
OSCE2 - mehtahospital.com fileOSCE2 Answers (1/2X10=05Marks) a)...
28
OSCE 2 Answers (1/2 X 10 = 05 Marks) a) Double blinded placebo controlled randomized clinical trial b) The outcome measures considered were clinical (duration taken, hospital stay, sequel, deaths and rate of adverse reactions) , bacteriological cure and neurological status after one year. c) Duration taken for clinical improvement, hospital stay – Mean (Sd) (Continuous data) ,Sequel, deaths and rate of adverse reactions and bacteriological cure – Proportions (discrete data) d) Tables & Diagrams e) Continuous data – Student t test , discrete data – Chi square test f) Type ( Quantitative / Qualitative ) and distribution (normal / skewed ) of data, sample size(Large / small) Number of groups , g) Selection bias , measurement bias – Randomization , blinding h) CONSORT (Consolidated Standards of reporting Trials) i) Yes j) 10.67% , Yes
Transcript of OSCE2 - mehtahospital.com fileOSCE2 Answers (1/2X10=05Marks) a)...

OSCE 2
Answers (1/2 X 10 = 05 Marks)
a) Double blinded placebo controlled randomized clinical trial
b) The outcome measures considered were clinical (duration taken,
hospital stay, sequel, deaths and rate of adverse reactions) ,
bacteriological cure and neurological status after one year.
c) Duration taken for clinical improvement, hospital stay – Mean (Sd)
(Continuous data) ,Sequel, deaths and rate of adverse reactions
and bacteriological cure – Proportions (discrete data)
d) Tables & Diagrams
e) Continuous data – Student t test , discrete data – Chi square test
f) Type ( Quantitative / Qualitative ) and distribution (normal /
skewed ) of data, sample size(Large / small) Number of groups ,
g) Selection bias , measurement bias – Randomization , blinding
h) CONSORT (Consolidated Standards of reporting Trials)
i) Yes
j) 10.67% , Yes

OSCE 3
Growth chart (5 marks)
7 year old girl with height 95 cm, weight 25 kg and bone age 3 years.
a) Plot height (0.5)
b) Plot weight (0.5)
c) Calculate BMI – 27.7 (0.5)
d) Plot BMI (0.5)
e) Interpretation of BMI - obesity (0.5)
f) Height age – 3 y (0.5)
g) Weight age – 8y (0.5)
h) Arrange HA, WA, BA, CA in ascending order – WA > CA > HA =
BA (0.5)
i) Choose the diagnosis: nutritionalobesity , hypothyroidism, PEM –
hypothyroidism (1)

OSCE 4
A)
1.a) Increased volume & translucency left (0.25x3= 0.75)
b) Bronchovascular markings present on left
c) Mediastinal shift to the right side
2.Obstructive Emphysema (left side) (1)
B)
1.a)Increased volume & Translucency left (0.25 x 3=0.75)
b) Absence of bronchovascular markings left
c) Collapse (Compression) of left lung & Mediastinal shift to right side
2.Pneumothorax with collapse ( left side ) (1)
C)
1) Increased densities of (0.25 x 2 =0.5)
- anterior end of all the ribs ,
- upper end of humerus and- scapular border
2) Heavy metal poisoning (1)

OSCE 5VaccinesA)Immune Deficiency
Contraindicated
Vaccines
Risk specific recommended vaccines
B lymphocyte
(Bruton's)
OPV, BCG,YF (0.25) Pneumococcal
measles and Varicella vaccine(0.25)
T lymphocyteand combined( SCID)
BCG,OPV,MMR,MMRV,OPV, YF, ZOSTER, ROTAVIRUS (0.25)
Pneumococcal (0.25)
Complement None (0.25 ) Pneumococcal (0.25)
Meningococcal
Phagocyte function
BCG (0.25) Pneumococcal (0.25)
HIV symptomatic
OPV,BCG, MMR, VARICELLA ( 0.25)
Pneumococcal (0.25)
Hib
meningococcal

B) (0.125 x 2=0.25)
1. SENSITIVE TO HEAT: OPV, MEASLES,MR, MMR, BCG,
YELLOW FEVER ROTAVIRUS, VARICELLA, MMRV
SENSITIVE TO FREEZING: DTwP, DTaP, DT, TT, Td, HEPB,HEPA,HPV, PCV7, IPV, PPV 23,INACTIVATEDINFLUENZA VACCINE,MENINGOCOCCAL,ROTAVIRUS, TYPHOID, HIB ,VARICELLA
(0.125 x 2=0.25)
SENSITIVE TO LIGHT: BCG, MEASLES,MMR, VARICELLA,ROTAVIRUS, HPV, DTaP (0.125 x 2=0.25)
2. Varicella= 30 minutes; MMR= 4to 6 hours; BCG= 6 hours (0.75)
3.Measles, BCG,MMR ,MMRV,MR (0.75)
4.Door= none; Baffle tray= none (0.25)
OSCE 7
A)
1. A : Coronal view (0.5 x 2 = 1)B: Parasagittal View
2. IVH with ventriculomegaly (0.5)
3. Grade I : Germinal Matrix bleed (0.25 x 3= 0.75)Grade II : Germinal Matrix bleed without ventricular dilatationGrade III : Intraventricular bleed with ventricular dilatation
4. Antenatal steroids (0.25)
B)
1.RDS (0.75)
2. Surfactant Deficiency (0.5)
3. Group B Streptococcus pneumonia, pulmonary hemorrhage,
pulmonary edema (0.25 x 3 = 0.75)
4. Obstructed TAPVC (0.5)

OSCE 8A) Match the following (0.25 x 8 =2 )
Toxicity Symptoms1. Kerosene2. Chloroquine3. Camphor4. Methylsalicylate5. Tricyclic antidepressants6. Clonidine7. Caustics8. CCBs
Answer• 1.b,2.c,3.a,4. E,5.d,6.g,7.h,8.f
B)1. ABC, supplemental oxygen, vascular access, plan intubation,
send electrolytes, blood glucose, calcium , Mg, toxicologyscreening, urgent ECG. (0.75)
2. Cardiac arrhythmias, prolongation of QT interval, R wave inaVR > 3 mv, preterminal sinus bradycardia, wide complex VTand VF (0.5)
3. Coma, convulsions, cardiac arrhythmias, acidosis (0.5)
(0.25 x 5 = 1.25)4. Management Principle
Activated charcoal To prevent absorption
IV soda bicarbonate To maintain pH above 7.45To prevent dysrhythmias
Normal saline To prevent hypotension
lidocaine To prevent ventriculararrhythmias
Avoid phenytoin As it is arrhythmogenic
A. seizuresB. acute lung injuryC. arrhythmiasD. hypotensionE. metabolic acidosisF. hyperglycemiaG. bradycardiaH. airway burns

OSCE 9
A1. Christmas tree appearance / neurogenic bladder (0.5)
A2. Extreme spectrum of voiding dysfunction – a form of non neurogenic
neurogenic bladder (0.5)
A3. Clean Intermittent Catheterization (CIC) (0.5)
A4. Usually no need for chemoprophylaxis (0.5)
A5. Oxybutinin hydrochloride, vasopressin and imipramine (0.5)
B)1. How will you diagnose acute pyelonephritis by this imaging? (0.5)
Photopenic areas in DMSA supports the diagnosis
2. Define complicated UTI? (0.5)
Presence of fever >39ºC, systemic toxicity, persistent vomiting,
dehydration, renal angle tenderness and raised serum creatinine
3. What are the imaging modalities one should do in an infant with
first UTI? (0.5)
USG abdomen, DMSA and MCU as per ISPN guidelines for first febrile
UTI in less than 1 year old
4. Name four risk factors for UTI? (0.5)
Female gender, Uncircumcised male, Voiding dysfunction, VURPinworm infestation, Obstructive uropathy & Urethral
instrumentation
5. Give your comment on uroprophylaxis for this child? (0.5)
Cephalexin 10 mg/kg day as single night dose till VUR is ruled out
by imaging

OSCE 10
A)1.Cystic Hygroma (0.25)2.Abnormality Of Jugular Lymph Sac Development (0.25)3.Stabilisation (1)
Oral airwayNeck ExtensionAvoid mechanical compression of the lesion ( lateralise the child tothe side of lesion )Requires immediate decompressionMRI – look for intraoral / Mediastinal extension
4.Intralesional Sclerosant Injection / Surgery (0.5)Micro- sx / macrocystic variety - sclerosant
5.Bleomycin (0.5)DoxycyclineEthanol (pure)Picibanil (OK-432)Sodium tetradecyl sulfateOK 432 Or Picibanil – Derived From Low Virulent Strain OfStreptococcus Pyogenes.
B)
1.Intussussception (0.5)
2.Intermittent Colicky Pain Abdomen(incessant Cry ), Vomiting ,Bleeding Per Rectum. (0.5)
3.Doughnut or Target Sign / (0.5)Pseudokidney Sign .
4.Meckel/Polyp/Duplication Cyst/ Lymphoma/ HSP (0.5)
5.Pneumatic Reduction / Hydrostatic Reduction (0.5)Laproscopic / Open Manual Reduction .

OSCE 11A)
1.FVC (0.25 x 4 = 1)FEV1FEV1/FVCFEF25-75
B)1.Forced Expired Volume in One second (FEV1) (1)The amount of air that can be blown in the first secondin the FVC maneuver
2.FEF 25-75(Maximal mid expiratory flow rate) (0.75 x 2 = 1.5)Forced expiratory flow rate between 25 to 75% of FVCRepresent early evidence for obstructionNormal range is 75-125%
C)Post bronchodilator test - ↑ in FVC, FEV1, FEV1/FVC , FEF25-75 & PEF (1)Diagnosis- Asthma (0.5)

OSCE 12A) (0.5 x4 = 2)
1. Hyperbilrubinemia, Azotemia, Shock,Thrombocytopenia,Extremeprematurity,RDS
2. Na+ - 510 meq/LCl- - 510 meq/LK+ - 0
3. K+ - 5meq/L
4. 12 %
B) (0.75 X 4=3)1.N-NUTRITIONI-IMMUNISATIONM-MEDICAL CARE &MENTAL HEALTHF-FAMILY PLANNINGE-EDUCATIONS-STIMULATION & SOCIAL SUPPORT
2.”Two hit” hypothesis
3.ORSH- Obesity related stentohepatitisUPSH- Undernutrition related stentohepatitis
4.Vitamin E (600-800 IV/DAY)Vitamin C (500 mg/day)

OSCE 14
A)ABG: Metabolic and respiratory acidosis,Hyperoxia (1.5)
B)1.High anion gap ,Metabolic acidosis ,compensated and hypokalemia;(2)
2. DKA (1.5)

OSCE 15Capnography
A)1. Capnography (trend) tracing during CPR(0.5)
2. Return Of Spontaneous Circulation (0.5)
3. Abrupt increase in PETCO2 from 25 to 40mms (0.5)
4. Substantial improvement in blood flow indicative of ROSC(0.5)
B) (1.5)1.Uneven emptying of alveolar gas alters emptying on exhalation
Produces changes in ascending phase (II) with loss of the sharp
upslope Alters alveolar plateau (III) producing a “shark fin”
2.Bronchospasm(0.5)
C)1.Verification of ETT placement – Esophageal intubation (0.5)
2.Exhaled air present in the stomach (0.5)

OSCE 16A)
(3 x 0.5 =1.5)
1.Varying RR, constant PR INTERVAL,P wave shape and sizenormal
2.Sinus arrhythmia(1)
B)
1.Characteristic findings? 1. Short PR 2. Delta wave (Initial slurring
of QRS) 3. Wide QRS ( 2 x 0.5 =1.0)
2.Diagnosis? WPW (Wolff-Parkinson White) syndrome (0.5)
3.Drug contraindicated : Digoxin . (0.5)
Risk or complication : SVT. (0.5)

OSCE 17
A. 1) Goldenhar syndrome (0.5)
2) hypoplasia of malar, maxilla and mandible (0.25X4=1)
hypoplasia of facial musculature
microtia, malformed ears, preauricular tags/pits, deafness
diminished to absent parotid secretion
notch in upper eyelid, epibulbar dermoid micropthalmia
cleft lip and plalate
fused/ectopic kidney
VSD, PDA
B.1) Treacher Collins syndrome (0.5)
2) malformed ears, external ear canal defects (0.25X4=1)
Conductive deafness
Malar hypoplasia with or without zygomatic cleft
Mandibular hypoplasia
Antimongoloid slant of eyes
Lower lid coloboma
Visual loss
Cleft plalate
Projection of scalp hair into lateral cheek
Fusion of radius and ulna

C.
1) Noonan syndrome (0.5)
(0.25X4=1)2) Short stature, webbed neck, pectus carinatum /excavatum, wide
carrying angle, vertebral anomalies, clinodactyly Hypertelorism, down
slanting eyes, epicnathus, ptosis, sensorineural deafness,Peripheral
pulmonary stenosis, HOCM, ASD,Hypergonadotrophic hypogonadism,
cryptorchidism, delayed puberty,Clotting factor 11 & 12 defects, prone to
ALL, CML
3) PTPN11 mutation, chromosome 12q24.1 (0.5)

OSCE 18
( Total- 5 marks )
A. Right ear conductive deafness ( 1 )
B. Left ear sensorineural deafness ( 1 )
C. Right ear normal hearing ( 1 )
D. Right ear mixed hearing loss ( 2 )

OSCE 20A.
1) Pneumocystis jiroveci (1)
2) Infantile interstitial plasma cell pneumonitis & diffuse desquamative
alveolar pneumonitis (1)
3) Trimethoprim - sulphamethaxazole- 3 weeks treatment for AIDS
patients and 2 weeks treatment for others (1)
B.
1) Leishman Donovan bodies in bone marrow smear (1)
2) Female Phlebotomous argentipes (0.5)
3) Sodium stibogluconate (0.5)

OSCE 21
( 1x5=5)
1.Beta thalassemia trait
2.Sickle cell anemia
3.Hb SC disease
4.Beta thalassemia major
5.Alpha thalassemia HbH –Barts disease

OSCE 22
A)
1) Pityriasis rosea (1)2) Herald patch with erythematous discrete lesions on the trunk
(0.5)3) Unknown cause, suspected human herpes virus 6,7,8
(0.5)4)Usually self limiting, severe pruritus needs lubricants/oral
antihistamines (0.5)
B)
1) Erythema multiforme (1)
2) Doughnut shaped, target lesions/ iris or bulls eye lesions, papules
with erythematous outer border, inner pale ring and necrotic center
(0.5)
3) HSV and mycoplasma (0.5)
4) Supportive treatment- emollients, systemic antihistamines (0.5)

OSCE 23(0.5x10=5)
REFLEX APPERANCE DISAPPEARANCE
a. Sucking 32-34 weeks 6 months
b. Rooting 24-28 weeks 6 months
c. Stepping 28 weeks 6 weeks
d. Placing Birth 1.5 months
e. Palmar grasp Birth 4 -7 months
f. Plantar grasp Birth 9-12 months
g. Moro 28 weeks 4 months
h. ATNR Birth 5-6 months
i. Landau 3 months 12 months
j. Parachute 8-12 months Persists life long

OSCE 24
A.
1) Pavlik harness splint ( 1 )
2) Developmental dysplasia of the hip (0.5)
3) Barlows test and Ortalanis test (0.5)
4) Hip ultrasound (0.5)
B)
1) Congenital talipes equinovarus ( club foot ) (1)
2) CAVE –cavus, adductus, vaus, euinus (0.5)
3) Ponseti method- specific method of foot manipulation and serial
casting (0.5)
4) Multifactorial polygenic inheritance (0.5)

OSCE 25
1) Moderate DKA weight: 20kg (10 marks)
Three IV lines RBS, VBG, electrolytes, blood / urine ketones, HbA1C,
CBC, CRP, blood c/s(1) 7% dehydration(1) IVF NS / plasmalyte A (48 hrs maintenance + 7%
dehydration correction) = 2880ml +1400ml = 4280mlover 48 hrs (88ml/hr)(2)
Add potassium to the IV fluids after documenting theRFT and urine output (1)
IV insulin (after 1 hour of starting IV fluids) 40 unitsin 40 ml NS @ 1ml/hr(0.05u/kg/hr) (2)
Change to dextrose containing fluid if CBG <300mg/dL.
Monitor the following: (3)o CBG Q1Ho VBG & electrolytes Q4H – Q6Ho Anion gapo Measured sodium trendo Corrected serum sodium and serum osmolalityo Watch for altered sensorium/ cerebral
edema/seizures
FLUID INTAKE AND OUTPUT MONITORING

OSCE 27A)
1.Phenylketonuria, (0.25)
2.Seizures, spasticity, hyperreflexia & tremors (0.5)
B)1.Homocystinuria (0.25)
2.Increased Methionine & Homocystine in body fluids; low or absent
cystine in plasma; enzyme assay in liver biopsy, cultured fibroblasts;
DNA analysis (1)
3.High doses of Vitamin B6 with folic acid; Betaine, dietary
restriction (1)
OSCE 3
1.Hurler disease MPS 1 (0.25)
2.Obstructive airway disease, respiratory infection & cardiac
complications (0.75)
3.Skeletal dysplasia- dysostosis multiplex- thick ribs , ovoid vertebral
bodies, coarsely trabeculated diaphyses of long bones with irregular
metaphyses & epiphyses (1)

OSCE 28NRP OSCE STATION
. How will you prepare and proceed. Demonstrate and describe.(1)
PERFORMANCE STEPS1. Places baby under radiant warmer (1)2. Performs initial steps (1)3. Evaluates breathing and heart rate
BABY IS GASPING AND HEART RATE IS 80BPM1. Starts PPV with room air after selecting appropriate mask and applying
correctly.(1)2. Calls for additional help (0.5)3. After 5 breaths, evaluates heart rate (1)
HEART RATE IS 40BPM AFTER INITIAL 5 INFLATIONS1. Checks chest rise (1)2. Performs ventilation corrective steps (MRSOPA) (1)3. After corrective measures administer PPV for 30 sec (1)4. Assess breathing and heart rate
BABY IS BREATHING WELL AND HEART RATE 120BPM1. Stop PPV (1)2. Places the baby in skin to skin contact, monitor breathing, HR, color and
temperature, initiate breast feeding. (0.5)

OSCE 29
Counsel the mother whose 3year old child was
brought on day 3 of fever and has been diagnosed
to have dengue fever with no other complications
and been sent as OP.
1.Greets, gets Introduced & Establishes rapport with the parents
2.Asks what has been understood so far about the disease by the parents.(0.5)3.Explains the disease in simple words and the mode of transmission. (0.5)
4.Explains the natural course of the disease- three phases- febrile, critical andrecovery phase.(1)5.Explains the warning signs- abdominal pain, persistent vomiting, mucosalbleed, decreased urine output, clinical fluid accumulation, puffiness of eyes,mucosal bleed, lethargy, restlessness.(1)6.Explains the home management plan if no warning signs present and theimportance of input/output monitoring and adequate liquid diet(1)
7.Explains the need for hospitalisation if warning signs present andmonitoring(vitals) the condition of the child and serial bloodinvestigations(pcv,platelet,sgot,sgpt) and might need intensive caremonitoring if signs of severe dengue present.(1)8.Explains that there is no specific medication and only supportive measuresrequired (1)9.Explain about the follow up. If any warning signs present to reportimmediately in emergency department, if no warning signs once a day visitwith doctor as OPD from the day of afebrile period till day 7 of illness.(1)
10.Explains the complications (bleeding ,shock,) (1)
11.To inform parents about to avoid drugs like NSAID and aspirin. (1)
12.Advise on prevention of mosquito breeding and protection from mosquitobite to prevent recurrences. (1)
TOTAL (10 MARKS)

OSCE 30A 3 years old child with recurrent wheezing episodes has been prescribed
budesonide inhaler (100 micrograms one puff morning and once in night)
medications. Demonstrate the technique of use of Metered Dose Inhaler with
spacer and mask.
Metered Dose Inhaler with mask and spacer –demonstration technique (10 marks)STEPS 1 2 3 4 5 6 7
Reg No. of the candidate
Greets, getting introduced and establishes rapport
Attaches the mask to the mouth piece of spacer device (1)
Shakes inhaler 1-2 times before use (1)
Inserts the inhaler into spacer correctly(1)
Makes the child sit on the mother’s lap with back straight andhead straight(1)
Places the mask over child’s nose and mouth so that it fitssnugly(2)
Presses the inhaler once(actuates) (1)
Allows the child to breathe normally through the mask(4-5breaths) (1)
Disassembles the mask from the spacer and keeps both in theappropriate box(1)
Explains the technique of cleaning with water and airdrying(once in a month) (1)
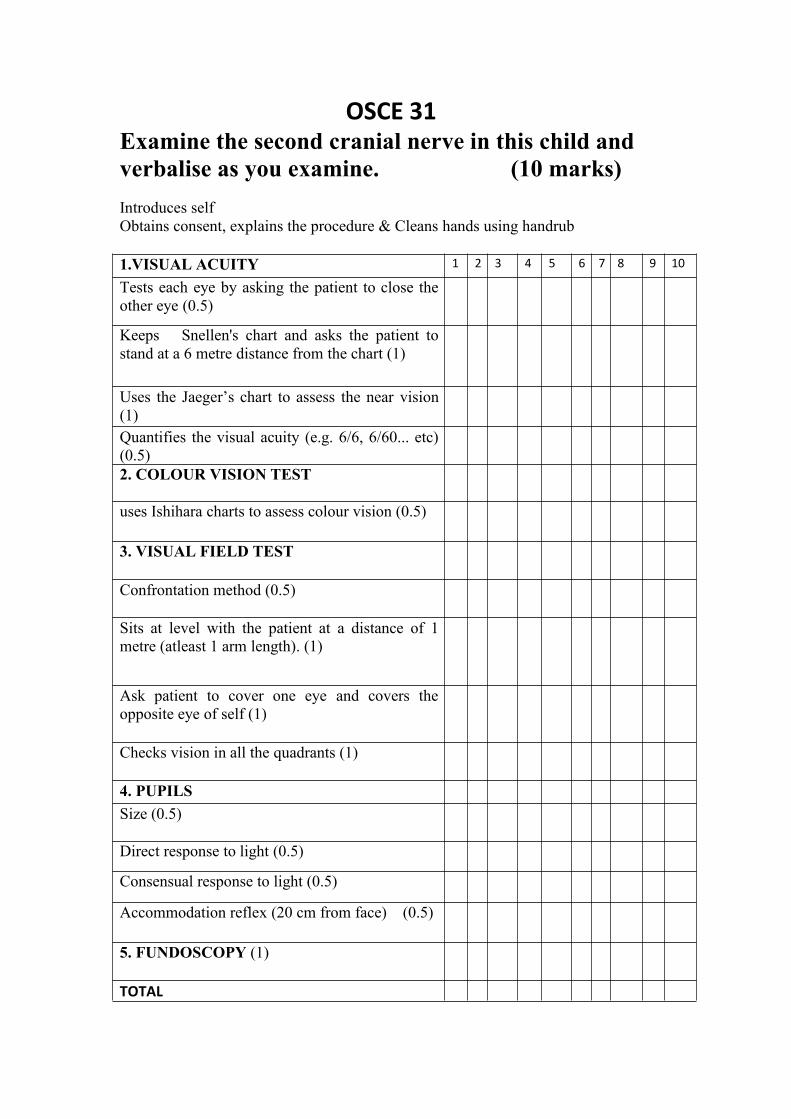
OSCE 31Examine the second cranial nerve in this child andverbalise as you examine. (10 marks)Introduces selfObtains consent, explains the procedure & Cleans hands using handrub
1.VISUAL ACUITY 1 2 3 4 5 6 7 8 9 10
Tests each eye by asking the patient to close theother eye (0.5)
Keeps Snellen's chart and asks the patient tostand at a 6 metre distance from the chart (1)
Uses the Jaeger’s chart to assess the near vision(1)Quantifies the visual acuity (e.g. 6/6, 6/60... etc)(0.5)2. COLOUR VISION TEST
uses Ishihara charts to assess colour vision (0.5)
3. VISUAL FIELD TEST
Confrontation method (0.5)
Sits at level with the patient at a distance of 1metre (atleast 1 arm length). (1)
Ask patient to cover one eye and covers theopposite eye of self (1)
Checks vision in all the quadrants (1)
4. PUPILSSize (0.5)
Direct response to light (0.5)
Consensual response to light (0.5)
Accommodation reflex (20 cm from face) (0.5)
5. FUNDOSCOPY (1)
TOTAL

















