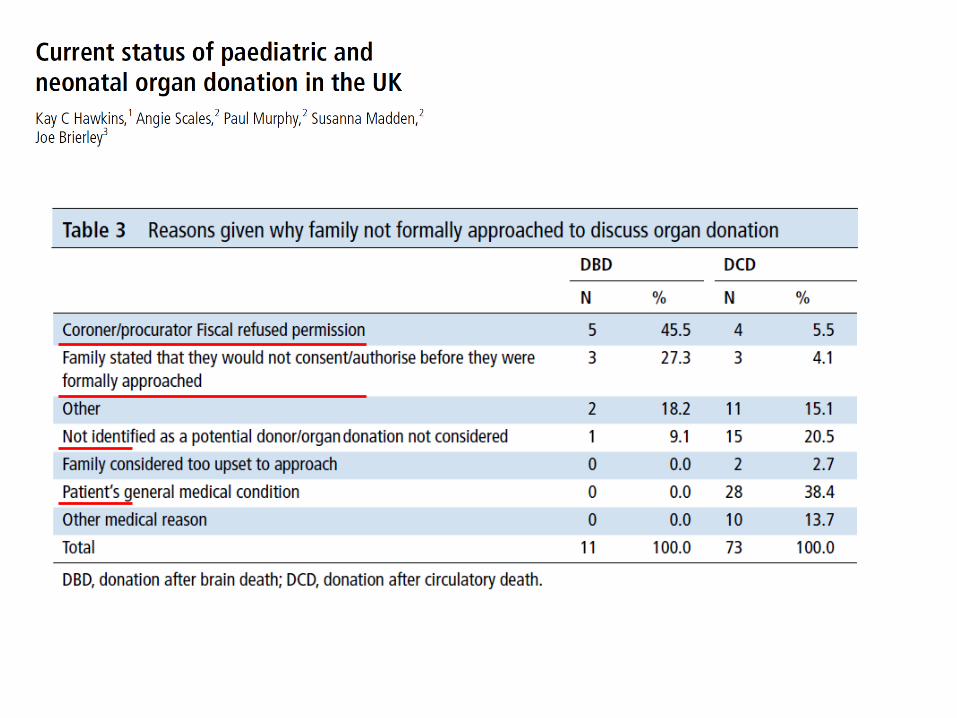
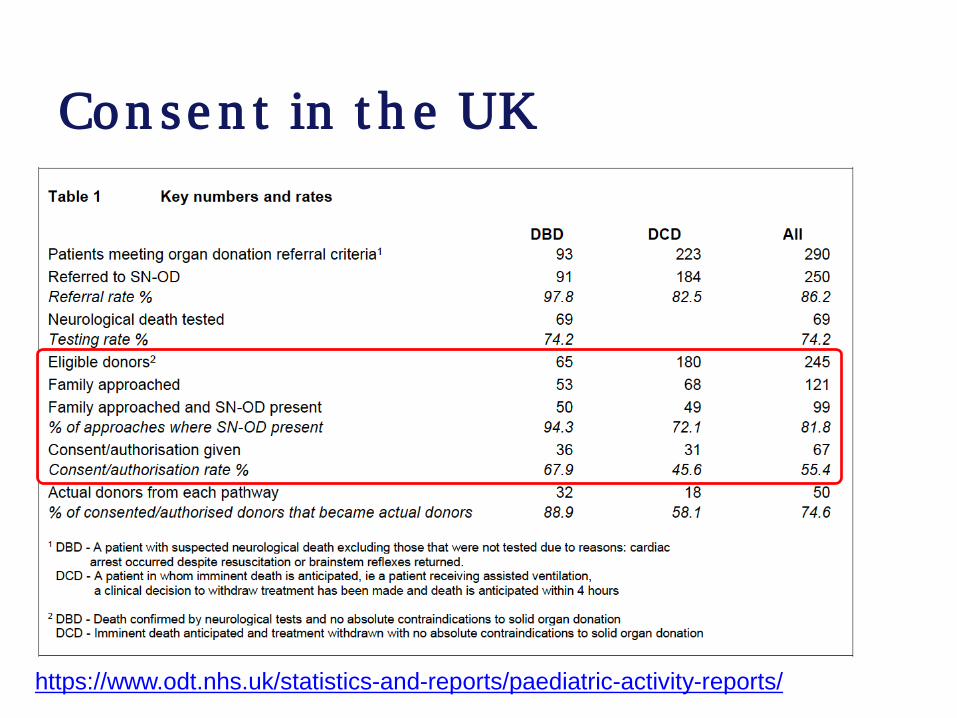
Con se n t in t h e UK
https://www.odt.nhs.uk/statistics-and-reports/paediatric-activity-reports/
Th e fa m ily&p a t ie n t p e r sp e ct iveCh a lle n ge s• Fam ilia rity with donation
fram ework, te sting in ch ild ren• Fam ilia rity with donation
conversa tions in ch ild ren• Low num ber of pa tien ts pe r
PICU; d ifficu ltie s acqu iring experience for PICU sta ff
• Organ donation sta ff m ay be le ss fam ilia r with ped ia tricdonation conversa tions
• Paren ts m ay wish to he lp another ch ild
• In tegrity of the ch ild ` s body
Op p or t u n it ie s• Paren ts m ay wish to he lp o the rs
on behalf of the ir ch ild• a ltru istic• Schools d iscussing organ
donation• Fam ily d iscussions a t hom e –
previous views• Im portance of a fam ily-cen te red
approach ; paren ts as surrogate decision m akers
Orga n d on a t ion – w h y love d on e s sa y ye s?
“I thought if I cou ld give som eone e lse a chance a t a fu ll life then a t least som eth ing good has com e from th is. I know tha t the recip ien ts of these organs will be ab le to live a fu ll and hea lthy life , and pe rhaps even "have it a ll”.”Extract from “Da m ia n 's Gift o f Life ”Book o f Lifehttp :/ /www.dona te life .gov.au/read-book-life# sthash .VvgQjz1a .dpuf
Fa m ily & con ve r sa t ion• Sim ila r cha llenges & opportunitie s as in adults• Im portance of a fam ily-cente red approach; paren ts as
surroga te decision m akers• Donor registrie s usua lly exclude <16 years• Explore d iscussions in fam ily or school on organ dona tion • Explore the fam ily` s pe rception on the ch ild• Anticipa te tha t fam ilie s m ay worry about pa in or d istre ss• Offe r fam ily a ttendance during BD te sting• Enable fam ily presence as logistica lly feasib le during
d iagnosis of DCD• Ensure professiona l socia l worke r/psychologica l support
tra ined with deceasing ch ildren as ab le
Con t e n t• Patte rns of dea th in ch ild ren• Pedia tric cha llenges and in fan t dona tion• Recognizing the poten tia l donor • Bra in dea th te sting in ch ild ren• Pedia tric dona tion a fte r ca rd iac dea th• The fam ily pe rspective and consen t
conside ra tions• Su m m a ry
Ke y p o in t s• Pedia tric organ dona tion is in frequent – im portance of
tra in ing & com m unica tion• Overa ll sim ila r crite ria as adults, BD and DCD• Guide lines require cau tion /obse rva tion pe riods with ea rly
age groups (neona ta l/in fan ts) bu t vary substan tia lly• cha llenges & poten tia l of neona ta l dona tion – technica l
advancem ent• Opportunitie s exist to deve lop dona tion possib ility for
fam ilie s • Understand the poten tia l donor popula tion• Donor recognition & dona tion conversa tions• Deve lop procurem ent and transp lan tpa thways for pedia tric donors



![[PPT]PowerPoint Presentation - MOHAN Foundation - Organ ... · Web viewOrgan Donation Presentation Organ Donation What is Organ donation Organ donation is the process of removing](https://static.fdocuments.net/doc/165x107/5adac0627f8b9a6d7e8d1ad7/pptpowerpoint-presentation-mohan-foundation-organ-vieworgan-donation-presentation.jpg)