
Overview of the tool - University of Aberdeen tool documents omissions (vaginal omission score,...
15
1 Near-miss and quality of care tool Overview of the tool The improvement of quality of care in referral facilities is critical to the success of programmes and policies aimed at reducing maternal and perinatal mortality. This document describes a tool developed and used to measure the technical quality of maternal and perinatal care in referral facilities in the context of the FEMHEALTH evaluation: http://www.abdn.ac.uk/femhealth/ The tool enables researchers or healthcare providers in low and middle income country settings to extract information from medical records. The information extracted can be used for monitoring and evaluation over a period of time at a facility level or across facilities or for clinical audit where target setting is required for particular indicators (“criterion based audit”). How was the tool developed? The tool was developed on the basis of: - a review of existing tools, including data extraction forms used by: the London School of Hygiene and Tropical Medicine (LSHTM) and its partners in multi-country near-miss projects in Francophone Africa, the World Health Organization (WHO) Multi Country Survey Project on severe maternal morbidity and the Unmet Obstetric Need (UON) projects led by the Institute of Tropical Medicine in Antwerp. -a review of process and outcome indicators proposed or used in quality of care studies including in particular: (1) the UK Department of Health document entitled “An organisation with a memory” for the concept of “health care near-miss”; (2) UK National Collaborative Centre for Women’s and Children’s Health 2004 clinical guidelines on caesarean section as well research done by Dr Fabienne Richard and others on a “quality caesarean delivery”; (3) other published studies in the quality of care in obstetric services in high or low income settings; (4) the intrapartum still birth and early neonatal death indicator (QUIP-Care) proposed by Dr Vincent Fauveau; and (5) suggestions made for the neonatal near-miss criterion, for example by Lubega and Pattinson in South Africa. - a series of consultations with maternal and neonatal health experts, with relevant research or clinical experience in low and middle income settings, during and after an international workshop in London in 2011. - research hypotheses on the probable effects of the removal of user fees policies on quality of care and health outcomes.
Transcript of Overview of the tool - University of Aberdeen tool documents omissions (vaginal omission score,...

1
Near-miss and quality of care tool
Overview of the tool
The improvement of quality of care in referral facilities is critical to the success of programmes and
policies aimed at reducing maternal and perinatal mortality.
This document describes a tool developed and used to measure the technical quality of maternal
and perinatal care in referral facilities in the context of the FEMHEALTH evaluation:
http://www.abdn.ac.uk/femhealth/
The tool enables researchers or healthcare providers in low and middle income country settings to
extract information from medical records.
The information extracted can be used for monitoring and evaluation over a period of time at a
facility level or across facilities or for clinical audit where target setting is required for particular
indicators (“criterion based audit”).
How was the tool developed?
The tool was developed on the basis of:
- a review of existing tools, including data extraction forms used by: the London School of Hygiene
and Tropical Medicine (LSHTM) and its partners in multi-country near-miss projects in Francophone
Africa, the World Health Organization (WHO) Multi Country Survey Project on severe maternal
morbidity and the Unmet Obstetric Need (UON) projects led by the Institute of Tropical Medicine in
Antwerp.
-a review of process and outcome indicators proposed or used in quality of care studies including in
particular: (1) the UK Department of Health document entitled “An organisation with a memory”
for the concept of “health care near-miss”; (2) UK National Collaborative Centre for Women’s and
Children’s Health 2004 clinical guidelines on caesarean section as well research done by Dr Fabienne
Richard and others on a “quality caesarean delivery”; (3) other published studies in the quality of
care in obstetric services in high or low income settings; (4) the intrapartum still birth and early
neonatal death indicator (QUIP-Care) proposed by Dr Vincent Fauveau; and (5) suggestions made for
the neonatal near-miss criterion, for example by Lubega and Pattinson in South Africa.
- a series of consultations with maternal and neonatal health experts, with relevant research or
clinical experience in low and middle income settings, during and after an international workshop in
London in 2011.
- research hypotheses on the probable effects of the removal of user fees policies on quality of care
and health outcomes.

2
What type of information is collected?
The tool collects information on health outcomes (maternal near-miss, neonatal near-miss, unmet
need for obstetric complication, maternal deaths, neonatal deaths, stillbirths) and on the process of
care (health care near-miss indicators). In addition, information on demographic and reproductive
risk factors is collected.
The information collected with this tool enable us to:
Determine the frequency of maternal near-miss before and after admission
Determine the frequency of neonatal near-miss
Determine the case fatality of severe obstetric or perinatal complications
Measure the unmet need for life-saving obstetric surgery
Determine the quality of care provided for vaginal birth, caesarean section, the baby, twins,
breech presentations and forceps delivery
Investigate risk factors for complications and deaths
What are the definitions of maternal, neonatal and health care near-
misses?
Maternal near-miss refers to situations where women nearly died during pregnancy, childbirth or
after pregnancy and they survived either by chance or because of the good quality of care they
received. Their complications are so severe that their chance of survival without any clinical
assistance in the community is very small.
In the attached tool two types of criteria were used.
Organ system criteria proposed by the World Health Organisation to enable international
comparison (questions 116-122) (WHO, 2011).
Clinical criteria based on complications to enable comparison over time with previous
projects in the focus countries (questions 111-115) and question 123 (the criteria presented
in the attached document are AUDOBEM criteria).
The WHO criteria are very stringent and focus very much on the severe end of the morbidity
spectrum. Therefore they identify a smaller number of near-miss cases compared to the clinical
criteria based on complications. We do not advocate the use of both types of criteria in all studies.
The choice of the criteria will depend on the objectives of the study and on the sample size that is
required to gain meaningful results on near-miss cases.
Neonatal near-miss also refers to situations where the newborns nearly died between 0-28 days and
they survived either by chance or because of the good quality of care they received. Neonatal near-
miss criteria are more difficult to define than maternal near-misses, and WHO has not yet produced
a global definition and global criteria. FEMHEALTH questions are based on criteria used by Pileggi et
al. and Lubega and Pattinson in South Africa.

3
For Pillegi et al., the criteria are proxies for the main causes of early neonatal deaths and
include Agpar <5, birthweight <1500 g, and gestational age < 31 weeks (questions 85a, 82a,
and 47)
For Lubega and Pattinson, criteria are based on dysfunctions of the organ system (question
125).
Health care near-miss were defined in the FEMHEALTH project as negative events or omissions
which occurred in the process of care but which did not (necessarily) lead to serious harm.
The tool documents omissions (vaginal omission score, caesarean omission score, and neonatal
omission score), delays (decision to intervention for caesarean, blood transfusion) and treatment
failures (near-miss after admission for women admitted in normal labour, etc). Appendix 1 has a list
of the indicators considered.
Unmet Obstetric Need is an indicator which include all major obstetric interventions (caesarean
section, laparotomy, hysterectomy, symphysiotomy, craniotomy, internal version) for absolute
indication (i.e. complications for which women have a high probability of dying). Questions for
calculating this indicator are in section E (question 100) and A3 (hysterectomy, craniotomy etc)
QUIP-Care is an indicator of quality of care proposed by Fauveau– it measures the proportion of
intrapartum (fresh) stillbirths and very early (first 24 hours) newborn deaths over all births in a
facility and excludes newborn under 2.5 kg.
How is the tool structured? The tool is divided in 11 sections.
Section labelled “Instructions”
This section enables the supervisor and data extractor to check that women and babies are
recruited in the categories of interest, such as near-miss or caesarean. This is either because
the outcomes are of direct interest to the study (e.g. deaths) or there are quality of care
indicators specific to certain conditions. If possible, all women admitted in the facilities
during the period of interest should have their medical records extracted as this facilitates
the calculation of incidences. In FEMHEALTH, because of logistic constraints, we recruited
only a sample among the women in the “other” admission categories.
Several categories can be checked e.g. neonatal near-miss and maternal near-miss; but it is
not possible to be both a neonatal/ maternal near-miss and death, as near-miss cases
survive by definition. It is also not possible to be an “other” admission and have another
category checked.
Section A1:
Section A1 includes information on the researcher who filled in the questionnaire, facility
and the geographical location of the patient. For ethical and confidential reasons, the name
and addresses should not be entered into a database. The name of the patient is only
included for quality control at the time of supervision and to facilitate the retrieval of

4
information when the data extracted from medical records need to be supplemented by
information from registers. The addresses are used to understand the catchment area of the
facility. If this information is used for patient follow-up in a cohort study, remember that the
patient might be known under a different name in her locality
The section also includes information on the date of admission. Together with the date of
discharge in section A3, the duration of stay in the facility can be calculated. Duration of stay
is an indicator of quality of care and of complications severity.
Detailed questions on referral are also included. This information is very useful to calculate
delays, and can sometimes be obtained from the referral letters.
Section A2
This section is very short as medical records include limited information on the demographic
and socio-economic characteristics of the patients. Depending on the country, the only
information on the socio-economic status might be the marital status, the occupation of the
husband, or the religion of the woman. This information is useful to understand whether the
access to facilities and treatment is equitable.
If the study needs additional information on demographic characteristic, a special form can
be added to all records to remind staff to collect these data during the period of the data
collection.
Section A3
This section is concerned with reproductive risk factors such as age and parity.
The section also documents the patient’s “gate to gate” journey in the facility from
admission (dates and reasons for admission, gestational age, foetal heart rate at admission),
to delivery (date and time of delivery, as well as the mode of delivery), and discharge (vital
status at discharge, date and time, referral to another facility).
It includes information on some specific interventions and therapeutic treatments such as
hysterectomy, blood transfusion (volume, delays, and timing).
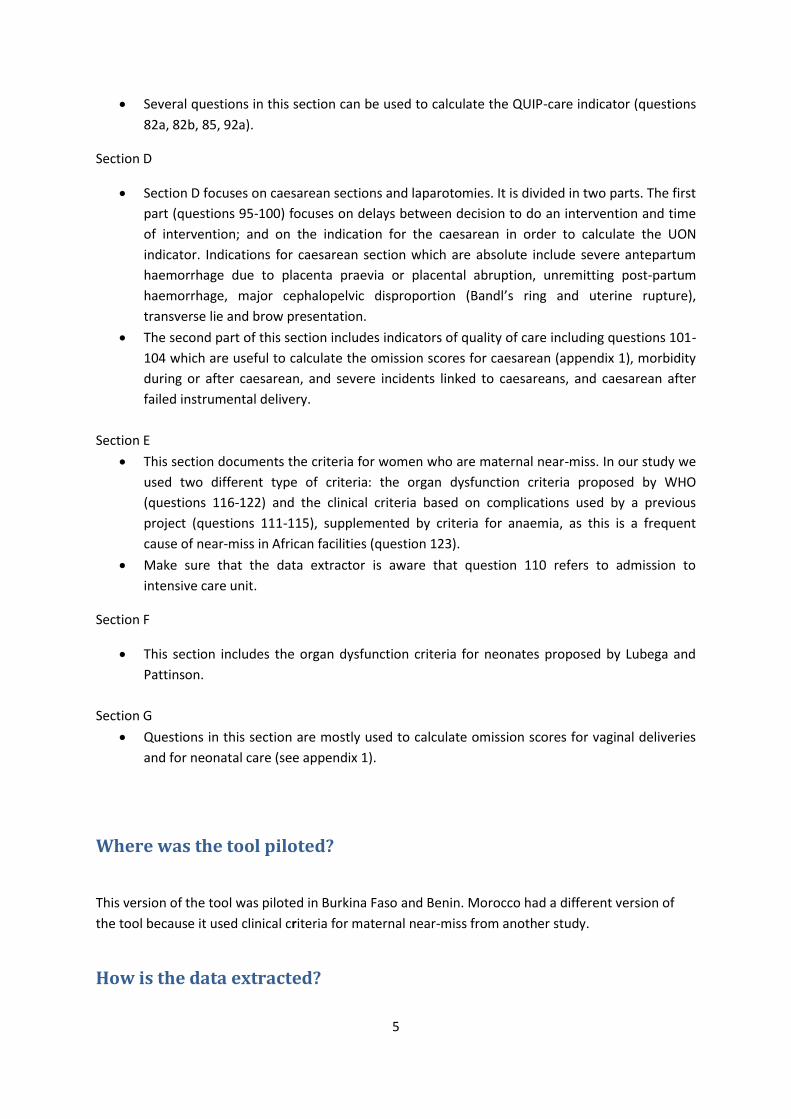
Section B
As not all obstetric complications are maternal near-miss, this section document diagnoses
for women who had a morbidity during their hospital stay under six categories
(haemorrhage, hypertension, anaemia, infection, dystocia and other pathologies).
Section C
This section is concerned with the newborn(s), and there is enough space to document twin
deliveries. When there are more than 2 babies, an extra form can be used and attached to
this section.
This section documents the presentation at birth, the sex of the baby, birthweight, whether
the baby was born alive or was stillborn, Apgar score, neonatal complications, trauma,
referral, admission to intensive care, vital status at discharge, date of discharge, cause of
death.
5
Several questions in this section can be used to calculate the QUIP-care indicator (questions
82a, 82b, 85, 92a).
Section D
Section D focuses on caesarean sections and laparotomies. It is divided in two parts. The first
part (questions 95-100) focuses on delays between decision to do an intervention and time
of intervention; and on the indication for the caesarean in order to calculate the UON
indicator. Indications for caesarean section which are absolute include severe antepartum
haemorrhage due to placenta praevia or placental abruption, unremitting post-partum
haemorrhage, major cephalopelvic disproportion (Bandl’s ring and uterine rupture),
transverse lie and brow presentation.
The second part of this section includes indicators of quality of care including questions 101-
104 which are useful to calculate the omission scores for caesarean (appendix 1), morbidity
during or after caesarean, and severe incidents linked to caesareans, and caesarean after
failed instrumental delivery.
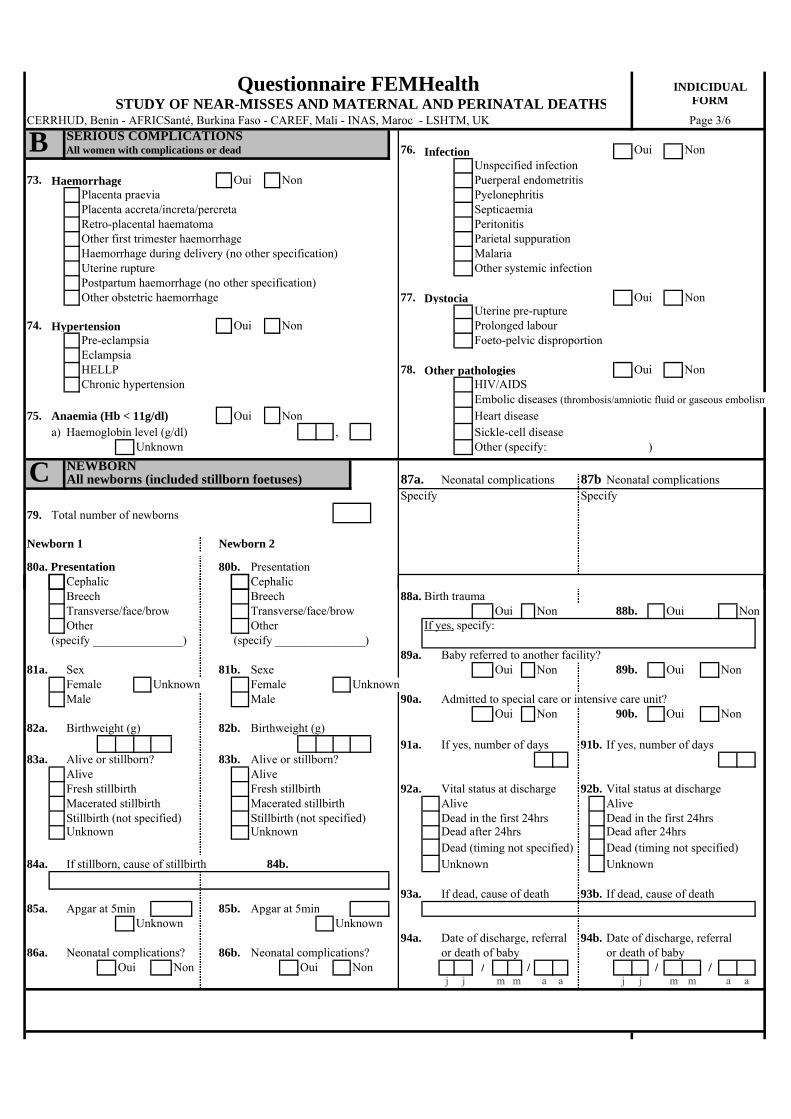
Section E
This section documents the criteria for women who are maternal near-miss. In our study we
used two different type of criteria: the organ dysfunction criteria proposed by WHO
(questions 116-122) and the clinical criteria based on complications used by a previous
project (questions 111-115), supplemented by criteria for anaemia, as this is a frequent
cause of near-miss in African facilities (question 123).
Make sure that the data extractor is aware that question 110 refers to admission to
intensive care unit.
Section F
This section includes the organ dysfunction criteria for neonates proposed by Lubega and
Pattinson.
Section G
Questions in this section are mostly used to calculate omission scores for vaginal deliveries
and for neonatal care (see appendix 1).
Where was the tool piloted?
This version of the tool was piloted in Burkina Faso and Benin. Morocco had a different version of
the tool because it used clinical criteria for maternal near-miss from another study.
How is the data extracted?

6
Depending on the number of hospitals included, it is probably best if the data is extracted by the
health care staff employed by the facilities as they can identify the patients prospectively. In some
countries, all health care staff in the maternity unit were trained and paid by completed
questionnaires to a sufficient standard. In other settings, the data was extracted by a small number
of providers who had been selected because of their interest with the research. In both cases, the
research team must visit the facilities at regular interval to check the quality of the data extraction.
Extracting data for a normal delivery takes about 10 minutes, and for a caesarean section or near-
miss, the average extraction time is between 15-20 minutes.
What are the limitations of the tool?
Neonates who are re-admitted after discharge or admitted after home delivery need a special form
for themselves, as there may be no information on the mother. It can also be difficult to link
neonates medical records to their mothers’ record when they have been transferred to the neonatal
services because they were ill.
When the identification is done prospectively, it can take several days to finish the form as a woman
admitted for a complication in pregnancy may develop a near-miss later on during her stay.
This tool has been developed for use in low income and middle income settings where medical
records are not computerised and information included in records is patchy. Therefore it only
includes a small range of quality of care indicators.
What Resources are required to apply the tool?
The resources required to carry out a study of near-miss and quality of care will vary depending on
the objectives of the study, the primary outcomes for the study, the sample size required for to
demonstrate changes or variations in the primary outcomes, the number of hospitals involved, and
other local factors such as whether computerised records exist and how much staff are paid for this
type of activities.
Who can I contact for further information on this tool?
In Benin: Dr Sourou Goufodji ([email protected]), Centre de Recherche en Reproduction Humaine
et en Demographie
In Burkina Faso: Dr Rasmane Ganaba ([email protected]) and Dr Cheick Traore
([email protected]), AfricSanté
In Morocco: Dr Bouchra Assarag ([email protected]), INSP

7
In London: Dr Veronique Filippi ([email protected]), Professor Carine Ronsmans
([email protected]) and Dr Jenny Cresswell ([email protected]), London
School of Hygiene and Tropical Medicine
References Health Foundation. Levels of Harm. London: Health Foundation, 2011.
National Collaborating Centre for Women’s and Children’s Health, Caesarean Section, National
Evidence Based Guideline, RCOG Press, London, UK, 2004.
Pillegi C, Souza JP, Cecatti JC, Faundes A. Neonatal near-miss approach in the 2005 WHO global
survey Brazil. Jornal de Pediatria 2010 86(1):21-26
Richard F, Ouedraogo C, de Brouwere V. Quality cesarean delivery in Ouagadougou, Burkina Faso: a
comprehensive approach. International Journal of Gynecology and Obstetrics, 2008 103, 283-290

8
Appendix 1
Table 1: Recommended indicators
Indicator Definition
Omission
Omission scores for vaginal deliveries
The proportion of routine procedures for vaginal deliveries not done, including postpartum care. Numerator: Negative or don’t know responses to measurement of blood pressure at admission, measurement of heart beat of baby during labour, partogram use, measurement of postpartum pulse, measurement of postpartum blood pressure, measurement of postpartum bleeding, measurement of postpartum temperature Denominator: number of procedures x women Women included: singleton live birth and stillbirths
Omission score for caesarean delivery
The proportion of routine procedures for caesarean deliveries not done, including postpartum care. Numerator: Negative or don’t know responses to measurement of haemoglobin pre-surgery, of foetal heart beat pre-surgery, prescription of antibiotics at any point, provision of oxytocin during procedures, measurement of blood pressure postpartum, measurement of respiration postpartum, measurement of pulse postpartum Denominator: number of procedures x women Women included: all women with routine and emergency caesarean
Omission score for neonate
The proportion of routine procedures not done for babies born alive vaginally, including postnatal care. Numerator: Negative or don’t know responses to measurement of baby heart during active phase, measurement of Apgar at 5 minutes, assessment of colour during postnatal period, assessment of respiration during postnatal period, assessment of breastfeeding, measurement of temperature during postnatal period Denominator: Number of procedures x number of babies Babies included: singleton babies born alive and vaginally
Transfusion less than requested
Proportion of women requiring a blood transfusion who received less transfusion than requested Women included: women requiring a blood transfusion
Delays
Delays for caesarean section (c/s) between decision to intervene and start of intervention
Average duration of delays between decisions and intervention Numerator: sum of average length of time for all c/s in facilities, except planned c/s Denominator: number of c/s except planned c/s NB: Accepted decision to delivery time for caesarean section in high income settings is usually set at 30 minutes for audit purpose (National Collaborating Centre for Women’s and Children’s Health, 2004).
Treatment failure
Serious events or incidents for caesarean sections
Proportion of women who delivered by caesarean section who have at least one serious morbidity or incidents
Baby’s heart present when women arrived among stillbirths
Proportion of stillbirths among women admitted with positive foetal heart beat Numerator : stillbirths with positive heart beat at admissions

9
Denominator : women with positive foetal heart beat at admission (including those who are born alive and stillbirths)
Maternal near-miss after admission
Proportion of women admitted for a normal labour who develop a near-miss after admission Numerator: women with near-miss after admission Denominator: women admitted in normal labour
Case fatality among SAMM
Proportion of women with a severe morbidity who die Numerator: maternal deaths Denominator: maternal near-miss cases and deaths
Table 2: Indicators which need further development or large sample
Indicators Reasons for further development or larger sample
Omission score for complicated childbirth
Women have admitted for a range of complications, and it was difficult to construct a meaningful indicators which reflect the full range of needs. For this reason, we only included on indicator on omission for haemorrhage which is the most frequent complication
Twins diagnosed during delivery
Useful for large study with an interest in the performance of antenatal care
Breech diagnosed during delivery
As above
Instrumental deliveries with position of occiput undetermined
Rare event ; difficult to collect retrospectively
Delays for blood transfusion
Important indicator, particularly for projects focussing on reducing maternal deaths and near-miss cases from haemorrhage. But difficult to interpret because we do not have a threshold as for caesarean section. Further technical specification required
Return to delivery room for placenta retention
Rare event ; difficult to collect retrospectively
Emergency c/s following attempted instrumental deliveries
Difficult to interpret with respect to performance
Readmission following complications
Rare event ; difficult to collect retrospectively
Hospital discharge against advice
Rare event ; difficult to collect retrospectively

Questionnaire FEMHealth INDIVIDUAL
STUDY ON NEAR-MISSES AND MATERNAL AND PERINATAL DEATHS FORM
CERRHUD, Benin - AFRICSanté, Burkina Faso - CAREF, Mali - INAS, Maroc - LSHTM, UK Page 1/6Instructions Echantillon(s) au(x)quel(s) appartient ce dossierThe target population is specified in thetitle of each section. Certain sections Caesarean Neonatal near-miss Twins Other admissionscan be skipped according to the patient. Maternal near-miss Neonatal death Breech presentationIf the information is not known, Maternal death Stillbirth Vacuum/forcepsrecord a "9" in the field.
A1IDENTIFICATIONAll women included in the study sample 15. Admission mode Self-referred
1. Health facility name Referred from another facilityIf referred16. Name of referring facility
2. Health facility code
3. Woman's ID number 17. Date of arrival at referring facility / /j j m m a a
4. Date form filled / / 18. Time of arrival at referring facility :j j m m a a h h m m
5. Researcher name
19. Date of decision to refer / /j j m m a a
6. Researcher code 20. Time of decision to refer :
7. Woman's name h h m m
21. Date of departure from facility / /8. Town j j m m a a
22. Time of departure from facility :
9. Village/neighbourhood h h m m
23. Means of transport used Ambulance10. Administrative area of origin Personal vehice
Other11. District of origin If referred from a study facility
24. Code of referring facilityIf readmitted
12. Admission date / / 25. Date of readmission / /j j m m a a j j m m a a
13. Admission time : 26. Time of readmission :h h m m h h m m
14. Maternity record number 27. Preceding record number
A2DEMOGRAPHIC CHARACTERISTICSAll women included in the study sample 30. Type of insurance
28. Age (years) 31. Woman's occupation
29. Status MarriedSingleWidowed 32. Partner's occupationOther
A3REPRODUCTIVE HISTORYAll women included in the study sample 37. Number of children died (born alive)
33. Number of pregnancies 38. Does the women have a history of Oui Non NSPcaesarean or abdominal scar?
34. Number of live births 39. Does the woman have a history of Oui Non NSPabortion?
35. Number of stillbirths 40. Does the woman have FGM? Oui Non NSP
36. Number of children alive (today) 41. Did the woman receive antenatal care? Oui Non NSP

y
Questionnaire FEMHealth INDIVIDUALSTUDY OF NEAR-MISSES AND MATERNAL AND PERINATAL DEATHS FORM
CERRHUD, Benin - AFRICSanté, Burkina Faso - CAREF, Mali - INAS, Maroc - LSHTM, UK Page 2/6
A3REPRODUCTIVE HISTORY (CONT')All women included in the study sample If readmitted
42. Reason for admission Normal delivery 43. Reason for readmission Normal deliveryComplicated delivery Complicated deliveryExtra-uterine pregnancy Other complication during deliveryOther complication during delivery Prophylactic caesareanProphylactic caesarean Abortion, miscarriage, orAbortion, miscarriage, or post-abortion complicationpost-abortion complication Postpartum complicationPostpartum complication
44. Was the fœtal heart beat audible Yes Were the following interventions done?upon admission? No 51. External version Oui Non NSP
Not perceivedNot measured 52. Hysterectomy Oui Non NSP
45. Date of delivery or end of / / 53. Blood transfusion Oui Non NSPp yregnanc j j m m a a
46. Time of delivery or end of : If yes: 54. Number of units requiredp yregnanc h h m m
47. Gestational age Estimated at term 55. Number of units transfusedEstimated pre-termEstimated post-term 56. tDate of laboratory reques / /Unknown j j m m a a
57. Time of laboratory request :If known 48. Weeks of amenorrhea h h m m
49. Month of pregnancy 58. Date of beginning of transfusion / /j j m m a a
If abortion, miscarriage or extra-uterine pregnancy: go to question 52 59. nTime of beginning of transfusio :h h m m
50. Mode of delivery Vaginal - perineum intactg pVaginal - episiotomy 60. Was a complication identified Oui Non NSPVaginal - with tears during hospitalisation?Vaginal - not specifiedInstrumental - vacuum/forceps Specify (summarise main events):Planned caesareanEmergency intrapartum caesareanEmergency antepartum caesareanLaparotomy for uterine ruptureDestructive - symphysiotomyDestructive - craniotomy/embryotomyUknown
61. Vital status of woman at discharge Alive Dead
62. Date of discharge or death / / If readmitted 64. Date of second discharge / /of woman j j m m a a or d heat j j m m a a
63. Time of discharge or death : 65. Time of second discharge :of woman h h m m or death h h m m
If alive 66. Mode of exit Normal discharge If dead 67. Time of death Dead on arrivalLeft against medical advice Dead between arrival and admissionReferred to other hospital Dead in the first 24hrsEscaped Dead after 24hrs
If referred 68. Referral facility name
70. Date of decision to refer / /69. Reason for referral j j m m a a
71. Time of decision to refer :h h m m
If referred to a study facility 72. Referral facility code
Questionnaire FEMHealth INDICIDUALSTUDY OF NEAR-MISSES AND MATERNAL AND PERINATAL DEATHS FORM
CERRHUD B i é B F Ma M P, en n - AFRICSant , urkina aso - CAREF, li - INAS, aroc - LSHTM, UK age 3/6
B SERIOUS COMPLICATIONSAll women with complications or dead 76. Infection Oui Non
Unspecified infection73. Haemorrhage Oui Non Puerperal endometritis
Placenta praevia PyelonephritisPlacenta accreta/increta/percreta SepticaemiaRetro-placental haematoma PeritonitisOther first trimester haemorrhage Parietal suppurationHaemorrhage during delivery (no other specification) MalariaUterine rupture Other systemic infectionPostpartum haemorrhage (no other specification)Other obstetric haemorrhage 77. Dystocia Oui Non
Uterine pre-rupture74. Hypertension Oui Non Prolonged labour
Pre-eclampsia Foeto-pelvic disproportionEclampsiaHELLP 78. Other pathologies Oui NonChronic hypertension HIV/AIDS
Embolic diseases (thrombosis/amniotic fluid or gaseous embolism75. Anaemia (Hb < 11g/dl) Oui Non Heart disease
a) Haemoglobin level (g/dl) , Sickle-cell diseaseUnknown Other (specify: )
C NEWBORNAll newborns (included stillborn foetuses) 87a. Neonatal complications 87b Neonatal complications
Specify Specify79. Total number of newborns
Newborn 1 Newborn 2
80a. Presentation 80b. PresentationC h liCephalic C h liCephalicBreech Breech 88a. Birth traumaTransverse/face/brow Transverse/face/brow Oui Non 88b. Oui NonOther Other If yes, specify:
(specify _______________) (specify _______________)89a. Baby referred to another facility?
81a. Sex 81b. Sexe Oui Non 89b. Oui NonFemale Unknown Female UnknownMale Male 90a. Admitted to special care or intensive care unit?
Oui Non 90b. Oui Non82a. Birthweight (g) 82b. Birthweight (g)
91a. If yes, number of days 91b. If yes, number of days83a. Alive or stillborn? 83b. Alive or stillborn?
Alive AliveFresh stillbirth Fresh stillbirth 92a. Vital status at discharge 92b. Vital status at dischargeMacerated stillbirth Macerated stillbirth Alive AliveStillbirth (not specified) Stillbirth (not specified) Dead in the first 24hrs Dead in the first 24hrsUnknown Unknown Dead after 24hrs Dead after 24hrs
Dead (timing not specified) Dead (timing not specified)84a. If stillborn, cause of stillbirth 84b. Unknown Unknown
93a. If dead, cause of death 93b. If dead, cause of death85a. Apgar at 5min 85b. Apgar at 5min
Unknown Unknown94a. Date of discharge, referral 94b. Date of discharge, referral
86a. Neonatal complications? 86b. Neonatal complications? or death of baby or death of babyOui Non Oui Non / / / /
j j m m a a j j m m a a

g)
Questionnaire FEMHealth INDIVIDUAL
STUDY OF NEAR-MISSES AND MATERNAL AND PERINATAL DEATHS FORM
CERRHUD, Benin - AFRICSanté, Burkina Faso - CAREF, Mali - INAS, Maroc - LSHTM, UK Page 4/6
D CAESAREANS AND LAPAROTOMIESAll caesareans and laparotomies for uterine rupture d) Malpresentation Oui Non
If yes: Transverse95. Date of decision of intervention / / Oblique
j j m m a a Brow96. Time of decision of intervention : Face with posterior chin/"enclaved" face
h h m m Arm or shoulder97. Date of intervention / /
j j m m a a e) Poor progression of labour Oui Non98. Time of beginning of intervention : If yes: Prolonged labour
h h m m Failed induction99. Time of end of intervention : Other
h h m m Yes (no specification)100. Indication for caesarean or laparotomy
a) Foeto-pelvic disproportion Oui Non f) Previous caesarean Oui NonIf yes Small or deformed pelvis
Fœtal macrosomia h) Fœtal indication Oui NonUnspecified disproportion If yes: Fœtal distress
Cord prolapseb) Severe antepartum haemorrhage Oui Non Cord around neckIf yes: Placenta praevia Intra-uterine growth retardation
Retro-placental haematomaYes (no specification) i) Breech presentation Oui Non
c) Uterine rupture or pre-rupture Oui Non j) Psychosocial indications Oui NonIf yes: Uterine rupture Yes, maternal request
Uterine pre-rupture Yes, "precious" pregnancy
g) (Pre-)eclampsia( ) p Oui Non k)) Other Oui NonIf yes: Eclampsia Specify _________________________________
Pre-eclampsiaIndication not specified
Quality of care indicators for caesareans and laparotomies of uterine rupture101. Before the surgery, 105. Morbidity during or after caesarean
a) Was the haemoglobin level checked? Blood transfusionOui Non NSP Wound infection
b) Was the fœtal heart beat checked just before the Puerperal feveranaesthesia? N/A (stillborn) Oui Non NSP Evacuation of a haematoma
Secondary postpartum haemorrhagec) Were prophylactic antibiotics prescibred? Severe postpartum anaemia
Oui Non NSP SepticaemiaIf yes: 102. When were they administered? Hysterectomy
Before the surgery 106. Severe incidents linked to caesareansDuring the surgery Admission for over 1 week due toAfter the surgery post-surgical infection
Anaesthetic accident103. During the surgery, was prophylactic oxytocin administered? Accident of blood transfusion
Oui Non NSP Uterine artery piercedAccident of other organs
104. During the first 2hrs post-surgery, did someone monitor Return to operating roomevery 30 minutes: Other specifya) Arterial blood pressure ________________________________________
Yes Done less frequently No NSP ________________________________________)b) Respiratory rate?
Yes Done less frequently No NSP 107. Caesarean after failed instrumental deliveryc) Pulse? Oui Non NSP
Yes Done less frequently No NSP
Seve dos
Questionnaire FEMHealth INDIVIDUAL
STUDY OF NEAR-MISS AND MATERNAL AND PERINATAL DEATHS FORM
CERRHUD, Benin - AFRICSanté, Burkina Faso - CAREF, Mali - INAS, Maroc - LSHTM, UK Page 5/6
E MATERNAL NEAR-MISS 109. When did the state of near-miss occur?All women in state of near-miss Before arrival at the facility
During hospitalisation108. Is the woman considered to be in a state of near-miss?
Yes - according to clinical criteria (AUDOBEM) 110. Did the woman require intensive care?Yes - according to organ dysfunction criteria (WHO) Yes UnknownYes - anaemia NoNo
Clinical criteria 113. Infections111. Uterine rupture and pre-rupture Temp >38,0° or <36,5 or obstetric infectious seat
Dystiocia with rapid maternal pulse or fœtal distress AND jaundice or state of shock or cardiac arrestAND sub-pubic tenderness or bandl ring Diagnosis of septicaemia in medical record
Diagnosis of rupture/pre-rupture in medical recordDystocia with shock or cardiac arrest 114. Severe pre-eclampsiaDystocia requiring laparotomy Dyastolic BP >=110 mmHg or Proteinuria/albuminuria +++
AND hyper reflectivity or headache or blurred vision 112. Haemorrhage or oliguria or high abdominal pain or pulmonary oedema
Haemorrhage with state of shock or jaundiceHaemorrhage with cardiac arrest 115. EclampsiaHaemorrhage with laparotomy Dyastolic BP>=90 mm Hg or proteinuria/albuminuria ++Haemorrhage with blood transfusion AND convulsions or coma
Organ dysfunction criteria116. Cardiovascular dysfunction 119. Renal dysfunction
Shock Oliguria non responsive to fluids or diureticsCardiac arrest Severe acute azotemia (creatinine >300umol/ml Severe hypoperfusion (lactate >5mmol/l or >45mg/dl) Dialysis for acute renal failure or >3.5mg/dL)Severe acidosis (pH<7.1)e c s (p 7. )Use of continuous vasoactive drugs 120. Coagulation dysfunctionCardio-pulmonary ressuscitation Failure to form clots
Severe acute thrombocytopenia (<50,000 platelets/ml)117. Respiratory dysfunction Massive transfusion of blood or red cells (≥5 units)
Acute cyanosisGasping 121. Hepatic dysfunctionSevere tachypnea (respiratory rate/min>40) Jaundice in the presence of pre-eclampsiaSevere bradypnea (respiratory rate/min<6) Severe hyperbilirubinemia Severe hypoxaemia (O2 saturation <90% for ≥60min or PaO2/FiO2<200) 122. Neurological dysfunctionIntubation and ventilation not related to anaesthesia Prolonged unconsciousness or coma lasting >12hrs
Stroke118. Uterine dysfunction Status epilepticus / uncontrollable fits
Haemorrhage or infection leading to hysterectomy Total paralysis
Anaemia criteria123. Severe anaemia Haemoglobin level 4-7g/dl; OR Cutaneo-mucosal pallor
or haematocrit level <20%Haemoglobin level <4g/dl OR ANDOR haematocrit level <12% State of shock (cold sweat + thready pulse + cold extremities + tachycardia)
Difficulty breathingBlood transfusion performedBlood transfusion requested

Questionnaire FEMHealth INDIVIDUAL
STUDY OF NEAR-MISSES AND MATERNAL AND NEONATAL DEATHS FORM
CERRHUD, Benin - AFRICSanté, Burkina Faso - CAREF, Mali - INAS, Maroc - LSHTM, UK Page 6/6
F NEONATAL NEAR-MISSAll newborns in a state of near-miss All non-trauma bleeding
Visible haematuria124. Is the newborn considered near-miss? Oui Non Anuria >24 hours
Apathy/poor tolerance of food125. Neonatal near-miss criteria Absominal distension AND vomiting
Respiratory rate >70/min Elongation of brachial plexus Cyanosis without assisted breathing Cranial fractureIrregular breathing gasping, suffocation, frequent apnea) Any intubationCardiac arrest Cardio-pulmonary resuscitationPersistent bradicardia <80bpm Use of vasoactive drugPeristent tachycardia >200bpm Volemic expansion/vascular filling/umbilical lineConvulsions Use of anticonvulsivantsSevere neurologic dysfunction (inability to suckle) Phototherapy in the first 24hrsJaundice visible in the first 24 hours Use of blood products
G OTHER QUALITY OF CARE INDICATORSAll women included in study sample All women with instrumental delivery
131. Was the position of the occiput determined?At admission Oui Non NSP126. Was arterial pressure measured? Oui Non NSP
132. Was the presentation engaged?All women with twins Pelvic floor
127. When was the diagnosis made? Mid-cavityBefore admission HigherUpon admission NoDuring delivery Unknown
All women with breech presentation: 133. How long did the active phase of labour last? (min)128. When was the diagnosis made? Unknown
Before admissionUpon admissionDuring delivery After delivery and before discharge
134. For the woman: in the 6 hours following delivery, werethe following signs measured at least once?
a) Pulse Oui NonTreatment and monitoring of parturient during delivery b) Arterial pressure Oui Non129. All women: c) Uterine bleeding Oui Non
Was the fœtal heart rate measured at least once d) Temperature Oui Nonduring the active (second) phase of labour?
N/A (stillbirth diagnosed Oui Non NSP 135. For the baby: in the 6 hours following delivery, were before delivery) the following signs measured at least once?
a) Colour Oui NonAll women admitted during latent or active phase: b) Breathing Oui Non
130. Was a partogramme used? c) Feeding Oui NonN/A (ex: expulsive phase) Oui Non NSP d) Temperature Oui Non
136. Return to labour room for revision of placental retention Oui Non
137. Is the final diagnosis the same as the one given at admission? Oui Non NSP
If yes, specify: ___________________________________









![Finale 2009 - [PC Score Revival.mus] · · 2016-12-16Hack, Punt, Tool Piano - Conductor & & &? ## ## ## ## ## j. # ...](https://static.fdocuments.net/doc/165x107/5ac599e07f8b9a2b5c8db6f9/finale-2009-pc-score-punt-tool-piano-conductor-j-.jpg)








