Oral Orthopedicsand Movementof Maxillary Segments ...
6
Oral Orthopedics and Movement of Maxillary Segments A Roentgen Stereophotogrammetric Study BODIL RUNE, D.D.S. KARL-VICTOR SARNAS, D.D.S. GORAN SELVIK, M.D. Lund, Swedgn An infant with a complete unilateral cleft of the lip and palate underwent maxillary expansion treatment using an oral orthopedic appliance. Movement of the maxillary bone segments was studied by means of metallic implants and roentgen stereophotogrammetry, and intra-oral changes were recorded by measuring transverse dimensions on casts. Expansion treatment had almost no influence on the positions of the maxillary segments, and movements of the segments showed little agreement with measures on casts. The findings suggest that the appropriate use of the term oral orthopedics and the evaluation of treatment effects would benefit from evaluating the movement of the segments by methods other than measurements of casts. Introduction "Oral orthopedics" is a term used "to con- vey that a different type of movement is achieved by certain appliances, i.e. a move- ment of the entire jaw segment, tooth, bone and soft tissues, as one unit," (Robertson and Hilton, 1971). Treatment results have been evaluated mainly by measuring series of casts to determine intra-oral changes (Huddart, 1961; Graber, 1964; Huddart, 1967; Neuman, 1967; Robertson and Hilton, 1971; Huddart, 1974; Robertson and Fish, 1975; Robertson, Shaw, and Volp, 1977; Shaw, 1978). Mea- surement points are poorly defined, however, and are difficult to identify because of rapid changes in surface morphology and tooth eruption. Besides, appositional growth and remodelling disguises displacement of the bone segments. Movements of the segments can not, therefore, be accurately identified by means of surface measurement points. To obtain identifiable measurement points in the infant maxilla, metallic implants have been inserted and used as bone markers in a few roentgen studies (Robertson, and Hilton, 1968; Robertson, 1971; Robertson and Hil- Dr. Rune is Orthodontist at the Center for Craniofa- cial Anomalies, General Hospital, Malmo, Sweden and Dr. Sarnas is Orthodontist and Head of the Center at the same hospital. Dr. Selvik is Assistant Professor at the Department of Anatomy, University of Lund, Lund. The study was supported by grants from Segerfalks Foundation, Helsingborg. ton, 1971; Robertson, Shaw, and Volp, 1977; Shaw, 1978). Implant stability, however, was not ascertained in the two-dimensional coor- dinate systems, and Shaw (1977) stated that the implant technique "is of limited value since the implants may be disturbed by the developing teeth and because slight inaccu- racy in head positioning may lead to substan- tial errors of interpretation." Since exact methods for recording move- ment of the maxillary bone segments in in- fants have been unavoidable, it has been im- possible to verify the claims which have been made relative to the effects of oral orthope- dics. With a recently developed roentgen ster- eophotogrammetric method (Selvik, 1974) based on the use of metallic implants, move- ment between bone segments is recorded three-dimensionally. Implant stability is checked with a high degree of accuracy, and the need for identical head positioning is elim- inated (Rune et al., 1977 a; Rune et al., 1977 b). In the present study this method was used to record movement of the maxillary bone segments in an infant who underwent oral orthopedic treatment prior to primary palate repair. Materials and Methods The study concerns a girl with a complete cleft of the lip and palate on the right side. Surgical treatment included primary lip clo- 385
Transcript of Oral Orthopedicsand Movementof Maxillary Segments ...

Oral Orthopedics and Movement of Maxillary Segments
A Roentgen Stereophotogrammetric Study
BODIL RUNE, D.D.S.
KARL-VICTOR SARNAS, D.D.S.
GORAN SELVIK, M.D.Lund, Swedgn
An infant with a complete unilateral cleft of the lip and palate underwent maxillary
expansion treatment using an oral orthopedic appliance. Movement of the maxillary
bone segments was studied by means of metallic implants and roentgen stereophotogrammetry,
and intra-oral changes were recorded by measuring transverse dimensions on casts.
Expansion treatment had almost no influence on the positions of the maxillary segments,
and movements of the segments showed little agreement with measures on casts. The
findings suggest that the appropriate use of the term oral orthopedics and the evaluation of
treatment effects would benefit from evaluating the movement of the segments by
methods other than measurements of casts.
Introduction
"Oral orthopedics" is a term used "to con-
vey that a different type of movement is
achieved by certain appliances, i.e. a move-
ment of the entire jaw segment, tooth, bone
and soft tissues, as one unit," (Robertson and
Hilton, 1971). Treatment results have been
evaluated mainly by measuring series of casts
to determine intra-oral changes (Huddart,
1961; Graber, 1964; Huddart, 1967; Neuman,
1967; Robertson and Hilton, 1971; Huddart,
1974; Robertson and Fish, 1975; Robertson,
Shaw, and Volp, 1977; Shaw, 1978). Mea-
surement points are poorly defined, however,
and are difficult to identify because of rapid
changes in surface morphology and tooth
eruption. Besides, appositional growth and
remodelling disguises displacement of the
bone segments. Movements of the segments
can not, therefore, be accurately identified by
means of surface measurement points.
To obtain identifiable measurement points
in the infant maxilla, metallic implants have
been inserted and used as bone markers in a
few roentgen studies (Robertson, and Hilton,
1968; Robertson, 1971; Robertson and Hil-
Dr. Rune is Orthodontist at the Center for Craniofa-
cial Anomalies, General Hospital, Malmo, Sweden and
Dr. Sarnas is Orthodontist and Head of the Center at
the same hospital. Dr. Selvik is Assistant Professor at the
Department of Anatomy, University of Lund, Lund.
The study was supported by grants from Segerfalks
Foundation, Helsingborg.
ton, 1971; Robertson, Shaw, and Volp, 1977;
Shaw, 1978). Implant stability, however, was
not ascertained in the two-dimensional coor-
dinate systems, and Shaw (1977) stated that
the implant technique "is of limited value
since the implants may be disturbed by the
developing teeth and because slight inaccu-
racy in head positioning may lead to substan-
tial errors of interpretation."
Since exact methods for recording move-
ment of the maxillary bone segments in in-
fants have been unavoidable, it has been im-
possible to verify the claims which have been
made relative to the effects of oral orthope-
dics.
With a recently developedroentgen ster-
eophotogrammetric method (Selvik, 1974)
based on the use of metallic implants, move-
ment between bone segments is recorded
three-dimensionally. Implant stability is
checked with a high degree of accuracy, and
the need for identical head positioning is elim-
inated (Rune et al., 1977 a; Rune et al., 1977
b). In the present study this method was used
to record movement of the maxillary bone
segments in an infant who underwent oral
orthopedic treatment prior to primary palate
repair.
Materials and Methods
The study concerns a girl with a complete
cleft of the lip and palate on the right side.
Surgical treatment included primary lip clo-
385

386 Cleft Palate Journal, October 1979, Vol. 16 No. 4
sure (lip adhesion) at about three months ofage; primary palate repair (Wardill proce-dure) at about 20 months; and secondary liprepair (Randall-Johanson procedure) atabout 27 months. Prior to primary palaterepair, maxillary expansion treatment wascarried out by means of an acrylic plate witha fan screw. After surgery, the infant refused
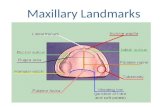
FIGURE 1. Locations of implants. L, inferior ridge
of the infrazygomatic crest. 4, anterior aspect of themaxilla, medial to and at the level of the infraorbitalforamen. P, oral aspect of the palatal shelf, halfwaybetween the incisive foramen and the transverse palatinesuture.
mm |primary lipclosure
o
primary palaterepair
+60-LU
+5.04'
+4.0
+304
+2.04
+1.04
o 4
-1.04
-2.07 expansion
---
-3.0-
to wear the retention appliance, and no fur-
ther orthopedic treatment was attempted.
Imptants. Tantalum implants (pins 1.5 %
0.5 mm) were inserted in each maxillary seg-
ment at the time of primary lip closure at
locations previously described (Figure 1)
(Rune et al., 1977 a).
ROENTGEN EXAMINATION. Stereo roentgeno-
grams were obtained three days after primary
lip closure and five times thereafter (Figure
2).
STEREOMETRIC CALCULATIONS. The stability
of the implants was checked at each exami-
nation by calculating the distance between
either of the two implants in each segment
and comparing the actual value to that of the
initial examination (Selvik, 1974, p 177). The
implant triangles represent the segments in
the calculations of movement which is ex-
pressed in terms of rotations about and trans-
lations along the cardinal axes of the head
(Figure 3). The calculated rotation angles are
valid for the entire bone segment provided no
deformity of the bone takes place. The cal-
culated translations refer to the center of grav-
ity of the implant triangles in each segment.
In the present study, movement of the right
(cleft) segment was calculated relative to the
left (non-cleft) segment which was regarded
as fixed. Additionally, the translations of each
individual implant in the right segment were
secondary
repair
x
lip
A-Aq
Tome... first primary
molars
T T
18
i
I
o-
111
1 C IC
24 42 age (months)
roentgen
examinations
1
Y M
FIGURE 2. Changes in intra-oral transverse dimensions measured on casts and given in relation to age. Surgery,
oral orthopedic treatment, and roentgen examinations (I-VI) are indicated. T-Ti: intertuberosity width, A-A;1:
intercanine width (Hellquist and Skoog, 1976).

Rune, et al., ORAL ORTHOPEDICS STUDIED BY ROENTGEN STEREOMETRY
calculated relative to the implant triangle in
the left segment. Rotations larger than 1.2
degrees, translations larger than 0.4 mm, and
distance changes larger than 0.3 mm were
Z
FIGURE 3. Directions of the cardinal axes aboutand along which rotations and translations are calculatedfor the skeletal segments. Positive directions of the rota-tions are indicated.
387
considered significant, as determined from
tests of the accuracy of the method (Rune et
al., 1979). For a detailed account of the radio-
graphic and kinematic principles see Selvik
(1974).
MrasurEmENTs oN casts. An alginate
impression was taken of the maxilla at the
time of each roentgen examination, and an
additional impression was taken during the
expansion treatment period. Transverse di-
mensions (Hellquist and Skoog, 1976) were
measured on the casts, and changes were
noted (Figure 2). Additionally, the change in
distance was noted between the lingual cusps
of the first primary molars from the beginning
of their eruption at the age of 17 months.
Results
Imprant sramBILTy. The three implants in
the left segment remained stable in the bone
for 1084 days (Table 1). In the right segment,
the distance between two anterior implants
(A, Figure 1) changed by 0.6 mm during the
interval between roentgen examinations I and
II. (In the right segment, two anterior im-
plants, 4, and one implant located in the
palate, P, constituted the implant triangle
while an unstable lateral implant, L, was
TABLE 1. Implant stability (mm) calculated for three implants in the right (cleft) and three implants in the left
(non-cleft) maxillary segment. The figures indicate the total amount of displacement of the three implants within
each bone segment measured from their positions at the initial examination. Examination numbers according to
indications in Figure 2.
Examination
Days after Right LeftInitial Examination Number Segment Segment
398 ' II .349 096515 III .669 105525 IV 114 A114722 V 202 .0981084 VI 172 110
TABLE 2. Movement of right (cleft) segment relative to left (non-cleft) segment given as rotations about andtranslations along the body-fixed cardinal axes (X-, Y-, and Z- axes) with positive direction of rotations asindicated in Figure 3. The data for rotation and translation all refer to changes from exammatlon time I.
Examination numbers according to indications in Flgure 2.
Rotation about (degrees) Translation along (mm)
_ Days after _ Examination
First Examination Number X-axis Y-axis Z-axis X-axis Y-axis Z-axis
398 II -1.6 -3.0 12.1 -O0.9 -1,5 1.0515 III 1.5 -4.5 22.2 -2,.4 -1,.2 0.9525 IV -2.3 -3.6 6.2 -1.5 -O," 0.7722 V -3.0 -3.9 10.8 -O," -1.6 1.0
1084 VI 3.1 -5.6 31.1 . -0.4 -2.8 1.2

388 Cleft Palate Journal, October 1979, Vol. 16 No. 4
disregarded). During intervals II to III and
III to IV, the distance 4-4 in the right seg-
ment changed by 0.9 and -1.4 mm respec-
tively, with one implant A4 moving laterally-
caudally (II to III) and medially-cranially (IIl
to IV). During interval V to VI the distance
A-A changed by 1.0 mm (one implant 4
moving caudally-distally). The total change
in distance 4-4 was 1.3 mm in 1084 days (I to
VI).
Right
10 mm{
10 mm <
10 mm-<
MovEMENT RECORDED BY ROENTGEN STER-
EomMETrRY. Movement of the right (cleft) seg-
ment calculated relative to the left (non-cleft)
segment was modest except for rotations
about the sagittal (Z-) axis (Table 2, Figure
4). In the 398 days following primary lip
closure (I to II), the cleft segment rotated with
the lateral alveolar ridge turning medially
(positive direction about the Z-axis); and it
was translated laterally, caudally, and ante-
Left
---------
Left
FIGURE 4. Computed move-
ment between implant triangles
projected on the frontal (XY), the
sagittal (ZY), and the transverse
(XZ) plane. The changes are given
in relation to the positions in the
coordinate system of the initial ex-
amination. Outlines of the segments
are drawn schematically. The figure
does not represent movement of the
alveolar areas and the dental arch.
The numbers refer to roentgen ex-
aminations indicated in Figure 2.

Rune, et al., ORAL ORTHOPEDICS STUDIED BY ROENTGEN STEREOMETRY
riorly (along the X-, Y-, and Z- axes). During
117 days when expansion treatment was oc-
curring (II to III), the segment rotated with
the lateral alveolar ridge turning further me-
dially (about the Z-axis); and it was translated
further laterally by 1.5 mm.
In the ten days after primary palate repair
(III to IV), the segment rotated with the
anterior part turningcranially (negative di-
rection about the X-axis) and the lateral al-
veolar ridge turning laterally (negative direc-tion about the Z-axis); and it was translatedmedially.
During the following 559 days (IV to Vand V to VI), the segment rotated with thelateral alveolar ridge turning medially (aboutthe Z-axis); and it was translated mediallyand caudally.
MEasurEs on casts. After primary lip clo-sure, a small decrease in the intercanine dis-tance occurred while the intertuberosity dis-tance remained unchanged (Figure 2). Duringexpansion, all measured distances increased.After primary palate repair, when oral or-thopedic treatment was terminated, a contin-uous narrowing of the dental arch occurred.The intertuberosity distance was stabilizedfrom ten days and the intercanine distancefrom 107 days after primary palate repair,while the distance between the first primarymolars decreased during the entire remamlngobservation period.
Discussion
ImpLANT staABILITY. In the right segment, atotal change of 1.3 mm was considered ac-ceptable between two implants measuring 1.5X 0.5 mm during an observation period of
almost three years (1084 days). Certain insta-bility should be expected during a period ofsettling-in after insertion (Aronson, 1976;Rune et al., 1977 a; Rune et al., 1979). Themeasured changes between implants 4-4 inthe right segment during intervals II to IIIand III to IV may have been caused by elasticdeformity of the bone, however, as a result ofthe expansion treatment. Movement of im-plant 4 during interval V to VI followed thegeneral direction of tooth eruption.
__ MovEmMENT RECORDED BY ROENTGEN STER-, EOMETRY. The predominant movement of theright (cleft) segment was a continuous rota-tion about the sagittal (Z-) axis with thelateral alveolar ridge turning medially. The
389
- direction of this rotation was reversed onlyduring a short period after primary palaterepair. After this procedure, even a smalltranslation laterally of the cleft segment wasreversed into a continuous translation medi-ally. Thus, movement of the cleft segmentseemed to be influenced by palatal surgery,while no effect was observed from secondary:lip repair. Orthopedic expansion treatmentprior to primary palate repair had little influ-ence on the position of the cleft segment. Itresulted only in a limited translation laterally,and this relapsed completely within sevenmonths. Generally, the movements of the cleftsegment followed a developmental pattern ofrotations about the Z- and Y- axes as previ-ously observed after primary palate repair infive UCLP patients who had had no oralorthopedic treatment (Rune et al., 1979).Mrasures on casts. A continuous decrease
of the intercanine distance after primary lipclosure (I to II) corresponded with the ob-served rotation of the cleft segment about theZ-axis (with the lateral alveolar ridge turningmedially), while it contrasted with the rota-tion about the Y-axis (with the anterior part -of the segment turning laterally). The increasein intra-oral transverse distances during ex-pansion treatment was consistent with thelimited translation laterally of the bone seg-ment, while it contrasted with the directionof the rotation of the cleft segment about theZ-axis (with the lateral alveolar ridge turningmedially). Thus, changes brought about bythe orthopedic appliance appeared to havebeen restricted mainly to movements of teethand adaptation of supporting alveolar bone.Appliance-related changes in positions ofmaxillary bone segments appeared to be min- |imal. Immediately after primary palate re-pair, when expansion treatment was discon-tinued, all transverse intra-oral dimensionsdecreased while, at the same time, the cleftsegment rotated (about the Z-axis) with thelateral alveolar ridge turning laterally. Againintra-oral changes differed from the rotationaldirections of the bone segment movement.This was the case even after secondary liprepair when the intercanine and the intertu-berosity distance remained unchanged, whilethe cleft segment continued its rotation (aboutthe Z-axis) with the lateral alveolar ridgeturning medially. The intro-oral changes ob-served after primary palate repair (IV to VI) -

390 Cleft Palate Journal, October 1979, Vol. 16 No. 4
-were similar to changes which Robertson and
Fish (1975) declared "consistent with the con-
cept of rotation of the maxillary fragments
about axes in the molar or retromolar areas,
together with growth of the arches." In our
patient, however, a small rotation about the
Y-axis occurred during this period with the
anterior part of the segment turning laterally.
Thus, rotational movements of the cleft
segment occurred mainly in opposite direc-
tions to the changes measured on casts, a
finding which seems paradoxical since the
casts are models of the oral parts of the seg-
ments. We have no explanation for these dif-
ferences. It may be stressed, however, that the
recorded segmental movements occur through
growth changes and/or deformity in the cir-
cum-maxillary sutures, while the measured
intra-oral dimensions change by appositional
growth and remodelling as well. In our pa-
tient the bone segment seemed to move ac-
cording to a certain developmental pattern,
while the changes in the alveolar areas and
the dental arch could be regarded as compen-
satory. The maxillary bones and the alveolar
areas did not move "as one unit" at any time,
and movement of the maxillary bone seg-
ments could not be verified from transverse
measurements on casts. Treatment effects on
alveolar bone and dental arch dimensions
were recorded by this method, however.
Taken together, the two methods of monitor-
ing change gave more information than either
taken alone.
References
Aronson, A. S., X-ray Stereophotogrammetry of Longi-tudinal Bone Growth, Thesis, AV-centralen, Lund,1976.
Graser, T. M., A study of cranio-facial growth anddevelopment in the cleft palate child from birth to sixyears of age, In Early Treatment of Cleft Lip andPalate, Hotz, R., Editor: Symposium Zurich, 1964;Berne, 1964, Huber and Company, pp. 30-43.
Herrquist, R., and Sxooc, T., The influence of primary
periosteoplasty on maxillary growth and deciduousdentition in cases of complete unilateral cleft lip andpalate. A longitudinal study from infancy to the age of5, Scand. J. Plast. Reconstr. Surg., 10, 197-208, 1976.
HupparRt, A. G., Pre-surgical dental orthopadics, Trans.Brit. Soc. Orthodont., 107-118, 1961.
Huppart, A. G., An analysis of the maxillary changesfollowing presurgical dental orthopaedic treatment inunilateral cleft lip and palate cases, Trans. Europ.Orthod. Soc., 299-314, 1967.
HuppaARt, A. G., An evaluation of pre-surgical treatment,Br. J. Orthod., 1, 21-25, 1974.
Neuman, B., Measurements of changes produced by pre-surgical treatment of unilateral clefts, Trans. Europ.Orthod. Soc., 315-323, 1967.
RomERTsoN, N. R. E., Recent trends in the early treat-ment of cleft lip and palate. Dent. Pract., 21, 326-339,1971.
N. R. E., and FisH, J., Early dimensionalchanges in the arches of cleft palate children. Am. J.Orthod., 67, 290-303, 1975.
RosErtson, N. R. E., and Hirton, R., A method ofdemonstrating changes produced by presurgical oralorthopaedics, Dent. Pract., 18, 449-450, 1968.
RosErRrtson, N. R. E., and Hirton, R., The changesproduced by pre-surgical orthopadics, Br. J. Plast. Surg.,24, 57-68, 1971.
RoBERTsoN, N.; Saw, W.; and Vorr, C., The changesproduced by presurgical orthopedic treatment of bilat-eral cleft lip and palate, Plast. Reconstr. Surg., 59, 86-93,1977.
Rune, B.; Jacossson, S.; Sarnas, K. V.; and G.,Roentgen stereophotogrammetry applied to the cleftmaxilla of infants, Implant technique, Scand. J. Plast.Reconstr. Surg., 11, 131-137, 1977 a.
Rung, B.; Jacomsson, S.; Nirsson, M.; SAarnias, K. V.;and Servi, G., Roentgen stereophotogrammetry ap-plied to the cleft maxilla of infants. Motion betweenthe segments, Scand. J. Plast. Reconstr. Surg., 11, 139-146, 1977 b.
Rung, B.; Jacomsson, S.; Sarnias, K. V.; and SeEuvik, G.,A roentgen stereophotogrammetric study of implantstability and movement of segments in the maxilla ofinfants with cleft lip and palate, Cleft PalateJ., 16, 267-278, 1979.
SELvIk, G., A Roentgen Stereophotogrammetric Methodfor the Study of the Kinematics of the Skeletal System,Thesis, AV-centralen, Lund, 1974.
SHnaw, W. C., Problems of accuracy and reliability incephalometric studies with implants in infants withcleft lip and palate, Br. J. Orthod., 4, 93-100, 1977.
Snaw, W. C., Early orthopaedic treatment of unilateralcleft lip and palate, Br. J. Orthod., 5, 119-132, 1978.