
Packaging Evidence: Integrating Evidence Into the Care ... · PDF fileA Prepaid Integrated...
42
Canadian Agency for Drugs and Technology in Health 2008 CADTH Invitational Symposium April 28, 2008 Marguerite Koster, MA, MFT Practice Leader Technology Assessment and Guidelines Unit Kaiser Permanente Southern California Packaging Evidence: Integrating Evidence Into the Care Delivery Process
Transcript of Packaging Evidence: Integrating Evidence Into the Care ... · PDF fileA Prepaid Integrated...
Canadian Agency for Drugs and Technology in Health 2008 CADTH Invitational Symposium April 28, 2008
Marguerite Koster, MA, MFTPractice LeaderTechnology Assessment and Guidelines UnitKaiser Permanente Southern California
Packaging Evidence: Integrating Evidence Into the Care Delivery Process

2
Presentation Overview
About Kaiser Permanente
About KP Southern California
Knowledge Transfer/Exchange Issues
Example: Pap/HPV Screening
Lessons Learned

3
Social Mission
Quality Driven
Shared Accountability for Program Success
Integration along Multiple Dimensions
Prevention & Health Maintenance Focus
A Prepaid Integrated Health Care Delivery System
KaiserFoundationHospitals
PermanenteMedicalGroup
KaiserFoundationHealth Plan
Kaiser Permanente
About Kaiser Permanente

4
About Kaiser Permanente
Nation’s largest nonprofit health plan (founded 1945)
Integrated health care delivery system
8.7 million members13,000+ physicians150,000+ employees
8 regions in 9 states and D.C.32 hospitals and med centers430+ medical offices
$37.8 billion annually (2007)
Description:
People:
Facilities:
Revenue:
CO
OR
SCal
GA
OHVA
MDDC
HI
WA
NCal

5
KP Southern California
One of KP’s largest regions
3.3 million members• from 140 countries• 90 different languages spoken
6,000 physicians13,000 nurses55,000 employees
12 hospitals and med centers130 medical offices
$9 billion annually (2007)
Description:
People:
Facilities:
Revenue:
CO
OR
SCal
GA
OHVA
MDDC
HI
WA
NCal

6
Clinical Practice Guidelines
Medical Technology Assessment
Evidence-Based Implementation
Produce evidence-based technology assessments (evaluate devices, equipment, medical and surgical procedures)
Staff Medical Technology Inquiry Service (respond to 500-600 inquiries per year)
KPSC Technology Assessment & Guidelines Unit
Develop/update 30 evidence-based clinical guidelines to support KPSC clinical strategic goals
Focus on key levers in process of care
Produce evidence reviews on the effectiveness of implementation strategies
Produce evidence reviews to support clinical content for KP electronic health system (“KP HealthConnect”)

7
KPSC Technology Assessment & Guidelines Unit (cont.)
Function has been performed within KPSC since the early 1990s
Unit includes 10 research analysts with backgrounds in epidemiology, statistics and research methods
With support from senior leadership, has helped to build a strong evidence-based culture among clinicians and administrators
Knowledge products generally well-received due to involvement of key clinician leaders in all phases:
topic selection
evidence review/synthesis
content development for knowledge products
implementation and knowledge exchange activities

8
The Challenge
Integrating evidence-based knowledge into the care delivery process
“Making the right thing easy to do”
Selecting implementation strategies that are effective for a wide range of clinicians, administrators, operations staff and members

9
Knowledge Transfer/Exchange Process
Synthesis Transfer Exchange Goals
Identify issues; obtain input from target audience
and analysts
Stakeholder review and approval of
recommendations
Key messages for
clinicians
Key messages for
members
Key messages for champions/
leaders
•Printed booklets•Newsletters•Web content•Outreach•Health risk assessment•“Thrive” media campaign
•Direct mail•Online content•CME presentations•EHS alerts/orders•Proactive encounter
•Detailing toolkit –modified to suit local context
•Module posters/signage•Local presentations
Increase member awareness/
engagement in preventive health
Increase appropriate
ordering Pap/HPV x 3
years
Change operations at
medical center level to support
screening initiatives
Systematic evidence review, documentation
and draft recommendations

10
Example: Pap/HPV Screening
Screening practice inconsistent
internal data showed that practitioners not following KPSC guidelines (Pap x3 yrs, after 2 normal tests w/in KP system)
medical specialty societies continued to recommend annual screening despite evidence
members requesting annual screening (influenced by media)
HPV test approved in 2003 for use in conjunction with conventional or liquid-based cytology
Opportunity to standardize practice, increase screening rates, offer reassurance to clinicians and members that 3-year screening interval was effective
“Win-Win”

11
Evidence Synthesis
Formed Guideline Development Team of key stakeholder groups
Defined key research topics for evidence review
Conducted formal, systematic review and critical appraisal of available evidence
Involved key stakeholder groups in development, review and approval of recommendations
Physicians on Guideline Team
Medical Directors
Chiefs of Service (Family Medicine, Internal Medicine, Ob/Gyn)
Operations: Regional/local lab managers, department administrators, clinic assistants
Physician champions
12
Evidence Synthesis (cont.)
Results of 2004 KPSC systematic evidence review and cost/benefit analysis:
Sensitivity of high-risk HPV tests for CIN II or worse (95%) exceeds that of liquid based cytology (90%) and conventional pap (71%)
Pap + HPV every 3 years – as effective as annual Pap, but at a lower cost– MORE cost-effective than current practice (mix of annual,
biennial and triennial screening)

13
Enlisted Guideline Team to develop key messages for:
Champions/Leaders
Clinicians
Operations/support staff
Health Education staff
Members
Initially focused on combination of “passive” and “active” strategies:
Printed materials via direct mail and online
Toolkit developed for detailing by champions at all medical centers
CME presentations by a respected gynecologic oncologist given at all medical centers and selected symposia (“peer to peer”)
Regional implementation manager conducted site visits at all medical centers
Training of physicians, nurses and medical assistants
Knowledge Packaging

14
Why use “passive” strategies?
KPSC physician survey conducted in 2004:
Response Rate Information Totals
SCPMG physicians identified (partners & associates) 5,495
SCPMG physicians with a KP e-mail address listed N = 4,418 (80.4%)
Number of SCPMG physicians included in survey pretest 22
Number of e-mails returned as ‘undeliverable’ 184
Number of survey responses (including pretest) 1,409
Response Rate = 1,409/(4,418-184) * 100 = 33.3%
Source: KPSC Clinical Practice Guidelines Physician Survey, May 2004

15
Why use “passive” strategies?
5%
7%
9%
12%
26%
42%
0% 10% 20% 30% 40% 50%
Other/Missing
CD-ROM
Hard copy
Online web site
Handbook
Sour
ce
Percent of Responding Physicians
Preferred Format For Receiving Guideline Information
Source: KPSC Clinical Practice Guidelines Physician Survey, May 2004

16
Clinical Practice Guideline Mailer
• Physicians (family/internal medicine, Ob/Gyn and Pediatrics
• Physician assistants, nurses• Department Administrators• Quality improvement staff• Physician & member
education staff• Executive/operations staff
Direct mailing of 4-page printed booklet to:
17
Clinical Practice Guidelines Handbook
• All physicians, physician assistants, nurses
• Department Administrators• Quality improvement staff• Physician & member
education staff• Executive/operations staff
Direct mailing of handbook to:

18
Intranet Web Site
Content posted on KPSC intranet web site

19
Intranet Web Site (cont.)
• Guideline• Evidence review• Links to member
education• HTML & PDF
formats
Content posted on KPSC intranet web site:
20
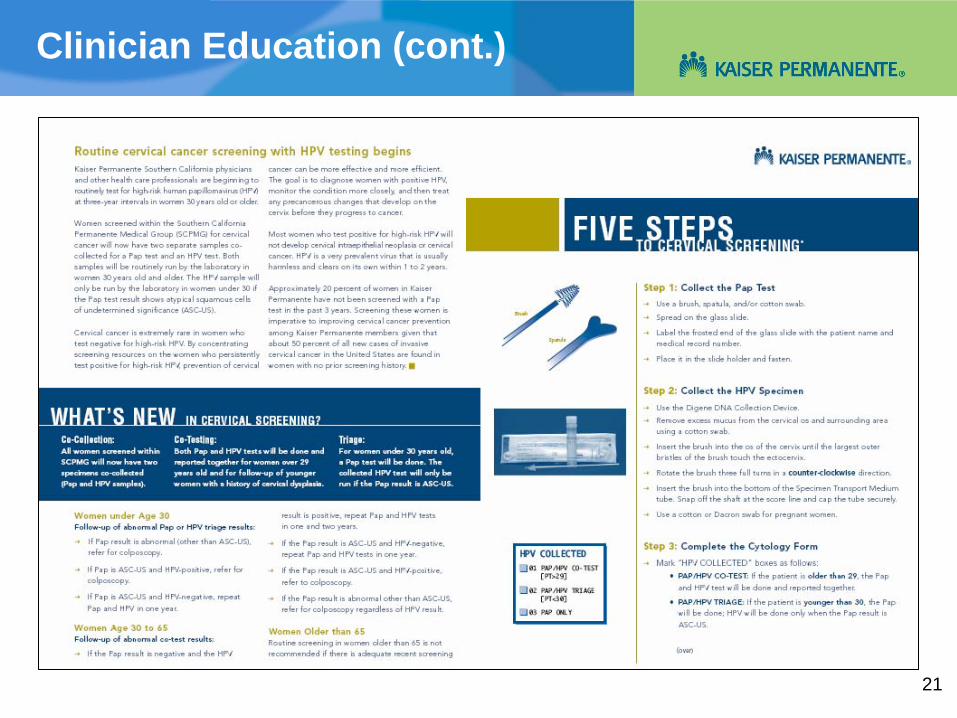
Clinician Education
Detailing toolkit – modified to suit local context
Training sessions with staff
CME presentations at each medical center
Detailing, training and education sessions:
21
Clinician Education (cont.)

22
Physician Education (cont.)

23
Physician Education (cont.)

24
Point-of-Care Posters

25
Point-of-Care HPV Instructions
• HPV specimen kits developed, including instructions for sample collection and submission to lab
• Available in exam rooms

26
Member Education Materials
• Booklet available to members
• Addressed key messages re screening interval and HPV virus
• Languages: English, Spanish, Chinese, Armenian
27
Transition to Electronic Health System
In the past three years, KPSC has implemented an extensive electronic health system – KP HealthConnect™
Offers opportunity to integrate evidence and influence clinician decision making at the point of care
“Making the right thing easy to do”

28
Pap/HPV Decision Support Alerts
Designed to support workflow and facilitate actions
Separate alert displays for the provider and is designed to complement the alert for “back office” staff
Alerts focus on the partnership between clinicians, staff and patients in providing quality, evidence- based preventive care while supporting organizational goals
29
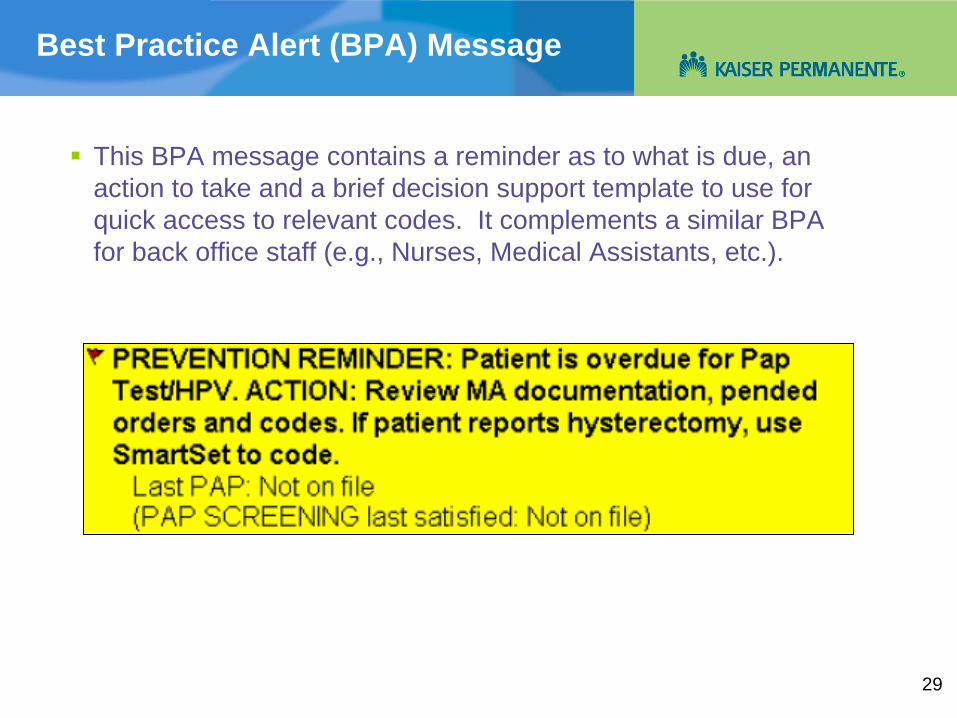
Best Practice Alert (BPA) Message
This BPA message contains a reminder as to what is due, an action to take and a brief decision support template to use for quick access to relevant codes. It complements a similar BPA for back office staff (e.g., Nurses, Medical Assistants, etc.).

30
Progress Notes
Information added from back office staff (e.g., nurses, medical assistants, etc.) can be read in a section for “progress notes”

31
Pending Orders
Orders pended for physician review and signature, if appropriate, are marked as “pending”

32
Proactive Office Encounter
All processes, tools, and workflow which support the healthcare team in all settings, prior to, during, and after a member-initiated encounter (e.g., face-to-face office visit, telephone message, e-mail, etc.)

33
Proactive Office Encounter (cont.)
34
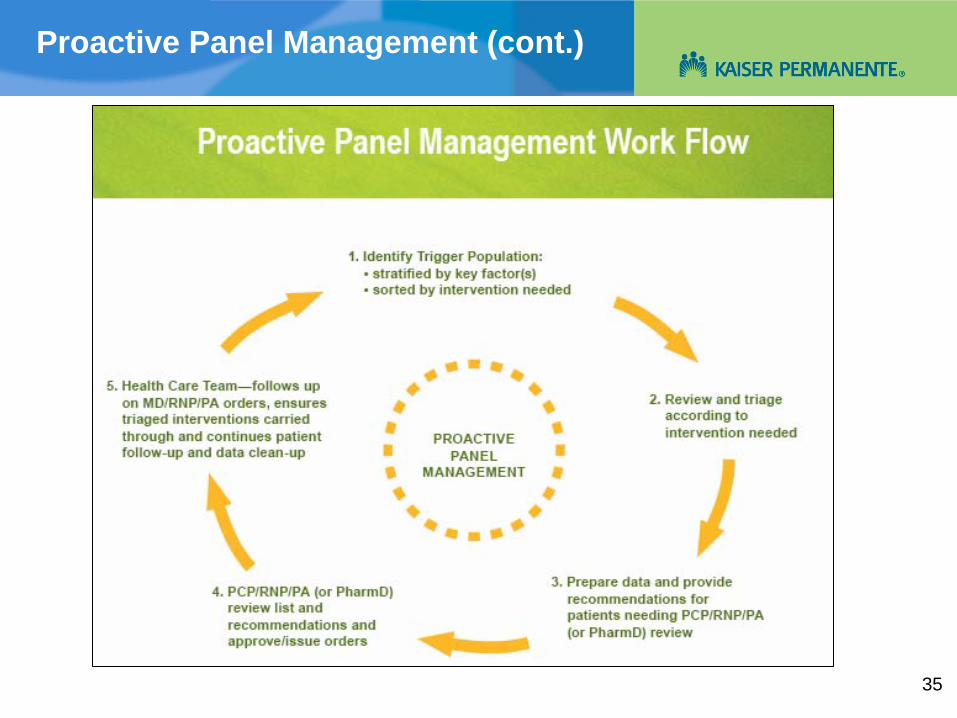
Proactive Panel Management
Supports the physician outside of an encounter to reliably and effectively manage the care of their panel of members, especially those not actively seeking care
It is a process for the systematic and periodic review of a target group (“trigger” population) of a physician’s panel of patients
Triages patients and produces decisions and patient-specific, physician orders for actions the health care team can put into effect
The outcome advances the patient along an agreed-upon care path for the purpose of closing care gaps
35
Proactive Panel Management (cont.)

36
Outreach Efforts
A centrally coordinated system that targets populations through batch mechanisms outside of the patient encounter (e.g. letters, calls, e-mails, etc.)
Supports physician efforts to engage members in actions that improve health outcomes
Targets members who do not come in for regular visits
Process:
Recorded call notifies member of a message from Kaiser Permanente (due for a Pap/HPV test)
Member calls KP Notification System to retrieve message
Member makes appointment
If no response, call followed up by mailed letter, e-mail, etc.

37
KP Online – My Health Manager
Reminders for Pap/HPV screening are available online in member’s personal medical record
38
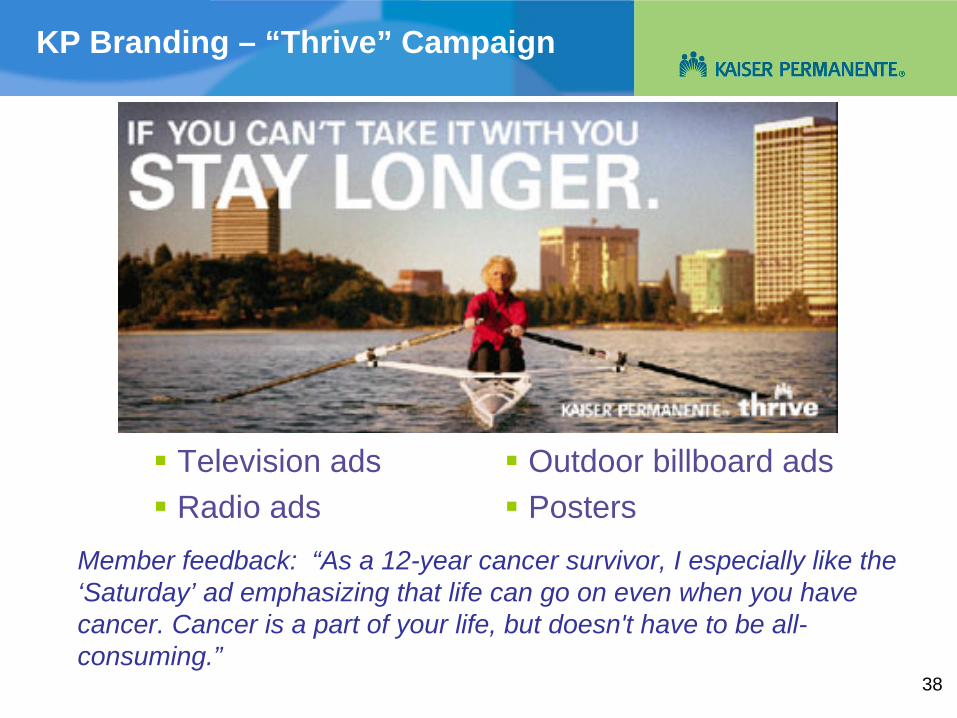
KP Branding – “Thrive” Campaign
Television ads
Radio ads
Member feedback: “As a 12-year cancer survivor, I especially like the ‘Saturday’ ad emphasizing that life can go on even when you have cancer. Cancer is a part of your life, but doesn't have to be all- consuming.”
Outdoor billboard ads
Posters
39
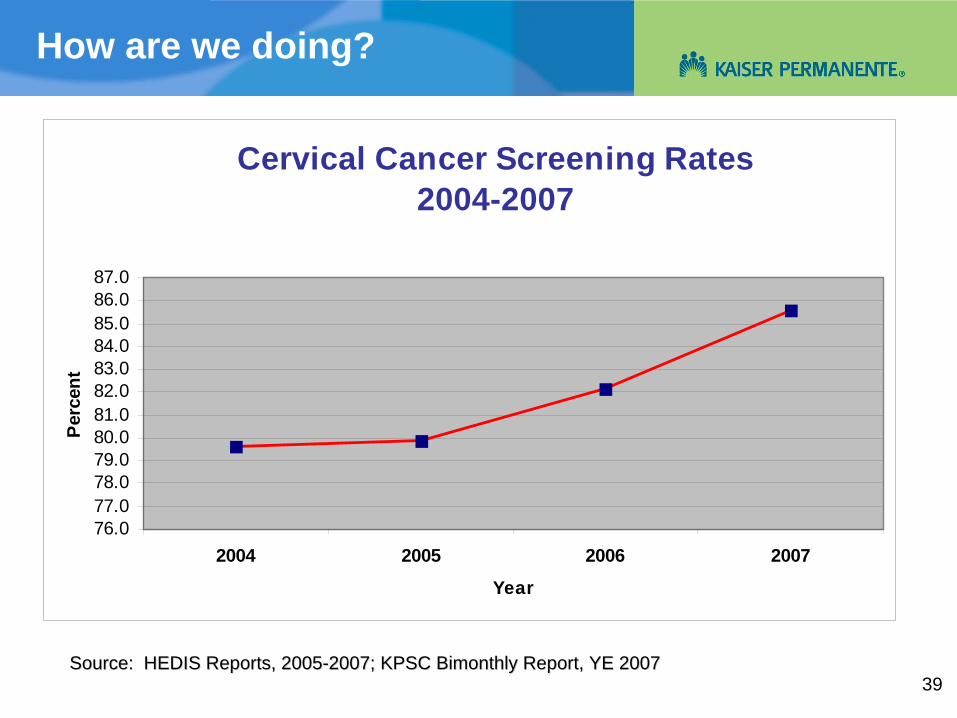
How are we doing?
Cervical Cancer Screening Rates2004-2007
76.077.078.079.080.081.082.083.084.085.086.087.0
2004 2005 2006 2007
Year
Perc
ent
Source: HEDIS Reports, 2005Source: HEDIS Reports, 2005--2007; KPSC Bimonthly Report, YE 20072007; KPSC Bimonthly Report, YE 2007
40
Lessons Learned
Importance of developing an evidence-based culture
Strong support of senior leadership to fund and maintain an infrastructure for evidence-based research and content development
Readiness to change
Evidence-based content development
Involve important stakeholders in all phases (topic selection, evidence review, development of guidance and knowledge exchange)
Manage the scope of the content
Focus on key levers in process of health care, not entire care path
Develop clear summaries with recommendations – concise, plain language
Keep written materials as short as possible, tailor to audience
Larger evidence documents will not be used by clinicians, operations staff or administrators

41
Lessons Learned (cont.)*
Impact of electronic health systems on evidence packaging:
Pieces of content that do one thing quickly and well
All-encompassing content not generally well accepted
Actively promoted
Leadership mandates, Resource Stewardship
Modal alerts (can’t avoid seeing it)
Granular content• Very specific recommendations• Codable elements• Operational definitions of disease, drugs, labs• Guidance must be correct and actionable
Define pivot points• Prioritize among the recommendations• Prioritize between guidelines (comorbidities)
*With thanks to Dr. Wiley Chan, KP Northwest
42
Lessons Learned (cont.)
Create measures that drive desired performance
Consider Operational Environment• Alert fatigue• Regional priorities• Regional leadership & culture• Local workflows
Guideline writers should help build content• KP National content was little used in NW• Requires knowledge of local operational environment
*With thanks to Dr. Wiley Chan, KP Northwest


















