Otolaryngology: Open Access...a laryngeal cyst is reported. • Endoscopic marsupialization with...
2
Open Access Case Report Steineger and Brøndbo, Otolaryngol 2012, S:4 DOI: 10.4172/2161-119X.S4-001 Otolaryngol ISSN:2161-119X Otolaryngology an open access journal Pediatric Otolaryngology Corresponding author: Johan Steineger, M.D, Department of Otorhinolaryngology, Head and Neck Surgery, Oslo University Hospital, Norway, E-mail: [email protected] Received January 31, 2012; Accepted February 20, 2012; Published February 27, 2012 Citation: Steineger J, Brøndbo K (2012) A Congenital Malformation of the Piriform Sinus Mimicking a Laryngeal Cyst. A Case Report. Otolaryngol S4:001. doi:10.4172/2161-119X.S4-001 Copyright: © 2012 Steineger J, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. A Congenital Malformation of the Piriform Sinus Mimicking a Laryngeal Cyst. A Case Report Johan Steineger* and Kjell Brøndbo Department of Otorhinolaryngology, Head and Neck Surgery, Oslo University Hospital, Norway Keywords: Congenital malformation; Stridor; Pediatric airway; Laser surgery; Laryngeal cyst Introduction Laryngomalacia is the most common cause of stridor in the newborn, accounting for 75% of the cases [1]. Congenital laryngeal cysts are a much rarer entity, the incidence reported as low as 1.82 per 100,000 live births [2], but should always be considered as a cause of stridor during the first weeks of life. e symptoms which also may include hoarseness, cyanosis and feeding problems, usually appear the first day, but may be delayed up to several weeks or even years [3]. e upper airway obstruction caused by the cyst can be potentially lethal. Different localizations of congenital laryngeal cysts have been reported and several classifications have been proposed [4,5]. In our case the localization of the cyst, the piriform sinus, was very special and to our knowledge not described in modern literature. Case Report e patient was a five days old girl, born by vaginal delivery at a local hospital with gestational age 36.2 weeks, with an Apgar score 9-10 and birth weight 2500 grams. 30 minutes post partum the patient developed respiratory distress with inspiratory stridor, demanding treatment with CPAP. Preliminary flexible laryngoscopy showed a supraglottic lesion on the leſt side, obstructing the laryngeal inlet. e CT scan, although of very low quality, supported this finding. She was then transferred to our clinic, a tertiary referral centre, for further treatment. Upon admission the infant was still in need of CPAP, and the respiratory frequency was 40. Flexible videolaryngoscopy showed a cystic lesion in the leſt supraglottic area (Figure 1). Intubation proved to be very difficult due to the narrowing of the laryngeal inlet, but at the end was achieved with a 2.5 mm endotracheal tube via the pediatric Lindholm laryngoscope. With the Sharplan CO 2 laser attached to the Leica microscope and the Unimax 2000 micromanipulator with strength 2 watt, a regular pulse and a continuous mode, marsupialization of the cystic lesion with drainage of a mucous fluid was carried out. It now became apparent that the cyst was a compartment consisting of the piriform recess forming the floor, the anterior and the lateral walls, while the medial portion was made up by the lateral aspect of the arytenoid fold. e roof and the posterior aspect consisted of a rather thin membrane covered with mucosa (Figure 2). Due to its size the cystic mass bulged into the supraglottic area. At the end of the operation the anatomy of the region was restored and the supraglottic area looked more or less normal. e histological specimen showed regular columnar epithelium with mucous glands and a fibrous stroma. Postoperatively the patient did excellent; she could be extubated the following day and was discharged without any respiratory symptoms the third postoperative day. e parents reported Abstract Objective: We report a type of hypopharyngeal congenital malformation not previously described in the world literature. Case report: A slightly preterm, female newborn presented with stridor immediately after birth. Flexible laryngoscopy showed the presence of a huge supraglottic cystic mass and endoscopic laser surgery under general anesthesia was carried out. During the operation it became clear that the cystic lesion had its origin from the piriform recess and not the laryngeal structure. The child was extubated the day after the operation without any problems and has since shown a normal development. Conclusions: A unique cystic congenital malformation of the piriform sinus is described. The challenges related to intubation and surgical treatment of this particular case and similar lesions are addressed. Figure 1: Preoperative image showing the cystic lesion protruding into the supraglottic area. O t o l a r y n g o l o g y : O p e n A c c e s s ISSN: 2161-119X Otolaryngology: Open Access
Transcript of Otolaryngology: Open Access...a laryngeal cyst is reported. • Endoscopic marsupialization with...
-
Research Article Open AccessOpen AccessCase Report
Steineger and Brøndbo, Otolaryngol 2012, S:4 DOI: 10.4172/2161-119X.S4-001
Otolaryngol ISSN:2161-119X Otolaryngology an open access journalPediatric Otolaryngology
Corresponding author: Johan Steineger, M.D, Department of Otorhinolaryngology, Head and Neck Surgery, Oslo University Hospital, Norway, E-mail: [email protected]
Received January 31, 2012; Accepted February 20, 2012; Published February 27, 2012
Citation: Steineger J, Brøndbo K (2012) A Congenital Malformation of the Piriform Sinus Mimicking a Laryngeal Cyst. A Case Report. Otolaryngol S4:001. doi:10.4172/2161-119X.S4-001
Copyright: © 2012 Steineger J, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
A Congenital Malformation of the Piriform Sinus Mimicking a Laryngeal Cyst. A Case ReportJohan Steineger* and Kjell Brøndbo
Department of Otorhinolaryngology, Head and Neck Surgery, Oslo University Hospital, Norway
Keywords: Congenital malformation; Stridor; Pediatric airway;Laser surgery; Laryngeal cyst
IntroductionLaryngomalacia is the most common cause of stridor in the
newborn, accounting for 75% of the cases [1]. Congenital laryngeal cysts are a much rarer entity, the incidence reported as low as 1.82 per 100,000 live births [2], but should always be considered as a cause of stridor during the first weeks of life. The symptoms which also may include hoarseness, cyanosis and feeding problems, usually appear the first day, but may be delayed up to several weeks or even years [3]. The upper airway obstruction caused by the cyst can be potentially lethal. Different localizations of congenital laryngeal cysts have been reported and several classifications have been proposed [4,5]. In our case the localization of the cyst, the piriform sinus, was very special and to our knowledge not described in modern literature.
Case ReportThe patient was a five days old girl, born by vaginal delivery at a
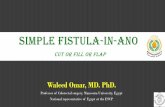
local hospital with gestational age 36.2 weeks, with an Apgar score 9-10 and birth weight 2500 grams. 30 minutes post partum the patient developed respiratory distress with inspiratory stridor, demanding treatment with CPAP. Preliminary flexible laryngoscopy showed a supraglottic lesion on the left side, obstructing the laryngeal inlet. The CT scan, although of very low quality, supported this finding. She was then transferred to our clinic, a tertiary referral centre, for further treatment. Upon admission the infant was still in need of CPAP, and the respiratory frequency was 40. Flexible videolaryngoscopy showed a cystic lesion in the left supraglottic area (Figure 1).
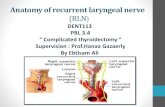
Intubation proved to be very difficult due to the narrowing of the laryngeal inlet, but at the end was achieved with a 2.5 mm endotracheal tube via the pediatric Lindholm laryngoscope. With the Sharplan CO2 laser attached to the Leica microscope and the Unimax 2000 micromanipulator with strength 2 watt, a regular pulse and a continuous mode, marsupialization of the cystic lesion with drainage of a mucous fluid was carried out. It now became apparent that the cyst was a compartment consisting of the piriform recess forming the floor, the anterior and the lateral walls, while the medial portion was made up by the lateral aspect of the arytenoid fold. The roof and the
posterior aspect consisted of a rather thin membrane covered with mucosa (Figure 2).
Due to its size the cystic mass bulged into the supraglottic area. At the end of the operation the anatomy of the region was restored and the supraglottic area looked more or less normal. The histological specimen showed regular columnar epithelium with mucous glands and a fibrous stroma. Postoperatively the patient did excellent; she could be extubated the following day and was discharged without any respiratory symptoms the third postoperative day. The parents reported
AbstractObjective: We report a type of hypopharyngeal congenital malformation not previously described in the world
literature.
Case report: A slightly preterm, female newborn presented with stridor immediately after birth. Flexible laryngoscopy showed the presence of a huge supraglottic cystic mass and endoscopic laser surgery under general anesthesia was carried out. During the operation it became clear that the cystic lesion had its origin from the piriform recess and not the laryngeal structure. The child was extubated the day after the operation without any problems and has since shown a normal development.
Conclusions: A unique cystic congenital malformation of the piriform sinus is described. The challenges related to intubation and surgical treatment of this particular case and similar lesions are addressed.
Figure 1: Preoperative image showing the cystic lesion protruding into the supraglottic area.
Oto
lary
ngology: OpenAccess
ISSN: 2161-119X
Otolaryngology: Open Access
-
Citation: Steineger J, Brøndbo K (2012) A Congenital Malformation of the Piriform Sinus Mimicking a Laryngeal Cyst. A Case Report. Otolaryngol S4:001. doi:10.4172/2161-119X.S4-001
Page 2 of 2
Otolaryngol ISSN:2161-119X Otolaryngology an open access journalPediatric Otolaryngology
three and fourteen months postoperatively no complications following the surgery and that the child was thriving and developed normally.
DiscussionCystic laryngeal lesions have been classified into saccular, ductal
and thyroid cartilage for animal cysts. In our case this classification could not be used since the cystic lesion arose outside the laryngeal structure. We were not able to find any similar reports in the medical literature. Hence, we will call this pathological finding a congenital malformation of the piriform sinus. Compared to the previously classified laryngeal cysts, the special anatomical location in this case made no difference concerning the surgical treatment.
A retrospective study showed that almost 50% of the reported cases of congenital laryngeal cysts were diagnosed at autopsy [6]. This underlines the importance of a swift, correct diagnosis and a proper treatment. Flexible videolaryngoscopy with a very slim laryngoscope (in our case an Olympus ENF XP with a distal tip of 1.8 mm) will in most cases be a safe, diagnostic procedure and make further exams superfluous. CT or MRI may be difficult and even hazardous due to the respiratory distress and in our case the quality
of the scan was too poor to be of any value. The most challenging part of the surgical treatment is probably the anesthesia, in particular the intubation. This may be extremely difficult due to the compromised and diminished laryngeal inlet. The anesthesia should be very light with the patient in spontaneous respiration and the possibility of an emergency tracheotomy should always be kept in mind. The surgery itself of congenital laryngeal cysts is fairly simple when conducted by an experienced surgeon. Endoscopic marsupialization with laser, with removal of the roof and posterior wall of the cystic lesion, proves to be an effective and adequate surgical technique [2]. Since the cystic lesion in our case originated from the piriform sinus, complete excision was not feasible. This could have created a larger wound area with increased risk of postoperative adhesions and a possible hypopharyngeal stenosis. External approaches should be reserved for the more complex cases [5]. The prognosis and outcome is usually excellent and we will not advocate postoperative CT/MRI or an endoscopy control at this stage, if the infant is thriving and shows a normal development. “The proof of the pudding is in the eating!”
Bullet Point Summary• Congenital laryngeal cysts are a rare cause of stridor in the newborn.
• A not previously described congenital hypopharyngeal malformation mimicking a laryngeal cyst is reported.
• Endoscopic marsupialization with laser proved to be an effective surgical technique for treatment.
References1. Cotton RT, Richardson MA (1981) Congenital laryngeal anomalies. Otolaryngol
Clin North Am 14: 203-218.
2. Pak MW, Woo JK, van Hasselt CA (1996) Congenital laryngeal cysts: current approach to management. J Laryngol Otol 110: 854-856.
3. Gutierrez JP, Berkowitz RG, Robertson CF (1999) Vallecular cysts in newborns and young infants. Pediatr Pulmonol 27: 282-285.
4. DeSanto LW, Devine KD, Weiland LH (1970) Cysts of the larynx--classification. Laryngoscope 80: 145-176.
5. Forte V, Fuoco G, James A (2004) A new classification system for congenital laryngeal cysts. Laryngoscope 114: 1123-1127.
6. Kristensen S, Tveteras K (1986) Congenital laryngeal cyst in infancy. A rare cause of life-threatening stridor. ORL J Otorhinolaryngol Relat Spec 48:150-155.
A
B
C
Figure 2: Per operative image with the endotracheal tube to the right.A: the floor of the cavity, B: the posterior wall of the cystic lesion (partly removed), C: the esophageal inlet.
This article was originally published in a special issue, Pediatric Otolaryngology handledbyEditor(s).Dr.RichardKangD,TheOhioStateUniversity,USA
http://www.ncbi.nlm.nih.gov/pubmed/7254841http://www.ncbi.nlm.nih.gov/pubmed/7254841http://www.ncbi.nlm.nih.gov/pubmed/8949296http://www.ncbi.nlm.nih.gov/pubmed/8949296http://www.ncbi.nlm.nih.gov/pubmed/10230929http://www.ncbi.nlm.nih.gov/pubmed/10230929http://www.ncbi.nlm.nih.gov/pubmed/5411821http://www.ncbi.nlm.nih.gov/pubmed/5411821http://www.ncbi.nlm.nih.gov/pubmed/15179225http://www.ncbi.nlm.nih.gov/pubmed/15179225http://www.ncbi.nlm.nih.gov/pubmed/3714197http://www.ncbi.nlm.nih.gov/pubmed/3714197http://www.ncbi.nlm.nih.gov/pubmed/3714197
TitleCorresponding authorAbstractKeywordsIntroductionCase ReportDiscussion Bullet Point SummaryFigure 1Figure 2References