Orientated foam sclerosis
19
55 ORIENTATED FOAM SCLEROTHERAPY (OFS) A new safe and effective method treating G.S Varicose Veins Altarazi Louay M.D Damascus - Syria
-
Upload
uvcd -
Category
Presentations & Public Speaking
-
view
145 -
download
1
Transcript of Orientated foam sclerosis
55
ORIENTATED FOAM SCLEROTHERAPY (OFS)
A new safe and effective method treating G.S Varicose Veins
Altarazi Louay M.DDamascus-Syria

Methods Advantages Disadvantages
Surgery •More than 50 years experience
•Well known long term results
•Aggressive
•Late return to activity and work
Thermal endovenous
..ablation:
•Laser
• RFO
• hyperheated steam
•Minimally aggressive
•Easy to learn
•rapid ambulation
•Early return to work
•Good medium term results
•Expensive
•Treat only GSV main trunk but not
..junction and tributaries incontinence
• not for large, superficial&tortuous veins
•Frequent mild complications&suffering
Liquid sclerotherapy •No anesthesia
•Easy outpatient procedure
• relatively safe
•Needs large doses of sclerosing agents
•mild efficacy
•Moderate medium term results
Ultrasounds guided
Foam sclerotherapy
•Good short term results
•Easy outpatient procedure
•Rare but serious complications
•Instable efficacy
Orientated foam
sclerotherapy (OFC)
Eventually; best efficacy for all
GSV varicose veins types
immediate ambulation&comfort
•Inexpensive
•Eventually; rare mild complications
• needs fluroscopy device & experience
•Waiting for long term results
looking for an ideal GSV reflux treatment

3/5/2015 3
OFC Aim
Orientated GSV Foam Sclerotherapy
• beginning with clinical and ultrasonographic reflux cartography and marking
•All the cases undertaken by the same vascular surgery team
•Procedures took places in a fluroscopy and ultrasonography equipped
…theater preferably on a tilting radio transparent table.
•No premedication but occasionally some sedative for anxious women
•Post op padding and tow layers bandage stoking compression for 5-7 days
•Patient walks for 10 minutes around the treatment center before discharge
…and is advised to walk a lot the first week.
•No post-op Aspirin or Warferin, no systematic heparin, LMWH single dose
…post op in older, immobile, thrombophilic and phlebitic antecedents patients
•1 month,6 months,1 year,2 years and as needed review appointments
Methods generalities:
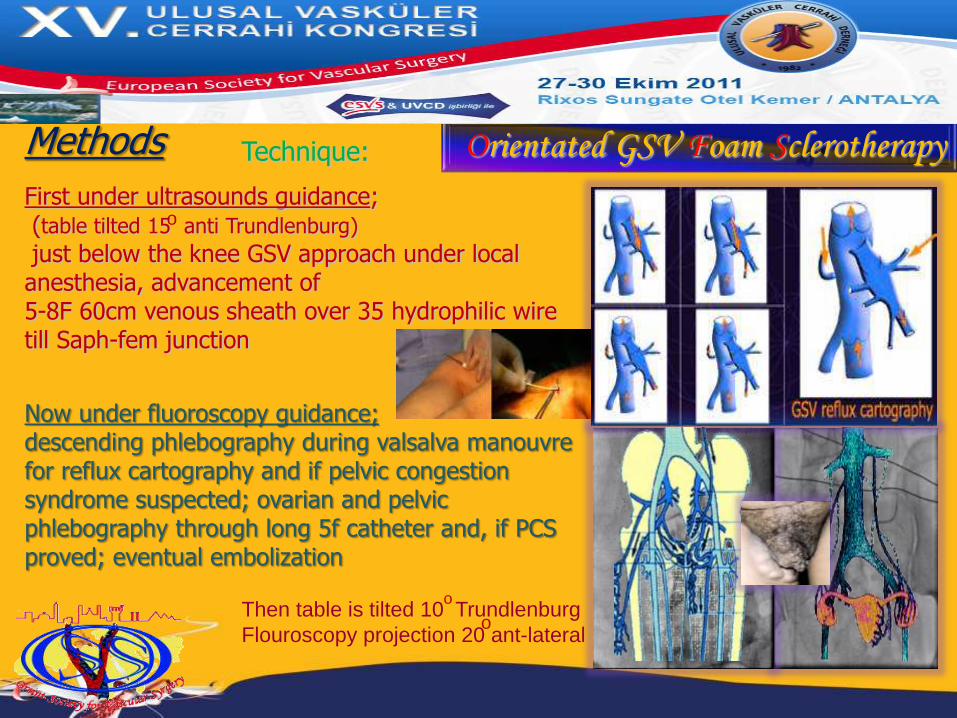
Then table is tilted 10 Trundlenburg
Flouroscopy projection 20 ant-lateral
First under ultrasounds guidance;(table tilted 15 anti Trundlenburg)
just below the knee GSV approach under local anesthesia, advancement of 5-8F 60cm venous sheath over 35 hydrophilic wire till Saph-fem junction
Now under fluoroscopy guidance;descending phlebography during valsalva manouvrefor reflux cartography and if pelvic congestion syndrome suspected; ovarian and pelvic phlebography through long 5f catheter and, if PCS proved; eventual embolization
Methods
o
o
Orientated GSV Foam SclerotherapyTechnique:
o

Orientated GSV Foam Sclerotherapy
Orientated GSV Foam Sclerotherapy
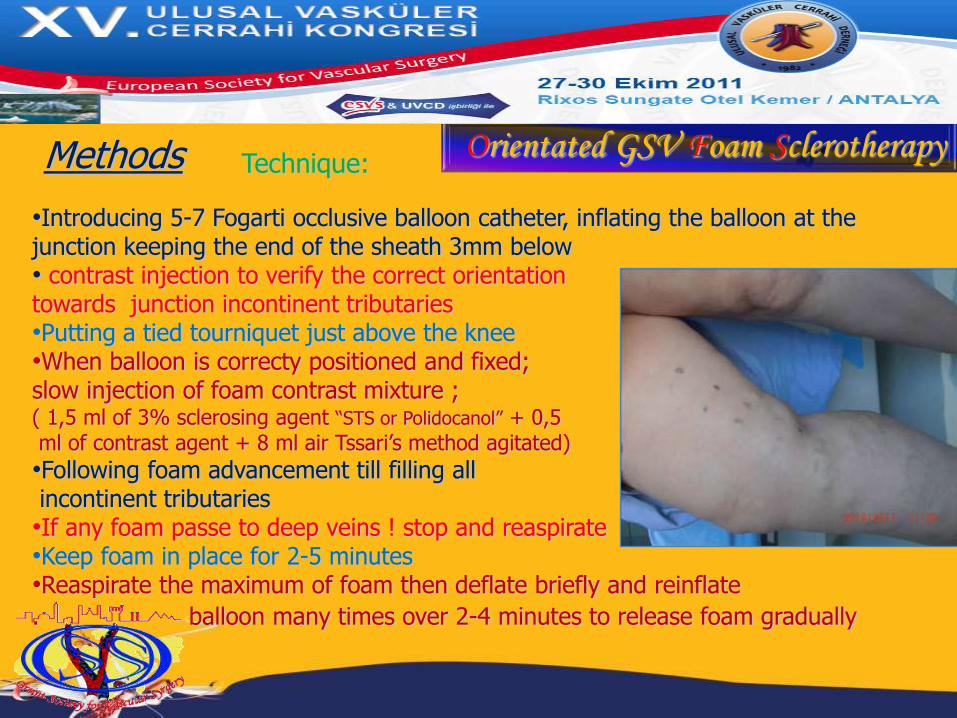
•Introducing 5-7 Fogarti occlusive balloon catheter, inflating the balloon at the junction keeping the end of the sheath 3mm below • contrast injection to verify the correct orientation towards junction incontinent tributaries•Putting a tied tourniquet just above the knee•When balloon is correcty positioned and fixed; slow injection of foam contrast mixture ;( 1,5 ml of 3% sclerosing agent “STS or Polidocanol” + 0,5ml of contrast agent + 8 ml air Tssari’s method agitated)
•Following foam advancement till filling allincontinent tributaries•If any foam passe to deep veins ! stop and reaspirate•Keep foam in place for 2-5 minutes•Reaspirate the maximum of foam then deflate briefly and reinflate
. balloon many times over 2-4 minutes to release foam gradually
Methods Technique:

catheter
balloon
Six months later
Orientated GSV Foam Sclerotherapy

Orientated GSV Foam Sclerotherapy
Difficult case;
Huge Greater Saphenous Vein; 13 mm at knee.
Sever venous spasm. Atypical anatomy. Tortuous and
aneurismal dilatation. Huge groin tributaries.
Deep femoral vein incontinence. Insufficient equipment
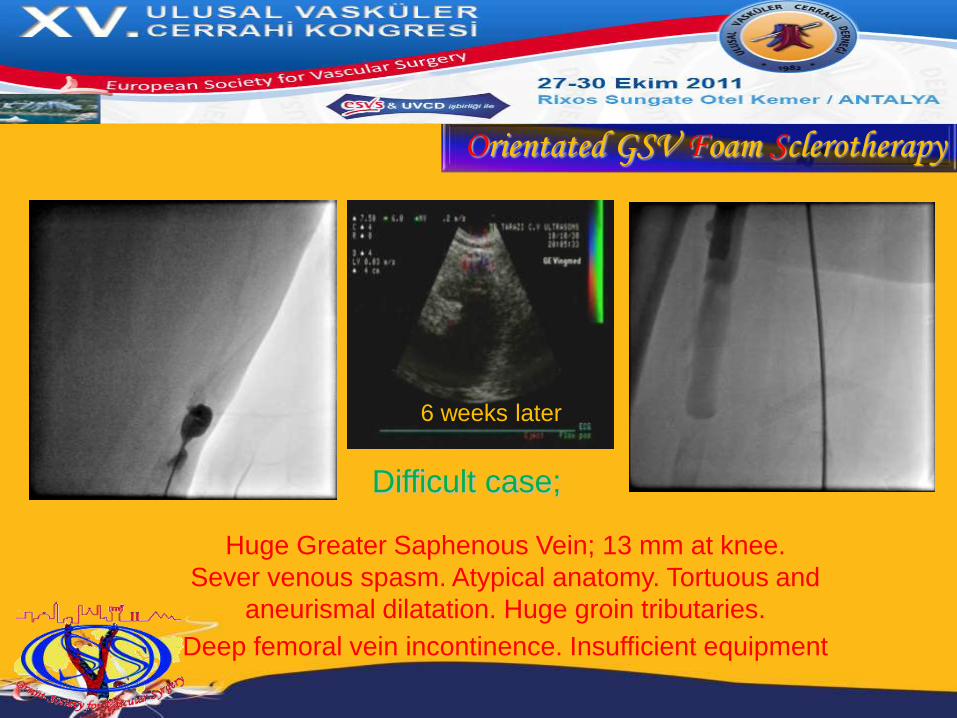
6 weeks later
Orientated GSV Foam Sclerotherapy
Difficult case;
Huge Greater Saphenous Vein; 13 mm at knee.
Sever venous spasm. Atypical anatomy. Tortuous and
aneurismal dilatation. Huge groin tributaries.
Deep femoral vein incontinence. Insufficient equipment

Bilateral case;
RGSV , LGSV+LAAGSV
Before After
AAV
GSV
CFA
LCFV
Orientated GSV Foam Sclerotherapy

Bilateral case;
RGSV , LGSV+LAAGSV
AAV
GSV
CFA
LCFV
Before After
Orientated GSV Foam Sclerotherapy
Orientated GSV Foam Sclerotherapy
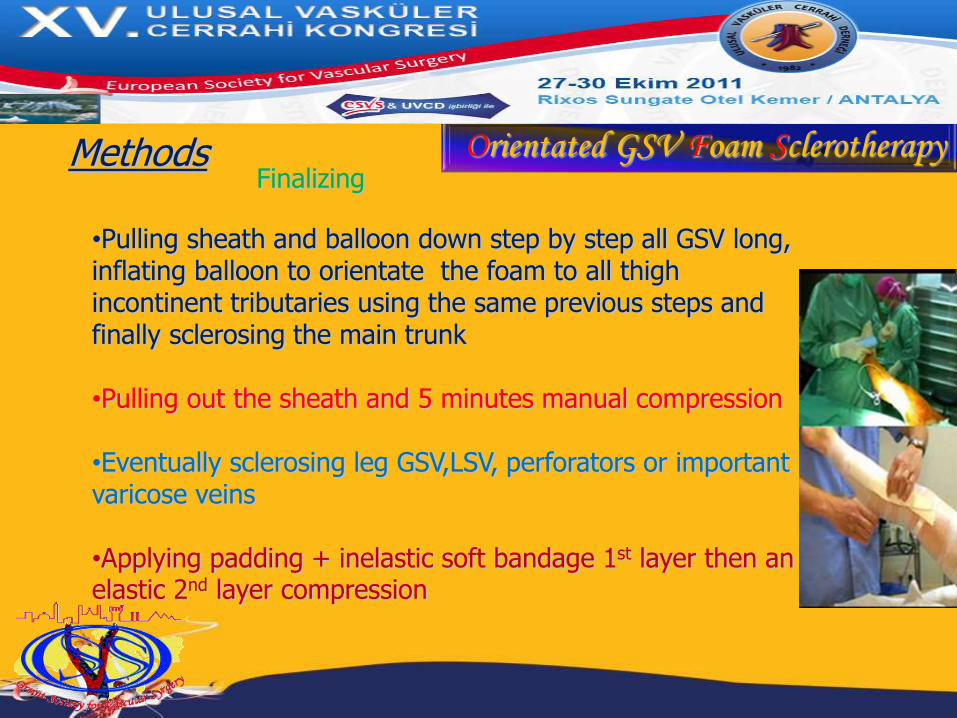
•Pulling sheath and balloon down step by step all GSV long, inflating balloon to orientate the foam to all thigh incontinent tributaries using the same previous steps and finally sclerosing the main trunk
•Pulling out the sheath and 5 minutes manual compression
•Eventually sclerosing leg GSV,LSV, perforators or important varicose veins
•Applying padding + inelastic soft bandage 1st layer then an elastic 2nd layer compression
FinalizingMethods

Orientated GSV Foam Sclerotherapy
Between Mars 2008 and June 2011:42 patients (48 legs: 6 bilateral) underwent OFS for GSV varicose veins
Associated simultaneous procedures:• 7 small incision to expose spasmodic GSV • 5 LSV and 4 perforators sclerosis• 6 pelvic congestion syndrome and 1 varicocele embolizsation
Late procedures:• 5 clots aspiration, 1 entry point tiny abscess incision,• 6 complimentary leg small varicose veins sclerosis
Methods
•Procedure time average is 21m (for the last ten cases associated
procedures excluded)
•3% sclerosing agent average dose is 4.5ml (1,5 - 8)
Orientated GSV Foam Sclerotherapy
• Out of 34 legs duplex controlled for more than 1 year, 31 show
complete occlusion of GSV, tributaries and junction till the CFV witch keeps a normal aspect with no deformity or bulging thrombus
• one AASV recurrence (continent AASV and junction were not treated, only `GSV trunk and PCS were sclerosed)
•One atypical lateral thigh recurrence due to omitted PVC
• development of one continent 3.5mm diameter vein parallel and more superficial to the occluded GSV ending in the EIV
Results:
Orientated GSV Foam SclerotherapyComplications: 6 superficial phlebitis1 small entry point abscess ,3 mild transient feverno general, D.V.T, P.E, neurological or optical complicationsno serious pain or discomfort
The rarity of complications may due to• Minimal sclerosing agent dose, can be mostly re aspirated• Under fluoroscopy control; foam passage to CFV or deep FV
(Through perforators) can be easily detected & stopped•Gradual slow release of tiny foam quantities
Orientated GSV Foam SclerotherapyAdvantages ; (OFS )•As effective as surgery and laser,RFO therapy – probably more (due to
..prolonged foam contact with vein wall) •Can treat tortuous, superficial & large GSVs (diameter more than 10 mm)
•Can realize continuous reflux cartography •Can treat eventual PCS or varicocele at the same time
•Can deal with incontinent collaterals selectively •Can occlude the hole junction (VS Laser-RFO)
•Far less expensive•No tumescent anesthesia, no incision, outpatient procedure.
•Can deal with incontinent LSV and perforators at the same scene •Patients walk home, continue to work normally
•Excellent patient comfort and satisfaction•Few contraindications (pregnancy, contrast allergy, renal failure)
•Extremely rare complications
Orientated GSV Foam SclerotherapyConclusion
Looking for a safe, durable and highly cost effective treatment for GSV varicose veins;
(OFS) is associated with an excellent medium term results and extremely low complications and
recurrence rate
it must be encouraged and be subjectto further trails and evaluation.

Marvelous south Egypt
Petra, rock sculpted old city
Istanbul, Orient’s gate
Esfahan = half of the world
Damascus
World oldest
Inhabited
Capital
EX ORIENT LUX