Overview The Liver and Biliary System - VCU SOM · 1 1 The Liver and Biliary System 10 cases to...
10
1 1 The Liver and Biliary System 10 cases to guide you Chapy Venkatesan, MD Department of Medicine VCU School of Medicine Inova Campus 2 Overview To be familiar with the approach to differential diagnosis and management hepatobiliary disease – will not be all-encompassing Case and image based Interactive Hope for you to get three learning points out of this Will review what we covered at the end – motivate/challenge you to read on your own Show you that medicine is FUN! 3 Background/Patterns Hepatocellular - ALT, AST > 3x uln; AP < 2x uln Cholestatic/Obstructive - AP > 3x uln; AST, ALT < 2x uln Mixed - ALT and AP > 2-3x uln Bili variable in all Alcohol - AST>ALT in 2-3:1, AST < 300, ALT < 100 – ratios outside of these ranges in someone who drinks EtOH suggests a concomitant disorder 4 Liver Function PT/INR Albumin Glucose 5 Case #1 42 year old male with recent onset jaundice Vague epigastric/RUQ discomfort No IVDU, transfusions, unprotected sex Recently taking acetaminophen 3g/day for a viral URI BP - normal Alert and oriented, jaundiced INR - 4.2; Cr - 3.0; AST - 14,380; ALT - 6,740; Alk Phos - 70; tb - 11.2 6 www.merck.com/.../ mmanual/plates/125pla5.jsp
Transcript of Overview The Liver and Biliary System - VCU SOM · 1 1 The Liver and Biliary System 10 cases to...

1
1
The Liver and Biliary System 10 cases to guide you
Chapy Venkatesan, MDDepartment of MedicineVCU School of Medicine Inova Campus
2
OverviewTo be familiar with the approach to differential diagnosis and management hepatobiliary disease– will not be all-encompassing
Case and image basedInteractiveHope for you to get three learning points out of thisWill review what we covered at the end– motivate/challenge you to read on your own
Show you that medicine is FUN!
3
Background/PatternsHepatocellular - ALT, AST > 3x uln; AP < 2x ulnCholestatic/Obstructive - AP > 3x uln; AST, ALT < 2x ulnMixed - ALT and AP > 2-3x ulnBili variable in allAlcohol - AST>ALT in 2-3:1, AST < 300, ALT < 100– ratios outside of these ranges in someone who
drinks EtOH suggests a concomitant disorder
4
Liver Function
PT/INRAlbuminGlucose
5
Case #142 year old male with recent onset jaundiceVague epigastric/RUQ discomfortNo IVDU, transfusions, unprotected sexRecently taking acetaminophen 3g/day for a viral URIBP - normalAlert and oriented, jaundicedINR - 4.2; Cr - 3.0; AST - 14,380; ALT -6,740; Alk Phos - 70; tb - 11.2
6www.merck.com/.../ mmanual/plates/125pla5.jsp
2
7www.edu.rcsed.ac.uk/ photoalbum/ph93.htm
8
©2004 UpToDate®
9http://medicine.ucsd.edu/clinicalmed/Abdomen-Caput-Medusa.jpg 10
http://www.medicouncilalcol.demon.co.uk/handbook/images/palmar_erythema.jpg
11
QuestionsWhat is the most likely underlying risk factor for the patient’s acute liver disease?– alcoholic cirrhosis
What is the most likely diagnosis for the acute liver disease?– acetaminophen hepatotoxicity
What is the therapy/antidote?– N-acetylcysteine
What are other causes of transaminases in the 1,000’s– acute viral hepatitis (risk factors), ischemic
hepatitis/shock liver (hypotension, diminished cardiac output)
12
Induced by alcohol
No synthesis due to liver dz
TOXIC
Current Diagnosis & Treatment in Gastroenterology - 2nd Ed. (2003)
N-acetylcysteineis a substitute

3
13
Rumack BH, Matthew H: Acetaminophen poisoning and toxicity. Pediatrics 1975;55:871
14Lee 333 (17): 1118, Table 2 October 26, 1995 - NEJM
15
Case #224 y.o. female prostitute, IV drug user presents with headache, malaise, fever, arthralgias, and nausea followed by jaundice Hepatomegaly and jaundice on examAST - 850, ALT - 1,250; bili - 4.0; AP -normalAnti-HAV IgM, Anti-HCV, HBsAg, HBsAb all negative
16
QuestionsWhat is the best serologic test to make the diagnosis?– HBcAb IgM
What is the pattern of vaccination versus hepatitis B; remote hepatitis B?– + HBsAb, neg HBcAb; +HBsAb, +HBcAb
The patient’s liver enzymes fall and then peak 4 weeks later, what is the best way to make the diagnosis?– Anti HDV or HDV RNA
17
Questions
Twenty years later, the HBsAg is positive. There is no evidence of cirrhosis. The alkphos and AFP are elevated and the pt has fever and polycythemia. What is the most likely diagnosis?– hepatocellular carcinoma
What are other risk factors for hepatoma?
18
©2004 UpToDate®

4
19
Risk factors for hepatoma
Cirrhosis of any etiologyAlcoholHepatitis B (does not have to progress through cirrhosis)Hepatitis CHemochromatosis
20
Case #3
20 y.o. female with jaundice for one weekHad nausea and abdominal pain for three weeksFriends brought her in d/t hallucinationsYou note a tremor on examALT - 170, AST - 95; AP - 120; bili - 8.0Retic - 10.5%; LDH - 1000, Hct - 33, Coombs negative
21 22
QuestionsWhat are blood and urine tests that support this diagnosis?– Wilson’s disease - low ceruloplasmin, high
24 hr urine copperWhat is the medical therapy?– penicillamine– may need liver transplant - especially if
presenting with fulminant hepatic failure (acute liver failure with hepatic encephalopathy)
23
Case #452 y.o. white female (nondrinker, diabetic w/ A1C - 9.2%)with incidentally noted ALT - 75, AST - 52, AP - 65, bili normalBMI - 36LDL - 245, TG - 380U/S demonstrates a hyperechoic liverhep B, C, iron studies, ceruloplasmin, alpha one antitrypsin level, anti-mitochondrial antibody, anti-smooth muscle antibodies negative
24
Questions
What is the best treatment?– pt has NASH / NAFLD– gradual weight loss and treatment of DM,
hyperlipid / triglyceridemiaWhat are other causes of chronically elevated liver enzymes?
5
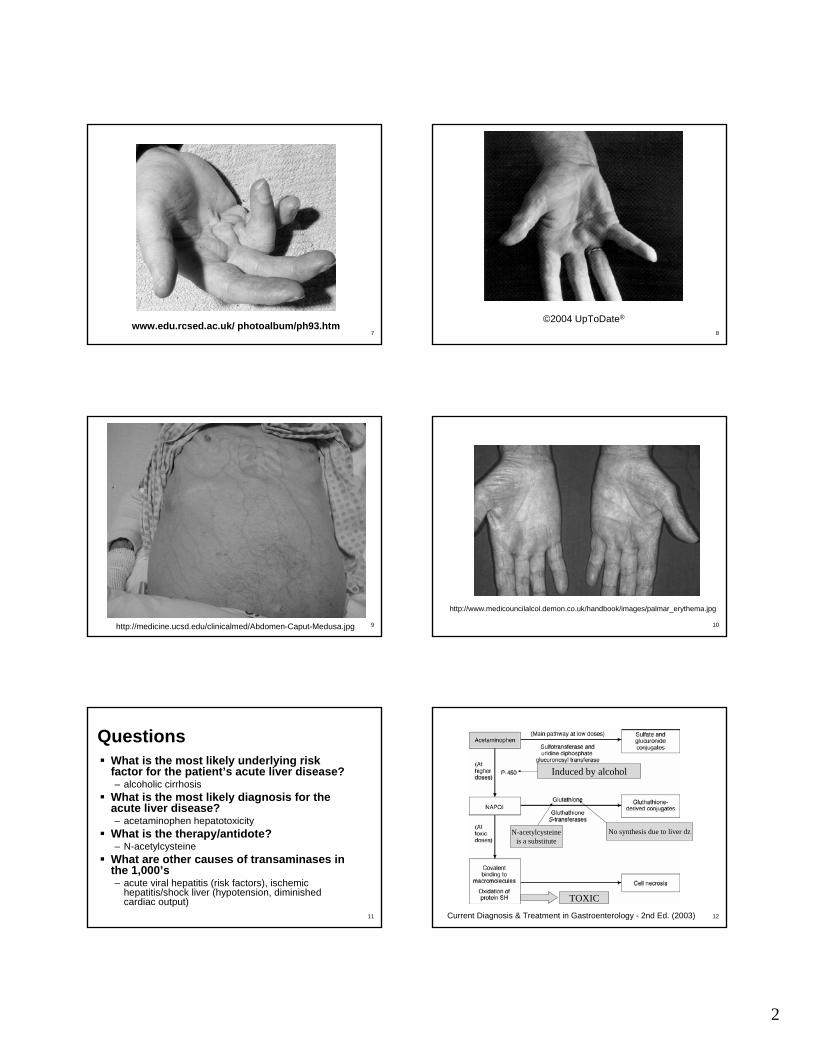
25
HistorySerology
Obesity, DM, hyperlipidemia;
exclusion of other causes
Polyclonal gammopathy,Anti Sm m Ab, Anti LKM Ab
Hypogonadism,Arthritis,DM, CHF
Fe studies, geneticstudies
KF rings; neuro,Psyc, Hepatic,
Heme; ceruloplasmin,urine Cu
Emphysema, FmHxliver dz, panniculitis,
level, genotype
Malabsorption, Fe def,osteoporosis, misdx with IBS
CK, aldolase,TSH
Causes of Chronically Elevated Aminotransferase Levels
26
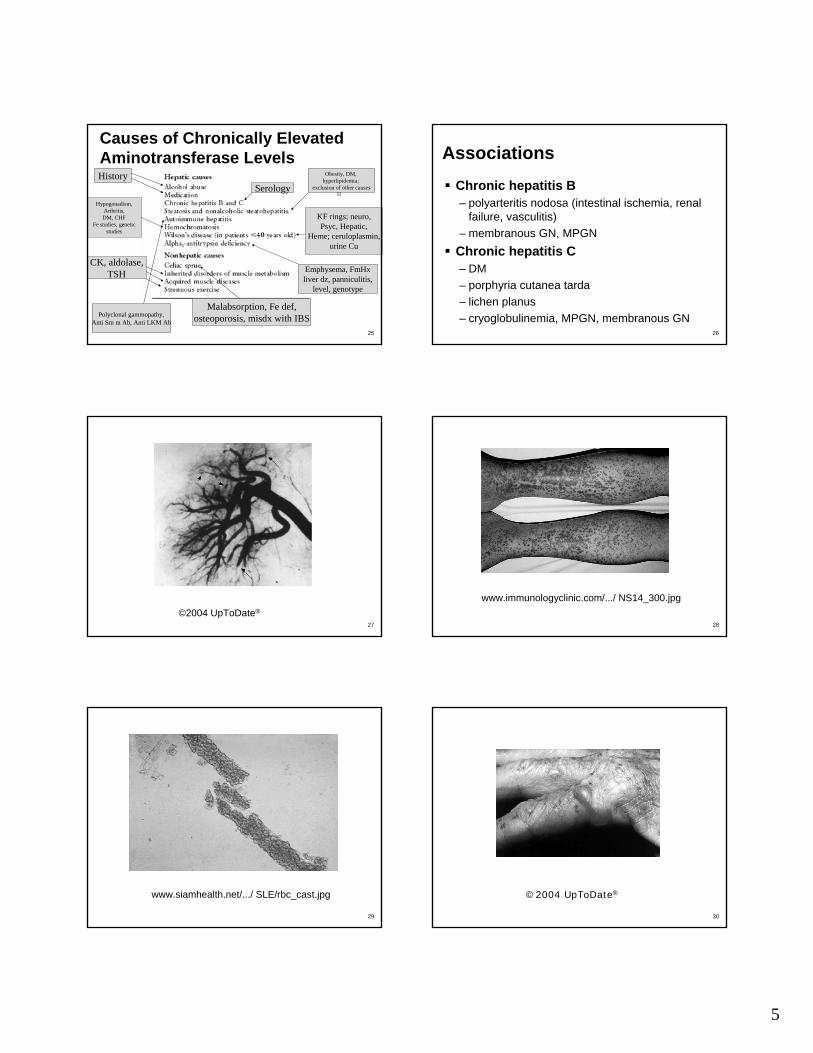
AssociationsChronic hepatitis B– polyarteritis nodosa (intestinal ischemia, renal
failure, vasculitis)– membranous GN, MPGN
Chronic hepatitis C– DM– porphyria cutanea tarda– lichen planus– cryoglobulinemia, MPGN, membranous GN
27
©2004 UpToDate®
28
www.immunologyclinic.com/.../ NS14_300.jpg
29
www.siamhealth.net/.../ SLE/rbc_cast.jpg
30
©2004 UpToDate®
6
31
©2004 UpToDate®
32
Case #5
43 y.o. female with fatigue and pruritis at all timesHad a recent pathologic fracture and Z score on DEXA was - 2.9ALT - 70, Alk Phos - 600
33
Questions
What is the most likely diagnosis?– primary biliary cirrhosis
What are sources of alk phos?– placenta, bile duct epithelium, and bone
• Paget’s disease of bone, bone metastases, primary hyperparathyroidism, Vitamin D deficiency
34
Case #6
25 y.o. male returned from a trip to India three months agoDevelops two weeks of fever and RUQ pain without diarrheaWBC 14K
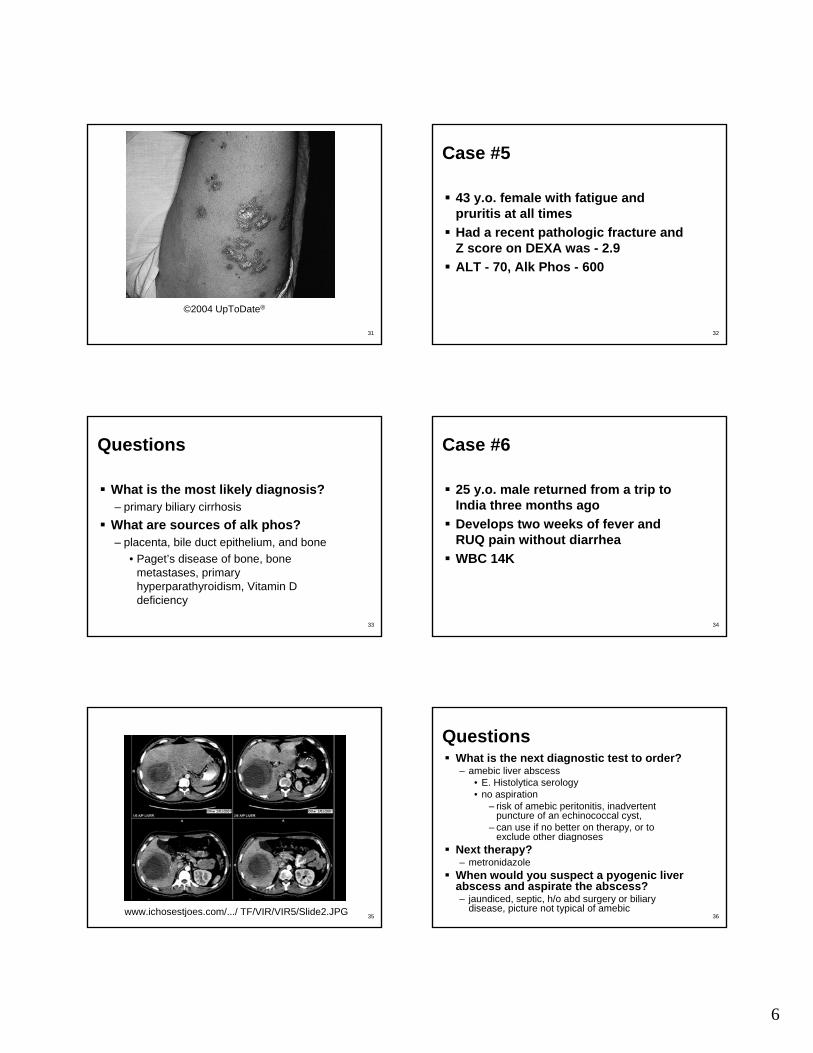
35www.ichosestjoes.com/.../ TF/VIR/VIR5/Slide2.JPG 36
QuestionsWhat is the next diagnostic test to order?– amebic liver abscess
• E. Histolytica serology• no aspiration
– risk of amebic peritonitis, inadvertent puncture of an echinococcal cyst,
– can use if no better on therapy, or to exclude other diagnoses
Next therapy?– metronidazole
When would you suspect a pyogenic liver abscess and aspirate the abscess?– jaundiced, septic, h/o abd surgery or biliary
disease, picture not typical of amebic

7
37
Case #763 y.o. female with acute onset of fever, chills, n/vT - 103 F, P - 120, RR - 28, BP - 80/50Pt is jaundiced with scleral icterus on examAST and ALT - 125, Alk Phos - 800, bili -12.5, dbili - 11.6U/S shows gallstones and CBD dilatationHypotension persists despite 4L of NS
38
QuestionsWhat is the next step in addition to supportive care and broad spectrum antibiotics?– ERCP for drainage and relief of the
obstruction– can do abx only with ERCP electively
unless:• no better over 1st 24 hours, fever > 103,
persistent pain, hypotension despite resuscitation
39
Case #8
22 y.o. with ulcerative colitis presents with jaundice, alk phos of 500, ALT of 75
40www.gastroenterologe.de/ _gfx/pscholangitis.jpg
41
Questions
What is the diagnosis?– Primary sclerosing cholangitis– most have UC, most of UC do not have
PSCWhat is the concern if the patient develops a dominant biliarystricture?– Cholangiocarcinoma
42

8
43
Case #9
45 y.o. male admitted with an acute MIFound to have a total bili of 6.0, dbili -0.3One year later, the bili decreases to 2.5, dbili - 0.3The remainder of the liver panel is normal, as is the CBC, retic count and peripheral smear
44
Questions
What is the next diagnostic test?– NONE
What is the therapy?– NONE
Gilbert’s syndromeIndirect hyperbilirubinemia– hemolysis, ineffective erythropoiesis
45
Case #10A
27 y.o. female, G1P0; at 38 weeksPresents with acute onset N/V, jaundice, encephalopathyAST and ALT ~ 700; Alk Phos - nl; NH3 - 95; Plt - 45K; PT/PTT -elevated; d-dimer - elevated; fibrinogen - low
46
Questions
What is the diagnosis?– acute fatty liver of pregnancy– can recur with subsequent pregnancies– stabilize the mother and deliver the fetus
47
Case #10B
26 y.o. female, G4P3, 34 wksRUQ pain, N/VBP - 145/90; 2+ edemaHct - 24; Plt - 75K; bili - 5.0 (dbili -0.5); ALT - 300; LDH - 1000; 4+ urine protein; Uric acid - 7.0
48
www.academic.marist.edu/. ../description31.jpg

9
49
Diagnosis?
HELLP Syndrome
50
Case #10C
28 y.o. G1P0 living in PakistanThe pt and her husband develop an illness characterized by jaundice, N/V, malaise, anorexiaHer husband’s illness is self-limitedShe develops encephalopathy, ALT -1200, and dies
51
Diagnosis?
Hepatitis E - increased mortality and FHF in pregnancy
52
Other pregnancy tidbits
Hyperemesis gravidarum causes elevations in the transaminases -usually below 300Benign Recurrent IntrahepaticCholestasis of Pregnancy -intractable pruritis, elevated alkphos, can recur with subsequent pregnancies
53
What did we cover?Patterns of liver panelPhysical findings of cirrhosisAcetaminophen hepatotoxicity and other forms of drug-induced liver diseaseCauses of AST and ALT > 1000Drug induced liver diseaseHepatitis B serologiesHepatocellular carcinoma RF’s
54
What did we cover?Wilson’s diseaseNASH/NAFLDChronically elevated aminotransferasesAssociations of hepatitis B and CPBCAmebic liver abscessCholangitis

10
55
What did we cover?
PSCCholangiocarcinomaGilbert’s syndromePregnancy and liver disease