Paediatric ICU: Acute Respiratory Distress
26
Paediatric ICU: Acute Respiratory Distress Aylin Seven
description
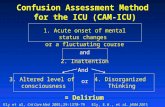
Paediatric ICU: Acute Respiratory Distress. Aylin Seven. Upper – croup/epiglottis Lower – bronchiolitis Lung – pneumonia/ARDS, pulmonary oedema. Neuromuscular Chest wall trauma Pleural effusion Pneumothorax. CAUSES OF RESPIRATORY FAILURE. Cardiac Metabolic Hypovolaemia Septic Shock. - PowerPoint PPT Presentation
Transcript of Paediatric ICU: Acute Respiratory Distress

Paediatric ICU: Acute Respiratory Distress
Aylin Seven

CAUSES OF RESPIRATORY
FAILURE
Upper – croup/epiglottis
Lower – bronchiolitis
Lung – pneumonia/ARD
S, pulmonary oedema
Status EpilepticusApnoea of
prematurityIntoxication
Trauma
NeuromuscularChest wall
traumaPleural effusionPneumothorax
CardiacMetabolic
HypovolaemiaSeptic Shock

Why are kids so vulnerable?• Metabolism
• Risk of apnoea
• Upper airway resistance
• Lower airway resistance
• Efficiency of muscles
• Endurance of muscles (less type 1)
• Lung volumes

Identifying the deteriorating patient
• Respiratory rate• Work of breathing• Bradycardia = BAD

PAT

Normal Respiratory Rates• 1 month to 1 year 24-38
breaths/min• 1-3 y 22-30 breaths/min• 4-6y 20-24breaths/min• 7-9 18-22 breaths/min

What to do next?!

What are your options?
BMVHFONIV
Intubation + Mechanical Ventilation

Positioning etc…• Midline sniffing position• Prominent occiput in
infants towel roll under the shoulders
• Suction (remember nasal suctioning!)
• Nasal + oropharyngeal airways


HFO• Indications:
– Respiratory distress from bronchiolitis, pneumonia, heart failure– Post extubation– Weaning from mask CPAP/BiPAP– Neuromuscular disease– Apnoea of prematurity
• High flow can be used if there is hypoxaemia (SpO2<90%) and signs of moderate to severe respiratory distress despite standard flow oxygen.
• Contraindications:– Blocked nasal passages/choanal atresia– Trauma/surgery to nasopharanyx


Mechanisms of Action • Delivered at near body temp, up to 100% relative
humidity delivering up to 8L/min in neonates without irritation
• Washout of inspiratory dead space improves alveolar ventilation
• HFNC may stent the upper airway reduce upper airway resistance
• Positive distending pressure (but signifcant affected by flow rate, leakage, cannula size)

NIV
• Bubble CPAP • (Others: BiPAP/CPAP)

Bubble CPAP• Indications:– Acute lower airway obstruction – Dynamic upper airway obstruction
(laryngomalacia, tracheomalacia)– Parenchymal lung disease (e.g.
pneumonia)– Ventilation weaning

Bubble CPAP• Contraindications:– Severe cardiovascular instability– Poor respiratory drive (frequent
apnoea/brady)– Congenital malformations of airway– NOTE: relative contraindication in >10-
12kg

Bubble CPAP• Mechanism:– Expiratory arm is under water
generates pressure and oscillations (almost similar to high frequency 15-30Hz)
– Gentle bubbling = vigorous bubbling– No bubbling = loss of seal (often open
mouth)



Intubation• Some important differences in intubating kids:
– Large tongue– High, anterior airway– Acute angle between tracheal opening and epiglottis– Narrowest diameter is cricoid ring (adults = vocal cords)– Laryngospasm (2 x more common in older children, and 3 x more
common in younger children) light sedation, secretions, extubation. Up to 96/1000 in URTI patients.
– Cuffed vs uncuffed and oral vs nasal– ? Apnoeic oxygenation

Mechanical Ventilation
• Indications:– Apnea– Respiratory failure not responsive to O2, HFNC, CPAP, or BiPap– Neurologic compromise– Impaired cardiovascular function – Post-Operative states with impaired ventilatory function
• Some considerations in paediatrics:– Inspiratory time is usually 0.35-0.45s for full term babies
progressively increases to 1.0-1.4s by 8y– No difference in outcomes (mortality and length of ventilation) based
on variety of modes including HFOV

Zebras and PICU• Vascular rings/slings from aberrant
vessels (pulmonary artery sling – anomalous L pulmonary artery and ductus encircling trachea)
• Congenital diaphragmatic hernia• Spinal muscular atrophy• Diaphragmatic palsy (post CTx
surgery)• Tick bite paralysis (toxin binds
covalently to AchR)• Tumours (neuroblastoma and
lymphoma)

Case 1• 10 month old• Admitted to ward with bronchiolitis D3• Increased WOB on the ward transferred to
PICU• Placed on WHO 2L/kg/min initially• Ongoing significant work of breathing• What next?

Case 1• Bubble CPAP no significant
improvement• For intubation unsuccessful
intubation attempts x 3 • Eventual intubation with sevoflurane
induction

References• HNE – ICU guidelines for care of paediatric airway, paediatric
bubble CPAP• Paediatric Airway Management, Santillanes and Gausche-Hill (2008)• Ventilatory strategies in the neonatal and paediatrc intensive care
units, Mesiano & Davis, Paediatric Respiratory Reviews (2008)• Oh’s Intensive Care Manual 2013• The evidence for high flow nasal cannula devices in infants, Haq et
al, Paediatric Respiratory Reviews (2014)• Acute respiratory failure in children, Hammer, Paediatric
Respiratory Reviews (2013)

Questions?