Pleural cavities Fig. 17-11 Diaphragm Right pleural cavity Left pleural cavity.
Upload
makoto-nonakaCategory
view
212download
0
Surg Today (2005) 35:22–27DOI 10.1007/s00595-004-2894-2
Outcome Following Surgery for Primary Lung Cancer with InterlobarPleural Invasion
Makoto Nonaka1, Daisuke Kataoka1, Shigeru Yamamoto1, Naoya Horichi2, Yoshimitsu Ohgiya3,Miki Kushima4, Toshiaki Kunimura5, and Toshihiro Takaba1
1 First Department of Surgery, 2 First Department of Internal Medicine, 3 Department of Radiology, 4 Department of Hospital Pathology, and5 First Department of Pathology, Showa University School of Medicine, 1-5-8 Hatanodai, Shinagawa-ku, Tokyo 142-8666, Japan
Key words Primary lung cancer · Interlobarpleural invasion · Prognosis · Tumor-node metastasisclassification
Introduction
Primary lung cancer is classified based on the tumor-node metastasis (TNM) staging system defined by theInternational Union against Cancer (UICC).1 In thisclassification a tumor that directly invades the pleuralcavity and parietal pleura (P3 lesion) is categorized asT3.1 However, the UICC has not clearly defined whatT factor should be assigned to a tumor that invadesthrough the interlobar pleura into an adjacent lobe.1
The Japan Lung Cancer Society has decided that a trueP3 tumor should be categorized as T3 while a tumor thatdirectly invades an adjacent lobe (interlobar P3) shouldbe categorized as T2.2,3 To study whether interlobar P3cancers should be categorized as T3 or T2, the charac-teristics and survival in patients with surgically treatedprimary lung cancer were analyzed.
Patients and Methods
A total of 322 patients with primary lung cancer under-went a surgical resection at Showa University Hospitalfrom 1987 to 2000. Among them, 50 patients who hadinterlobar P3 tumors were compared with the 272 pa-tients without interlobar P3. The clinicopathologic dis-ease stage and histologic typing were determined basedon the General Rules for Clinical and PathologicalRecord of Lung Cancer as revised in 1999.2 The T and Ncategories were determined by a clinicopathologic ex-amination of surgical specimens. The M category wasdetermined preoperatively by computed tomography ofthe chest and abdomen, magnetic resonance imaging of
AbstractPurpose. To determine whether interlobar pleural inva-sion into the adjacent lobe (interlobar P3) should beassessed as T3 according to the tumor-node metastasisclassification.Methods. Surgically treated patients with primary lungcancer (n � 322) were analyzed.Results. Tumors with interlobar P3 had a significantlylower incidence of mass screening detection, a higheroccurrence rate of squamous cell carcinoma, and alarger tumor diameter than tumors without interlobarP3. The lymph node metastatic rate did not differ be-tween the patients with and without interlobar P3. The5-year survival rate of patients with interlobar P3 was63% and the rates of other patients were 56% with T1disease, 57% with T2, 31% with T3, and 19% with T4.The survival rate for patients with interlobar P3 washigher than for those with T3 without interlobar P3(P � 0.05). The 5-year survival rate of the patients withinterlobar P3 was lower in adenocarcinoma (39%) thanin squamous cell carcinoma (69%, P � 0.01). The re-sults were similar when the analysis was restricted topatients without lymph node metastasis. In adenocarci-noma, the survival rate for interlobar P3 was betweenthe rates for T2 (53%) and T3 (13%) without interlobarP3, whereas in squamous cell carcinoma, the survivalrate for interlobar P3 was between the rates for T1(88%) and T2 (54%) without interlobar P3.Conclusion. Tumors with interlobar P3 should be classi-fied as T2 only in squamous cell carcinoma.
This study was presented at the 10th World Conference of theInternational Association for the Study of Lung Cancer, heldin Vancouver, Canada, August 10–14, 2003Reprint requests to: M. NonakaReceived: September 4, 2003 / Accepted: July 13, 2004

23M. Nonaka et al.: Lung Cancer with Interlobar Invasion
the brain, and bone scintigraphy. The results were ex-pressed as the mean � standard error of the mean, anddifferences in the numbers of patients in each groupwith a given feature were analyzed with the chi-squaredtest. Survival was measured as the time from the opera-tion until either death or the most recent follow-upexamination. The survival rates, including deaths notrelated to cancer, were calculated using the Kaplan-Meier method; curves were compared using thelog-rank test. Significance was defined by a value ofP less than 0.05.
Results
The patients without interlobar P3 included 189 malesand 83 females, and the patients with interlobar P3 in-cluded 37 males and 13 females. The gender distributiondid not differ significantly (Table 1). The mean age ofthe patients without interlobar P3 was 61.9 � 1.5 yearsold while that of the patients with interlobar P3 was 64.7� 0.6 years old (not significant, Table 1).
The tumors were detected by mass screening in 88patients and, among them, 7 tumors were interlobar P3.The tumors were detected by other means in 234 pa-tients and, among them, 43 tumors were interlobar P3.The patients with interlobar P3 demonstrated a signifi-cantly lower mass screening detection rate than the pa-tients without interlobar P3 (P � 0.05, Table 1).
The tumor types in the 272 patients without interlo-bar P3 included 177 adenocarcinomas (AD, 65%); 75squamous cell carcinomas (SQ, 28%); and 20 tumors ofother types. Of the 50 patients with interlobar P3, 28(56%) had SQ; 19, AD (38%); and 3, other types. Thedifference in the proportion of SQ was highly significant(P � 0.01). Of all 103 SQ, 28 (27%) were interlobar P3,while only 19 of 196 AD (10%) were interlobar P3 (P �0.01, Table 1).
Among the 272 patients without interlobar P3, 97were classified as T1; 95, T2; 34, T3; and 46, T4. The T3tumors included parietal pleural invasion in 13 patients,the chest wall in 14, the pericardium in 5, and the dia-phragm in 2. The T4 tumors included intrapulmonarymetastasis in the same lobe in 27 patients and otherfactors in 19. Among the 50 patients with inerrlobar P3,provided that the interlobar invasion was not used toscore the T factor, 7 were classified as T1; 27 as T2; 10 asT3; and 6 as T4 (intrapulmonary metastasis in the samelobe in 4 patients, other factors in 2) (Table 1). The T1distribution was lower in the patients with interlobar P3than in the patients without interlobar P3 (P � 0.01).
The size of lung cancer without interlobar P3 was34.6 � 1.1 mm, while the size of those with interlobar P3was 42.5 � 2.8mm. The cancers representing interlobarP3 were significantly larger than the others (P � 0.01,Table 1). Among interlobar P3 tumors, SQ weresignificantly larger than AD (49.9 � 3.6mm vs 33.6 �3.9mm, P � 0.01).
Table 1. Patient distribution
Interlobar P3 (n � 50) Others (n � 272) P value
Male 37 189Female 13 83 n.s.Age (years) 61.9 � 1.5 64.7 � 0.6 n.s.Mass screening 7 81Others 43 191 �0.05AD 19 177SQ 28 75Others 3 20 �0.01T1 7 97T2 27 95T3 10 34T4 6 46 �0.01Tumor size (mm) 42.5 � 2.8 34.6 � 1.1 �0.01�3 cm 11 135�3 cm 39 137 �0.01�3cm (AD) 9 111�3cm (AD) 10 66�3cm (SQ) 2 24�3cm (SQ) 26 51N0 27 146N1 12 60N2 11 66 n.s.
AD, adenocarcinoma; SQ, squamous cell carcinoma; n.s., not significant

24 M. Nonaka et al.: Lung Cancer with Interlobar Invasion
A tumor diameter of less than 3cm was observed in146 patients and 11 patients were interlobar P3 (8%). Atumor diameter over 3 cm was observed in 176 patientsand 39 patients were interlobar P3 (22%). Interlobar P3was observed more frequently in tumors measuringover 3cm in size than in tumors measuring less than3 cm (P � 0.01). In AD (196 patients), 120 patients hadtumors less than 3cm and 9 patients were interlobar P3(8%), while 76 patients had tumors measuring over 3 cmin size and 10 patients were interlobar P3 (13%); thetumor size did not reflect the interlobar P3 invasion inAD (not significant). In SQ (103 patients), 2 patientshad interlobar P3 among the 26 patients with tumorsmeasuring less than 3 cm in size (8%), while 26 patientshad interlobar P3 among the 77 patients with tumorsmeasuring over 3 cm in size (34%); therefore, the tumorsize reflected the interlobar P3 invasion in SQ (P � 0.01,Table 1).
The rate of mediastinal or hilar lymph node (LN)metastasis in patients with interlobar P3 (23 of 50 pa-tients, 46%) was similar to that in the patients withoutinterlobar P3 (126 of 272 patients, 46%; not significant).In AD, mediastinal or hilar LN metastasis was observedin 8 of 19 patients with interlobar P3 (42%) and it wasalso observed in 79 of 177 patients without interlobar P3(45%, not significant). In SQ, mediastinal or hilar LNmetastasis was observed in 13 of 28 patients with inter-lobar P3 (46%) and in 32 of 75 patients without inter-lobar P3 (52%, not significant).
Among the 50 patients with interlobar P3, 13 under-went a single lobe resection with a partial resection ofthe adjacent lobe; 35 received a bilobectomy or pneu-monectomy; and 2 had only a thoractomy. The inter-lobar P3 patients undergoing a single lobe resectionwith a partial resection of the adjacent lobe included 8with AD and 5 with SQ. The 35 patients undergoing abilobectomy or pneumonectomy included 10 with AD,23 with SQ, and 2 with other tumor types. Patients withSQ tended to undergo bilobectomy or pneumonectomymore often than the patients with AD (P � 0.05) be-cause many AD arose peripherally while SQ often arosemore centrally. Peripheral interlobar P3 lung cancerswere easily removed by a single lobe resection with apartial resection of the adjacent lobe, but more centrallysituated cancers with interlobar invasion required eithera bilobectomy or pneumonectomy.
The 5-year survival rates of the patients with inter-lobar P3 were 39% in AD and 69% in SQ (P � 0.01).The 5-year survival rates of the patients with interlobarP3 without LN metastases were 39% in AD and 75% inSQ (P � 0.01).
To compare the survival rates between the patientswith interlobar P3 and those without interlobar P3, 31T4 patients with interlobar metastasis in the same lobe(PM1) were excluded from the survival analysis. The 5-
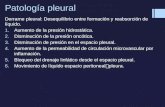
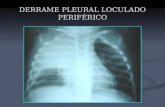
year survival rate of patients with interlobar P3 was63% (Fig. 1), while the 5-year survival rates of thosewithout interlobar P3 were 56% in T1, 57% in T2, 31%in T3, and 19% in T4 (Fig. 2). The survival rate forpatients with interlobar P3 was significantly higher for
Fig. 1. Survival curve of patients with interlobar P3. The T4patients with interlobar pulmonary metastasis in the samelobe were excluded from the survival analysis in order tocompare the survival rates in patients with and without inter-lobar P3 according to the true T factor alone
Fig. 2. Survival curves of patients without interlobar pleuralinvasion. The T4 patients with interlobar pulmonary metasta-sis in the same lobe were excluded from the survival analysisin order to compare the survival rates in patients with andwithout interlobar P3 according to the true T factor alone.Circles, T1; triangles, T2; squares, T3; crosses, T4

25M. Nonaka et al.: Lung Cancer with Interlobar Invasion
the T3 patients without interlobar P3 (P � 0.05), whilethe survival rates did not differ between the patientswith interlobar P3 and the T2 patients without interlo-bar P3. The 5-year survival rate for patients with inter-lobar P3 (63%) was significantly higher than that forthose with parietal pleural invasion without interlobarP3 (23%, P � 0.05). In AD, the 5-year survival rate forpatients with interlobar P3 was 39%, while the rate forthose without interlobar P3 was 50% (not significant).The 5-year survival rates for patients without interlobarP3 were 54% in T1, 53% in T2, 13% in T3, and 12% inT4. In SQ, the 5-year survival rate of the patients withinterlobar P3 was 69%, while the rate for those withoutinterlobar P3 was 70% (not significant). The 5-year sur-vival rates for patients without interlobar P3 were 88%in T1, 54% in T2, 58% in T3, and 40% in T4. In AD, thesurvival rate with interlobar P3 was between the ratesfor T2 (53%) and T3 (13%) without interlobar P3whereas in SQ, the survival rate with interlobar P3 wasbetween the rates for T1 (88%) and T2 (54%) withoutinterlobar P3.
The survival of the patients having no LN metastaseswas analyzed in terms of interlobar P3 invasion. The 5-year survival rate of these patients with interlobar P3was 78% (Fig. 3), while that of those without interlobarP3 was 87% in T1, 61% in T2, 47% in T3, and 0% in T4disease (Fig. 4). The survival rate for patients with inter-lobar P3 was significant higher than for T3 patientswithout interlobar P3 (P � 0.05); in fact it was notdifferent from that for T2 patients without interlobar
P3. The 78% 5-year survival rate for patients with inter-lobar P3 was significantly higher than that for those withparietal pleural invasion in the absence of interlobar P3(50%, P � 0.05).
Postoperative local recurrence or distant metastasiswas observed in 16 patients with interlobar P3 (16 of 50,Table 2). The local recurrence rate did not differ be-tween the patients undergoing a lobectomy with a par-tial resection (3 of 13 patients) and those undergoing abilobectomy or pneumonectomy (7 of 35 patients).When postoperative survival with interlobar P3 wascompared according to the surgical procedure, the 5-year survival rate for patients with a lobectomy in-cluding a partial resection was 64%, while that for abiobectomy was 75%, and that for a pneumonectomywas 62%; no significant differences were observed be-tween these rates.
Discussion
A lung cancer that invades the parietal pleura is catego-rized as T3 regardless of its size.1,2,4 Invasion of theparietal pleura upgrades the T factor, and the tumor isconsidered to be more invasive. However, the T classi-fication according to the UICC is not clear for inter-lobar pleural invasion;1 whether a lung cancer withinterlobar pleural invasion is more invasive or progres-
Fig. 3. Survival curves of patients with interlobar P3 withoutlymph node metastasis. T4 patients with interlobar pulmonarymetastasis in the same lobe were excluded from the survivalanalysis in order to compare the survival rates in patients withand without interlobar P3 according to the true T factor alone
Fig. 4. Survival curves of patients without interlobar pleuralinvasion but no lymph node metastasis. T4 patients with inter-lobar pulmonary metastasis in the same lobe were excludedfrom the survival analysis in order to compare the survivalrates in patients with and without interlobar P3 according tothe true T factor alone. Circles, T1; triangles, T2; squares, T3;crosses, T4

26 M. Nonaka et al.: Lung Cancer with Interlobar Invasion
Table 2. Postoperative local recurrence or distant metastasis in patients with interlobarP3 according to surgical procedure
Recurrence Metastasis Disease-free Total
Lobectomy with partial resection 3 2 8 13Bilobectomy 2 1 9 12Pneumonectomy 5 1 17 23Probe thoracotomy 2 0 0 2
Total 12 4 34 50
sive than one without interlobar pleural invasion re-mains uncertain. Whether the background data orprognosis differs between lung cancers with interlobarpleural invasion and those with parietal pleural invasionalso remains an unresolved question.
We observed 50 interlobar P3 patients among 322patients. The rate is high when compared with otherreports, and one explanation is that a large number ofSQ measuring over 3cm in size is included in this studyperiod. In SQ, tumors measuring over 3 cm in sizeshowed a high rate (26/77 patients) of interlobar P3.
Studies by Morita et al. and Suzuki et al. found thatthe distribution of histopathologic types did not differaccording to the interlobar P3 status,5,6 while Sensaki etal. reported that patients with interlobar P3 had rela-tively more AD than patients without interlobar P3.7
However, we found that patients with interlobar P3 hadrelatively more SQ than patients without interlobar P3.This difference may reflect a larger size in tumors withinterlobar P3 than in tumors without interlobar P3 inour study because the SQ tumor was larger in diameterthan the AD tumor.
In our study, if interlobar invasion was not used toscore the T factor, then the distribution of the “pure” Tfactor was statistically different between the tumorswith and without interlobar P3. In addition, the maxi-mum diameter of tumors with interlobar P3 was signifi-cantly larger than for tumors without interlobar P3.Since the mean diameter of the tumors with interlobarP3 was over 3 cm, tumors with interlobar P3 should thusnot be categorized as T1.
Although the tumor size was larger in patients withinterlobar P3 than in those without interlobar P3, theLN metastatic rate did not differ between the patientswith and without interlobar P3. Lung cancers with inter-lobar invasion would not seem more progressive thancancers without interlobar P3 in terms of the LN prolif-eration. Morita et al. also reported that the N distribu-tion did not differ according to the degree of interlobarpleural invasion.5
This study excluded PM1 patients from the survivalanalysis. Although the new TNM classification catego-rizes PM1 as T4,1,2 this classification remains controver-sial. Many authors have demonstrated the survival rate
for patients with PM1 to be significantly higher for pa-tients with T4 without PM1.8 To compare the prognosisof patients with and without interlobar P3 according tothe “pure” T factor, the PM1 patients were excludedfrom the present postoperative survival analysis.
The 5-year survival rate of the patients with interlo-bar P3 was 63% and this rate is favorable in comparisonto other reports. The rates were reported to be 39% byMorita et al., 44% by Suzuki et al., 34% by Miura et al.,and 37% by Okada et al.5,6,9,10 In our study, the prognosisof the patients with interlobar SQ was extremely highbut the survival of the patients with interlobar AD wassimilar to the findings of other reports. As a result, thehistological type might be a key factor in the prognosisof patients with interlobar pleural invasion.
The prognosis for patients with interlobar P3 provedto be better than for patients with T3 without interlobarP3; in fact, the prognosis of patients with interlobar P3was the same as that for T2 patients without interlobarP3. This outcome pattern was also true when the analy-sis was limited to patients without LN metastasis. Al-though a tumor that invades through the interlobarpleura into an adjacent lobe is technically “P3,” thuspresumably considered to be T3, interlobar P3 tumorsshould not be considered T3 given the patient distribu-tion and the prognosis. Our study supports the decisionof the Japan Lung Cancer Society to classify interlobarP3 lesions as T2.3 However, controversy persists as tohow the P factor is related to the T factor in these cases,and additional study is thus warranted.
Controversy prevails concerning the optimal choiceof operation for lung cancer with interlobar P3. For-merly, the Japan Lung Cancer Society determined in1983 that when either a bilobectomy or pneumonec-tomy is performed for lung cancer with interlobar P3without parietal pleural invasion (i.e. P0,1,2), the tumorshould be categorized as T1 or 2. Meanwhile, when asingle lobe resection with a partial resection of the adja-cent lobe is performed for lung cancer with interlobarP3 without parietal pleural invasion (i.e. P0,1,2), thetumor should be categorized as T3. Sagawa et al. re-ported that survival was worse after a lobectomy with apartial resection than after a bilobectomy.11 Sensaki etal. showed that local recurrence was observed in pa-

27M. Nonaka et al.: Lung Cancer with Interlobar Invasion
tients after a lobectomy with a partial resection but wasnot seen in patients after a bilobectomy.7 Meanwhile,Morita et al. and Okada et al. described that postopera-tive survival did not differ between patients who re-ceived a lobectomy with a partial resection and thosewith either a bilobectomy or pneumonectomy.5,10 In ourstudy, the local recurrence rate and postoperative prog-nosis did not differ according to the surgical procedure.Accordingly, the operation should be selected accord-ing to the T factor and the lesion site, and neither abilobectomy nor a pneumonetomy should be routinelyperformed.9,10
References
1. UICC. Lung and pleural tumors. In: Sobin LH, Wittekind C,editors. TNM classification of malignant tumors. 5th ed. NewYork: Wiley; 1997. p. 91–100.
2. The Japan Lung Cancer Society. General rule for clinical andpathological record of lung cancer 5th ed. (in Japanese). Tokyo:Kanehara; 1999.
3. Kobayashi K, Yasumitsu T. A complement of general rule forclinical and pathological record of lung cancer, 5th ed. (inJapanese). Haigan (Jpn J Lung Cancer) 1999;39:preface.
4. Nonaka M, Kadokura M, Kataoka D, Yamamoto S, Horichi N,Kushihashi T, et al. The outcome of surgically treated T3 lung
cancer invading adjacent structures. Showa Univ J Med Sci2001;13:271–8.
5. Morita R, Kaneko K, Nakamura S, Akaishi T, Yamazaki N.Should interlobar pleural invasion be categorized as T2 or T3? (inJapanese with English abstract). Haigan (Jpn J Lung Cancer)2002;42:583–7.
6. Suzuki H, Shio Y, Ohsugi J, Higuchi M, Fujii K, Kanno R, et al.Clinical study for adjacent lobe invasion beyond the interlobarpleura in non-small-cell lung cancer (in Japanese with Englishabstract). Haigan (Jpn J Lung Cancer) 2002;42:163–7.
7. Sensaki K, Kikuchi K, Kase K, Abe Y, Ozeki Y, Takagi K, et al.Result of surgical treatment on interlobar pleural invasion (p3)lung cancer (in Japanese with English abstract). Kokyuki Geka(Jpn J Chest Surg) 1990;4:765–8.
8. Nonaka M, Kadokura M, Yamamoto S, Kataoka D, Michihata T,Inoue K, et al. Surgically treated primary lung cancer withsynchronous intrapulmonary metastasis in the same lobe. In:proceedings of the 33rd World Congress of the InternationalCollege of Surgeons. Bologna: Monduzzi Editiore; 2002. p. 199–202.
9. Miura H, Taira O, Uchida O, Kato H. Invasion beyond interlobarpleura in non-small cell lung cancer. Chest 1998;114:1301-4.
10. Okada M, Tsubota N, Yoshimura M, Miyamoto, Y, Matsuoka H.How should interlobar pleural invasion be classified? Prognosis ofresected T3 non-small cell lung cancer. Ann Thorac Surg 1999;68:2049–52.
11. Sagawa M, Saito Y, Takahashi S, Endo C, Usuda K, Sugama K, etal. Relationship between operative procedure and prognosis ofpatients with interlobar invading lung cancer lesions (in Japanesewith English abstract). Haigan (Jpn J Lung Cancer) 1993;33:323–31.