Osteoporosis in Athletes

of 9
-
Upload
rusty-hogan -
Category
Documents
-
view
218 -
download
0
Transcript of Osteoporosis in Athletes
-
8/12/2019 Osteoporosis in Athletes
1/9
Osteoporosis in Athletes
Osteoporosis or osteopenia in athletes is associated with: the age of onset of training, duration,
intensity and volume of training, the sport concerned (e.g. light weight rowers, synchronised
swimmers, ballet dancers, gymnastics, marathon runners) diet and stress, psychological as well as
physical stress. The loss is mainly of trabecular bone, which is found in the vertebrae and the neck of thefemur.
Exercise plays a very important role both in the formation of bone and the maintenance of bone
throughout the life cycle. Bones require normal levels of sex hormones, adequate calories, particularly
protein. Daily Calcium 1000 -1500mg and 800 international units of Vitamin D and regular weight
bearing exercise. Exercise affects the skeleton in different ways. The direct effect of stress loading can
be to increase bone mineral density. Intensive aerobic exercise, however, can adversely affect bone
density indirectly by its effect on the hypothalamic-pituitary-gonadal axis, which results in low oestrogen
levels in females (Wolman 1994 ;O Brien 2007). Overtrained male athletes may also show low levels of
testosterone and may develop stress fractures and osteoporosis (Gillooly 2002, Rigby 2003).
Wolff's Law states that changes in bone function lead to changes in bone. Bone is laid down where it is
needed. Bone is resorbed where it is not needed (Wolff 1892). Osteogenesis is induced by dynamic not
static strains. The optimal type of osteogenic activity should provide relatively high levels of strain.
(Rubin and Lanyon1984). Tensile Forces result in osteoclastic activity on the convex side of an angulated
bone. Compressive force results in osteoblastic activity on the concave side.
Muscle action is the main stimulus for bone formation, the mechanical force and weight bearing. (O
Brien 2001). Greater loads and fewer repetition of a load will result in greater gains in bone mass. Lower
loads repeated a greater number of times result in lower gains (Kerr et al., 1994) Weight bearing activity
accounted for up to 17% of the variance in B.M.D. between individuals in their late twenties (Welten etal. 1994).
Peak Height Velocity for girls occurs usually between 10.5 - 13 Years and is earlier than 12.5 - 15 years
for boys. Around this period, bone is most responsive to exercise and during the time of Peak Weight
Velocity and Menarche, which occur approx 6 months and 1 year after Height Peak (Sanborn et al 1994).
Average age in Ireland is 12-13 years - A late menarche is after 16 years.
Bone mass is affected by peak bone mass and the degree of subsequent bone loss. 60-80% of Peak bone
mass is due to genetics. (Khan et al 2001) Other factors include, hormones, nutrition, environmental
factors and mechanical strain. Growing bone has a greater capacity to add new bone to skeleton than
mature bone, 7-8% gain of bone mass per year is gained during childhood and early adolescence.
(Matkovic et al 2000).
Many factors, hormones, diet, exercise, medication, and their chronological age, which can be affected
by their skeletal or bone age and the stage of sexual maturation, can affect Low Peak Bone Mass.
(McKay et al. 1998). Woods (1999) in a study of apprentice jockeys found that the majority had a bone
age 18-24 months below their chronological age. Apprentice jockeys had significantly lower BMD than
-
8/12/2019 Osteoporosis in Athletes
2/9
flat and jump jockeys. The jockeys had lower BMD in spine and neck of femur than rugby players and
sedentary controls (Woods 1999).
Daily weight bearing exercise has a positive effect on BMD, while immobilisation and space flight have a
negative effect (Kanis 1994). The effects of exercise are not homogenous; they reflect the strains
imposed at individual sites. Osteogenic response to mechanical loading is site specific. ProfessionalTennis players have 30% greater bone density in dominant forearm (Krahl et al. 1994) Weight bearing
exercises such as running on the spot, jumping, skipping, dancing, walking are gravity stimulated and are
more effective than non weight bearing such as swimming, equestrian.
Weight bearing activity during adolescence and early adulthood was a far more important predictor of
peak bone mass than calcium intake. (Welten et al. 1994). Young women participating regularly in sports
at school demonstrated higher bone mass than those who did not. (Heinonen 2001).
Highest bone mineral content and bone mineral density are found in strength and power- trained
athletes. (Suominen 1993). World class and recreational weight lifters had 10-35% greater lumbar spine
B.M.D. Athletes with habitually high levels of physical activity show increased B.M.D. value when
compared with controls that undertake moderate physical activity. Road cyclists have lower bone
mineral density in their lumbar spine compared to mountain bikers. (Gillooly 2002, Rigby 2003).
Premenopausal women who participate regularly in high impact exercise tend to have higher B.M.D.
than sedentary controls. But intensive endurance training and amenorrhea may be associated with
decreased trabecular bone density in young females (Suominen 1993). Menstrual irregularities occurred
in elite university athletes, swimmers who had lower B.M.D. in their spine and hip than gymnasts.
Untreated amenorrhea is associated with long -term morbidity especially in young women (Drinkwater
et al 1990).
"Overtraining" due to excessive physical or psychological stress, particularly if it is associated with
inadequate caloric intake, results in low levels of sex hormones in both male and female athletes and an
increased risk of osteopenia or osteoporosis. There is a higher incidence of gonadal insufficiency
particularly in sports where there are weight categories, such as light weight rowing, judo, diving,
synchronised swimming, gymnasts, skating and ballet dancers, long distance running but it can occur in
any sport. Non-weight bearing sports particularly swimming and the lumbar spine in road cyclists are
prone to low bone mineral density, either osteopenia or osteoporosis. (Taafe et al. 1995).
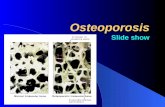
Osteoporosis is a systemic skeletal disorder characterized by low bone mass and micro-architectural
deterioration of bone tissue, with a consequence increase in bone fragility. Osteoporosis is associated
with a reduction in bone mineral density and an increased risk of fractures. Bone is a dynamic tissue in
which the process of resorption, (mediated by the osteoclasts), is coupled with the processes of
formation, (mediated by the osteoblasts) when they are in a state of balance. Osteoporosis results when
uncoupling occurs and there is an imbalance between resorption and formation. The bone most
frequently affected is the trabecular bone in the distal end of the radius, vertebral bodies and the neck
of the femur. The commonest cause of osteoporosis in women and men is hypogonadism, which are
due to low levels of oestrogen in females and testosterone in males.
-
8/12/2019 Osteoporosis in Athletes
3/9
Hormones secreted by the hypothalamus, anterior pituitary, and ovary and to a lesser extent the
adrenal gland regulate the menstrual cycle. Acting on the uterus and ovaries, they are dependent on a
feedback mechanism. This is necessary for the normal development of the follicle. The Gonadotrophin
Releasing Hormone (GnRH) causes the synthesis, storage, activation and release of Follicle Stimulating
Hormone (FSH) and Lutenizing Hormone (LH). The timing and intensity of the GnRH determines the
amount of FSH and LH released, and their ratio relative to each other. ( Prior 86 ). Physical exercise
produces marked changes in the post exercise pulsatile nature of LH, FSH and oestrodial. (Keizer 1983).
During strenuous exercise there is an increased concentration of dopamine, beta-endorphins and
Catechol-oestrogens. Dopamine has an inhibitory effect on the release of GnRH. Beta-endorphins act in
two ways; they appear to stimulate dopamine and this is their main action on GnRH (Yen, 1982), but
they also combine with the nor-adrenaline receptors in the hypothalamus and prevent the stimulatory
effects of nor-epinephrine on GnRH. The normal pulsatile release of gonadatrophin releasing hormone is
altered, resulting in changes in the secretion of FSH and LH and the ovarian hormones.
Corticotrophin - releasing hormone may also act indirectly by endorphins. The level of Cortisol is
increased by intense exercise and in athletes who are overtrained. Cortisol levels are increased in
amenorrheic athletes compared to sedentary women and cyclic athletes. Long term elevated levels of
Cortisol affect calcium and bone metabolism resulting in osteopenia and osteoporosis. Cortisol increases
bone resorption and decreases bone formation. Cortisol also decreases intestinal absorption of calcium.
Hypothyroidism may also be a complication of overtrained athletes who may also be amenorrheic.
Amenorrhoeic athletes who are hypo-oestrogenic have reduced bone mass. This may be due to late
menarche, irregular menstruation, or may be part of the Athletic Triad, which consists of amenorrhea,
an eating disorder and osteoporosis or osteopenia. (Khan et al 2001).
Menstrual irregularities result in alterations in the normal levels of sex hormones and predispose to
osteopenia and in some cases osteoporosis. Menstrual irregularities tend to occur in the athletes with
the most intense training schedules, who had trained for the longest period of time. Vegetarians and
people with a low caloric intake had the highest incidence of oligomenorrhea and amenorrhea.
Menstrual irregularities are not consistent across sports; 7% recreational runners, 12% swimmers and
25% distance runners. Many so-called normal cycles are abnormal when serum hormone levels are done
after 21st day of cycle.
There are multifactorial causes; Stress, both psychological and physical stress. This may be due to an
increase in the amount and intensity of training and in the numbers of competitions with inadequate
rest periods.
Other factors which predispose to menstrual irregularities include a late menarche (>16 years), irregular
cycles prior to sports participation, intense training prior to menarche, immature pituitary axis. Tall thin
girls and those with a poor maternal menstrual history, have a later menarche than small overweight
girls. Average age for menarche in USA for Caucasians is 12.8 years, for European's it is 12-13.4 years.
Progression of menstrual changes to abnormal is from,
-
8/12/2019 Osteoporosis in Athletes
4/9
1. Normal follicular, phase and a normal luteal phase.2. A prolonged follicular phase and a shortened luteal phase, this can only be diagnosed by taking
bloods to measure progesterone levels after the 21st day of the cycle. Luteal phase defects are
associated with low progesterone levels, premenstrual tension and infertility.
3. Further progression results in euoestrogenic anovulatory oligomenorhea, if this phase persiststhere is a risk of endometrial hyperplasia.
4. Hypo oestrogenic amenorrhea results in osteoporosis and genital atrophy due to low levels ofoestrogen. (O'Brien 2007 , Shangold 1988).
Diet also plays an important role. Decreased caloric intake and a high fibre diet are associated with a
raised level of Serum Sex Hormone Binding Globulin and lowered levels of biological active oestrogens.
There is a higher incidence of amenorrhea in athletes who have a low caloric intake or who are
vegetarians. The increased fibre is thought to bind with calcium and reduce calcium absorption. Excess
fibre may also lead to decreased bone density by the binding of steroids to fibre or indirectly by
decreasing enterohepatic circulation of oestrogens, either of which would have a negative effect on
bone remodelling.
Increases in dietary fat consumption are associated with increased levels of circulating oestrogens.
Amenorrheic athletes have an increased risk of musculosketal injuries and may have a low calcium and
vitamin D intake. The recommended daily calcium for an adolescent is 1500mg and 800 international
units of vitamin D.
Drinkwater et al (1990) reported vertebral BMD to be significantly lower in athletes with a long history
of menstrual irregularity. There is a higher incidence of stress fractures in amenorrheic athletesparticularly those with a late menarche. (Warren et al. 1991). The mean bone mineral density is
comparable in some cases to a 60-year-old woman. If untreated they have a high risk of developing
stress fractures now and osteoporotic fractures now and also at the menopause. Moderate exercise
protects but excessive exercise may cause osteoporosis.
"The Athletic Triad" (Yeager et al 1993) is the name of the syndrome, which occurs, in female athletes,
when amenorrhoea, an eating disorder and osteoporosis occur together. Bennell 2004: Khan et al. 2004
have found that they may have osteopenia rather than osteoporosis. They may each occur on their own,
or in combination.
The female athlete is most at risk to develop the athletic triad during adolescence and young adulthood.
This may be due to psychological, biological and social pressures at this time. During the prepubertal
spurt 60% of the final bone mass is laid down. Anorexia and bulimia are now more frequently
recognised, both in the general population and among athletes (Grinspoon et al., 1999; Sundgot-Borgen,
1993; Sundgot-Borgen, 2000; Miller et al., 2005).
-
8/12/2019 Osteoporosis in Athletes
5/9
Individuals with eating disorders strive for perfection; have a marked preoccupation with food, a
distorted body image and fear of gaining weight or becoming fat, despite being at least 15% below their
ideal body mass. Amenorrhea is one of the cardinal features of anorexia and is associated with
hypothalamic dysfunction with low levels of oestrogen (Lindsay 1995; Compston et al., 2006); in
addition, anorexics may also have high levels of the stress hormone cortisol (Katz, 1988). BMD is also
significantly lower in females who have developed anorexia during their growth period than in those
who have developed anorexia at an older age (Biller et al., 1989).
Athletes, parents and coaches, who have unrealistic goals and poorly designed training programmes
with inadequate recovery periods are placing the athlete at a much higher risk of developing an eating
disorder. Talented athletes participating in more than one sport and who are training and playing for
school club and county, "Win at all costs, ambitious coaches, and pushy parents with unrealistic goals,
wrong training plan, emphasis on weight," are detrimental to talented athletes.
Osteoporosis in young female athletes is sports specific; there is a much greater incidence in appearance
sports, such as diving, figure skating, gymnastics synchronised swimming and ballet. Endurance sports,
which involve distance running, particularly in marathon runners. Weight category sports: jockeys, judo
and light weight rowers. It is associated with age of onset of training, duration of participation in
training, intensity and volume of training, the sport concerned, diet and stress (Riggs, 1981).
Stress, both psychological and physical , play a role in menstrual irregularity, which may progress to
oligomenorrhea or amenorrhea. Physical stress may be due to a sudden increase in the intensity and
duration of training or too many competitions. A sudden marked increase in the intensity and the
amount of aerobic exercise may cause problems particularly in the younger nulliparous female with an
immature hypothalamic - pituitary axis.
Nattiv et al. (1994) state that eating disorders such as anorexia and bulimia affect as many as one thirdof athletic females. Disordered eating has become a major concern in female and in some male athletes.
Some researchers have estimated the prevalence to be as high as 50% in certain sports. Female athletes
who had a late menarche (after 16 years) or who have irregular cycles, particularly if they have had long
periods of oligomenorrhea or amenorrhea, e.g. athletes with eating disorders and hypogonadism due to
any cause, are more at risk to develop osteopenia or osteoporosis, particularly if they are " overtrained".
Long-term Corticosteroid users, patients with malabsorption, hypothyroidism, and hyperparathyroidism,
high levels of prolactin, Cortisol, Parathyroid hormone, hyperthyroidism, low levels of vitamin D are also
at risk.
If a female athlete has been amenorrhoea for six months and is not pregnant, hormonal studies shouldbe carried out and her bone mineral density should be assessed using a Dual Energy X-ray
Absorptiometer (DXA). DXA is non invasive and is currently the most precise and widely used method of
assessing Bone Mineral Density. Measurement of the spine and hip should be carried out and bone
markers, if they are available. If osteoporosis is diagnosed in either a male or female she/he should be
treated. Medical causes must be excluded.
The treatment for amenorrhoeic athletes:
-
8/12/2019 Osteoporosis in Athletes
6/9
1. Reduce the amount and intensity of the exercise and competition.2. Reduce psychological stress if possible.3. Prescribe combination low dose pill or HRT.4. Increase the calcium content to 1000-1500mg per day.5. Increase the total calorific content, if it is below the required level for the activity performed.
They should be advised to decrease their exercise intensity and a 2-3% increase in weight should be
encouraged. Recreational athletes will reduce the intensity of their exercise; elite athletes are unlikely to
take this advice. If the female athlete will not reduce the amount of training and competition, she
should be advised to go on hormone replacement therapy or the low dose contraceptive pill. Some
athletes do not want to go on any medication, as they think it will affect their weight, but they must
consider that if they get a stress fracture they will be unable to compete or train.
All athletes should keep a training diary, which should include details of their diet, exercise regime and
menstrual cycle. Excessive carbohydrate loading may result in some athletes developing diarrhoea, due
to intolerance to gluten. This will affect absorption of Calcium, vitamin D iron and protein.
"Overtrained athletes" you should measure sex hormones, oestrogen, progesterone, serum sex
hormone binding globulin (SHBG),and free testosterone, androstenedione in males, cortisol,
gonadotrophins (LH,FSH ) and prolactin, thyroid, hepatic, and renal and intestinal function. Female
athletes who had a late menarche, or irregular cycles, particularly if they have had long periods of
oligomenorrhea or amenorrhea are more vulnerable and should have a DXA and hormone levels done in
the second half of the cycle if they are having periods.
Maximum bone loss probably occurs in the early phase of amenorrhoea, so they should start treatment
early. A large number of amenorrhea athletes develop breast tenderness and bloating, when they start
hormone therapy and they should be warned about this and reassured that the symptoms are usually
transitory. Adolescent athletes are at high risk of developing eating disorders.
All athletes should be given nutritional advice from a nutritionist interested in sport and eating disorders
and consult a psychiatrist with a special interest in eating disorders. Ensure they have an adequate
caloric intake and increase the calcium intake to 1500 mg, and 800 IU of vitamin D.
Medical Team Approach: Physician, Physiotherapist, Nutritionist, Physiologist, Psychologist working with
athlete and coach. The successful treatment and prevention of Osteoporosis is to identify those at risk atan early stage and assess their hormone levels and bone mineral density.
REFERENCES:
Biller B, Saxe V, Herzog D, et al. Mechanisms of osteoporosis in adults and adolescent womenwith anorexia nervosa. J Clin Endocrinol Metab 1989; 68: 548-554.
-
8/12/2019 Osteoporosis in Athletes
7/9
Bennell K, The female Athlete in Clinical Sports Medicine, Editors Brukner P., Khan K. 2nd EditionMcGraw- Hill2004; 674-699.
Compston J, McConachie C, Stott C, Hannon R, Kaptoge S, Debiram I, Love S, Jaffa, A. Changes inbone mineral density, body composition and biochemical markers of bone turnover during
weight gain in adolescent with severe anorexia nervosa: A 1 Year prospective study.Osteoporosis International; 2006. 17: 77-78.
Drinkwater BL., Bruemmer B., and Chestnut III CH: Menstrual history as a determinant of currentbone mineral density in young athletes. JAMA; 1990; 263:545
Gillooly JJ The relationship between cycle training, hormone levels, mood state, bone mineraldensity and fracture incidence in male road cyclists MSC Thesis in Sports Medicine, Trinity
College Dublin, 2002; 66-67.
Grinspoon S, Miller K, Coyle C, et al. Severity of osteopenia in oestrogen deficient women withanorexia nervosa and hypothalamic amenorrhea. J Clin Endocrinol Metab 1999; 84: 2049-2055.
Heinonen A Physical activity, targeted bone loading and bone mineral density in premenopausalwomen in. In: Physical activity and bone health. Human Kinetics.2001; 129-142
Kanis J.A in: Osteoporosis. Blackwell Science, London. 1994:22-55. Katz, J.L. Eating disorders in: Women in exercise, edited by Shangold, M. and Mirkin G.
Philadelphia, Davis; 1988; 248-263.
Keizer H.A. Hormonal responses in women as a function of physical exercise and training.Uitgeverij de Vrieseborch, Harlem. 1983
Kerr D.A., Prince R.L., Morton A., Dick I., Does high resistance weight training have a greatereffect on bone mass than low resistance weight training? (Abstract 128) Journal Bone Mineral
Research (Supplement 1) 1994;S152
Khan K, McKay H, Kannus P, Bailey D, Wark J, Bennell K. In: Physical Activity and bone health.Human Kinetics. 2001; 111-114.
Klibanski A, Biller BMK, Rosenthal DI, Schoenfeld D A, Saxe V. Effects of prolactin and oestrogendeficiency in amenorrhoeic bone loss. . Journal of Clinical Endocrinology and Metabolism; 1998.
; 67: 124-130.
Kral H, Michaelis U., Peiper H.G., Quack G., Montag M., Stimulation of bone growth throughsports; American Journal Sports medicine 1994; 22:751-7
Lindsay R. Oestrogen deficiency. In: Osteoporosis: Etiology, Diagnosis and Management, 2ndedition, edited by Riggs, B.L. and Melton L.J.Lippincott Raven, Philadelphia, 1995.133-160.
-
8/12/2019 Osteoporosis in Athletes
8/9
Lutter J.M., Prevalence of menstrual Change in Athletes and Active Women. In: The menstrualCycle and Physical Activity, edited by Puhl, J.L., and Brown, C.H. Human Kinetics, 1986; 29-44.
Matkovic V. Badenhop N.E., Landoll J.E., Mobley S.L., Calcium, hormones and bone health.Osteoporosis Int. Suppl. 2000; 4,1-11
McKay HA, Bailey DA Mirwald RL et al peak bone mineral accrual and age of menarche inadolescent girls: A6year longitudinal study J Pediatrics 1998; 133; 682-687).
Miller K, Grinspoon, S, Ciampa J, Hier J, Herzog D, Klibanski A. Medical findings in outpatientswith anorexia nervosa. Archives of Internal Medicine; 2005. ; 165: 561 -566.
Nattiv A., Agostini R., Drinkwater B., Yeager K K., The Female triad; The Athletic Woman. ClinicsIn Sports Medicine, 1994 Vol 13; 2 April. 405-418
O'Brien M " Exercise and Osteoporosis" 7th Samuel Haughton lecture, Irish Journal of MedicalScience 2001 (Volume 170, Number 1): 58-62; 27.
O'Brien M Women, Oxford Handbook of Sports and Exercise Medicine Ed Domhnall Macauley;Oxford University press 2007: 749-772.
Prior JC. Hormonal mechanisms of reproductive function and Hypothalamic adaptation toendurance training; The Menstrual Cycle And Physical Activity. Human Kinetics. 1984 63-80:
Rigby O. M., fractures, hormones and bone mineral density in competitive male mountain bikersand road cyclists, MSc Thesis Sports Medicine, Trinity College Dublin, 2002; 60,69.
Riggs, B.L., Wahner H.W., Dunn W.L., et al. Differential changes in bone mineral density of theappendicular and axial skeleton with ageing .J. Clin. Investigations 1981:67:328-335.
Rubin C.T. and Lanyon L.E. Regulation of bone formation by applied dynamic loads Journal BoneJoint Surgery 1984; 66:397-402
Sanborn C.F., Martin B.J., Wagner W.W Is athletic amenorrhea specific to runners? IS J ObstetGynaecology 1982; 142: 589
Shangold M. Menstrual disorders in: Women in exercise, edited by Shangold, M. and Mirkin G.)Philadelphia, Davis; 1988: 248-263.
Suominen H., Bone mineral density and long term exercise. An overview of cross-sectionalathlete studies Sports Medicine 1993; 16:316-30
Sundgot-Borgen, J. Prevalence of eating disorders in elite female athletes. International Journal of Sports Nutrition; 1993. ; 3: 29-40. Sundgot-Borgen, J. Eating Disorders.
In: Women in Sport (Ed. Drinkwater, B.L.) Oxford, Blackwell Science. 2000; 364-377.
-
8/12/2019 Osteoporosis in Athletes
9/9
Taafe D.R., Snow-Harter C., Connolly D.A., Robinson T.L., Marcus R., Differential effects ofswimming versus weight bearing activity on bone mineral density: Status of eumenorrhoeic
athletes.
Journal Bone Mineral Research .1995;10:586-93. Warren MP. Brooks- Gunn J., Fox RP. et al. Lack of bone accretion and amenorrhea: Evidence for
a relative Osteopenia in weight bearing bones. Clin. Endocrinol Metab. 72: 847-853, 1991
Welten D.C., Kemper H.C., Post G.B. Weight bearing activities during youth is a more importantfactor for peak bone mass than calcium, Journal Bone Mineral Research 1994; 9:1089-96
Wolff J., Das Gesetz der transformation der Knocher: Berlin Hirschwold 1892 Wolman R. L. Osteoporosis and exercise BMJ 1994; 309:400-3 Woods C. MSc in Sports Medicine Thesis Bone mineral of male jockeys, rugby players and
sedentary controls, 1999. Trinity College Dublin
Yeager K.K., Agostini R., Nattiv A., Drinkwater B., The female athlete triad; Disordered eating,amenorrhea osteoporosis Med.Sci Sports Exerc, 1993: 25:775,
Yen S.S. Neuroendocrine regulation of gonadatrophin and prolactin secretion in women. Clin.Reproductive Neuroendrocrinology N.Y.1982; 137-174.
Zanker C, Swaine I. The relationship between bone turnover, oestradiol and energy balance inwomen distance runners. British Journal of Sports Medicine; 1998. 32: 167-171.
Professor Moira O Brien FFSEM