Oral Manifestation

of 18
-
Upload
doktergigi -
Category
Documents
-
view
241 -
download
0
Transcript of Oral Manifestation
-
8/9/2019 Oral Manifestation
1/18
September 2012265
ORIGINAL ARTICLE
Keywords: Oral medicine, autoimmune diseases, aphthous stomatitis, Sjogren’s syndrome, systemic lupuserythematosus
Corresponding Author: Niki Moutsopoulos,
DDS, PhD, National Institutes of Health/
Nidcr Building 30, Room 327, 30 Convent
Dr Msc 4320, Bethesda, MD 20892-4320;
E-mail: [email protected]
J Evid Base Dent Pract 2012:S1:
[265-282]
1532-3382/$36.00
© 2012 Elsevier Inc . All rights reser ved.
Clinical Research Core, NationalInstitute of Dental and CraniofacialResearch, National Institutes ofHealth, Bethesda, MD 20892
ORAL MANIFESTATIONS OF SYSTEMIC
AUTOIMMUNE AND INFLAMMATORYDISEASES: DIAGNOSIS AND CLINICAL
MANAGEMENT Jacqueline W. Mays, DDS, PhD, Mojgan Sarmadi, DDS, MD, Niki M. Moutsopoulos DDS, PhD
ABSTRACT
Context: Systemic autoimmune and inammatory diseases often manifest oral le-sions in their earliest stages, and early diagnosis, which may be spurred by a dental
examination, is key for improved outcomes. After systemic diagnosis, oral lesionsbenet from specialized care by dentists in collaboration with the medical team.
This review aims to educate dental clinicians about the most relevant systemic
autoimmune and inammatory conditions with accompanying oral lesions, theirimplications for health, and management strategies supported by the biomedi-
cal literature and clinical experience. Ulcerative conditions including Behcet andCrohn diseases are discussed, along with rheumatic conditions including Sjögren
syndrome, lupus erythematosus, and rheumatoid arthritis.
Evidence Acquisition: Evidence was accumulated through PubMed searches usingpertinent keywords for each subsection. References were reviewed and originalpublications examined to verify the accuracy of the information. We focused on
evidence included in current reviews and randomized trials. Recommendations
were supported by multiple studies and consensus expert opinion.
Evidence Synthesis: Disease phenotypes described and clinical recommendations
were synthesized from best-quality evidence available for each disease. Effortswere made to describe evidence selection within each disease section.
Conclusions: Dentists play an important role in the early detection and multidis-ciplinary medical management of complex autoimmune diseases. It is important to recognize prevalent medical and dental issues and special needs of patients
with autoimmune conditions. The management of many inammatory conditions
is similar, and often begins with the use of topical steroids, analgesics, and antimi-
crobial treatments, in addition to careful attention to oral hygiene and appropriateuoride usage.
In this brief review, we aim to discuss the presentation/prevalence, diagnosis, and treatment of oral manifestations encountered in autoimmune, autoinammatory
and systemic chronic inammatory diseases. Systemic autoimmune conditions are
estimated to affect 5% to 8% of Americans.1 Oral manifestations are encountered
with high frequency, and are often the rst clinical signs or symptoms of the general
disease. Optimal management of complex autoimmune diseases requires a multi -
disciplinary medical team including dentists to care for lesions of the oral cavity. Thedental practitioner may be asked to play a primary role in the diagnosis of such
-
8/9/2019 Oral Manifestation
2/18
266Volume 12, Supplement 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
on nonkeratinized mucosa of inner lips, cheeks, oor of the
mouth, ventral surface of the tongue, and the soft palate. Itspares keratinized surfaces like the hard palate and attached
gingival,6 which are more likely to be involved in intraoralviral (herpes simplex virus [HSV]) infection.7 There are noinitial blisters with RAS.8,9 Some patients notice a prodromal
tingling sensation in the local mucosa, which may correlatewith inammation in the preulcerative epithelium.10 Aph-
thous stomatitis without an underlying systemic disease orinfection is not a febrile condition but is often associated with
pain. When ulcers are closer to the oropharynx, the patientmay come in with a sore throat or even ear pain. Extraoral
examination is essential and generally normal.9 Mild ipsilateralregional lymphadenopathy may occasionally be found withlarge active ulcers of the tongue or oor of the mouth but it
is important to consider periodic fever, aphthous-stomatitis,pharyngitis, adenitis (PFAPA) or infection with nding of cer -
vical lymphadenopathy.11,12
Aphthous has been categorized based on physical presenta- tion or morphology as minor (smaller than 1 cm in diameterand most often smaller than 5 mm) and major (larger than
1 cm in diameter and rarely several centimeters, may affectkeratinized gingiva).6 RAS lesions of different morphology can
clinically present as “simple” or “complex” forms of aphthosis.Simple minor aphthosis is the most typical clinical presenta-
tion of RAS. It usually heals in 5 to 10 days, leaves no scar,and has a prior history of similar uncomplicated ulcers since
childhood.13 The term complex aphthosis is used when thereare very frequent or continuous ulcers, concurrent genital
ulcers, or associated discomfort mounting to the level of dis-
ability.3,13
Complex RAS is more likely to involve major ulcers.An association between complex or simple aphthosis withother disorders may exist and highlights the importance offormulating a differential diagnosis. A systemic condition is
more likely when RAS is complex or recalcitrant.13
Diagnosis of RAS is by exclusion and largely relies on history,review of systems, and examination. History of present illnessmust address ulcer activity and pattern. Review of systems
should screen for gastrointestinal (GI), dermatological, andimmunological/hematological symptoms, including fever and
malaise, skin rash, GI disturbances, and pain. Family historyand recent smoking cessation are relevant, as they increase
the likelihood of RAS in an individual.4 Medications and re-cent infection exposure, history, diet, oral hygiene products,
and lifestyle practices should be reviewed, as they may beassociated with oral ulcers. Matute and Alonso6 provide a list
of more than 80 medications that produce oral ulcers in their2011 review article.
During the exam, adjacent mucosa, teeth, and denturesshould be examined to identify possible sources of local ir-
ritation. Recent exposure to nuts or spices may be reportedbut often no inciting factor is identied.13 Patients should be
conditions and to participate with other health professionals
working together to achieve effective clinical management.
To aid in this process, we discuss in this article the current
general knowledge of systemic autoimmune conditions thatpresent with prevalent oral manifestations. The focus is on
the diagnosis and management of the oral component of
each disease. Importantly, whereas the etiology and patho-genesis and systemic clinical presentation may vary, presenta- tion in the oral cavity is often similar and many conditionsinvolve oral ulcerations. For this reason, we discuss the dif-
ferential diagnosis and management of the most commonoral ulcerations in a general section and subsequently ad -
dress individual conditions that present with oral ulcerations.Similarly, treatment of various autoimmune/inammatory
oral conditions is often common and involves modulation orsuppression of the immune response locally and/or systemi-
cally and will be therefore addressed in a common section aswell as individually for each disease when unique treatment
regimens are recommended. We present here our general treatment recommendations based on clinical experienceand literature review; however, it is critical that good clinical
judgment and specics of an individual case should deter -mine the appropriate dental/oral medicine intervention for
a specic patient.
ULCERATIVE CONDITIONS
Recurrent Aphthous Stomatitis
Recurrent aphthous stomatitis is an ulcerative oral mucosal
condition encountered in various ethnicities and geographi-
cal locations.2,3 In the literature it is referred to as RAS andin lay terms as the “canker sore.” RAS is not contagious andusually heals in 7 to 14 days without any treatment. Aphthousis painful and may cause signicant morbidity depending on
its location, duration, and frequency.4,5 RAS or RAS-like le-sions can also be indicative of an underlying illness or de-
ciency and may often be a presentation of a systemic auto-immune or inammatory disorder.3,5 Furthermore, although
the etiology and pathogenesis of RAS is not fully understoodand may involve multiple factors, the inammatory nature of
the disease makes it relevant to the audience of this article.Hence, in this article we review RAS followed by some sys-
temic autoimmune conditions that manifest with oral ulcers.Diagnosis
Aphthous is dened as a round to oval ulcer with well-de-ned margins and a shallow necrotic center. The ulcer base is
covered in a thin gray to white pseudomembrane or brin-ous clot and is surrounded by an erythematous halo fromlocalized vasculitis. Lesions form as “erosions” but involve the
entire epithelial lining and can affect the underlying connective tissue. The margins are red, and may feel slightly raised.6 There
is no associated drainage. Aphthous almost always develops
-
8/9/2019 Oral Manifestation
3/18
September 2012267
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
manifestation of a process with several inter-related networks
that independently or together promote an ulcer. When oneof the contributing systems is signicantly impaired, a distinct
disease may be seen together with aphthous ulcers.19
Existence of genetic predisposition in RAS is generally ac-
cepted. The likelihood if both parents are affected is 90% and
with none affected it is only 20%.6 T-cell mediated immunityappears to play a key role.4 Tumor necrosis factor (TNF)-alpha inhibition appears to signicantly reduce RAS activity.5 Various connections to heat shock protein (HSP) 65–60
have been postulated,20 in addition to other immune-relatedaberrations in people with RAS, including primary antibody
deciencies,21 changes in interleukin (IL)-1β, IL-2, and IL-6.22 Hematological abnormalities, nutritional deciencies, hor -
monal inuence,18 and smoking status are other contributingfactors.6
The list of external factors associated with RAS is very longand contains many dietary items, including nuts, spices, gluten,
and acidic fruits; environmental agents like sodium lauryl sul-fate in toothpaste and nitrates in water 23; medications; and
local mechanical irritation.6 Educating patients about thesefactors may be helpful. A list of systemic conditions reported
in association with aphthous stomatitis appears in Ship et al,24 which includes multiple deciencies in addition to systemic
diseases.
Treatment
Clinical management of the disease may require more than
one agent or modality depending on severity of RAS. Prin-
ciples of treatment include:
• Ulcer management to promote healing
• Pain management
• Nutritional management
• Disease control. Currently this means reducing recur-
rence because there is no cure.4
A search in PubMed for controlled tr ials in treatment of RASidentied more than 100 modalities and agents evaluated.
This diversity is a testimony to the lack of an effective univer-sal treatment. A multipronged approach of combined simple
treatments may be more successful. The clinical form of RAS,comorbidities, age, previous treatments, and a patient’s ability
to comply with treatment should guide recommendations.3
The best time for intervention is before ulcer formation.9
Elimination of contributing factors like irritants and decien-cies is key. Supplementation with B12 may reduce RAS fre-quency in patients with or without B12 deciency.3,25 For re-currence of active ulcers not suspected of infectious etiology,local anti-inammatory or immunomodulatory treatments
as early as possible have been recommended. Maintenance therapy after resolution is indicated if the frequency and
burden of disease justies the continued treatment. Patient
asked to return for follow-up of simple aphthous ulcer if the
lesion lasts more than 2 weeks or if their RAS changes forworse. Under these circumstances, follow-up examination
and laboratory work-up are needed. In persistent lesionswith an unusual presentation, an infectious etiology shouldbe higher on the differential. Viral cultures of intraoral HSV
lesion have high false-negative results (unless blister uid isobtained), so polymerase chain reaction (PCR) and smear
testing are recommended. Fungal cultures are more impor- tant in immunocompromised patients but are low yield so
addition of potassium hydroxide fungal preparations and fun-gal smears may be helpful in their diagnosis.14 Steroids should
not be used if an infectious or malignant etiology is suspected.Biopsy of nonhealing ulcers that resemble RAS has been rec-
ommended after 3 weeks. Biopsy is also indicated if lesionsdo not respond to regular therapy after 3 to 6 weeks. It maybe done sooner in high-risk patients represented by males,
smokers, heavy alcohol users, and those older than 45.13 Evenrepeat biopsy of oral ulcers may be needed under certain
circumstances to verify the continued benign nature of a veryrecalcitrant lesion.
Epidemiology
The onset of RAS is in childhood. Incidence of ulcers increas-
es after the age of 5,7 peaks before the age of 30,6,13,15 and de-creases in advanced age.6,13 Reported rates of RAS in adults
vary from less than 0.5% in some ethnicities in Southeast Asiaup to 66% in some subpopulations in the United States.16,17
Within US rates of 6% to 66% have been reported in studiesof different segments of the population,16,17 but these rates
are often self-reported. For all Americans, RAS prevalence
was reported as 1030 per 100,000 people based on an anal-ysis of National Health and Nutrition Examination SurveyIII.3 Higher rates are noted among women, professionals andchildren of higher socioeconomic status, adults, whites, and
those with a positive family histor y of RAS. The most com-mon morphology is minor RAS.7
The presence of underlying systemic disorders with presen- tation of RAS varies among subpopulations. Association of
complex RAS with future development of Behcet disease,for example, depends on the ethnicity of patient (very high in
Korea and Turkey, low in Western Europe and Nor th Ameri-ca). Some systemic conditions associated with RAS, like ane-
mia, are prevalent and some conditions like systemic lupuserythematosus (SLE) are less common but potentially life-
threatening.3,18 Among other systemic conditions associatedwith higher rates of RAS are diabetes, rheumatoid arthritis,
cyclic neutropenia, and Reiter syndrome.
Etiology
RAS may not be a truly autoimmune disease but a dysregu-lation of the local immune response to a variety of irritants
or stimuli.6 Most cases of RAS occur in otherwise healthyindividuals.3 It may be best to consider RAS as the nal
-
8/9/2019 Oral Manifestation
4/18
268Volume 12, Supplement 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
Patients with especially frequent or severe RAS may require
systemic immunosuppressive therapy. Systemic agents usedin treatment of RAS include oral corticosteroids, anti-TNF-
alpha agents, and calcineurin inhibitors.27 Systemic corticoste-roids are the best-studied group with proven efcacy. They
may be ineffective in certain cases or contraindicated in oth-ers for medical reasons like high risk of infection. Thalidomide
can clear aphthous ulcers and is used for recalcitrant lesions,particularly when associated with another disease.28 Of inter-est is that some immunomodulators may produce a period
of remission up to 12 months after therapy but potential sideeffects remain a concern.29
Pain management in RAS may be challenging. Typically, painis reduced concurrent with effective therapy for the lesion.
Topical anesthetics have been used with efcacy but need
frequent application. Diphenhydramine may be used as an
alternative topical anesthetic without bitter taste. Some over-
the-counter preparations may provide relief through ulcerprotection. Use of systemic analgesics like acetaminophenmay reduce the overall discomfort when pain is signicant.
Behcet’s Disease
Behcet’s disease (BD) is a chronic, multisystem inammatory
disease that generally begins with ulcers of the oral mucosa,
and then is characterized by recurring mucocutaneous le-sions of the oral cavity, genitalia, and dermis, and involvement
of the ocular, vascular, digestive, and nervous systems. It is
education is important to improve effectiveness and reduce
side effects of any treatment. Two large classes of medications traditionally used for RAS are topical steroids and antimicro-
bials. Topical agents are considered the rst line of therapy.3
Topical corticosteroids are currently the rst-line therapy
for RAS. Topical corticosteroids vary in strength as well aspotency. They may be given as mouth rinses, sprays, oint-
ments, creams, pastes, or adhesive delivery systems. Almostall commercial corticosteroids have been formulated for skin
application, and their intraoral use is off label. Their long-termapplication promotes candidiasis, mucosal atrophy, and poses
the potential for systemic effects. For these reasons, often thesmallest effective dose is recommended in a form that canhave adequate contact with lesions. A detailed list of topical
steroids is provided by Ference and Last.26
We recommend that mucosa/ulcer is rst dried, as cor tico-
steroids are not water soluble. The topical medication is ap-plied and, if safely possible, the ulcer is covered with an avail-able dressing like gauze or intraoral patch at least for a few
minutes to reduce dilution by saliva and increase absorption.
The patient should later expectorate the excess medicineand avoid eating or drinking for 20 minutes.
Table 1 shows a limited list of topical treatments that havebeen used in RAS with demonstrated benet in randomized
control trials.
Table 1.
Local Anti-inammatory Treatments Formulation Dose
Nonsteroidal anti-infammatory
Viscous lidocaine-diphenhydramine-Maalox 1:1:1 Oral Rinse prn pain/discomfort
Diphenhydramine Syrup Rinse prn and before meals
Amlexanox 2-5% Paste ~2mg QID, apply to affected tissue
Steroids
Hydrocortisone 1.0% OTC gel or ointment QID
Dexamethasone Rinse (0.01%) Oral Rinse 5 mL TID or QID
Clobetasol ointment (0.05%) ointment or cream dry and apply with gauze
Treatment of Secondary Infections
Anti-Fungal
Nystatin Oral Rinse or troche 5 mL >1 min QID
Clotrimazole troches QID, melt on tongue
Diucan Pill 150 mg
Antimicrobial
Chlorhexidine Gluconate rinse, alcohol-free (0.12%) Oral Rinse
Minocycline 0.2% Oral Rinse 5 mL >1 min QID
Tetracycline Oral Rinse 5 mL >1 min QID
prn, as needed; QID, 4 times per day; TID, 3 times per day.
-
8/9/2019 Oral Manifestation
5/18
September 2012269
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
with BD acquire hypersensitivity against streptococci in the
oral cavity, and often, an IL-12–mediated delayed-type hyper-
sensitivity (DTH) response is present in the various Behcetlesions. One theory postulates that antigen-presenting cells
uptake streptococcal agents, and during the trafcking pro-cess, are adhered to the damaged vessel walls to initiate a
local DTH-type response and subsequent clinical symptoms
characteristic of BD.32
Oral fndingsOral aphthosis is the most common and frequent symptom
of BD, reported to occur in 98.1% of patients with BD.31 Oralaphthous ulcers in patients with BD are identical to these
seen in other diseases and 25% of the healthy population.Lesions are well dened with a white to yellowish necrotic
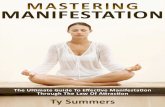
base surrounded by a red rim. Often, clusters of ulcers arenoted in patients with BD (Fig. 1, B), and occur, in order offrequency, on the lips, cheeks, tongue, gingival, palate, tonsils,
and pharynx.31 Giant aphthous lesions are less frequent in the oral cavity than on the genital mucosa in BD. As with all
oral ulcers, it is important to establish a differential diagnosis
for suspected BD lesions. Infectious etiologies, pemphigus vul-garis, and oral lichen planus should be ruled out, particular ly if the initial BD diagnosis has not been well established.
Diagnosis
The diagnosis of BD relies on clinical examination, as pathog-
nomonic symptoms and laboratory ndings have not been
dened. Several sets of criteria are in use for diagnosis of
BD, however the most widely accepted are the criter ia from the International Study Group for Behcet’s Disease.33 For
diagnosis of BD, these criteria mandate that recurrent oral
generally a relapsing and remitting condition, and inamma- tory ares may occur.
Frequency
Patients with BD historically cluster along the ancient SilkRoad countries, with a higher incidence (1-10 per 10,000) in
the countries of the Far East, Mediterranean, and Middle East than in North America and the United Kingdom (1-2 per1,000,000).30 In 2008, the International Team for the Revision
of the International Criteria for Behcet’s Disease (ITR-ICBD)published data on 2488 patients with BD collected from 27
countries worldwide.31 In this cohort, 98.1% of patients ex-perienced oral aphthosis, 76.9% experienced genital aphtho-
sis, and skin manifestations were present in 71.9% of patients.Ocular manifestations, which can result in severe loss of vi-
sion or blindness, were found in 53.7% of patients. Joints wereaffected in 50.5% of patients, the nervous system was affect-ed in 15.3%, and vascular involvement (dened as thrombosis
of deep veins, large veins or arteries, pulse weakness as wellas aneurysms and supercial phlebitis) was seen in 18.2%
of cases. Fewer than 10% of the surveyed BD cohort had
pulmonary or cardiac manifestations, orchitis, or epididymitis.
Etiology and pathogenesis
The precise etiology of BD is unclear; however, the clinicalpresentation begins with oral aphthous ulceration and pro-gresses to systemic involvement. A close relationship between
genetic and external triggering factors is believed to exist inBD. More than 60% of patients with BD are associated with
a single genotype: HLA-B51.30,32 Many recent studies have fo-cused on the function of B and T cells, infectious agents, and
the mechanisms involved in thrombophilia.30 Most patients
Figure 1. Oral ulcers may be idiopathic or part of a larger autoimmune sequelae. Typical aphthous ulcers
(A) are single round or ovoid lesions that present most often on nonkeratinized mucosa of inner lips,
cheeks, oor of the mouth, ventral surface of the tongue and the soft palate. Behcet disease is typically
accompanied by oral aphthous ulcers that may present as singular or clustered (B) lesions. Oral cGVHD
ulcers do not have a typical form, but may present as large or small mucoid lesions, deep linear ulcerations
(C), or erosions of the oral mucosa most often on the buccal mucosa, palate, lips, labial mucosa, and the
lateral and ventral tongue. (Behcet disease photos courtesy of Dean Edwards, DDS.)
A B C
-
8/9/2019 Oral Manifestation
6/18
270Volume 12, Supplement 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
for constant reinforcement of OHI in patients with BD tomaintain optimal oral health and minimize oral symptoms.
Crohn’s Disease
Inammatory bowel disease (IBD) is a complex inam-
matory disorder that has both genetic and environmentalpathogenic components. Two subsets have been identied,
including autoimmune Crohn’s disease (CD) and ulcerativecolitis, separated on the basis of their pathophysiology andclinical manifestations. CD is an idiopathic inammatory
bowel disease that may affect part or all of the alimentary
canal from the mouth to the anus. It results from defectsin mucosal immunity and intestinal epithelial barrier function.Characteristic chronic granulomatous lesions are present in
the gastrointestinal tract in CD, and may be accompaniedby strictures, adhesions, and stulae. These physical changes
result in clinical symptoms including frequent diarrhea, fever,
fatigue, anemia, reduced appetite, and weight loss. Manifesta-
tions may occur outside the alimentary tract, including skinrashes, arthritis, neurological complications, episcleritis, and
uveitis.
Frequency
The highest frequency of CD is found in white Ashkenazi
Jewish individuals of Central European origin.36 According
to the Centers for Disease Control and Prevention (CDC),worldwide prevalence of CD varies between 0.1 and 16 per
100,000 persons.37 It is estimated that as many as 1.4 millionpersons in the United States suffer from IBD, with that num-
ber evenly split between CD and ulcerative colitis.
Etiology and pathogenesis
The cause of CD is multifactorial, although the precise rela- tionships among contributing factors are not well established.
Interaction between environmental risk factors and changesin the immune system are thought to tr igger the onset of thedisease in a genetically susceptible host.38 CD has a strong
genetic component, and more than 30 genes have beenassociated with the incidence and severity of CD. It is an
autoimmune disease, and emerging research indicates thatCD may result from an impaired innate immune response.
In this scenario, aberrant cytokine secretion by macrophagesimpairs the body’s natural antimicrobial defenses and leads
to a sustained proinammatory environment in the colon,
where the bacterial load is high. This theory is supported bya recent association between patients with CD and impairedgene expression, which may induce autophagy and dampen the body’s ability to attack invasive bacteria. So far, several
genetic associations with CD have been demonstrated asdisease modiers and susceptibility genes.36,39 An association
between CD and a specic bacterial species has not been
shown, although evidence clearly points to bacterial involve-
ment in CD development. There is an increased incidence ofCD in industrialized countries, pointing to an environmental
ulceration is present, plus at least 2 of the following: recur-
rent genital ulceration, eye lesions, skin lesions, or a positivepathergy test. The pathergy test entails the oblique insertion
of a sterile 20- to 22-gauge needle into the vascular skin toa depth of 5 mm. The test is considered positive if an ery- thematous papule develops at the test site after 48 hours. As
suggested by the criteria, this test is not positive in every BDpatient. Studies have found a higher rate of positive pathergy
test in patients with BD when the needle was rst dipped
in the patient’s own saliva, the majority of which contained
streptococci species, versus sterile-ltered saliva or saline.32 This nding was attributed to DTH response to streptococ-
cal species.
Clinical Management
Systemic management of BD typically involves systemic im-munosuppressive therapy or colchicine to manage disease-
related symptoms, including oral ulcers. Newer biologic therapies including anti–TNF-alpha therapies have been
tried with promising results.31 Not all Behcet patients requiresystemic management, and some rely on topical therapy asneeded to manage symptoms.31
Oral management of Behcet patients includes care of recur-
rent aphthous ulcers, meticulous attention to oral hygieneand frequent reinforcement of oral hygiene instruction. Local
antiseptics and local antibiotics may be helpful for symptom-atic ulcers, and these may be managed as standard aphthousulcers. Of interest, one single-center study found that patients
reported an improved oral health-related quality of life, as
assessed by the oral health impact prole-14, when on a sys-
temic immunosuppressive therapy versus those on colchi-
cine, which may warrant discussion with a patient’s medical team if oral symptoms are especially prevalent.34
As discussed previously, local infections may be an impor-
tant part of the pathogenesis of BD. The oral cavity is closely tied to BD pathogenesis, and oral ulcerations are typically the
rst clinical manifestation of BD. Many Behcet patients have
a heightened immune response to oral streptococci. Taken
together, these factors underscore the importance of goodoral hygiene in patients with BD. However, dental prophylaxisand other dental treatment may briey induce oral aphthous
ulcerations in susceptible populations. A 2009 prospective
clinical study followed patients with BD for 8 months to track the incidence of oral ulceration with and without dental andperiodontal treatments when all patients received oral hy-
giene instruction (OHI).35 In this cohort, the number of neworal ulcers increased in the 2 days following dental treatment,
but then signicantly decreased throughout the 6-month
posttreatment follow-up period when compared with the
OHI-only group. This report also noted that tooth-brushingfrequency increased after dental treatment, but had returned
to baseline values at the end of 6 months, indicating a need
-
8/9/2019 Oral Manifestation
7/18
September 2012271
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
patients with potential inammatory bowel disease, particu-
larly when the diagnosis is not clear from other parts of theclinical examination.
Diagnosis
There are no gold standard criteria for the diagnosis of CD.
Diagnosis of CD relies on a constellation of clinical data from
the patient history, physical examination, and laboratory tests.This may include blood tests for anemia, autoimmune an- tibodies, and genotyping, although the latter 2 are not cur-rently endorsed by the American College of Gastroenterol-
ogy, and other tests to rule out infections and confoundingfactors. Endoscopic examination may include colonoscopy
for determination of the presence and extent of disease. This typically includes biopsy of the colon for histological evidence
of disease. Barium studies of the upper and lower GI tractand small bowel imaging may also be done.
Clinical Management
No cure exists for CD; thus, the goal of medical treatment
is to suppress the inammatory response. This allows the in- testinal tissue to heal, and it typically relieves the symptoms
of fever, diarrhea, and abdominal pain. Once a patient is in astate of remission, treatment is focused on decreasing thefrequency of disease ares. Five major classes of drugs are
currently used to treat systemic CD. These include amino-
salicylates (5-ASA), corticosteroids, immunomodulators,including methotrexate and azathioprine, antibiotics, and
several newer biologic therapies including anti–TNF-alpha
therapies.
As with all autoimmune conditions discussed here, multidis-
ciplinary management of patients with CD is crucial so that they receive appropriate and comprehensive health care.Standard management of recurrent aphthous ulcers shouldbe used in this patient population. One case report in the
literature details successful use of thalidomide, which blocksproduction of TNF-alpha by monocytes, for the treatment of
recalcitrant RAS in a 13-year-old female patient with CD.45 This treatment strategy could conceivably be supplanted by
a newer biologic therapy to block TNF-alpha so as to avoid thalidomide-induced side effects. Patients with CD are prone to nutritional deciencies, and working with the patient and
medical team to correct areas of nutritional deciency may
help to decrease the incidence of ulceration. As CD involveschronic inammation of mucosal tissue, there is an increasedrisk for oral cancer. Patients with CD should receive regular
oral cancer screenings with biopsy of suspicious or nonheal-ing lesions along with their routine dental care. Other charac-
teristic oral manifestations of CD are reported to abate withsuccessful systemic management of CD.
Chronic Graft-Versis-Host-Disease
Allogeneic hematopoietic stem cell transplantation (al-loHSCT) is used with increasing frequency to treat
component that seems to include psychological stress, diet,
and tobacco smoking.37
In the oral cavity, less is known about why only some of the
CD population develops oral lesions. It is theorized that there
is an association between ileocolonic disease and CD; how-
ever, this is not supported by all population studies. Some
groups have found an association of oral CD in children withperianal disease; however, these lesions did not differ phe-notypically from children without oral CD.40 Little is known,mechanistically, about the immunological basis for oral CD,
although it seems to be a fur ther manifestation of the patho-logical processes occurring throughout the GI tract and may
result from similar impairments of the innate immune systemin patients with CD and other factors that promote general
oral inammatory disease.
Oral fndings
Oral lesions characteristic for CD are present in many cases,and the potential clinical relevance of these oral ndings is
emergent.40 Oral aphthous ulcerations are frequently pres-ent in patients with CD; however, these general ulcerations
also occur in patients with inammatory bowel disease and
in the general population. Jose et al41 reported from a large
cohort of patients (n = 1649) that aphthous ulceration was the most frequent extraintestinal manifestation of IBD before
diagnosis. Oral lesions that are characteristic for CD includeswelling of the lips, cobblestoning or edema of the buccal mu-cosa, deep linear ulcerations, mucosal tags, and mucogingivitis.
Patients with CD reported a poorer self-perception of oralhealth in one study, specically caries incidence and gingival
bleeding; however, a case-control study of 62 patients with
BD and 59 matched healthy controls found a minor increasein dentin caries in IBD, with no signicant change in clinical
attachment loss.42,43
Oral manifestations seem to be more prevalent in children than in adults. A recent retrospective char t review that was
followed up with a 3-year prospective study of oral mani-festations of CD at a pediatric hospital found 40% to 48%
of children had CD-specic oral lesions at the time of CD
diagnosis.40,44 Additionally, in clinically indicated biopsies, 75%
to 100% contained noncaseating granulomas, which are clas-sic oral CD lesions.40,44 Routine biopsies were not performedduring the study, so it is not known how frequent oral granu
-lomas are in patients with CD. The prospective study furthercompared the frequency of oral ndings in children with CD
when examined by a gastroenterologist in a clinical settingversus formal oral exam by a pediatric dentist. Even through
the gastroenterologists were reported to have an establishedinterest in oral lesions, the ability of the physicians to iden-
tify and accurately classify oral CD lesions was poor when the dentist’s exam was used as a comparator.40 Harty et al40
advocate that involvement of an experienced dental profes-sional can be a valuable adjunct during the diagnosis phase in
-
8/9/2019 Oral Manifestation
8/18
272Volume 12, Supplement 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
indications for its use, cGVHD will continue to be seen in
the numbers of alloHSCT performed each year. Thirty per-cent to 65% of patients who sur vive longer than 1 year after
transplantation wil l develop cGVHD,46 which may be fatal inapproximately 15% of transplant recipients.48 In the UnitedStates, almost 6000 patients underwent HCT in 2009, an
increase of 30% since 2005. With this dramatic increase inHCT, the incidence of GVHD will also continue to increase.49
Although cGVHD can affect multiple organs, the oral cavityis the second most commonly involved organ system, and is
reported in approximately 45% to 83% of patients withcGVHD.50
Patients with cGVHD have specialized oral health needs that
can be addressed in a general practice setting with a well-educated clinician, and it is important that diligent care isavailable for patients with cGVHD, as their numbers continue
to increase.
Etiology and pathogenesisMajor known risk factors for developing cGVHD includeolder recipient age, major allele for human leukocyte antigen
(HLA) mismatch between donor and recipient, peripheralblood stem cell source, conditioning regimen, and GVHD
prophylaxis regimen.51 Grafts that include more donor Tcells are typically more effective at eradicating malignancy;
however, also lead to a higher incidence of severe cGVHD.The essential pathogenesis of cGVHD, in which donor im-
munocompetent cells recognize and attack host tissues in
immunocompromised recipients, remains current.52,53 ThecGVHD has many autoimmune and brotic features, and
current evidence demonstrates involvement of the patient’sown immune cells in the autoimmune attack. The process hasa strong proinammatory T-cell component, with additional
involvement of B cells and regulatory T cells.46,54,55
Oral fndings
Oral cGVHD has 3 components: mucosal involvement,salivary gland involvement, and sclerotic involvement of themouth and surrounding tissues.56 The oral mucosa presents
with classic ndings in cGVHD, including lichenoid changes,
erythema, ulcerations, hyperkeratotic patches, and mucosal
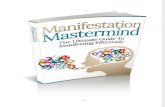
atrophy (Fig. 2). Limited mouth opening may be caused byinvolvement of the temporomandibular joints, or by sclerotic
changes in the perioral tissues. Salivary gland dysfunction mayresult from medication, inammation, and/or brosis of the
major and minor salivary glands. Individually, these changesmimic oral ndings in several classic autoimmune diseases.
The lichenoid lesions mirror those seen in oral lichen pla-nus, whereas the lymphocytic salivary gland inltrates and
resulting dry mouth are reminiscent of Sjögren’s syndrome.
Restricted oral opening and perioral brosis in patients with
GVHD are similar to changes observed in patients with
scleroderma.
malignancies of the blood, bone marrow, and lymphoid sys- tem; systemic immunodeciencies; and a variety of other dis-
orders. It is the only curative option for many hematologicalmalignancies.46 In alloHSCT, multipotent hematopoietic stem
cells from a non-self donor, harvested from bone marrow,peripheral blood, or umbilical cord blood, are transfused into
the patient.Graft-versus-host disease (GVHD) results from an immuno-
logical attack on the patient’s tissues by donor T cells that are transferred along with the graft. Chronic GVHD (cGVHD)
is a common complication after HCT. cGVHD was initiallydened as occurring at or beyond 100 days posttransplanta-
tion; however, its classication is now based on characteristic
clinical presentation, regardless of timing.47
Patients with cGVHD suffer from mild to severe morbidity,with variable manifestations in the skin, mouth, eyes, gut, liver,
lungs, joints, and genitourinary tract. These are painful, impairfunctional ability, and reduce quality-of-life. The disease pre-
sentation of cGVHD resembles many autoimmune disorders,including scleroderma, Sjögren’s syndrome, and oral lichenplanus. Furthermore, owing to the inammatory nature of
the condition and the use of immunosuppressive therapies
in its treatment, cGVHD is relevant in the context of auto-immune and inammatory conditions.
Frequency
The occurrence of GVHD is the limiting factor in the suc-
cess of alloHSCT. With increasing success and long-termsurvival of patients after alloHSCT, as well as the increasing
Figure 2. Oral chronic graft-versus-host-disease
typically manifests more than 100 days after
allogeneic stem cell transplantation. Common oral
ndings include mucoceles (A), atrophy, perioral
brosis (B) or TMJ involvement resulting in limited
mouth opening, mucosal edema (C), lichenoid
lesions (C), ulceration (C), and mucosal erythema
(D). (A and B courtesy of Carol Bassim, DMD, MS,and Dean Edwards, DDS.)
A B
C D
-
8/9/2019 Oral Manifestation
9/18
September 2012273
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
saliva substitute products. Several studies support the use
of short-term or prolonged pilocarpine therapy for salivarystimulation in patients with cGVHD; however, pilocarpinealso increases secretion of gastric uids, which may be prob-lematic in patients with GI tract GVHD.59,60
ORAL BLISTERING DISEASES OF AUTOIMMUNEORIGIN
Most bullous autoimmune diseases affect the skin and/ormucosal sites, including the oral cavity. Major bullous condi-
tions that involve the oral cavity include pemphigus vulgar is(PV), mucosal pemphigoid (MP-cicatricial pemphigoid), bul-
lous pemphigoid, and oral lichen planus (OLP).61,62 Lesionsin many of these conditions appear similar clinically, and di-
agnosis may be difcult and denitive only after histological
evaluation and support from a multidisciplinary medical team.Furthermore, it is often that such conditions are rst mani-fested in the mouth, rendering the dentist practitioner key
for initial diagnosis.
Treatment of autoimmune bullous diseases is geared (as inmany autoimmune or inammatory based disorders) toward
the remission of the disease by modulating or suppressing
the overreactive immune response locally and/or systemical-ly.62 Although pathogenesis and treatment of these disordersis addressed in a separate article of this publication, many of
the immune suppressive therapies used for the treatmentof oral manifestations in autoimmunity are common and are
discussed in a following section of our ar ticle and in Table 1.
RHEUMATIC DISORDERS
Sjögren’s Syndrome
Sjögren syndrome (SS) is a fairly common chronic auto-
immune disorder, affecting 0.5% to 5.0% of the general popu-lation, but most commonly females (at a 9:1 ratio) in theirfth decade. This large reported range of disease prevalence
may be attributed to differences in the denition and applica- tion of diagnostic criteria among the studies, the diverse geo-
graphic study origin, as well as the different initial sample size
and sex distribution.63,64 The hallmark of SS is the lymphocytic
inltration of the exocrine glands, particularly the periductal
areas of mainly the lacrimal and salivary glands. This resultsin impaired secretory function and consequently xerostomia(dry mouth) and xerophalmia (dry eyes) (Table 2).64,65 Si-
multaneously, systemic features of cutaneous, respiratory, re-nal, hepatic, neurologic, and vascular nature often occur. The
syndrome can present either alone (as primary SS) or in thecontext of underlying connective tissue disease (as second-ary SS).
Diagnosis
The multiple aspects of the syndrome make it difcult to
diagnose. As a consequence, SS commonly remains either
Clinically detectable oral cGVHD was present in 24% of pa-
tients from a referral-based multinational cohort of patientsseverely affected with cGVHD assessed at the National In-
stitutes of Health (NIH). In this cohort, most patients withoral cGVHD presented with erythema (54%) and lichenoidchanges of the oral mucosa, whereas only a few presented
with ulcerations (4%) and mucoceles (7%). Many of these pa- tients reported subjective oral dryness (66.7%), pain (45.6%),
and sensitivity (59.3%).57
Clinical Management
Goals of therapy for patients with oral cGVHD include painmanagement, healing of lesions, and suppression of inam-
mation in the oral cavity. Early detection and diagnosis, ap-propriate therapeutic management, and regular follow-up
are essential to ensure optimal outcomes and improvedquality of life of patients with oral cGVHD. The NIH con-
sensus conference on ancillary therapy and supportive carefor cGVHD has provided recommendations for the man-
agement of symptoms and guidelines for the prevention ofinfections and other common complications of treatment re-lated to cGVHD.56 Although oral cGVHD symptoms reduce
quality of life and, in severe cases, lead to malnutrition, they
are generally not life-threatening.58 Treatment, particularly any
systemic therapy, should be coordinated in conjunction with the medical team.
Most therapy currently recommended for the managementof mucosal manifestations of oral cGVHD is directed at the
use of topical high- and ultra–high-potency corticosteroids(Table 1), calcineurin inhibitors, and analgesics. These topical
treatments are not always effective, and also carry the risk
of systemic absorption owing to a breakdown in mucosalintegrity in some patients with oral cGVHD. Efcacy may be
improved by compounding some of the topical agents to a
rinse formulation; however, clinical trials are lacking to sup-port specic agents and dosing schedules.
Patients with cGVHD should be regularly screened for oralcancer, as oral squamous cell carcinoma has been reported
in this population. Suspicious lesions should be biopsied. Pa- tients on systemic or oral topical corticosteroids are prone
to overgrowth of oral Candida, and it is impor tant to differ-entiate cGVHD-related hyperkeratosis and erythema from
an ongoing oral fungal infection before starting an aggres-sive course of treatment. Although patients with cGVHDare regularly screened for serum antibodies to viruses, virus-
related oral ulcers may still occur in serum-negative patients,and PCR-based screening or biopsy is recommended when
clinically indicated. The cGVHD induces changes in both thequality and quantity of saliva, which leaves patients suscep-
tible to dental decay. Excellent professional and home oralhygiene, use of supplemental uoride and mild dentifrice are
strongly indicated in patients with cGVHD. Patients shouldbe counseled on use of sugar-free beverages, sialagogues, and
-
8/9/2019 Oral Manifestation
10/18
274Volume 12, Supplement 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
undiagnosed or is diagnosed years after the onset of symp-
toms. Early recognition of this disease is of pivotal impor- tance to prevent delay in appropriate diagnostic evaluation,and optimize therapeutic intervention. Diagnosis of SS is
based on the concurrent presence of various signs and symp- toms of the disease (see Table 3 for diagnostic criteria).66-69
The role of dentists in the diagnosis and treatment of SS iscrucial. Patients often present rst to their dentists because
of their predominantly oral symptomatology. Proper educa- tion of the general dentist to recognize signs and symptoms
of xerostomia, to include SS in their differential diagnosis, and to refer patients for evaluation with a rheumatologist in a
timely fashion, is key in the proper diagnosis and treatmentof the condition.
Etiology and Pathogenesis
The etiology of SS remains unknown to date. As for many
autoimmune diseases, it is believed for SS as well that aninitial unknown environmental trigger, in genetically suscep-
tible individuals, leads to aberrant activation of the immunesystem. Although genetic susceptibility has been speculated, there are limited studies investigating genetic linkage in SS.
Studies to date have focused on associations between HLAalleles and SS and genes that are known risk factors for
other autoimmune conditions, including polymorphisms in type I interferon (IFN)-related genes.63 Beyond susceptibility,
various triggers that initiate disease progression have beenspeculated and are under investigation. Viral triggers includ-
ing Epstein Barr, human T lymphotropic virus 1, hepatitis C,and enteroviruses have been previously proposed as poten-
tial initiating factors.63 Stress and hormonal factors have also
been linked to disease susceptibility and initiation. Followingdisease initiation in SS, there is compelling evidence of ac- tivation of the epithelium in target organs that appears todrive and/or perpetuate the inammatory response. In this
context, epithelial cells may act as antigen-presenting cells aswell as proinammatory immune cells by expressing major
histocompatibility complex (MHC) molecules and costimula- tory molecules and producing high levels of proinammatory
cytokines.63,65 Finally, the aberrant immune response leads toglandular immunopathology, dysfunction in glandular secre-
tion, and increase prevalence of lymphoma transformation inpatients with SS.63
Oral fndingsThe oral manifestations observed in patients with SS are at-
tributable to the involvement of salivar y glands, which leads to decreased salivary secretion. Loss of the lubricating, buff-
ering, and antimicrobial capacities of saliva leads to an in-creased incidence of oral/dental infection, mucosal friability,and subjective symptoms of dryness, irritation, and burning
sensation.64,65 Most common oral ndings are dental caries(often rampant) with the uncommon presentation of root
and incisal caries. Most often mucosal infections are fungal(primarily candidiasis/oral thrush), which can be manifested
Table 2. Common Oral Lesions of Systemic
Autoimmune Disorders
Bechet’s Disease
1. Minor recurrent apthous ulceration
2. RAS
Crohn’s Disease
1. Recurrant apthous ulcers
2. Swelling of the lips
3. Cobblestoning of the buccal mucosa
4. Deep linear ulceration
5. Mucosal tags
6. Mucogingivitis
7. Noncaseating granulomas in biopsy specimins
GVHD
1. Lichenoid changes
2. Ulcerations
3. Mucosal atrophy
3. Salivary gland dysfunction
4. Xerostomia
5. Restricted oral opening – Perioral brosis
– TMJ involvement
6. Hyperkeratosis (white patches)
7. Mucoceles
8. Buccal edema
Sjogren’s syndrome
1. Xerostomia (Dry Mouth)2. Rampant caries/Root caries
3. Oral Candidiasis
4. Unilateral parotid gland enlargement
Rheumatoid Arthritis
1. TMJ involvement (mostly in juvenile arthritis)
2. Increased prevelance of periodontal disease
Lupus Erythematosus
1-RAS
2-mucosal discoid lesion
3-white plaques/Lichen planus-like lesions
4-red plaques or macules
5-mucosal autoimmune ulcers with or without surroundingstraiae or telngiectasia
6-Transformation to squamous cell carcinoma
7-Secondary Sjogren’s oral sequela
8-Secondary Steven-Johnson’s syndrome
9-Secondary activation of HSV
10-Secondary fungal infections
11-Secondary light brown pigmentation from antimalarials
-
8/9/2019 Oral Manifestation
11/18
September 2012275
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
and mucosal infections are common, the prevalence and se-verity of periodontal disease has not been reported to be
increased in SS. Mucosal friability in SS often leads to soft
as pseudomembranous or erythematous mucosal lesions,median rhomboid glossitis and tongue ssuration, denture-
associated stomatitis, or angular cheilitis.64,65 Although dental
Table 3.
Revised International Classication Criteria for Diagnosis of Sjogren’s Syndrome [73]
I. Ocular symptoms: a positive response to at least one of the following questions:
1. Have you had daily, persistent, troublesome dry eyes for more than 3 months?
2. Do you have a recurrent sensation of sand or gravel in the eyes?
3. Do you use tear substitutes more than 3 times a day?II. Oral symptoms: a positive response to at least one of the following questions:
1. Have you had a daily feeling of dry mouth for more than 3 months?
2. Have you had recurrently or persistently swollen salivary glands as an adult?
3. Do you frequently drink liquids to aid in swallowing dry food?
III. Ocular signs—that is, objective evidence of ocular involvement dened as a positive result for at least one of the following two tests:
1. Schirmer’s I test, performed without anesthesia (≤5 mm in 5 minutes)
2. Rose bengal score or other ocular dye score (≥4 according to van Bijsterveld’s scoring system)
IV. Histopathology: In minor salivary glands (obtained through normal-appearing mucosa) focal lymphocytic sialoadenitis, evaluated byan expert histopathologist, with a focus score ≥1, dened as a number of lymphocytic foci (which are adjacent to normal-appearing
mucous acini and contain more than 50 lymphocytes) per 4 mm2 of glandular tissue
V. Salivary gland involvement: objective evidence of salivary gland involvement dened by a positive result for at least one of the follow-ing diagnostic tests:
1. Unstimulated whole salivary ow (≤1.5 mL in 15 minutes)
2. Parotid sialography showing the presence of diffuse sialectasias (punctate, cavitary, or destructive pattern), without evidence ofobstruction in the major ducts
3. Salivary scintigraphy showing delayed uptake, reduced concentration, and/or delayed excretion of tracer
VI. Autoantibodies: presence in the serum of the following autoantibodies:
1. Antibodies to Ro(SSA) or La(SSB) antigens, or both
Revised Rules for Classication [73]
For primary SS
In patients without any potentially associated disease, primary SS may be dened as follows:
a. The presence of any 4 of the 6 items is indicative of primary SS, as long as either item IV (Histopathology) or VI (Serology) is
positive
b. The presence of any 3 of the 4 objective criteria items (that is, items III, IV, V, VI)
c. The classication tree procedure represents a valid alternative method for classication, although it should be more properly used
in clinical-epidemiological survey
For secondary SS
In patients with a potentially associated disease (for instance, another well dened connective tissue disease), the presence of item I or
item II plus any 2 from among items III, IV, and V may be considered as indicative of secondary SS
Exclusion criteria:
Past head and neck radiation treatment
Hepatitis C infection
Acquired immunodeciency disease (AIDS)
Preexisting lymphoma
Sarcoidosis
Graft-versus-host disease
Use of anticholinergic drugs (since a time shor ter than fourfold the half-life of the drug)
SS, Sjogren’s Syndrome .
-
8/9/2019 Oral Manifestation
12/18
276Volume 12, Supplement 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
in preserving the natural dentition in patients with SS, inves-
tigating the possibility of dental implant treatment is of greatimportance. Unfortunately, there is very limited evidence in
the literature regarding the success of dental implants in pa- tients with SS.
Treatment of Candidiasis For the treatment of oral candidia-
sis, topical antifungal treatment (see Table 1) can be followedby systemic antifungal agents for persistent or recurrent epi-sodes. A typical regimen includes nystatin cream and a pastilleor oral suspension of nystatin 3 to 4 times daily for 1 week,
followed by systemic treatment with an azole. For prevention
of candidiasis, wearing dentures overnight should be discour-
aged and dentures should be cleaned with 2% chlorhexidine.A biopsy should be undertaken in individuals with the hy-
perplastic variant of Candida infection, because of the risk ofmalignant transformation.64
Treatment of Xerostomia Traditional treatment of xerosto-mia in SS has focused on palliative measures using salivary
substitutes, which can improve lubrication and hydration oforal tissues, despite the transient nature of their activity. Lu-
bricating agents in the form of gels, mouthwashes, lozenges,
and toothpastes have been used, with various results. Tran-
sient comfort can also be achieved by sipping water andother sugar-free uids.
For patients with SS who have residual salivary gland function,stimulation of saliva ow with a secretagogue is the treat-
ment of choice and is, at present, the most efcacious means
of preventing long-term oral complications. Nonpharmaco-
logical secretagogues might be useful in patients with reason-
able levels of sal ivary ow, such as stimulation with sugar-freegums.
Two muscarinic acetylcholine receptor agonists (pilocarpine
and cevimeline) are licensed and have been widely used for the treatment of sicca symptoms in SS. These agents stimulate
the muscarinic acetylcholine receptors M1 and M3 presenton salivary glands, leading to increased secretory function.69
Management of the glandular and extraglandular manifesta- tions of SS may often involve the use of immunomodulatory/
suppressive, antimalarial, and/or biologic agents, depending ondisease presentation and severity of symptoms. In all cases, though, successful management of patients with SS requires a
multidisciplinary approach with involvement of primary carephysicians, rheumatologists, ophthalmologists, dentists, gyne-
cologists, and hematologists.
Lupus Erythematosus
Lupus erythematosus refers to a group of autoimmune dis-eases with a wide range of presentations from cutaneous to
systemic.70 The term lupus is often used as short for systemiclupus or SLE, which is the most common form. Systemic lu-pus is a serious illness usually with ares and intermittent
tissue lesions in patients with SS. Such signs include oral mu-
cosal scores, dry and cracked lips, and tongue depapillation(Fig. 3). Finally, another fairly common oral manifestation is
the asymptomatic and self-limiting enlargement of the pa-rotid gland or another major salivar y gland (Fig. 3). Persistentenlargement should be carefully followed to exclude bacte-
rial super infection and, more importantly, the developmentof lymphoma.
Clinical Management
Treatment of Dental Caries Aggressive routine and preven-
tive dental care and use of uoride is crucial for patientswith SS. Fluoride gels, prescription-strength toothpaste, and/
or oral rinses containing 0.40% to 1.25% uoride should be
used. The provider should keep in mind the additional chal-
lenges of treating dental caries in patients with xerostomia.The commercially available agents are often acidic and can
cause irritation of the oral mucosa, resulting in poor com-pliance. Also, in extreme cases of hyposalivation, destruction
of the tooth enamel might theoretically occur because ofinsufcient remineralization, even in the presence of uoride,
resulting from the lack of saliva.64 Finally, given the difculties
Figure 3. Common manifestations of Sjögren
syndrome include benign lymphoepithelial lesion of
the parotid gland (A) and dry and ssured tongue
(B). (Photos courtesy of Clio Mavragani, MD.)
A
B
-
8/9/2019 Oral Manifestation
13/18
September 2012277
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
Diagnosis and Oral Findings
Signs and symptoms of lupus depend on which organ is af-fected and often include fever, fatigue, oral ulcers, weight loss,
malar rash, photosensitivity, and joint pain. Circular (disc-like)plaques, renal failure, arthritis, coronary artery disease, pul-monary hypertension, hemolysis, stroke, seizures, or psycho-
sis may be seen. Early treatment could be critical, and familiar-ity with unique association of oral ndings in lupus may help
clinicians in recognizing lupus earlier.
The classical oral lupus lesion is a whitish plaque with ery -
thema in the center and keratotic str iae in the periphery at times with telangiectasia.70 Patterns of oral lesions may differ
among different types of lupus.82 Diagnosis of lupus-relatedlesions requires biopsy; intraoral biopsy is generally preferred
over skin biopsy when there is a choice to avoid scarring.
It may be difcult to delineate oral lesions of different forms
of lupus.76 Overall, red mucosal macules and plaques (ery - thematous lesions), mucosal ulcers and RAS, and lesions that
resemble lichen-planus or leukoplakia are described.76 Lichen-oid mucositis with acanthosis and deep perivascular inltrate
on histology have been reported.70,76 In DLE, discoid lesionscan occur intraorally and are seen on buccal mucosa, gingival,
and lips.74 Some other histological characteristics frequently
reported are hyperkeratosis with keratotic plugs, liquefaction/
vascular degeneration of the basal epithelial cells, thickeningof the basement membrane, atrophy of rete ridges, edema in the lamina propria, subepithelial mononuclear inltrate, and
at times periodic acid-Schiff –positive deposits.70,76 Direct im-munouorescence is often positive and shows linear deposits
of immunoglobulin (Ig)G or IgM and/or C3 in the basement
membrane. CD4+ T lymphocytes prevail in the ulcer base,which is also inltrated by other immune cells.70,74
RAS and oral ulcers are not only common in SLE but also
correlate well with the underlying systemic disease activity.New onset of RAS in adults or sudden unexplained worsen-
ing of preexisting RAS may be the earliest manifestation of asystemic disorder, including lupus.
Like worsening RAS, appearance of oral lupus lesions maysignal increased disease activity in a lupus patient. Pediatric
patients with discoid cutaneous lupus and mucosal involve-ment, including RAS lesions, are more likely to transition to
SLE and may benet from closer follow-up.83
Patients with lupus on systemic therapy with immunosuppres-
sant agents are prone to secondary infections. Viral and fungalinfections are common in the oral cavity. Some of these may
be mistaken for RAS or lupus ulcer but must not be treatedwith steroids. Stevens-Johnson syndrome is a rare but serious
complication of HSV that may appear a few weeks after anoutbreak. Skin and any of the mucosal surfaces, including eyes,
may be involved with ulcers in Stevens-Johnson syndrome.84
remissions. In SLE, internal organs are affected. The other
main category of lupus is cutaneous lupus erythematosus(CLE), which has various forms with different signs and se-
verity presenting as acute to chronic. Chronic CLE includesdiscoid lupus or DLE, with disc-like lesions of skin and/or mu-cosa.71 CLE can be mild or severe. It may remain limited to
skin or progress to SLE.
70,71
Neonatal lupus is secondary tomaternal autoantibodies,72 and drug-induced lupus produces
symptoms of lupus but usually resolves after the inciting fac- tor is removed. Most literature on oral lesions in lupus per-
tains to SLE and DLE.
Oral lesions are among the most common ndings in lupus73
and provide an opportunity for early diagnosis and interven- tion. Oral lesions may be found in systemic or cutaneous
lupus and may be the only lesion in some patients.74 Lupusis often difcult to diagnose because presentations vary and
mimic other diseases.
Epidemiology
According to the Lupus Foundation of America, 1.5 millionindividuals in the United States have lupus and16,000 new
cases are reported annually. Systemic lupus is the most com-mon presentation. CLE is less prevalent74 and DLE is the most
common cutaneous form.71 A higher rate of lupus has beennoted in Asian, Hispanic, and Native American individuals. Lu-
pus can occur at any age in both sexes but it is diagnosed inwomen more than men and often during the child-bearingyears. Lupus is also 2 to 3 times more likely to affect Ameri-
can black females.70,75
Prevalence of oral manifestation in lupus has been reported
at various rates from low to more than 50% of cases andusually more than 1 lesion is present on examination.70 Thevariation in reported rates may reect the fact that many
medical examinations do not include a complete routine oral
exam, and rates that are repor ted pertain only to some typesof ulcers in different forms of lupus. Systemic therapy may re-
duce prevalence in treated patients.76 The mouth is the mostcommonly affected site in lupus.77
Etiology/ Pathogenesis
Immunological factors, genetics, environmental exposures,
smoking, infection, vaccines, and UV light, as well as hormonalfactors, are each reported to play a role in the development
of lupus.78,79 Neutrophil extracellular traps induce innateimmunity early on in the disease.80 Activation of type I IFN
pathways, B- and T-cell dysfunction, as well as presence ofantinuclear antibodies are seen.70 Many other autoantibodies
have been reported.79 A number of genetic loci that increaselupus susceptibility have been established but none has beenidentied as the cause of the disease. Instead, they appear to
correlate with the variations seen in lupus and may work byepigenetic modulation.80 Cer tain alleles of STAT4 were found
to correlate with protection from oral ulcers in patients withlupus.81
-
8/9/2019 Oral Manifestation
14/18
-
8/9/2019 Oral Manifestation
15/18
September 2012279
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
REFERENCES1. Comittee , A.D.C., Autoimmune Diseases Research Plan. Depar tment
of Health and Human Services, National Institutes of Health, NationalInstitute of Allergy and Infectious Disease; 2002. NIH Publication No.03-5140.
2. Jurge S, et al. Mucosal disease series. Number VI. Recurrent aphthousstomatitis. Oral Dis 2006;12(1):1-21.
3. Baccaglini L, et al. Urban legends: recurrent aphthous stomatitis. OralDis 2011;17(8):755-70.
4. Datau W EA. Recurrent aphthous stomatitis caused by food allergy.Acta Med Indones 2010;42(4):236-40.
5. O’Neill I, Scully C. Biologics in oral medicine: ulcerative disorders. OralDis 2012 (Epub ahead of print) doi: 10.1111/j.1601-0825.2012.01931.x
6. Riera Matute G, Riera Alonso E. Recurrent aphthous stomatitis in rheu-matology. Reumatol Clin 2011;7(5):323-8.
7. Bagan JV, et al. Recurrent aphthous stomatitis . A study of the clinical char-acteristics of lesions in 93 cases. J Oral Pathol Med 1991;20(8):395-7.
8. Kleinman DV, Swango PA, Niessen LC. Epidemiologic studies of oralmucosal conditions—methodologic issues. Community Dent Oral Epi-demiol 1991;19(3):129-40.
9. Chan MH, Wolf JC. Biopsy techniques and diagnoses & treatment of
mucocutaneous lesions. Dent Clin North Am 56(1):43-73, vii-viii.
10. Murray B, et al. A comparative study of the efcacy of Aphtheal in
the management of recurrent minor aphthous ulceration. J Oral PatholMed, 2005;34(7):413-9.
11. Thomas KT, et al. Periodic fever syndrome in children. J Pediatr1999;135(1):15-21.
12. Thomas KT, Edwards KM. Periodic fever syndrome. Pediatr Infect Dis J1999;18(1):68-9.
13. Keogan MT. Clinical Immunology Review Series: an approach to the pa- tient with recurrent orogenital ulceration, including Behcet’s syndrome.Clin Exp Immunol 2009;156(1):1-11.
14. Chowdhary A, et al. Bipolaris hawaiiensis as etiologic agent of allergicbronchopulmonary mycosis: rst case in a paediatric patient. Med My -col 2011;49(7):760-5.
15. Chattopadhyay A, Chatterjee S. Risk indicators for recurrent aphthousulcers among adults in the US. Community Dent Oral Epidemiol2007;35(2):152-9.
16. Kleinman DV, Swango PA, Pindborg JJ. Epidemiology of oral mucosal le-sions in United States schoolchildren: 1986-87. Community Dent OralEpidemiol 1994;22(4):243-53.
17. Ship II. Epidemiologic aspects of recurrent aphthous ulcerations. OralSurg Oral Med Oral Pathol 1972;33(3):400-6.
18. Oh SH, et al. Comparison of the clinical features of recurrent aphthousstomatitis and Behcet’s disease. Clin Exp Dermatol 2009;34(6):e208-12.
19. Lohrer R, et al. Autoinammatory diseases as cause of wound healing
defects. Hautarzt 2011;62(7):524-33.
20. Hasan A, et al. Dening a T-cell epitope within HSP 65 in recurrent
aphthous stomatitis. Clin Exp Immunol 2002;128(2):318-25.
21. Meighani G, et al. Oral and dental health status in patients with primaryantibody deciencies. Iran J Allergy Asthma Immunol 2011;10(4):289-93.
22. Bazrafshani MR, et al. IL-1B and IL-6 gene polymorphisms encode signif -icant risk for the development of recurrent aphthous stomatitis (RAS).Genes Immun 2002;3(5):302-5.
specialized treatment may also be necessary. TMJ signs and
symptoms should be treated by a trained specialist with tradi- tional measures effective for other forms of TMJ dysfunction,
including physical medicine, jaw appliance, and biobehavioral therapy. If medical management is not effective, surgical treat-ment may be necessary, as it is for other joints in the body.98
Increased prevalence of periodontitis It has been speculated that the existence of systemic inammatory conditions, such
as RA, may contribute to the initiation and progression of the inammatory nature of periodontal disease. Although
the etiologic factors of the 2 diseases may be both commonand distinct (genetic predisposition, bacterial triggers, envi-
ronment factors), the mechanisms that lead to inammatory
bone loss appear to be shared between the 2 disease enti-
ties. To date, a large number of clinical studies have shownan association between periodontitis and RA.99-111 Unfortu-
nately, the studies investigating the association between RAand periodontitis have had a great variability in their selection
criteria, denition of periodontitis and RA, and selection ofcontrols throughout the study populations, so it is difcult
to conclude on the level of association between the 2 con-
ditions. However, most studies conducted to date report alevel of association between periodontitis and RA that range
from an odds ratio of 1.8 to 6.99. The studies performed todate show increased tooth loss and presence and severity
of periodontitis in patients with RA compared with healthysubjects.112 Some, but not all, studies have evaluated the level
of oral hygiene in patients, by recording plaque index. The im-paired manual dexterity in patients with RA may conceivably
contribute to increased oral health issues in this population.
Secondary SS: Close to a third of patients with RA sufferfrom secondary SS,113 and therefore timely diagnosis and ap-propriate management of SS-related disease is important in
this population (see SS section).
Clinical management recommendations:
Successful management of RA-related oral disease dependson accurate diagnosis and referral to appropriate dental spe-
cialists. Knowledge of the potential involvement of the TMJ joint, particularly in juvenile arthritis will help the generaldentist suspect and recognize potential signs and symptoms
of TMJ dysfunction. Additionally, careful and clinical examina-
tion with a particular focus on the evaluation of periodontalhealth and signs/symptoms of xerostomia will aid in the di-agnosis and treatment of disease-related periodontitis or SS.
Finally, the dental provider should address difculties in per -forming oral hygiene in patients with RA that are related to
their impaired manual dexterity and recommend appropriatemeasures, including the use of an electrical tooth brush, sup-
portive oral rinses, and more frequent dental visits.
-
8/9/2019 Oral Manifestation
16/18
280Volume 12, Supplement 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
44. Pittock S, et al. The oral cavity in Crohn’s disease. J Pediatr2001;138(5):767-71.
45. Weinstein TA, Sciubba JJ, Levine J. Thalidomide for the treatment oforal aphthous ulcers in Crohn’s disease. J Pediatr Gastroenterol Nutr1999;28(2):214-6.
46. Blazar BR, Murphy WJ, Abedi M. Advances in graft-versus-host disease
biology and therapy. Nat Rev Immunol 2012;12(6):443-58.
47. Filipovich AH, et al. National Institutes of Health consensus develop-ment project on criteria for clinical trials in chronic graft-versus-hostdisease: I. Diagnosis and staging working group report. Biol Blood Mar-row Transplant 2005;11(12):945-56.
48. Pasquini MC, Wang Z, Horowitz MM, Gale RP. 2010 repor t from the
Center for International Blood and Marrow Transplant Research (CIB-MTR): current uses and outcomes of hematopoietic cell transplants forblood and bone marrow disorders. Clin Transpl 2010:87-105.
49. Horwitz ME, Sullivan KM. Chronic graft-versus-host disease. Blood Rev,
2006;20(1):15-27.
50. Schuber t MM, Correa ME. Oral graft-versus-host disease. Dent ClinNorth Am 2008;52(1):79-109, viii-ix.
51. Flowers ME, et al. Comparative analysis of risk factors for acute graft-versus-host disease and for chronic graft-versus-host disease ac-cording to National Institutes of Health consensus criteria. Blood2011;117(11):3214-9.
52. Barnes DW, Loutit JF, Micklem HS. “Secondar y disease” of radiationchimeras: a syndrome due to lymphoid aplasia. Ann N Y Acad Sci,1962;99:374-85.
53. Billingham RE. The biology of graft-versus-host reactions. Harvey Lect1966;62:21-78.
54. Imanguli MM, et al. Increased T-bet+ cytotoxic effector s and type I in- terferon-mediated processes in chronic graft-versus-host disease of theoral mucosa. Blood 2009;113(15):3620-30.
55. Pavletic SZ, Baird K. Chronic graft versus host disease. Curr Opin He-
matol 2006;13(6):426-435.
56. Couriel D, et al. Ancillar y therapy and supportive care of chronic graft-versus-host disease: National Institutes of Health consensus develop-ment project on criteria for clinical trials in chronic graft-versus-hostdisease: V. Ancillary Therapy and Supportive Care Working Group Re-port. Biol Blood Marrow Transplant 2006;12(4):375-96.
57. Fassil B, Mays, Edwards, Baird, Steinberg, Williams, et al. Oral chronicgraft-vs.-host disease characterization using the NIH scale. J Dent Res
2012. In press(Article # 450881).
58. Jacobsohn D, et al. Weight loss and malnutrition in patients with chronicgraft-versus-host disease. Bone Marrow Transplant 2002;(29):231-236.
59. Nagler RM, Nagler A. Pilocarpine hydrochloride relieves xerostomia in
chronic graft-versus-host disease: a sialometrical study. Bone MarrowTransplant 1999;23(10):1007-11.
60. Singhal S, et al. Pilocarpine hydrochloride for symptomatic relief of xe-rostomia due to chronic graft-versus-host disease or total-body irradia- tion after bone-marrow transplantation for hematologic malignancies.Leuk Lymphoma 1997;24(5-6):539-43.
61. Sciubba JJ. Autoimmune oral mucosal diseases: clinical, etiologic,diagnostic, and treatment considerations. Dent Clin North Am2011;55(1):89-103.
62. Ramos-e-Silva M, Ferreira A, Jacques CM. Oral involvement in auto-immune bullous diseases. Clin Dermatol 2011;29(4):443-54.
23. Gupta SK, et al. Epidemiological evaluation of recurrent stomatitis, ni- trates in drinking water, and cytochrome b5 reductase activity. Am JGastroenterol 1999;94(7):1808-12.
24. Ship JA, et al. Recurrent aphthous stomatitis. Quintessence Int2000;31(2):95-112.
25. Volkov I, et al. Effectiveness of vitamin B12 in treating recurrent aph- thous stomatitis: a randomized, double-blind, placebo-controlled trial. J
Am Board Fam Med 2009;22(1):9-16.
26. Ference JD, Last AR. Choosing topical corticosteroids. Am Fam Physi-cian 2009;79(2):135-40.
27. Elad S, et al. Topical immunomodulator s for management of oral muco-sal conditions, a systematic review. Part II: miscellaneous agents. ExpertOpin Emerg Drugs 2011;16(1):183-202.
28. Cheng S, Murphy R. Refractory aphthous ulceration treated with tha-lidomide: a report of 10 years’ clinical experience. Clin Exp Dermatol2012;37(2):132-5.
29. O’Neill ID. Efcacy of tumour necrosis factor-alpha antagonists in aph- thous ulceration: review of published individual patient data. J Eur AcadDermatol Venereol 2012;26(2):231-5.
30. Mendoza-Pinto C, et al. Etiopathogenesis of Behcet’s disease. Autoim-mun Rev 2010;9(4):241-5.
31. Davatchi F, et al. How to deal with Behcet’s disease in daily practice. Int J Rheum Dis 2010;13(2):105-16.
32. Kaneko F, et al. Behcet’s disease (Adamantiades-Behcet’s disease). ClinDev Immunol 2011;2011:681956.
33. International Study Group for Behcet’s Disease. Criter ia for diagnosis ofBehcet’s disease. Lancet 1990;335(8697):1078-80.
34. Mumcu G, et al. Oral health related quality of life is affected by disease
activity in Behcet’s disease. Oral Dis 2006;12(2):145-51.
35. Karacayli U, et al. The close association between dental and periodontal treatments and oral ulcer course in Behcet’s disease: a prospective clini-
cal study. J Oral Pathol Med 2009;38(5):410-5.
36. Tukel T, et al. Crohn disease: frequency and nature of CARD15 muta- tions in Ashkenazi and Sephardi/Oriental Jewish families. Am J Hum
Genet 2004;74(4):623-36.
37. Loftus EV Jr. Clinical epidemiology of inammatory bowel disease: in-cidence, prevalence, and environmental inuences. Gastroenterology
2004;126(6):1504-17.
38. Friedr ichs F, et al. The Crohn’s disease susceptibility gene DLG5as a member of the CARD interaction network. J Mol Med (Berl)2008;86(4):423-32.
39. Tsianos EV, Katsanos KH, Tsianos VE. Role of genetics in the di-agnosis and prognosis of Crohn’s disease. World J Gastroenterol2011;17(48):5246-59.
40. Harty S, et al. A prospective study of the oral manifestations of Crohn’sdisease. Clin Gastroenterol Hepatol 2005;3(9):886-91.
41. Jose FA, et al. Development of extraintestinal manifestations in pedi-atric patients with inammatory bowel disease. Inamm Bowel Dis
2009;15(1):63-8.
42. Grossner-Schreiber B, et al. Prevalence of dental caries and periodon- tal disease in patients with inammatory bowel disease: a case-control
study. J Clin Periodontol 2006;33(7):478-84.
43. Rikardsson S, et al. Perceived oral health in patients with Crohn’sdisease. Oral Health Prev Dent 2009;7(3):277-82.
-
8/9/2019 Oral Manifestation
17/18
September 2012281
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
84. Paton NI. Infections in systemic lupus erythematosus patients. Ann AcadMed Singapore 1997;26(5):694-700.
85. Grimaldo-Carjevschi M, Lopez-Labady J, Villarroel-Dorrego M. Squa-mous cell carcinoma on the palate in a patient with systemic lu-pus erythematosus: case report and review of literature. Lupus2011;20(5):519-22.
86. Tao J, et al. Squamous cell carcinoma complicating discoid lupus erythe-
matosus in Chinese patients: review of the literature, 1964-2010. J AmAcad Dermatol 2012;66(4):695-6.
87. Franks AL, Slansky JE. Multiple associations between a broad spectrumof autoimmune diseases, chronic inammatory diseases and cancer. An- ticancer Res 2012;32(4):1119-36.
88. Carroll CL, Fleischer AB Jr. Tacrolimus ointment: the treatment of atopicdermatitis and other inammatory cutaneous disease. Expert Opin
Pharmacother 2004;5(10):2127-37.
89. Walker SL, Kirby B, Chalmers RJ. Use of 0.1% tacrolimus ointment inpatients with various forms of lupus erythematosus. Eur J Dermatol2002;12(4):387-8; author reply 389.
90. Walker SL, Kirby B, Chalmers RJ. The effect of topical tacrolimus onsevere recalcitrant chronic discoid lupus erythematosus. Br J Dermatol2002;147(2):405-6.
91. Lo JS, Berg RE, Tomecki KJ. Treatment of discoid lupus erythematosus. Int J Dermatol 1989;28(8):497-507.
92. Deeming GM, Collingwood J, Pemberton MN. Methotrexate and oralulceration. Br Dent J 2005;198(2):83-5.
93. Sagar P, Shailam R, Nimkin K. Avascular necrosis of the metacarpalhead: a report of two cases and review of literature. Pediatr Radiol2010;40(12):1895-901.
94. Gabriel SE, et al. Is rheumatoid arthritis care more costly when pro-vided by rheumatologists compared with generalists? Arthritis Rheum2001;44(7):1504-14.
95. Gabriel SE. The epidemiology of rheumatoid arthritis. Rheum Dis Clin
North Am 2001;27(2):269-81.
96. McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med 2011;365(23):2205-19.
97. Lipsky PE. Rheumatoid arthr itis. In: Harrison’s Principals of Internal Med-icine. Fauci AS, Kasper DL, Hauser SL, Longo DL, Jamesong JL, Loscalzo
J, editors. New York, NY, McGraw-Hill Professional; 2008.
98. Scrivani SJ, Keith DA, Kaban LB. Temporomandibular disorders. N Engl JMed 2008;359(25):2693-705.
99. de Pablo P, et al. Periodontitis in systemic rheumatic diseases. Nat RevRheumatol 2009;5(4):218-24.
100. Tolo K, Jorkjend L. Serum antibodies and loss of periodontal bone in pa- tients with rheumatoid arthritis. J Clin Periodontol 1990;17(5):288-91.
101. Kasser UR, et al. Risk for periodontal disease in patients with longstand-ing rheumatoid arthritis. Arthritis Rheum 1997;40(12):2248-51.
102. Mercado F, et al. Is there a relationship between rheumatoid arthritisand periodontal disease? J Clin Periodontol 2000;27(4):267-72.
103. Mercado FB, et al. Relationship between rheumatoid arthritis and peri-odontitis. J Periodontol 2001;72(6):779-87.
104. Abou-Raya A, Abou-Raya S, Abu-Elkheir H. Periodontal disease and rheu-matoid arthritis: is there a link? Scand J Rheumatol 2005;34(5):408-10.
105. Abou-Raya S, et al. Rheumatoid arthritis, periodontal disease and coro-nary ar tery disease. Clin Rheumatol 2008;27(4):421-7.
63. Mavragani CP, Moutsopoulos HM. The geoepidemiology of Sjogren’ssyndrome. Autoimmun Rev 2010;9(5):A305-10.
64. Moutsopoulos NM, Moutsopoulos HM. Therapy of Sjogren’s syndrome.Springer Semin Immunopathol 2001;23(1-2):131-45.
65. Mavragani CP, Moutsopoulos NM, Moutsopoulos HM. The managementof Sjogren’s syndrome. Nat Clin Pract Rheumatol 2006;2(5):252-61.
66. Vitali C, et al. Assessment of the European classication criteria for Sjo-gren’s syndrome in a series of clinically dened cases: results of a pro-spective multicentre study. The European Study Group on DiagnosticCriteria for Sjogren’s Syndrome. Ann Rheum Dis 1996;55(2):116-21.
67. Vitali C, Moutsopoulos HM, Bombardier i S. The European CommunityStudy Group on diagnostic criteria for Sjogren’s syndrome. Sensitivityand specicity of tests for ocular and oral involvement in Sjogren’s syn-drome. Ann Rheum Dis 1994;53(10):637-47.
68. Shiboski SC, et al. American College of Rheumatology classication cri- teria for Sjogren’s syndrome: a data-driven, expert consensus approachin the Sjogren’s International Collaborative Clinical Alliance Cohort. Ar- thritis Care Res (Hoboken) 2012;64(4):475-87.
69. Ramos-Casals M, et al. Topical and systemic medications for the treat-ment of primary Sjogren’s syndrome. Nat Rev Rheumatol 2012; 8:399-411.
70. Lourenco SV, et al. Lupus erythematosus: clinical and histopathologicalstudy of oral manifestations and immunohistochemical prole of the
inammatory inltrate. J Cutan Pathol 2007;34(7):558-64.
71. Callen JP. Clinically relevant information about cutaneous lupus erythe-matosus. Arch Dermatol 2009;145(3):316-9.
72. Akin MA, et al. Review of literature for the striking clinic picture seenin two infants of mothers with systemic lupus erythematosus. J MaternFetal Neonatal Med 2011;24(8):1022-6.
73. Jonsson R, et al. Oral mucosal lesions in systemic lupus erythemato-sus—a clinical, histopathological and immunopathological study. J Rheu-matol 1984;11(1):38-42.
74. Schiodt M. Oral manifestations of lupus erythematosus. Int J Oral Surg1984;13(2):101-47.
75. Lutalo PM, D’Cruz DP. Belimumab for the management of systemic
lupus erythematosus. Expert Opin Biol Ther 2012; 12: 957-63.
76. Lopez-Labady J, et al. Oral manifestations of systemic and cutaneous
lupus erythematosus in a Venezuelan population. J Oral Pathol Med
2007;36(9):524-7.
77. Hallegua DS, Wallace DJ. Gastrointestinal manifestations of systemiclupus erythematosus. Curr Opin Rheumatol 2000;12(5):379-85.
78. Lutalo PM, D’Cruz DP. Belimumab for the management of systemic
lupus erythematosus. Expert Opin Biol Ther 2012;12(7):957-63.
79. Zandman-Goddard G, et al. Environment and lupus-related diseases.
Lupus 2012;21(3):241-50.
80. Dorner T, Giesecke C, Lipsky PE. Mechanisms of B cell autoimmunity inSLE. Arthritis Res Ther 2011;13(5):243.
81. Taylor KE, et al. Specicity of the STAT4 genetic association for severe
disease manifestations of systemic lupus erythematosus. PLoS Genet2008;4(5):e1000084.
82. Munoz-Corcuera M, et al. Oral ulcers: clinical aspects. A tool for derma- tologists. Part II. Chronic ulcers. Clin Exp Dermatol 2009;34(4):456-61.
83. Sayarlioglu M, et al. Risk factors for avascular bone necrosis in patientswith systemic lupus erythematosus. Rheumatol Int 2012;32(1):177-82.
-
8/9/2019 Oral Manifestation
18/18
282V l 12 S l 1
JOURNAL OF EVIDENCE-BASED DENTAL PRACTICE SPECIAL ISSUE— PERIODONTAL AND IMPLANT TREATMENT
106. Albandar JM. Some predictors of radiographic alveolar bone height re-duction over 6 years. J Periodontal Res 1990;25(3):186-92.
107. Al-Shammari KF, et al. Risk indicators for tooth loss due to periodontaldisease. J Periodontol 2005;76(11):1910-8.
108. Pischon, N, et al. Association among rheumatoid arthritis, oral