Osteoporosis AACC PPCC web
22
4/20/2015 1 Laboratory Evaluation of Osteoporosis in Women William E. Winter, MD University of Florida Departments of Pathology and Pediatrics 2-15-2015 Case: A 65 y/o woman steps off of a curb, falls and severe pain develops in her left hip. After a 911 call, EMS brings the woman to the local ED. What is the most likely underlying case of this clinical scenario? Learning objectives: At the conclusion of this presentation, the laboratorian will be able to: 1. Describe the circumstances when the diagnosis of osteoporosis should be considered. 2. List the causes of pathological fractures. 3. Define osteoporosis. 4. Discuss the causes of osteoporosis. 5. Interpret the results of laboratory testing that is conducted during the evaluation of pt’s w/ possible osteoporosis. 6. Interpret bone marker testing results. 7. Understand the controversy that relates to the value of bone marker testing in the evaluation of osteoporosis and its therapy. Women w/: (1) Loss in height, kyphosis, other acquired skeletal deformities. (2) Low BMD on DEXA scan. (3) Fractures. Fracture Pathologic Traumatic (“Routine” Force > bone strength) (“Exceptional” Force > bone strength) Stepping off a curb ‐ > hip fracture Falling off of a tall ladder ‐ > hip fracture Under what clinical circumstances is the diagnosis of osteoporosis considered in women? BMD = bone mineral density
Transcript of Osteoporosis AACC PPCC web
4/20/2015
1
Laboratory Evaluation of Osteoporosis in Women
William E. Winter, MDUniversity of Florida
Departments of Pathology and Pediatrics2-15-2015
Case: A 65 y/o woman steps off of a curb, falls and severe pain develops in her left hip. After a 911 call, EMS brings the woman to the local ED. What is the most likely underlying case of this clinical scenario?
Learning objectives: At the conclusion of this presentation, the laboratorian will be able to:
1. Describe the circumstances when the diagnosis of osteoporosis should be considered.
2. List the causes of pathological fractures.3. Define osteoporosis.4. Discuss the causes of osteoporosis.5. Interpret the results of laboratory testing that is
conducted during the evaluation of pt’s w/ possible osteoporosis.
6. Interpret bone marker testing results.7. Understand the controversy that relates to the value
of bone marker testing in the evaluation of osteoporosis and its therapy.
Women w/:(1) Loss in height, kyphosis, other acquired skeletal deformities.(2) Low BMD on DEXA scan.(3) Fractures.
Fracture
Pathologic Traumatic
(“Routine” Force > bone strength) (“Exceptional” Force > bone strength)
Stepping off a curb ‐ > hip fracture
Falling off of a tall ladder‐ > hip fracture
Under what clinical circumstances is the diagnosis of osteoporosis considered in women?
BMD = bone mineral density

4/20/2015
2
What are the causes of pathologic fractures?
Focal bone diseaseNeoplasms‐ Malignant‐ Benign
Non‐neoplastic disease (e.g., bone cyst, osteomyelitis; dysostoses, osteonecrosis)
Generalized bone diseaseCongenital disorders (e.g., dysplasias)
Acquired disorders
See: http://www.wheelessonline.com/ortho/pathologic_fracture
What are examples of neoplasms that can cause pathologic fractures?Malignant‐ Bone cancers
‐ Malignant fibrous histiocytoma (a.k.a. ‐ fibrous histiocytoma pleomorphic sarcoma)
‐ Osteosarcoma‐ Malignant giant cell tumor of bone
‐ Non‐bone cancers (e.g., multiple myeloma)
‐ Metastasis (e.g., breast, lung, kidney, prostate, thyroid)
Benign‐ Benign fibrous histiocytoma‐ Nonossifying fibroma‐ Benign giant cell tumor of bone
What are the causes of pathologic fractures?
Focal bone diseaseNeoplasms‐ Malignant‐ Benign
Non‐neoplastic disease (e.g., bone cyst, osteomyelitis; dysostoses)
Generalized bone diseaseCongenital disorders (e.g., dysplasias)
Acquired disorders
See: http://www.wheelessonline.com/ortho/pathologic_fracture

4/20/2015
3
What are examples of dysplasias that can cause pathologic fractures?Dysplasia: congenital, global disorders of abnormal tissue development affecting cartilage and bone.
Examples EtiologiesAchondroplasia GOF mutation in FGFR3
Thanatophoric dysplasia “ “ “
Osteopetrosis LOF in osteoclasts
Osteogenesis imperfecta Mutations in alpha 1 or alpha 2 chains that constitute type 1 collagen
McCune‐Albright syn. LOF in GS ATPase
In DD of osteoporosis
What are the causes of pathologic fractures?
Focal bone diseaseNeoplasms‐ Malignant‐ Benign
Non‐neoplastic disease (e.g., bone cyst, osteomyelitis; dysostoses)
Generalized bone diseaseCongenital disorders (e.g., dysplasias)
Acquired disorders
See: http://www.wheelessonline.com/ortho/pathologic_fracture
Besides osteoporosis, what are examples of generalized, “acquired” disorders that can cause pathologic fractures?
Examples EtiologiesRickets / Osteomalacia Decr. vit D activity; hypophosphatemia
10 hyperparathyroidism Excess PTH activity
Renal osteodystrophy Vit D def., hyperphosphatemia,20 hyperparathyroidism
Paget disease of bone Excess bone turnover
Humoral hypercalcemia of Malignancy: PTHrP
Scurvy Dietary vitamin C def.
Gaucher disease Inborn error of sphingomyelin metab.
In DD of osteoporosis

4/20/2015
4
What is osteoporosis?
NIH Consensus Statement, Vol 17 (1), March 27-29, 2000
“. . . . (A) skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture.”
Eponym: “Porous bone disease”
Consequences Loss in height, collapsedof reduced bone vertebra, lumbar lordosis; strength: kyphosis; scoliosis;
factures & associated mortality
Most common fractures: Hip, spine, and wrist
11
12
Bone density- gm/area or volume of bone - Bone mineral density = ~70% of bone strength
What determines bone strength?
Bone quality- Architecture- Bone turnover- Damage accumulation- Mineralization
Note: Can not measure bone strength directlyCan measure bone density (DEXA scan)
Young Old
Vertebral bodies

4/20/2015
5
What is the biology of osteoporosis in adults?
Following attainment of maximum adult BMD, over time:
Osteoclast activity > Osteoblast activity
Outcome: - Reduced bone density (= osteopenia)- Disordered microarchitecture
Scanning electron microscopy of 3rd lumbar vertebra.
Normal Osteoporosis
Resorb bone Build bone
What cells build bone and which cells resorb bone?
Function Origin
Osteoblasts Build bone Mesoderm
Osteoclasts Resorb bone BM stem cell
15
A
B
DE
OSTEOCLAST (resorption)
C
OSTEOBLAST (formation)
What is the cycle of normal bone turnover?
“Basic multicellular unit”*
* includes osteocytes

4/20/2015
6
16
Macrophage
M‐CSF
OPG
RANKL
M-CSF = macrophage colony stimulating factor; OPG = osteoprotegerin; RANK = receptor activator of nuclear factor NF kappaB
Osteoblast
Intermittent PTH
Monocyte
Osteoclastprecursor
RANK
What regulates osteoclasts?
Stromal (osteoprogenitor) cell
A mesenchymalcell
HSC
Restingosteoclast
Precursor
fusion
17
NOTE: Normal pulses of PTH (“intermittent” secretion) from the parathyroid gland stimulate the development of osteoblasts from stromal cells.
Stimulated osteoblasts secrete macrophage colony‐stimulating factor (M‐CSF). This stimulates the replication of macrophages into osteoclast precursors.
Osteoblasts also express on their surface osteoclast differentiating factor (ODF) which stimulate osteoclast precursors differentiation into osteoclasts. ODF is also known as receptor activator of NF kappaB ligand (RANKL) and osteoprotegerin‐ligand (OPGL).
Osteoprotegerin (OPG), secreted by osteoblasts, antagonizes the effects of RANKL. OPG serves as a soluble decoy receptor for RANKLantagonizing RANKL’s ability to bind to its receptor which is RANK on osteoclast precursors.
18
Restingosteoclast
OsteoprotegerenRANKL
Osteoclastprecursor
Inhibitionof osteoclast
activation
Stimulationof osteoclastactivation;precursorfusion
Osteoblast
(incr. expression w/ IL‐1, IL‐6, IL‐11, TNF)
RANK
Competition
Therefore: Osteoblasts regulate osteoclasts
See fig 26‐3, Robbins
4/20/2015
7
19
Osteoprotegeren
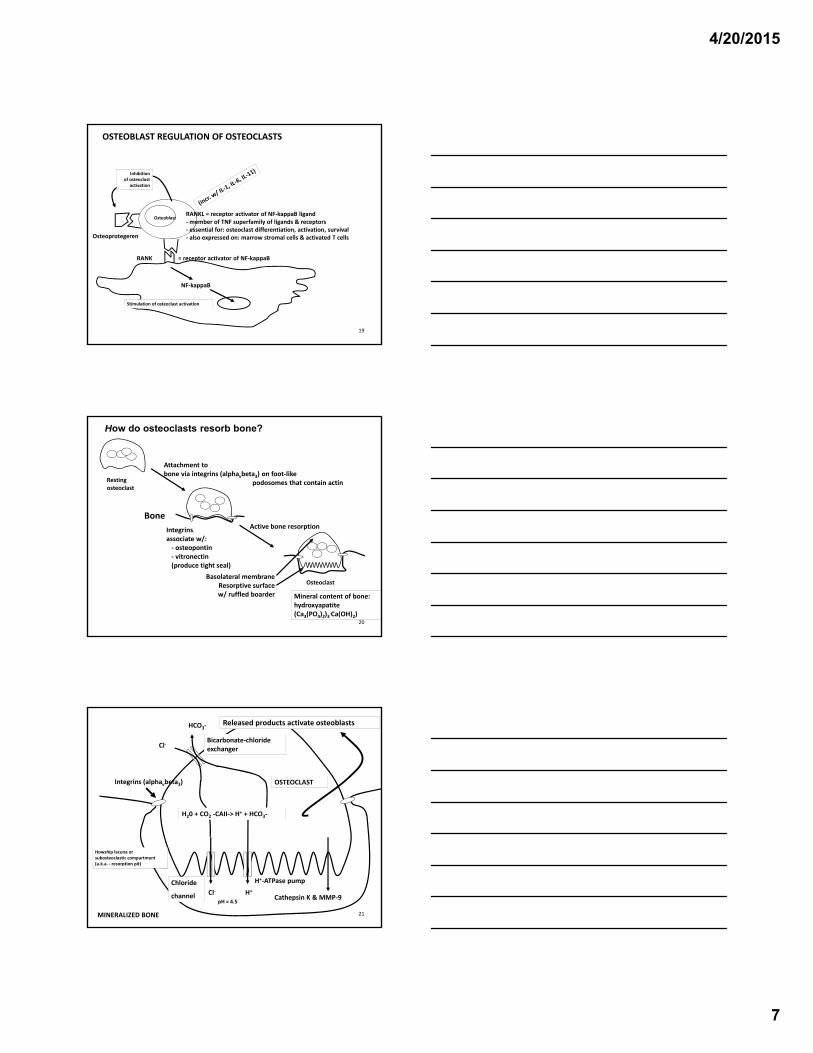
RANKL = receptor activator of NF‐kappaB ligand‐member of TNF superfamily of ligands & receptors‐ essential for: osteoclast differentiation, activation, survival‐ also expressed on: marrow stromal cells & activated T cells
RANK = receptor activator of NF‐kappaB
OSTEOBLAST REGULATION OF OSTEOCLASTS
Inhibitionof osteoclast
activation
Stimulation of osteoclast activation
Osteoblast
NF‐kappaB
20
Restingosteoclast
Bone
Attachment tobone via integrins (alphavbeta3) on foot‐like
podosomes that contain actin
Osteoclast
Active bone resorptionIntegrins associate w/:‐ osteopontin‐ vitronectin(produce tight seal)
Basolateral membraneResorptive surfacew/ ruffled boarder Mineral content of bone:
hydroxyapatite(Ca3(PO4)2)3
.Ca(OH)2)
How do osteoclasts resorb bone?
21MINERALIZED BONE
Bicarbonate‐chloride exchanger
OSTEOCLASTIntegrins (alphavbeta3)
Cathepsin K & MMP‐9H+
H+‐ATPase pump
pH = 4.5
Cl‐
Cl‐Chloride
channel
HCO3‐
H20 + CO2 ‐CAII‐> H+ + HCO3‐
Howship lacuna or subosteoclastic compartment(a.k.a. ‐ resorption pit)
Released products activate osteoblasts
4/20/2015
8
22
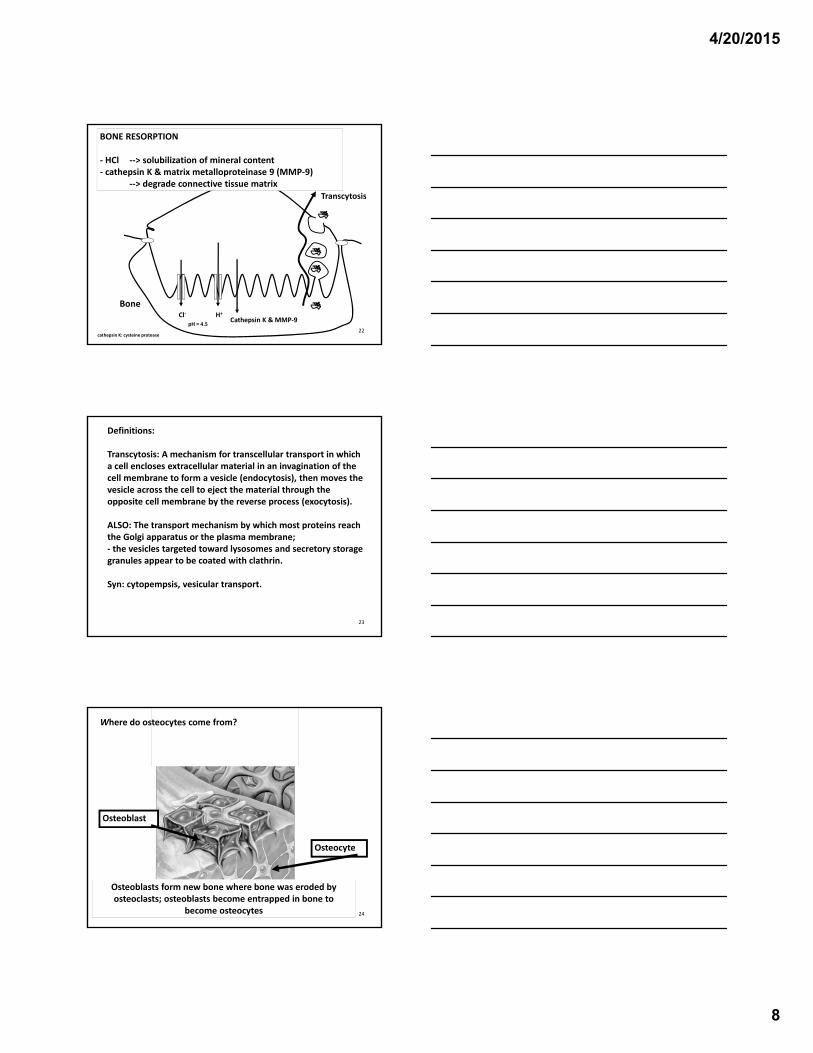
Transcytosis
BONE RESORPTION
‐ HCl ‐‐> solubilization of mineral content‐ cathepsin K & matrix metalloproteinase 9 (MMP‐9)
‐‐> degrade connective tissue matrix
Bone
cathepsin K: cysteine protease
H+
pH = 4.5
Cl‐Cathepsin K & MMP‐9
23
Definitions:
Transcytosis: A mechanism for transcellular transport in which a cell encloses extracellular material in an invagination of the cell membrane to form a vesicle (endocytosis), then moves the vesicle across the cell to eject the material through the opposite cell membrane by the reverse process (exocytosis).
ALSO: The transport mechanism by which most proteins reach the Golgi apparatus or the plasma membrane; ‐ the vesicles targeted toward lysosomes and secretory storage granules appear to be coated with clathrin.
Syn: cytopempsis, vesicular transport.
24
Osteoblasts form new bone where bone was eroded byosteoclasts; osteoblasts become entrapped in bone to
become osteocytes
Osteoblast
Osteocyte
Where do osteocytes come from?

4/20/2015
9
25
Nutrition: dietary Ca++ intake and absorption (Vit D)*
Exercise & Gravity : load bearing (fosters bone remodeling)
Sex steroidsE2 (women and men) Testosterone (men)
Growth hormone
Thyroid hormone
* Need: Functional intestine & 1,25(OH)2D; 1,25(OH)2D is a function of 25(OH)D, PTH, PO4
‐‐‐, renal tubular cell
What maintains bone mass?
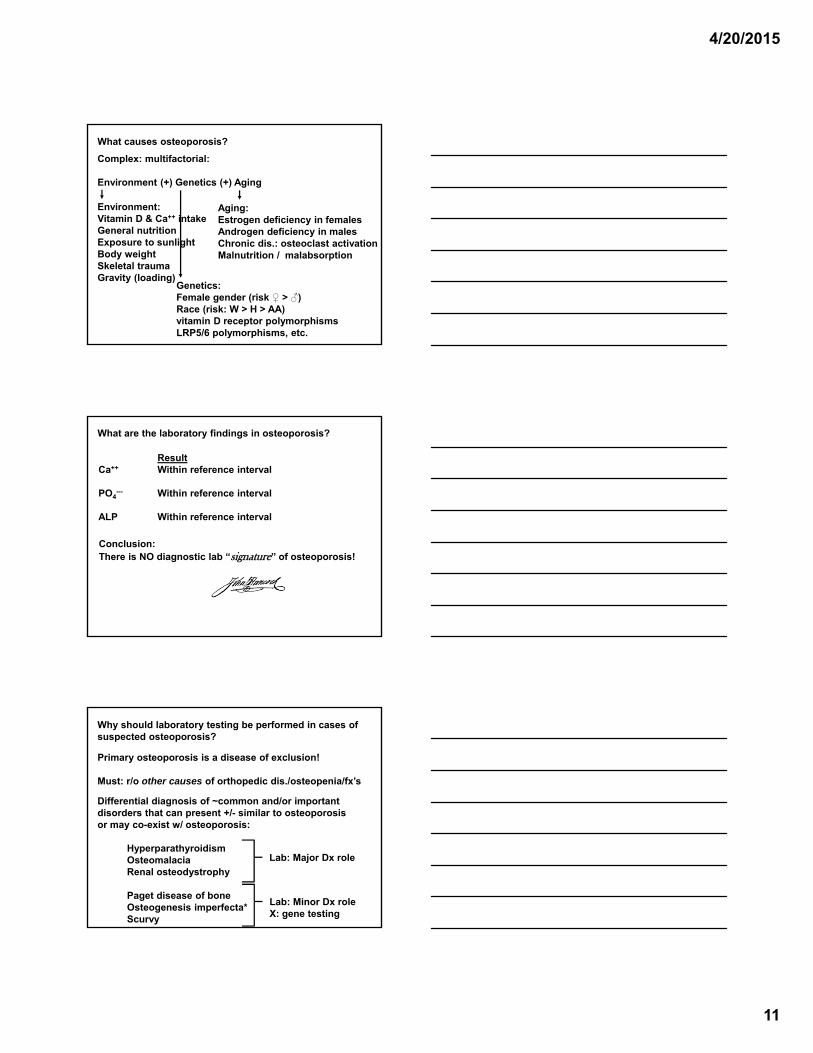
What causes osteoporosis?
Complex: multifactorial:
Environment (+) Genetics (+) Aging
Environment:Vitamin D & Ca++ intakeGeneral nutritionExposure to sunlightBody weightSkeletal traumaCurrent smoking
Genetics:Female gender (risk ♀ > ♂)Race (risk: W > H > AA)FHx of osteoporosis or fractureGene polymorphisms, etc.
Aging:Estrogen deficiency in femalesAndrogen deficiency in malesChronic dis.: osteoclast activationMalnutrition / malabsorption
What environmental factors contribute to osteoporosis?
Environment (+) Genetics (+) Aging
Environment: Incr. risk w/:
Vitamin D & Ca++ intake Low intakeGeneral nutrition Poor nutritionExposure to sunlight Lack of exposureBody weight Low body weightSkeletal trauma History of previous fractureCurrent smoking Chronic inflammationDrugs Glucocorticoids (>3 mo),

4/20/2015
10
What genetic factors contribute to osteoporosis?
Environment (+) Genetics (+) Aging
Genetics: Comment:
Female gender Risk ♀ > ♂Race W > H > AAFHx of osteoporosis In 10 relative(s)FHx of fractures In 10 relative(s)Gene polymorphisms Vitamin D receptor
LRP5/6(+) ~=>80 other genes
Genome Med. 2013 May 29;5(5):44. doi: 10.1186/gm448. eCollection 2013.Genome-wide approaches for identifying genetic risk factors for osteoporosis.Wu S1, Liu Y2, Zhang L3, Han Y1, Lin Y1, Deng HW3.Author informationAbstract
Osteoporosis, the most common type of bone disease worldwide, is clinically characterized by low bone mineral density (BMD) and increased susceptibility to fracture. Multiple genetic and environmental factors and gene-environment interactions have been implicated in its pathogenesis. Osteoporosis has strong genetic determination, with the heritability of BMD estimated to be as high as 60%. More than 80 genes or genetic variants have been implicated in risk of osteoporosis by hypothesis-free genome-wide studies. However, these genes or genetic variants can only explain a small portion of BMD variation, suggesting that many other genes or genetic variants underlying osteoporosis risk await discovery. Here, we review recent progress in genome-wide studies of osteoporosis and discuss their implications for medicine and the major challenges in the field.
How does aging contribute to osteoporosis?
Environment (+) Genetics (+) Aging
Aging: Comment:
Estrogen deficiency MenopauseAndrogen deficiency AndropauseChronic disease Cytokine-induced
osteoclast activationMalnutrition Impaired appetite w\ agingMalabsorption Impaired absorption w\ aging
4/20/2015
11
What causes osteoporosis?
Complex: multifactorial:
Environment (+) Genetics (+) Aging
Environment:Vitamin D & Ca++ intakeGeneral nutritionExposure to sunlightBody weightSkeletal traumaGravity (loading)
Genetics:Female gender (risk ♀ > ♂)Race (risk: W > H > AA)vitamin D receptor polymorphismsLRP5/6 polymorphisms, etc.
Aging:Estrogen deficiency in femalesAndrogen deficiency in malesChronic dis.: osteoclast activationMalnutrition / malabsorption
What are the laboratory findings in osteoporosis?
ResultCa++ Within reference interval
PO4--- Within reference interval
ALP Within reference interval
Conclusion:There is NO diagnostic lab “signature” of osteoporosis!
Why should laboratory testing be performed in cases of suspected osteoporosis?
Primary osteoporosis is a disease of exclusion!
Must: r/o other causes of orthopedic dis./osteopenia/fx’s
Differential diagnosis of ~common and/or important disorders that can present +/- similar to osteoporosis or may co-exist w/ osteoporosis:
HyperparathyroidismOsteomalaciaRenal osteodystrophy
Paget disease of boneOsteogenesis imperfecta*Scurvy
Lab: Major Dx role
Lab: Minor Dx roleX: gene testing
4/20/2015
12
How can hyperparathyroidism be diagnosed in women with orthopedic disease, osteopenia and/or fractures?
ResultCa++ Increased
PO4--- Decreased (or low normal)
ALP Increased (PTH - > osteoblast - > ALP)
Next diagnostic steps:Always: r/o renal disease (w/ untx’ed CRF: +/- incr. PO4
---)
Confirm hypercalcemia: iCa++ (or alb): r/o dehydration
Measure: PTH (WNL or incr. = 10 hyperparathyroidism)
How can osteomalacia be diagnosed in women with orthopedic disease, osteopenia and/or fractures?
ResultCa++ Usually: lower range of reference interval
PO4--- Decreased (Incr. PTH - > hyperphosphaturia
- > hypophosphatemia)
ALP Increased (PTH - > osteoblast - > ALP)
Next diagnostic steps: (r/o renal disease)Measure:
PTH (incr. = 20 hyperparathyroidism)
25-OHD (decr. w/ vit D def.)- Many rare forms: hepatic rickets, VDDR, VDRR, etc.

4/20/2015
13
How can renal osteodystrophy be diagnosed in women with orthopedic disease, osteopenia and/or fractures?
ResultCa++ Within reference interval
PO4--- Increased (PO4
--- retention)
ALP Increased (PTH - > osteoblast - > ALP)
Cr Increased (decr. eGFR, CrCl)
Next diagnostic steps:
Measure: PTH (incr. = 20 hyperparathyroidism)
How can Paget disease of bone (osteitis deformans) be diagnosed in women with orthopedic disease and/or fractures?
ResultCa++ Within reference interval
PO4--- Within reference interval
ALP Increased (cytokine? - > osteoblast - > ALP)
Paget disease of bone: Not a lab diagnosis!
Physical examination: deformities; hearing, CN problems
Radiologic findings
Remember: r/o renal disease
How can osteogenesis imperfecta be diagnosed in women with orthopedic disease, osteopenia and/or fractures?
ResultCa++ Within reference interval
PO4--- Within reference interval
ALP Increased w/ fracture
Osteogenesis imperfecta: Not a chem. lab diagnosis!
Brittle bones that fracture+/- Hearing loss; blue sclera; dental problemsMany disorders w/ variable severity
Radiologic findings: Extremely helpful; Gene testing avail.

4/20/2015
14
How can scurvy be diagnosed in women with orthopedic disease and/or fractures?
ResultCa++ Within reference interval
PO4--- Within reference interval
ALP Increased w/ fracture
Scurvy: ~Not a chem. lab diagnosis (unless vit C is measured)! (Dietary vit C def.)
4 H’s: Hemorrhage, hyperkeratosis, hypochondriasis*, and hematologic abnormalities (anemia from blood loss).
*an overwhelming fear that you have a serious disease, even though health care providers can find no evidence of illness.
Plain film
This is the preferred initial examination.
head, neck and spinebasilar invaginationwormian boneskyphoscoliosisvertebral compression fracturescodfish vertebraeplatyspondyly
chestpectus excavatum or carinatum
pelvisacetabular protrusio
generalsevere osteoporosisdeformed, gracile (over-tubulated) bonescortical thinninghyperplastic callus formationpopcorn calcification: the metaphyses and epiphyses exhibit numerous scalloped radiolucent areas with
sclerotic margins 1zebra stripe sign: cyclic bisphosphonate treatment produces sclerotic growth recovery lines in the long bonesexuberant callus formationformation of pseudarthrosis at sites of healing fractures
Source: http://radiopaedia.org/articles/osteogenesis-imperfecta-1
How can bone formation be evaluated through laboratory testing?
Markers of bone formation (incr. = bone accretion)Marker Comment
Bone alkaline Produced by osteoblastsphosphatase(BAP)
Osteocalcin Produced by osteoblastsNon-collagenous bone matrix protein
Procollagen Formed by conversion of procollagenN-terminal -- > collagenpropeptide(s-PINP)

4/20/2015
15
How is procollagen N-terminal propeptide (s-PINP) formed?
Procollagen N-terminal propeptide (s-PINP)
Procollagen
Procollagen amino proteinase Procollagen carboxy proteinase
How can bone turnover be evaluated through laboratory testing?
Markers of bone degradationMarker CommentN-telopeptides Bone collagen degradation product
Urine NTx 30-40% decr. from NTx baseline post-3 mos tx = typical response to anti-resorptive therapy.*
Serum NTx Target value for tx’ed post-menopausal women = premeno-pausal reference interval.**
Urine C-telo- Bone collagen degradation productPeptides (CTx)* http://ltd.aruplab.com/Tests/Pub/0070062; ** http://ltd.aruplab.com/Tests/Pub/0070500
How are NTx and CTx formed?

4/20/2015
16
One NTx assay: ex:MoAb 1H11 to this octapeptide
NTx from N-terminus of α2 collagen protein
N-Telopeptide: released with collagen degradation
CTx, CrossLapsTM
assay: MoAb to thisoctapeptide
Type 1 collagen
C-Telopeptide: released with collagen degradation
How can bone turnover be evaluated through laboratory testing?
Markers of bone degradationMarker Comment
Urine deoxy- Bone collagen degradation productpyridinoline Target value for tx’ed post-(DPD) menopausal women = premeno-
pausal reference interval.*
Urine pyridino- Bone collagen degradation productline
* http://ltd.aruplab.com/Tests/Pub/0070212

4/20/2015
17
HO
NH2
CH‐COOH
CH2
N
CH2‐CH‐CH2‐CH2‐CH‐COOH
OH NH2
CH2‐CH2‐CH‐COOH
NH2
Pyridinoline
HO
NH2
CH‐COOH
CH2
N
CH2‐CH2‐CH2‐CH2‐CH‐COOH
NH2
CH2‐CH2‐CH‐COOH
NH2
Deoxypyridinoline(more bone-specific)
How are deoxypyridinoline and pyridinoline formed?
Pyridinium crosslinks: either: - pyridinoline or deoxypyridinoline
Released w/ collagen breakdown
How can bone turnover be evaluated through laboratory testing?
Markers of bone degradationMarker Comment
Tartrate-resistant Produced by osteoclastsacid phosphatase - reflect bone resorption(TRACP5b)
4/20/2015
18
Ir J Med Sci. 2014 Mar;183(1):47-52. doi: 10.1007/s11845-013-0970-6. Epub 2013 Jun 5.Limited utility of tartrate-resistant acid phosphatase isoform 5b in assessing response to therapy in osteoporosis.Brady JJ1, Crowley RK, Murray BF, Kilbane MT, O'Keane M, McKenna MJ.Author informationAbstractBACKGROUND:
Tartrate-resistant acid phosphatase isoform 5b (TRACP5b) is a serum bone resorption marker. Our aim was to investigate its utility in monitoring metabolic bone disease.METHODS:
Serum TRACP5b, C-terminal cross-linking telopeptide of type I collagen, urine N-terminal cross-linking telopeptide of type I collagen and free deoxypyridinoline were measured pre- and post-treatment with a parathyroid hormone analogue [PTH (1-34)] (n = 14) or a bisphosphonate (N-BP) (n = 8). TRACP5b, bone alkaline phosphatase (bone ALP), 25-hydroxyvitamin D (25OHD) and parathyroid hormone (PTH) were measured in 100 osteoporosis patients on prolonged bisphosphonate therapy.RESULTS:
Changes in TRACP5b were smaller in magnitude but mimicked those of other bone resorption markers. Absolute changes in TRACP5b and the other resorption markers correlated significantly (p < 0.001). In patients on long-term bisphosphonates, TRACP5b and bone ALP levels were not suppressed. Vitamin D status was consistent with the level of supplementation.CONCLUSION:
TRACP5b has limited utility as a single marker of metabolic bone disease treatment.
Clin Lab. 2006;52(9-10):499-509.Tartrate-resistant acid phosphatase 5b (TRACP 5b) as a marker of bone resorption.Halleen JM1, Tiitinen SL, Ylipahkala H, Fagerlund KM, Väänänen HK.Author informationAbstract
Tartrate-resistant acid phosphatase (TRACP) is an enzyme that is expressed in high amounts by bone resorbing osteoclasts, inflammatory macrophages and dendritic cells. Two forms of TRACP circulate in human blood, TRACP 5a derived from macrophages and dendritic cells, and TRACP 5b derived from osteoclasts. Recent data have demonstrated the utility of TRACP 5b as a marker of osteoclast number and bone resorption, and serum TRACP 5a as a marker of inflammatory conditions. This review summarizes the scientific knowledge on the role of TRACP in osteoclastic bone resorption, the mechanism of TRACP 5b generation in osteoclasts and its secretion into the blood circulation, the methodology of measuring TRACP 5b, diagnostic evidence for the use of TRACP 5b as a resorption marker, and characteristics of TRACP 5b compared to other commonly used bone turnover markers.
What are other novel bone markers?
Marker Comment
Sclerostin Produced by osteocytes- negative regulator of bone mass
Inter alpha-trypsin- Serum-borne reflection of the inhibitor heavy increased osteoclast activitychain H4 precursor(ITIH4)

4/20/2015
19
What are other novel bone markers?
Marker Comment
Undercarboxylated Used to assess the vitamin K osteocalcin (ucOC) status in bone metabolism
Serum N-terminal Stable fragment of osteocalcinmidfragment Osteocalcin
Bone sialoprotein Produced by osteoblasts- Fn (?): protein nucleator of hydroxyapatite crystal formation
What are other novel bone markers?
Marker Comment
Osteoprotegerin Produced by osteoblasts(OPG) - Decoy receptor for RANKL
N-terminal propeptide Serum concentrations correlateof the C-type with bone cortical area and natriuretic peptide endosteal circumference(NT-proCNP)
J Bone Joint Surg Am. 2014 Oct 1;96(19):1659-68. doi: 10.2106/JBJS.M.01096.A review of osteocyte function and the emerging importance of sclerostin.Compton JT1, Lee FY1.Author informationAbstract
➤ Osteocytes, derived from osteoblasts, reside within bone and communicate extensively with other bone cell populations to regulate bone metabolism. The mature osteocyte expresses the protein sclerostin, a negative regulator of bone mass.➤ In normal physiologic states, the protein sclerostin acts on osteoblasts at the surface of bone and is differentially expressed in response to mechanical loading, inflammatory molecules such as prostaglandin E2, and hormones such as parathyroid hormone and estrogen.➤ Pathologically, sclerostin dysregulation has been observed in osteoporosis-related fractures, failure of implant osseous integration, metastatic bone disease, and select genetic diseases of bone mass.➤ An antibody that targets sclerostin, decreasing endogenous levels of sclerostin while increasing bone mineral density, is currently in phase-III clinical trials.➤ The osteocyte has emerged as a versatile, indispensable bone cell. Its location within bone, extensive dendritic network, and close communication with systemic circulation and other bone cells produce many opportunities to treat a variety of orthopaedic conditions.
4/20/2015
20
Arch Biochem Biophys. 2014 Nov 1;561:74-87. doi: 10.1016/j.abb.2014.07.034. Epub 2014 Aug 23.Bone tissue remodeling and development: focus on matrix metalloproteinase functions.Paiva KB1, Granjeiro JM2.Author informationAbstract
Bone-forming cells originate from distinct embryological layers, mesoderm (axial and appendicular bones) and ectoderm (precursor of neural crest cells, which mainly form facial bones). These cells will develop bones by two principal mechanisms: intramembranous and endochondral ossification. In both cases, condensation of multipotent mesenchymal cells occurs, at the site of the future bone, which differentiate into bone and cartilage-forming cells. During long bone development, an initial cartilaginous template is formed and replaced by bone in a coordinated and refined program involving chondrocyte proliferation and maturation, vascular invasion, recruitment of adult stem cells and intense remodeling of cartilage and bone matrix. Matrix metalloproteinases (MMPs) are the most important enzymes for cleaving structural components of the extracellular matrix (ECM), as well as other non-ECM molecules in the ECM space, pericellular perimeter and intracellularly. Thus, the bioactive molecules generated act on several biological events, such as development, tissue remodeling and homeostasis. Since the discovery of collagenase in bone cells, more than half of the MMP members have been detected in bone tissues under both physiological and pathological conditions. Pivotal functions of MMPs during development and bone regeneration have been revealed by knockout mouse models, such as chondrocyte proliferation and differentiation, osteoclast recruitment and function, bone modeling, coupling of bone resorption and formation (bone remodeling), osteoblast recruitment and survival, angiogenesis, osteocyte viability and function (biomechanical properties); as such alterations in MMP function may alter bone quality. In this review, we look at the principal properties of MMPs and their inhibitors (TIMPs and RECK), provide an up-date on their known functions in bone development and remodeling and discuss their potential application to Bone Bioengineering.
J Bone Miner Res. 2008 Jul;23(7):1106-17. doi: 10.1359/jbmr.080235.Serum biomarker profile associated with high bone turnover and BMD in postmenopausal women.Bhattacharyya S1, Siegel ER, Achenbach SJ, Khosla S, Suva LJ.Author informationAbstract
Early diagnosis of the onset of osteoporosis is key to the delivery of effective therapy. Biochemical markers of bone turnover provide a means of evaluating skeletal dynamics that complements static measurements of BMD by DXA. Conventional clinical measurements of bone turnover, primarily the estimation of collagen and its breakdown products in the blood or urine, lack both sensitivity and specificity as a reliable diagnostic tool. As a result, improved tests are needed to augment the use of BMD measurements as the principle diagnostic modality. In this study, the serum proteome of 58 postmenopausal women with high or low/normal bone turnover (training set) was analyzed by surface enhanced laser-desorption/ionization time-of-flight mass spectrometry, and a diagnostic fingerprint was identified using a variety of statistical and machine learning tools. The diagnostic fingerprint was validated in a separate distinct test set, consisting of serum samples from an additional 59 postmenopausal women obtained from the same Mayo cohort, with a gap of 2 yr. Specific protein peaks that discriminate between postmenopausal patients with high or low/normal bone turnover were identified and validated. Multiple supervised learning approaches were able to classify the level of bone turnover in the training set with 80% sensitivity and 100% specificity. In addition, the individual protein peaks were also significantly correlated with BMD measurements in these patients. Four of the major discriminatory peaks in the diagnostic profile were identified as fragments of interalpha-trypsin-inhibitor heavy chain H4 precursor (ITIH4), a plasma kallikrein-sensitive glycoprotein that is a component of the host response system. These data suggest that these serum protein fragments are the serum-borne reflection of the increased osteoclast activity, leading to the increased bone turnover that is associated with decreasing BMD and presumably an increased risk of fracture. In conjunction with the identification of the individual proteins, this protein fingerprint may provide a novel approach to evaluate high bone turnover states.
Clin Calcium. 2009 Dec;19(12):1815-21. doi: CliCa091218151821.[Clinical implications of undercarboxylated osteocalcin].[Article in Japanese]Hosoi T1.Author informationAbstract
Importance of vitamin K has been suggested to maintain and improve bone strength. The serum concentration of undercarboxylated osteocalcin (ucOC) is utilized to assess the vitamin K status in bone metabolism. The clinical threshold for ucOC has been determined to discriminate the people at risk for fragility fractures from the view points of vitamin K metabolism. The measurement of ucOC would be useful to select the patients who require vitamin K(2) regimen and to assess the effectiveness of vitamin K(2) therapy.
Cytokine Growth Factor Rev. 2013 Oct;24(5):401-9. doi: 10.1016/j.cytogfr.2013.06.001. Epub 2013 Jul 1.Osteoprotegerin: multiple partners for multiple functions.Baud'huin M1, Duplomb L, Teletchea S, Lamoureux F, Ruiz-Velasco C, Maillasson M, Redini F, Heymann MF, Heymann D.
Osteoprotegerin (OPG) is an essential secreted protein in bone turnover due to its role as a decoy receptor for the Receptor Activator of Nuclear Factor-kB ligand (RANKL) in the osteoclasts, thus inhibiting their differentiation. However, there are additional ligands of OPG that confer various biological functions. OPG can promote cell survival, cell proliferation and facilitates migration by binding TNF-related apoptosis inducing ligand (TRAIL), glycosaminoglycans or proteoglycans. A large number of in vitro, pre-clinical and clinical studies provide evidences of OPG involvement in vascular, bone, immune and tumor biology. This review describes an overview of the different OPG ligands regulating its biological functions.

4/20/2015
21
Horm Res Paediatr. 2010;74(3):201-6. doi: 10.1159/000282111. Epub 2010 Jun 10.N-terminal C-type natriuretic propeptide is associated with the endosteal apposition of bone in females with a persistent eating disorder.Fricke O1, Beccard R, Semler O, Stabrey A, Tutlewski B, Lehmkuhl G, Schoenau E.Author informationAbstractBACKGROUND/AIM:
Females with anorexia nervosa (AN) are often affected by osteoporosis. The study intends to investigate the association between serum levels of the N-terminal propeptide of the C-type natriuretic peptide (NT-proCNP) and bone development in anorexic females.SUBJECTS AND METHODS:
In a catamnestic visit, 21 females, formerly treated for AN, were assessed for the presence of eating disorders and analyzed for bone parameters of the distal radius (4% site) with peripheral quantitative computed tomography (pQCT), for maximal isometric grip force (MIGF) and for NT-proCNP serum levels.RESULTS:
The 9 females with a persistent eating disorder had lower height and weight than the recovered girls. NT-proCNP was correlated with the cortical area (r = 0.521), the endosteal circumference (CE, r = -0.468) and the ratio of MIGF to cross-sectional bone area (r = 0.434). CE explained 40% of the variance of NT-proCNP in females with persistent eating disorders, but was not associated with NT-proCNP in recovered girls (p = 0.691). The association between CE and NT-proCNP was not existent when the correlation was controlled for the duration of amenorrhea and the supplemented cumulative dose of ethinylestradiol (p = 0.275).CONCLUSION:
NT-proCNP reflects metaphyseal inwaisting which is modified by estrogens and the pressure on the growth plate.
What is the value of bone marker testing in the evaluation of osteoporosis and its therapy?
“BTMs (bone turnover markers) are widely used in bone research including therapeutic trials of new medications for osteoporosis and other bone disease. Whilst further data are awaited to confirm their utility in the clinical management of osteoporosis, they are currently used in specialist clinical practices, especially in monitoringtreatment.”
-Vasikaran SD, Chubb SA, Schneider HG Towardsoptimising the provision of laboratory services for bone turnover markers. Pathology. 2014 Jun;46(4):267-73.
Summary
Osteoporosis is NOT a biochemical diagnosis
Laboratory testing to: r/o:
HyperparathyroidismOsteomalaciaRenal osteodystrophy
Clinical/radiologic evaluation for:
Paget disease of boneOsteogenesis imperfecta
Bone turnover markers: clinical value?
4/20/2015
22
THE END
What is hypophosphatasia?
Hypophosphatasia is an inherited disorder that affects the development of bones and teeth. This condition disrupts a process called mineralization, in which minerals such as calcium and phosphorus are deposited in developing bones and teeth. Mineralization is critical for the formation of bones that are strong and rigid and teeth that can withstand chewing and grinding.
The signs and symptoms of hypophosphatasia vary widely and can appear anywhere from before birth to adulthood. The most severe forms of the disorder tend to occur before birth and in early infancy. Hypophosphatasia weakens and softens the bones, causing skeletal abnormalities similar to another childhood bone disorder called rickets. Affected infants are born with short limbs, an abnormally shaped chest, and soft skull bones. Additional complications in infancy include poor feeding and a failure to gain weight, respiratory problems, and high levels of calcium in the blood (hypercalcemia), which can lead to recurrent vomiting and kidney problems. These complications are life‐threatening in some cases.
The forms of hypophosphatasia that appear in childhood or adulthood are typically less severe than those that appear in infancy. Early loss of primary (baby) teeth is one of the first signs of the condition in children. Affected children may have short stature with bowed legs or knock knees, enlarged wrist and ankle joints, and an abnormal skull shape. Adult forms of hypophosphatasia are characterized by a softening of the bones known as osteomalacia. In adults, recurrent fractures in the foot and thigh bones can lead to chronic pain. Affected adults may lose their secondary (adult) teeth prematurely and are at increased risk for joint pain and inflammation.
The mildest form of this condition, called odontohypophosphatasia, only affects the teeth. People with this disorder typically experience abnormal tooth development and premature tooth loss, but do not have the skeletal abnormalities seen in other forms of hypophosphatasia.How common is hypophosphatasia?
Severe forms of hypophosphatasia affect an estimated 1 in 100,000 newborns. Milder cases, such as those that appear in childhood or adulthood, probably occur more frequently.
Hypophosphatasia has been reported worldwide in people of various ethnic backgrounds. This condition appears to be most common in Caucasian (white) populations. It is particularly frequent in a Mennonite population in Manitoba, Canada, where about 1 in 2,500 infants is born with severe features of the condition.What genes are related to hypophosphatasia?
Mutations in the ALPL gene cause hypophosphatasia.
The ALPL gene provides instructions for making an enzyme called alkaline phosphatase. This enzyme plays an essential role in mineralization of the skeleton and teeth. Mutations in the ALPL gene lead to the production of an abnormal version of alkaline phosphatase that cannot participate effectively in the mineralization process. A shortage of alkaline phosphatase allows several other substances, which are normally processed by the enzyme, to build up abnormally in the body. Researchers believe that a buildup of one of these compounds, inorganic pyrophosphate (PPi), underlies the defective mineralization of bones and teeth in people with hypophosphatasia.
ALPL mutations that almost completely eliminate the activity of alkaline phosphatase usually result in the more severe forms of hypophosphatasia. Other mutations, which reduce but do not eliminate the activity of the enzyme, are often responsible for milder forms of the condition.
Read more about the ALPL gene.How do people inherit hypophosphatasia?
The severe forms of hypophosphatasia that appear early in life are inherited in an autosomal recessive pattern. Autosomal recessive inheritance means that two copies of the gene in each cell are altered. Most often, the parents of an individual with an autosomal recessive disorder each carry one copy of the altered gene but do not show signs and symptoms of the disorder.
Milder forms of hypophosphatasia can have either an autosomal recessive or an autosomal dominant pattern of inheritance. Autosomal dominant inheritance means that one copy of the altered gene in each cell is sufficient to cause the disorder.
Source: http://ghr.nlm.nih.gov/condition/hypophosphatasia