
Original Article Vascular endothelial growth factor ... · Original Article Vascular endothelial...
10
Int J Clin Exp Pathol 2015;8(2):1165-1174 www.ijcep.com /ISSN:1936-2625/IJCEP0004039 Original Article Vascular endothelial growth factor receptor-2 inhibitor cediranib causes regression of endometriotic lesions in a rat model Fang Liu 1,2,3 , Li Wang 1,2,3 , Xian-Xia Zhang 1,2,3 , Shu-Yun Min 1,2,3 , Yi-Xuan Liu 1,2,3 , Zhi Zuo 1,2,3 , Zhi-Xing Jin 1,2,3 , Zhi-Ling Zhu 1,2,3 1 Obstetrics and Gynecology Hospital, Fudan University, 419 Fang-Xie Road, Shanghai 200011, PR China; 2 Department of Obstetrics and Gynecology of Shanghai Medical School, Fudan University, 138 Yi-Xueyuan Road, Shanghai 200032, PR China; 3 Shanghai Key Laboratory of Female Reproductive Endocrine Related Diseases, 413 Zhao-Zhou Road, Shanghai 200011, PR China Received November 21, 2014; Accepted January 28, 2015; Epub February 1, 2015; Published February 15, 2015 Abstract: Vascular endothelial growth factor (VEGF) receptor-2 plays an essential role in angiogenesis, and it also expressed in the glandular epithelium and stromal cells of ectopic endometrium. Cediranib is a protein tyrosine kinase inhibitor that potently inhibits VEGF receptor-2, but there is no study about its effects on the endometriosis. We induced endometriosis on both sides of the abdominal wall in 20 female Sprague-Dawley rats and randomly divided them into 2 groups. They were administered: cediranib 4 mg/kg/day (group 1), equal saline (group 2) for 12 days. Then, the lesion volumes were calculated, and Masson trichrome was used to detect fibrosis. Angiogenesis was evaluated by CD-31 immunohistochemistry and serum VEGF levels. Proliferation was indicated by proliferating cell nuclear antigen immunohistochemistry. Apoptosis was measured by a TUNEL assay and cleaved caspase-3 im- munohistochemistry. In the treatment group, the lesion volumes were smaller (P < 0.05), and the degree of fibrosis was greater. The microvessel density was lower (P < 0.05) than control, however, serum VEGF was up-regulated by a negative feedback mechanism (P < 0.01). In addition, proliferation was significantly suppressed (P < 0.01), and apoptosis in the lesions was more obvious in the treatment group. These data indicated that cediranib can inhibit development of endometriotic lesions in rats. Keywords: Angiogenesis, cediranib, endometriosis, vascular endothelial growth factor receptor-2 Introduction Endometriosis is defined as the appearance of endometrial glands and stroma outside the uterine cavity and is characterized by the pres- ence of chronic pelvic pain and infertility [1-3]. About 6%-10% reproductive women suffer from this disease [4]. Hypotheses about its patho- genesis include retrograde menstruation, dif- ferentiation of epithelium, immune dysfunction, genetic predisposition to the condition, and environmental causes [5, 6]. However, these hypotheses can only partly explain the occur- rence of endometriosis; the cause of endome- triosis in most patients still remains unknown. Furthermore, the side effects of traditional medicine and recurrence after operation result in additional treatment difficulties. Recently, it has become widely accepted that angiogenesis is necessary for the growth and survival of endometriotic lesions [7]. During laparoscopy, numerous peritoneal blood ves- sels are observed around active endometriotic lesions. Furthermore, among women with endo- metriosis, peritoneal fluid and endometrial vas- cular endothelial growth factor (VEGF) concen- trations are increased [8]. Angiogenesis has become a promising target candidate for future endometriosis therapy. VEGF and its receptors are major regulators in the formation of blood vessels. VEGF receptor-2 (VEGFR-2; KDR in humans, Flk-1 in mice) plays an essential role in angiogenesis during adult- hood and is the predominant mediator of VEGF- stimulated endothelial cell migration, prolifera- tion, survival, and enhanced vascular permea- bility [9]. Further study indicated this receptor was expressed not only in vascular endothelial cells but also in certain tumor cells, and its acti- vation can regulate cell proliferation, apoptosis,
-
Upload
dinhnguyet -
Category
Documents
-
view
221 -
download
0
Transcript of Original Article Vascular endothelial growth factor ... · Original Article Vascular endothelial...

Int J Clin Exp Pathol 2015;8(2):1165-1174www.ijcep.com /ISSN:1936-2625/IJCEP0004039
Original ArticleVascular endothelial growth factor receptor-2 inhibitor cediranib causes regression of endometriotic lesions in a rat model
Fang Liu1,2,3, Li Wang1,2,3, Xian-Xia Zhang1,2,3, Shu-Yun Min1,2,3, Yi-Xuan Liu1,2,3, Zhi Zuo1,2,3, Zhi-Xing Jin1,2,3, Zhi-Ling Zhu1,2,3
1Obstetrics and Gynecology Hospital, Fudan University, 419 Fang-Xie Road, Shanghai 200011, PR China;
2Department of Obstetrics and Gynecology of Shanghai Medical School, Fudan University, 138 Yi-Xueyuan Road, Shanghai 200032, PR China; 3Shanghai Key Laboratory of Female Reproductive Endocrine Related Diseases, 413 Zhao-Zhou Road, Shanghai 200011, PR China
Received November 21, 2014; Accepted January 28, 2015; Epub February 1, 2015; Published February 15, 2015
Abstract: Vascular endothelial growth factor (VEGF) receptor-2 plays an essential role in angiogenesis, and it also expressed in the glandular epithelium and stromal cells of ectopic endometrium. Cediranib is a protein tyrosine kinase inhibitor that potently inhibits VEGF receptor-2, but there is no study about its effects on the endometriosis. We induced endometriosis on both sides of the abdominal wall in 20 female Sprague-Dawley rats and randomly divided them into 2 groups. They were administered: cediranib 4 mg/kg/day (group 1), equal saline (group 2) for 12 days. Then, the lesion volumes were calculated, and Masson trichrome was used to detect fibrosis. Angiogenesis was evaluated by CD-31 immunohistochemistry and serum VEGF levels. Proliferation was indicated by proliferating cell nuclear antigen immunohistochemistry. Apoptosis was measured by a TUNEL assay and cleaved caspase-3 im-munohistochemistry. In the treatment group, the lesion volumes were smaller (P < 0.05), and the degree of fibrosis was greater. The microvessel density was lower (P < 0.05) than control, however, serum VEGF was up-regulated by a negative feedback mechanism (P < 0.01). In addition, proliferation was significantly suppressed (P < 0.01), and apoptosis in the lesions was more obvious in the treatment group. These data indicated that cediranib can inhibit development of endometriotic lesions in rats.
Keywords: Angiogenesis, cediranib, endometriosis, vascular endothelial growth factor receptor-2
Introduction
Endometriosis is defined as the appearance of endometrial glands and stroma outside the uterine cavity and is characterized by the pres-ence of chronic pelvic pain and infertility [1-3]. About 6%-10% reproductive women suffer from this disease [4]. Hypotheses about its patho-genesis include retrograde menstruation, dif-ferentiation of epithelium, immune dysfunction, genetic predisposition to the condition, and environmental causes [5, 6]. However, these hypotheses can only partly explain the occur-rence of endometriosis; the cause of endome-triosis in most patients still remains unknown. Furthermore, the side effects of traditional medicine and recurrence after operation result in additional treatment difficulties.
Recently, it has become widely accepted that angiogenesis is necessary for the growth and
survival of endometriotic lesions [7]. During laparoscopy, numerous peritoneal blood ves-sels are observed around active endometriotic lesions. Furthermore, among women with endo-metriosis, peritoneal fluid and endometrial vas-cular endothelial growth factor (VEGF) concen-trations are increased [8]. Angiogenesis has become a promising target candidate for future endometriosis therapy.
VEGF and its receptors are major regulators in the formation of blood vessels. VEGF receptor-2 (VEGFR-2; KDR in humans, Flk-1 in mice) plays an essential role in angiogenesis during adult-hood and is the predominant mediator of VEGF-stimulated endothelial cell migration, prolifera-tion, survival, and enhanced vascular permea-bility [9]. Further study indicated this receptor was expressed not only in vascular endothelial cells but also in certain tumor cells, and its acti-vation can regulate cell proliferation, apoptosis,
Cediranib causes regression of endometriotic lesions in a rat model
1166 Int J Clin Exp Pathol 2015;8(2):1165-1174
invasion, and migration [10]. Recently, it has been reported that VEGFR-2 may be expressed in vascular endothelial cells, endometrial glan-dular epithelium, and stroma cells [11, 12]. Research using animal models of endometrio-sis and endometriosis patients also indicated that VEGFR-2 is related to this disease [13-17].
Cediranib (AZD2171) is an orally bioavailable protein tyrosine kinase inhibitor for the treat-ment of cancer. It was found to potently inhibit VEGF-A-induced VEGFR-2 phosphorylation in human umbilical vein endothelial cells and
some tumor cells [18, 19]. Based on these facts, we used cediranib to treat endometriosis in rats and aimed to evaluate the effects of VEGFR-2 inhibition on peritoneal endometri- osis.
Materials and methods
Animals
Female Sprague-Dawley rats (6-8 weeks of age) were obtained from Slac Laboratory Animal Co. Ltd (Shanghai, China). Experimental ani-
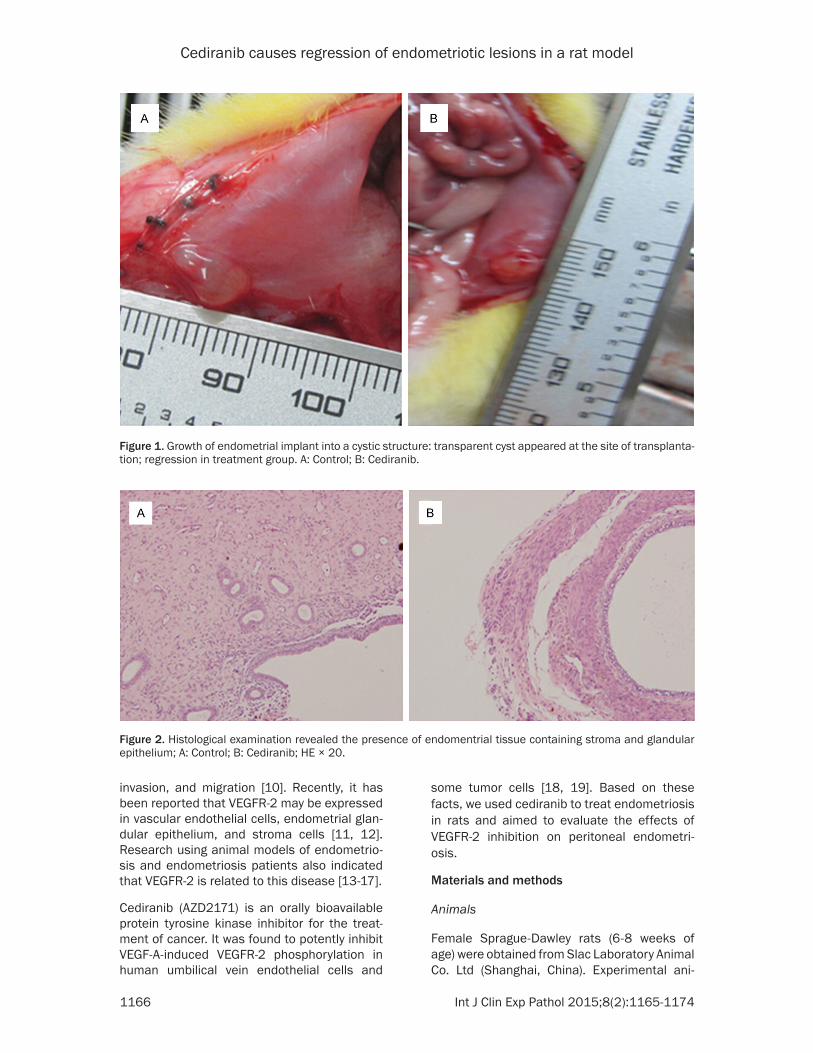
Figure 1. Growth of endometrial implant into a cystic structure: transparent cyst appeared at the site of transplanta-tion; regression in treatment group. A: Control; B: Cediranib.
Figure 2. Histological examination revealed the presence of endomentrial tissue containing stroma and glandular epithelium; A: Control; B: Cediranib; HE × 20.
Cediranib causes regression of endometriotic lesions in a rat model
1167 Int J Clin Exp Pathol 2015;8(2):1165-1174
mals, which were housed in groups of 5 per wire cage, were kept under standard laboratory conditions (12 hours of light, 12 hours of dark; 20-25°C) for 2 weeks to acclimatize to labora-tory conditions. Standard rat feed and water were provided ad libitum.
First surgery: inducing the animal models of endometriosis
Rats were anesthetized with intraperitoneal administration of 0.35 ml/100 mg 10% chloral-hydrate (Sinopharm, China). Before surgery, the abdominal skin was shaved, and antisepsis was obtained with 75% ethanol. A 1 cm ventral incision was made, and then 1 cm of the right
uterine horn was excised and placed in normal saline. Each uterine horn was cut along the lon-gitudinal axis, and then divided in half. Two squares of 5 × 5 mm open uterus were pre-pared. Then, the 2 squares were sutured to the inner surface of the abdominal wall (1 on each side), with the endometrium facing the perito-neal cavity, using a 6-0 nylon suture. After clos-ing the abdominal muscle and skin, 40,000 units/kg penicillin was injected into the mu- scle.
Treatment
Twenty-four days after the operation was per-formed, animals were randomly divided into 2
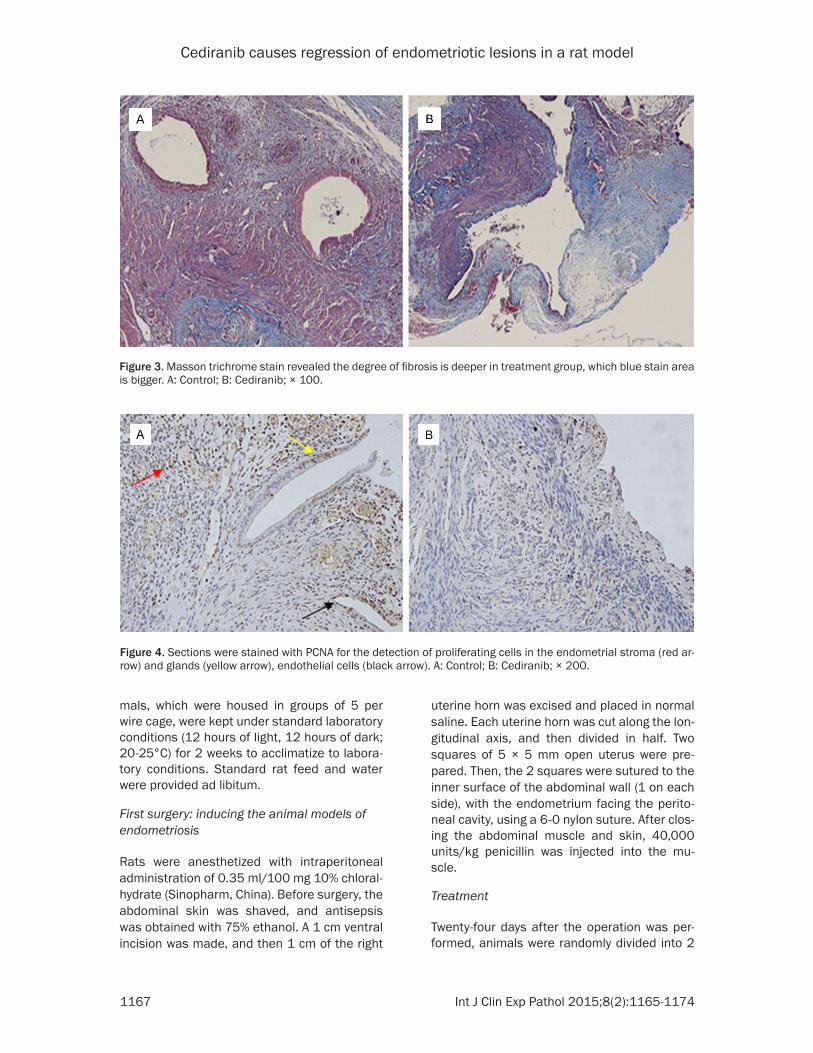
Figure 3. Masson trichrome stain revealed the degree of fibrosis is deeper in treatment group, which blue stain area is bigger. A: Control; B: Cediranib; × 100.
Figure 4. Sections were stained with PCNA for the detection of proliferating cells in the endometrial stroma (red ar-row) and glands (yellow arrow), endothelial cells (black arrow). A: Control; B: Cediranib; × 200.
Cediranib causes regression of endometriotic lesions in a rat model
1168 Int J Clin Exp Pathol 2015;8(2):1165-1174
different groups. Group 1 (10 rats) received 4 mg/kg cediranib (Selleck, USA) dissolved in DMSO and then diluted (1:200) in normal saline. Group 2 (10 rats) received the same amount of normal saline including an equal vol-ume of DMSO. The treatment was given by intragastric administration once daily for 12 days. The dose was determined based on a pre-vious study [20]. During the treatment, 2 rats in group 1 died from postoperative obstruction.
Second surgery: taking the implant samples
Rats were anesthetized with 10% chloralhy-drate, and then laparotomy was performed. During the operation, the implant volumes were calculated by measuring the dimensions and using the ellipsoid volume formula (π/6 × length × width × height). The investigator who mea-sured the dimensions was blinded with to the
treated rats and treatment. There were 11 endometriotic cysts in group 1 and 12 in group 2. After measurement, the implants, left uter-us, and both ovaries were excised, fixed in 4% paraformaldehyde (Sinopharm, China), and embedded in paraffin wax for histopathological examination. Blood was taken from the heart and centrifuged to get blood serum.
Histology of ovary and uterus
Tissues were fixed in 4% paraformaldehyde for a minimum of 12 hours and then embedded in paraffin and cut into 5-mm sections. The paraf-fin sections were stained with hematoxylin and eosin for microscopic observation.
Masson trichrome
Paraffin sections were deparaffinized in xylene and rehydrated through graded concentrations
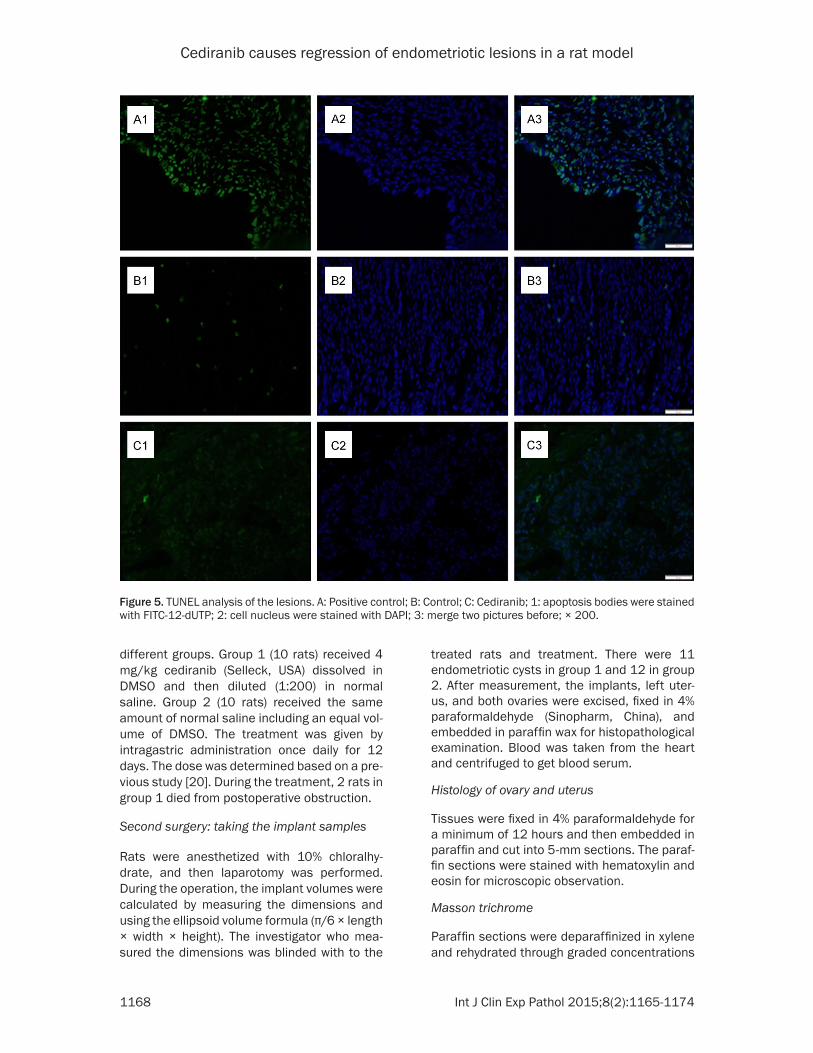
Figure 5. TUNEL analysis of the lesions. A: Positive control; B: Control; C: Cediranib; 1: apoptosis bodies were stained with FITC-12-dUTP; 2: cell nucleus were stained with DAPI; 3: merge two pictures before; × 200.

Cediranib causes regression of endometriotic lesions in a rat model
1169 Int J Clin Exp Pathol 2015;8(2):1165-1174
of ethanol. Sections were then stained with Masson trichrome.
Immunohistochemistry
Sections were deparaffinized in xylene and rehydrated through graded concentrations of ethanol. Antigen retrieval was performed by incubating the sections in 0.01 M citrate buffer (pH 6.0) and applying high microwave irradia-tion for 20 minutes. The slides were allowed to cool to room temperature, endogen peroxidase activity was inhibited with 3% H2O2 for 10 min-utes, and nonspecific binding was blocked with normal goat serum for 15 minutes at room tem-perature. The sections were further incubated with primary antibodies against CD31 (1:100, rabbit polyclonal; Wuhan Goodbio Technology CO., LTD, China), proliferating cell nuclear anti-gen (PCNA; 1:200, mouse monoclonal; Santa Cruz Biotechnology Inc., CA, USA), and cleaved caspase-3 (1:800, rabbit polyclonal; CST, USA) overnight at 4°C and then placed for 45 min-utes at room temperature. Slides were then
incubated with horseradish peroxidase-labeled secondary antibodies (1:200, anti-rabbit; KPL, USA; 1:100, anti-mouse and 1:200, anti-goat; Genentech, China) for 45 minutes at room tem-perature. Then, visualization of the antigens was achieved with diaminobenzidine. Finally, the slides were counterstained with hematoxy-lin, dehydrated, and mounted.
TUNEL assay
Terminal deoxynucleotidyl transferase-mediat-ed dUTP nick-end labeling (TUNEL) assay was performed using the In Situ Cell Death Detection Kit (Roche Company, Germany). Sections were deparaffinized and rehydrated as previously described. After washing with phosphate-buffered saline 3 times, all sections were incubated for 8 minutes in freshly pre-pared 0.1% Triton X-100 permeabilization solu-tion with 0.1% citrate buffer and then washed with phosphate-buffered saline. TUNEL TdT enzyme reaction mixture (50 µL) was added to each sample and incubated for 1 h in a humidi-
Figure 6. Sections were stained with cleaved caspase-3 for apoptosis of endometriotic lesions. A: Control, × 200; B: Cediranib, × 200; C: Control, × 400; D: Cediranib, × 400.
Cediranib causes regression of endometriotic lesions in a rat model
1170 Int J Clin Exp Pathol 2015;8(2):1165-1174
fying chamber at 37°C. Slides were then washed and observed under a fluorescence microscope.
ELISA
Blood samples were separated from heart blood and then centrifuged at 3,000 rpm for 15 minutes to separate serum. Serum VEGF was measured by enzyme-linked immune sorbent assay (ELISA) using the Rat VEGF ELISA kit (R&D System, USA), according to the manufac-turer’s instructions.
Statistical analysis
Immunohistochemical staining was scored by integrated optical density using Image Pro-plus 6.0.This analysis was performed in 5 visual fields from each section at x 200 magnification. Data were presented as the mean ± standard deviation. Differences were compared by inde-pendent sample t-test using SPSS software (version 17.0). A P value < 0.05 was considered statistically significant.
Results
Volumes of endometriotic cysts
During treatment, 2 rats in group 1 (received 4 mg/kg cediranib) died from postoperative obstruction. There were 11 endometriotic cysts in group 1 and 12 in group 2, because there
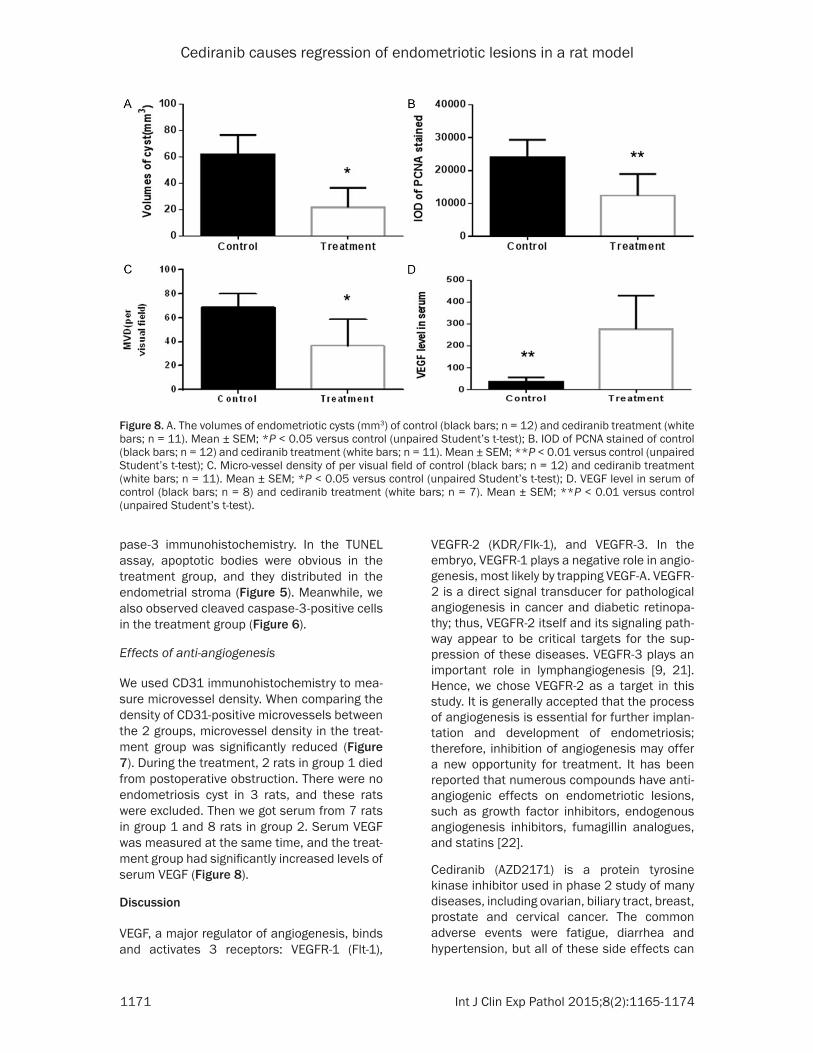
were no cysts formation on one side or both sides in some rats. All other uterine implants appeared as transparent cystic areas (Figure 1). Histological examination revealed the pres-ence of endometrial tissue containing stroma and glandular epithelium (Figure 2). The length, width, and height of cysts were measured using calipers and volumes were then calculated. Compared with the control group, lesions in the cediranib group were smaller, and this differ-ence was significant (P < 0.05).
Degree of fibrosis in endometriotic lesions
The results of Masson trichrome revealed that lesions from both groups were stained by blue pigments, but the area stained by blue pig-ments was larger in the cediranib group (Figure 3).
Proliferation and apoptosis of endometriotic lesions
To evaluate cell proliferation in the endometri-otic tissue, we stained for the proliferation marker PCNA. The stroma cells were predomi-nantly PCNA-positive in both groups. Compared with the control group, the number of PCNA-positive cells in the treatment group was signifi-cantly reduced (Figure 4). In addition, the prolif-eration index in the treatment group was signifi-cantly lower than that in the control group.
Apoptosis in the endometriotic lesions was assessed by TUNEL assay and cleaved cas-
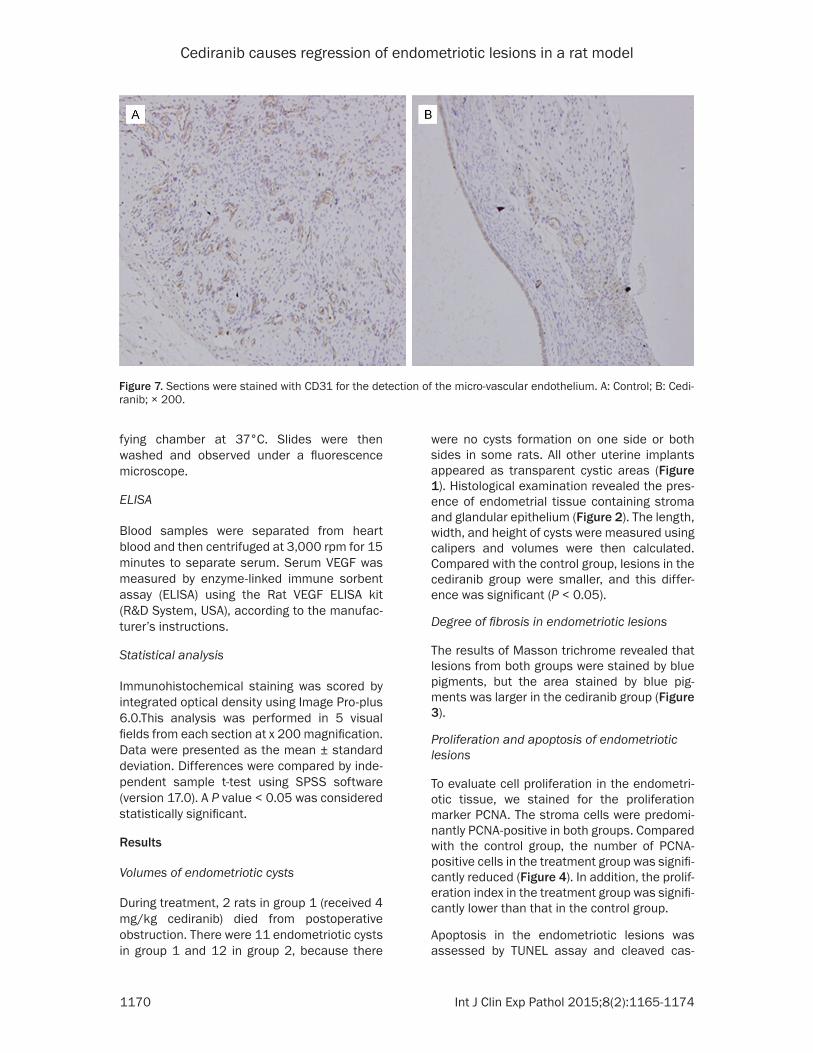
Figure 7. Sections were stained with CD31 for the detection of the micro-vascular endothelium. A: Control; B: Cedi-ranib; × 200.
Cediranib causes regression of endometriotic lesions in a rat model
1171 Int J Clin Exp Pathol 2015;8(2):1165-1174
pase-3 immunohistochemistry. In the TUNEL assay, apoptotic bodies were obvious in the treatment group, and they distributed in the endometrial stroma (Figure 5). Meanwhile, we also observed cleaved caspase-3-positive cells in the treatment group (Figure 6).
Effects of anti-angiogenesis
We used CD31 immunohistochemistry to mea-sure microvessel density. When comparing the density of CD31-positive microvessels between the 2 groups, microvessel density in the treat-ment group was significantly reduced (Figure 7). During the treatment, 2 rats in group 1 died from postoperative obstruction. There were no endometriosis cyst in 3 rats, and these rats were excluded. Then we got serum from 7 rats in group 1 and 8 rats in group 2. Serum VEGF was measured at the same time, and the treat-ment group had significantly increased levels of serum VEGF (Figure 8).
Discussion
VEGF, a major regulator of angiogenesis, binds and activates 3 receptors: VEGFR-1 (Flt-1),
VEGFR-2 (KDR/Flk-1), and VEGFR-3. In the embryo, VEGFR-1 plays a negative role in angio-genesis, most likely by trapping VEGF-A. VEGFR-2 is a direct signal transducer for pathological angiogenesis in cancer and diabetic retinopa-thy; thus, VEGFR-2 itself and its signaling path-way appear to be critical targets for the sup-pression of these diseases. VEGFR-3 plays an important role in lymphangiogenesis [9, 21]. Hence, we chose VEGFR-2 as a target in this study. It is generally accepted that the process of angiogenesis is essential for further implan-tation and development of endometriosis; therefore, inhibition of angiogenesis may offer a new opportunity for treatment. It has been reported that numerous compounds have anti-angiogenic effects on endometriotic lesions, such as growth factor inhibitors, endogenous angiogenesis inhibitors, fumagillin analogues, and statins [22].
Cediranib (AZD2171) is a protein tyrosine kinase inhibitor used in phase 2 study of many diseases, including ovarian, biliary tract, breast, prostate and cervical cancer. The common adverse events were fatigue, diarrhea and hypertension, but all of these side effects can
Figure 8. A. The volumes of endometriotic cysts (mm3) of control (black bars; n = 12) and cediranib treatment (white bars; n = 11). Mean ± SEM; *P < 0.05 versus control (unpaired Student’s t-test); B. IOD of PCNA stained of control (black bars; n = 12) and cediranib treatment (white bars; n = 11). Mean ± SEM; **P < 0.01 versus control (unpaired Student’s t-test); C. Micro-vessel density of per visual field of control (black bars; n = 12) and cediranib treatment (white bars; n = 11). Mean ± SEM; *P < 0.05 versus control (unpaired Student’s t-test); D. VEGF level in serum of control (black bars; n = 8) and cediranib treatment (white bars; n = 7). Mean ± SEM; **P < 0.01 versus control (unpaired Student’s t-test).

Cediranib causes regression of endometriotic lesions in a rat model
1172 Int J Clin Exp Pathol 2015;8(2):1165-1174
be manageable [20, 23]. To the best of our knowledge, this is the first study investigating the effect of cediranib on surgically induced endometriosis in rats.
In the present study, we demonstrated that treatment with cediranib significantly reduced lesion size, and development of endometriosis was severely decreased as a consequence. These results are in agreement with previous research which used similar drugs, such as sorafenib and sunitinib [24, 25]. Furthermore, we observed that cediranib treatment resulted in the reduction of microvessel density in experimental animals. This indicated that inhi-bition of angiogenesis may lead to regression of lesion size, which was previously proposed in many studies [26-28]. In our study, the VEGF level in serum increased significantly. This can be explained by a negative feedback mecha-nism. Cediranib inhibits the activation of VE- GFR-2, and then more VEGF stimulation is needed to meet the requirement of vascular endothelial cells growth. However, the extent of receptor inhibition was greater than the extent of VEGF elevation. Unfortunately, we only mea-sured serum VEGF levels and did not assess levels in peritoneal fluid and endometriotic lesions.
Endometriosis is characterized by fibrous tis-sue surrounding the endometrial glands and stroma [29]. Excess fibrosis may lead to scar-ring, adhesion, chronic pain, and altered tissue function [30]. Some scholars have suggested anti-fibrosis treatment as a new endometriosis therapy [31, 32]. In our study, there was greater extent of fibrosis after treatment, but we did not observe severe adhesion during the prog-ress of the second operation. We considered this fibrosis resulted from hypoxia due to inhibi-tion of angiogenesis. This was consistent with fibrosis occurring in ischemic kidney injury [33, 34].
Cediranib treatment has also been shown to have an effect on the proliferative activity of endometriotic lesions. We found significantly fewer PCNA-positive cells in the treatment group than in the control group. However, most PCNA-positive cells were stromal cells in both groups, and few glandular cells were stained. In the TUNEL assay, we found more apoptotic bodies in the treatment group than in the con-trol group, and they were mainly distributed in
endometriotic stromal cells. Furthermore, we detected cleaved caspase-3; activation of cas-pase-3 plays a critical role in the regulation of cell apoptosis. It is known that hypoxia can induce many types of cellular apoptosis [35, 36]. Cediranib inhibited microvessel formation, resulting in tissue hypoxia. At the same time, it has already demonstrated that in vascular endothelial cells and some tumor cells, activa-tion of VEGFR-2 can activate Erk1/2 and p38 to regulate cell proliferation and migration [9, 10]. In our research, we found glandular cells and parts of stromal cells also expressed VEGFR-2, consistent with previous research [11, 12]. An in vitro study is needed to confirm the direct effects of this receptor on endometriotic cells.
In summary, we demonstrated that cediranib caused regression of endometriotic implants in rat models. This was associated with a decrease in microvessel density and prolifera-tive activity and an increase in fibrosis and apoptosis. The mechanism of this drug was previously unclear. Further studies are needed to clarify the direct and indirect effects of this drug on endometriotic cells and angiogenesis. In addition, using rat model with auto-trans-planted uterine tissue is the limitation of our research. There must be some difference between the rats and endometriosis women. Transplanting endometriosis lesion from patients to nude mice may be a better model to further study.
Acknowledgements
This study was supported by the Shanghai Committee of Science and Technology (Grant Number: 12401902200).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Zhi-Ling Zhu, Obstetrics and Gynecology Hospital, Fudan University, 419 Fang-Xie Road, Shanghai 200011; Department of Obstetrics and Gynecology of Shanghai Medical School, Fudan University, 138 Yi-Xueyuan Road, Shanghai 200032; Shanghai Key Laboratory of Female Reproductive Endocrine Related Diseases, 413 Zhao-Zhou Road, Shanghai 200011, PR China. E-mail: [email protected]
References
[1] Rogers PA, D’Hooghe TM, Fazleabas A, Gargett CE, Giudice LC, Montgomery GW, Rombauts L,
Cediranib causes regression of endometriotic lesions in a rat model
1173 Int J Clin Exp Pathol 2015;8(2):1165-1174
Salamonsen LA, Zondervan KT. Priorities for endometriosis research: Recommendations from an international consensus workshop. Reprod Sci 2009; 16: 335-46.
[2] Rogers PA, D’Hooghe TM, Fazleabas A, Giudice LC, Montgomery GW, Petraglia F, Taylor RN. Defining future directions for endometriosis re-search: workshop report from the 2011 World Congress of Endometriosis In Montpellier, France. Reprod Sci 2013; 20: 483-99.
[3] Giudice LC. Clinical practice. Endometriosis. N Engl J Med 2010; 362: 2389-2398.
[4] Eskenazi B, Warner ML. Epidemiology of endo-metriosis. Obstet Gynecol Clin North Am 1997; 24: 235-258.
[5] Nap AW, Groothuis PG, Demir AY, Evers JL, Dunselman GA. Pathogenesis of endometrio-sis. Best Pract Res Clin Obstet Gynecol 2004; 18: 233-244.
[6] Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril 2012; 98: 511-9.
[7] Groothuis PG, Nap AW, Winterhager E, Grü- mmer R. Vascular development in endometrio-sis. Angiogenesis 2005; 8: 147-56.
[8] Rocha AL, Reis FM, Taylor RN. Angiogenesis and endometriosis. Obstet Gynecol Int 2013; 2013: 859619.
[9] Roskoski R Jr. VEGF receptor protein-tyrosine kinases: structure and regulation. Biochem Biophys Res Commun 2008; 375: 287-91.
[10] Patyna S, Laird AD, Mendel DB, O’farrell AM, Liang C, Guan H, Vojkovsky T, Vasile S, Wang X, Chen J, Grazzini M, Yang CY, Haznedar JO, Sukbuntherng J, Zhong WZ, Cherrington JM, Hu-Lowe D. SU14813: a novel multiple recep-tor tyrosine kinase inhibitor with potent antian-giogenic and antitumor activity. Mol Cancer Ther 2006; 5: 1774-82.
[11] Machado DE, Abrao MS, Berardo PT, Takiya CM, Nasciutti LE. Vascular density and distri-bution of vascular endothelial growth factor (VEGF) and its receptor VEGFR-2 (Flk-1) are significantly higher in patients with deeply infil-trating endometriosis affecting the rectum. Fertil Steril 2008; 90: 148-55.
[12] Bourlev V, Volkov N, Pavlovitch S, Lets N, Larsson A, Olovsson M. The relationship be-tween microvessel density, proliferative activity and expression of vascular endothelial growth factor-A and its receptors in eutopic endome-trium and endometriotic lesions. Reproduction 2006; 132: 501-9.
[13] Fainaru O, Adini A, Benny O, Adini I, Short S, Bazinet L, Nakai K, Pravda E, Hornstein MD, D’Amato RJ, Folkman J. Dendritic cells support angiogenesis and promote lesion growth in a murine model of endometriosis. FASEB J 2008; 22: 522-9.
[14] Machado DE, Berardo PT, Palmero CY, Nasciutti LE. Higher expression of vascular endothelial growth factor (VEGF) and its receptor VEGFR-2 (Flk-1) and metalloproteinase-9 (MMP-9) in a rat model of peritoneal endometriosis is simi-lar to cancer diseases. J Exp Clin Cancer Res 2010; 29: 1-9.
[15] Kang S, Shi YY, Li Y, Wang N, Lu YC, Zhou RM, Zhao XW. Association between Genetic Variants of the VEGFR-2 Gene and the Risk of Developing Endometriosis in Northern Chinese Women. Gynecol Obstet Invest 2013; 76: 32-7.
[16] Kim CH, Ahn JW, Kim SH, Chae HD, Kang BM. Effects on in vitro fertilization-embryo transfer outcomes of vascular endothelial growth fac-tor receptor-1, -2 and -3 in eutopic endometrial tissue of women with endometriosis. J Obstet Gynaecol Res 2011; 37: 1631-7.
[17] Novella-Maestre E, Carda C, Ruiz-Sauri A, Gar- cia-Velasco JA, Simon C, Pellicer A. Identification and quantification of dopamine receptor 2 in human eutopic and ectopic endometrium: a novel molecular target for endometriosis ther-apy. Biol Reprod 2010; 83: 866-73.
[18] Wedge SR, Kendrew J, Hennequin LF, Valentine PJ, Barry ST, Brave SR, Smith NR, James NH, Dukes M, Curwen JO, Chester R, Jackson JA, Boffey SJ, Kilburn LL, Barnett S, Richmond GH, Wadsworth PF, Walker M, Bigley AL, Taylor ST, Cooper L, Beck S, Jürgensmeier JM, Ogilvie DJ. AZD2171: a highly potent, orally bioavailable, vascular endothelial growth factor receptor-2 tyrosine kinase inhibitor for the treatment of cancer. Cancer Res 2005; 65: 4389-400.
[19] Kendrew J, Odedra R, Logié A, Taylor PJ, Pearsall S, Ogilvie DJ, Wedge SR, Jürgensmeier JM. Anti-tumour and anti-vascular effects of cediranib (AZD2171) alone and in combination with other anti-tumour therapies. Cancer Chemother Pharmacol 2013; 71: 1021-32.
[20] Sahade M, Caparelli F, Hoff PM. Cediranib: a VEGF receptor tyrosine kinase inhibitor. Future Oncol 2012; 8: 775-81.
[21] Shibuya M. Differential roles of vascular endo-thelial growth factor receptor-1 and receptor-2 in angiogenesis. J Biochem Mol Biol 2006; 39: 469-78.
[22] Laschke MW, Menger MD. Anti-angiogenic treatment strategies for the therapy of endo-metriosis. Hum Reprod Update 2012; 18: 682-702.
[23] Liu JF, Barry WT, Birrer M, Lee JM, Buckanovich RJ, Fleming GF, Rimel B, Buss MK, Nattam S, Hurteau J, Luo W, Quy P, Whalen C, Obermayer L, Lee H, Winer EP, Kohn EC, Ivy SP, Matulonis UA. Combination cediranib and olaparib ver-sus olaparib alone for women with recurrent platinum-sensitive ovarian cancer: a random- ised phase 2 study. Lancet Oncol 2014; 15: 1207-14.

Cediranib causes regression of endometriotic lesions in a rat model
1174 Int J Clin Exp Pathol 2015;8(2):1165-1174
[24] Ozer H, Boztosun A, Açmaz G, Atilgan R, Akkar OB, Kosar MI. The efficacy of bevacizumab, sorafenib, and retinoicacid on rat endometrio-sis model. Reprod Sci 2013; 20: 26-32.
[25] Abbas MA, Disi AM, Taha MO. Sunitinib as an anti-endometriotic agent. Eur J Pharm Sci 2013; 49: 732-6.
[26] Onalan G, Zeyneloglu HB, Bayraktar N. Fenofibrate causes regression of endometriot-ic implants:a rat model. Fertil Steril 2009; 92: 2100-2.
[27] Rudzitis-Auth J, Menger MD, Laschke MW. Resveratrol is a potent inhibitor of vasculariza-tion and cell proliferation in experimental en-dometriosis. Hum Reprod 2013; 28: 1339-47.
[28] Xu H, Lui WT, Chu CY, Ng PS, Wang CC, Rogers MS. Anti-angiogenic effects of green tea cate-chin on an experimental endometriosis mouse model. Hum Reprod 2009; 24: 608-18.
[29] Giudice LC, Kao LC. Endometriosis. Lancet 2004; 364: 1789-99.
[30] Matsuzaki S, Canis M, Darcha C, Dechelotte P, Pouly JL, Bruhat MA. Fibrogenesis in peritoneal endometriosis: A semi-quantitative analysis of type-I collagen. Gynecol Obstet Invest 47: 197-199.
[31] Matsuzaki S, Darcha C. Antifibrotic properties of epigallocatechin-3-gallate in endometriosis. Hum Reprod 2014; 29: 1677-87.
[32] Matsuzaki S, Darcha C. Involvement of the Wnt/β-catenin signaling pathway in the cellu-lar and molecular mechanisms of fibrosis in endometriosis. PLoS One 2013 4; 8: e76808.
[33] Sun S, Ning X, Zhai Y, Du R, Lu Y, He L, Li R, Wu W, Sun W, Wang H. Egr-1 Mediates Chronic Hypoxia-Induced Renal Interstitial Fibrosis via the PKC/ERK Pathway. Am J Nephrol 2014; 39: 436-48.
[34] Kapitsinou PP, Sano H, Michael M, Kobayashi H, Davidoff O, Bian A, Yao B, Zhang MZ, Harris RC, Duffy KJ, Erickson-Miller CL, Sutton TA, Haase VH. Endothelial HIF-2 mediates protec-tion and recovery from ischemic kidney injury. J Clin Invest 2014; 124: 2396-409.
[35] Gao W, Ferguson G, Connell P, Walshe T, O’Brien C, Redmond EM, Cahill PA. Glucose at-tenuates hypoxia-induced changes in endothe-lial cell growth by inhibiting HIF-1α expression. Diab Vasc Dis Res 2014; 11: 270-280.
[36] Carmeliet P, Dor Y, Herbert JM, Fukumura D, Brusselmans K, Dewerchin M, Neeman M, Bono F, Abramovitch R, Maxwell P, Koch CJ, Ratcliffe P, Moons L, Jain RK, Collen D, Keshert E. Role of HIF-1alpha in hypoxia-mediated apoptosis, cell proliferation and tumour angio-genesis. Nature 1998; 394: 485-90.


















