Overview Síndromes Mielodisplásicos - aamds.org Spanish Higher Risk... · 9/15/2016 1 Rafael...
9
9/15/2016 1 Rafael Bejar MD, PhD Aplastic Anemia & MDS International Foundation Regional Patient and Family Conference September 17 th , 2016 Síndromes Mielodisplásicos: SMD de alto riesgo y los avances en el tratamiento Overview • Pronóstico y refinación de "alto" riesgo • Nuevos tratamientos • Avances en el trasplante de células madre • Ejemplos del laboratorio Refinación del Pronóstico Low Blood Counts Hombre de 71 años de edad con glóbulos rojos grandes y recuentos bajos de sangre que se desarrollaron durante los últimos 6 meses. Rango Normal 1.9 7.9 45 Low Blood Counts Way too many cells in the bone marrow 4% blasts in aspirate Dysplasia in all three cell types Normal Karyotype (chromosomes ok) Rango Normal 1.9 7.9 45 Hombre de 71 años de edad con glóbulos rojos grandes y recuentos bajos de sangre que se desarrollaron durante los últimos 6 meses. Greenberg et al. Blood. 1997;89:2079-88; Greenberg et al. Blood. 2012:120:2454-65. International Prognostic Scoring System
Transcript of Overview Síndromes Mielodisplásicos - aamds.org Spanish Higher Risk... · 9/15/2016 1 Rafael...

9/15/2016
1
Rafael Bejar MD, PhD
Aplastic Anemia & MDS International Foundation
Regional Patient and Family Conference
September 17th, 2016
Síndromes Mielodisplásicos: SMD de alto riesgo y los avances en el
tratamiento
Overview
• Pronóstico y refinación de "alto" riesgo
• Nuevos tratamientos
• Avances en el trasplante de células madre
• Ejemplos del laboratorio
Refinación del Pronóstico
Low Blood CountsHombre de 71 años de edad con glóbulos rojos grandes y recuentos bajos de sangre que se desarrollaron durante los últimos 6 meses.
RangoNormal
1.9 7.9
45
Low Blood Counts
Way too many cells in the bone marrow4% blasts in aspirate
Dysplasia in all three cell types
Normal Karyotype (chromosomes ok)
RangoNormal
1.9 7.945
Hombre de 71 años de edad con glóbulos rojos grandes y recuentosbajos de sangre que se desarrollaron durante los últimos 6 meses.
Greenberg et al. Blood. 1997;89:2079-88; Greenberg et al. Blood. 2012:120:2454-65.
International Prognostic Scoring System
9/15/2016
2
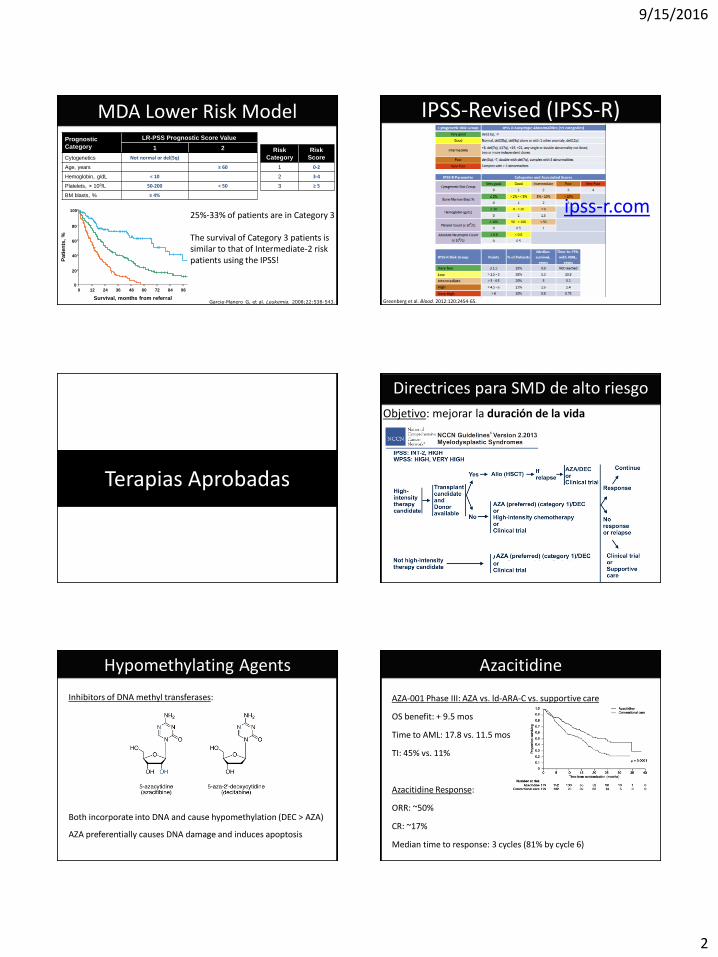
MDA Lower Risk ModelPrognostic
Category
LR-PSS Prognostic Score Value
1 2
Cytogenetics Not normal or del(5q)
Age, years ≥ 60
Hemoglobin, g/dL < 10
Platelets, × 109/L 50-200 < 50
BM blasts, % ≥ 4%
Garcia-Manero G, et al. Leukemia. 2008;22:538-543.
Risk
Category
Risk
Score
1 0-2
2 3-4
3 ≥ 5
Survival, months from referral
Pa
tie
nts
, %
0 2412 4836 60 8472 960
20
40
60
80
100
25%-33% of patients are in Category 3
The survival of Category 3 patients is similar to that of Intermediate-2 riskpatients using the IPSS!
IPSS-Revised (IPSS-R)
Greenberg et al. Blood. 2012:120:2454-65.
ipss-r.com
Terapias Aprobadas
Directrices para SMD de alto riesgo
Objetivo: mejorar la duración de la vida
Inhibitors of DNA methyl transferases:
Both incorporate into DNA and cause hypomethylation (DEC > AZA)
AZA preferentially causes DNA damage and induces apoptosis
Hypomethylating Agents
AZA-001 Phase III: AZA vs. ld-ARA-C vs. supportive care
OS benefit: + 9.5 mos
Time to AML: 17.8 vs. 11.5 mos
TI: 45% vs. 11%
Azacitidine Response:
ORR: ~50%
CR: ~17%
Median time to response: 3 cycles (81% by cycle 6)
Azacitidine

9/15/2016
3
Decitabine Phase III Trial ADOPT Trial and 3-Schedule Trial
Dosed q8h x 3 days per 28 days Dosed q24h x 5 days per 28 days
CR: 17% CR: 17%
CR+PR: 30% CR+PR: 32%
ORR: 52% (+ heme response)
Best response: 50% at 2 cycles
Major Toxicity:Neutropenia: 31% (FN 11%)
Thrombocytopenia: 18%
Decitabine Guidelines for Higher Risk MDS
Special Considerations:
Refer for Transplant Early- Even patients in their 70’s can benefit from RIC transplant
AZA > DEC (for now)- AZA has been shown to have a survival advantage, DEC has not (yet)
Don’t forget Quality of Life- Consider treatment palliative and weigh against patient needs
Look for Clinical Trials- Few option after AZA are available and none are approved
Objetivo: mejorar la duración de la vida
Outcomes After Azacitidine
Comparison to decitabine failures @ MDACC: median survival 4.3 months, n=87
Prébet T et al, J Clin Oncol 2011; Aug 20;29(24):3322-7. Epub 2011 Jul 25.Jabbour E et al, Cancer 2010; 116:3830–3834.
9% didn’t tolerate AZA (69% were not responding, 31% had an initial response)
55% primary failure (progression in 60% , stable disease without response in 40%)
36% secondary failure after initial response (best response: CR 20% , PR 7%, HI 73%)
Reasons for “failure” in azacitidine failure study
Outcomes after failure
Median overall survival for whole cohort post-AZA: 5.6 months
2 year survival: 15%
Favorable factors: female, younger (<60), better risk karyotype, <10% blasts, some response to azacitidine
Slide borrowed from Dr. David Steensma
• Data available on 435 pts – from AZA001, J9950, J0443, French compassionate program
• Overall median survival after azacitidine failure: 5.6 months
Prébet T et al J Clin Oncol 2011; 29:3322-7Jabbour E et al Cancer 2010;116(16):3830-4
Subsequent therapy Number of patients (%) Median survival
Allogeneic transplant 37 (9%) 19.5 months
Investigational therapy (e.g. IMiD, HDACi, other)
44 (10%) 13.2 months
Intensive cytotoxic therapy (e.g., 3&7)
35 (8%) 8.9 months
Low-dose chemotherapy (e.g. LDAC, 6-MP)
32 (7%) 7.3 months
Palliative / supportive care 122 (28%) 4.1 months
Subsequent therapy unknown 165 (38%) 3.6 months
Slide borrowed from Dr. David Steensma
Outcomes After Azacitidine
Tratamiento del SMD de alto Riesgo
Necesitamos terapias MEJORES!
Necesitamos MÁS terapias!Mejores Formulaciones
9/15/2016
4
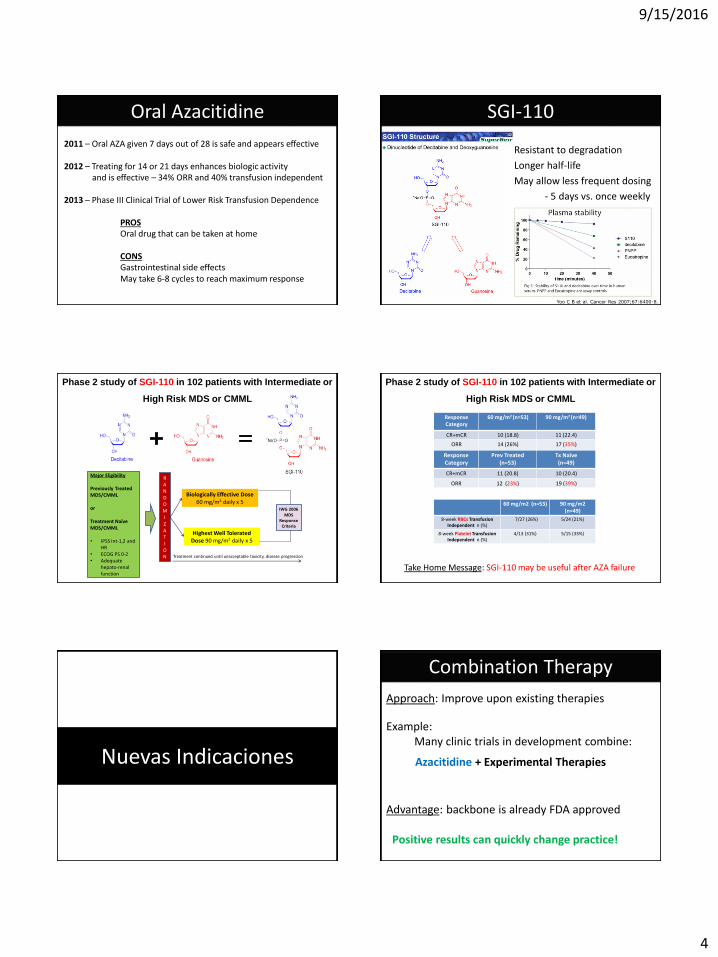
Oral Azacitidine
2011 – Oral AZA given 7 days out of 28 is safe and appears effective
2012 – Treating for 14 or 21 days enhances biologic activityand is effective – 34% ORR and 40% transfusion independent
2013 – Phase III Clinical Trial of Lower Risk Transfusion Dependence
PROSOral drug that can be taken at home
CONSGastrointestinal side effectsMay take 6-8 cycles to reach maximum response
SGI-110
Resistant to degradation
Longer half-life
May allow less frequent dosing
- 5 days vs. once weekly
Yoo C B et al. Cancer Res 2007;67:6400-8.
Phase 2 study of SGI-110 in 102 patients with Intermediate or
High Risk MDS or CMML
Biologically Effective Dose 60 mg/m2 daily x 5
Highest Well Tolerated Dose 90 mg/m2 daily x 5
RANDOMI Z A T I ON
IWG 2006 MDS
Response Criteria
Treatment continued until unacceptable toxicity, disease progression
Major Eligibility
Previously Treated MDS/CMML
or
Treatment Naïve MDS/CMML
• IPSS Int-1,2 and HR
• ECOG PS 0-2 • Adequate
hepato-renal function
Phase 2 study of SGI-110 in 102 patients with Intermediate or
High Risk MDS or CMML
ResponseCategory
60 mg/m2 (n=53) 90 mg/m2 (n=49)
CR+mCR 10 (18.8) 11 (22.4)
ORR 14 (26%) 17 (35%)
ResponseCategory
Prev Treated(n=53)
Tx Naïve (n=49)
CR+mCR 11 (20.8) 10 (20.4)
ORR 12 (23%) 19 (39%)
60 mg/m2 (n=53) 90 mg/m2 (n=49)
8-week RBCs TransfusionIndependent n (%)
7/27 (26%) 5/24 (21%)
8-week Platelet Transfusion Independent n (%)
4/13 (31%) 5/15 (33%)
Take Home Message: SGI-110 may be useful after AZA failure
Nuevas Indicaciones
Combination Therapy
Example: Many clinic trials in development combine:
Azacitidine + Experimental Therapies
Approach: Improve upon existing therapies
Advantage: backbone is already FDA approved
Positive results can quickly change practice!

9/15/2016
5
Take Home Message: LEN has activity in non-del(5q) LR MDS
• Transfusion dependent Lower Risk MDS without del(5q) randomized to:
- Lenalidomide 10 mg daily or Placebo
• 26.9% became transfusion independent
• Median response duration of 32.9 weeks
• Being female, prior ESA, and low EPO were factors predictive of response
• Rates of AML progression were similar in both arms
Lenalidomide in non-del(5q)
Nuevos Tratamientos
Pipeline of Completely New Drugs
PD1-PDL1 Inhibitors
BCL2 Inhibitors
TGF-beta Inhibitors
Neddylation Inhibitors
Indolamine Dioxygenase Inhibitors
p53 Modulators
Hedgehog Inhibitors
Aminopeptidase Inhibitors
LSD-1 Inhibitors
Anti-CD33a AntibodiesOpciones
Disease
ON 01910
Gumireddy K, et. al. Cancer Cell 2005; 7: 275.
Rigosertib (ON-01910)
PLK1 & Cdc25C Inhibition
Multikinase Inhibitor
Finished Phase III Trial
3-day continuous infusion
Slide borrowed from Dr. Rami Komrokji
N BM CR (+HI) HI ORR
All patients 32 6 (1) 4 10/32 (31%)
3-day infusions 17 4 (1) 3 7/17 (41%)
3-day pivotal (1800 mg/d) 13 4 (1) 2 6/13 (46%)
0 20 40 60 80
0
20
40
60
80
100
Weeks
Su
rviv
al p
rob
ab
ility
(%
)
BM Blast Response
Not Assessed
Progressive Disease
Stable BM Blast Count
50%+ BM Blast Decrease
OS by Marrow
Blast Response
Median:
68 wks
Raza et al. Blood 2011; 3822
Rigosertib after Azacitidine
Slide borrowed from Dr. Rami Komrokji
Randomized Phase III Study of IV Rigosertib vs. BSC in Higher-risk MDS After HMA Failure
RigosertibN = 199
BSCN = 100
Number (%) of deaths 161 (81%) 81 (81%)
Median follow-up (months) 17.6 19.5
Median survival (months) 8.2 5.9
95% CI 6.0 - 10.1 4.1 - 9.3
Stratified HR (rigosertib/BSC) 0.87
95% CI 0.67 - 1.14
Stratified log-rank p-value 0.33
All Patients

9/15/2016
6
Randomized Phase III Study of IV Rigosertib vs. BSC in Higher-risk MDS After HMA Failure
RigosertibN = 199
BSCN = 100
Number (%) of deaths 161 (81%) 81 (81%)
Median follow-up (months) 17.6 19.5
Median survival (months) 8.2 5.9
95% CI 6.0 - 10.1 4.1 - 9.3
Stratified HR (rigosertib/BSC) 0.87
95% CI 0.67 - 1.14
Stratified log-rank p-value 0.33
Primary HMAFailure
Randomized Phase III Study of IV Rigosertib vs. BSC in Higher-risk MDS After HMA Failure
Take Home Message: Rigosertib is underwhelming after HMA failure,But we don’t have good alternatives either
Hedgehog Inhibitor – Phase II
Gumireddy K, et. al. Cancer Cell 2005; 7: 275.
Hedgehog Inhibitors
Slide borrowed from Dr. Rami Komrokji
Pathway important for stem cells
Several inhibitors in development
Drug PF-04449913Phase I in AML and MDS had several responders (7/21)
Combination of PF-04449913 and azacitadine is available at UCSD to previously untreated MDS patients.
Luspatercept
TPO mimetics
G-CSF (neupogen)
ESAs
EPO/ESAs
TGF-b
Luspatercept
TPO mimetics
G-CSF (neupogen)
ESAs
EPO/ESAs
TGF-b

9/15/2016
7
Promoting Red Cell Production
Luspatercept (ACE-536) and Sotatercept (ACE-011)
Promoting Red Cell Production
Luspatercept (ACE-536) and Sotatercept (ACE-011)
Immune Based Therapies
PD1 and PD-L1 Inhibitors
Combination Trial will be opening at UCSD in the Fall
Trasplante de Células Madre
Trends in Transplantation
Goal of Hematopoietic Stem Cell Transplantation:
#1) Replace a dysfunction host hematopoietic system with normal, healthy donor marrow.
#2) Allow the donor immune system to destroy the abnormal, diseased host cells (MDS).
Conditioning
Donor Cells
Engraftment Graft-vs.-MDS
<5% of patients with MDS currently undergo allogeneic SCT
“Only curative therapy”
Survives transplant;MDS cured!
(35-40%)
Survives transplant;MDS recurs/persists
(30-40%)
Patients who go in to RIC allo SCT with <10% blasts appear to have lower relapse
Transplant candidateDonor identified
Dies from complication of transplant
(20-25%)
Optimal timing, pre-transplant therapy, conditioning unclear;usually reserved for IPSS Int-2/High (IBMTR Markov analysis)
Cutler C et al Blood 2004; 104(2):579-85Sekeres M et al JNCI 2008;100(21):1542-51. Slide borrowed from Dr. David Steensma
Allogeneic Stem Cell Transplantation for MDS

9/15/2016
8
Obstacles to TransplantationGraft Rejection
– need to suppress the host immune system
Toxicity– infection– organ damage– graft versus host disease
Finding a Donor– siblings match only 25% of the time– and are often too old or ill to donate
Overcoming ObstaclesAvoiding Graft Rejection
– better approaches to immune suppression
Less Toxicity– better supportive care– better antigen matching– reduced intensity conditioning
Alternative Sources for Stem Cells– haploidentical – “half” match– umbilical cord blood stem cells
0
20
40
60
80
100
1990-1996 1997-2003 2004-2010 1990-1996 1997-2003 2004-2010
< 50 years
>= 50 years
Trends in Allogeneic Transplantsby Transplant Type and Recipient Age*
1990-2010
* Transplants for AML, ALL, NHL, Hodgkin Disease, Multiple Myeloma
Tra
nspla
nts
, %
0
20
40
60
80
100
2001-2005 2006-2010 2001-2005 2006-2010
<=20 yrs
21-40 yrs
41-50 yrs
51-60 yrs
>60 yrs
Allogeneic Transplants for Age > 20yrs,Registered with the CIBMTR, 1993-2010
- by Donor Type and Graft Source -
Num
ber
of Tra
nspla
nts
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
11,000
12,000
13,000
14,000
1993-94 1995-96 1997-98 1999-00 2001-02 2003-04 2005-06 2007-08 2009-10
Related BM/PB
Unrelated BM
Unrelated PB
Unrelated CB
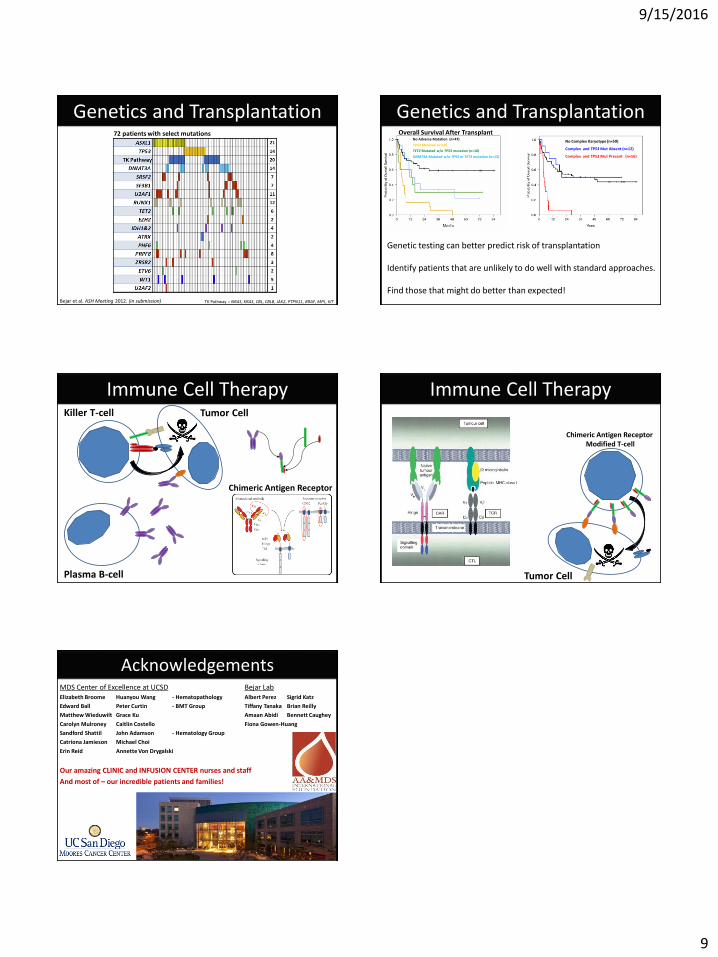
Bejar et al. ASH Meeting 2012. (in submission)
Blasts < 5% (n=42)
Blasts ≥ 5% (n=45)
p = 0.029
Other karyotype (n=59)
Complex karyotype (n=28)
p = 0.005
Overall Survival After Transplant
Genetics and Transplantation
9/15/2016
9
72 patients with select mutations
TK Pathway = NRAS, KRAS, CBL, CBLB, JAK2, PTPN11, BRAF, MPL, KITBejar et al. ASH Meeting 2012. (in submission)
Genetics and TransplantationNo Complex Karyotype (n=59)
Complex and TP53 Mut Absent (n=12)
Complex and TP53 Mut Present (n=16)
Overall Survival After TransplantNo Adverse Mutation (n=47)
TP53 Mutated (n=18)
TET2 Mutated w/o TP53 mutation (n=10)
DNMT3A Mutated w/o TP53 or TET2 mutation (n=12)
Genetics and Transplantation
Genetic testing can better predict risk of transplantation
Identify patients that are unlikely to do well with standard approaches.
Find those that might do better than expected!
Immune Cell TherapyKiller T-cell
Plasma B-cell
Tumor Cell
Chimeric Antigen Receptor
Immune Cell Therapy
Chimeric Antigen Receptor Modified T-cell
Tumor Cell
Bejar LabAlbert Perez Sigrid Katz
Tiffany Tanaka Brian Reilly
Amaan Abidi Bennett Caughey
Fiona Gowen-Huang
AcknowledgementsMDS Center of Excellence at UCSDElizabeth Broome Huanyou Wang - Hematopathology
Edward Ball Peter Curtin - BMT Group
Matthew Wieduwilt Grace Ku
Carolyn Mulroney Caitlin Costello
Sandford Shattil John Adamson - Hematology Group
Catriona Jamieson Michael Choi
Erin Reid Annette Von Drygalski
Our amazing CLINIC and INFUSION CENTER nurses and staff
And most of – our incredible patients and families!