Smarthometechshort 13304126815608-phpapp01-120228010616-phpapp01
description

ORTHOPEDIC ASPECTS OFORTHOPEDIC ASPECTS OF
METABOLIC BONE METABOLIC BONE DISEASEDISEASE
Presented by EKKASIT SRITHAMMASIT, MD.Presented by EKKASIT SRITHAMMASIT, MD.
Leon Lenchik , MD et al
Department of Radiology, The Bowman Gray School of Medicine, Wake Forest University (LL), Winston-Salem, North Carolina
Orthopedic Clinics of North America - Volume 29, Issue 1 (January 1998)

Metabolic bone diseaseMetabolic bone disease (MBD) (MBD)• Encompasses a diverse group of disorders
associated with altered calcium and phosphorus homeostasis.
• To orthopedic surgeons; MBD is often silent until the patient presents with fracture.
IntroductionIntroduction

Table of contentTable of content
Osteoporosis. Osteomalacia and rickets. Hyperparathyroidism. Hypoparathyroidism. Hyperthyroidism. Hypothyroidism. Renal osteodystrophy. Paget's disease.

OSTEOPOROSISOSTEOPOROSIS

OSTEOPOROSISOSTEOPOROSIS
• Most common metabolic bone disease.
• One of the most prevalent conditions associated with aging.

OSTEOPOROSISOSTEOPOROSIS
Definition : reduced bone mass of normal composition.

OSTEOPOROSISOSTEOPOROSIS
• Clinical definition: requires the presence of a nontraumatic fracture.
• Histologic definition: requires normally mineralized bone to be present in reduced quantity.

OSTEOPOROSISOSTEOPOROSIS

Diagnosis OsteoporosisDiagnosis Osteoporosis
Bone densitometryBone densitometry; gold standard1. Detection osteoporosis before fractures.
2. Determination disease severity.
3. Estimation risk of fracture. – Serial BMD measurements enable determination
of rate of bone loss or gain and thereby help in monitoring therapy.
Plain filmPlain film; loss of 30% to 50% of bone is required before it is detected on conventional radiographs.


Ostoporosis ClassificationOstoporosis Classification
• Primary osteoporosis. (idiopathic) : more common– Type 1 (postmenopausal) – Type 2 (age-related or senile)
• Secondary osteoporosis. – Metabolic (acromegaly, hypercorticism, hyperthyroidism,
hyperparathyroidism, hypogonadism, pregnancy, diabetes mellitus)
– Congenital (osteogenesis imperfecta, Ehlers-Danlos syndrome, homocystinuria, mastocytosis, ochronosis, Gaucher's disease)
– Nutritional (alcoholism, malnutrition, calcium deficiency, scurvy)– Drug-related (steroids, heparin).

Radiological finding (1)Radiological finding (1)
• The m/c radiologic finding is generalized osteopenia.
– Cortical thinning and accentuation of weightbearing trabeculae.
– The bone surfaces are well defined, with sharp margins.

Radiological finding (2)Radiological finding (2)
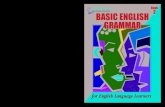
• Fractures - vertebral deformities, which are also common, include biconcave end plates (fish vertebrae) and anterior wedging.

Lateral radiograph of the lumbar spine in a 55-year-old woman with postmenopausal osteoporosis shows generalized osteopenia,
compression fractures, and biconcave vertebral endplates ("fish vertebra"). Notice thin, well-defined vertebral cortices ( arrows).


Radiological finding (3)Radiological finding (3)
• Patients with osteoporosis secondary to excess steroids.
– Generalized osteopenia.– Fractures with exuberant callus – Steroid-related complications;
• Intravertebral vacuum (nitrogen gas); • Avascular necrosis.• Osteomyelitis.

Differential considerations for Differential considerations for diffuse osteopeniadiffuse osteopenia
1. Osteomalacia.– indistinct trabeculae and poorly defined interfaces
between cortical and trabecular bone. – Presence of Looser's zones.
2. Hyperparathyroidism.– bone resorption at characteristic sites.
3. Multiple myeloma. – MR imaging may show areas of marrow
replacement.

Regional or localized Regional or localized osteoporosisosteoporosis
1. Immobilization and disuse
2. Reflex sympathetic dystrophy syndrome (RSDS)
3. Transient regional osteoporosis– Transient osteoporosis of the hip.– Regional migratory osteoporosis.
4. Inflammatory arthritis.
5. Tumors
6. Infection.

Radiologic findings in regional Radiologic findings in regional osteoporosisosteoporosis (1)
• RSDS : mediated by the sympathetic nervous system and is characterized by
– aggressive osteoporosis, – soft tissue swelling. The cause is usually traumatic, but the
disease may also be idiopathic.

AP radiograph of the hand in a patient with reflex sympathetic dystrophy syndrome shows soft-tissue swelling and periarticular osteopenia.


RICKETS AND RICKETS AND OSTEOMALACIAOSTEOMALACIA

Rickets and osteomalacia Rickets and osteomalacia
• Rickets and osteomalacia are similar histologically.
• Abnormality in vitamin D metabolism.
• Incomplete mineralization of normal osteoid tissue.
Rickets Rickets
Occurs in childrenOccurs in children
AAffects immature ffects immature bonebone
Osteomalacia Osteomalacia
Occurs in adultOccurs in adult
Affects mature boneAffects mature bone

Rickets and osteomalacia Rickets and osteomalacia
Maintain calcium and phosphate homeostasis.

Clinical findings ofClinical findings of Rickets and OsteomalaciaRickets and Osteomalacia
Rickets:Rickets: stunted skeletal growth.• Apathetic, Irritable, Hypokinetic.• Frontal bossing, softening of the skull,
dental caries, rachitic rosary, kyphosis, joint enlargement, or bowing of long bones.
• Fractures and slipped capital femoral epiphyses.
Depend in part on the etiology and severity of the disorder, as well as the age of the patient at presentation


Clinical findings ofClinical findings of Rickets and OsteomalaciaRickets and Osteomalacia
Osteomalacia:Osteomalacia: more subtle.
• Fatigue, malaise, or bone pain.
• Proximal muscle weakness and abnormal gait may be present.
Depend in part on the etiology and severity of the disorder, as well as the age of the patient at presentation

Radiologic findings ofRadiologic findings of
OsteomalaciaOsteomalacia
• The M/C radiologic sign is generalized osteopenia.
• Coarsened and indistinct bony trabeculae.• Poorly defined interfaces between cortical
and trabecular bone. • Looser's zone, or pseudofracture. (more
specific but less common) • End plate deformities and fractures of
vertebral bodies, bowing and fractures of long bones, and basilar invagination of skull.
The radiologic findings of osteomalacia are often nonspecific, difficult to confirm the diagnosis with imaging studies

Radiologic findings ofRadiologic findings of
OsteomalaciaOsteomalacia
Looser's zone.Looser's zone.• Linear areas of undermineralized
osteoid that occur in a bilateral and symmetric distribution.
• Characteristic sites; inner margins of femoral neck, proximal ulna, axillary margin of the scapula, pubic rami, and ribs.
• DDx; Paget's disease or fibrous dysplasia.

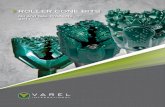
AP radiograph of the hip in a 50-year-old man with osteomalacia shows coarsened trabecular pattern with indistinct trabeculae.

AP radiograph of the hip in a patient with osteomalacia shows multiple Looser zones ( arrows) in the superior pubic ramus.


Osteomalacia. AP radiograph of the pelvis showing osteopenia with bilateral femoral neck pseudofractures (arrows).

Radiologic findings ofRadiologic findings of
RicketsRickets • The M/C radiologic sign is generalized
osteopenia. • Increased lucency, widening, elongation,
irregularity, and cupping of the metaphyses.– Earliest; Slight axial widening of the physis– Next; Increased lucency of the zone of provisional
calcification. – More advance; The physis widens and its contour
becomes irregular.
• Occasionally, in patients with rickets caused by chronic renal disease, increased sclerosis may be seen.

Radiologic findings ofRadiologic findings of
RicketsRickets • The regions of highest yield on
radiologic evaluation of rickets are those that are undergoing rapid growth.
– Costochondral junctions of middle ribs (rachitic rosary)
– Distal femur– Both ends of the tibia– Distal radius and ulna– Proximal humerus.

Radiologic findings ofRadiologic findings of
RicketsRickets • The complication of rickets.
– Skeletal deformities. – In neonates; posterior flattening and squaring of
the skull, or craniotabes, may be seen. – In early childhood; bowing deformities of arms and
legs are common.– Older children: scoliosis, vertebral end plate
deformities, basilar invagination of the skull may be seen.
– Advance disease: Slipped capital femoral epiphysis.

A, AP radiograph of the knee in a 2-year-old girl with rickets shows generalized osteopenia and widening of the metaphyses of the proximal tibia and fibula. B, AP radiograph of
the wrist in another child with rickets shows generalized osteopenia, as well as widening and irregularity of the metaphyses of the distal radius and ulna.

Rickets in a young child with growth plate widening and irregularity in the wrist (A) and knees (B). Note the small epiphyses in the knees.

Rachitic rosary. (A) and lateral (B) radiographs of the chest showing prominence of the costochondral junctions (arrows).

Vitamin D-resistant rickets in a 1-year-old child. (A) AP radiograph of the knees showing irregularity and widening of the growth plates. The epiphyses are s
mall and irregular as well. (B) Three years after high-dose vitamin D therapy, the knees appear normal. There is residual femoral bowing.

HYPERPARATHYROIDISHYPERPARATHYROIDISMM

HYPERPARATHYROIDISHYPERPARATHYROIDISMM
• Primary– Parathyroid adenoma
• Secondary– chronic renal insufficiency.
Hyperparathyroidism may result in either bone resorption or bone formation, bone resorption usually dominates.


Radiologic findings ofRadiologic findings of
HYPERPARATHYROIDISMHYPERPARATHYROIDISM • The M/C radiologic abnormality is generalized
osteopenia.
• Bone resorption, bone sclerosis, brown tumors, chondrocalcinosis, soft tissue calcification, and vascular calcification.
• Brown tumors appear as well-defined lytic lesions. – After resection of parathyroid adenomas, the lesions may
become sclerotic and may mimic blastic metastasis.
• Bone resorption, the most characteristic finding, is usually classified as
– subchondral, trabecular, endosteal, intracortical, subperiosteal, subligamentous, and subtendinous.


Radiologic findings ofRadiologic findings of
HYPERPARATHYROIDISMHYPERPARATHYROIDISM • Subperiosteal resorption - M/C
– Usually occurs in the hands and feet. – M/C affected site: radial aspects of the middle phalanges.– Acro-osteolysis or phalangeal tufts resoption may also be
present.
• Trabecular resorption– Often seen in the diploic space of the skull, where it has a
characteristic salt and pepper appearance.
• Subchondral resorption – May be seen in the sacroiliac joints, sternoclavicular joints,
acromioclavicular joints, symphysis pubis, and discovertebral junction .

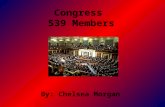
AP radiograph of the hand in a 66-year-old woman with primary hyperparathyroidism owing to parathyroid adenoma shows subperiosteal bone
resorption ( arrows) along the radial aspect of 2nd, 3rd, and 4th middle phalanges.


AP radiograph of the knee in a child with hyperparathyroidism shows subperiosteal bone resorption ( arrow) along the proximal medial tibia.

Lateral radiograph of the skull in a 23-year-old man with secondary hyperparathyroidism shows trabecular resorption of the diploic space ("salt and pepper" appearance).


Dental radiograph in another child with hyperparathyroidism shows resorption ( arrow) of the lamina dura of the mandible.

Radiologic findings ofRadiologic findings of
HYPERPARATHYROIDISMHYPERPARATHYROIDISM
SecondarySecondary• Bony sclerosis; focal
or generalized.• Rugger-jersey
appearance of spine.
• Soft tissue and vascular calcification.
PrimaryPrimary• Chondrocalcinosis• usually seen in the
menisci of the knee, the triangular fibrocartilage of the wrist, and the pubic symphysis

AP radiograph of the wrist in an 83-year-old woman with primary hyperparathyroidism shows chondrocalcinosis ( arrow) of the triangular fibrocartilage.


Secondary HPT. Radiograph of the pelvis and hips showing diffuse osteosclerosis.

A, AP radiograph of the spine in a patient with secondary hyperparathyroidism shows generalized bone sclerosis, small kidneys, and left renal calculi. B, Lateral radiograph of the lumbar spine in another
patient with secondary hyperparathyroidism shows horizontal, bandlike ("rugger jersey") sclerosis of the vertebral bodies ( arrows).


AP radiograph of the hand in a 50-year-old man with renal osteodystrophy shows acro-osteolysis ( short arrows), subperiosteal bone
resorption ( long arrows), and vascular calcifications.

Secondary HPT. Radiograph of the hand showing resorption of the first to third tufts with soft tissue calcification (1). There is articular
calcification (2), and subperiosteal and subligamentous resorption (3).

The differential diagnosis of The differential diagnosis of
HYPERPARATHYROIDISMHYPERPARATHYROIDISM • Focal subperiosteal resorption involving a single bone
– Neoplasms or osteomyelitis.
• Bone sclerosis in patients with secondary hyperparathyroidism.
– Metastatic disease, radiation-induced bone disease, hypoparathyroidism, myelofibrosis, mastocytosis, sickle-cell disease, and Paget's disease.
• Chondrocalcinosis – Pyrophosphate arthropathy (CPPD) or hemochromatosis.
• Brown tumors– includes other focal lytic lesions, such as giant cell tumor
and fibrous dysplasia.

HYPOPARATHYROIDISMHYPOPARATHYROIDISM

• The M/C cause is The M/C cause is excision of or trauma excision of or trauma to the parathyroid glandsto the parathyroid glands..– may not be recognized for years after may not be recognized for years after
surgery.surgery.
HYPOPARATHYROIDISMHYPOPARATHYROIDISM

Clinical presentation:Clinical presentation:• Neuromuscular Neuromuscular
dysfunction.dysfunction.• Short stature. Short stature. • Delay or failure of tooth Delay or failure of tooth
eruption.eruption.• Gastrointestinal Gastrointestinal
complaints. complaints.
HYPOPARATHYROIDISMHYPOPARATHYROIDISM

Radiologic findings are varied.Radiologic findings are varied. • Bony sclerosis. = Bony sclerosis. = M/C findingM/C finding
– Focal or generalizedFocal or generalized• Subcutaneous calcification.Subcutaneous calcification.• Calvarial thickeningCalvarial thickening• Basal ganglia calcificationBasal ganglia calcification• Hypoplastic dentitionHypoplastic dentition• Premature physeal fusionPremature physeal fusion• Spinal ossification. Spinal ossification. • Occasionally : Osteoporosis, Enthesopathy, Occasionally : Osteoporosis, Enthesopathy,
Dense metaphyseal bands.Dense metaphyseal bands.
Radiologic findings ofRadiologic findings of
HYPOPARATHYROIDISMHYPOPARATHYROIDISM

Lateral radiograph of the skull in a 5-year-old girl with pseudohypoparathyroidism shows thickening ( arrows) of the calvarium.

• Widespread bony sclerosis.Widespread bony sclerosis.– Blastic metastasis, myelofibrosis, renal Blastic metastasis, myelofibrosis, renal
osteodystrophy, sickle-cell disease, and fluorosis. osteodystrophy, sickle-cell disease, and fluorosis. • Dense metaphyseal.Dense metaphyseal.
– Leukemia therapy, heavy-metal poisoning, or Leukemia therapy, heavy-metal poisoning, or hypothyroidism.hypothyroidism.
• Calcifications of the basal gangliaCalcifications of the basal ganglia– Toxoplasmosis or cytomegalovirus infections, after Toxoplasmosis or cytomegalovirus infections, after
radiation therapy, and after carbon monoxide radiation therapy, and after carbon monoxide exposure. exposure.
• Subcutaneous calcifications.Subcutaneous calcifications.– Collagen-vascular diseases, hypervitaminosis D, Collagen-vascular diseases, hypervitaminosis D,
and renal osteodystrophy.and renal osteodystrophy.
differential diagnosis of differential diagnosis of
HYPOPARATHYROIDISMHYPOPARATHYROIDISM

• Inherited disorderInherited disorder• End-organ resistance to parathyroid End-organ resistance to parathyroid
hormone. hormone. • X-linked dominant traitX-linked dominant trait• More common in women.More common in women.• Shares many features with Shares many features with
hypoparathyroidism.hypoparathyroidism.
PseudohypoparathyroidisPseudohypoparathyroidismm

Similar to those of hypoparathyroidismSimilar to those of hypoparathyroidism• Bony sclerosis, Soft tissue calcification, Dense Bony sclerosis, Soft tissue calcification, Dense
metaphyseal bands, Calvarial thickening and Basal metaphyseal bands, Calvarial thickening and Basal ganglia calcification.ganglia calcification.
In additionIn addition• Short metacarpals, metatarsals, and phalanges; Short metacarpals, metatarsals, and phalanges;
diaphyseal exostoses; and cone-shaped epiphyses.diaphyseal exostoses; and cone-shaped epiphyses.• Typically, the first, fourth, and fifth rays are shortened. Typically, the first, fourth, and fifth rays are shortened. • Growth deformitiesGrowth deformities
– Bowing of long bones. Bowing of long bones.
Radiologic findings ofRadiologic findings of PseudohypoparathyroidismPseudohypoparathyroidism

Pseudohypoparathyroidism. (A,B) AP radiographs of the hands showing shortening of the fourth and fifth metacarpals.

AP radiograph of the hand in another child with pseudohypoparathyroidism shows short 3rd, 4th, and 5th metacarpals.

• Incomplete genetic manifestation of Incomplete genetic manifestation of PHP.PHP.
• End-organ resistance to parathyroid End-organ resistance to parathyroid hormone.hormone.
• Share most of their clinical and Share most of their clinical and radiologic features of radiologic features of pseudohypoparathyroidism. pseudohypoparathyroidism.
PseudopseudohypoparathyroidisPseudopseudohypoparathyroidismm

HYPERTHYROIDISMHYPERTHYROIDISM

HYPERTHYROIDISMHYPERTHYROIDISM
• Children; causes accelerated skeletal maturation and advanced bone age.
• Adults; causes generalized osteoporosis leading to vertebral fractures and kyphosis.

HYPERTHYROIDISMHYPERTHYROIDISM
• The M/C causes of hyperthyroidism in adults are toxic diffuse goiter and toxic nodular goiter.
• Excessive production of thyroid hormone by the thyroid gland results in bone resorption is dominant.

HYPERTHYROIDISMHYPERTHYROIDISM
• Patients may experience – Weakness.– Fatigue– Nervousness– Weight loss– Palpitations– Diarrhea– Hypersensitivity to heat.

Radiologic findings in HYPERTHYROIDISMHYPERTHYROIDISM
Pt with radiologic abnormalities typically have had the disease for at least 5 years, more common in men

Radiologic findings in HYPERTHYROIDISMHYPERTHYROIDISM
Skeletal findingsSkeletal findings
• Generalized osteopenia: M/C Finding
• Thyroid acropachy (0.5% to 1%) .
• Kyphosis and insufficiency fractures are occasionally seen.

Radiologic findings in HYPERTHYROIDISMHYPERTHYROIDISM
Thyroid acropachyThyroid acropachy
• A dense, solid periosteal reaction with a feathery contour
– Asymmetric distribution– Radial margin of metacarpals and
phalanges. – Occasionally, long bones are also involved.
• Soft tissue swelling – Hands, feet, and pretibial region of the leg.

AP radiographs of the hand in a 46-year-old man with thyroid acropachy who presented with hand swelling and hypothyroidism 2 years after a thyroidectomy. Note the
dense, solid periosteal reaction with feathery contour ( arrows) along the shafts of 2nd, 3rd, and 4th proximal and middle phalanges.

Thyroid acropachy. (A,B) Radiographs of the hands showing diaphyseal periostitis (arrows) and generalized swelling. (C) Radiograph in a different patient showing marked soft tissue prominence.

Differential for
HYPERTHYROIDISMHYPERTHYROIDISM
• Thyroid acropachyThyroid acropachyPeriosteal reaction involving multiple bones– Hypertrophic osteoarthropathy:
• long bones.• Feathery contour is absent.
– Pachydermoperiostosis: • Long bones. • Periosteal reaction extends to the metaphyses
and epiphysis.

A, AP radiograph of the leg in a child with hypertrophic osteoarthropathy shows thin periosteal reaction ( arrowheads) along the diaphyses of the tibia and fibula. The hands were not involved.
B, Frontal radiograph of both forearms in a patient with pachydermoperiostosis shows dense periosteal reaction involving the diaphyses and metaphyses of both radii and ulnae.

HYPOTHYROIDISMHYPOTHYROIDISM

HYPOTHYROIDISMHYPOTHYROIDISM
Manifests Manifests • Delayed physeal closure and bone age.• In infants: cretinism• In children: mental retardation, obesity,
developmental delay, growth retardation, lethargy, and constipation.
• In adults: dry coarse skin and hair, fatigue, lethargy, paresthesias, constipation, and bradycardia.
Causes of hypothyroidismCauses of hypothyroidism• Surgery, tumors, iodine deficiency, medications, and
pituitary disorders.

The radiologic findings inThe radiologic findings in HYPOTHYROIDISMHYPOTHYROIDISM
Depend on the patient's age at presentation.
• In infants:– Absence epiphysis : distal femoral and
proximal tibial. – In the skull, wormian bones and prolonged
separation of sutures.

The radiologic findings inThe radiologic findings in HYPOTHYROIDISMHYPOTHYROIDISM
• Depend on the patient's age at presentation.• In children:
– Fragmented, irregular epiphysis. Referred to as epiphyseal dysgenesis, the appearance may simulate that of Legg-Calve-Perthes disease.
– Slipped capital femoral epiphysis.– In the spine, anteriorly wedged bullet vertebrae.– Dentition and pneumatization of the sinuses may
be delayed.– Occasionally, dense metaphyseal bands are seen.

A, Radiograph of the knee in a 2-year-old boy with delayed bone maturity owing to hypothyroidism shows nonossification of the epiphysis of the distal femur and proximal tibia. Both epiphyses
should be ossified by 1 month of age. B, AP radiograph of the left hip in another child with hypothyroidism shows a fragmented, irregular ( arrow) proximal femoral epiphysis. This appearance may mimic Legg-Calve-Perthes disease.

The radiologic findings inThe radiologic findings in HYPOTHYROIDISMHYPOTHYROIDISM
• Depend on the patient's age at presentation.
• In adults :
– Usually mild.– Generalized osteoporosis is M/C. – Occasionally, soft tissue edema, dystrophic
calcification, ligamentous laxity, and carpal tunnel syndrome are present.
– Coxa vara may develop.

ACROMEGALYACROMEGALY

ACROMEGALYACROMEGALY
• Results from excessive growth hormone after physeal closure.
• Third or fourth decade of life.
• Usually caused by a pituitary adenoma.

ACROMEGALYACROMEGALY
Clinical findings;Clinical findings;• Coarse facial features• Thick skin• Poor dental occlusion• Thick calvarium• Deepening of voice• Lantern jaw• Prominent tongue• Broad hands• Organomegaly (kidneys, liver, pancreas, spleen thyroid, heart).• Arthropathy mostly involves large joints.• Compressive neuropathy, such as carpal tunnel syndrome or
spinal cord compression, may result from soft tissue and bony hypertrophy.
• Fatigue and lethargy are also quite common.

Radiographic findings ofRadiographic findings of ACROMEGALYACROMEGALY
Bony and soft tissue overgrowthBony and soft tissue overgrowth• Soft tissue thickening is classically seen in the heel
pads and digits .• Bony enlargement is most notable in the skull,
vertebra, phalnageal tufts.• Calvarial thickening, prominent supraorbital ridges.
JointJoint• In the early stages of the disease, joint-space
widening is seen.• In later stages, as the thickened cartilage, and
radiologic signs of joint-space narrowing, subchondral sclerosis, subchondral cysts, and osteophytes become apparent.

Radiographic findings ofRadiographic findings of ACROMEGALYACROMEGALY
• Additional radiologic findings– enlargement of costochondral junctions– enlargement of the sella turcica and paranasal sinuses– intervertebral disk widening– posterior vertebral scalloping– Spade like phalangeal tufts.– degenerative enthesopathy– periarticular calcification– osteoporosis.
• The most common musculoskeletal complications of acromegaly are premature osteoarthritis and degenerative disk disease.

A, Lateral radiograph of the foot in a patient with acromegaly shows soft-tissue thickening of the heel pad. B, Lateral radiograph of the skull in another patient with acromegaly
shows enlarged prognathic mandible and enlarged sella turcica ( arrow).

AP radiograph of the hand in a patient with arthropathy of acromegaly shows joint-space narrowing and osteophytes involving the 3rd and 4th interphalangeal joints.

AP radiograph of the distal phalanx in a 36-year-old man with acromegaly shows spade-like phalangeal tuft with soft-tissue overgrowth.

The radiologic differential diagnosis in The radiologic differential diagnosis in
ACROMEGALYACROMEGALY
• In advanced disease, the combination of soft tissue and bony findings allows accurate diagnosis.
• Earlier in the disease course, isolated radiologic findings allow some differential considerations.

The radiologic differential diagnosis in The radiologic differential diagnosis in
ACROMEGALYACROMEGALY
• Pachydermoperiostosis– Enlarged sinuses, prominent supraorbital
ridges, and thickened phalanges.– Sella turcica is normal, no joint-space
widening. does not occur.
• Long-term phenytoin therapy- Heel pad thickening

RENAL RENAL OSTEODYSTROPHYOSTEODYSTROPHY

RENAL OSTEODYSTROPHYRENAL OSTEODYSTROPHY
• Bone disease in patients with chronic renal insufficiency.
• It combines features of rickets, osteomalacia, secondary hyperparathyroidism, and osteoporosis.
• Aluminum toxicity is an additional component that may be seen in patients undergoing dialysis.
• In children with chronic renal failure, the findings of rickets dominate, whereas in adults the findings of secondary hyperparathyroidism are more prominent.

Radiologic findings inRadiologic findings in RENAL OSTEODYSTROPHYRENAL OSTEODYSTROPHY
Combination of the findings of rickets, osteomalacia, secondary hyperparathyroidism, and osteoporosis
• Periosteal neostosis (lucency between the periosteum and subjacent bone) may be present.
– It is usually seen in asymmetric distribution in the metatarsals, femur, and pubic rami.

The differential diagnosis of The differential diagnosis of
RENAL OSTEODYSTROPHYRENAL OSTEODYSTROPHY
• Periosteal neostosis– hypertrophic osteoarthropathy,
osteomyelitis, or neoplasm.
• Soft tissue calcification– Collagen-vascular diseases, idiopathic
tumoral calcinosis, hydroxyapatite crystal deposition disease, and hypervitaminosis D.

RENAL OSTEODYSTROPHYRENAL OSTEODYSTROPHY
• The most common complications in patients with renal osteodystrophy are insufficiency fractures.
• In patients who have had renal transplantation, osteonecrosis, insufficiency fractures, tendinitis, and tendon ruptures are common.

Frog-lateral radiograph of the hip in a patient with osteonecrosis of the femoral head shows a characteristic subchondral
lucency ( arrow) and collapse of the femoral head.

PAGET'S DISEASEPAGET'S DISEASE

PAGET'S DISEASEPAGET'S DISEASE
• A common disorder of unknown etiology that is characterized by excessive and abnormal remodeling of bone.
• Men > women
• Age > 40 years.
• Polyostotic > monostotic.

PAGET'S DISEASEPAGET'S DISEASE
• Asymptomatic.• Bone pain, progressive bony enlargement,
bowing of long bones, or fractures at presentation.
• Deafness– from cranial-nerve compression at the skull base
or from middle-ear ossicle involvement.
• The spinal cord compressed – basilar invagination of the skull or enlargement of
the vertebrae.

Radiologic findings of PAGET'S DISEASEPAGET'S DISEASE
• Epiphyseal involvement with sharply demarcated lysis that advances down the diaphyses is quite specific.
• Three sequential stages may be seen: 1. Lytic; most common in skull and long bones.2. Mixed3. Sclerotic; typically involves the axial skeleton.
• The hallmarks of advanced Paget's disease are bone enlargement and increased bone sclerosis.
• Cortical and trabecular thickening and distortion are also frequently present.

Radiologic findings of PAGET'S DISEASEPAGET'S DISEASE
• Spine – M/C in lumbar region: picture-frame vertebra, ivory vertebra,
or compression fractures.
• Skull– Lytic phase, or osteoporosis circumscripta, usually begins in
the frontal or occipital bones.– More advanced disease in the skull manifests a cotton wool
appearance of mixed sclerosis and lysis.
• Pelvis– The earliest finding = thickening of the iliopectineal line.– Occasionally, patchy areas of lucency and sclerosis. – Protrusion deformity of the acetabula is a well-recognized
complication of advanced disease of the pelvis.

Radiologic findings of PAGET'S DISEASEPAGET'S DISEASE
• Long bones– Lysis of subarticular bone is seen initially.– A wedge of lucency down the diaphyses:
flame-shaped or blade-of-grass. – In the tibia, the lytic phase occasionally
begins in the diaphysis. – Advanced disease of the long bones is
characterized by coarsened trabecula, bony sclerosis, bony enlargement, and deformity.







A, Frontal radiograph of the pelvis in a patient with advanced Paget's disease shows bony enlargement, bone sclerosis, and trabecular disorganization involving the right femur, right
hemipelvis, and sacrum. B, Frontal radiograph of humerus in another patient with advanced Paget's disease shows bony enlargement, cortical and trabecular thickening, and trabecular disorganization.

Frontal radiograph of the femur in a patient with advanced Paget's disease shows bowing deformity of the femur along with bony enlargement, bone sclerosis, cortical
thickening, and trabecular disorganization.

Complications of
PAGET'S DISEASEPAGET'S DISEASE
• Basilar invagination
• Spinal stenosis
• Premature osteoarthritis
• Insufficiency fractures
• Osteomyelitis
• Neoplasms: osteosarcomas.
• Sarcomatous degeneration: common in patients with widespread disease

Frontal radiograph of the pelvis in a patient with widespread Paget's disease shows enlargement and cortical thickening of the pelvis. Additionally, there is an expansile lytic
lesion ( arrows) in the ischium, representing malignant degeneration of Paget's disease into fibrosarcoma.