Orthotopic mouse liver transplantation to study liver ... Mouse Liver.pdforthotopic liver...
12
© 2016 Macmillan Publihers Limited. All rights reserved. PROTOCOL NATURE PROTOCOLS | VOL.11 NO.7 | 2016 | 1163 INTRODUCTION Development and applications of the protocol Organ transplantation is the established treatment for patients with end-stage organ disease. The importance of animal models in transplantation is widely recognized among researchers in the field to improve the understanding of transplant pathology and to identify novel therapeutic strategies 1 . Orthotopic liver transplantation in the mouse was first described by Qian et al. 2 at the University of Pittsburgh in 1991. This technique was developed by applying the cuff technique principle previ- ously used in orthotopic liver transplantation in the rat, which simplified venous vascular anastomosis as compared with hand- suture technique 3 . Since then, our laboratory and others have used the model to elucidate mechanisms of liver lymphocyte homeostasis 4 , transplant ischemia–reperfusion injury 5–10 , liver allograft tolerance 11–17 , liver regeneration 18–20 , and other liver immunopathologies 21,22 . The liver is a life-sustaining organ, and orthotopic liver trans- plantation in the mouse provides a more clinically relevant model than heterotopic heart transplantation or single-lung transplan- tation, which are not life sustaining 1 . Moreover, with respect to human/clinical relevance, the liver is a unique/tolerogenic immune organ with hematopoietic and immune regulatory properties that can promote operational tolerance in a signifi- cant proportion of stable human liver allograft recipients 23–25 . Although the precise mechanisms of liver transplant tolerance are yet to be elucidated, a better understanding of the unique features of the liver as a tolerogenic organ has significant implica- tions for an improved understanding of regulation of inflamma- tory and immune-mediated liver and other organ diseases and their therapy. Thus, the mouse liver transplant model remains an exceptionally useful and powerful tool with which to elucidate the cellular and molecular mechanisms involved in inflammatory liver disease and its resolution. This procedure is of interest not only to microvascular surgeons, gastroenterologists, hepatologists, and investigators in the transplantation community, but also to those interested in applying the model to study the regulation of liver immu- nopathology and liver biology in general. Because in adult mice the liver is a hematopoietic organ, the liver transplant model is also of considerable potential interest to investigators studying hematopoiesis. Overview of the protocol: advantages and limitations The surgical procedure is divided into three main stages: (i) donor surgery, (ii) back-table preparation of the liver graft, and (iii) the recipient operation 2,26 . The final stage of the recipient operation is the most difficult, as it requires efficient removal of the recipient’s liver and implantation of the donor liver within 20–30 min to minimize the duration of portal vein (PV) clamping 2 . The liver graft is placed ‘orthotopically’, thus occupying the normal anatomical site in a manner similar to that seen in clinical trans- plantation in humans 27 , as opposed to ‘heterotopic’ transplanta- tion, in which the organ is placed in an alternative site. Thus, the orthotopic transplantation model is more clinically relevant than heterotopic transplantation, which is purely an experimen- tal model. However, prolonged PV clamping in the orthotopic liver transplantation model may lead to death of the recipient. Thus, this model is considered surgically demanding compared with other organ transplant models in mice such as heterotopic heart transplantation and orthotopic kidney transplantation 1,26 . We speculate that technical difficulty is the main reason that this model has been used by only a few research groups in the world. Here we describe techniques and materials in meticulous step- wise detail, including several modifications that have not been described in the literature previously—e.g., surgical instruments, preparation of vascular cuffs and bile duct stents, anesthetic technique during donor and recipient operations, preparation before the anhepatic phase, and the suprahepatic inferior vena cava (SHIVC) suture during the anhepatic phase. We hope that this will allow researchers who are not currently proficient with Orthotopic mouse liver transplantation to study liver biology and allograft tolerance Shinichiro Yokota 1,2,5 , Shinya Ueki 1,5 , Yoshihiro Ono 1 , Naoya Kasahara 2 , Angélica Pérez-Gutiérrez 1 , Shoko Kimura 1 , Osamu Yoshida 1 , Noriko Murase 1 , Yoshikazu Yasuda 2 , David A Geller 1,3 & Angus W Thomson 1,4 1 Thomas E. Starzl Transplantation Institute, Department of Surgery, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA. 2 Department of Surgery, Jichi Medical University, Shimotsuke, Tochigi, Japan. 3 Liver Cancer Center, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA. 4 Department of Immunology, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA. 5 These authors contributed equally to this work. Correspondence should be addressed to A.W.T. ([email protected]). Published online 2 June 2016; doi:10.1038/nprot.2016.073 Orthotopic liver transplantation in the mouse is a powerful research tool that has led to important mechanistic insights into the regulation of hepatic injury, liver immunopathology, and transplant tolerance. However, it is a technically demanding surgical procedure. Setup of the orthotopic liver transplantation model comprises three main stages: surgery on the donor mouse; back-table preparation of the liver graft; and transplant of the liver into the recipient mouse. In this protocol, we describe our procedure in stepwise detail to allow efficient completion of both the donor and recipient operations. The protocol can result in consistently high technical success rates when performed by personnel experienced in the protocol. The technique can be completed in ~2–3 h when performed by an individual who is well practiced in performing mouse transplantation in accordance with this protocol. We have achieved a perioperative survival rate close to 100%.
Transcript of Orthotopic mouse liver transplantation to study liver ... Mouse Liver.pdforthotopic liver...

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
nature protocols | VOL.11 NO.7 | 2016 | 1163
IntroDuctIonDevelopment and applications of the protocolOrgan transplantation is the established treatment for patients with end-stage organ disease. The importance of animal models in transplantation is widely recognized among researchers in the field to improve the understanding of transplant pathology and to identify novel therapeutic strategies1. Orthotopic liver transplantation in the mouse was first described by Qian et al.2 at the University of Pittsburgh in 1991. This technique was developed by applying the cuff technique principle previ-ously used in orthotopic liver transplantation in the rat, which simplified venous vascular anastomosis as compared with hand-suture technique3. Since then, our laboratory and others have used the model to elucidate mechanisms of liver lymphocyte homeostasis4, transplant ischemia–reperfusion injury5–10, liver allograft tolerance11–17, liver regeneration18–20, and other liver immunopathologies21,22.
The liver is a life-sustaining organ, and orthotopic liver trans-plantation in the mouse provides a more clinically relevant model than heterotopic heart transplantation or single-lung transplan-tation, which are not life sustaining1. Moreover, with respect to human/clinical relevance, the liver is a unique/tolerogenic immune organ with hematopoietic and immune regulatory properties that can promote operational tolerance in a signifi-cant proportion of stable human liver allograft recipients23–25. Although the precise mechanisms of liver transplant tolerance are yet to be elucidated, a better understanding of the unique features of the liver as a tolerogenic organ has significant implica-tions for an improved understanding of regulation of inflamma-tory and immune-mediated liver and other organ diseases and their therapy. Thus, the mouse liver transplant model remains an exceptionally useful and powerful tool with which to elucidate the cellular and molecular mechanisms involved in inflammatory liver disease and its resolution.
This procedure is of interest not only to microvascular surgeons, gastroenterologists, hepatologists, and investigators
in the transplantation community, but also to those interested in applying the model to study the regulation of liver immu-nopathology and liver biology in general. Because in adult mice the liver is a hematopoietic organ, the liver transplant model is also of considerable potential interest to investigators studying hematopoiesis.
Overview of the protocol: advantages and limitationsThe surgical procedure is divided into three main stages: (i) donor surgery, (ii) back-table preparation of the liver graft, and (iii) the recipient operation2,26. The final stage of the recipient operation is the most difficult, as it requires efficient removal of the recipient’s liver and implantation of the donor liver within 20–30 min to minimize the duration of portal vein (PV) clamping2. The liver graft is placed ‘orthotopically’, thus occupying the normal anatomical site in a manner similar to that seen in clinical trans-plantation in humans27, as opposed to ‘heterotopic’ transplanta-tion, in which the organ is placed in an alternative site. Thus, the orthotopic transplantation model is more clinically relevant than heterotopic transplantation, which is purely an experimen-tal model. However, prolonged PV clamping in the orthotopic liver transplantation model may lead to death of the recipient. Thus, this model is considered surgically demanding compared with other organ transplant models in mice such as heterotopic heart transplantation and orthotopic kidney transplantation1,26. We speculate that technical difficulty is the main reason that this model has been used by only a few research groups in the world. Here we describe techniques and materials in meticulous step-wise detail, including several modifications that have not been described in the literature previously—e.g., surgical instruments, preparation of vascular cuffs and bile duct stents, anesthetic technique during donor and recipient operations, preparation before the anhepatic phase, and the suprahepatic inferior vena cava (SHIVC) suture during the anhepatic phase. We hope that this will allow researchers who are not currently proficient with
Orthotopic mouse liver transplantation to study liver biology and allograft toleranceShinichiro Yokota1,2,5, Shinya Ueki1,5, Yoshihiro Ono1, Naoya Kasahara2, Angélica Pérez-Gutiérrez1, Shoko Kimura1, Osamu Yoshida1, Noriko Murase1, Yoshikazu Yasuda2, David A Geller1,3 & Angus W Thomson1,4
1Thomas E. Starzl Transplantation Institute, Department of Surgery, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA. 2Department of Surgery, Jichi Medical University, Shimotsuke, Tochigi, Japan. 3Liver Cancer Center, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA. 4Department of Immunology, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA. 5These authors contributed equally to this work. Correspondence should be addressed to A.W.T. ([email protected]).
Published online 2 June 2016; doi:10.1038/nprot.2016.073
orthotopic liver transplantation in the mouse is a powerful research tool that has led to important mechanistic insights into the regulation of hepatic injury, liver immunopathology, and transplant tolerance. However, it is a technically demanding surgical procedure. setup of the orthotopic liver transplantation model comprises three main stages: surgery on the donor mouse; back-table preparation of the liver graft; and transplant of the liver into the recipient mouse. In this protocol, we describe our procedure in stepwise detail to allow efficient completion of both the donor and recipient operations. the protocol can result in consistently high technical success rates when performed by personnel experienced in the protocol. the technique can be completed in ~2–3 h when performed by an individual who is well practiced in performing mouse transplantation in accordance with this protocol. We have achieved a perioperative survival rate close to 100%.

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
1164 | VOL.11 NO.7 | 2016 | nature protocols
the protocol to implement the procedure successfully. We have also provided step-by-step videos (Supplementary Videos 1–8) that depict the important stages of the donor surgery, cuffing, and recipient surgery. Our objective is to enable research groups to implement the mouse liver transplantation procedure with high technical success and a high perioperative survival rate.
Although technically demanding, the mouse model provides unique advantages over other, larger animal liver transplant models, such as the rat and pig models, because the mouse genome is well characterized and there is much greater diversity and availability of both genetically modified animals (knockout or transgenic) and research reagents at a relatively low cost2,26.
Alternative methodsAlthough some institutions have developed an arterialized liver graft, this adds a further level of difficulty to the procedure described in this protocol. In addition, the benefit of arterializa-tion in mouse liver transplantation remains controversial5,26,28. One study from the University of Oxford28 found that graft arte-rialization did not have a major impact on liver injury, cytokine mRNA expression, or graft survival compared with nonarterial-ized liver transplantation in a syngeneic donor–recipient combina-tion (CBA/Ca → CBA/Ca). However, studies from the University Hospital of Zurich26 and UCLA5 showed that re-arterialization of the graft significantly (P < 0.05) reduced liver injury and prolonged survival with or without prolonged (24 h) cold preservation in a syngeneic combination (BALB/c → BALB/c). The difference in the conclusions drawn regarding the impact of graft arterialization may reflect differences in the mouse strains used or technical
differences between these groups. The impact of graft arterializa-tion in allogeneic liver transplantation has not been examined.
Partial liver transplantation, or reduced-size liver transplanta-tion, has also been developed in mice18,19. This model represents clinical living-donor liver transplantation, which uses a reduced-size, partial liver graft, rather than a whole liver graft. However, reduced-size liver transplantation is essentially the same opera-tion as the intact liver transplantation procedure, except that it requires hepatectomy, which can be achieved relatively easily by ligating certain lobes (the left lateral, the caudate, and/or the median lobe) with silk sutures18,19. Thus, we describe our proto-col for nonarterialized, orthotopic mouse liver transplantation. This protocol can be applied to establish both arterialized and partial liver transplantation in mice.
Experimental designMouse weight. Ideally, donor mice should weigh between 25 and 30 g, because bile duct stent insertion is difficult for mice weigh-ing less than 25 g. In addition, the PV and infrahepatic inferior vena cava (IHIVC) may be too short for anastomosis. However, mice weighing more than 35 g should be avoided, as recipients with large amounts of intra-abdominal fat make the operation more difficult.
Choosing appropriate mouse donor and recipient strains. In contrast to allogeneic heart or skin transplantation, alloge-neic liver transplantation in the mouse usually does not result in rejection in most strain combinations11,13,29. In most published work, the male C57BL/6 (H-2b) to C3H (H-2k) combination has been used.
MaterIalsREAGENTS crItIcal The reagents and microsurgical equipment listed represent the authors’ preference. Similar setups and equipment can be used as alternatives and are likely to be equally effective. crItIcal All of the reagents listed can be used and stored according to the manufacturers’ instructions.
Appropriate pairs of mice. For example, male C57BL/6 (H-2b; donor) and C3H (H-2k; recipient) mice, 8–12 weeks of age (preferred body weight for donors is 25–30 g, and preferred body weight for recipients is 30–35 g) (The Jackson Laboratory) ! cautIon All experiments involving animals must be performed in accordance with national and institutional regula-tions. This protocol has been approved by the University of Pittsburgh and Jichi Medical University institutional animal care and use committees and in accordance with criteria outlined in the Guide for the Care and Use of Laboratory Animals, a publication of the US National Institutes of Health (Supplementary Videos 1–8 were recorded at Jichi Medical University).Isoflurane, United States Pharmacopeia (USP) liquid for inhalation, 250 ml (Piramal Healthcare, cat. no. NDC 66794-017-25)Heparin sodium injection, USP (1,000 USP units per ml; Fresenius Kabi, cat. no. 504031)0.9% (wt/vol) sodium chloride injection (saline), USP (Baxter Healthcare Corporation, cat. no. 2B1324X)Viaspan (Belzer University of Wisconsin solution) 1L (Teva Pharmaceuti-cals, cat. no. 004606)Buprenex injectable (buprenorphine hydrochloride; Reckitt Benckiser Pharmaceuticals, cat. no. NDC 12496-0757-1)Cefazolin for injection, USP (APP Pharmaceuticals, cat. no. NDC 63323-238-61)PVP scrub solution (povidone–iodine 7.5%; Medline, cat. no. NDC 12496-0757-1)70% Ethanol (Decon Labs, cat. no. 2716)
•
•
•
•
•
•
•
•
•
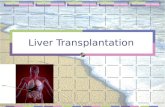
EQUIPMENTJELCO IV catheter, 16-gauge × 1–1/4 (Smiths Medical, cat. no. 4042; Fig. 1a)IV catheter, 20-gauge × 1–1/4 (Excel International, cat. no. 26742; Fig. 1a)Becton, Dickinson and Company (BD) Intramedic polyethylene tubing (PE10; BD, cat. no. 427400; Fig. 1a)Heavy-duty razor blade (Titan, cat. no. 11039)Microscope-Leica Wild M650, 6–40× magnification (Leica Microsystems)Tec 3 isoflurane funnel fill vaporizer (General Anesthetic Services)Vetroson V-10 bi-polar electrosurgical unit (Summit Hill Laboratories)Cautery, high-temperature fine tip (Bovie Medical Corporation, cat. no. AA01)Mosquito classic delicate hemostatic forceps (Codman, cat. no. 30-4472; Fig. 1b)Micro-retractor (Murdock; Roboz Surgical Instrument, cat. no. RS-6550; Fig. 1b)Nonwoven gauze sponges (Fisherband, cat. no. 870-PC-DBL; Fig. 1b)Sterile cotton swab, double cone hard sharp point tip (Puritan Medical Products Company, cat. no. 870-PC-DBL)Microneedle holder (Aesculap Surgical Instruments, cat. no. FD231R; Fig. 1c)McPherson tying forceps (Accurate Surgical & Scientific Instruments Corporation, cat. no. ASSI-4388; Fig. 1c)Weldon miniature bulldog clamps, curved jaws (V. Mueller, cat. no. CH6077-002; Fig. 1c)Johns Hopkins bulldog clamps (V. Mueller, cat. no. CH5151-1; Fig. 1c)Vannas capsulotomy scissors (Accurate Surgical & Scientific Instruments Corporation, cat. no. ASSI-21288; Fig. 1c)Gill Iris forceps (V. Mueller, cat. no. OP3424; Fig. 1c)Hoskin Mk II micro forceps with long curved jaws, 6-mm tying platform (Accurate Surgical & Scientific Instruments Corporation, cat. no. ASSI-2177; Fig. 1c)
•
••
•••••
•
•
••
••
•
••
••

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
nature protocols | VOL.11 NO.7 | 2016 | 1165
IHIVC cuff
PV cuff
BD stent
Needle holder
McPherson forceps
Weldon miniture bulldog clamp
Johns Hopkins bulldog clamp
Vannas capsulotomy scissors
Gill iris forceps
Hoskin Mk II micro forceps with curved jaws
a b c
Stevens tenotomy scissors (Accurate Surgical & Scientific Instruments Corporation, cat. no. ASSI-9193)Durmont #5 forceps (Fine Science Tools, cat. no. 11251-20)Adson forceps (V. Mueller, cat. no. NL1400)Jewelers forceps (Codman, cat. no. 30-6712)Tube occluding forceps (Roboz Surgical Instrument, cat. no. 65-7480)Vannas spring scissors, 3-mm cutting edge (Fine Science Tools, cat. no. 15000-00)Micro serrefine-straight/15 mm (Fine Science Tools, cat. no. 18055-03)Micro serrefine clamp applicator with lock (Fine Science Tools, cat. no. 18056-14)2-0 Silk (Ethicon, cat. no. SA-85)5-0 Silk (Braintree Scientific, cat. no. SUT-S106)7-0 Silk (Braintree Scientific, cat. no. SUT-S103)Micro AROSuture, sterile 10-0 nylon suture, 70 µm, TAP points (AROSurgical Instruments Corporation, cat. no. T4A10N07)4-0 Vicryl (Ethicon, cat. no. J662H)5-ml Syringe (BD, cat. no. 309646)BD 1-ml insulin syringe U-100 slip tip (BD, cat. no. 329654)BD 0.5-ml U-100 insulin syringe, 28-gauge × 1/2 (BD, cat. no. 329461)IV catheter 22-gauge × 1–1/4 inches (Excel International, cat. no. 26746)BD PrecisionGlide needle, 27-gauge × 1/2 (BD, cat. no. 305109)BD PrecisionGlide needle, 30-gauge × 1/2 (BD, cat. no. 305106)
•
•••••
••
••••
•••••••
Blunt-tip L-shaped injector (custom-made) crItIcal All microsurgical equipment listed above should be sterilized by autoclaving (>120 °C) before use.Insulated foam container without lid (for back-table preparation of the liver graft), dimensions (length × width × height): inside, 18 × 15 × 4 cm; outside, 21 × 18 × 5.5 cm; wall thickness, 1.5 cm (Marko Foam Products, cat. no. IC-103)Falcon tissue culture dish, 60 × 15 mm (Corning, cat. no. 353002)
EQUIPMENT SETUPInjector setup To make a blunt-tip L-shaped injector, take the sharp tip off a 30-gauge needle by holding the tip with mosquito forceps and bending it back and forth. Once the sharp tip comes off, blunt and smooth the end of the injector using a tool such as a flat metal file.
••
•
•
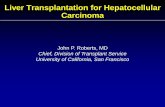
Figure 1 | Instruments used in the mouse liver transplantation model and diagram of mouse position during surgery. (a) Cuffs for IHIVC and PV, and bile duct (BD) stent. (b) Schematic drawing of mouse position and setting for donor and recipient operations. Use mosquito forceps to hold the xiphoid process and retract toward the head of the mouse. Wrap the small and large intestines using a wet, nonwoven gauze sponge and gently retract the left and middle lobes of the liver toward the xiphoid process. (c) Instruments used throughout the protocol. Scale bars, 1 mm (a) and 1 cm (c).
proceDurepreparation of pV and inferior vena cava cuffs ● tIMInG 5–10 min1| Prepare the cuff for the PV from a 20-gauge angiocatheter using a razor blade. Although an 18-gauge angiocatheter can be used as an alternative, we prefer a 20-gauge angiocatheter because of the ease of inserting the 20-gauge cuff into the PV. The metal needle of the angiocatheter should be used as a cutting surface. The main body of the cuff should be 2 mm in length. The extension handle can be 1 mm or longer, depending on the preference of the operator (Fig. 1a).
2| Make two shallow grooves on the main body of the cuff using a razor blade. One of these grooves will help secure the attachment of the cuff to the donor PV with silk suture ligation during the back-table preparation. The second groove will be helpful with the anastomosis of the PV during the recipient operation.
3| Repeat Steps 1 and 2 using a 16-gauge angiocathether to prepare the cuff for IHIVC.
preparation of bile duct stent ● tIMInG 5 min4| Prepare the bile duct stent. Use a razor blade to cut the polyethylene tubing (PE10) into a trapezoid shape 2 mm in length (Fig. 1a). Use a hard, blunt object (e.g., a ruler) to repeatedly push down the length of the tube to narrow its width to 0.3–0.5 mm. crItIcal step Be careful not to push down too hard, as this will cause narrowing of the lumen of the bile duct stent. Narrowing or occlusion of the stent could cause obstruction of the bile duct and negatively influence graft recipients’ survival.
Donor surgery ● tIMInG 40–50 min5| Anesthesia and laparotomy. Anesthetize the donor mouse by putting the animal in an induction chamber. Use the appropriate amount (~1–2 ml per 25–30 g of animal body weight) of isoflurane to anesthetize the animal. Observe the respiration rate of the animal carefully. When a respiration rate of one breath per second is achieved, the mouse is ready to be placed on the surgical table.

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
1166 | VOL.11 NO.7 | 2016 | nature protocols
6| Place the anesthetized mouse under the surgical microscope. Maintain the mouse under general anesthesia using isoflurane inhalation. Adjust the vaporizer and use 3–4% for induction with continuous air or oxygen flow of 0.5–1 L/min. Prep the abdominal wall with povidone–iodine first and then with 70% ethanol.
7| Make a midline abdominal incision from the xiphoid process to the pubis. Next, make a transverse incision and use the bi-polar electrosurgical unit to stop bleeding from the abdominal wall. After making the incisions, decrease isoflurane to 0.5–1% for maintenance of anesthesia. Alternative concentrations of isoflurane may be used. crItIcal step It is critical to observe the respiration of the mouse during the operation to assess the depth of anesthesia. Adjust the isoflurane vaporizer to maintain a respiration rate of approximately one breath per second.
8| Use mosquito forceps to hold the xiphoid process and retract toward the head of the mouse. Fix the mosquito forceps in place using soft clay (Fig. 1b). crItIcal step See supplementary Video 1 for additional guidance on preparation before liver graft harvest (Steps 8–19).
9| Wrap the small and large intestines using a wet nonwoven gauze sponge (6 × 6 cm) and place them on the left side of the abdominal cavity.
10| Use a small (3.5 × 3.5 cm), wet nonwoven gauze sponge to gently retract the left and middle lobes of the liver toward the xiphoid process to expose the caudate lobe (Fig. 1b).
11| Cut the ligament around the caudate lobe.
12| Expose the proper hepatic artery (PHA). Dissect the PHA using McPherson forceps (Fig. 1c) and ligate it with 10-0 nylon (Fig. 2a).
13| Dissect the extrahepatic bile duct using McPherson forceps and put 7-0 silk under the dissected portion of the bile duct. Cut the anterior portion of the bile duct above the pancreas. Insert a bile duct stent into the bile duct and secure it in place with 7-0 silk.! cautIon Make sure not to insert the bile duct stent too deep, to avoid obstructing the bile duct confluence (Fig. 2b).? trouBlesHootInG
14| Gently retract the right lobe of the liver with a small, wet sponge toward the xiphoid process to expose the IHIVC.
15| Use a fine-tip cautery to dissect the retroperitoneum above the right renal artery and veins. Slightly displace the IHIVC with a cotton swab to cauterize small veins merging into the IHIVC on the right side.
16| Remove the small sponge retracting the right lobe and use it to cover the PV to avoid injury to the PV. Dissect the left side of the IHIVC above the left renal artery and veins. Slightly displace the IHIVC with a cotton swab to cauterize veins merging into the IHIVC on the left side. Also cauterize the lumbar veins merging into the IHIVC.
17| Ligate the right adrenal vein with 7-0 silk. Ligation should be placed close to the IHIVC.
18| Skeletonize the right renal vein and separate it from the right renal artery. Put 10-0 nylon under the right renal vein.
19| Dissect the retroperitoneum and the fat on the IHIVC.
20| Inject 20 U (20 µl) of heparin sodium using a 0.5-ml U-100 insulin syringe (28-gauge) via the penile vein. crItIcal step Avoid infusing any air bubbles. Even a small amount of air could cause air embolism and potentially be fatal for the animal. crItIcal step See supplementary Video 2 for additional guidance on donor liver perfusion and harvest (Steps 20–34).
21| While waiting for 1 min for the heparin to distribute systemically, use a small, wet gauze to retract the duodenum to expose the PV. Confirm the location of the pyloric vein and the splenic vein merging into the PV.
22| Slowly inject cold 4 °C saline or UW solution to perfuse the donor liver from the IHIVC using a 5-ml syringe with a 27-gauge needle. The needle should be inserted slightly below where the left renal vein merges with the IHIVC. When blood

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
nature protocols | VOL.11 NO.7 | 2016 | 1167
from the donor liver is flushed and the liver turns evenly pale, stop the infusion. It usually requires 2–3 ml of perfusion solution to achieve good perfusion of the graft. Immediately cut the PV below the splenic vein to make an outlet for the perfusion solution. crItIcal step Remove any air bubbles from the syringe before infusion to avoid infusion of air into the graft and subsequent air embolism. Air embolism of the donor liver would be visible as multiple red patches, indicating nonperfused areas. This would lead to poor graft function after implantation.
23| Cut the bile duct below the area where the bile duct stent is inserted (Fig. 2b). We prefer to cut the bile duct after perfusion rather than before, to avoid bleeding before perfusion, which may compromise the cardiodynamic stability of the donor and the condition of the graft.
24| Using a cotton swab and forceps, skeletonize the PV. crItIcal step Removal of fat from the PV will make the cuff attachment easier and also help avoid stenosis in the cuff.? trouBlesHootInG
25| Ligate the pyloric vein and the splenic vein with 10-0 nylon. Leave one segment of 10-0 nylon on the splenic vein for the cuff attachment. Cut the PV trunk below the splenic vein (Fig. 2c). crItIcal step Alternatively, this step can be performed before graft perfusion at Step 20 if preferred.
26| Ligate the right renal vein with 10-0 nylon and cut it.
27| Separate the right renal artery from the IHIVC.
28| Put a 10-0 nylon needle through the IHIVC above the left renal vein. Leave one segment of 10-0 nylon for the cuff attachment.
29| Cut the IHIVC above the left renal vein (Fig. 2d).
30| Use a small, wet nonwoven gauze sponge to gently retract the liver to expose the gall bladder. Use 10-0 nylon with a needle with a needle holder (Fig. 1c), and put the swaged end of the needle under the cystic duct and ligate it. Cut the gall bladder with scissors or cauterize it with a cautery to drain bile.
31| Retract the liver downward to expose the SHIVC. After cutting the falciform ligament, cut the anterior wall of the SHIVC first, and then cut the posterior wall of the SHIVC (Fig. 2e). If the confluence of the left phrenic vein and the SHIVC is close to the liver, it is necessary to ligate and cut the left phrenic vein to avoid bleeding after SHIVC anastomosis during the recipient operation. However, in our experience, it is not necessary to ligate the left phrenic vein in the majority of cases when using C57BL/6 mice as donors. crItIcal step It is important to cut both the anterior and the posterior wall as close to the diaphragm as possible, to preserve enough margin for anastomosis of the SHIVC in the recipient operation.
32| Cut the left triangle ligament and retract the left lateral lobe to the right side. Ligate the paraesophageal vessel located at the cranial end of the caudate lobe with 7-0 silk.
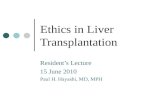
SpV
SpA
LGA
PHA
Pyloric vein
GB
Rt. RV
Lt. RV
Rt. adrenal vein
Lumbar veins(Step 25)
a (Step 12)b (Steps13 and 23)
d (Step 29)
c
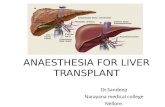
e (Step 31)Figure 2 | Schematic drawing of mouse liver and demonstration of incisions for donor harvest. Labels indicate the following: (a) PHA incision line, (b) bile duct stent inserted in the common bile duct, (c) PV incision line, (d) IHIVC incision line, and (e) SHIVC incision line. Dashed lines represent the locations of incisions only, and solid lines represent the locations of tie and incision procedures. GB, gallbladder; LGA, left gastric artery; Lt. RV, left renal vein; Rt. RV, right renal vein; SpA, splenic artery; SpV, splenic vein.

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
1168 | VOL.11 NO.7 | 2016 | nature protocols
33| Cut the ligament and connective tissue between the liver and the retroperitoneum.
34| Harvest the whole liver and immediately place the organ in a container with cold (4° C) saline or UW solution. Discard the carcass of the donor mouse according to institutional guidelines.
Back-table preparation of the liver graft ● tIMInG 15–30 min35| Place crushed ice in an insulated foam container without a lid, and use a tissue culture dish on ice to prepare the liver graft. The dish should be filled with cold (4 °C) saline or UW solution. Carefully rotate the donor liver floating in the dish so that the inferior surface faces upward. Clamp the handle of a Weldon miniature bulldog clamp (Fig. 1c) with a mosquito clamp (Fig. 3a). Put soft clay on the handle of the mosquito clamp to fix it in place on the ice. crItIcal step See supplementary Video 3 for additional guidance on cuff attachment (Steps 35–40).
36| Clamp the extension handle of a 16-gauge cuff with a bulldog clamp and hold it in place (Fig. 3a). Pull the 10-0 nylon tied to the IHIVC at Step 25 through the 16-gauge cuff, and also pull the IHIVC through the cuff (Fig. 3b).
37| Confirm the lumen of the IHIVC and fold the IHIVC over the 16-gauge cuff to expose the inner endothelial surface. crItIcal step The extension handle of the cuff should be on the ventral side of the IHIVC to avoid twisting.? trouBlesHootInG
38| Secure the IHIVC to the cuff by ligating it with 7-0 silk (Fig. 3c). Two ties should be enough to secure the IHIVC to the cuff. Ligation should be at one of the grooves made on the cuff body to avoid detachment of the ligation from the cuff. Cut excess 7-0 silk close to the tie.
39| Put 5-0 silk around the IHIVC between the attached cuff and the right inferior lobe, and make one tie. crItIcal step This tie should be tight enough to prevent bleeding from the IHIVC immediately after PV anastomosis, but it should be loose enough to release after the IHIVC anastomosis.
40| Attach a 20-gauge cuff to the PV in a similar manner as the IHIVC cuff attachment at Step 39 (Fig. 3d). crItIcal step The extension handle of the cuff should be on the ventral side of the PV. Avoid twisting of the PV by having the pyloric vein and the splenic vein at 3 o’clock and 6 o’clock.
41| Rotate the liver and expose its superior side. Put a stay suture on the SHIVC using 10-0 nylon on the bilateral edge (Fig. 3e). Use a Johns Hopkins bulldog clamp (Fig. 1c) to hold the stay suture on both sides. crItIcal step See supplementary Video 4 for additional guidance on stay suture attachment (Step 41).
recipient operation ● tIMInG 70–90 min42| Anesthesia and laparotomy. Anesthetize the recipient mouse, make a midline incision, wrap the intestine with wet gauze, and expose the liver in the same way as in the donor surgery (Steps 5–10). Use a micro-retractor to retract the abdominal wall (Fig. 1b).
a
b c
d e
Figure 3 | Back-table preparation of the liver graft. (a) Donor liver is placed with the inferior surface facing upward in a tissue culture dish placed on ice filled with cold (4 °C) saline or UW solution. The cuff attachment is set into position with a Weldon miniature bulldog clamp and a mosquito clamp fixed into place with soft clay. (b) To begin attachment of the cuff to the IHIVC, pull the 10-0 nylon tied to the IHIVC through the 16-gauge cuff. (c) Confirm the lumen of the IHIVC and fold the IHIVC over the 16-gauge cuff to expose the inner endothelial surface. (d) Appearance after cuff attachment of both the IHIVC and the PV. (e) Appearance after putting stay sutures on the SHIVC using 10-0 nylon on the bilateral edge. Experiments were performed under an institutional animal care and use committee–approved protocol.

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
nature protocols | VOL.11 NO.7 | 2016 | 1169
43| Cut the ligament around the caudate lobe. Cut the falciform ligament. Use a small, wet gauze to retract down the liver to expose left triangle ligaments for cutting. crItIcal step See supplementary Video 5 for additional guidance on preparation before anhepatic phase (Steps 43–55).
44| Ligate the left phrenic vein with 10-0 nylon. crItIcal step Put the needle through the diaphragm with suture placed as close to the left phrenic vein as possible.
45| Expose the paraesophageal vessels and ligate with 7-0 silk.
46| Retract the liver with a small, wet gauze to expose the retroperitoneal space below the SHIVC. First, cut the ligament between the liver and the retroperitoneum using Vannas capsulotomy scissors (Fig. 1c). Then, use Gill iris forceps (Fig. 1c) to dissect the space between the liver and the retroperitoneum.
47| Put the liver back in its normal position. Carefully put Gill iris forceps behind the liver just below the SHIVC. Put 2-0 silk through behind the SHIVC.
48| Expose the IHIVC, cauterize the small veins behind the IHIVC, and cauterize the lumbar veins in the same manner as in Steps 14–16.
49| Cauterize the right adrenal veins.
50| Use Gill iris forceps to dissect behind the IHIVC. Make sure that the IHIVC is free from any retroperitoneal structure.
51| Expose the hilum with a small, wet gauze. Ligate the PHA with 10-0 nylon (Fig. 4a).
52| Dissect the common bile duct and isolate from the PV. Ligate with 7-0 silk as close to the confluence as possible, and cut above the ligation (Fig. 4b). Use a cotton tip to gently separate the bile duct from the PV.
53| Ligate the right PV with 10-0 nylon (Fig. 4c, solid line). Leave one end long enough to use as the stay suture during the anhepatic phase.
54| Prepare for the anhepatic phase by adjusting the anesthesia so that the respiration rate is about one breath per second. crItIcal step Anesthesia adjustment needs to be done before clamping of the IHIVC and the PV in Step 56. If the anesthesia is too deep and the respiration is slower than one breath per second, the respiration may stop and the animal may die during the anhepatic phase.
55| Using a 5-ml syringe filled with cold (4 °C) saline and with a 22-gauge catheter attached, slowly flush the liver graft from the PV to remove UW solution. Use 2–3 ml to perfuse. crItIcal step Avoid allowing any air into the graft.
56| Place microclamps first on the IHIVC and then on the PV. crItIcal step Place clamps as low as possible to leave the margin for anastomoses as long as possible. Expose the SHIVC and gently pull 2-0 silk to create space to put the jaw
a (Step 51)
b (Step 52)
e
c (Steps 53 and 59)
d
SpV
SpA
LGA
PHA
Pyloric vein
GB
Rt. RV
Lt. RV
Rt. adrenal vein
Lumbar veins
(Step 58)
(Step 59)
Figure 4 | Schematic drawing of recipient hepatectomy illustrating where graft incisions occur. (a) PHA incision line. (b) Bile duct incision line; ligate the common bile duct with 7-0 silk as close to the confluence as possible and make the incision above the ligation. (c) PV incision line; ligate the right PV with 10-0 nylon and cut the bifurcation of the PV just above the right PV ligation after clamping the PV. (d) SHIVC incision line; cut the SHIVC as close to the liver as possible. (e) IHIVC incision line. Dashed lines represent a cut, solid lines represent a tie and cut procedure, and the solid double line represents a tie only. GB, gallbladder; LGA, left gastric artery; Lt. RV, left renal vein; Rt. RV, right renal vein; SpA, splenic artery; SpV, splenic vein.

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
1170 | VOL.11 NO.7 | 2016 | nature protocols
of a Weldon miniature bulldog clamp behind the SHIVC. Place the bulldog clamp on the diaphragm slightly above the border between the diaphragm and the SHIVC. Firmly press on the jaws of the bulldog clamp with forceps to make sure that the bulldog clamp is closed tightly. A Satinsky clamp can be used instead of a bulldog clamp, if one with appropriate size for clamping mouse SHIVC is available. crItIcal step See supplementary Video 6 for additional guidance on the anhepatic phase (Steps 56–71).
57| Cut the anterior wall of the SHIVC from the right edge as close to the recipient liver as possible so as to keep a margin for anastomosis as long as possible.
58| Cut the posterior wall of the SHIVC, also from the right edge. crItIcal step Leave some liver parenchyma on the posterior wall, as it helps avoid tearing of the SHIVC during the posterior wall suture (Fig. 4d).
59| Cut the bifurcation of the PV just above the right PV ligation, and then cut the IHIVC as close to the liver as possible so as to leave the margin as long as possible for anastomosis (Fig. 4c,e).
60| Hold the liver by hand and gently lift it. Cut the ligament and connective tissue between the liver and the retroperitoneum. Discard the harvested liver according to institutional guidelines.
61| Rotate the operating table 90° so that the recipient’s head is on the left side in the operator’s view. Use cotton tips to wipe any blood from the retroperitoneal surface, and make sure that there is no active bleeding.
62| Place the graft in the recipient’s abdominal cavity by holding the bulldog clamp on the stay sutures attached to the bilateral edge of the SHIVC.
63| Put a suture on the bilateral edge of the recipient’s SHIVC. crItIcal step Ligate the stay suture on the left edge of SHIVC, and clamp the loose end of the suture with tube-occluding forceps. Place the forceps on soft clay, and gently pull toward the left side of the recipient so that the posterior wall of the SHIVC becomes straight.? trouBlesHootInG
64| Start continuous suture on the posterior wall from the left side of the SHIVC (Fig. 5a). It takes ~7–8 stitches. The stitches should be placed closer together at both edges of the SHIVC to avoid bleeding. crItIcal step The posterior wall of SHIVC is extremely easy to tear. Avoid any abrupt movement when tightening the suture.
65| Continue the suture on the anterior wall from the right side of the SHIVC. Before closing the anterior wall of the SHIVC, flush any air from the SHIVC cavity to avoid air thrombosis, which can be fatal for the recipient. Close the anterior wall. Ligate stay sutures on the bilateral edge of the SHIVC. crItIcal step Ligation of stay sutures should not be too tight, as this may cause narrowing of the SHIVC and outflow block of the graft.
66| Turn the operating table 90° so that the recipient’s head is now in a midline position.
a b
cFigure 5 | Schematic drawings of venous anastomoses and bile duct reconstruction in the recipient operation. (a) SHIVC anastomosis. After placing the bilateral stay suture on the recipient SHIVC, start continuous suture on the posterior wall from the left side of the SHIVC and then continue the suture on the anterior wall from the right side. (b) PV anastomosis. Hold and pull the thread tied to the right PV and a stay suture on the left edge of posterior wall of the PV and slightly lift the anterior wall of the recipient’s PV using an L-shaped injector; then insert the donor PV cuff. (c) Bile duct reconstruction; cut the anterior wall of the recipient bile duct and insert the bile duct stent into the recipient’s bile duct.

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
nature protocols | VOL.11 NO.7 | 2016 | 1171
67| Retract the liver with a wet gauze and expose the liver hilum. Move the intestine upward so that the recipient’s PV is close to the donor PV.
68| Clamp the thread tied to the right PV with a Johns Hopkins bulldog clamp. Place the bulldog clamp on the right side of the recipient so that the recipient PV is in an upright position.
69| Place a stay suture on the left edge of the posterior wall of the PV. Use a Johns Hopkins bulldog clamp to hold the suture, and place the bulldog on the left side of the recipient. crItIcal step The anterior wall of the PV should be arching downward and should not overlap with the posterior wall. Nonoverlapping anterior and posterior walls make the insertion of the PV cuff easier.
70| Put 7-0 silk around the recipient PV, and make one knot. Using an L-shaped injector, slightly lift the anterior wall of the recipient’s PV, hold the extension handle by Hoskin Mk II micro forceps (Fig. 1c), and insert the donor PV cuff (Fig. 5b). Fix the donor PV cuff in the recipient PV with 7-0 silk placed around the recipient PV. crItIcal step Insert the cuff while flushing the recipient’s PV with saline using an L-shaped injector. This helps remove air bubbles and avoids any air embolism. Avoid any abrupt movement, and make sure that PV anastomosis is completed without any torsion.? trouBlesHootInG
71| Release the clamp on the PV first, and then the one on the SHIVC. The graft should be perfused and systemic circulation should be restored.
72| Put a stay suture on the bilateral edge of the recipient IHIVC so that the anterior wall is slightly hanging downward and not overlapping the posterior wall. Put a 7-0 silk around the recipient IHIVC and make one knot. Use an L-shaped injector to slightly lift the anterior wall of the recipient’s IHIVC, and insert the donor IHIVC cuff. Fix the donor IHIVC cuff in the recipient’s IHIVC with 7-0 silk. crItIcal step Insert the cuff while flushing the recipient’s IHIVC with saline using an L-shaped injector to remove air. In contrast to rat liver transplantation, we have found that it is unnecessary to evacuate some blood at the end of PV or IHIVC anastomosis in the mouse liver transplantation model. crItIcal step The IHIVC anastomosis is performed in a similar manner as the PV anastomosis. See supplementary Video 7 for additional guidance on IHIVC anastomosis (Steps 72 and 73).
73| Release the 5-0 silk tied around the donor IHIVC first and then release the clamp on the recipient IHIVC.
74| Expose the hilum and use tube- occluding forceps to pull down the thread fixing the donor bile duct stent. Put 7-0 silk around the recipient bile duct and make one knot. Hold the recipient bile duct so that it becomes straight and parallel to the donor bile duct. Cut the anterior wall of the
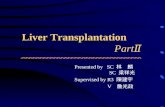
IHIVC cuff
PV cuff
Bile duct stent
Duodenum
Pancreas head
SMV
a b
Figure 6 | Perfused liver graft immediately after completing all anastomoses in mouse liver transplantation. (a) Top, perfused liver graft immediately after completing all anastomoses. Bottom, a higher-power view (25× magnification) of the PV, the IHIVC, and the bile duct anastomoses in the field above (10× magnification). Scale bars, 5 mm. (b) Schematic drawing of transplanted liver after completing anastomoses. SMV, superior mesenteric vein. Experiments were performed under an institutional animal care and use committee–approved protocol.

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
1172 | VOL.11 NO.7 | 2016 | nature protocols
bile duct with scissors and insert the bile duct stent into the recipient’s bile duct (Fig. 5c). Ligate the bile duct stent in place with 7-0 silk to complete the bile duct anastomosis. A representative photograph and a schematic drawing of a transplanted liver graft after completion of all anastomoses are shown in Figure 6. crItIcal step See supplementary Video 8 for additional guidance on bile duct anastomosis (Step 74).
75| Abdominal closure. Put 2–3 ml of warm saline in the abdominal cavity. Make sure that there is no intra-abdominal bleeding.
76| Close the abdominal incision in two layers, using a continuous running 4-0 vicryl.
animal recovery ● tIMInG 4–6 h77| Place the recipient mouse in a warm cage to recover. Use buprenex and cefazolin as indicated in institutional guidelines.
78| Observe the recipient mouse every 1–2 h for the first 4–6 h to make sure that it is fully awake and does not show any signs of pain before returning the cage to the housing location.
? trouBlesHootInGTroubleshooting advice can be found in table 1.
● tIMInG Steps 1–3, preparation of PV and inferior vena cava cuffs: 5–10 minStep 4, preparation of bile duct stent: 5 minSteps 5–34, donor surgery: 40–50 minSteps 35–41, back-table preparation of the liver graft: 15–30 minSteps 42–76, recipient operation: 70–90 minSteps 77 and 78, animal recovery: 4–6 h
antIcIpateD resultsWe have trained four surgeons in the past 5 years to perform mouse liver transplantation proficiently. All of these surgeons had experience and were proficient in liver transplantation in the rat before they started training in mice. It took ~50 operations for each of them to achieve consistent success (i.e., survival of the recipient beyond 7 postoperative days in a healthy condition) using the mouse model. Hematoxylin and eosin–stained sections of normally functioning liver grafts obtained 30 d after syngeneic (C57BL/6 → C57BL/6) or allogeneic (C57BL/6 → C3H) mouse liver transplantation are shown in Figure 7a,b. In allogeneic transplantation, there is mild inflammatory infiltration in the periportal and sinusoidal areas as compared with syngeneic transplantation, as described in a previous paper30. Mouse liver allograft transplantation has been studied extensively at our institution, and we have shown that liver allografts between most mouse strain combinations survive over 100 d and exhibit a state of tolerance without the use of immunosuppressive
taBle 1 | Troubleshooting table.
step problem possible reason possible solution
13 Difficulty inserting the stent into the bile duct
Not able to visualize the inner lumen of the common bile duct
Hold the anterior wall of the bile duct with forceps and confirm the inner lumen before insertion
24 Difficulty removing fat from the PV
Cotton tip is wet and cannot apply enough friction to remove fat
Use a dry cotton tip when removing fat from vessels
37 Difficulty folding the vessel over the cuff
Poor visualization of the inner lumen of the IHIVC
Conduct cuff attachment underwater to keep the lumen open for visualization
63 Difficulty visualizing the posterior wall because the anterior wall is overlapping
Stay sutures on the bilateral edge of recipient SHIVC were placed inappropriately
Place stay sutures on the posterior wall of the recipient SHIVC
70 The donor PV inserted into the recipient PV slips out
The recipient PV is not close enough to the donor PV
Move the recipient’s small intestine upward to the hilum of the donor liver

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
nature protocols | VOL.11 NO.7 | 2016 | 1173
agents11,13,29. Cellular and molecular mechanisms underlying liver transplant tolerance have not been fully elucidated, but those that have been described in the mouse and other species are discussed in recent articles and reviews24,31–33.
10. Yokota, S. et al. IRF-1 promotes liver transplant ischemia/reperfusion injury via hepatocyte IL-15/IL-15Ralpha production. J. Immunol. 194, 6045–6056 (2015).
11. Qian, S. et al. Murine liver allograft transplantation: tolerance and donor cell chimerism. Hepatology 19, 916–924 (1994).
12. Dahmen, U. et al. Split tolerance induced by orthotopic liver transplantation in mice. Transplantation 58, 1–8 (1994).
13. Yoshida, O. et al. DAP12 deficiency in liver allografts results in enhanced donor DC migration, augmented effector T cell responses and abrogation of transplant tolerance. Am. J. Transplant. 14, 1791–1805 (2014).
14. Qian, S. et al. Apoptosis within spontaneously accepted mouse liver allografts: evidence for deletion of cytotoxic T cells and implications for tolerance induction. J. Immunol. 158, 4654–4661 (1997).
15. Li, W. et al. Il-12 antagonism enhances apoptotic death of T cells within hepatic allografts from Flt3 ligand-treated donors and promotes graft acceptance. J. Immunol. 166, 5619–5628 (2001).
16. Li, W. et al. New insights into mechanisms of spontaneous liver transplant tolerance: the role of Foxp3-expressing CD25+CD4+ regulatory T cells. Am. J. Transplant. 8, 1639–1651 (2008).
17. Morita, M. et al. PD-1/B7-H1 interaction contribute to the spontaneous acceptance of mouse liver allograft. Am. J. Transplant. 10, 40–46 (2010).
18. Conzelmann, L.O., Zhong, Z., Bunzendahl, H., Wheeler, M.D. & Lemasters, J.J. Reduced-size liver transplantation in the mouse. Transplantation 76, 496–501 (2003).
19. Tian, Y., Graf, R., Jochum, W. & Clavien, P.A. Arterialized partial orthotopic liver transplantation in the mouse: a new model and evaluation of the critical liver mass. Liver Transpl. 9, 789–795 (2003).
20. Tian, Y. et al. Kupffer cell-dependent TNF-alpha signaling mediates injury in the arterialized small-for-size liver transplantation in the mouse. Proc. Natl. Acad. Sci. USA 103, 4598–4603 (2006).
21. Garuti, C. et al. Hepcidin expression does not rescue the iron-poor phenotype of Kupffer cells in Hfe-null mice after liver transplantation. Gastroenterology 139, 315–322 (2010).
22. Li, X.K. et al. Fulminant hepatitis by Fas-ligand expression in MRL-lpr/lpr mice grafted with Fas-positive livers and wild-type mice with Fas-mutant livers. Transplantation 71, 503–508 (2001).
23. Demetris, A.J. et al. Monitoring of human liver and kidney allograft tolerance: a tissue/histopathology perspective. Transpl. Int. 22, 120–141 (2009).
24. Sanchez-Fueyo, A. & Strom, T.B. Immunologic basis of graft rejection and tolerance following transplantation of liver or other solid organs. Gastroenterology 140, 51–64 (2011).
25. Feng, S. et al. Complete immunosuppression withdrawal and subsequent allograft function among pediatric recipients of parental living donor liver transplants. JAMA 307, 283–293 (2012).
26. Tian, Y., Rudiger, H.A., Jochum, W. & Clavien, P.A. Comparison of arterialized and nonarterialized orthotopic liver transplantation in mice: prowess or relevant model? Transplantation 74, 1242–1246 (2002).
27. Kamada, N. The immunology of experimental liver transplantation in the rat. Immunology 55, 369–389 (1985).
a bFigure 7 | Histology of normally functioning mouse liver grafts 30 d after transplantation. The tissue was fixed in 10% formalin for 24–48 h (at 4 °C). Hematoxylin and eosin staining was performed using paraffin-embedded tissue section. (a) Liver graft 30 d after syngeneic liver transplantation (C57BL/6 → C57BL/6). (b) Liver graft 30 d after allogeneic liver transplantation (C57BL/6 → C3H). In syngeneic transplantation, there are fewer infiltrating inflammatory cells in periportal and sinusoidal areas compared with allogeneic transplantation. Experiments were performed under an institutional animal care and use committee–approved protocol. Scale bars, 50 µm.
Note: Any Supplementary Information and Source Data files are available in the online version of the paper.
acknoWleDGMents This work was supported by the US National Institutes of Health (NIH) (grants P01 AI81678 and R56 AI118777 to A.W.T. and grant T32 AI74490 to O.Y.) and by the Japan Society for the Promotion of Science (Grant-in-Aid for Scientific Research C-26461926 to N.K.). S.Y. was supported by funds from Jichi Medical University (Shimotsuke, Tochigi, Japan). O.Y. was supported by an American Society of Transplantation Basic Science Fellowship. We thank S. Qian and M. Morita (Department of Immunology, Lerner Research Institute, Cleveland Clinic) for valuable advice. We thank T. Teratani (Jichi Medical University) for valuable input.
autHor contrIButIons S.Y. and A.W.T. conceived and designed the outline of the manuscript. S.Y., S.U., Y.O., N.K. and A.P.-G. wrote the manuscript and prepared the pictures and images. S.K., O.Y., N.M., Y.Y., D.A.G. and A.W.T. revised and provided input during final editing of the manuscript.
coMpetInG FInancIal Interests The authors declare no competing financial interests.
Reprints and permissions information is available online at http://www.nature.com/reprints/index.html.
1. Chong, A.S., Alegre, M.L., Miller, M.L. & Fairchild, R.L. Lessons and limits of mouse models. Cold Spring Harb. Perspect. Med. 3, a015495 (2013).
2. Qian, S.G., Fung, J.J., Demetris, A.V., Ildstad, S.T. & Starzl, T.E. Orthotopic liver transplantation in the mouse. Transplantation 52, 562–564 (1991).
3. Kamada, N. & Calne, R.Y. Orthotopic liver transplantation in the rat. Technique using cuff for portal vein anastomosis and biliary drainage. Transplantation 28, 47–50 (1979).
4. Klein, I. & Crispe, I.N. Complete differentiation of CD8+ T cells activated locally within the transplanted liver. J. Exp. Med. 203, 437–447 (2006).
5. Shen, X.D. et al. Inflammatory responses in a new mouse model of prolonged hepatic cold ischemia followed by arterialized orthotopic liver transplantation. Liver Transpl. 11, 1273–1281 (2005).
6. Conzelmann, L.O. et al. Graft tumor necrosis factor receptor-1 protects after mouse liver transplantation whereas host tumor necrosis factor receptor-1 promotes injury. Transplantation 82, 1214–1220 (2006).
7. Ueki, S. et al. Critical role of interferon regulatory factor-1 in murine liver transplant ischemia reperfusion injury. Hepatology 51, 1692–1701 (2010).
8. Ueki, S. et al. Hepatic B7 homolog 1 expression is essential for controlling cold ischemia/reperfusion injury after mouse liver transplantation. Hepatology 54, 216–228 (2011).
9. Yoshida, O. et al. CD39 expression by hepatic myeloid dendritic cells attenuates inflammation in liver transplant ischemia-reperfusion injury in mice. Hepatology 58, 2163–2175 (2013).

©20
16 M
acm
illan
Pu
blih
ers
Lim
ited
. All
rig
hts
res
erve
d.
protocol
1174 | VOL.11 NO.7 | 2016 | nature protocols
28. Steger, U., Sawitzki, B., Gassel, A.M., Gassel, H.J. & Wood, K.J. Impact of hepatic rearterialization on reperfusion injury and outcome after mouse liver transplantation. Transplantation 76, 327–332 (2003).
29. Starzl, T.E. & Lakkis, F.G. The unfinished legacy of liver transplantation: emphasis on immunology. Hepatology 43, S151–S63 (2006).
30. Qian, S., Fung, J.J., Demetris, A.J. & Starzl, T.E. Allogeneic orthotopic liver transplantation in mice: a preliminary study of rejection across well-defined MHC barriers. Transplant. Proc. 23, 705–706 (1991).
31. Benseler, V. et al. The liver: a special case in transplantation tolerance. Semin. Liver Dis. 27, 194–213 (2007).
32. Morita, M. et al. Rejection triggers liver transplant tolerance: involvements of mesenchyme-mediated Immune Control Mechanisms. Hepatology 62, 915–931 (2015).
33. Yokota, S., Yoshida, O., Ono, Y., Geller, D.A. & Thomson, A.W. Liver transplantation in the mouse: insights into liver immunobiology, tissue injury and allograft tolerance. Liver Transpl. 22, 536–546 (2016).