
Outpatient Chemotherapy Planning: a Literature Review with ...

Service Improvement Team
Outpatient Services Review and Improvement
(3 Clinician pilot) Full Report - May 2010
SUMMARY
The purpose of this report is to present the findings from the outpatient services review and to make recommendations as to how improvements can be delivered.
BACKGROUND & METHODOLOGY
The Service Improvement Team were requested to look into improving the experience for patients and staff in outpatient clinics at RNOH. The first phase of this work has concentrated on the clinics of Professor Tim Briggs, Mr John Skinner and Mr Stewart Tucker, with a view to extending any agreed changes across the entire outpatient service. A review has been carried out at both sites including demand & capacity analysis (referrals and activity for new and follow-up patients), a review of clinic templates, and appointment booking processes, clinic observation and patient pathway walk-through. In addition front-line and back-office members of staff have been shadowed or interviewed. The team have also researched best practice in other NHS Trusts, primary care and in the independent sector. A detailed project plan can be found in Appendix A.
CLINIC PROFILES
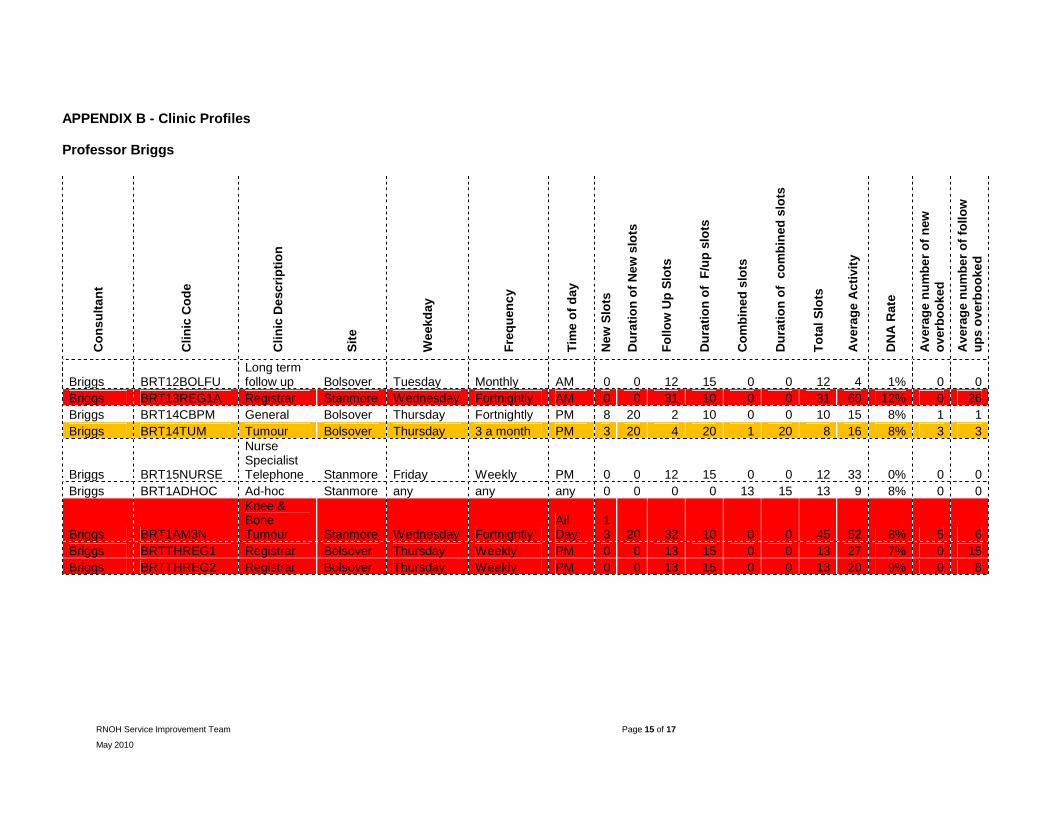
A profile of clinics for each consultant is shown in Appendix B. Clinics which are regularly (over)booked in excess of manageable levels are shown in red. Those shaded in amber are slightly above tolerance levels. The remainder are routinely being booked at acceptable activity levels. It should be noted that the overbooking and DNA figures shown are based on average numbers for the last financial year.

RNOH Service Improvement Team Page 2 of 17
May 2010
Capacity/activity profile
The data was collected for a 6 week period from 22nd March – 30th April. All data has been extracted from Insight and has undergone validation to ensure accuracy. The graphs below demonstrate the actual demand, capacity and activity.
Professor Briggs Outpatient Activity Analysis 22nd March 2010 - 30th April 2010
0
50
100
150
200
250
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6
Num
ber
of Patients
Activity Demand (Booked + referrals)
Actual Capacity
DNA
Mr Skinner Outpatient Activity Analysis 22nd March 2010 - 30th April 2010
0
50
100
150
200
250
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6
Num
ber of
Pat
ient
s
Activity Demand (Booked + referrals) Actual Capacity DNA
Mr Tucker Outpatient Activity Analysis 22nd March 2010 - 30th April 2010
0
50
100
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6
Num
ber of Patients
Activity Demand (Booked + referrals)
Actual Capacity
DNA

RNOH Service Improvement Team Page 3 of 17
May 2010
Professor Briggs and Mr Skinner both hold clinics at Bolsover Street and Stanmore whilst Mr Tucker runs clinics on the Stanmore site only. The majority of patients seen within the clinics are follow ups. Prof. Briggs and Mr Skinner’s joint fortnightly clinics are typically heavily overbooked with the majority of over-bookings being made for the follow-up patients. Clinics often begin late due to competing demands. Slot durations range from 15-30 minutes for new appointments and 10-30 minutes for FU’s. Mr Tucker specialises in spinal deformity although there were patients with degenerative & cervical spine seen within the sessions observed.
Mr Tucker’s demand is managed by slightly overbooking each clinic (by an average of 3 patients) and diverting additional patients into extra (ad-hoc) clinics, this results in his level of overbooking’s appearing tolerable in his clinic profile (Appendix B), although it can be seen in the tables on page 3 that his demand also outstrips capacity. Often ad-hoc clinics are arranged with insufficient notice for patients resulting in high levels of patients failing to attend (DNAs).
Clinic Observations Observations were carried out across site where applicable during March and April. It was noted that clinical staff were productive and worked efficiently and there were no notable delays once the patient was in the consulting room. However, due to the large numbers of patients being overbooked and late starts in clinics, patients waited a long time to be seen. A summary of the time spent in the consulting room and the time patients waited to go into their consultations is shown below. Observations would indicate that the current slot length for new patients is sufficient, but that 15 minute duration for follow-up patients may better reflect the actual current length of consultation.
A summary of the time spent in the consulting room and the time patients waited to go into their consultations is shown below.
Consultation length Time waited to be seen Template slot length Min Max Avg Min Max Avg
Briggs 20mins 11mins 20mins 15.5mins 2hrs 58mins
3hrs 22mins
3hrs 10mins
Skinner 15-20mins 5mins 16mins 8.5mins 2mins 25mins 54mins
5secs
New
Pat
ien
ts
Tucker 20-30mins 9mins 23mins 12.5mins 12mins 1min
3secs 28mins 10secs
Briggs 10-20mins 3mins 1hr
44mins 15mins 53secs
48mins 3hrs 26mins
1hrs 59mins
Skinner 10-20mins 3mins 30mins 16mins
30secs 5mins 3hrs 43mins
1hr 54mins
Fo
llow
-up
P
atie
nts
Tucker 10-30mins 3mins 16mins 7mins
35secs 12mins 1min
3secs 28mins 10secs

RNOH Service Improvement Team Page 4 of 17
May 2010
Clinic Start Times - planned versus actual
Briggs Skinner Tucker
Pla
nned
Sta
rt T
imes
Act
ual
Tim
es000000000000000000000000000000Start 000000000000000000000000000000Start 00000000000000000000Start 0000000StartStartStartStart StartStartEndEndEndStartStartStartStartStartStart StartEndEndEndEndEndEndEndStartStartStartStartStartStartStartStartStartStartStartEndStart EndEndEndEndEndStartStartStartStartStartStart EndEndEndEndEndEndEndEndEndEndStart EndStartStartStartStartStartStartStartEndEndStart EndEndEndEndEndStartStartStartEndEndStart EndEndStartStartStartStartStartStartStartStartStart StartStartStartStartStartStartEndEndEndEndStart EndEndEndEndEndEndEndEndEndEndEndEndEndEndEndEndEndEndEndStartStartStartStartStartStartStartStartEndEndEndEndStartStartStartStartStartStartStartStartStartStart StartStartStartStartStartStartStartEndEndEndStart EndEndEndEndEndEndEndEndEndEndStart EndEndEndEndEndEndEndEndEndEndEndStartStartStartStartStartStartStartStartEndStart EndEndStartStartStartStartStartStartStartStartStartStartEndEndEndStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartEndEndEndEndEndEndEndEndEndEndEndEndStartStartStartStartStart StartStartStartStartStartStartStartStartStartStartStart StartStartStartStartStartStartStartStartStartStartStart StartStartStartEndEndEndEndEndEndEndStart EndEndEndEndEndStart EndEndEndEndEndEndEndEndEndEndEndEndEndEndEndStart EndEndEndStartStartStartStartStartStartStartStartStartStartStartStartStart StartStartEndEndEndEndEndStartStartStartStartStartStartStartStartStart StartStartStartEndEndStartStartStartEndEndStartEndEndEndEndStart StartEndStartEndStartEndStartEndStartEndStartEndEndEndEndEndStartStartStartStartStartStart StartStartEndEndEndEndEndEndEndEndEndEndEndEndEndStart EndEndEndStartStartStartStartStartStartStartStartStartEndEndEndEndEndEndStartStartStartStartStartEndEndStartEndStartEndStartEndEndEndStartStartStartStartStartStartEndEndEndStartStartStartEndEndEndEndEndEndEndEndEndStartStartEndEndEndEndEndStartStartStartStartEndEndStartStartEndEndEndEndEndEndEndEndEnd
16:0016:1016:20
15:2015:3015:4015:50
14:4014:5015:0015:10
14:0014:1014:2014:30
13:2013:3013:4013:50
12:4012:5013:0013:10
12:0012:1012:2012:30
11:2011:3011:4011:50
10:4010:5011:0011:10
10:0010:1010:2010:30
9:209:309:409:50
8:408:509:009:10
8:008:108:208:30
Pla
nn
ed S
tart
Tim
es
Act
ual
Tim
es
00000Start 000000000000000Start 000000000000000000000000000000Start 0000000000000000000000000000000000000000Start 00000000000000000000Start 000000000000000000000000000000Start 0000000000Start 0000000000Start 00000000000000000000Start 00000000StartStartStartStartStartStartEndStartEndStartEndStartEndStartEndStartEndStartEndStart EndEndEndEndEndStartStartStartStartEndStart EndEndEndStartStartStart StartStartStartStartStartStart StartStartStartEndEndEndStartStartStartStartStart StartStartStartStartStartStartEndEndEndEndStart EndStartStartStartStartStart StartStartStartStartStartStart StartStartStartEndEndEndEndStartStartStartStart StartStartStartStartStartStartEndEndEndEndStart EndEndEndEndEndStart EndEndStartStartStartStart StartStartStartStartStartStartEndStartEndStartEndEndEndStart StartStartEndEndEndEndStartStartEndEndStart StartStartStartEndEndStart EndEndEndEndEndEndEndEndStartStartStartStartStartStartStartStartEndEndEndEndEndEndEndStartEndEndEndStartStartStartStartStartEndEndEndStart EndStartStartStartStartStartStartStartStartStartEndEndEndEndEndEndEndEndStartStartStartStartStartStartStartEndEndEndEndEndStartStartStartStartStartStartEndEndEndEndEndEndEndEndEndEndStartStartStartStartStartStartStartEndStartEndStartEndStartEndStartStartStartStartStartEndEndEndEndEndEndEndEndEndStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartStartEndEndEndEndEndEndEndEndEndEnd
17:2017:3017:4017:50
16:4016:5017:0017:10
16:0016:1016:2016:30
15:2015:3015:4015:50
14:4014:5015:0015:10
14:0014:1014:2014:30
13:2013:3013:4013:50
12:4012:5013:0013:10
12:0012:1012:2012:30
11:2011:3011:4011:50
10:4010:5011:0011:10
Pla
nn
ed S
tart
Tim
es
Act
ual
Tim
es
00000000000000000000000000000000000000000000000000000000000000000000000000000000Start 00000000000000000000Start 000000000StartStartStartStartStartStartStartEndEndEndEndStartStartStartStartStartStartStartStartStartStartStart StartEndEndEndEndEndEndEndEndEndStart EndEndStartStartStartStartStartStartStartStartStart StartEndEndStartStartStartStartStartEndEndStart EndEndEndEndEndEndEndEndEndEndStart EndEndEndEndEndStartStartStartStartStartStart StartStartStartStartEndEndEndEndEndEndStart StartEndStartEndStartEndStartEndStartEndStartEndStartEndStartEndStartEndStartEndStart StartEndStartStartStartStartStartStartStartEndEndEndEndEndStartStartStartStartStartEndEndStart EndStartStartStartStartStartStartEndEndEndStart EndStartStartStartStartStartStartStartEndStartStartStartEndEndEndEndEndEndEndEndEndEndEndStartStartStartStartStartStartStartEndEndEndEndEndEndEndEndEndEnd
12:0012:1012:20
11:2011:3011:4011:50
10:4010:5011:0011:10
10:0010:1010:2010:30
9:209:309:409:50
8:408:509:009:10
8:008:108:208:30
Key:
Scheduled Appointment start
Time in consultation room

RNOH Service Improvement Team Page 5 of 17
May 2010
New to follow up ratios
All 3 Consultants are not meeting the new to follow up target ratios for the Trust of 3 follow ups for every new attendance. However the ratios for cancer patients are higher due to the nature of the condition treated and long term FU. Actual ratios for 2009-10 are shown below:
Professor Briggs 1:5
Mr Skinner 1:4
Mr Tucker 1:3.3
This pattern is reflected in the allocation of new to follow up slots within the respective consultant’s clinic templates.
FINDINGS The specialty breakdown and case mix varies between the 3 clinicians, however the majority of findings, issues and recommendations are common to all the clinics studied. There was a high volume of activity within the clinics but no major patient flow issues were identified although there were some delays in x-ray. The main areas which need to be considered are: 1. Conflict with outpatient and inpatient sessions. In almost all afternoon clinics observed, the
impact of theatre overruns resulted in patients having to wait to be seen. The cumulative effect of a late start impacts on subsequent appointments.
2. Conflict with outpatient sessions and ward rounds. Morning clinic sessions start as early
as 8.00 am at which time the surgical teams are completing ward rounds that seldom finish before 9.30 am. During the ward rounds there is no doctor available to see outpatients. This diary conflict results in a late start to clinics on the day which will have a knock-on effect throughout the day.
3. Advance knowledge of available capacity in future clinics. Many clinics are fully booked
weeks or months in advance with appointments being given to 6 monthly and annual follow-ups. High volume over bookings could be avoided if clinicians have advance notice of slot availability.
4. Overbooking. The clinics were generally overbooked with as many as 4 patients booked into
1 slot. The last afternoon appointments are often booked at 14.30 despite knowledge that the clinic will run until at least 5 pm due to volume of over bookings. This results in patients having to wait longer than is necessary. Clinic finish times need to reflect volume of work and over bookings should be evenly spread across clinic. After investigation it was found that there were various reasons for overbooking. For new patients overbooking’s tended to occur to avoid breaching 18week targets. Patients that are not new are followed up at fixed points during their care e.g. 6 weeks after going home after surgery (Ward discharge patient), every 6 months for joint replacement and will be booked during that week, regardless of whether that week’s clinic is already fully booked. In addition patients that are in pain or are having problems with implants/prostheses will request an appointment at short-notice via the consultant’s medical secretary.
5. Large volume of Follow-Up patients. The new to follow-up ratios for all 3 clinicians are over
the RNOH target. A significant number of patients travel long distances for regular long-term follow-up or routine monitoring. In addition very few follow-up patients are discharged within clinic. An audit of clinic attendances for the 3 consultants for the last 6 months shows a 4% discharge rate for follow ups.

RNOH Service Improvement Team Page 6 of 17
May 2010
6. Inconsistent approach to diagnostic requests. There is an inconsistent approach to diagnostic requests, irrespective of how far a patient has to travel to attend clinic. This results in patients either being expected to travel back to the RNOH or sent back to their local provider. The Trust should consider one stop clinics were appropriate.
7. Sarcoma patients. Sarcoma patient appointments are often mixed randomly with those of
other patients which often results in inadequate time being spent with these patients. 8. Admin and Nursing. The workforce in the department has a high skill mix and work efficiently and
cohesively under pressure. It was also observed that the admin and nursing teams are courteous in dealing with patients and have demonstrable good levels of customer care.
ISSUES AND CHALLENGES
� Capacity. There is limited capacity in the waiting area and this is particularly evident on the Stanmore site particularly on Wednesdays.
� Stress within the department. Due to sheer volume of patients the team is under considerable
pressure to achieve the smooth-running of clinics. There are a significant number of complaints due to the lack of space in the waiting areas and the long wait times.
� Patient facilities. There is a lack of facilities / distractions for patients who have long waits in
outpatients for example, they are unable to get refreshments at Stanmore site after 4pm and there is no visual distraction such as a plasma screen information system, television or similar.
� Clinic Rooms. Patients leaving consulting rooms after just being told they have cancer would
benefit from having a room available in which to further discuss their diagnosis with a specialist nurse. There is currently no availability for this.
� Impact on x-ray. High numbers of outpatients requiring an x-ray will impact negatively on
inpatient work by delaying ward rounds and discharge. There is currently no system in place to enable the x-ray department to advance plan in order to be able to flex radiography and portering staff according to anticipated workload.

RNOH Service Improvement Team Page 7 of 17
May 2010
RECOMMENDATIONS The main recommendations of the review are listed below. These have been tabled below and divided into short, medium and long-term changes in recognition that some will take longer than others to implement Description Timescale Predicted
duration to completion
Workplans. A review of individual workplans should be carried out for each clinical firm. This should include scheduling of outpatient and inpatient sessions to avoid conflict where possible.
Long-term 4-6 months
Planning/Preparation. Clinicians should have information of future clinic slot availability when planning a patient’s follow-up care in clinic. Arrangements should also be put in place for x-ray to receive notification of the numbers of patients that can be expected 48 hours in advance of the clinic.
Short-term
Short-term
2-4 weeks
2-4 weeks
Overbooking. Overbooking should be rationalised and overbooked/double-booked slots spread over the duration of the whole clinic.
Short-term 2-4 weeks
Templates. Clinic start and finish times should be changed to reflect the number of patients seen. A whole scale review of templates should be carried out with clinicians and outpatient management and alterations made accordingly. Consideration should be given to realistic start and finish times for clinics, practicability of moving fortnightly clinics to weekly and the impact that would have on rotations, staffing and room availability
Short-term
Medium-term
2-4 weeks
2-3 months
Capacity for Follow-ups. In order to reduce the numbers of follow-ups in clinic and relieve the stress on the department, it is recommended that clinical teams develop alternative ways to follow patients up (e.g. Telephone follow-up). This should include consideration for out-of-area patients to have follow-up diagnostics locally and only return to RNOH clinic if necessary. In addition, consideration should be given to a nurse or registrar triage system for patients wanting appointments brought forward It is recommended that a review and clinical assessment be considered out for long-term follow up patients in order to assess either suitability for onward referral to primary care/local hospital or discharge. Patients needing to return to clinic could then be triaged by a nurse as detailed above in order to assess suitability to return to RNOH clinics. Long term follow-up patients (yearly or two-yearly) could be booked using an outpatient partial booking list where a reminder is sent to patient 8 weeks before the patient needs to be seen prompting the patient to phone in and book. This would save on blocking clinics in advance and will reduce DNA rates.
Medium-term
Short-term Long-term Long-term
2-3 months
2-4 weeks
4-6 months
4-6 months

RNOH Service Improvement Team Page 8 of 17
May 2010
Referral and discharge criteria. Teams should consider the development of discharge criteria that is accessible and understood by middle grade doctors
Long-term
4-6 months
Booking process change. A new booking process for follow ups should be developed to avoid overbooking above tolerance levels.
Medium Term
2-3 months
Sarcoma patients. Teams in JRU are already working towards the separation of Sarcoma and Joint Reconstruction patients in clinic. It was also noted that the supporting nursing staff are often spending time in the clinic area with very little patient contact time during the clinic session. Consideration should be given to the redesign of the clinic template / patient pathway for new sarcoma patients following diagnosis to accommodate the breaking of bad news and facilitate the work of the Macmillan nursing team.
Ongoing
Medium-term
2-3 months
2-3 months
One stop clinics for admitted patients. Patients coming in for surgery would benefit from a one-stop service in outpatients once the decision to admit has been made. A leaner patient pathway could be implemented whereby patients are given a date to come in (TCI) during consultation and then sent straight to pre-operative screening, thus avoiding delays and repeated visits to the department. This is a process that is currently reported to be working well in the RNOH Foot and Ankle service and should be considered for general roll-out.
Long-term 4-6 months
General
Pagers at Stanmore. Patients who are experiencing delays in clinic at Bolsover street are given pagers and allowed to leave the premises. This eases congestion in the waiting areas and ensures that the patients do not miss their slot. This could be considered for Stanmore site.
Clinic Space. Restricted clinic space presents a substantial barrier to the management of demand and capacity in the department. it is recommended that additional rooms are found onsite and within local satellite clinics which can be used for outpatient consultation
OPD development should ensure the best possible utilisation of space for levels of demand and activity.
Refreshments. Discussions should be held with Medirest regarding extending the opening hours for the hot drinks facility at Stanmore site
Plasma screen / Television at Stanmore. Consideration should be given to visual distraction at Stanmore site
Signage at Stanmore. There is no clear sign over main reception. This can be confusing for patients as there are various desks and waiting areas within the department.
Medium-term
Short-term
Medium-Long term
Short-term
Short-term
Short-term
2-3 months
2-4 weeks
2-6 months
2-4 weeks
2-4 weeks
2-4 weeks
RNOH Service Improvement Team Page 9 of 17
May 2010
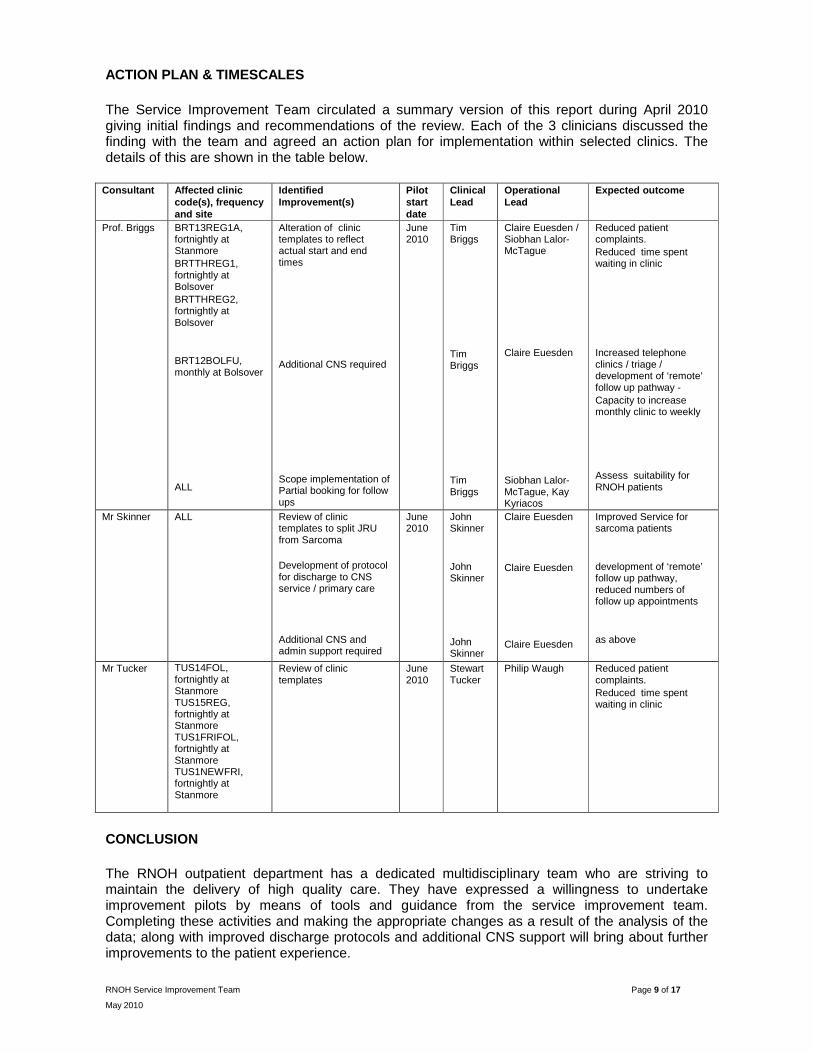
ACTION PLAN & TIMESCALES The Service Improvement Team circulated a summary version of this report during April 2010 giving initial findings and recommendations of the review. Each of the 3 clinicians discussed the finding with the team and agreed an action plan for implementation within selected clinics. The details of this are shown in the table below.
Consultant Affected clinic code(s), frequency and site
Identified Improvement(s)
Pilot start date
Clinical Lead
Operational Lead
Expected outcome
Prof. Briggs BRT13REG1A, fortnightly at Stanmore BRTTHREG1, fortnightly at Bolsover BRTTHREG2, fortnightly at Bolsover BRT12BOLFU, monthly at Bolsover ALL
Alteration of clinic templates to reflect actual start and end times Additional CNS required Scope implementation of Partial booking for follow ups
June 2010
Tim Briggs Tim Briggs Tim Briggs
Claire Euesden / Siobhan Lalor-McTague Claire Euesden Siobhan Lalor-McTague, Kay Kyriacos
Reduced patient complaints. Reduced time spent waiting in clinic Increased telephone clinics / triage / development of ‘remote’ follow up pathway - Capacity to increase monthly clinic to weekly Assess suitability for RNOH patients
Mr Skinner ALL Review of clinic templates to split JRU from Sarcoma Development of protocol for discharge to CNS service / primary care Additional CNS and admin support required
June 2010
John Skinner John Skinner John Skinner
Claire Euesden Claire Euesden Claire Euesden
Improved Service for sarcoma patients development of ‘remote’ follow up pathway, reduced numbers of follow up appointments as above
Mr Tucker TUS14FOL, fortnightly at Stanmore TUS15REG, fortnightly at Stanmore TUS1FRIFOL, fortnightly at Stanmore TUS1NEWFRI, fortnightly at Stanmore
Review of clinic templates
June 2010
Stewart Tucker
Philip Waugh Reduced patient complaints. Reduced time spent waiting in clinic
CONCLUSION The RNOH outpatient department has a dedicated multidisciplinary team who are striving to maintain the delivery of high quality care. They have expressed a willingness to undertake improvement pilots by means of tools and guidance from the service improvement team. Completing these activities and making the appropriate changes as a result of the analysis of the data; along with improved discharge protocols and additional CNS support will bring about further improvements to the patient experience.
RNOH Service Improvement Team Page 10 of 17
May 2010
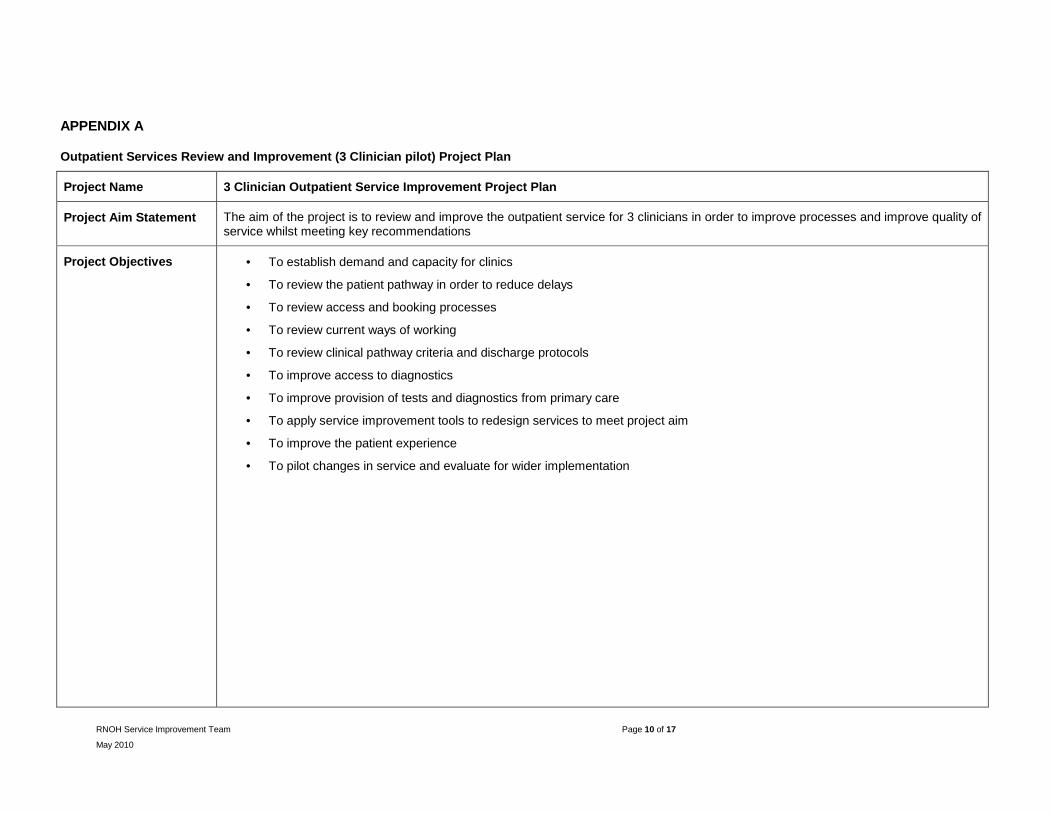
APPENDIX A
Outpatient Services Review and Improvement (3 Clinician pilot) Project Plan
Project Name 3 Clinician Outpatient Service Improvement Project Plan
Project Aim Statement The aim of the project is to review and improve the outpatient service for 3 clinicians in order to improve processes and improve quality of service whilst meeting key recommendations
Project Objectives
• To establish demand and capacity for clinics
• To review the patient pathway in order to reduce delays
• To review access and booking processes
• To review current ways of working
• To review clinical pathway criteria and discharge protocols
• To improve access to diagnostics
• To improve provision of tests and diagnostics from primary care
• To apply service improvement tools to redesign services to meet project aim
• To improve the patient experience
• To pilot changes in service and evaluate for wider implementation

RNOH Service Improvement Team Page 11 of 17
May 2010
Project Work stream Initiative/ Improvement Actions/Progress Milestone/Outcome
Milestone Date / outcome
Project team To establish project team � Identify key stakeholders
� Develop team
Project group with appropriate representation and understanding of roles
COMPLETE
Communication plan To ensure that stakeholders are well informed on project progress and share learning
� Identity key arenas for reporting on project progress i.e. internal meetings
Project progress is available to all
ONGOING
Demand and Capacity Determine current demand on service and capacity within the service for named clinicians
� Carry out Demand & Capacity work for each clinic
� Review clinic templates
� Develop Models for individual consultants
� Review room usage at both sites
� Review alternative venues for clinics
Report on demand and capacity to help determine service redesign
28/04/2010
Clinic observation and Data analysis
Determine current practice � Collect data - clinical case mix and outcomes
� Review of follow ups
� Process Map patient journey and compare with pathway
Report on observation to help determine service redesign
28/04/2010
Pathways
To work up criteria for referral and discharge
� Review current pathway
� Develop referral, diagnostic and discharge criteria
� Review alternatives to outpatient appointments
� Review current referral process
� Review current booking process
Pathways and Criteria in place 04/05/2010
One-stop Outpatient Services
To improve patient experience and reduce waste
� Review way patients attend for test for new and FU OPA
Robust process in place which reduces delays within OPD
04/05/2010
RNOH Service Improvement Team Page 12 of 17
May 2010
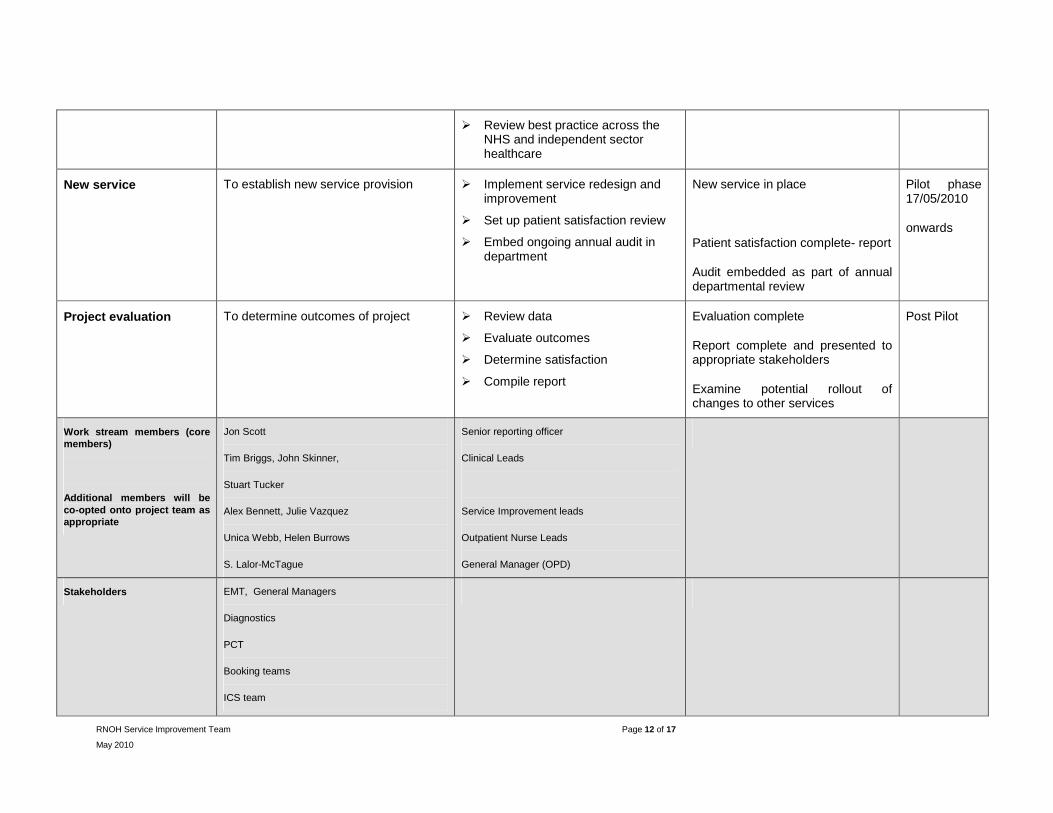
� Review best practice across the NHS and independent sector healthcare
New service To establish new service provision � Implement service redesign and improvement
� Set up patient satisfaction review
� Embed ongoing annual audit in department
New service in place
Patient satisfaction complete- report
Audit embedded as part of annual departmental review
Pilot phase 17/05/2010
onwards
Project evaluation To determine outcomes of project � Review data
� Evaluate outcomes
� Determine satisfaction
� Compile report
Evaluation complete
Report complete and presented to appropriate stakeholders
Examine potential rollout of changes to other services
Post Pilot
Work stream members (core members)
Additional members will be co-opted onto project team as appropriate
Jon Scott
Tim Briggs, John Skinner,
Stuart Tucker
Alex Bennett, Julie Vazquez
Unica Webb, Helen Burrows
S. Lalor-McTague
Senior reporting officer
Clinical Leads
Service Improvement leads
Outpatient Nurse Leads
General Manager (OPD)
Stakeholders EMT, General Managers
Diagnostics
PCT
Booking teams
ICS team

RNOH Service Improvement Team Page 13 of 17
May 2010
Project Plan
RNOH Service Improvement Team Page 14 of 17
May 2010
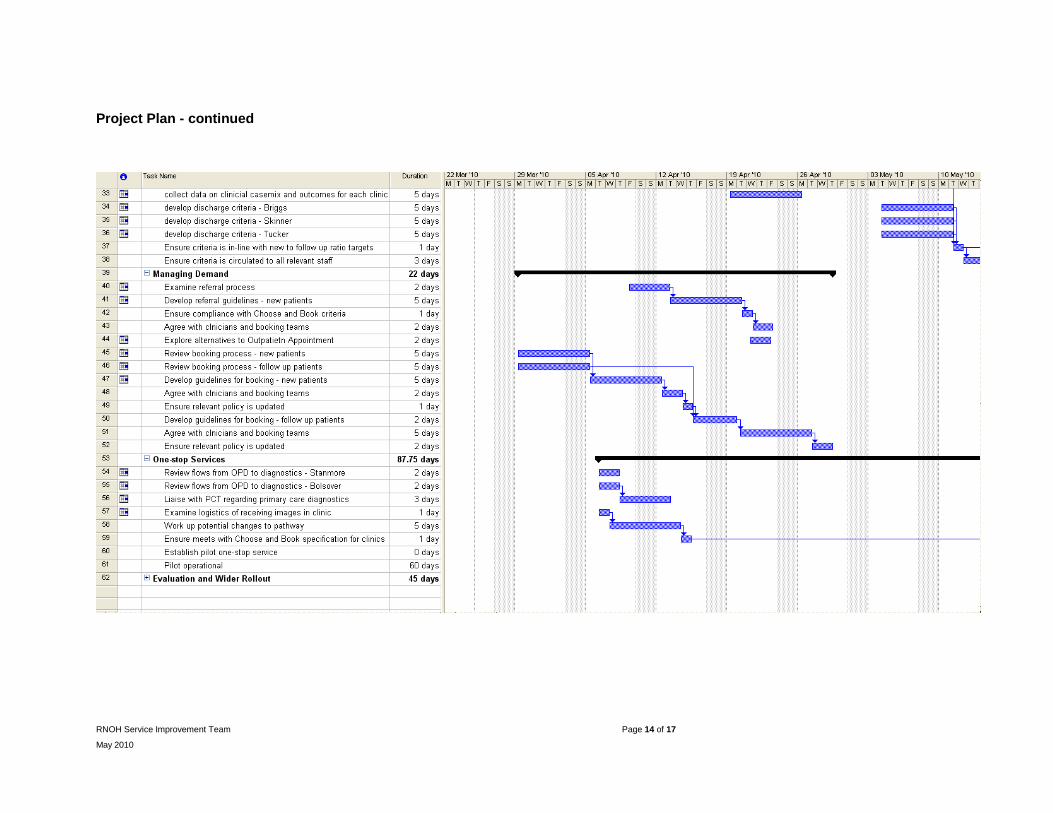
Project Plan - continued
RNOH Service Improvement Team Page 15 of 17
May 2010
APPENDIX B - Clinic Profiles
Professor Briggs
Co
nsu
ltan
t
Clin
ic C
od
e
Clin
ic D
escr
ipti
on
Sit
e
Wee
kday
Fre
qu
ency
Tim
e o
f d
ay
New
Slo
ts
Du
rati
on
of
New
slo
ts
Fo
llow
Up
Slo
ts
Du
rati
on
of
F/u
p s
lots
Co
mb
ined
slo
ts
Du
rati
on
of
co
mb
ined
slo
ts
To
tal S
lots
Ave
rag
e A
ctiv
ity
DN
A R
ate
Ave
rag
e n
um
ber
of
new
o
verb
oo
ked
Ave
rag
e n
um
ber
of
follo
w
up
s o
verb
oo
ked
Briggs BRT12BOLFU Long term follow up Bolsover Tuesday Monthly AM 0 0 12 15 0 0 12 4 1% 0 0
Briggs BRT13REG1A Registrar Stanmore Wednesday Fortnightly AM 0 0 31 10 0 0 31 60 12% 0 26 Briggs BRT14CBPM General Bolsover Thursday Fortnightly PM 8 20 2 10 0 0 10 15 8% 1 1 Briggs BRT14TUM Tumour Bolsover Thursday 3 a month PM 3 20 4 20 1 20 8 16 8% 3 3
Briggs BRT15NURSE
Nurse Specialist Telephone Stanmore Friday Weekly PM 0 0 12 15 0 0 12 33 0% 0 0
Briggs BRT1ADHOC Ad-hoc Stanmore any any any 0 0 0 0 13 15 13 9 8% 0 0
Briggs BRT1AM3N
Knee & Bone Tumour Stanmore Wednesday Fortnightly
All Day
13 20 32 10 0 0 45 52 8% 5 6
Briggs BRTTHREG1 Registrar Bolsover Thursday Weekly PM 0 0 13 15 0 0 13 27 7% 0 15 Briggs BRTTHREG2 Registrar Bolsover Thursday Weekly PM 0 0 13 15 0 0 13 20 9% 0 8

RNOH Service Improvement Team Page 16 of 17
May 2010
Mr Skinner
Co
nsu
ltan
t
Clin
ic C
od
e
Clin
ic D
escr
ipti
on
Sit
e
Wee
kday
Fre
qu
ency
Tim
e o
f d
ay
New
Slo
ts
Du
rati
on
of
New
slo
ts
Fo
llow
Up
Slo
ts
Du
rati
on
of
F/u
p s
lots
Co
mb
ined
slo
ts
Du
rati
on
of
co
mb
ined
slo
ts
To
tal S
lots
Ave
rag
e A
ctiv
ity
DN
A R
ate
Ave
rag
e n
um
ber
of
new
o
verb
oo
ked
Ave
rag
e n
um
ber
of
follo
w
up
s o
verb
oo
ked
Skinner SKIJ1CNSPM Nurse Specialist Bolsover Monday Weekly PM 0 0 12 15 0 0 12 10 5% 0 0
Skinner SKIJ1REGPM Registrar follow ups Bolsover Monday Weekly PM 0 0 15 10 0 0 15 26 10% 0 14
Skinner SKIJ1WDPM
Follow up post discharge from ward Bolsover Monday Weekly PM 0 0 6 10 0 0 6 9 7% 0 4
Skinner SKJ13AM Tumour Stanmore Wednesday Fortnightly AM 0 0 0 0 7 15 7 4 3.5% 0 0 Skinner SKJ13CNSAM CNS Stanmore Wednesday Fortnightly AM 0 0 21 15 0 0 21 20 9% 0 1 Skinner SKJ13REG Registrar Stanmore Wednesday Fortnightly AM 0 0 27 10 0 0 27 42 7% 0 16 Skinner SKJ14FEL Fellow Bolsover Friday Fortnightly PM 6 15 5 15 0 0 11 9 2% 0 0
Skinner SKJ15NURSE Nurse Specialist Stanmore Friday Weekly AM 0 0 12 15 0 0 12 11 0% 0 0
Skinner SKJ1ADHOC Ad-hoc Stanmore any any any 12 15 0 0 0 0 12 11 0% 0 0 Skinner SKJ1AM3N General Stanmore Wednesday Fortnightly AM 10 20 7 20 0 0 17 19 3.5% 1 3 Skinner SKJ1FEL2PM Fellow Stanmore Tuesday Weekly PM 4 20 8 10 0 0 12 12 4% 0 0 Skinner SKJ1PM1N General Bolsover Monday Weekly PM 8 15 4 10 0 0 12 19 7.5% 5 4
Skinner SKJ1TELWED Nurse Specialist Stanmore Wednesday Weekly AM 0 0 20 15 0 0 20 18 0% 0 0

RNOH Service Improvement Team Page 17 of 17
May 2010
Mr Tucker
Co
nsu
ltan
t
Clin
ic C
od
e
Clin
ic D
escr
ipti
on
Sit
e
Wee
kday
Fre
qu
ency
Tim
e o
f d
ay
New
Slo
ts
Du
rati
on
of
New
slo
ts
Fo
llow
Up
Slo
ts
Du
rati
on
of
F/u
p s
lots
Co
mb
ined
slo
ts
Du
rati
on
of
co
mb
ined
slo
ts
To
tal S
lots
Ave
rag
e A
ctiv
ity
DN
A R
ate
Ave
rag
e n
um
ber
of
new
o
verb
oo
ked
Ave
rag
e n
um
ber
of
follo
w
up
s o
verb
oo
ked
Tucker TUS14FOL Ward discharge Stanmore Thursday Fortnightly PM 0 0 10 15 0 0 10 10 4% 0 1
Tucker TUS15REG Registrar follow up Stanmore Friday Fortnightly
All Day 0 0 33 10 0 0 33 34 7% 0 3
Tucker TUS1ADHST Ad-hoc (registrar) Stanmore any any
All Day 0 0 0 0 14 30 14 15 4% 0 0
Tucker TUS1CONADH Ad-hoc (cons) Bolsover any any any 0 0 0 0 6 30 6 7 6% 0 0
Tucker TUS1FELADH Ad-hoc (Fellow) Stanmore Friday Monthly
All Day 0 0 0 0 14 30 14 11 18% 0 0
Tucker TUS1FRIFOL Follow up Stanmore Friday Fortnightly AM 0 0 18 10 0 0 18 19 6% 0 2 Tucker TUS1LECADH Ad-hoc Stanmore any any any 0 0 0 0 7 30 7 7 28% 0 0
Tucker TUS1NEWFRI New patients Stanmore Friday Fortnightly PM 6 20 0 0 0 0 6 8 3% 1 0
Tucker TUS1TELCL Telephone clinic Stanmore Monday Weekly AM 0 0 5 30 0 0 5 5 0% 0 0


















