Orofacial Candidiasis
21
OROFACIAL CANDIDIASIS
-
Upload
vidhi-thakur -
Category
Documents
-
view
49 -
download
0
description
candiasis
Transcript of Orofacial Candidiasis

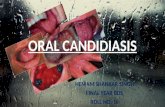
OROFACIAL CANDIDIASIS

Candidiasis is caused by a yeast like fungus candida albicans. Although other species such as C.tropicalis , C.parasilosis , C.glabrata and C.krusei may be invoved.
This microorganism is a relatively common inhabitant of oral cavity, git, vagina of clinically normal persons.
This disease is said to be the most oppurtunistic infection in the world.

• Its occurrence has remarkably increased since the prevaent use of antibiotics which destroy the normal inhibitory bacterial flora and immunosuppressive drugs like corticosteroids and cytotoxic drugs.
• In addition to affecting the oral cavity, monilial infection frequently involves the skin as well as git, vaginal tract, urinary tract and lungs.


CLINICAL FEATURES
• Candidal infection may range from mild superficial involvement to severe , fatal disseminated form seen in immunocompromised patients.
• Oral Candidiasis can be divided into 2 main categories


Pseudomembrane candidiasis
• This is the most common form of the disease and commonly called oral thrush.
• The oral cavity lesions are chaacterised by appearance of soft, white patches, mostly occurinf in buccal mucosa and tongue.The white patche consists of tangles masses og fungal hyphae with intermingled desquamated epithelium,keratin,fibrin, necrotic debris,leukocytes and bacteria.
• The white patch can be scraped off with a gauze piece leaving a raw bleeding erythematous area.



Erythematous Candidiasis
• Also known as antibiotic sore mouth• Usually occurs as sequalae to a course of
broad spectrum antibiotics, corticosteroids.• Lesion appears red. Redness is due to increased
vascularity and loss of filliform papillae on tongue
• Can be distinguished from erythroplakia by its diffused border in contrast to erythroplakia where borders are sharp and well demarcated.


Chronic hyperplastic candidiasis
• In this type, the oral lesions consist of firm, white, persistent plaques, usually on the lips, cheeks, tongue and appears similar to leukoplakia.
• The white plaques are due to hyperkeratosis and cannot be scraped off.The lesion may be homogenous or speckled.


Denture stomatitis and angular cheilitis
• Denture stomatitis is also known as denture sore mouth which occurs in patients wearing dentures for a lond period of time and poor oral hygiene.
• It is characterized by diffuse erythema and edema on the denture bearing area.
• Angular cheilitis also occurs mostly in edentulous patinets who have decreased vertical dimensions, resulting in chronic wetness at corner of the mouth and subsequent yeast growth.



diagnosis
• By clinical appearance and by detection of organism on smears.
• Smears are taken by gently drawing a wooden tongue depressor across lesion and is tranferred into a drop of KOH on a slide and examined under microscope for hyphae and blastospores.
• Cultures can also be grown on specifis media like sabouraud’s agar.

management

• Topical antifungal agents used commonly are nystatin and clotrimazola. Both are prepared as lozenges and are delivered by sucking till they get dissolved. They are used 4 to 5 times daily for 2 weeks.
• Treatement of denture involes thin layer og acrylic from internal surface and antiseptic soaks over night.

• Systemic administed new antifungals, such as fluconazole, ketoconazole and itraconazole are used to treat oropharyngeal candidiasis in immunocompromised individuals.
• Because of their expense and severe drug interactions, these are reserved for immunocompromised pateints.
• Another alternatives include amphotericin B.