
Oxford Colorectal Restorative Proctocolectomy The Failing Pouch Neil Mortensen MD FRCS Department of...
44
Oxford Colorecta Restorative Proctocolectomy The Failing Pouch The Failing Pouch Neil Mortensen MD FRCS Neil Mortensen MD FRCS Department of Colorectal Department of Colorectal Surgery Radcliffe Hospital, Surgery Radcliffe Hospital, Oxford Oxford M62 Course 2006
-
Upload
juliana-carson -
Category
Documents
-
view
222 -
download
3
Transcript of Oxford Colorectal Restorative Proctocolectomy The Failing Pouch Neil Mortensen MD FRCS Department of...
Oxford
Colorectal
Restorative Proctocolectomy
The Failing PouchThe Failing Pouch
Neil Mortensen MD FRCS Neil Mortensen MD FRCS Department of Colorectal Surgery Department of Colorectal Surgery
Radcliffe Hospital, OxfordRadcliffe Hospital, Oxford
M62 Course 2006
Oxford
Colorectal
Restorative Proctocolectomy
Parks and Nicholls
Proctocolectomy without ileostomy for ulcerative colitis
BMJ 1978;2:65-8

Oxford
Colorectal
Restorative Proctocolectomy
Pouches around the World 2000Pouches around the World 2000
USA 7600
UK 2500
Sweden 2500
Canada 1500
Germany 1100
France 250
Australia 200
Estimated Total 15650
Oxford
Colorectal
Restorative Proctocolectomy
Pouch surgery – the ecstasy

Oxford
Colorectal
Restorative Proctocolectomy
Pouch surgery – the agony
Oxford
Colorectal
Restorative Proctocolectomy
Pouch Failure
Oxford
Colorectal
Restorative Proctocolectomy
Bleeding
Infarction
Peritonitis
Anastomotic leak
Pouch cutaneous fistula
Pouch vaginal fistula
Stricture
Small bowel stricture
Pouch complications
Oxford
Colorectal
Restorative Proctocolectomy
Oxford Pouch ExcisionOxford Pouch Excision
408 IPAA
30 Pouch excisions, 7 immediate
27 (6.6%) in house
3 elsewhere
Oxford
Colorectal
Restorative Proctocolectomy
Oxford Pouch ExcisionOxford Pouch Excision
Reasons for excision
8 pouchitis
6 ischaemia
6 sepsis
5 Crohns
3 incontinence
1 bleeding
1 desmoid
Oxford
Colorectal
Restorative Proctocolectomy
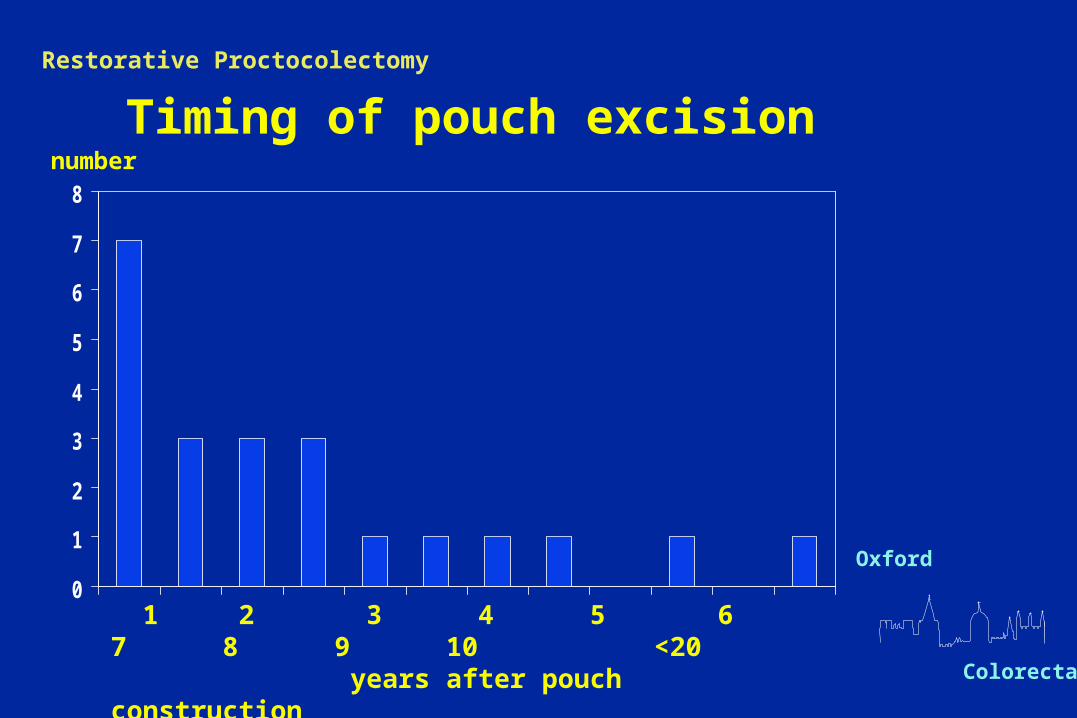
Timing of pouch excision
0
1
2
3
4
5
6
7
8
1 2 3 4 5 6 7 8 9 10 <20 years after pouch construction
number
Oxford
Colorectal
Restorative Proctocolectomy
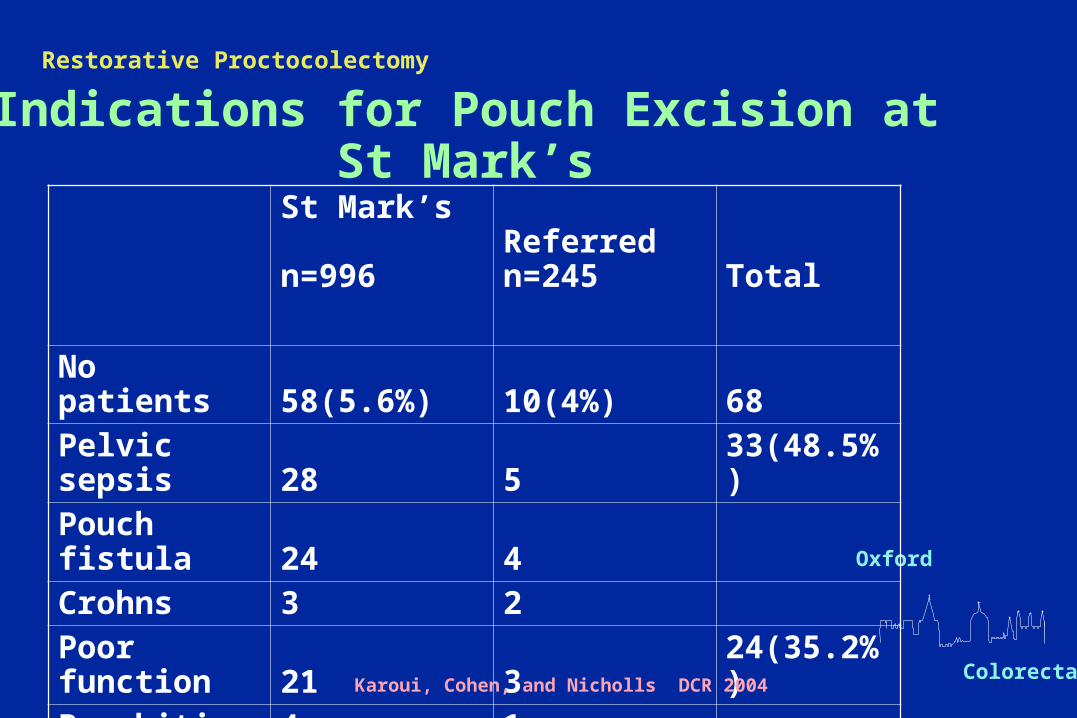
Indications for Pouch Excision at St Mark’s
St Mark’s n=996
Referred n=245 Total
No patients 58(5.6%) 10(4%) 68Pelvic sepsis 28 5 33(48.5%)
Pouch fistula 24 4
Crohns 3 2Poor function 21 3 24(35.2%)
Pouchitis 4 1
other 5 1Karoui, Cohen, and Nicholls DCR 2004
Oxford
Colorectal
Restorative Proctocolectomy
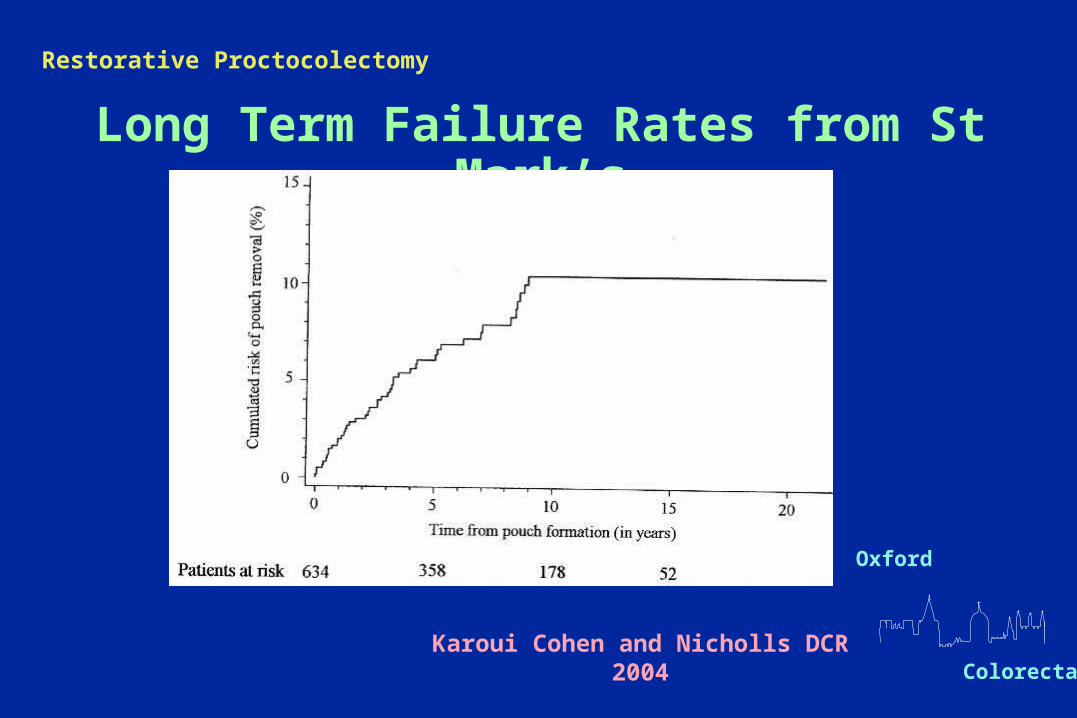
Long Term Failure Rates from St Mark’s
Karoui Cohen and Nicholls DCR 2004
Oxford
Colorectal
Restorative Proctocolectomy
Please don’t let it
leak
Oxford
Colorectal
Restorative Proctocolectomy
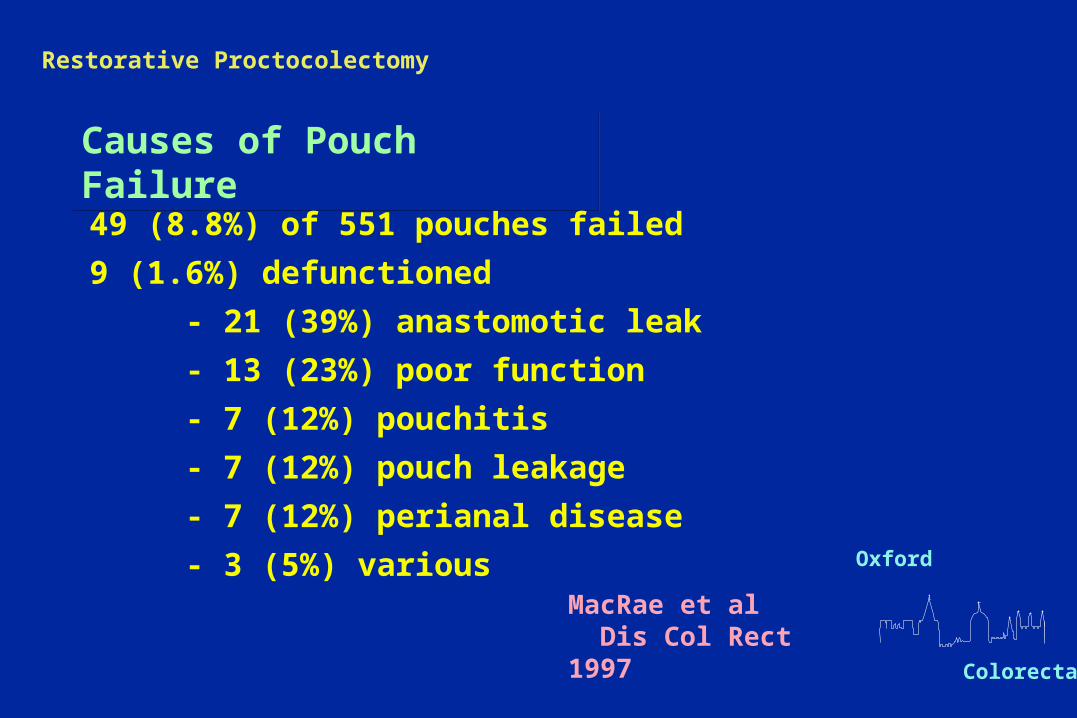
Causes of Pouch FailureCauses of Pouch Failure
49 (8.8%) of 551 pouches failed
9 (1.6%) defunctioned
- 21 (39%) anastomotic leak
- 13 (23%) poor function
- 7 (12%) pouchitis
- 7 (12%) pouch leakage
- 7 (12%) perianal disease
- 3 (5%) variousMacRae et al Dis Col Rect 1997
Oxford
Colorectal
Restorative Proctocolectomy
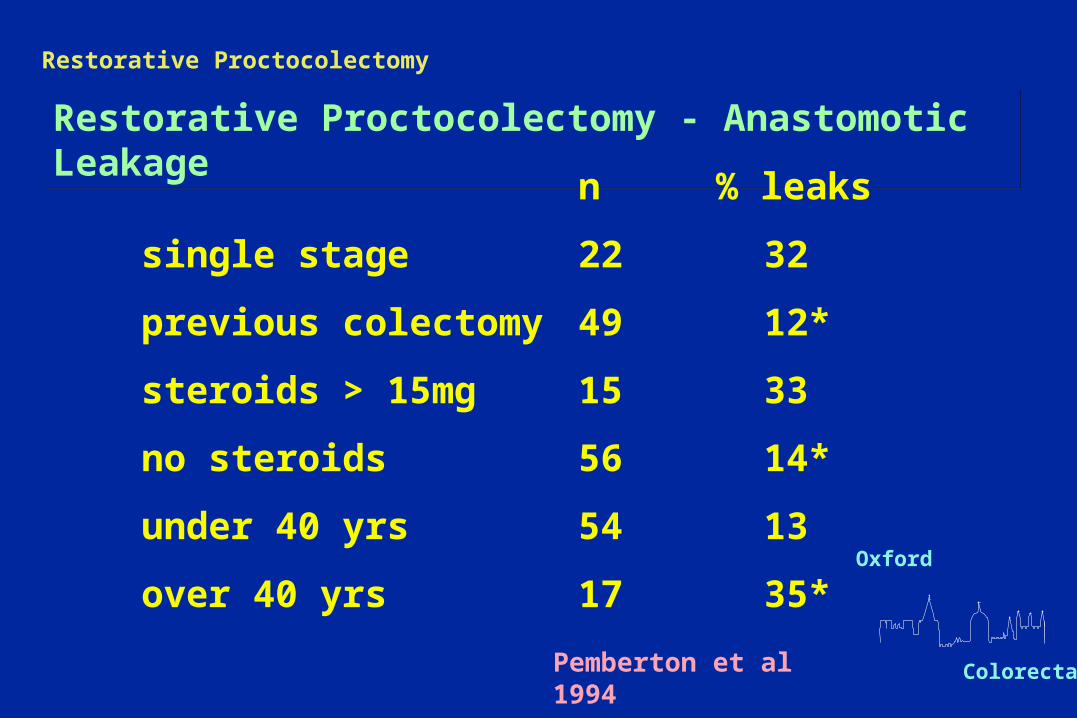
Restorative Proctocolectomy - Anastomotic LeakageRestorative Proctocolectomy - Anastomotic Leakage
n % leaks
single stage 22 32
previous colectomy 49 12*
steroids > 15mg 15 33
no steroids 56 14*
under 40 yrs 54 13
over 40 yrs 17 35*
Pemberton et al 1994
Oxford
Colorectal
Restorative Proctocolectomy
Patient Selection : Patient Selection : SteroidsPatient Selection : Patient Selection : Steroids
• 671 patients
• 20 mg Prednisolone threshold
• no differences in septic complications
• IPAA without diversion, 50% complication on high dose steriods
Ziv et al Dis Col Rect 1996
Oxford
Colorectal
Restorative Proctocolectomy
Incidence and Impact Pelvic Abscess after IPAAIncidence and Impact Pelvic Abscess after IPAA
73 of 1508 pelvic abscess
• pouch failure 26%
• 55% need transabdominal salvage
• 8% local surgery
• 37% non surgical
• functional outcome poorer
Farouk et al Dis Col Rect 1998
Oxford
Colorectal
Restorative Proctocolectomy
Patient Selection - indeterminate colitisPatient Selection - indeterminate colitis
• 71 indeterminate v. 1232 UC
• no difference in frequency, continence or pouchitis
• failure rate 19% v. 8%
McIntyre et al Dis Col Rect 1995

Oxford
Colorectal
Restorative Proctocolectomy
Long Term Results of IPAA in Patients with Crohn’s DiseaseLong Term Results of IPAA in Patients with Crohn’s Disease
37 patients
Original diagnosis UC (22), indeterminate (9), Crohn’s (6),
Complex fistulas in 11
Site of Crohn’s pouch (20), anal (4), both (10)
Failure in 17 Sagar et al Dis Col Rect 1996
Oxford
Colorectal
Restorative Proctocolectomy
Pouch Failure & Crohn’s - Cleveland ClinicPouch Failure & Crohn’s - Cleveland Clinic
Overall failure 3.4%, 1.1% non function
Of 34 failures - 17 had Crohn’s
25% Crohn’s fail
Fazio et al Ann Surg 1995

Oxford
Colorectal
Restorative Proctocolectomy
Treating the early abscess or anastomotic dehiscence
• EUA assessment
• Abscess – drain mushroom catheter, CT drain
• Dehiscence – drain, early resuture or advancement
• Wait, pouchogram, consider re operation
Oxford
Colorectal
Restorative Proctocolectomy
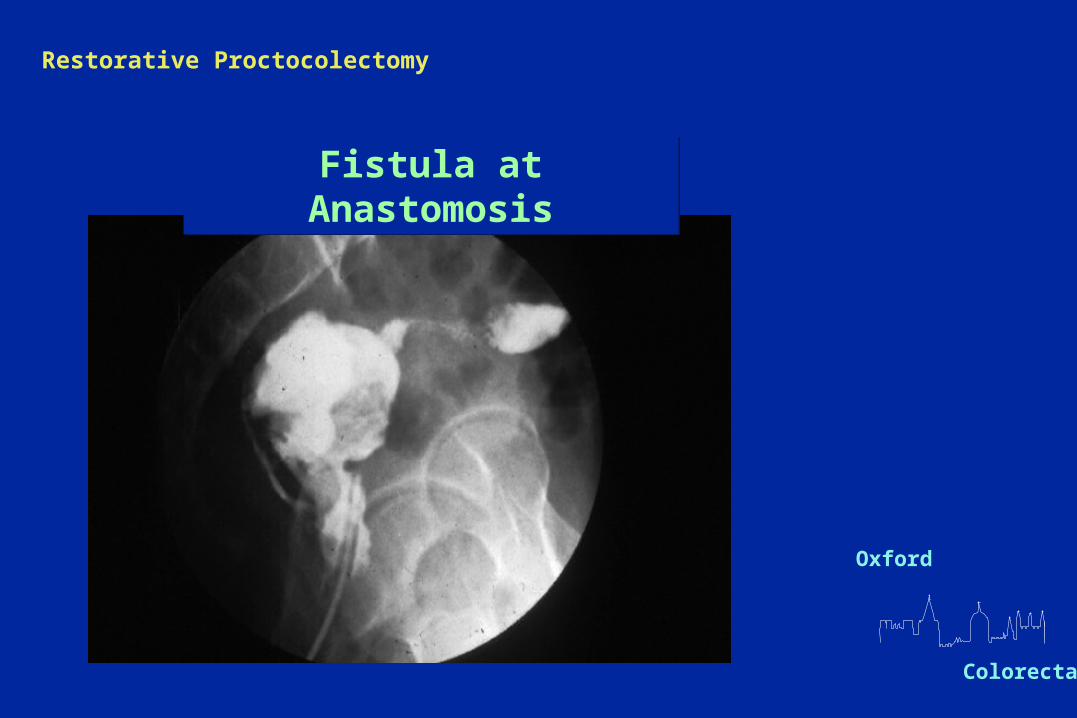
Fistula at AnastomosisFistula at Anastomosis
Oxford
Colorectal
Restorative Proctocolectomy
Pouch related fistulaPouch related fistula
59 of 1040 IPAA
• 24 pouch vaginal
• 11 pouch cutaneous
• 16 pouch perineal
• 8 pouch presacral
32% eventually excised
Ozuner et al Dis Col Rect 1997
Oxford
Colorectal
Restorative Proctocolectomy
Pouch Related Fistula after Restorative ProctocolectomyPouch Related Fistula after Restorative Proctocolectomy
21 patients, in 6 > 5 m after ileostomy closure
Site : anastomosis 14
vertical staple line 2
efferent limb end 5
Adverse factors : late fisutula
enterocutaneous
pouch vaginal
suspect Crohn’s
Paye et al 1996 BJS

Oxford
Colorectal
Restorative Proctocolectomy
Try Local Repair First if:Try Local Repair First if:
• gross sepsis absent
• granulation tissue minimal
• fistulas close to anal verge
• strictures are short
Oxford
Colorectal
Restorative Proctocolectomy
Repeat IPAA - indicationsRepeat IPAA - indications
• mechanical outlet obstruction
• lack of reservoir capacity
• sepsis
Oxford
Colorectal
Restorative Proctocolectomy
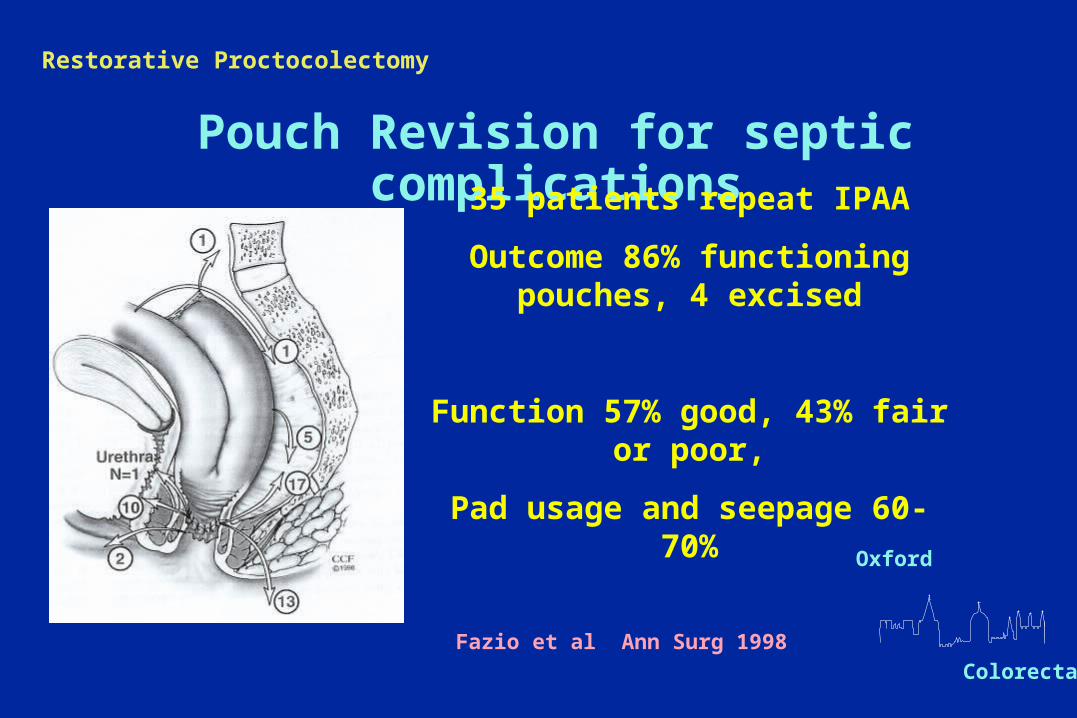
Pouch Revision for septic complications35 patients repeat IPAA
Outcome 86% functioning pouches, 4 excised
Function 57% good, 43% fair or poor,
Pad usage and seepage 60-70%
Fazio et al Ann Surg 1998
Oxford
Colorectal
Restorative Proctocolectomy
Pouch Revision by Disconnection - ReconnectionPouch Revision by Disconnection - Reconnection
23 patients 9 long efferent
4 sepsis fistula
3 redundant blind limb
3 twisted pouch
3 anastomotic problem
Pouch Salvaged in 16
Good function 11
Pouch excision 6
Sagar et al 1996 BJS

Oxford
Colorectal
Restorative Proctocolectomy
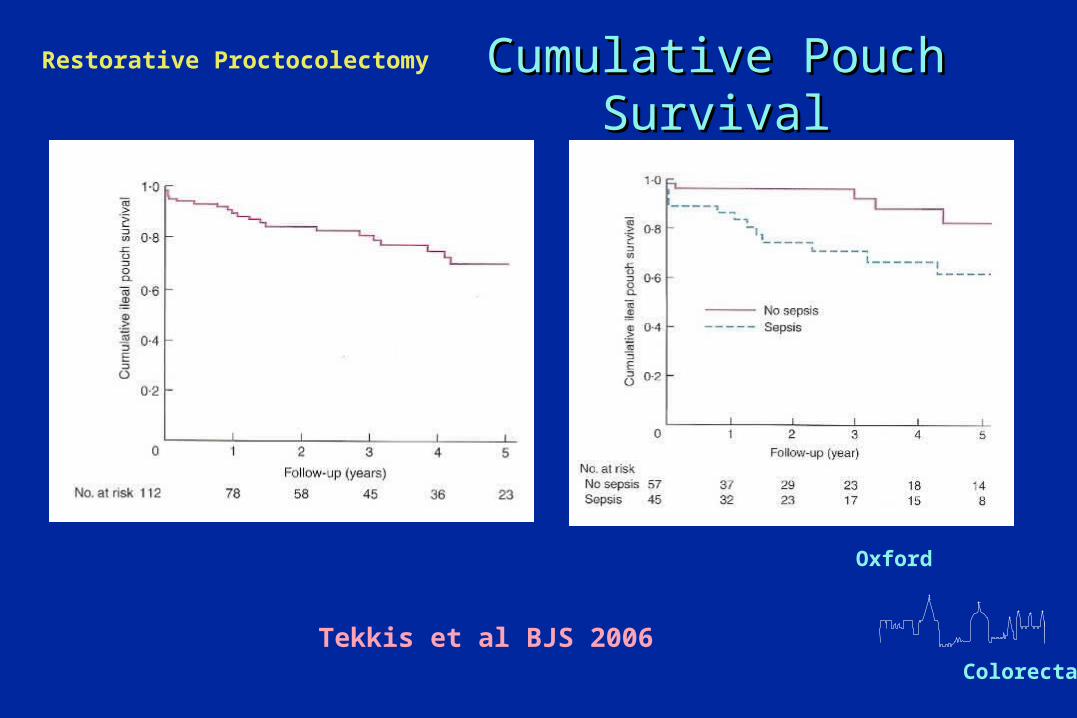
Long Term Results of Abdominal SalvageLong Term Results of Abdominal Salvage
• 112 underwent 117 pouch salvage procedures
• Common indications - sepsis 45, stricture 13, retained stump 35
• 21% pouch failure
• Associated with Crohn’s, sepsis
Tekkis et al BJS 2006
Oxford
Colorectal
Restorative Proctocolectomy Cumulative Pouch SurvivalCumulative Pouch Survival
Tekkis et al BJS 2006
Oxford
Colorectal
Restorative Proctocolectomy
Restorative Proctocolectomy - TechniqueRestorative Proctocolectomy - Technique
Get it right first timeGet it right first time
Oxford
Colorectal
Restorative Proctocolectomy
Oxford
Colorectal
Restorative Proctocolectomy
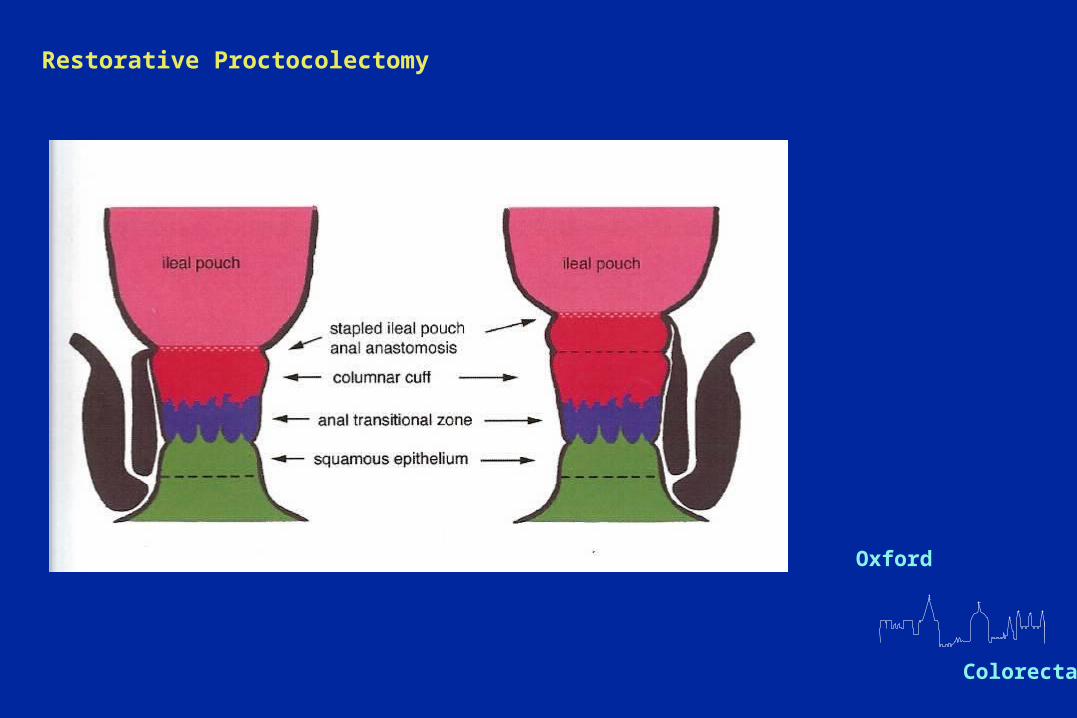
The risks of maintaining Columnar CuffThe risks of maintaining Columnar Cuff
- Some 6-10% of the total anorectal mucosa is retained
- risk of malignancy
- risk of inflammation

Oxford
Colorectal
Restorative Proctocolectomy
Cuffitis - symptomsCuffitis - symptoms
• urgency
• frequency
• leakage
• bleeding
• anal irritation or burning discomfort
Oxford
Colorectal
Restorative Proctocolectomy
Cuffitis and Inflammatory ChangesCuffitis and Inflammatory Changes
113 patients, 715 biopsies
• acute inflammation in columnar cuff in 13%
• in 9% symptomatic with endoscopic inflammation
• no relationship with pouchitis, pouch frequency or anastomotic height
Thompson-Fawcett, Warren, Mortensen Dis Col Rect 1999
Oxford
Colorectal
Restorative Proctocolectomy
Cuffitis - TreatmentCuffitis - Treatment
• medical - largely empirical
- steroids, per anal or oral
- 5ASA compounds, per anal or oral
- lignocaine jelly, per anal
• surgery - mucosectomy Curran & Hill 1992
- mucosectomy & pouch advancement
Fazio & Tjandra 1994

Oxford
Colorectal
Restorative Proctocolectomy
Pouch Vaginal FistulaPouch Vaginal Fistula
• avoid catching vagina with stapler
• repair by endo vaginal advancement flap
• defunction ?
Oxford
Colorectal
Restorative Proctocolectomy
Oxford
Colorectal
Restorative Proctocolectomy
Small Bowel ProblemsSmall Bowel Problems
Adhesions 15-30% symptomatic
5-10% need re-operation
Functional obstruction - ileal brake
Small bowel bacterial overgrowth
Crohn’s disease (5-7%)
Oxford
Colorectal
Restorative Proctocolectomy
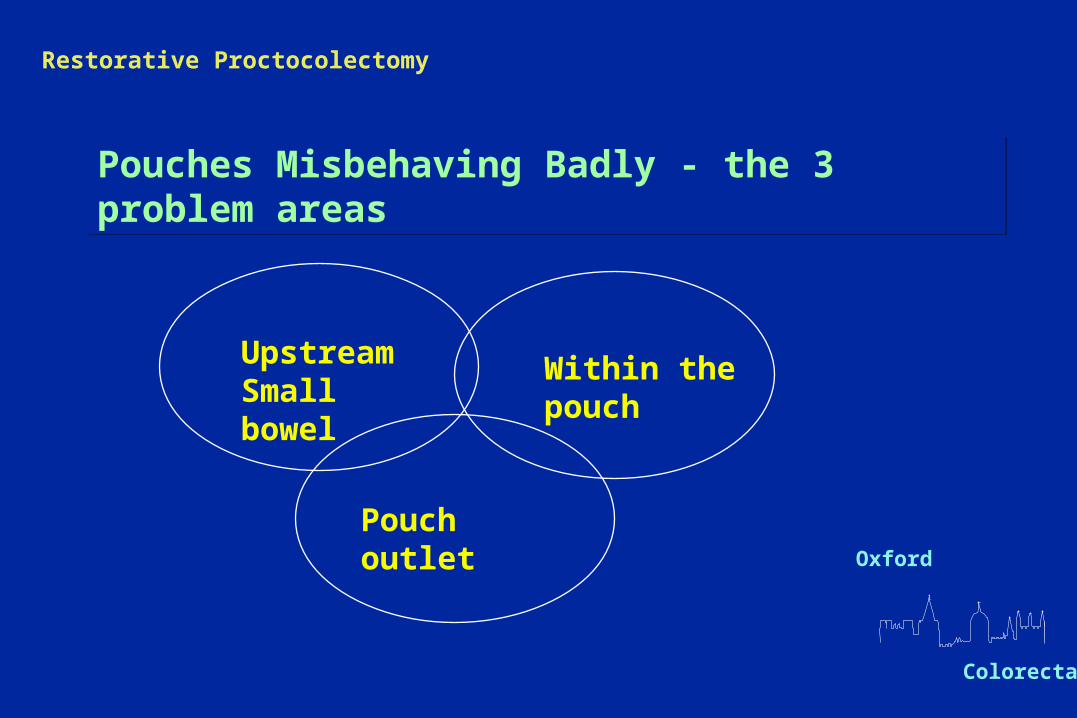
Pouches Misbehaving Badly - the 3 problem areasPouches Misbehaving Badly - the 3 problem areas
Upstream Small bowel
Within the pouch
Pouch outlet
Oxford
Colorectal
Restorative Proctocolectomy
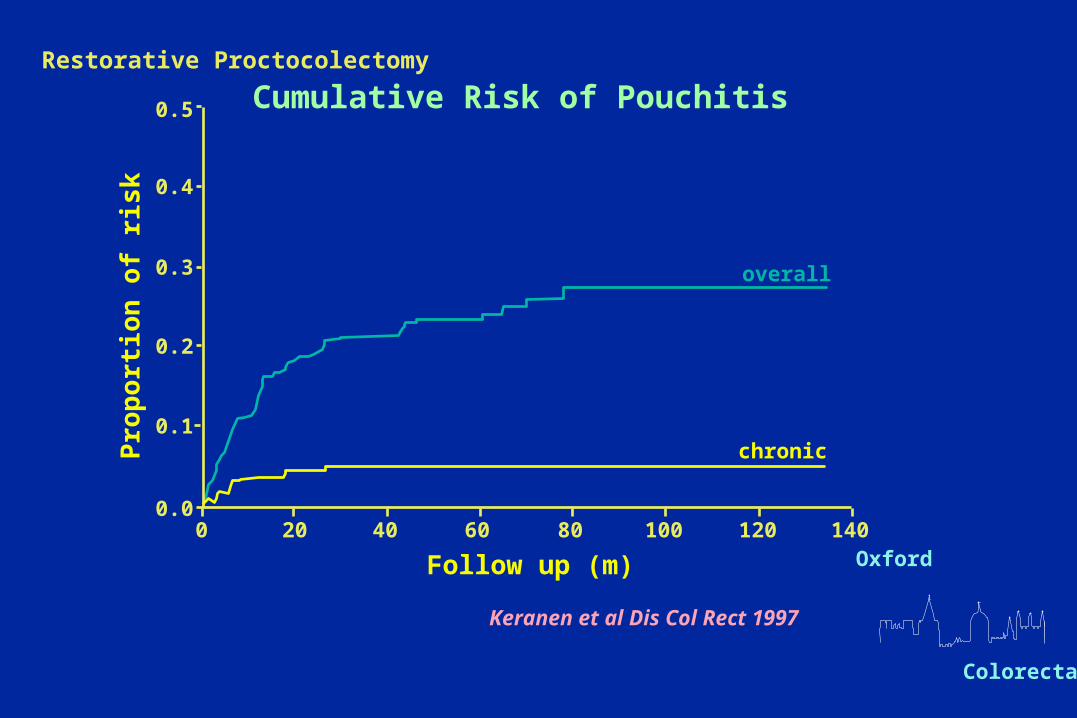
0.5
0.4
0.3
0.2
0.1
0.00 20 40 60 80 100 120 140
overall
chronic
Follow up (m)
Pro
po
rtio
n o
f ri
sk
Keranen et al Dis Col Rect 1997
Cumulative Risk of Pouchitis
Oxford
Colorectal
Restorative Proctocolectomy
Refractory PouchitisRefractory Pouchitis
• Review the previous histology
• Is there a pelvic abscess?
• Is there partial obstruction to ileum?
• Is there a small bowel motility disturbance
• Is there dietary intolerance?
Oxford
Colorectal
Restorative Proctocolectomy
SummarySummary
10% lose pouch
10% have poor function but prefer to keep their pouch
80% report an excellent quality of life
Oxford
Colorectal
Restorative Proctocolectomy
But….. Some worries
Increasing numbers of patients needing chronic
ciproxin dosingPerianal disease
being treated with infliximab


















