Overview of liver transplantation
56
OVERVIEW OF OVERVIEW OF LIVER LIVER TRANSPLANTATIO TRANSPLANTATIO N N Dr. Harshal Rajekar Dr. Harshal Rajekar
-
Upload
hr77 -
Category
Health & Medicine
-
view
162 -
download
4
description
liver transplantation
Transcript of Overview of liver transplantation

OVERVIEW OF OVERVIEW OF LIVER LIVER
TRANSPLANTATITRANSPLANTATIONON
Dr. Harshal RajekarDr. Harshal Rajekar

Cirrhosis – HCV relatedCirrhosis – HCV related

Cirrhosis- Cirrhosis- HemochromatosisHemochromatosis
Cirrhosis – Alcohol Cirrhosis – Alcohol inducedinduced

Liver Transplantation HistoryLiver Transplantation History
• • 1958 Research programs on liver 1958 Research programs on liver replacement at Northwestern and replacement at Northwestern and HarvardHarvard
• • 1963 First liver transplant (Univ. of CO)1963 First liver transplant (Univ. of CO)
• • 1967 First long survival1967 First long survival
• • 1979 Cyclosporine1979 Cyclosporine
• • 1987 Univ. of WI solution for improved 1987 Univ. of WI solution for improved organ preservationorgan preservation
• • 1989 FK 5061989 FK 506
• • 1999 Living donor liver transplantation1999 Living donor liver transplantation

Liver TransplantationLiver Transplantation
Liver transplantation is the OPTIMAL Liver transplantation is the OPTIMAL treatment for end stage liver disease treatment for end stage liver disease (ESLD)(ESLD)
ESLD has 2 forms: Acute and ChronicESLD has 2 forms: Acute and Chronic
- Acute = Fulminant Hepatic Failure- Acute = Fulminant Hepatic Failure
- Chronic = Cirrhosis- Chronic = Cirrhosis

Fulminant Hepatic Failure Fulminant Hepatic Failure (FHF)(FHF)
Synonymous with Acute Liver FailureSynonymous with Acute Liver Failure Definition: Development of Definition: Development of
encephalopathy within about 8 weeks encephalopathy within about 8 weeks of the onset of symptoms or within of the onset of symptoms or within about 2 weeks of the onset of jaundiceabout 2 weeks of the onset of jaundice
Pathology: Pan-lobular or Sub-massive Pathology: Pan-lobular or Sub-massive necrosisnecrosis
Classically seen in Paracetamol Classically seen in Paracetamol poisoning. In India – commonest cause poisoning. In India – commonest cause is HEV, HAV and drug induced.is HEV, HAV and drug induced.

Criteria for transplantation of acute Criteria for transplantation of acute liver failureliver failure
KING’S COLLEGE CRITERIAKING’S COLLEGE CRITERIA• • Acetaminophen toxicityAcetaminophen toxicity
ph < 7.30 (after hydration and regardless of degree of encephalopathy)ph < 7.30 (after hydration and regardless of degree of encephalopathy)oror
INR >6.5INR >6.5creatinine >3mg/dlcreatinine >3mg/dl
Encephalopathy III-IVEncephalopathy III-IV• • Non-acetaminophen etiologyNon-acetaminophen etiology
••INR >6.5 irrespective of degree of encephalopathyINR >6.5 irrespective of degree of encephalopathyor 3 of the following five criteriaor 3 of the following five criteria
Age<10, >40Age<10, >40Etiology: nonA-E hepatitis, drugsEtiology: nonA-E hepatitis, drugs
Duration of jaundice before encephalopathy >7 daysDuration of jaundice before encephalopathy >7 daysINR >3.5INR >3.5
Serum bilirubin >17.5 mg%.Serum bilirubin >17.5 mg%.CLICHY CRITERIACLICHY CRITERIA• • Factor V <20% (age <30 years) or 30% (age >30 years)Factor V <20% (age <30 years) or 30% (age >30 years)• • Confusion and/or comaConfusion and/or coma

Acute Liver failure (PGIMER criteria Acute Liver failure (PGIMER criteria – Clinical prognostic Indicators)– Clinical prognostic Indicators)
age ≥50 yr, age ≥50 yr, JEI >7 days, JEI >7 days, grade 3 or 4 encephalopathy,grade 3 or 4 encephalopathy, presence of cerebral edema,presence of cerebral edema, prothrombin time ≥35 seconds, andprothrombin time ≥35 seconds, and creatinine ≥1.5 mg/dL. creatinine ≥1.5 mg/dL.
Presence of any 3 of 6 CPI was optimum in Presence of any 3 of 6 CPI was optimum in identifying survivors and nonsurvivorsidentifying survivors and nonsurvivors

Chronic Liver disease : Chronic Liver disease : CirrhosisCirrhosis
All patients with cirrhosis do not qualify for All patients with cirrhosis do not qualify for liver transplantation.liver transplantation.
Transplantation is generally considered Transplantation is generally considered when a patient has suffered from either a when a patient has suffered from either a complication of portal hypertension.complication of portal hypertension.
The onset of decompensation is associated The onset of decompensation is associated with significantly impaired survival.with significantly impaired survival.
The development of hepatorenal syndrome The development of hepatorenal syndrome is an ominous marker that signals the need is an ominous marker that signals the need for immediate transplant evaluation.for immediate transplant evaluation.

Chronic Liver Disease — Signs of Chronic Liver Disease — Signs of decompensationdecompensation
AscitesAscites EncephalopathyEncephalopathy Portal Hypertensive BleedingPortal Hypertensive Bleeding Hepatocellular Carcinoma in the Hepatocellular Carcinoma in the
setting of Cirrhosissetting of Cirrhosis

Chronic Liver Disease—Indications Chronic Liver Disease—Indications for Transplantationfor Transplantation
AscitesAscites Ascites has a two-year mortality of 50%Ascites has a two-year mortality of 50% SBP has a two-year mortality of 80%SBP has a two-year mortality of 80%
Hepato-Renal Syndrome : Hepato-Renal Syndrome : -- 2 types, type 1 has very poor 2 types, type 1 has very poor prognosis, >50% mortality at 2 weeks, and prognosis, >50% mortality at 2 weeks, and type 2 has 50% mortality at 1 year.type 2 has 50% mortality at 1 year.
Variceal bleed and hepatic encephalopathy: Variceal bleed and hepatic encephalopathy: difficult to quantify the effect on mortality difficult to quantify the effect on mortality as they are a mechanical result of portal as they are a mechanical result of portal hypertensionhypertension

When?When?
Quality of life issuesQuality of life issues
– – Severe lethargySevere lethargy
– – Intractable itchingIntractable itching
– – Recurrent bile duct infectionsRecurrent bile duct infections
– – Intractable ascitesIntractable ascites
– – Severe bone thinningSevere bone thinning
– – PainPain

Liver TransplantationLiver TransplantationQuestion for Transplant TeamQuestion for Transplant Team
• • When to list for liver When to list for liver transplantation?transplantation?
• • When to perform the liver When to perform the liver transplant?transplant?

When….?When….?
Patients who are too well should not be Patients who are too well should not be transplanted. transplanted.
Likewise, transplantation of patients who Likewise, transplantation of patients who are too sick is associated with poor are too sick is associated with poor outcomes. outcomes.
The goal of transplantation is to prolong The goal of transplantation is to prolong survival. survival.
Thus, liver transplantation should be Thus, liver transplantation should be performed at the time point when the performed at the time point when the patient is expected to have greater patient is expected to have greater survival with a liver transplant than survival with a liver transplant than without.without.

PrognosticationPrognostication
Survival of a patient with ‘‘Child’s C Survival of a patient with ‘‘Child’s C cirrhosis’’ is about 20–30% at 1 year and cirrhosis’’ is about 20–30% at 1 year and less than 5% at 5 years. less than 5% at 5 years.
In contrast, the survival rate after In contrast, the survival rate after transplantation is 85–90% at 1 year and transplantation is 85–90% at 1 year and over 70% at 5 years. over 70% at 5 years.
By the time the patient has evidence of By the time the patient has evidence of advanced clinical liver disease (Child’s C advanced clinical liver disease (Child’s C cirrhosis), the patient may not survive long cirrhosis), the patient may not survive long enough to get a transplant.enough to get a transplant.

MELD scoreMELD score
• • MELD -- Model for End-Stage Liver MELD -- Model for End-Stage Liver Disease Scoring System – MELD Score Disease Scoring System – MELD Score
= 0.957 x Log= 0.957 x Logee(creatinine mg/dl)(creatinine mg/dl)
+ 0.378 x Log+ 0.378 x Logee(bilirubin mg/dl)(bilirubin mg/dl)
+ 1.120 x Log+ 1.120 x Logee(INR)(INR)
+ 0.643+ 0.643
• MELD score depends upon kidney MELD score depends upon kidney function,function,
bilirubin level and clotting factor levelsbilirubin level and clotting factor levels

MELD scoreMELD score
Introduced in Feb 2002.Introduced in Feb 2002. The MELD score originally was The MELD score originally was
developed and validated to assess the developed and validated to assess the short-term prognosis of patients with short-term prognosis of patients with cirrhosis undergoing TIPS.cirrhosis undergoing TIPS.
Developed by the Mayo Clinic.Developed by the Mayo Clinic. Using the MELD model, patients are Using the MELD model, patients are
assigned a score from 6 to 40.assigned a score from 6 to 40. Estimated 3-month survival for a score Estimated 3-month survival for a score
of 6 is 90%, and for a score of 40 is 7%.of 6 is 90%, and for a score of 40 is 7%.

Chronic Liver Disease—Indications for Chronic Liver Disease—Indications for TransplantationTransplantation
Ultimately, the decision to transplant is Ultimately, the decision to transplant is based upon the patient’s likelihood of based upon the patient’s likelihood of survivalsurvival
Survival with transplantation:Survival with transplantation: One-year ~85-90%One-year ~85-90% Two-year ~80-88%Two-year ~80-88% Five-year ~65-75%Five-year ~65-75%
Usually a patient will be listed for liver tx at Usually a patient will be listed for liver tx at a MELD of 10 or more, when the expected a MELD of 10 or more, when the expected 3 month survival is less than 90%.3 month survival is less than 90%.

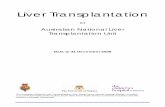
Patient Survival After Primary Liver Patient Survival After Primary Liver TransplantationTransplantation
0
10
20
30
40
50
60
70
80
90
100
0 12 24 36 48 60
Time (months)
Su
rviv
al (
%)
1984-2001 n=384
1991-2001 n=299
1995-2001 n=186

Guidelines for Organ AllocationGuidelines for Organ Allocation
Organs should be allocated to Organs should be allocated to transplant candidates in the order of transplant candidates in the order of medical urgencymedical urgency
The role of waiting times in The role of waiting times in determining allocation order should determining allocation order should be minimizedbe minimized
Every attempt should be made to Every attempt should be made to promote efficient use of donor organspromote efficient use of donor organs

Requirements for TransplantationRequirements for Transplantation
End stage liver diseaseEnd stage liver disease Physiologic ability to tolerate surgery: Physiologic ability to tolerate surgery:
Cardiac, pulmonary, renal, cerebral functionCardiac, pulmonary, renal, cerebral function Anatomy – status of vessels (PV/HA/HV)Anatomy – status of vessels (PV/HA/HV) Social support/ psychological supportSocial support/ psychological support No extra-hepatic infection or malignancyNo extra-hepatic infection or malignancy Alcohol abstinence for 6 months/ no Alcohol abstinence for 6 months/ no
substance abusesubstance abuse

Contra-indicationsContra-indications
Cardiopulmonary disease that cannot be corrected Cardiopulmonary disease that cannot be corrected and is a prohibitive risk for surgery.and is a prohibitive risk for surgery.
Malignancy outside of the liver within five years of Malignancy outside of the liver within five years of evaluation (not including superficial skin cancers) or evaluation (not including superficial skin cancers) or not meeting oncologic criteria for cure.not meeting oncologic criteria for cure.
Active alcohol and drug use. Minimum period of Active alcohol and drug use. Minimum period of abstinence of at least six months (+/- participation abstinence of at least six months (+/- participation in a structured rehabilitation program) may be in a structured rehabilitation program) may be needed.needed.
Advanced age and AIDS are examples of Advanced age and AIDS are examples of relative relative contraindications.contraindications.
Liver transplantation can be performed in those Liver transplantation can be performed in those older than 65 provided that there has been a older than 65 provided that there has been a comprehensive search made for co-morbiditiescomprehensive search made for co-morbidities

Liver TransplantationLiver TransplantationEvaluationEvaluation
Determine cause of liver diseaseDetermine cause of liver disease Document severity of liver diseaseDocument severity of liver disease Determine survival and functional Determine survival and functional
abilityability Concomitant medical problemsConcomitant medical problems Psychiatric evaluationPsychiatric evaluation Social EvaluationSocial Evaluation

LTx EvaluationLTx Evaluation
• • Medical historyMedical history– – Symptoms such as fatigue, itching, Symptoms such as fatigue, itching, swelling, changes in mental status and GI swelling, changes in mental status and GI bleedingbleeding– – Other medical problemsOther medical problems– – MedicationsMedications– – Includes alcohol use and drug use historyIncludes alcohol use and drug use history
• • Physical examinationPhysical examination• • Blood testsBlood tests
– – Determine underlying cause of liver Determine underlying cause of liver diseasedisease– – Determine current functional status of Determine current functional status of the liverthe liver

LTx EvaluationLTx Evaluation
Liver Ultrasound/CT scan/MRILiver Ultrasound/CT scan/MRI Liver biopsyLiver biopsy ERCP/ MRCP – Cholangiogram – ERCP/ MRCP – Cholangiogram –
examines bile ducts if cirrhosis is examines bile ducts if cirrhosis is otherwise unexplainedotherwise unexplained
PET scan and other inv for cancerPET scan and other inv for cancer

Evaluation of psychosocial support Evaluation of psychosocial support for LTxfor LTx
Psychosocial evaluationPsychosocial evaluation
– – Support systemsSupport systems
– – Compliance with post transplant Compliance with post transplant immunosuppression medication immunosuppression medication protocol after transplantationprotocol after transplantation
Social and family support around the Social and family support around the transplanttransplant

Limitations of MELDLimitations of MELD
• • Patients with liver cancerPatients with liver cancer
• • Bile duct infectionsBile duct infections
• • ItchingItching
• • Disabling mental status changes (hepatic Disabling mental status changes (hepatic encephalopathy)encephalopathy)
• • ? Criteria for living donors? Criteria for living donors
Other conditions like : HPS, metabolic Other conditions like : HPS, metabolic diseases, congenital errors of diseases, congenital errors of metabolism, fulminant liver failure, graft metabolism, fulminant liver failure, graft non-function, etcnon-function, etc

Surgical perspectiveSurgical perspective
Immediate function of a transplanted liver is Immediate function of a transplanted liver is essential. Unlike in kidney, pancreas, or, to some essential. Unlike in kidney, pancreas, or, to some extent, heart transplantation, there is no effective extent, heart transplantation, there is no effective artificial support for a hepatic patient in the event artificial support for a hepatic patient in the event of graft failure.of graft failure.
A complex surgical exercise in a severely A complex surgical exercise in a severely physiologically compromised patient – physiologically compromised patient –
- major surgery- major surgery
- blood loss – portal hypertension- blood loss – portal hypertension
- immunosuppression- immunosuppression
- risk of infection- risk of infection
- necessity of liver function- necessity of liver function

Donor selectionDonor selection
Cadaveric/ living donor.Cadaveric/ living donor. Blood group match. (HLA not Blood group match. (HLA not
required/ cross matching not required/ cross matching not required).required).
Size match.Size match. Marginal donors.Marginal donors. Split liver.Split liver.

Organ harvesting/ procurementOrgan harvesting/ procurement
HTK solution HTK solution (custodiol)(custodiol)
UW (Viaspan)UW (Viaspan) Goal: Cool the organs Goal: Cool the organs
and perfuse with and perfuse with preservative solution preservative solution while exsanguinating while exsanguinating the organs.the organs.
Aortic canulationAortic canulation Portal canulationPortal canulation

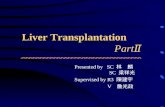
Donor liverDonor liver

Donor LiverDonor Liver
Cadaveric Cadaveric donor liver donor liver after back after back table table preparationpreparation

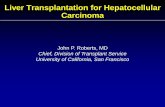
Donor LiverDonor Liver
Same Same cadaver liver cadaver liver with the with the hepatic hilum hepatic hilum displayeddisplayed

AnesthesiaAnesthesia Physiological processes, biological function, and drug Physiological processes, biological function, and drug
disposition, renal function, RBFdisposition, renal function, RBF Interpretation of liver function study resultsInterpretation of liver function study results Portal hypertension and complications: variceal Portal hypertension and complications: variceal
hemorrhage, SBP, sepsis, ascites, hepatorenal hemorrhage, SBP, sepsis, ascites, hepatorenal syndrome, encephalopathysyndrome, encephalopathy
Cardiac and circulatory effects: hyperdynamic Cardiac and circulatory effects: hyperdynamic circulation, vasodilatation.circulation, vasodilatation.
Portopulmonary hypertensionPortopulmonary hypertension CoagulopathyCoagulopathy Cholestasis, jaundiceCholestasis, jaundiceImpact of anesthesia on liver functionImpact of anesthesia on liver function Limited functional reserveLimited functional reserve Hepatic blood flowHepatic blood flow Drug clearanceDrug clearance Anesthesia-induced hepatitisAnesthesia-induced hepatitis Postoperative jaundicePostoperative jaundice Risk factors for decompensation in patients with Risk factors for decompensation in patients with
cirrhosiscirrhosis

Implantation of the new liver.Implantation of the new liver.
Orthotopic/ auxillaryOrthotopic/ auxillary begins with a controlled begins with a controlled
recipient hepatectomyrecipient hepatectomy formidable task in formidable task in
individuals with severe individuals with severe portal hypertension and portal hypertension and extensive collateralextensive collateral
Role of temporary porta-Role of temporary porta-caval shunt..caval shunt..
Engraftment with venous, Engraftment with venous, arterial and then biliary arterial and then biliary anastomoses.anastomoses.
Classic v/s piggy back Classic v/s piggy back implantation.implantation.


Classical v/s piggy back techniqueClassical v/s piggy back technique
Classical or cava Classical or cava replacementreplacement
Piggy-back technique

Graft functionGraft function
Helpful signs of hepatic function in Helpful signs of hepatic function in the immediate postoperative periodthe immediate postoperative period
1. Hemodynamic stability1. Hemodynamic stability
2. Awakening from anesthesia2. Awakening from anesthesia
3. Clearance of lactate3. Clearance of lactate
4. Resolution of hypoglycemia4. Resolution of hypoglycemia
5. Normalization of coagulation profile5. Normalization of coagulation profile
6. Resolution of elevated transaminases6. Resolution of elevated transaminases
7. Bile of sufficient quantity and golden 7. Bile of sufficient quantity and golden brown in colorbrown in color


After reperfusion.After reperfusion.

Immediate outcomeImmediate outcome
What factors:What factors: Organ harvesting.Organ harvesting. Organ preservation.Organ preservation. Warm and cold ischemia times.Warm and cold ischemia times. Graft selection/ graft quality.Graft selection/ graft quality. Donor-recipient matching.Donor-recipient matching. Surgical problems.Surgical problems. Medical issues.Medical issues.

Post-op monitoringPost-op monitoring
Monitor hemodynamics, vitals, and blood tests.Monitor hemodynamics, vitals, and blood tests. Blood tests: LFTs, lactate, ABG, CBC, and Blood tests: LFTs, lactate, ABG, CBC, and
coagulation parameters.coagulation parameters. Monitor immunosuppression.Monitor immunosuppression. rising transaminases and bilirubin in the 48 h rising transaminases and bilirubin in the 48 h
immediately after transplantation may not be immediately after transplantation may not be ominous signs as long as the prothrombin time, ominous signs as long as the prothrombin time, serum lactate, bile production, or other measures of serum lactate, bile production, or other measures of hepatic function are stable or improvinghepatic function are stable or improving
Usually anesthesia is not reversed and patients are Usually anesthesia is not reversed and patients are kept intubated for upto 48 hours.kept intubated for upto 48 hours.
Doppler examination of the transplanted liver.Doppler examination of the transplanted liver. Medication: immunosuppression, antibiotics, Medication: immunosuppression, antibiotics,
antiplatelets, analgesics, and PPIs.antiplatelets, analgesics, and PPIs.

ImmunosuppressionImmunosuppression
CNIs: tacrolimus/ cysclosporineCNIs: tacrolimus/ cysclosporine
mTOR inhibitors: Sirolimus, everolimusmTOR inhibitors: Sirolimus, everolimus
SteroidsSteroids
MycophenolateMycophenolate
AzathioprineAzathioprine
Antibodies: daclizumab, basiliximab, ATG, Antibodies: daclizumab, basiliximab, ATG,
ALG, OKT3ALG, OKT3
Newer agents: Efalizumab, Enlimomab, Newer agents: Efalizumab, Enlimomab,
Campath (Alemtuzumab), Natalizumab, Campath (Alemtuzumab), Natalizumab,
Betalacept, abatacept, etc.Betalacept, abatacept, etc.

ComplicationsComplications
Immediate, early and late.Immediate, early and late. Immediate Immediate – post-op.– post-op.
-- Bleeding (commonest – 12-15%)Bleeding (commonest – 12-15%)- - Graft non-function (PNF) [5%] or Graft non-function (PNF) [5%] or delayed graft function [6-7%].delayed graft function [6-7%].-- Vascular complications: HAT, PVT Vascular complications: HAT, PVT and venous thrombosis.and venous thrombosis.-- Renal dysfunction.Renal dysfunction.-- complications related to complications related to prolonged and major surgery, blood prolonged and major surgery, blood transfusion.transfusion.- Infections – viral and bacterial.- Infections – viral and bacterial.

ComplicationsComplications
Early: Early: - InfectionsInfections- RejectionRejection- Surgical/ wound complications.Surgical/ wound complications.- Biliary problemsBiliary problems- Vascular complicationsVascular complications- Recurrent diseaseRecurrent disease

ComplicationsComplications
Late complications:Late complications:- Usually late, after more than a year.Usually late, after more than a year.- Recurrent diseaseRecurrent disease- Medication adverse effectsMedication adverse effects- Chronic rejectionChronic rejection- InfectionsInfections- Metabolic problemsMetabolic problems- RecidivismRecidivism

Infections after a transplantInfections after a transplant

Waiting for a liverWaiting for a liver
Management of Ascites.Management of Ascites. Management of portal hypertensionManagement of portal hypertension Renal functionRenal function Hepatic encephalopathyHepatic encephalopathy General health and activityGeneral health and activity Treatment of viral diseaseTreatment of viral disease VaccinationVaccination Prevention of infection.Prevention of infection.

If waiting is not possible…., If waiting is not possible…., getting too late….getting too late….
LDLT: living donor liver transplant.LDLT: living donor liver transplant. India: only related/ approved by a ethical India: only related/ approved by a ethical
committee.committee. Advantages: Advantages:
-- elective surgery.elective surgery.
- - healthy known donorhealthy known donor
- - short cold ischemia timesshort cold ischemia times
-- reduced waiting timereduced waiting time Disadvantages:Disadvantages:
-- risk to donorrisk to donor
-- cost and more resourcescost and more resources
-- higher risk of biliary ad vascular higher risk of biliary ad vascular complicationscomplications
- - reduced size liverreduced size liver

Usual model Usual model for LDLTfor LDLT

Living donor firstsLiving donor firsts
• • LD Kidney - 1954LD Kidney - 1954 • • LD Intestine - 1988LD Intestine - 1988 • • LD Liver (pediatric) - 1990LD Liver (pediatric) - 1990 • • LD Pancreas - 1992LD Pancreas - 1992 • • LD Lung - 1994LD Lung - 1994 • • LD Liver (adult) - 1997LD Liver (adult) - 1997

Essential Concepts for UsingEssential Concepts for UsingLiving DonorsLiving Donors
• • No conflict of interestNo conflict of interest
• • No coercionNo coercion
• • Minimize donor risksMinimize donor risks
• • Donors must be given every Donors must be given every opportunity to change their mindsopportunity to change their minds
• • Emphasize alternativesEmphasize alternatives

How Much Liver Do You Need?How Much Liver Do You Need?
• • Liver = 2% body weightLiver = 2% body weight
• • Optimal: > 1% liver weight/body weight Optimal: > 1% liver weight/body weight ratioratio
• • 70 kg recipient needs at least 700 cc (gm)70 kg recipient needs at least 700 cc (gm)
• • Cannot go below 0.7 - 0.8%Cannot go below 0.7 - 0.8%
- GRWR.GRWR.- Graft/ SLV ratioGraft/ SLV ratio- Usually right lobe.Usually right lobe.- Recently the use of dual grafts has been Recently the use of dual grafts has been
done successfully.done successfully.

LDLT problemsLDLT problems
Risk to donor: 0.2 – 0.3% risk of deathRisk to donor: 0.2 – 0.3% risk of death
-- 2-4% risk of major complications2-4% risk of major complications
-- About 15-25% risk of minor About 15-25% risk of minor complications.complications.
Higher incidence of biliary problemsHigher incidence of biliary problems Higher incidence of vascular problemsHigher incidence of vascular problems Small for size syndromeSmall for size syndrome Ethical issuesEthical issues Initially had poorer graft survival, but Initially had poorer graft survival, but
recently has been equal to DDLT.recently has been equal to DDLT.

Diagnoses indicating potential candidacy for LT include the following: * 070 Viral hepatitis * 1550-1552 Malignant neoplasm of liver and intrahepatic bile ducts * 2115 Benign neoplasm of liver and biliary passages * 2308 Carcinoma of liver and biliary system * 2353 Neoplasm of uncertain behavior in liver and biliary passages * 2390 Neoplasm of unspecified nature in digestive system * 2710 Glycogenesis * 2720 Pure hypercholesterolemia * 2727 Lipidoses * 2751 Disorders of copper metabolism * 2770-2776 Cystic fibrosis, disorders of porphyrin metabolism, other disorders of purine and pyrimidine metabolism, amyloidosis, disorders of bilirubin excretion (like EHBA as well as Criggler Najar syndrome), mucopolysaccharidosis, other deficiencies of circulating enzymes including urea cycle disorders, an dother metabolic disorders. * 2860 Congenital factor VIII disorder * 2861 Congenital factor IX disorder * 4530 Budd-Chiari syndrome * 570 Acute and subacute necrosis of liver * 5710 Alcoholic fatty liver * 5712 Alcoholic cirrhosis of liver * 5714 Chronic hepatitis * 5715 Cirrhosis of liver without mention of alcohol * 5716 Biliary cirrhosis * 5718 Other chronic nonalcoholic liver disease * 5719 Unspecified liver disease without mention of alcohol * 5728 Other sequelae of chronic liver disease * 5758 Other specified disorders of gallbladder * 5761,5762 Cholangitis, obstruction of bile duct * 75161,75169 Biliary atresia, other anomalies of gallbladder, bile ducts, and liver * 7744 Perinatal jaundice due to hepatocellular damage * 7778 Other specified perinatal disorders of digestive system * 864 Injury to liver * 3483 Encephalopathy, unspecified* 452 Portal vein thrombosis.

THANK YOU!THANK YOU!