
ously due to deprivation of landular secretion, it w natual to
33
STUDS IN ACROMEGALY V. TE MICROSCOPICAL STRUCTURE OF THr ADENOMAS IN ACMOXEGAUIC DYSPixulTARISM (uGmvE ACROUEGALY) PucviL BAIzY AD HARVEY CumIN (From 1k Swgical Clinkc .d Laboratoy of 1k Pd. BadS Brigh.m Hospial, INTRODUCTION It is the purpose of this paper further to descibe a pituitary dis- order that appears to be associated with an addophilic adenoma of foetal type and in which the constitutional evidences of glandular oversecretion are so light or so masked by of gandular in - dency that they have usally been disregarded. For this disorder we have come to employ the desigation ive acromegaly. More thn twenty years elapsed after Marie'l gave its name to acromegaly before it was possible to say with any assurance that the hgphic features of the malady he had desbed wre actually pituitary in origin and in all probability an expression of glandular overaction. Another twenty years passed before this hy- pothesis received definite proof through the production first of ex- perimental gism in rats (Evans and Long u), and more recently of acromegalic gigantismn in the dog (Putnam, Ted and Benedict O9) by the parenteral injection of extracts of the anterior lobe. In the interval the chief arguments in favor of this hypothesis were based almost wholy on the negative evidence of experimental canine hypophysectomies (i908-9) Wkhich show that adult animals (Crowe, Cushing and H ) became thereby adipose and sex- ually dystrophic and that young animals (Aschner') remained dwarfed and sexually infantile. As these disturbances were obvi- ously due to deprivation of landular secretion, it w natual to assume that the overgowth of acomegaly and gigantism repre- sented the opposite state due to an excess of secretion. This as- sumption received further support from the apparent subsidence in. size in the extrities of the first few acrmegalic patients that had been succesfuly operated upon (Hochenegg,4 Cushing '). &cavuI for Dub&t;iO Augt Io, I928. S4S
Transcript of ously due to deprivation of landular secretion, it w natual to

STUDS IN ACROMEGALYV. TE MICROSCOPICAL STRUCTURE OFTHr ADENOMAS IN
ACMOXEGAUIC DYSPixulTARISM (uGmvE ACROUEGALY)
PucviL BAIzY AD HARVEY CumIN
(From 1k Swgical Clinkc .d Laboratoy of 1k Pd. BadS Brigh.m Hospial,
INTRODUCTION
It is the purpose of this paper further to descibe a pituitary dis-order that appears to be associated with an addophilic adenoma offoetal type and in which the constitutional evidences of glandularoversecretion are so light or so masked by of gandular in -dency that they have usally been disregarded. For this disorderwe have come to employ the desigation ive acromegaly.More thn twenty years elapsed after Marie'l gave its name to
acromegaly before it was possible to say with any assurance thatthe hgphic features of the malady he had desbed wreactually pituitary in origin and in all probability an expression ofglandular overaction. Another twenty years passed before this hy-pothesis received definite proof through the production first of ex-perimentalgism in rats (Evans and Long u), and more recentlyof acromegalic gigantismn in the dog (Putnam, Ted and Benedict O9)by the parenteral injection of extracts of the anterior lobe.In the interval the chief arguments in favor of this hypothesis
were based almost wholy on the negative evidence of experimentalcanine hypophysectomies (i908-9) Wkhich show that adult animals(Crowe, Cushing andH ) became thereby adipose and sex-ually dystrophic and that young animals (Aschner') remaineddwarfed and sexually infantile. As these disturbances were obvi-ously due to deprivation of landular secretion, it w natual toassume that the overgowth of acomegaly and gigantism repre-sented the opposite state due to an excess of secretion. This as-sumption received further support from the apparent subsidence in.size in the extrities of the first few acrmegalic patients that hadbeen succesfuly operated upon (Hochenegg,4 Cushing ').
&cavuI for Dub&t;iO Augt Io, I928.S4S

BAILEY AND CUSHING
Though there was still considerable confusion in regard to theindependent function of anterior as opposed to posterior lobe andthough the hypothalamic syndrome was as yet unappreciated, onthe basis of these experimental and clinical observations the seniorauthor in I909 6 ventured to describe pituitary disorders as divisiblein a general way into states of hyper- and of hypopituitarism. Theexistence of intermediary or transitional states was however recog-nized and in the following year an address on the subject 8 wasconcluded with the statement:
"It may be expected: (i) that in all cases of original hyperpituitarism asso-ciated with tumor, the functional end-result will be hypopituitarism; and(2) that in many of the cases in which existing hypopituitarism is the strikingfeature traces at least of an early tendency to hyperpituitarism can be detected.These mixtures of the two syndromes of glandular over- and under-activity aremost conveniently designated as dyspituitarism."
In a subsequent monograph 7 dealing with pituitary disorders ingeneral, chief attention was paid to the mechanical effects of intra-and extrasellar tumors of various sorts on the structures in theneighborhood of the gland and but little attention to. the histo-pathological nature of the lesions themselves. As a matter of fact,at that time (I9I2) the character of the glandular enlargement evenin acromegaly was but poorly understood and frequent recourse washad to the non-committal term struma in describing it. These" strumas," particularly when associated with hypopituitarism, wererecognized as having adenomatous characteristics and to be com-posed either of chromophobe or of chromophile cells, but in the caseof acromegaly it was not clear whether the lesion represented adiffuse functional hyperplasia of the chromophilic elements of theanterior lobe or whether it was actually an adenomatous tumorcomposed of these elements.Even Benda,4 who in I9OI was the first carefully to study and
compare the hypophysial changes in a series of acromegalics, issomewhat obscure in his description of the lesion which he calledstruma hyperplastica or adenomatosa; for though he recognized inthree of his four cases "the extraordinary increase of granular(acidophilic) gland-cells" in the lesions, he says that:
"The acromegalic hypophysial tumors diverge in unmistakable ways from thehabits of other diffuse organ-hyperplasias. On the one hand the tumor-char-acter is outspoken even in the smaller tumors by the sharply cut boundary of
546

ADENOXAS IN ACOGAIC DSFITUTAR
the growth; mn the other hand hitkglly the anakgnat of the gcells is neier absolutely lie that of the adult norof e foetal on. It remain an atypical fouin which mn s s the border of what we muscal malnant."
Unfortunately subsequent investigators were unable to substan-tiate Benda's views; whether this was from failure to employ suffi-cdenty ific methods of treating the tisses or because the hypo-physial "strumas" tey nced to study were not from cases ofactual acromegaly is not now possible to determine. The latter isthe more probable xlanation since more than ten years elapbefore it came slowly to be recgized that by far the most commonform of pituitary tumor was unassoated with acromegaly and wasa chromophobe type of adenoma which had been regarded previouslyas a smatous process.In 1921 Bailey and Davidoff,3 in the study of the tissues which
had been secured at operation in this dinic from thirty-five patientswith full-blown acromegaly, found, in complete agreemet withBenda, that almost without exception they were adenomas whosecels contained akddophilic granules, though in some cases these so-called alha ules were present only in small numbers in scatteredacls. Four years later, in another paper from this linic dealingfrom a general standpoint th pituitary adenas of al sorts, Dottand Bailey12 came to the condusion that not only might an acro-megalic show sgns of pituitary infficicy late in the course of themalady but that "in many cases at least, the features ofand of the hypopituitary syndrome develop synchnously ratherthan in sequence." They singled out from the series which thencomprised I62 verified adomas, thirtee exa es of what, inwant of a better term, they called "mixed types," the cinicalhistoxy of one of the patiets having bee inuded (Case VII) intheir report
MATERIL AND M ODS
In the hope of ding furte light on this obscure "mixed"syndrome, other examles of which have since come under obser-vation, we have undertaken the present study with the purpose ofdetermining whether it might be possible to correlate the degree ofeosnophlia found in an adenoma with the Moxistent dinical pictureWith this end in view the tissues from a hundred consective
S47

BAILEY AND CUSHING
adenomas that had been operated on between December 21, I92I,and January i, I927, and from which sufficient material for studyhad been secured and properly fixed, were re-examined. Almostwithout exception the tumors had attained sufficient size to affectvision by pressure on the chiasm, which was the primary reason forthe operation. We are therefore not here concerned with thoserare instances of acromegaly, of which Lewis17 and more recentlyKrumbhaar16 have recorded examples, due apparently to a func-tional hyperplasia of the anterior lobe without actual tumefaction.The method for identification of the alpha-granules already de-
scribed by one of us,2 of using on Regaud-fixed tissue the neutraldye made by a combination of ethyl-violet and orange-G, wasemployed throughout.
CLASSIFICATION
From a purely histological standpoint and with complete disregardof the associated clinical symptoms, such a series of adenomas maybe divided into six groups with the typical granular chromophilicadenoma of acromegaly at one end of the scale, the typical non-granular chromophobe adenoma at the other end, and with fourintermediary types of gradations, as follows:TYPE I (Fig. i). This is a highly eosinophilic adenoma which
consists of large, polygonal or rounded cells that lie in a loose massin which there is no stroma of connective tissue and practically novascular sinuses. The cells which have distinct boundaries, varygreatly in size and possess an abundant coarsely granular cytoplasm,often transformed centrally into a hyaline mass so that many nudeiare excentrically situated and crescentic in form. The nuclei arevesicular and show great variability in size. Multinucleated cellsare numerous. Crescent cells are also found. Practically all the cellsare packed with alpha-granules, often of large size.TYPE II (Fig. 2). This also is a definitely eosinophilic adenoma
though of less exaggerated type. The cells have the same sharpboundaries, abundant cytoplasm and vesicular nuclei of varying size.There is no connective tissue stroma and vascular sinuses are rare.The general structure however tends to be more compact so that thecells are largely polygonal and the cytoplasm has rarely undergonethe central hyaline change with resultant excentric position anddeformation of the nuclei. Multinucleated cells are also less fre-
548

ADENOXAS IN ACROGALIC DYSPTUITARIS9
quently encountered. Alkough many o-gralar ceUs are presenmost of hem contain large n bs of alpha-granles.TYE H (Fig. 3). The turs of this group are those descbed
by Dott and Bailey 12 as "mixed adenomas." Lie the above theyconsist of a compact mass of polygonal cells with well definedboundaries and vesicular nucleL The cells however have less abund-ant cytoplasm and multinudear cells are rarely found. There is nostroma but vascular sinuses are rather numerous. In the periphery ofa variabl number of the cels a thin ring of alpha-granueks is demon-strable.TwPE IV (Fig. 4). The tumors of this group differ from the pre-
ceeding in that the nudei are not so consistently vesicular and noalpha-granuks are demonstrabl. W-ithout a speific stain for thegranules it would scacely be possible to distingish these adenomasfrom those of Type m.*TYPE V (Fig. 5). In these tumors there may sometimes be a
poorly developed stroma, but the vasular sinuse are fairly numer-ous and the elongated neoplastic cells sometimes appear to radiatefrom them. Cellular boundaries are rather indistnct. The rela-tively scanty cytoplasm of the cells is less deeply stained than in theclls of Type IV and the nudei are of uniformly maller size andhave a heavier chromatinic network. No alpha-granules are present.TYPE VI (Fig. 6). These adenomas are dharacterized by a stroma
of connective tissue carrying numerous small tfiin-walled vascularsinuses, dividing the growth into broad cellular columns. Thenteoplastic cels are elongated or spindle ed and often stand atright angles to the septa of connective tisse. They have indistnctboundaries, a feeble staining cytoplasm, and oval, s nuclei con-taining a heavy chratinic network. No alpha-granses are presen.ATCAL CAsEs. A chromophobe adenoma which is mposed
of such narow columns of cells separated by numerous vascular* Attetiold bedawnto the fact that thee is evidence of diff ation
in cetain of the no-anular ces llym Sm of the tumors of this Type IV.If a fagnt Of suc a tumr be icmersed in a I perct soltiontof methyl gre and
examned nderthe m~ocpe, the nude of the cedk wil usually be stained brightgree and the m i w gr Hw a vaemble number ofdepending an the tmmor, will be stained bright violet and mdei rmainco111enncOfth violetcellsmkei rgertlmntheothers Inhfxedprprtosstinedby edtl-violet, the periphey of cels retains the dye with coMdrable talthou no definite granus are found. Ths facts seem to iuxa that the chromo-phohe care not all of the sme nature.
549
BAILEY AND CUSHING
sinuses that it resembles the normal structure of the anterior lobeis occasionally met with. In those cases of acromegaly also in whichthere is only a slight enlargement of the hypophysis a somewhatsimilar structure may be found. These exceptionally rare adenomashave been listed as "atypical."
In the order in which the hypophysial adenomas have been thussubdivided or graded, the cells become smaller, the boundaries lessdistinct, multinucleated cells disappear, the nuclei become morepycnotic, the cytoplasm less well stained and the stroma and sinusesbecome more abundant. But more important than all else is thefact that in the descending scale the highly granular cells of Type Ihave passed to a non-granular type.
CLINICAL CORRELATION
When the hundred adenomas were subdivided on the basis of theforegoing histological differentia without reference to the associatedclinical syndrome, the following result was obtained, the most strik-ing feature of the tabulation being the numerical preponderance ofthe purely chromophobe types.*
Type I ........ 8 cases
".II......... 8III ........ IIIV ......... IIV ........ 47VI ........ 12
Atypical ........ 3
Total ........ I100
After this histological study had been completed, the voluminousclinical histories were then independently abstracted with specialattention to any recorded signs or symptoms that might possiblybe interpreted as evidence of a fugitive hyperpituitary effect. Itwas found that:
i. The sixteen adenomas of Types I and II proved in all in-* This preponderance of chromophobe cases in the series can in part be accounted
for by the fact that the chromophobe adenomas are more likely to impair vision thanthe adenomas of acromegaly and consequently are for this reason more likely to beoperated upon. Though the thick walled sella of acromegaly is capable of distention,comparatively speaking the chromophilic adenomas are less favourable for operativeintervention by the usual transphenoidal operation than are the chromophobe ade-nomas
550
ADENOXAS IN COYEGAIIC DYSiru TARI'
stances to have been a d by definite clinical acromegalyand in general the more numeros the alpha-cells, the more pro-nounced was the acromegalic sndrome. To this rule, however,there were the following exceptions: In six of the cases with out-spoken acromegaly numeous alpha-Cells had been demonstrated inthe tissues, but they sed to be fewer than the intensity of thedinical picture would have led one to expec There were, however,in these cases some extenuating crcumstances. In two of them thetissues were fixed in Zenker's fluid and it is possible that morealpha-cells were present th could be demonstrated. In two othercases there was evidence that the acromegalic process was inactiveat the time of the operation.
2. The twenty-two transitional adenomas of Types m and IVwith which we are chiefly oDncerned proved to be associated in manyistancs th dinical indications of an abortive hyperpituitaryaction. This was almost invariably true of the eleven Type madenomas which showed occasional cells with a peripherally disposedthring of alpha-granules. In this group enlargement of hands andfeet was recorded in six instances; coarsening of the features in eight,hypertrichosis in two, normal or exaggerated ihbido in two, essiveheight in thre, essive perspiration in t, squaring and tuftingof the phalanges in four, persistent lactation in one, glycosuria in one,and four of the cases had a normal or slightly elevated basal meta-bolic rate whereas practically without exception the rate in allpatients with adenomas of Types IV, V and VI was subnormal,often maredly so.Among the eleven patients with Type IV adenomas, although no
alpha-granules were demonstrble, two prove to have been verytall and heavily built, one had spacng of the teeth, one hyper-trichosis and exaggeated libido and another definite tufting of theterminal phalanges.
3. The fifty-nine patients with purely chromophobe adenomasof Types V and VI had given no clinical evidence of anything sug-gesting even a trace of fugitive hyperpituitarism with thre possibleexceptions: In tw patients with TypeV lesions, a suggestive tuftingof the terminal phalanges had been mentioned in the X-ray report;and one patient with a Type VI lesion was a tall man with prminentlower jaw but no malocdusion of the teeth. Whether these triflescan be looked upon as suggesting a taint of acromegaly is doubtfuL
55I1

BAILEY AND CUISHING
As a result of this clinico-pathological study it may be statedwith reasonable conservatism: (i) that highly acidophilic adenomasare invariably accompanied by unmistakable acromegaly; (2) thatthe pure chromophobe types are with equal definiteness unassociatedwith any clinical traces of this disorder; and (3) that an intermediarygroup of adenomas with sparsely disposed cells containing a peri-pheral zone of alpha-granules, are likely to produce clinical evidencesof a fugitive hyperpituitary reaction.The histological characteristics of the adenomas of this interme-
diary group are in other words, sufficiently distinctive to enable thepathologist to state, without knowledge of the clinical symptoms,that the patient probably shows traces of hyperpituitarism. Whatis more, it is possible for the clinician to predict with some assurancewhen this intermediary type of adenoma will be disclosed by themicroscope. Such a clinical prediction has received histological veri-fication in four cases operated upon during the past year.
CASE REPORTSIt will suffice to give a few briefly abstracted case histories in
illustration of the condition that we have come to designate a transi-tional, abortive or fugitive acromegaly.
CASE ITransitional Adenoma of Type III with Marked Local Symptoms and Dyspitui-
tarism Chiefly Shown by Adiposity in a Man of Large Frame
On September I8, 1923, Harry P. (Surg. No. I9695), aged 24, single, a foreman,was referred to the hospital by Dr. L. Solis Cohen of Philadelphia with thediagnosis of pituitary tumor.
History: Prior to i9i8, he had always been well. In that year he began tobe troubled by indistinct vision, supposedly astigmatic. Shortly afterward hebegan to gain rapidly in weight from I70 to 220 pounds. During the past sixmonths vision has failed to such an extent that he is no longer able to readprint. His secondary sex characters appeared at a normal age; he has alwaysbeen somewhat sparsely bearded; libido has been undiminished during thepresent illness. There has been no polyuria or polydipsia, no headache, no lossof mental vigor.
Examination: This disclosed a bilateral primary optic atrophy, a completebitemporal hemianopsia, and a greatly enlarged and deepened sella turcica.The basal metabolic rate was -5 per cent. No glycosuria, no polyuria.
The patient was a heavy-boned, rather obese young man (Figs. 7 and 8),5 ft. io in. tall and weighing 225 pounds. His skin was smooth and hair wasscanty over face and chest. His extremities were disproportionately large. Hewore a 71 hat, a iI X shoe and No. g glove. The features were coarse and the
552

ADENOXAS IN AC IC DPIUIARM
lips thick; there was maillary rather than mprognathism. The ca-nial X-ray showed the a ry nasal s to be c b enla Teexterna gentalia wer no d lCnica Impressuio Hypophysial adenom with dyspituLitarismOperaJ;i On SepCMber 27, I923, the approach to the dis-
tended sella proved to be difficult because Of of the artilage of theseptum, and the presceof hyper sprs such as occur in acromegaly.The exposure of the ded selar floor waconsequetly difficult. Abouta thimbleful of softadnas tissue was removed.Cowe of lness: There was no immediate postopertive vement in the
visualfiekisbut the acuity e f 20/200to 20/o andhe discaedon O(dober 4, I923. He was given a series of X-ray treatments with further in-provement in vision which has been retained for five years. When last heardfrom on Jan 29, i928, he reprted himslf to be in excellet health and weigh-ing 2opoundslIs than in 1923, so that hismaladymaybecdstatioary.
Microsopical i atio Fixatives: Regad, 7Zenkr. Stains: MV.E.,P.T.A.H. E.V.O.G. The tumor is mposed of p al and ogated celswith abundant gran cytoplasm (Fig. ga). The nudei are large and vescular.An a ltinudeated cell is seen. Vascular sinuses are rare and thereis no te y to form a stroma of ntive tissue WiLth E.V.O.G. stainafewcelareseenwithblueingranestheprIperyof thecytoplasm (Fig. gb).
Patological Diagnosis: Transitionaladna of Type IIL
Commet: Although is patient might have passed in 1923 ashaving a mild hypopituitary sndrome, the fact of his unusuallylarge extremities with a heavy skeleton aroused the suspidon thatthere might be an acromegalic taint and this was further supportedby the hypertrophic condition of the nasal septa encountered at theoperation. The pathological diagnoss at the time of the operationwas that of pituitary adenoma (unqualified) and its foetal eosino-philic type was not recognized until the tissues were more recentlyreviewed.
CA IlIarge Transiona Adena of Type IH wilk Dyituiarism in an Adipos
Woman of Large Frame
On Noweber 3, z924, Ida H. (Surg. No. 2252I), a hmer'swife, 37 years ofage, was referred to the hospital by Dr. Wiliam R. Gdf of P r , WestVigna with the dia of pittary tumor.
Histoy: Tne patient had been a vigous woman th suscept torecurringattacks of "qumnzy" until er tonsls were removed in 1921. Afterbearing thr healthy chidre her mse ceased. 'This occrred in 1914, tenyears before enrance, and wasa d to apring attk of typhoid fever,after which she began to grow stout (13S POunds in 1914 to 193 Pounds On ad-.in). In 1922 she began having bi l hdach with progeSrive
obscuration of vidsnm. She has suffered of late fom igtion, dysMoea,sensitivity to oid and fatguability with weakness. She has noticed an increas-ing coarsse of her feaues and nease in size of her hands and feet.
553

BAILEY AND CUSHING
Examination: This showed a large, obese woman of middle age with heavyfeatures (Figs. io and ii) and large hands and feet. The skin was coarse anddamp with perspiration. There was pallor of the optic nerves, bitemporal fielddefects, and a greatly enlarged and deepened sella turcica. The X-ray films ofthe hands showed " suggestive squaring of the metacarpals but no other evidenceof acromegalic change." There was no glycosuria nor polyuria. The basalmetabolic rate was +5 per cent. The temperature tended to be subnormal.The clinical impression was that of a hypopituitary state with traces of
antecedent acromegaly.Operation: On November 14, 1924, a transphenoidal operation was performed
with intrasellar removal of considerable soft adenomatous tissue which wasunder tension and comparatively avascular. She made a good recovery withboth subjective and objective improvement in vision. She was given subsequentX-ray treatments and was discharged on December 4, 1924. No subsequentreports.
Microscopical Examination: Fixatives: Zenker, Regaud. Stains: M.V.E.,P.T.A.H., E.V.O.G. The tumor is composed of polygonal cells with ratherabundant, coarsely granular cytoplasm (Fig. 12a). The nuclei tend to be vesi-cular and often excentrically situated. Multinucleated cells are occasionallyseen. Small vascular sinuses are present but there is no tendency to form astroma. With E.V.O.G. stain a few scattered cells are seen which contain fineblue granules in the periphery of their cytoplasm (Fig. 12b).
Pathological Diagnosis: A transitional adenoma of Type III.
Comment: It would appear from the clinical record that thepatient was suspected of having dyspituitarism associated with atransitional or fugitive acromegaly though these descriptive termshad not yet come into use. The pathological diagnosis of the lesion,based on routine examination, was again "pituitary'adenoma"(unqualified) and it was not until our recent reclassification on thebasis of secretory granules that the suspicion of a transitory hyper-pituitarism received histological, support.
CASE IIIDispituitarism with Transitional Acromegaly in a Man with a Large Adenoma
of Type III that had Extruded into the Sphenoidal CeUs
On December 17, 1924, Harold P. (Surg. No. 22822), aged 44, a steamfitter,was referred to the hospital by Dr. William F. Regan of Boston with the com-plaint of headaches and numbness of extremities.
History: The patient was married and the father of one child I6 years of age.Previously of vigorous health, he for ten years had been having recurring head-aches, sometimes so severe they caused vomiting and profuse sweating, obliginghim to lay off from work. After a period of remission for a few years, theseheadaches have returned though in a milder form. During the past three orfour years he has gained 50 pounds in weight and there has been a noticeablediminution of energy and ambition together with loss of libido. Meanwhile hisvision has been noticeably failing. He has been on an antiluetic treatment.
554
ADENOXAS IN ACIDXGAIIC DISPTUTARIM
EzamiWation He was a pw y t, p dero and obese man (Fig. I3and L4) over six feet in height and hing 211 pounds. he skin was soft andsmooth with scanty axilary and pubic hair and sparse, slow beard sothat he shaved only once a week. The geitalia wer smalL The hands and feetwere big and broad and though the finrs taeed normally the X-aydiedslight tufting of the terminal phanges There was no prgathism but thefrotal and dwere large. The sella was huge, with pedestuction of the poserior clinoid procF . Tlere was a b choked discof low grade and left homonymous field defects. Thetpature tended to besubral; the basalmetal rate was-I I per cent. No glcosuiaaorpolyuria.
Cixii;d Imprssio: Hypophysial adema wit and trcesof atecedent acrmegaly.
Operatiox: On Janary 5, I9Q5, a ans l operation was performedin the course of which an hypert maxillary spur such as characromealy was encountered. An abundance of soft t sse hhad already extrded through the sefla and was the wasadially removed. The rcovey from the operation was uneventful but theheadaches cotinued and the left heu niaisk i proges Hewas given a course of X-ray treatments and was d hgonJauay 29, I925.
Cewse of Iless: He eported oMay 29, I925, when his visual fildds werfound to have filed out almost to normal, with a slight re1dul left upperquadrantal defect His general nditi was much mpd and he had goneback to work. On Februry i6, I926, he was found to have agabecome apa-thetic and the defect in his visual fields was arger. er seies of X-rayttments was given. When la heard from, July 3, I928, it was reprte thatthe patient had had two or three attackswih seemed like convulive seizuOtherwise his cndition was lagdyu ged and he was able to continue withhis work.
Microscopical Ezaxmixafio- Fiatives: formaln, R d, Zer. St:M.VE., P.T.A1L, E.V.O.G. The tnaor is cnposed of p l and irgulrells withabunt, coarselygralr cytoplasm and sarply defined bondaries
(Fig. x5a). The nucei are large and vesicular. A few multinueated e areseo. TIere is no stroma, but vascular sinuses are numeru and in some areasthere is a lage amount of genic te, probably seconday to degnerativechange in the tumor. With E.V.O.G. numerous cls have a ng of fine bluegranules in the periphery of the cytoplasm (Fig. xSb).
Pathological Diagnosis: Transitioalad of Type m.
Commen: This man obviously had a sufliently large intra-cranial eXtension of his adenoma to cause an increase in intacranialtension probably due to mild hydrocephalus with resultant papilloe-dema. The tumor had also broken through the floor of the distendedsella so that the sphenoidal cells were filled with the growth Ex-amples of similarly extensive adenomas in cases, however, of unmis-taable acromegaly have been recrded by Cushing and Davidoff ina previous paper in this series-' In this particular case the mixtureof cinical hypo- and hyperpituitary symptoms was sicentlydefinite to arouse the suspicion that an adenoma of transitional type
555
BAILEY AND CUSHING
would be disclosed. This prediction was upheld by the histologicalstudies of the tissues.
CASE IV
Large Transitional Adenoma with Marked Neighborhood Symptoms and Dys-pituitarism with Fugitive Hyperpituitarism Shown by Glycosuria
On Sept. 30, 1925, Robert P. (Surg. No. 25I20), a civil engineer, 33 years ofage, entered the hospital on the advice of Dr. Robert B. Giles of Dallas, Texas,with a diagnosis of pituitary tumor which had been long treated by antilueticmeasures and by radiotherapy. The sole complaint was of failing vision.
History: Shortly after the patient's discharge from the Army in I919, henoticed a periodical, bitemporal clouding of vision which by December of 1923had markedly increased. In 1924 he began to have fronto-temporal headachesand to gain in weight, which increased from his normal of I25 pounds to I83pounds by January of I925.
In I923, owing to a supposedly positive Wassermann, he was given a vigorousantiluetic treatment; and in July of I925, by which time his vision had becomemarkedly impaired, he was given X-ray treatment in spite of which visioncontinued to fail.
Examination: He was a well developed, over-well nourished man I76.3 cm.in height (Figs. i6 and I7). There was considerable puffiness of the face andcoarseness of the skin associated with a moderate hypertrichosis. The genitaldevelopment and libido were normal. Though married he had no children.There was no evidence of skeletal overgrowth either of skull, hands or feetshown by the X-ray. The basal metabolic rate was -i8 per cent.
The neighborhood symptoms were pronounced: the sella greatly enlarged;bilateral primary optic atrophy; a temporal hemianopsia in the left eye with20/I00 vision and vision in the right eye reduced to shadows. The patientbrought with him a perimetric chart taken three months previously at whichtime there was a fairly typical bitemporal field defect.The case would have been looked upon as an example of probable chromo-
phobe adenoma with hypopituitarism had it not been that he was found to haveglycosuria, the urine showing I.42 per cent of sugar.He had come across the country by automobile and arrived with a most
severe case of hemorrhoids which more urgently demanded attention than hishypophysial tumor in spite of his approaching blindness. The hemorrhoids wereoperated upon on October 5, 1925, and from this procedure he made a speedyrecovery. He was re-admitted to the hospital a month later.
Operation: On November 13, 1925, the usual transphenoidal operation wasperformed in the course of which it was found that the tumor had extruded intothe sphenoidal cells. In consequence of this a much less satisfactory and thoroughextirpation of the growth than usual was made and it was not certain how muchof the intrasellar portion of the growth had actually been removed. He madean excellent postoperative recovery but unfortunately without the usual markedimprovement in vision. However, he subsequently did well and on July 14, 1927,he reported that he had not missed a day at his office and was enjoying goodhealth.
Microscopical Examination: Fixatives: Regaud, Zenker. Stains: M.V.E.,P.T.A.H., E.V.O.G. Tissue removed consists of a portion of flattened anterior

ADENOXAS IN ACOGALTC DSTUISARISM
lobe and snafllragets of adenoma. The latter is ra e Of alwith dat, coarsyl cytoplasm Fig. I8a). Blood vesels are fre-quet and there is at to form a stroma. Tne nuclei are icular anda few minuceatedcs are seen. EV.O.G. stain shows numnrous cwbichontain blue gans (Fg 8b).Pakdogical Diagxasis: Transitionalad of Type II.
Comment: In spite of his glycosura, this patient was looked uponas a typical example of mild hypopituitarism. and the adenoma hadbeen recorded as chrmophobe in type untfl it was found durig ourrecet re-examination of the tissues that many of the cells had peri-pherally dispsed of granules.
In a previous number of this series of studies,"' it was stated byDavidoff and Cushing that whereas one out of every four patientswith acromegaly shows glycosuria at one time or another in thecourse of the disease, patients with pituitary insiciency on thecontrary alnost invariably show a high crbohydrate tolerance.The presence of glycosuria in this patient should consequently havesufficed to make us hesitate to accept the orginal dinical and path-ological diagnoses that were made. The subsequent disdosure inthise of an adenoma whose cels contain alpha-granules is con-sequently of particular interest and may possibly afford an explana-tion of other cases that have been reported in which glycosuria hasbeen observed in patients with supposed hypopituitarism
OTm CASES
It would merely prolong without st g this commumca-tion should we submit to the temptation of giving the dinical his-tories of the remaining seven patients in whom a Typem adenomawas found. In all of them the diagnosis of chromophobe adenomahad originally been made and yet, the notes on most of the historiesmake it apparent that the dinical observers were puzzled by thepresence of symptoms that are uncommon in pure hypopituitaystates. The usual syndrome was that shown by the first three ofthe four patients whose histories have been given, namely, suggestivesgns of a tendency to overgrowth; but acromegaly in Marie's sense,though the most striking feature of adult hyperpituitarism is by nomeans its only manifestation. Three of the patients were womenwho were victimized by an offensive degree of hypertrichosis inassociation with an exaggerated libido. Another woman foHowing
557

BAILEY AND CUSHING
second pregnancy failed to regain her menstrual function and hascontinued to lactate for a period of six years; she shows coarseningof the features, is troubled by excessive hyperhidrosis and has gainedthirty pounds in weight. The majority of these patients had a basalmetabolic rate estimated at slightly above zero per cent, whereasa rate of -20 to -3o is usual in uncomplicated hypopituitarism asso-ciated with chromophobe adenomas.The anterior lobe may possess a dual function with independent
principles influencing growth on the one hand and the organs ofsex on the other. Time will shed light on this. Meanwhile it is notat all unlikely that failure in the past to recognize fugitive expres-sions of hyperpituitarism, that are unaccompanied by any clinicallydemonstrable evidences of skeletal overgrowth, may have been asource of confusion. The cases described in the literature (e.g.,Kraus,"5 Case 23) in which an eosinophilic adenoma has been unac-companied by acromegaly may come to be thus explained.
DISCUSSION
We are aware that the histological studies of the tissues on whichour type-grouping has been based are open to criticism on twoscores: (I) in that only a small part of the tumor has been sub-jected to examination and the assumption must be made that theportion removed is representative of the entire growth; and (2) inthat the tumors vary in size so that there is no means from theoperative specimen of estimating the total number of alpha-cells ina given lesion. In spite of these possible sources of error the corre-lation between the dinical syndrome and the microscopical structureof the adenoma seems to us to be sufficiently consistent to justifythe condusion that there is a definite relationship between the numberof alpha-granules in a hypophysial adenoma and the intensity of theassociated acromegalic syndrome.
In an attempt, from the standpoint of functional pathology, tointerpret the clinico-pathological significance of this association oftransitional adenomas with fugitive acromegaly, we may begin withthe one fact concerning overgrowth that now has an experimentalbasis: namely, that the prolonged administration of extracts of theanterior lobe of the hypophysis can produce states in animals com-parable to gigantism and acromegaly in man. Almost certainly,
558

ADENOXAS IN AC A DISITUITARISM
therefore, these latter conditions are due to hypersecretion ratherthan to a possible perverson of secretion of the cells of the an-terior lobe.
Since acromegaly is ordinarily a ied by a tumor whichcomresses and seriously compromises or may even destroy thenormal hypophysial tissue, the continuous pathological overgrowthmust be due to the secretory activity of the tumor itself. This as-sumption is sgthened by fining that the cells of the tumor con-tain the same granules that are present in the normal eoinophilicceRs of the anterior lobe. Tihe further assumption is therefore justi-fiable that these alpha-ganules represent the secretory product thathas to do with growth.We are further struck by the fact that beta- (basophilic) granules
are never found in hypophysial adenomas. It is true that basophilicadenomas of microsopical size have been reported by Erdheim andothers, but we have never found, by the use of iic stains, beta-granules in the cels of any of the t hundred or more adenomasthat have been aefully mined. Though adenomas are occa-sionally descibed as basophilic, this is probably due to the fact thatthe cels of the ordinary chrophobe aden stain somewhatmore heavily with hematoxlin than with eosin. We have no dueas to the siificance of the beta-granules, either from the study ofadenas or from any other source. Whether they are in any wayrelated to the alpha-granules is a subject of dispute.Ihe chromophobe cels of the anterior lobe are supposed to be
more embryonic in type than the chromophile cells and this suP-position seems in accord with the fact that the chromophobe aden-omas are alnost always panied by symptoms of loweredhypophysial function and never by symptoms of overfunction. Theyappear, moreover, to be in general more rapidly growing tha theeosinophilic adenomas.While it is true that the cells of acrmegalic ad contain
alpha-granules, yet they have not the exact strcture of normaleosnophilic cells and great numbes of them contain no granules.It is dificult to say whether these non-granular cells are embryonicchromophobe cels or eosinophilic cels which have lost their secre-tory activity. Kraus,'5 believing that certain non-granular ofthe normal anterior lobe are chromophile lls which have lost theirgranules, seaks of them as "eagramuuirte Zdckx." On the other
559

BAILEY AND CUSHING
hand, as we have already noted, most of the chromophobe cells ofthe normal hypophysis appear to be of an undeveloped and more orless embryonic type.The possibilities are several: (i) that the cells of the adenomas
begin as chromophobe elements and subsequently acquire theiracidophilic granules; (2) that they originate as alpha-cells and laterlose their granules; or (3) that the cells in a given tumor, whetherchromophile, intermediary or chromophobe, remain of the sametype from the beginning to the end of the process.Although we have occasionally had the opportunity of studying
specimens from a given adenoma taken at different stages of thedisease, we have never observed any essential change to have takenplace in its cellular characteristics; as a matter of fact, surgicalspecimens are rarely secured from these tumors in other than thelate stage of their development. We accordingly are shut off fromemploying this direct method of observing cytological alterationsthat may possibly occur in the tumor as its growth progresses, andare obliged consequently to turn to indirect evidence in discussingthese hypotheses.In accordance with the first hypothesis we would expect the pa-
tient to show primary signs of hypofunction on which evidences ofacromegaly are subsequently grafted; if the clinical records are tobe relied upon, this seems actually to have happened in two of ourcases, but it must be exceedingly rare. The symptomatic converse,which would accord with the second hypothesis, namely to seesigns of ultimate pituitary insufficiency in a patient primarily acro-megalic, is, on the other hand, far from uncommon. But experiencenow teaches us that there are other patients with obvious dyspitui-tarism who show fugitive symptons of acromegaly from the begin-ning to the end of their disease.
It is in the adenomas of patients in this last category that thecells containing only a ring of fine alpha-granules in the peripheryof the cytoplasm are to be found. And since these cells have a closeresemblance to the young alpha-cells as they first appear in theembryo (Fig. i9) it is reasonable to suppose that they have neverattained maturity and that they remain of this embryonic typethroughout the course of the disease.In further consideration of the second hypothesis it is interesting
to consider the structure of the adenoma of those cases of well de-
56o

ADENOXAS IN A AGALIC DY IAI
v ped aomegaly, which at the time of operation have apparentlypassd minto a phase of hypofunction (as evidenced by a low basalmetabolic rate, hypotichosis, etc.) in the absence of cystic degener-ation, hemorrhage into the tumor or othe destructive lesion whichmight account for the change in the dinical s e. One wouldexpect from the general structure of the admas in these cases(i.e., rounded cells with central hyaiization, esceti excentricnudei, numerous multincat cells, rare vascular sinuses, etc.)that all of the cels would prove to be crowded with alpha-grnules.But as mentioned (cf. p. 55i) among the exceptions to the rule thatthe more numerous the alpha-cells the more pronounced was theacromegaly, numerous cels are found in these transitional caseswhich are entirely free from granules. On the basis that thes non-granular cells were probaby once easnophilic and now functionless(eagranuieUnk Zdke of Kraus), it is possible to understand thechange of the dinical syndrome occurring in these cases.These of necessity are purely theoretical considerations and when
one recalls how long a time we have been in coming to an under-Standng of the nature of the adenomas of the thyroid gland whichare far more accsible for study, impatience to get at the truthregarding the cytological evolution of the hypophysWal adenomasmay well be restained. Meanwhile in conduding is reort it issafe to say in:
SuImA
That wereas a highly chromophilic type of adenoma, whosec are heavily laden with alpha-granules, c outspokenacromegalic hyperpituitarism, and whereas an adenoma of purelychromophobe type with non-granular cels is cn ly assoatedwith adult hypopituitarism, there is an ritermediay group of casesin which races of these opposed symptoms have apparetly beenpresent from the outset and which are assodate with a histologicallydistinctive adenoma with cels of foetal type having sparse, peri-pherally disposed granules.
Since this ntermediary syndrome is distinisable dinically fromthe more mmon hypopituitary state by recogni e traces ofhyperpituitarism, we lid it convenient to refer to the disorder asfugitive acromegaly.
562 BAILEY AND CUSHING
REFERENCES
i. Aschner, B. Ueber die Funktion der Hypophyse. Pflilger's Arch. f. d.ges. Physiol., 19I2, CxIVi, 1-146.
2. Bailey, P. Cytological observations on the pars buccalis of the hypophysiscerebri of man, normal and pathological. J. Med. Res., I921, xlii, 349-38I.
3. Bailey, P., and Davidoff, L. M. Concerning the microscopic structure ofthe hypophysis cerebri in acromegaly. Am. J. Path., I925, i, I85-207.
4. Benda, C., Stadelman, E., and Fraenkel, A. Klinische und anatomischeBeitriage zur Lehre von der Akromegalie. Deutsche med. Wchnschr.,I90I, xxvii, 5I3, 536, 564.
5. Crowe, S. J., Cushing, H., and Homans, J. Experimental hypophysectomy.Bull. Johns Hopkins Hosp., I9IO, xxi, I27-I69.
6. Cushing, H. The hypophysis cerebri: clinical aspects of hyperpituitarismand of hypopituitarism. J. A. M. A., 1909, liii, 249-255.
7. Cushing, H. The Pituitary Body and its Disorders. Lippincott, Phila.,19I2.
8. Cushing, H. Dyspituitarism. The Harvey Lecture of December io, I9IO.9. Cushing, H. Partial hypophysectomy for acromegaly; with remarks on the
function of the hypophysis. Ann. Surg., I909, 1, I002-IOI8.io. Cushing, H., and Davidoff, L. M. The pathological findings in four autop-
sied cases of acromegaly with a discussion of their significance. Monogr.RockefeUer Inst. M. Research, No. 22, April, I927.
ii. Davidoff, L. M., and Cushing, H. Studies in acromegaly. VI. The dis-turbances of carbohydrate metabolism. Arch. Int. Med., 1927, ,75I-779.
I2. Dott, N. M., and Bailey, P. A consideration of the hypophysial adeno-mata. Brit. J. Surg., I925, Xiii, 3I4-366.
13. Evans, H. M., and Long, J. A. Characteristic effects upon growth, cestrusand ovulation induced by the intraperitoneal administration of freshanterior hypophyseal substance. Proc. Nat. Acad. Sc., I922, yin, 38.
I4. Hochenegg, J. (Cf. Stumme, E.). Akromegalie und Hypophyse. Arch. f.klin. Chir., I908, lxxxvii, 437-466.
i5. Kraus, E. J. Die Beziehungen der Zellen des Vorderlappens des mensch-lichen Hypophyse zueinander unter normalen Verhaltnissen und inTumoren. Beit. z. path. Anat. u. z. allg. Pathol., I914, lviii, I59-2IO.
i6. Krumbhaar, E. B. Pituitary disorders in their relation to acromegaly(hyper-prepituitarism) with suggestions for the use of a more preciseterminology. M. Clin. N. Amer., I92I, V, 927-956.
I7. Lewis, D. D. Hyperplasia of the chromophile cells of the hypophysis as thecause of acromegaly, with report of a case. Bull. Johns Hopkins Hosp.,i965, xvi, I57-164.

ADENOXAS IN AC AIC DYSITU1TARISK 563
x8. Marie, P. Sur de= cas daacmnuli te sinle mm con-gEnitale des _&trniit6s ee iFwrlerestIcealiqes R. demL, I886,,A297333
I9. Putnam, T. J., Ted, H. M., and Benct, E B. lbe PreVmationiof asterile, active extact frnm the ant or be of the h is Whsmle notes on it effects. Am. J. Pkysid., I928, lxxiv, I57-164.

DESCRIPTION OF PLATES
PLATE 123
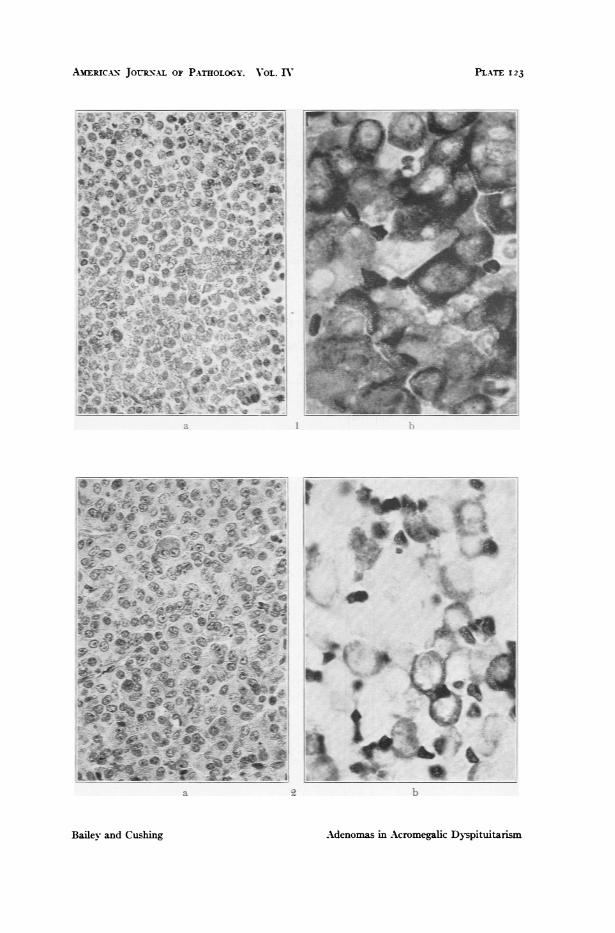
FIG. I. Chromophile adenoma of Type I. (a) The cells of variable size, oftenmultinuclear, lie in a loose, practically non-vascular mass (hematoxylinand eosin, x 300). (b) Practically every cell is packed with apha-granules(ethyl violet-orange G, x 850).
FIG. 2. Chromophile adenoma of Type II. (a) The tumor is more compact:one multinucleated cell is seen; the nuclei are more uniformly sphericaland vesicular (hematoxylin and eosin, x 300). (b) Many cells containabundant alpha-granules in the periphery of the cytoplasm (ethyl violet-orange G, x 850).
AmERIC-N JOURN-AL OF PATHOLOGY. VOL. IV
a b
Adenomas in Acromegalic Dyspituitarism
PLATE I 23
I
Bailev and Cushinlg
PLATE I24
FIG. 3. Transitional adenoma of Type III. (a) The cells have vesicular nucleiwith less abundant cytoplasm. No multinucleated cells. Few vascularsinuses. (Hematoxylin and eosin, x 300.) (b) Note the dark ring formedby alpha-granules in the peripheries of the cells (ethyl violet-orange G,x 850).
FIG. 4. Chromophobe adenoma of Type IV. (a) The tumor is similar toType III though the nuclei are less consistently vesicular (hematoxylinand eosin, x 300). (b) No alpha-granules. Only the nucleoli and erythro-cytes are stained (neutral ethyl violet-orange G, x 850).

ARiac.&x JorRx.u Or PATHOLOGY. OL. nV
B's
t- t
a b}
dAdenomas in Acromegalic Dyspituitarism
PLXTE 124
v
SS
.. I-
Bailev- and Cushing

PLATE 125
FIG. 5. Chromophobe adenoma of Type V. The poorly defined cells show atendency to radiate around numerous small vascular sinuses (methyleneblue-eosin, x 300).
FIG. 6. Chromophobe adenoma of Type VI. The broad columns of cells whosenuclei are non-vesicular are separated by a stroma of connectiveitissueholding vascular sinuses (hematoxylin and eosin, x 300).
FIGS. 7 and 8. Case I. Note the large hand, thick lips and nose, coarse skinand prominent maxillary region.

AMERICAN JOURNAL OF PATHOLOGY. VOL. IV
5 6
Bailey and Cushing
7 S
Adenomas in Acromegalic Dyspituitarism
PLATE I 2 5

PLATE I26
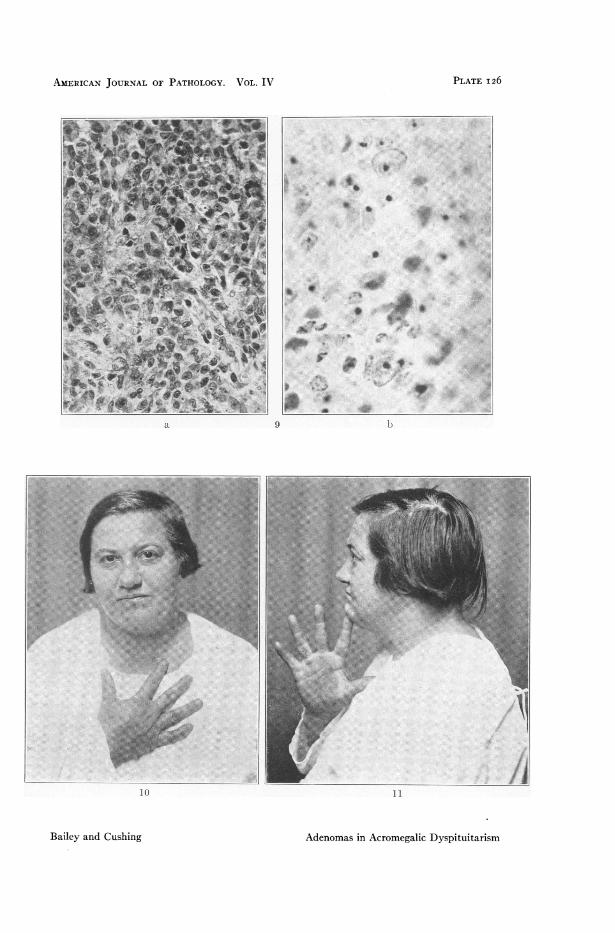
FIG. 9. Case I. Transitional adenoma of Type III. (a) (Hematoxylin andeosin, x 300.) The nuclei have a tendency to be vesicular. (b) (Neutralethyl violet-orange G, x 850.) Two cells may be seen with a rim of alpha-granules.
FIGS. io and ii. Case II. Slight obesity with coarsening of the skin andfeatures. Hand fairly normal.
AMERICAN JOURNAL OF PATHOLOGY. VOL. IV
a
N.b ,. . ... .
10
Bailey and Cushing
9 b
11
Adenomas in Acromegalic Dyspituitarism
PLATE I126
PLATE I27
FIG. I2. Case II. Transitional adenoma of Type III. (a) (Hematoxylin andeosin, x 300.) Nuclei tend to be vesicular, vascular sinuses rare, no stroma.(b) (Neutral ethyl violet-orange G, x 850.) Shows a single cell containinga ring of alpha-granules in the periphery of its cytoplasm.
FIGS. I3 and I4. Case Ill. Large, heavy-set man, with obesity and traces ofacromegaly shown by the X-ray films.

AMERICAN JOURNAL OF PATHOLOGY. VOL. IV
a 12
... ,...._..
b
13 14
Bailey and Cushing Adenomas in Acromegalic Dyspituitarism
PLATE 12 7

PLATE I28
FIG. I5. Case III. Transitional adenoma of Type III. (a) (Hematoxylin andeosin, x 300.) Nuclei tend to be vesicular, sinuses rare, no stroma. (b) (Neu-tral ethyl violet-orange G, x 850.) One cell is seen, in the center, with arim of alpha-granules.
FIGS. I6 and I7. Case IV. Dyspituitarism with thickening and puffiness of thesubcutaneous tissue of the face and with glycosuria.

A CAN JOUNAL OF PATHOLOGY. VOL. IV
a 1- b
t.s i;..f.
_ Xs .. a_
: s
*r :w..s
Bailey and Cushin
16 i
g Adenomas in Acromegalic Dypituitarism
PLATE, 128
PLATE 129
FIG. i8. Case IV. Transitional adenoma of Type III. (a) (Hematoxylin andeosin, x 300.) Nuclei are mostly vesicular, the vascular sinuses are rare,there is no stroma. (b) (Neutral ethyl violet-orange G, x 850.) Severalcells are seen with a rim of alpha-granules.
FIG. I9. Hypophysis of new-born rat, showing the first appearance of alphacells (neutral ethyl violet-orange G, x 850).

A AN JOUAL OF PATOLOGY. VOL IV
a 18 b
19
adCuinAdsi Anwc DyVituitarisn
PLATE I129
Baie and Cuhig


















