
Overview of MS and Strategies for Personalized Treatment Douglas S. Goodin, MD Professor of...
105
-
Upload
aleesha-berry -
Category
Documents
-
view
216 -
download
1
Transcript of Overview of MS and Strategies for Personalized Treatment Douglas S. Goodin, MD Professor of...
Overview of MS and Strategies for
Personalized Treatment
Douglas S. Goodin, MDProfessor of Neurology
Medical Director Multiple Sclerosis Center
University of California, San FranciscoSan Francisco, California
• Prevalence
– 1.0–1.5 per 1,000 population in the United States
– ~2.5 million cases worldwide
• Age at onset: 15–45 years
• 70%–75% of cases are women
• Increasing worldwide prevalence (especially in women)
• Ethnic origin: predominantly white, but does occur in other ethnicities as well
Multiple Sclerosis Epidemiology
Goodin DS. Epidemiology of MS. In: Handbook of Clinical Neurology. Philadelphia, PA: Elsevier; 2012. Compston A, et al. McAlpine’s Multiple Sclerosis. 4th ed. London, England: Churchill Livingstone; 2006.
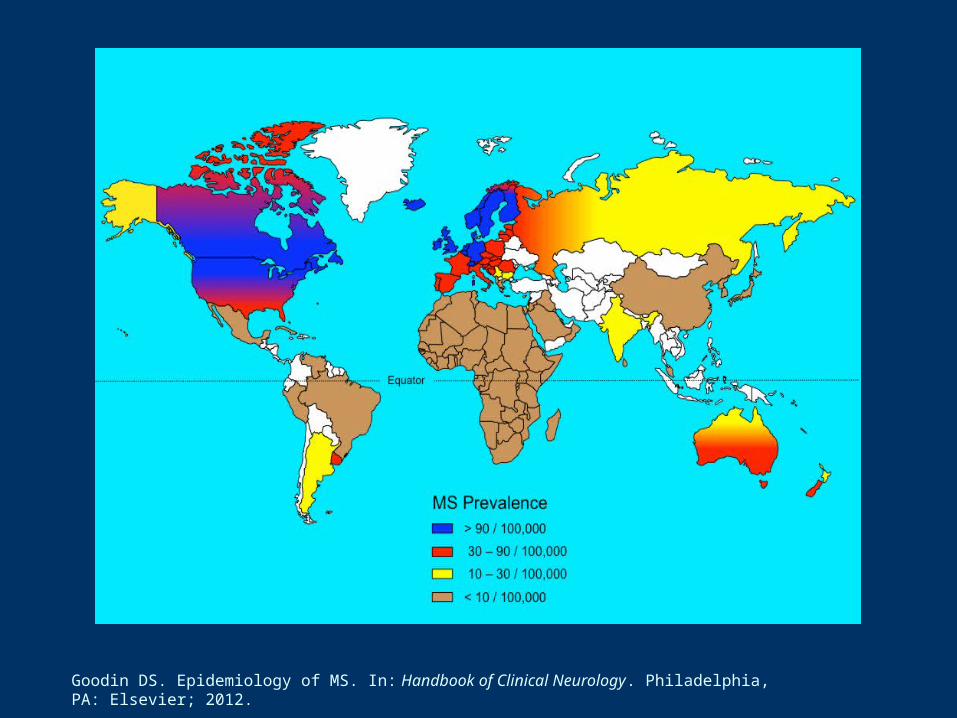
Goodin DS. Epidemiology of MS. In: Handbook of Clinical Neurology. Philadelphia, PA: Elsevier; 2012.
1. Goodin DS. PLoS One. 2009;4:e4565. 2. Goodin DS. Epidemiology of MS. In: Handbook of Clinical Neurology. Philadelphia, Pa: Elsevier; 2012. 3. Goodin DS. BMC Neurology. 2010;10:101. 4. Santon A, et al. Mult Scler. 2011;17:1295-1300. 5. Lucas RM, et al. Neurology. 2011;77:371-379. 6. Munger KL, et al. Neurology. 2004;62:60-65. 7. Handel AE, et al. PLoS One. 2011;6(1):e16149. 8. Hedström AK, et al. Mult Scler J. 2011;17:788-793.
Etiology of MS
• Genetics
– Increased risk in persons who have relatives with MS1-3
– 50–200 susceptibility alleles2,3
– Strongest association with HLA DRB1*15011-3
• Environmental factors, current hypotheses
– History of Epstein-Barr virus infection1,2,4,5
– Vitamin D deficiency1,2,6
– Smoking2 (active7 or passive8)
Pathophysiology of MS
• Acute inflammation demyelination/relapses– Blood-derived lymphocytes and monocytes– Breakdown of blood-brain barrier – Edema– White and grey matter lesions
Myelin injury, axonal transection
• Neurodegeneration irreversible disability– Neuronal loss– Brain atrophy
Trapp BD, et al. Annu Rev Neurosci. 2008;31:247-269.
Subtypes of MS
• Relapsing-remitting MS (RRMS)– Episodes of acute neurologic dysfunction (attacks) ± recovery– Stable disease between attacks– Initial diagnosis in ~85% of patients
• Primary-progressive MS (PPMS)– Steady functional decline from onset without attacks– ~10% of cases
• Secondary-progressive MS (SPMS)– Steady functional decline ± attacks; always follows RRMS– 50%–80% develop SPMS
• Progressive-relapsing MS (PRMS)– Steady functional decline from onset with occasional attacks – ~5% of cases
Lublin FD, Reingold SC. Neurology. 1996;46:907-911. Compston A, et al. McAlpine’s Multiple Sclerosis. 4th ed. London, England: Churchill Livingstone; 2006.

MS Symptoms
Common • Vision disturbances• Fatigue• Numbness• Incoordination • Gait impairment• Bladder/bowel
dysfunction• Dizziness and vertigo• Pain• Cognitive dysfunction• Depression• Spasticity
Less Common • Speech dysfunction• Swallowing difficulties• Hearing loss• Seizures• Respiratory impairment
Hauser SL, Goodin DS. Multiple sclerosis. In: Harrison’s Principles of Internal Medicine. New York, NY: McGraw-Hill; 2008:2611-2621.

Revised Diagnostic CriteriaMultiple Sclerosis
• Dissemination of lesions in space (DIS)
– ≥1 T2 lesion in ≥2 of 4 CNS areas: periventricular, juxtacortical, infratentorial, spinal cord*
• Dissemination of lesions in time (DIT)
– ≥2 clinical attacks, or 1 of the following MRI criteria
≥1 new T2 or gadolinium(Gd)-enhancing lesions not found on baseline scan, irrespective of timing of baseline scan
Simultaneous presence of asymptomatic Gd-enhancing and nonenhancing lesions
*If brain stem or spinal cord syndrome, the symptomatic lesions are excluded from criteria and do not count toward lesion count.
Polman CH, et al. Ann Neurol. 2011;69:292-302.

FDA-Approved Disease-Modifying Therapies
Drug Recommended Dose Indication
IFN beta-1b (2 brands)1,2 250 mcg SC q2d Relapsing MS, CIS
IFN beta-1a3 22 or 44 mcg SC TIW Relapsing MS
IFN beta-1a4 30 mcg IM weekly Relapsing MS, CIS
GA5 20 mg SC qd RRMS, CIS
Fingolimod6 0.5 mg orally qd Relapsing MS
Natalizumab7 300 mg IV over 1 h q4wk Relapsing MS
(nonresponders/intolerant to alternate therapy)
Mitoxantrone8 12 mg/m2 over 5–15 min IV q3mo
SPMS, PRMS, worsening RRMS
Abbreviations: CIS, clinically isolated syndrome; GA, glatiramer acetate; IFN, interferon; IM, intramuscular; IV, intravenous; SC, subcutaneous.
1. Betaseron [PI]. Montville, NJ: Bayer HealthCare Pharmaceuticals; 2010. 2. Extavia [PI]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2012. 3. Rebif [PI]. Rockland, MD: EMD Serono; 2011. 4. Avonex [PI]. Cambridge, MA: Biogen Idec; 2012. 5. Copaxone [PI]. Kansas City, MO: Teva Neuroscience; 2009. 6. Gilenya [PI]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2012. 7. Tysabri [PI]. Cambridge, MA: Biogen Idec; 2012. 8. Novantrone [PI]. Rockland, MD: EMD Serono; 2010.
Comparisons of Therapies

Short-Term Outcomes in MSEstablishing Efficacy in MS
Abbreviations: EDSS, Expanded Disability Status Scale; MSFC, Multiple Sclerosis Functional Composite.
• Outcome measures: disease activity
1. Clinical assessment (eg, attack rate or attack-free status)
2. Radiologic (MRI) assessment (eg, new T2, Gd+, or combined unique lesions)
• Outcome measures: disease severity
1. Clinical assessment (eg, confirmed EDSS progression or MSFC)
2. Radiologic (MRI) assessment (eg, T2 burden, T1 black holes, or atrophy)
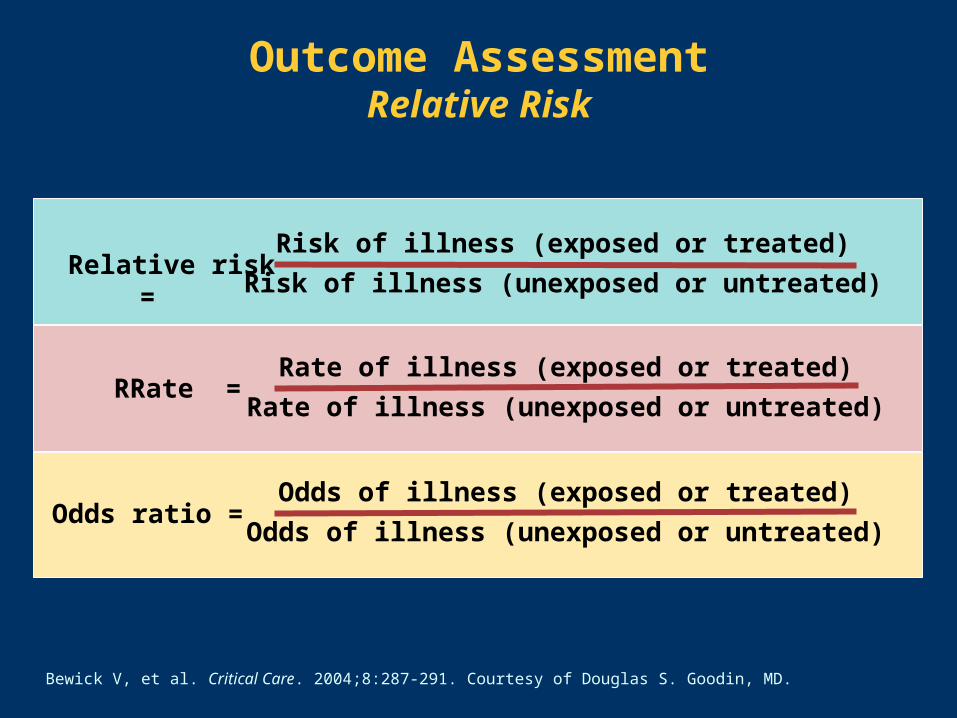
Bewick V, et al. Critical Care. 2004;8:287-291. Courtesy of Douglas S. Goodin, MD.
Risk of illness (exposed or treated)
Risk of illness (unexposed or untreated)Relative risk =
RRate = Rate of illness (exposed or treated)
Rate of illness (unexposed or untreated)
Odds ratio = Odds of illness (exposed or treated)
Odds of illness (unexposed or untreated)
Outcome AssessmentRelative Risk
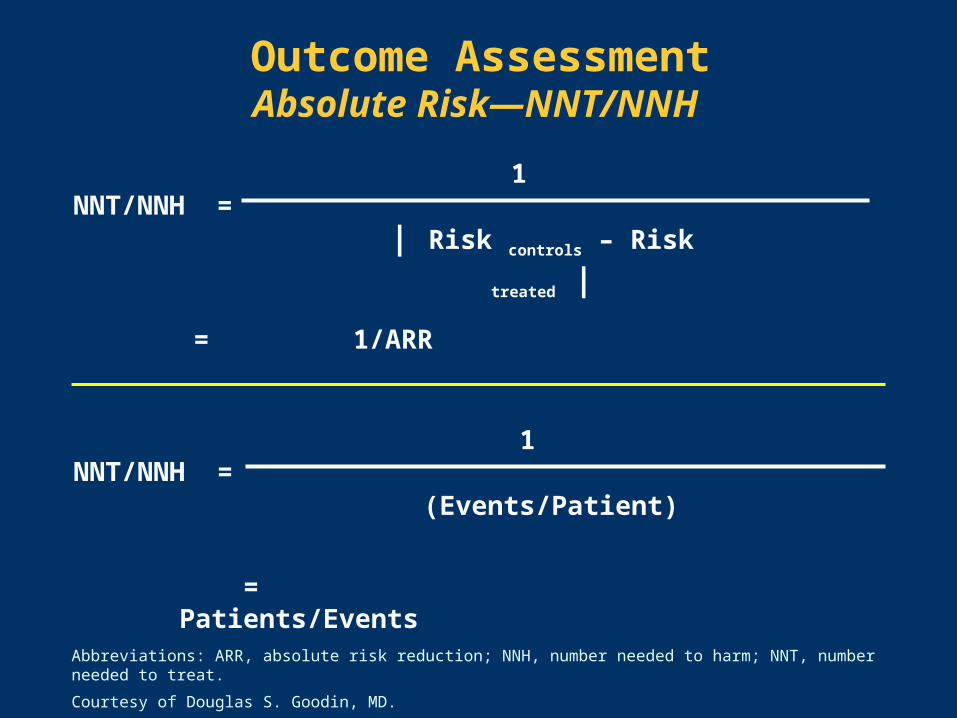
NNT/NNH = 1
(Events/Patient)
= Patients/Events
NNT/NNH = 1
| Risk controls – Risk treated |
= 1/ARR
Outcome AssessmentAbsolute Risk—NNT/NNH
Abbreviations: ARR, absolute risk reduction; NNH, number needed to harm; NNT, number needed to treat.
Courtesy of Douglas S. Goodin, MD.
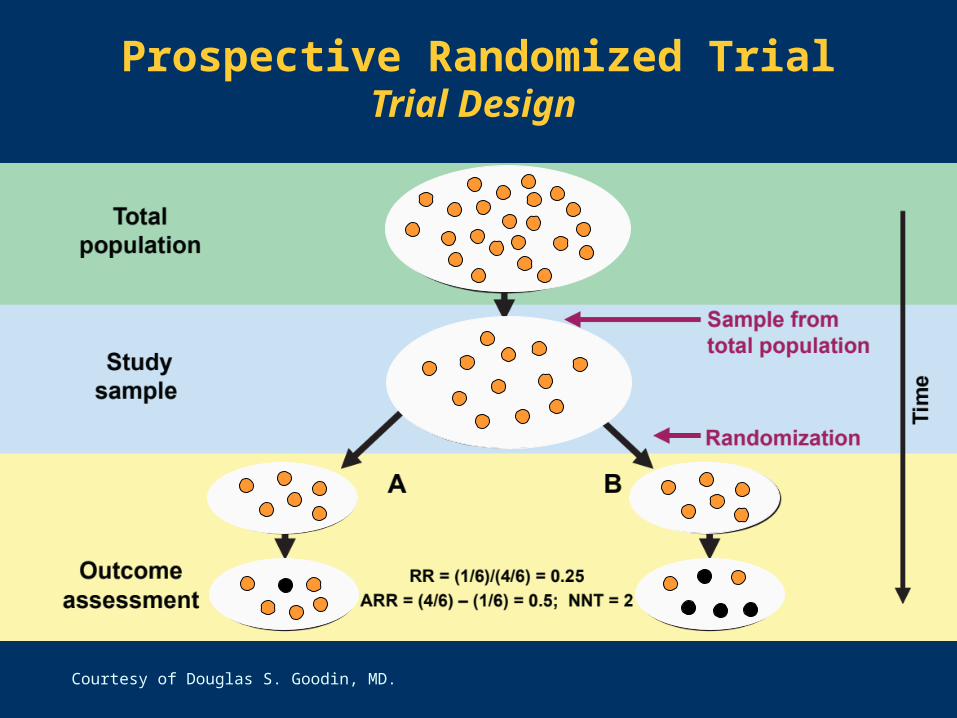
Prospective Randomized TrialTrial Design
Courtesy of Douglas S. Goodin, MD.

The Need for Head-to-Head Trials Relative Efficacy (RR)
GA 20 mg
qd
IFN beta-1a30 mcg IM qwk
IFN beta-1b, 250 mcgSC q2d
IFN beta-1a 44 mcg
TIW
Natalizumab300 mg/mo
Annualized relapse rate -29% -18% -34% -32% -68%
Relapse-free(2 years) +42% +36% +100% +36% +57%
3-month sustained progression (≥1 EDSS point)
-12% -37% -29% -30% -42%
New T2lesions -38% -36% -83% -78% -83%
Gd+ or CU lesions -33% -42% - -88% -92%
Goodin DS, et al. Neurology. 2008;71:766-773. Courtesy of Douglas S. Goodin, MD.

The Need for Head-to-Head Trials Absolute Efficacy (NNT and NNH)
GA 20 mg
qd
IFN beta-1a30 mcg IM
qwk
IFN beta-1b, 250 mcg SC
q2d
IFN beta-1a 44 mcg
TIW
Natalizumab300 mg/mo
Annualized relapse rate 4 7 2 2 2
Relapse-free(2 years) 15 9 7 6 4
Progression-free (%) 33 8 13 9 8
New T2lesions 0.17 1.3 0.34 0.3 0.11
Annualized rate of Gd+ lesions
0.09 1.4 - 0.11 0.91
Goodin DS, et al. Neurology. 2008;71:766-773. Courtesy of Douglas S. Goodin, MD.
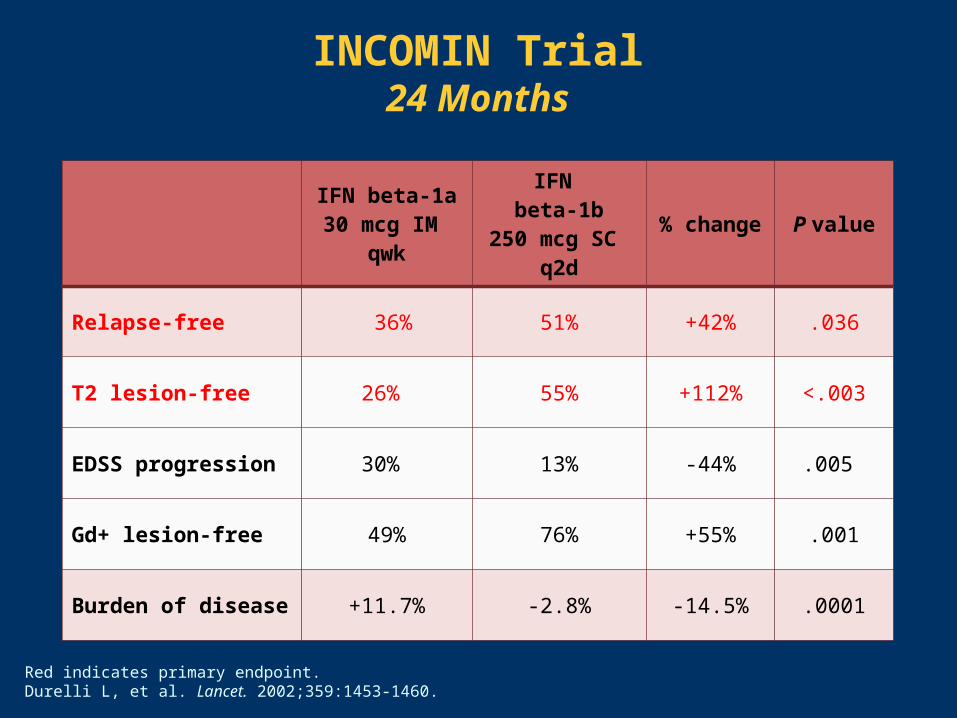
IFN beta-1a30 mcg IM
qwk
IFN beta-1b
250 mcg SC q2d
% change P value
Relapse-free 36% 51% +42% .036
T2 lesion-free 26% 55% +112% <.003
EDSS progression 30% 13% -44% .005
Gd+ lesion-free 49% 76% +55% .001
Burden of disease +11.7% -2.8% -14.5% .0001
INCOMIN Trial24 Months
Red indicates primary endpoint.Durelli L, et al. Lancet. 2002;359:1453-1460.
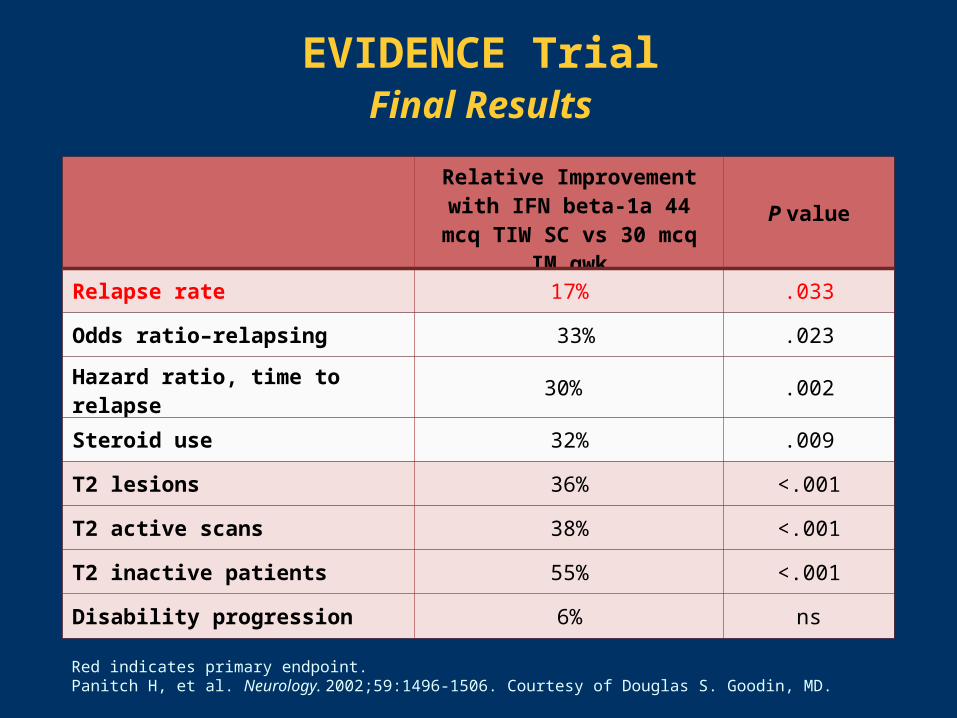
EVIDENCE TrialFinal Results
Red indicates primary endpoint.Panitch H, et al. Neurology. 2002;59:1496-1506. Courtesy of Douglas S. Goodin, MD.
Relative Improvement with IFN beta-1a 44 mcq TIW SC
vs 30 mcq IM qwkP value
Relapse rate 17% .033
Odds ratio–relapsing 33% .023
Hazard ratio, time to relapse 30% .002
Steroid use 32% .009
T2 lesions 36% <.001
T2 active scans 38% <.001
T2 inactive patients 55% <.001
Disability progression 6% ns

REGARD TrialFinal Results
IFN beta-1a 44 mcg SC TIW (n = 386)
GA 20 mg/d (n = 378) P value
Time to first relapse (30th percentile) 495 d 432 d ns
Patients free from relapse 62% 62% ns
Annualized relapse rate 0.30 0.29 ns
T2 active lesions 0.67 0.82 ns
Gd-enhancing lesions 0.24 0.41 .0002
CU lesions 0.91 1.22 .010
New T1 hypointense lesions 0.23 0.24 ns
Brain volume change -1.240 -1.073 .018
MRI measures reported as lesions per patient per scan. Red indicates primary endpoint.ns = not significant Mikol DD, et al. Lancet Neurol. 2008;7:903-914.

BEYOND TrialFinal Results
Red indicates primary endpoint.
O’Connor P, et al. Lancet Neurol. 2009;8:889-897.
Endpoint BEYOND P Values
IFN beta-1b250 mcg(n = 897)
GA(n = 448)
Relapse risk ns
Relapse rate 0.36 0.34 ns
Progression-free 89% 80% ns
New/Enlarging T2 Lesions 3.3 4.6 0.011
Gd+ Enhancing 0.9 1.2 ns
Change in Brain Volume -0.65% -0.61% ns
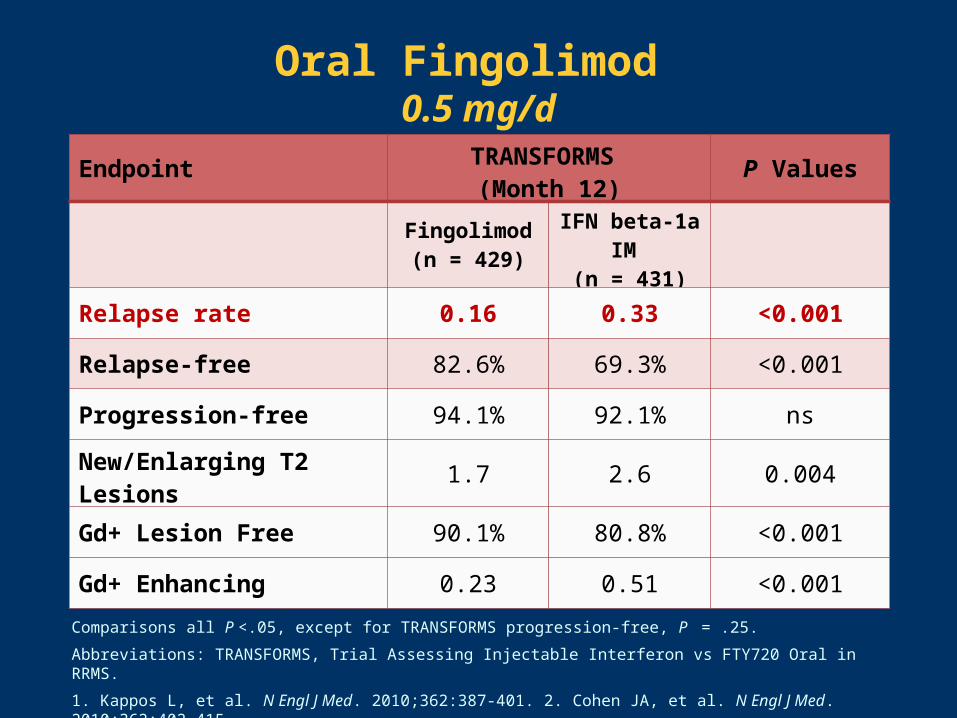
Oral Fingolimod 0.5 mg/d
Comparisons all P <.05, except for TRANSFORMS progression-free, P = .25.
Abbreviations: TRANSFORMS, Trial Assessing Injectable Interferon vs FTY720 Oral in RRMS.
1. Kappos L, et al. N Engl J Med. 2010;362:387-401. 2. Cohen JA, et al. N Engl J Med. 2010;362:402-415.
EndpointTRANSFORMS
(Month 12)P Values
Fingolimod(n = 429)
IFN beta-1a IM
(n = 431)
Relapse rate 0.16 0.33 <0.001
Relapse-free 82.6% 69.3% <0.001
Progression-free 94.1% 92.1% ns
New/Enlarging T2 Lesions 1.7 2.6 0.004
Gd+ Lesion Free 90.1% 80.8% <0.001
Gd+ Enhancing 0.23 0.51 <0.001
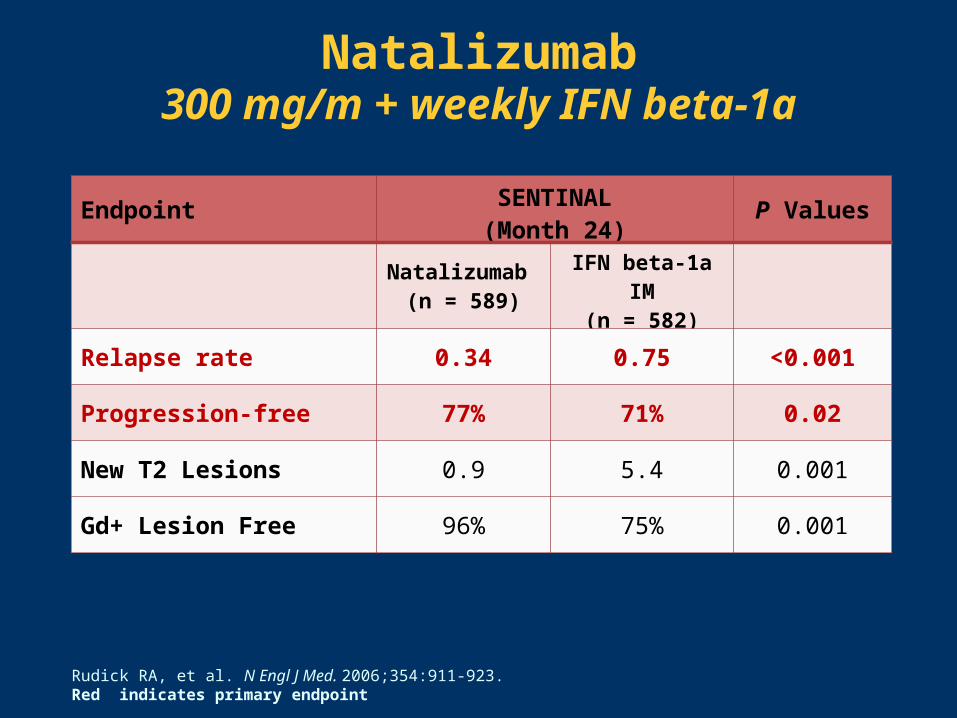
Natalizumab300 mg/m + weekly IFN beta-1a
Rudick RA, et al. N Engl J Med. 2006;354:911-923. Red indicates primary endpoint
EndpointSENTINAL(Month 24)
P Values
Natalizumab (n = 589)
IFN beta-1a IM(n = 582)
Relapse rate 0.34 0.75 <0.001
Progression-free 77% 71% 0.02
New T2 Lesions 0.9 5.4 0.001
Gd+ Lesion Free 96% 75% 0.001
The Value of Early Treatment

Disability threshold
RR to SP
IFN beta-1a SPMS
RRMS SPMS time
NA-SPMSIFN beta-1b
Mono-symptomatic MS Axonal loss
Disease stage
Potential therapeutic benefit of DMTs
RRMS
Natalizumab Fingolimod
IFN beta-1a GA
IFN beta-1bTh
era
pe
uti
c B
en
efi
tDisease-Modifying MS Therapies Disease Stage and Therapeutic Effects
Abbreviation: NA-SPMS, North American Secondary-Progressive MS Trial. Courtesy of Douglas S. Goodin, MD.
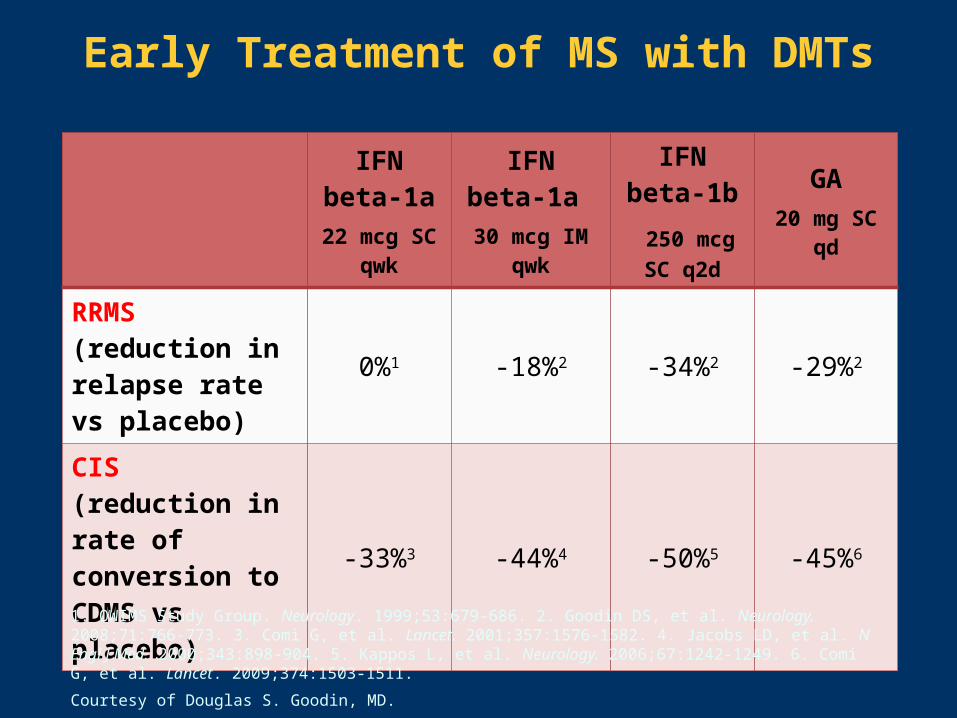
IFN beta-1a
22 mcg SC qwk
IFN beta-1a
30 mcg IM qwk
IFN beta-1b
250 mcg SC q2d
GA20 mg SC
qd
RRMS (reduction in relapse rate vs placebo)
0%1 -18%2 -34%2 -29%2
CIS(reduction in rate of conversion to CDMS vs placebo)
-33%3 -44%4 -50%5 -45%6
1. OWIMS Study Group. Neurology. 1999;53:679-686. 2. Goodin DS, et al. Neurology. 2008;71:766-773. 3. Comi G, et al. Lancet. 2001;357:1576-1582. 4. Jacobs LD, et al. N Engl J Med. 2000;343:898-904. 5. Kappos L, et al. Neurology. 2006;67:1242-1249. 6. Comi G, et al. Lancet. 2009;374:1503-1511.
Courtesy of Douglas S. Goodin, MD.
Early Treatment of MS with DMTs
Long-Term Treatment Outcomes

Propensity-Adjusted Cox PH ModelHigh Exposure to IFN beta-1b
Goodin DS, et al. PLoS One. 2011;6:e22444.

Regular medical care
RCT complete
IFN beta-1b 250 mcg q2d
IFN beta-1b 50 mcg q2d
Placebo
1988 1993 2005 2006 2009 2010
21-year LTF
IFN beta-1b 21-Year Long-Term Follow-UpStudy Design
Vital status of 366 (98.4%) of 372 original RCT participants was identified after 21 years
Abbreviations: LTF, long-term follow-up; RCT, randomized controlled trial.
Goodin DS, et al. Neurology. 2012;78:1315-1322. Courtesy of Douglas S. Goodin, MD.
Randomized trial (N = 372)
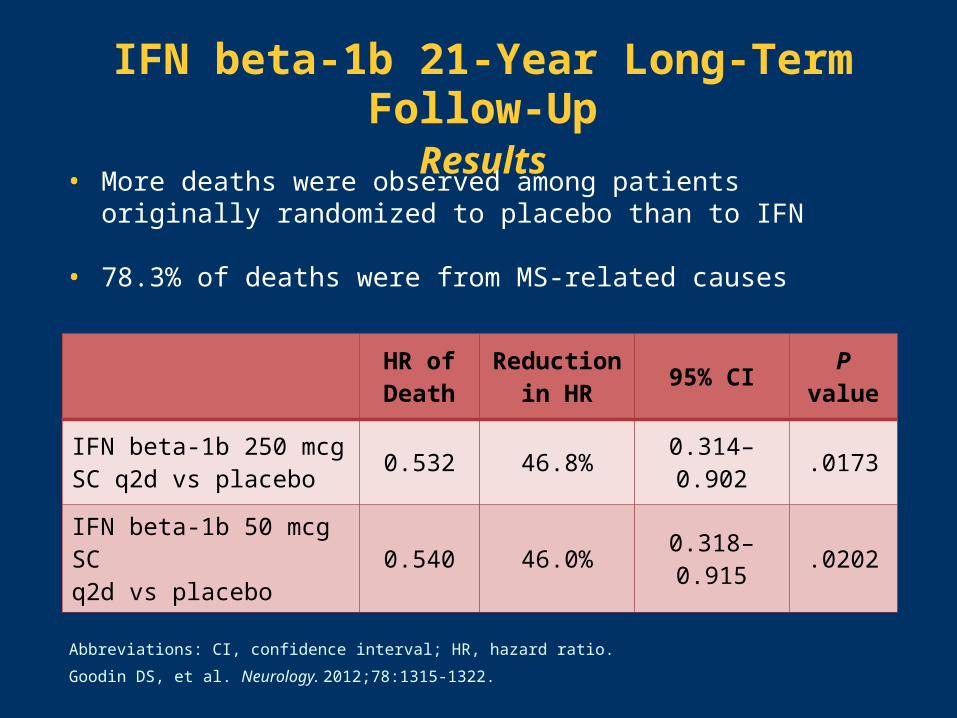
IFN beta-1b 21-Year Long-Term Follow-UpResults
HR of Death
Reduction in HR
95% CI P value
IFN beta-1b 250 mcg SC q2d vs placebo
0.532 46.8% 0.314–0.902 .0173
IFN beta-1b 50 mcg SC q2d vs placebo
0.540 46.0% 0.318–0.915 .0202
Abbreviations: CI, confidence interval; HR, hazard ratio.
Goodin DS, et al. Neurology. 2012;78:1315-1322.
• More deaths were observed among patients originally randomized to placebo than to IFN
• 78.3% of deaths were from MS-related causes

Long-Term Follow-Up in RRMS Glatiramer Acetate
• 15-year open-label extension of 2-year phase III trial1
− Relapses reduced to ~1 every 4 years compared with 1.12 every year at open-label entry
− 57% had improved or stable EDSS scores
− 65% had not progressed to SPMS
• Mean 5.8-year follow-up of open-label extension of 18-month trial2
− Patients taking glatiramer acetate at study onset less likely to need walking aids vs those starting active treatment at extension entry (P = .034)
1. Ford C, et al. Mult Scler. 2010;16:342-350. 2. Rovaris M, et al. Mult Scler. 2007;13:502-508.
Impact of DMTs on Cognitive Impairment
• Likelihood of cognitive impairment was reduced with
– Early vs delayed IFN beta-1b SC initiation in CIS1
– Higher-dose IFN beta-1a SC in RRMS2
• IFN beta-1a IM in relapsing MS improved information processing and learning/recent memory3
• Cognitive function was preserved in most patients taking glatiramer acetate during 10-year open-label follow-up4
1. Kappos L, et al. Lancet. 2007;370:389-397. 2. Patti F, et al. Mult Scler. 2010;16:68-77. 3. Fischer JS, et al. Ann Neurol. 2000;48:885-892. 4. Schwid SR, et al. J Neurol Sci. 2007;255:57-63.
Safety and Tolerability
Safety of Interferons
• Side effects: Flu-like symptoms, injection-site reactions, hepatotoxicity (hepatic enzyme elevations), leukopenia, depression (?), headache, thyroid dysfunction
• Pregnancy: Category C
• Laboratory tests: Periodic CBC with differential, liver function tests, thyroid function tests
Abbreviation: CBC, complete blood count.
Betaseron [PI]. Montville, NJ: Bayer HealthCare Pharmaceuticals; 2010. Extavia [PI]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2012. Rebif [PI]. Rockland, MD: EMD Serono; 2011. Avonex [PI]. Cambridge, MA: Biogen Idec; 2012.
Safety of Glatiramer Acetate
• Side effects
– Injection-site reactions, lipoatrophy
– Immediate postinjection reaction (flushing, chest pain, palpitations, anxiety, shortness of breath)
Self-limited; usually nonrecurrent; no treatment required
• Pregnancy: Category B
• Laboratory tests: None required
Copaxone [PI]. Kansas City, MO: Teva Neuroscience; 2009.
Safety of Fingolimod
• Side effects: Headache, liver enzyme elevations, bradycardia, atrioventricular block, severe lymphopenia, macular edema
• Pregnancy: Category C
• Drug interactions: QT prolonging drugs, beta-blockers
• Laboratory tests: CBC with differential, liver enzymes
– At least 6 hours of cardiovascular observation after 1st dose, with hourly pulse and blood pressure measurement for all patients
– EKG obtained prior to 1st dose and at end of observation period
– Cardiovascular monitoring should be extended past 6 hours in patients at higher risk of bradycardia and should include continuous overnight EKG monitoring
FDA Drug Safety Communication. May 14, 2012. Accessed 5/14/12 at:http://www.fda.gov/Drugs/DrugSafety/ucm303192.htm.
Safety of Natalizumab
• Side effects: Hypersensitivity reactions, fatigue, diarrhea, infections
– PML/IRIS
• Pregnancy: Category C
• Lab tests: JC virus antibody testing prior to/during treatment; antibody testing if persistent antibodies suspected
Abbreviations: IRIS, immune reconstitution inflammatory syndrome; PML, progressive multifocal leukoencephalopathy.
Tysabri [PI]. Cambridge, MA: Biogen Idec; 2012.

NatalizumabPML Risk Factors
• Duration of use1
− 1–12 months: 0.04 cases/1000 patients
− 13–24 months: 0.56 cases/1000 patients
− 25–36 months: 1.93 cases/1000 patients
− 37–48 months: 1.99 cases/1000 patients
• JC virus antibodies (JCV Ab) present in ~55%1
– FDA-approved screening test now available2
– 54 cases with samples all JCV Ab positive prior to PML1
– 3.80–3.87 cases per 1000 patients if JCV Ab positive1
– ≤0.09 cases per 1000 patients if JCV Ab negative1
• Prior immunosuppressive therapy1
− 34.5% in PML vs 20.3%–23.5% in all natalizumab users) • Risk is further increased if multiple risk factors1
1. Bloomgren G, et al. N Engl J Med. 2012;366:1870-1880. 2. Stratify JCV [PI]. Cypress, CA: Focus Diagnostics; 2011.
Natalizumab & IRIS
• IRIS follows PML; in most cases after PE1
– Due to rapid restoration of immune function after NTZ clearance2
• Typical PML Sx; days to weeks after PE; may require ICU care3
• Corticosteroids: Strike balance between adequate immunosuppression while maintaining effective immune response against JC virus4
– Methylprednisolone 1 g/d IV for 5 days followed by oral steroids; repeated courses may be necessary3
– In case studies, corticosteroids reduced IRIS and improved EDSS scores in most patients, compared with several deaths3 and worse EDSS scores in patients whose IRIS was untreated5
1. Tysabri [PI]. Cambridge, MA: Biogen Idec; 2012. 2. Carson KR, et al. Lancet Oncol. 2009;10:816-824. 3. Clifford DB, et al. Lancet Neurol. 2010;9:438-446. 4. Berger JR. Neurology. 2009;72:1454-1455. 5. Tan IL, et al. Neurology. 2011;77:1061-1067.
Emerging Disease-Modifying Therapies

Emerging Disease-Modifying Therapies
Small Molecules
• BAF312
• Dimethyl fumarate (BG-12)
• Laquinimod
• ONO-4641
• Teriflunomide
Monoclonal Antibodies
• Alemtuzumab
• Daclizumab
• Ocrelizumab and ofatumumab
Conclusions
• Early treatment more effective than late– Reduction in relapses, disability progression, MRI– Better long-term outcome (physical and cognitive)
• Recent studies of long-term follow-up show– Improved survival/reduced MS-related mortality– Good safety track record (GA, IFN)
• Natalizumab has serious adverse events and requires careful monitoring
• Fingolimod is probably safe but requires careful monitoring
• Mitoxantrone– Rarely used due to serious adverse events
• More options expected in the near future
Partnering with Patients to Improve Adherence in MS
Amy Perrin Ross, MSNNeuroscience Program Coordinator
Department of Neurosciences
Loyola University Chicago
Maywood, Illinois
Goals of Treatment with Disease-Modifying Therapy
• Reduce frequency and severity of relapses
• Reduce new/enhancing lesions on MRI
• Delay disability progression
• Increase overall quality of life and function
• Provide therapy that is well tolerated and safe– Acceptable benefit vs risk
A wellness philosophy is the focal point of comprehensive care
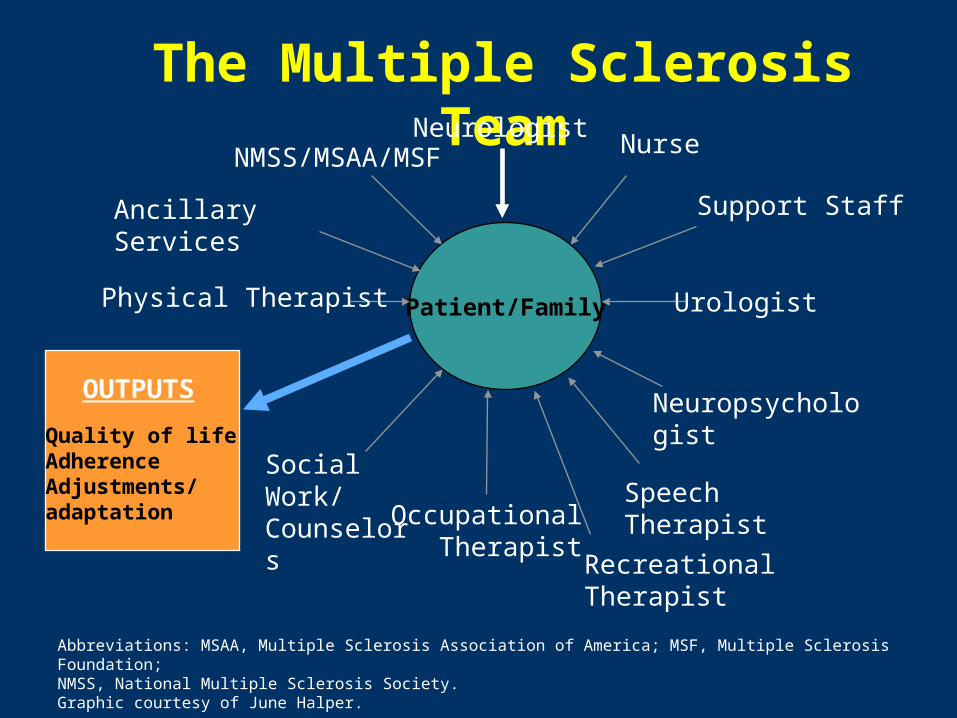
The Multiple Sclerosis Team
OUTPUTS
Quality of lifeAdherenceAdjustments/adaptation
Patient/Family
NeurologistNurse
Urologist
Neuropsychologist
Speech TherapistOccupational Therapist
Social Work/Counselors
Physical Therapist
NMSS/MSAA/MSF
Ancillary Services Support Staff
Recreational Therapist
Abbreviations: MSAA, Multiple Sclerosis Association of America; MSF, Multiple Sclerosis Foundation; NMSS, National Multiple Sclerosis Society. Graphic courtesy of June Halper.
Choosing the Right Treatment for the Individual Patient with MS
Initiation of treatment
• Which disease-modifying therapy will fit anindividual patient?
• 1st-line medications vs 2nd-line
• Ability to self-inject – SQ/IM vs oral/IV
• Lifestyle issues
• Career/family roles
• Planning pregnancy
• Planning trip? Vaccines
Decision Making
• Discussion of pros and cons with patients
• Partnership with patients and families
• Possible use of consent form/contract
• Future plans and therapies
• Long-term effects of certain medications
• Combination of therapies
• Safety of medications
• Pregnancy
Adherence vs Compliance
• Compliance implies giving in to a request, wish, or demand; it implies a subordinate position to healthcare professionals
Versus
• Adherence is voluntary, active collaborative involvement of the patient in a mutually acceptable course of behavior leading to a desired outcome
Adherence to Therapy
Although it is felt to be important• Adherence is difficult
– Nonadherence estimates are about 50%–70%; this is true for many chronic diseases
• Many reasons offered as to why– Perception that drug is not working
– Continued MS symptoms
– Side effects
– Insurance coverage
Barriers to Adherence
• Lifestyle issues
• Cultural considerations and healthcare literacy
• Fear of injections
• Concerns about adverse effects, including injection site reactions that can affect lifestyles
• Perceived benefits
• Lack of an effective support system
• Depression
• Cost

Barriers to Adherence
• Progression of disease – hopelessness
• Physical impairments – visual disturbances, tremor, weakness
• Absence of symptoms
• Fatigue – too tired to inject

Uncover Injection Barriers
• What is your schedule for injections?
• How many injection sites/areas do you use in 1 week?
• How many injections did you miss in the past month?
• What were your reasons for missing these injections? Was it because of site reactions, etc?
• Can you show me the last 3 sites you injected?
• If needed, would you ask for help with your injections?
Uncover Oral/IV Barriers
• What is your schedule for taking pills?
• How many pills did you miss in the past month?
• Have you had your follow-up monitoring done?
• Do you have trouble with IV access?
• Do you have storage/transportation issues?
Promoting Adherence
• Educate
• Identify and address barriers
• Develop individualized strategies
• Encourage realistic expectations
• Advocate– Assist with reimbursement
– Identify resources
– Involve family and support system
Fostering Realistic Expectations
• For MS patients, realistic expectations are critical to the success of long-term disease management
• Inform patients that disease-modifying therapies are not curative but that they can:
– Reduce the rate and frequency of relapses
– Slow the progression of the disease
Having relapses while on treatment does not mean therapy is ineffective; conversely, the lack of relapses when not on treatment does not mean disease is not progressing
– Improve quality of life
Fostering Realistic ExpectationsRisk of Not Treating/Delaying Treatment
• Compared with no treatment, treatment with disease-modifying therapy (IFN B-1a, IFN B-1b, or glatiramer acetate)– Significantly delays the onset of clinically definite MS1,2,3,4
– Significantly reduces annualized relapse rates4
– Significantly reduces loss of brain volume1
– Significantly reduces the number of new or enlarging lesions and gadolinium-enhancing lesions1,4
1. Jacobs LD, et al. N Engl J Med. 2000;343:898-904. 2. Kappos L, et al. Lancet. 2007;370:389-397. 3.Comi G, et al. Lancet. 2009;374:1503-1511. 4. Comi G, et al. Lancet. 2001;357:1576-1582.
Fostering Realistic ExpectationsRisk of Not Treating/Delaying Treatment
Early vs delayed treatment– Patients receiving early treatment had a significantly
reduced risk of progression of disability
– Patients receiving early treatment performed significantly better on tests of cognitive function than those receiving delayed treatment
Kappos L, et al. Lancet. 2007;370:389-397.
Provide Balanced Information
• Present balanced information about disease-modifying therapies; include pivotal trial data, mechanism of action, potential adverse effects
• Refer to:
– National Multiple Sclerosis Society
– Multiple Sclerosis Association of America
– Multiple Sclerosis Foundation
– Consortium of Multiple Sclerosis Centers
• Direct patients to appropriate websites and provide information kits if available
• Teach patients to critically evaluate MS educational materials

Strategies to Address Barriers
• Medication specifics– Develop realistic expectations
– Discuss dosing and consistent administration
– Provide tips to minimize side effects, including injection site reactions (eg, medications prior to injection, site rotation, lifestyle, and site of injection)
– Address side effects
• Patient/caregiver issues– Identify information gaps, provide education
– Assess patient’s financial status and support wherever possible with resources
Management of Injectable Side Effects
• Warm mixed medications to room or body temperature
• Warm or ice site for 30–60 seconds before injection
• Inject immediately after a shower
• Use aerosolized ethyl chloride
• Apply local anesthetics (lidocaine, benzocaine, etc)
• For flu-like symptoms, ibuprofen and acetaminophen can be recommended
Injection Mechanics
• Consider autoinjectors
• Modify needle length for body mass index
• Avoid medication on needle tip
• Fully penetrate the skin to avoid intradermal infiltration
• Ensure complete vertical needle penetration intoskin surface
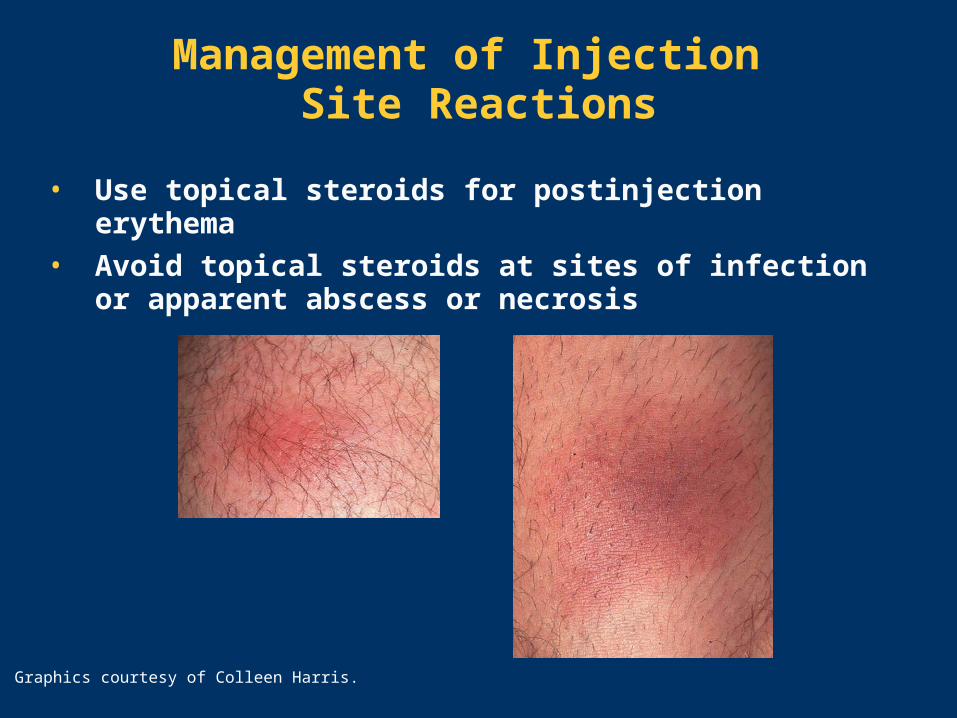
Management of Injection Site Reactions
• Use topical steroids for postinjection erythema
• Avoid topical steroids at sites of infection or apparent abscess or necrosis
Graphics courtesy of Colleen Harris.

To Be Successful, a Patient…
• Must be ready to begin therapy
• Must believe that therapies can makea difference
• Must be willing to make a commitment
• Must be well educated– Regarding MS
– Regarding therapies for MS
Who Can Help?• Neurologists• Nursing staff• Company-sponsored support• Multiple Sclerosis Association of America (MSAA)
– www.msassociation.org
• National Multiple Sclerosis Society (NMSS)– www.nationalmssociety.org
• Multiple Sclerosis Foundation (MSF) – www.msfocus.org
• Consortium of Multiple Sclerosis Centers– www.mscare.org
General Advice for Motivating Patients
• MS is lifelong; therapy is a lifelong commitment
• Take good care of yourself: a wellness approach– Rest
– Eat well
– Exercise
– Reduce stress
• Find a strong support network that includes other people with MS
• Find and develop a positive relationship with a healthcare provider whom you trust and respect
Dimensions of Wellness
Wellness
Environmental
Healthy setting Self-protection
PhysicalNutrition Fitness Lifestyle
habits
SocialRespect
Relationships Intimacy Tolerance
EmotionalStress management
Acceptance Expression of
feelings
Spiritual Life meaning
Purpose Values
IntellectualLearning Growth
New challenges
Anspaugh D, et al. Wellness: Concepts and Applications. New York: McGraw-Hill; 2008.
The Ultimate Goals in MS Treatment
• Prevent accumulation of disability
• Prevent relapses
• Improve quality of life—short- and long-term
• Develop convenient, effective, safe and tolerable treatments
• Repair damage and restore function• Promote realistic hope

Translating Science intoPractice: Case Studies
Patricia K. Coyle, MD
Acting Chair, Department of NeurologyDirector, MS Comprehensive Care CenterStony Brook UniversityStony Brook, New York
Case 1 18-Year-Old White Female
History
• Patient presented with monocular vision loss over 2 days, with right eye pain
• She has no prior medical history
• Exam showed diminished right eye vision (20/70), red color desaturation, central scotoma, and afferent pupil
• Brain/orbit MRI showed enhancement of the right optic nerve only
• Diagnosis is retrobulbar optic neuritis
Decision Point 1
Which best describes your diagnostic assessment?
a. Clinically isolated syndrome (CIS) at low risk for multiple sclerosis (MS)
b. CIS at high risk for MS
c. Definite MS
Decision Point 2
Would you encourage this patient to start disease-modifying therapy for MS?
a. Yes
b. No

Additional Nonenhancing Lesions
Suppose the brain MRI, in addition to enhancement of the optic nerve, showed 2 nonenhancing lesions: a 5-mm juxtacortical lesion and a 4-mm periventricular lesion?
Decision Point 3
What is your diagnostic assessment now?
a. CIS at low risk for MS
b. CIS at high risk for MS
c. Definite MS
Decision Point 4
Would you encourage the patient to start disease-modifying therapy?
a. Yes
b. No
Additional Enhancing Lesions
Suppose the brain MRI, in addition to enhancement of the optic nerve, showed 2 lesions, 1 of which enhanced: a 5-mm enhancing juxtacortical lesion and a 4-mm periventricular lesion?
Decision Point 5
What is your diagnostic assessment?
a. CIS at low risk for MS
b. CIS at high risk for MS
c. Definite MS
Decision Point 6
What would be your choice of treatment?
a. IFN beta-1a
b. IFN beta-1b
c. Glatiramer acetate
d. Natalizumab
e. Fingolimod
Case 228-Year-Old Lawyer
History
• Patient was diagnosed with relapsing-remitting MS following 2 attacks over 14 months
• Her exam is normal
• She feels well, believes she has benign disease, and is ambivalent about going on anything that can harm her body
• You counsel her about MS, the damage process, and the benefits of disease-modifying therapy
• You then discuss individual agents

Interferon Beta Counseling
• Adverse reactions include flu-like symptoms, injection reactions, headache/depression
• Monitoring includes liver function tests, thyroid, complete blood count and differential
• Therapy initiation involves dose escalation, pre-medication, and possible early evening dosing
• Blood tests are required every 3 months for 1 year, then every 6 months for higher-dosed interferon beta
Glatiramer Acetate Counseling
• Adverse reactions involve injection site reactions, systemic immediate postinjection reaction
• No routine blood testing is required
Natalizumab Counseling
• Associated with the risk of a potentially fatal adverse event (ie, progressive multifocal leukoencephalopathy)– Risk stratification (JC virus antibodies, duration of therapy,
prior immunosuppression)
• Monitoring includes liver function test, neutralizing antibodies at 6 months
Fingolimod Counseling
• Prescreen patients for exclusion criteria, macular edema, complete blood count and differential, liver function tests (LFTs), IgG/M to VZV, electrocardiogram (EKG)
• 6-hour initiation dose monitoring with EKG pre and post
• Repeat ophthalmologic screen, liver function tests at 4 months
Decision Point
What would be your treatment choice for this
patient?
a. IFN beta-1a
b. IFN beta-1b
c. Glatiramir acetate
d. Natalizumab
e. Fingolimod
Follow-Up Strategy
• Regular visits– Every 3–4 months on initiation or change in disease-
modifying therapy (for 1 year)
– Every 6–12 months when stable
• Surveillance brain MRI with contrast– At 12 months (6 months if high concern)
– Annually for the early course, then at the discretion of patient/physician
Suspected Relapse
• Clarify symptoms and time course
• Assess adherence
• Document objective changes
• Rule out pseudorelapse
• Consider whether you want MRI
• Discuss acute management
• Consider disease-modifying thrapy implications
General Counseling
• Stress adherence
• Continue close follow-up and reassessments (clinical, MRI)
• Advise patients to notify of any significant changes – Patients often bring up changes months after they occur
• Let patients know that current expected attack rate 1 every 3–5+ years
Case 342-Year-Old Female
History
• This 42-year-old relapsing-remitting patient has been on therapy with glatiramer acetate for 8 years
• She has now had her 1st relapse on therapy
• The relapse involved right leg hypesthesia, with complete recovery

Decision Point 1
Would you change disease-modifying therapy?
a. Yes
b. No
Paraparesis with Incomplete Recovery
Suppose the relapse involved paraparesis with gait ataxia, with incomplete recovery?
Decision Point 2
Would you change disease-modifying therapy?
a. Yes
b. No
Hypesthesia and New Lesions
• Suppose the relapse involved hypesthesia with complete recovery?
• Brain MRI showed 4 contrast lesions, and 10 new lesions from her last MRI a year ago
Decision Point 3
Would you change disease-modifying therapy?
a. Yes
b. No
Paraparesis and Stable MRI
Suppose the relapse involved paraparesis with gait ataxia, with incomplete recovery, and stable MRI?
Decision Point 4
Would you change disease-modifying therapy?
a. Yes
b. No

Switching Disease-Modifying Therapy
Suppose the patient was JC virus antibody negative?
Decision Point 5
What would you recommend?
a. Maintain current therapy
b. Switch to interferon beta
c. Switch to fingolimod
d. Switch to natalizumab
e. Other

Patient Outcomes
• Patient was started on IV natalizumab
• She does well, feels stronger, and experiencesno relapses
• Brain MRI is completely stable, with noenhancing lesions
• JC virus antibody is tested every 6 months
• She continues to do well at 3 years on therapy
JC Virus Antibody Positive
Suppose the patient was JC virus antibody positive?
Decision Point 6
What therapy would you recommend?
a. Interferon beta
b. Fingolimod
c. Natalizumab
d. Other
Patient Outcomes
• Patient was started on fingolimod
• Total lymphocyte level is below normal limits
• Since there is no infection issue, she remainson therapy
• There is no evidence of macular edema at 4 months
• Brain MRI is stable at 6 and 12 months
• She continues to do well on fingolimod at 24 months on therapy


















