Paediatric Anatomy
5
Paediatric anatomy Anthony Lander Jeremy Newman Abstract Technological and clinical advances in neonatal medicine have enabled the successful management of the preterm infant born at as early as 24 weeks’ gestation. An understanding of the anatomical differences between adults, infants and neonates is essential for the clinician managing newborns. This article illustrates the clinically important varia- tions in anatomy, focussing mainly on the normal neonatal anatomy. Keywords Anatomy; development; infant; neonate Musculoskeletal system Before birth the fetus is weightless within the amniotic sac and can assume any position and still develop normally. In prema- ture babies, malleable developing bones, especially the skull, may become distorted due to gravity, pressure from mattresses or medical equipment. The normal skull is approximately circular in cross-section, whereas many premature skulls develop elliptical cross-sections. This can mean that measurements of head circumference, used as a surrogate for brain volume, may overestimate volume. Head circumference is serially measured, as an abnormally enlarging head could indicate the development of hydrocephalous after a bleed for example. Poor head growth may indicate poor nutrition or neurological impairment. The bones of all children have an important haematopoietic function, which in adults is limited to the red marrow of the ribs, sternum, vertebrae and proximal ends of the humerus and femur. Fontanelles Ossification has not reached the suture lines of the skull at birth and the junctions between the calvarial bones are known as fontanelles. Of the six normally present, the anterior is the largest and transmits the pulsation of the sagittal dural venous sinus, which it overlies. The paired sphenoid and posterior are closed by 6 months and the paired mastoid and anterior by 2 years of age. During parturition the calvarial bones of the neurocranium are displaced and may even overlap at the suture lines to allow passage of the head through the birth canal. Vertebral column At birth the spinal column is very flexible and lacks the fixed curvatures present in adulthood. The thoracic curvature develops first, being concave anteriorly. The cervical develops at around 3 months when the child is able to support the weight of its head and the lumbar when learning to walk at about 1 year. Upper limbs These are well developed and long compared to the neonatal lower limbs. The elbow is unable to fully extend at birth by about 15 . The neonate has a relatively strong grasp reflex and is able to support its own weight within the first days of life. Lower limbs These are under-developed and remain in a flexed and abducted position in the neonate. They appear bowed due to the relative immaturity of the medial head of gastrocnemius compared with the lateral. The general musculature for walking is also not well developed at this stage, giving a rather flat appearance to the buttocks. Respiratory system Airway The tongue is relatively large and the nares small, in comparison with an adult. The larynx is anterior and cephalad (C3-4 vs C6) and the trachea and neck are short. Due to these differences, children up to the age of 5 years may be obligate nasal breathers. The trachea is short and the cricoid cartilage is the narrowest point of the airway in children under 5 years of age. Uncuffed endotracheal tubes can be used to intubate children under the age of 12 years, forming a good seal at the cricoid ring. The thyroid cartilage is shorter and broader in the child and lies nearer the hyoid and its superior notch and laryngeal prominence are less marked. The sexual differences in the larynx are evident by 3 years of age. The trachea is relatively soft in the first year of life and is easily compressed. Respiratory system Alveoli continue to increase in number and size until around 8 years of age. Growth beyond this is seen in both the airways and the alveoli. At term airway patency is maintained by surface active proteins, which are deficient in premature neonates, leading to a higher rate of respiratory failure. This may be treated with the administration of surfactants. Thorax (Figure 1) The neonatal thorax has a rounder circumference when compared to the adult more flattened appearance. It is very compliant and susceptible to collapse during negative intratho- racic pressure. The work of breathing is thus much greater in the child. The type 1 muscle fibres, which are fatigue resistant, seen in adult intercostals and diaphragms, are not prominent until about 2 years of age. The thymus is a large structure in the first year of life and easily causes confusion on chest X-rays. Gastrointestinal system (Figure 1) Oral cavity The large tongue is short and broad, lying entirely within the oral cavity. It begins to descend into the neck during the first year of life, the posterior third forming part of the anterior wall of the pharynx by age 4 years. During suckling the high position of Anthony Lander FRCS(Paed) is a Consultant Paediatric Surgeon at the Birmingham Children’s Hospital, Birmingham, UK. Conflicts of interest: none declared. Jeremy Newman FRCS is a Vascular Surgery Registrar at the Worcester Royal Infirmary, Worcester, UK. Conflicts of interest: none declared. BASIC SCIENCE SURGERY 31:3 101 Ó 2013 Elsevier Ltd. All rights reserved.
-
Upload
risma-pertiwi -
Category
Documents
-
view
242 -
download
4
description
anatomi
Transcript of Paediatric Anatomy
-
Paediatric anatomyAnthony Lander
Jeremy Newman
ences
and
can assume any position and still develop normally. In prema-
o the
hers.
ates,
in adult intercostals and diaphragms, are not prominent until
BASIC SCIENCEAnthony Lander FRCS(Paed) is a Consultant Paediatric Surgeon at the
Birmingham Childrens Hospital, Birmingham, UK. Conflicts of interest:
none declared.
Jeremy Newman FRCS is a Vascular Surgery Registrar at the Worcester
Royal Infirmary, Worcester, UK. Conflicts of interest: none declared.ture babies, malleable developing bones, especially the skull,
may become distorted due to gravity, pressure from mattresses
or medical equipment. The normal skull is approximately
circular in cross-section, whereas many premature skulls develop
elliptical cross-sections. This can mean that measurements of
head circumference, used as a surrogate for brain volume, may
overestimate volume. Head circumference is serially measured,
as an abnormally enlarging head could indicate the development
of hydrocephalous after a bleed for example. Poor head growth
may indicate poor nutrition or neurological impairment.
The bones of all children have an important haematopoietic
function, which in adults is limited to the red marrow of the ribs,
sternum, vertebrae and proximal ends of the humerus and femur.
Fontanelles
Ossification has not reached the suture lines of the skull at birth
and the junctions between the calvarial bones are known as
fontanelles. Of the six normally present, the anterior is the largest
and transmits the pulsation of the sagittal dural venous sinus,
which it overlies. The paired sphenoid and posterior are closed
by 6 months and the paired mastoid and anterior by 2 years of
age. During parturition the calvarial bones of the neurocranium
are displaced and may even overlap at the suture lines to allow
passage of the head through the birth canal.
Vertebral column
At birth the spinal column is very flexible and lacks the fixed
curvatures present in adulthood. The thoracic curvature developsBefore birth the fetus is weightless within the amniotic sacbetween adults, infants and neonates is essential for the clinician
managing newborns. This article illustrates the clinically important varia-
tions in anatomy, focussing mainly on the normal neonatal anatomy.
Keywords Anatomy; development; infant; neonate
Musculoskeletal systemthe successful management of the preterm infant born at as early
weeks gestation. An understanding of the anatomical differAbstractTechnological and clinical advances in neonatal medicine have enabled
as 24SURGERY 31:3 101The large tongue is short and broad, lying entirely within the oral
cavity. It begins to descend into the neck during the first year of
life, the posterior third forming part of the anterior wall of the
pharynx by age 4 years. During suckling the high position ofOral cavityabout 2 years of age. The thymus is a large structure in the first
year of life and easily causes confusion on chest X-rays.
Gastrointestinal system (Figure 1)child. The type 1 muscle fibres, which are fatigue resistant,leading to a higher rate of respiratory failure. This may be treated
with the administration of surfactants.
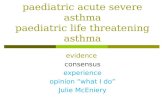
Thorax (Figure 1)
The neonatal thorax has a rounder circumference when
compared to the adult more flattened appearance. It is very
compliant and susceptible to collapse during negative intratho-
racic pressure. The work of breathing is thus much greater in the
seenthe alveoli. At term airway patency is maintained by su
active proteins, which are deficient in premature neonThe trachea is short and the cricoid cartilage is the narrowest
point of the airway in children under 5 years of age. Uncuffed
endotracheal tubes can be used to intubate children under the
age of 12 years, forming a good seal at the cricoid ring. The
thyroid cartilage is shorter and broader in the child and lies
nearer the hyoid and its superior notch and laryngeal prominence
are less marked. The sexual differences in the larynx are evident
by 3 years of age. The trachea is relatively soft in the first year of
life and is easily compressed.
Respiratory system
Alveoli continue to increase in number and size until around 8
years of age. Growth beyond this is seen in both the airways and
rfaceand the trachea and neck are short. Due to these differe
children up to the age of 5 years may be obligate nasal breatRespiratory system
Airway
The tongue is relatively large and the nares small, in comparison
with an adult. The larynx is anterior and cephalad (C3-4 vs C6)
nces,developed at this stage, giving a rather flat appearance t
buttocks.These are well developed and long compared to the neonatal
lower limbs. The elbow is unable to fully extend at birth by about
15. The neonate has a relatively strong grasp reflex and is ableto support its own weight within the first days of life.
Lower limbs
These are under-developed and remain in a flexed and abducted
position in the neonate. They appear bowed due to the relative
immaturity of the medial head of gastrocnemius compared with
the lateral. The general musculature for walking is also not wellUpper limbsfirst, being concave anteriorly. The cervical develops at around
3 months when the child is able to support the weight of its head
and the lumbar when learning to walk at about 1 year. 2013 Elsevier Ltd. All rights reserved.
-
than
BASIC SCIENCEthe larynx is elevated further so that the fluid passes directly into
the pharynx. This enables the infant to feed and breathe at theFigure 1falciform ligamentLarge liver
horizontal diaphragm
Umbilical vein andRelatively flatLarge thymus
Abdomen and chestsame time.
Oesophagus
At birth the oesophagus is approximately 8e10 cm long and
extends from the cricoid cartilage to the gastric cardia (C4 to T9)
and possesses the same constrictions as that of the adult. The
adult oesophagus starts and finishes two vertebral bodies lower
(C6 to T11).
Abdomen
In the adult the abdomen is generally rectangular with the long
axis vertical and the most common open surgical approaches are
made through vertical incisions. In babies the abdomen is
broader than it is long and open procedures are generally made
through transverse supraumbilical incisions.
Stomach
The stomach is very small at birth and lies under the liver. If
a gastrostomy is needed its placement may not be easy in the first
few days of life. This is particularly so if there is no antenatal
swallowing in the case of an isolated oesophageal atresia, when
the stomach may be less than 5 ml in volume. The stomach
distends fivefold in the first few days once swallowing and feeds
commence. Acid secretion begins during the first day of life. The
stomachs anterior surface is nearly entirely covered by the left
lobe of the liver, only a small portion of the greater curvature
being visible below. Its size increases rapidly from 30 ml in
a term baby to 100 ml by the fourth week. An adults stomach
has a capacity of approximately 1 litre.
SURGERY 31:3 102Small and large intestine
The small intestine has fewer and less marked circular foldsLateral umbilical fold (inferiorepigastrics)
Medial umbilical fold (umbilicalartery)
Urachusof liverSmall stomach under left lobe are seen in adults. The mesentery contains very little fat and is
much easier to manage when resecting intestine than in adults.
The small intestine is between 300 and 350 cm long in a term
baby. This is a measurement with the bowel under gentle tension
and the mesentery removed. At a laparotomy with normal
smooth muscle tone and a normal mesentery the small intestine
appears closer to 120 cm than 300. The small intestine lies in
a more transverse orientation than in the adult due to the
abdominal bladder. The large intestine is approximately 60 cm
long and has a very poorly developed muscularis. The ascending
and descending colon are relatively short and the transverse
colon relatively longer. The normal haustra and appendices
epiploicae are not present, giving it a very smooth outline. The
haustra appear over the first 6 months.
Liver
The liver is relatively large in the neonate being 4% of body
weight compared to the adult where it constitutes only 2.5e3%.
The right lobe extends below the costal margin anteriorly and lies
close to the iliac crest posteriorly. The left lobe can extend to the
lateral wall of the abdomen, overlying the stomach and the
spleen.
Gallbladder
The gallbladder does not extend to the edge of the liver and has
a small peritoneal surface. The majority are embedded within the
liver. After the second year of life it has proportionately similar
characteristics to an adult. It is easy to miss the gallbladder at
2013 Elsevier Ltd. All rights reserved.
-
a neonatal laparotomy, but its presence should be documented
since an absent gallbladder is associatedwith some rare anomalies.
Pancreas
The pancreas has a relatively large head and its body points
upwards and to the left towards the tail.
Peritoneal cavity
The anterior abdominal wall bulges forwards in the neonate to
accommodate the bladder, uterus and ovaries, which are pelvic
in the adult. This is accentuated by the flattened diaphragm
pushing down on the supracolic compartment.
Genitourinary system (Figures 2 and 3)
The kidneys
The kidneys are lobulated at birth, have wide-calibre ureters and
lie under relatively large adrenal glands.
Bladder
The apex of the unfilled bladder lies midway between the pubis
and the umbilicus and, when filled, may reach the umbilicus.
Only the posterior surface is covered with peritoneum and,
although considered intra-abdominal, about half lies within the
pelvic cavity. It does not truly become pelvic until about the sixth
million or so remaining at birth, only about 400 will actually
ovulate.
Uterus
The uterus is influenced by the maternal hormones during fetal
development and so usually decreases by about a third in size
after birth until puberty is reached. At birth it is approximately
2.5e5 cm long and 2 cm wide, the uterine cervix accounting for
two-thirds of this. Occasionally the early response to the with-
drawal of maternal hormones is accompanied by a small uterine
bleed.
Testes
The testes are situated at the deep ring by the sixth month of
gestation and 98% in term babies and 80% in preterm babies will
have descended into the scrotum by birth. The processus vagi-
nalis is collapsed at birth, but not necessarily obliterated. Eighty
percent are obliterated 10e20 days after birth. Undescended
testes are a common surgical problem and if a testis has not
descended to the scrotum by 3 months of age surgical referral is
essential and an orchidopexy is typically performed around 1
year of age.
Inguinal canals
The inguinal canal is similar to the adult and it is rarely true that
ough
lar
BASIC SCIENCEFigure 2Right gonadal vesselsLarge adrenalsInferior vena cavaOvaries
The ovaries are much larger than the testes at birth and weigh
approximately 0.3 g. They lie in the iliac fossae at birth and
descend into their pelvic position in early childhood. All the
primary oocytes are present after the first trimester. Of the 1
Lobulated newborn kidneys andThis may rarely be patent and leak urine.year of life. The ureters correspondingly do not have a pelvic
component until that time also. The top of the bladder is
continuous with the urachal remnant (median umbilical ligament
and the overlying median umbilical fold) reaching the umbilicus.SURGERY 31:3 103Left gonadal vesselsge adrenalsa small opening in the front of the canal is possible. The canal is
short, but so are the arms and legs!
Cardiovascular system
Heart
At birth the right ventricle has been working against systemic
pressure and the muscular bulk is therefore only 25% smalleringuinal hernias the canal has some length and a repair thrthe internal and external rings overlap e this is a common
misconception. Even in small premature neonates with large 2013 Elsevier Ltd. All rights reserved.
-
BASIC SCIENCEStraighter anorectal angle than in an adultPelvic anatomy
Ovary in the iliac fossa
Prominent uterus at birththan the left. However after birth, when the fetal circulation
changes and pulmonary circulation is established, the left
ventricle rapidly grows and its muscular bulk becomes about
twice of the right at 2 years of age. This difference continues into
adulthood. The ventricular volumes in a heart with normal
connections are of course very similar.
Foramen ovale
This lies at the level of the third intercostal space between the
right atrium and left atrium. It is approximately 5 mm vertically
by 4 mm wide in size and allows blood to bypass the pulmonary
circulation in the fetus. Once respiration starts and the pulmo-
nary circulation is established it functionally closes. It is oblit-
erated in 3% of infants by 2 weeks and 90% by 16 weeks.
Ductus arteriosus
The ductus arteriosus, roughly 8e12 mm long, bypasses the
pulmonary trunk to the arch of the aorta in the fetus. It arises
as a direct continuation of the pulmonary trunk at the point it
divides into left and right pulmonary arteries. Its diameter is
approximately the same size as the ascending aorta (5 mm)
and joins the descending aorta just below the left subclavian
artery.
Like the umbilical artery and vein which also occlude after
birth, the wall of the ductus arteriosus is populated by smooth
muscle, connective tissue and elastic fibres which proliferate close
to birth. Bradykinin is released by the lungs on adequate exposure
to oxygen and from the umbilical cord when the temperature
Figure 3
SURGERY 31:3 104Up to 2% of testes may be undescended at birth, 0.8% by 1 yearat birth96% of foreskinsadherent to glansApex of bladder lies highdrops after birth. This causes constriction of the ductus arteriosus
and the umbilical vein and artery. Occasionally the duct remains
patent and problematic. If closure does not follow drugs such as
indomethacin or a surgical ligation may be needed.
Umbilical arteries
These are a direct continuation of the internal iliac arteries. At
birth the smooth muscle in the wall constricts and the arteries are
obliterated. The remnants of these arteries become the medial
umbilical ligaments seen on the undersurface of the anterior
abdominal wall covered by the medial umbilical folds. For
completeness remember that more lateral, still, are the lateral
umbilical folds overlying the inferior epigastric vessels (see
Figure 1).
Umbilical vein
This passes from the umbilicus, within the falciform ligament,
superiorly and to the right for 2e3 cm to the porta hepatis. It
gives off several branches to the liver before joining the portal
vein. It also contracts after birth and its remnant is the liga-
mentum teres.
Ductus venosus
Before birth the ductus venosus shunts most of the umbilical
venous blood into the inferior vena cava allowing oxygenated
blood to bypass the liver. The ductus venosus closes during the
first week of life in term neonates but may take longer to close
in pre-term babies. The remnant of the ductus is the
2013 Elsevier Ltd. All rights reserved.
-
ligamentum venosum. The ductus can be used for venous
access in the newborn.
Lymphatic system
Lymphoid tissue is in abundance in the neonate and continues to
increase throughout childhood.
Thymus
This weighs approximately 10 g at birth and continues to
increase in size until puberty, when it weighs about 30 g. It
decreases in adulthood and weighs about 12 g in old age. It lies in
the anterior mediastinum overlying the great vessels of the
superior mediastinum and may reach up into the cervical region
as far as the thyroid gland.
Spleen
Accessory spleens are very common in the neonate and usually
found in the greater omentum.
Summary
The anatomical and mechanical differences that distinguish
babies and children from adults have implications for the
management of the airway and surgical approaches to the
abdomen. Some of the differences that persist into infancy and
early childhood also affect the response to trauma and have
implications for trauma management. A
FURTHER READING
Advanced trauma life support for doctors, 8th edn. American College of
Surgeons, 2009.
Advanced paediatric life support, 4th edn. American Academy of Pediat-
rics, 2009.
Grays anatomy: the anatomical basis of medicine and surgery, 38th edn
(British Edition). Edinburgh: Churchill Livingstone, 2009.
BASIC SCIENCESURGERY 31:3 105 2013 Elsevier Ltd. All rights reserved.
Paediatric anatomyMusculoskeletal systemFontanellesVertebral columnUpper limbsLower limbs
Respiratory systemAirwayRespiratory systemThorax (Figure 1)
Gastrointestinal system (Figure 1)Oral cavityOesophagusAbdomenStomachSmall and large intestineLiverGallbladderPancreasPeritoneal cavity
Genitourinary system (Figures 2 and 3)The kidneysBladderOvariesUterusTestesInguinal canals
Cardiovascular systemHeartForamen ovaleDuctus arteriosusUmbilical arteriesUmbilical veinDuctus venosus
Lymphatic systemThymusSpleen
SummaryFurther reading