Oral Histology - Alvelor bone
40
Alvelor bone
-
Upload
hamzeh-albattikhi -
Category
Education
-
view
168 -
download
14
Transcript of Oral Histology - Alvelor bone

Alvelor bone
Functions1. As a supporting tissue
2. Gives attachments to muscles
3. Reservoir for ions especially calcium
One of the most important properties of bone is its “ plasticity” : model/remodel according to it’s functional demands.
Alveolar bone depends on the presence of teeth for its development.

Classification of bone1. Developmentally
A. Endochondral bone B. Intramembranous
2. Histologically
A. compact (cortical) 80% B. cancellous(spongy): 20%
The immature bone is called woven bone; it has higher number of osteocytes , formed rapidly , has high turnover rate.
Seen at fracture sites, subsequently converted to adult lamellar bone.


Compact bone lining tooth socket called cribriform plate , it’s appearance is produced by numerous vascular canals (Volkmann’s canals).

Chemical properties of bone
• Mineralized connective tissue.
• 60% is inorganic material, 25% organic material, 15% water.
• Consists of carbonated hydroxyapatite which gives rigidity.
• The mineral is in the form of needle –like crystallites.
• Organic matrix is about 90% collagen type I .
• Collagen type III, type v are present in immature or healing bone.
• Presence of collagen is important in resisting loads to prevent fracture.
• Mutations in collagen genes give rise to inherited condition such as osteogenesis imperfecta, where the bone strength is reduced.

Non collagenous proteins
• comprise 10% of the total organic content.
• Most are produced by bone cells , others are derived from other sources like blood ( e.g cytokines, growth factors).
1. Proteoglycans
2. Glycoproteins
3. Bone Gla containing proteins
4. Serum proteins
Some have bone formative aspects while others are involved with bone resorption.
osteoid• Newly deposited, unmineralized bone matrix on the surface of active bone
formation.
• Thickness of 5-10 μm
• Consists of type I collagen , embedded in ground substances of proteoglycans and glycoproteins.
• Initial mineralization takes place by the osteoblast from whose cell membrane vesicles are budded off to the osteoid.

Haversian system/Osteon

Cell types in boneA. Osteoblasts
Mesenchymal origin.
Found in active bone.
functions
I. Secrete the organic matrix of bone.
II. Secretes molecules controlling it’s own activity e.g. growth factors.
III. Release molecules that affect the activity of osteoclasts.
IV. Have receptors for hormones that help regulate bone metabolism ; parathyroid hormone, sex steroids.


B. Osteocytes
They are the entrapped osteoblasts within the bone.
In constant communication with osteoblasts and bone lining cells.
They have numerous slender processes of actin filaments that extend to the canaliculi.
The processes of osteocytes are connected by gap junctions and the superficial ones are in contact with cells lining bone surface.
They are uniformly distributed and undergo apoptosis.
Regarded as primary mechanoreceptors in cases of stress.


C. Bone lining cells
On the surface of bone when not in formative or resorptive phase .
Flattened cells, with no osteoid present.
Functions:
1. Calcium and phosphate metabolism.
2. Protect surface from resorptive activity of osteoclasts.
3. Initiate bone remodeling.
4. Could be a source of osteoproginetor cells.
D.Osteoprogenitor cells
They are stem cells.
Found in the layer of cells beneath osteoblasts , periodontal ligament or in marrow spaces.
Their life cycle may involve up to 8 divisions before reaching osteoblast.

E.Osteoclasts• Derived from monocytes/macrophage linage ( hematopoietic origin).
• Resorbing surfaces are called Howship’s lacunae , osteoclasts lie in it.

Osteoclasts when active:
• Ruffled border (near bone).
• Sealing zone.
• Functional secretory domain.
• Basolateral surface.

• Osteoclasts have important receptors for calcitonin, prostaglandins, RANK and parathyroid hormone.
• Resorption occurs in two stages : first the mineral stage is removed .
later the remaining organic matrix is removed.
To provide low PH for dissolving the mineral stage, osteoclasts secrete protons across ruffled border by means of ATPase proton pump.
The organic matrix is then exposed in the resorbing lacunae then degraded by enzymes (MMP, lysosomal and non-lysosomal enzymes) .

Formation of osteoblasts• Stem cells of osteoblast are derived from perivascular cells in the PDL and adjacent
bone marrow.
• Process of bone formation requires:
1. Cell proliferation.
2. Synthesis and secretion of extracellular matrix.
3. Mineralization of tissue.
This process is characterized by low proliferative capacity and high degree of differentiation.

• Nuclear transcription core binding factor 1 is the earliest marker to indicate that the stem cell is processing along an osteogenic phenotype.
• Nuclear transcription factor regulates production of a number of important protein products in bone matrix.
• Osteoprogenitor cells are identified by the progressive expression of molecules such as collagen type 1 , alkaline phosphatase and osteopontin.
• Growth factors, cytokines, transcription factors and hormones regulate the differentiation of osteoblasts.


Formation of osteoclasts• C-Fos, PU-1 are important transcription factors for osteoclasts stem cells differentiation.
• M-CSF and receptor activator of nuclear factor к B ligand (RANKL) which are released by osteoblasts and are important for differentiation of myeloid cells to the mononuclear osteoclast precursor .
• Osteoblast secretes osteoprotegrin which binds with RANKL and inhibits osteoclast formation.
• RANKL/RANK system: fusion of mononuclear osteoclast to multinuclear osteoclasts.
• Two additional factors affect osteoclastic activity :
• A- Acidification B- Hypoxia

Acidification :
• Osteoclasts are inactive at PH 7.4 , however if PH drops to 7 resorption increases ,and osteoclastic agents such as RANKL get activated.
Hypoxia:
• Increases osteoclastic activity.
• Release factors such as prostaglandins , vascular endothelial growth factors.

Bone remodelling• 4 stages:
1. Resorption: recruitment, migration, and activation of osteaoclasts causing bone resorption.
2. Reversal: cessation of resorption and disappearance of osteoclasts by apoptosis or migration , the site becomes occupied by mononuclear cells.
3. Formation: osteoblasts recruitment, migration , differentiation and formation of new bone in resorption site.
4. Resting: formation of new bone ceases and the surface is lined by a flattened layer of cells.


• Initial cutting zone of osteoclastic activity moves along the center of the osteon, followed by closing zone of osteoblastic activity.
• Initially before resorption any osteoprogenitor cells or osteoblast have to retract or migrate away from the surface in order to expose bone surface, because osteoclasts are activated when are in contact with the mineralized bone surface.
• Load causing modelling/remodelling of bone are intermittent rather than continuous; to maintain constant bone mass relatively few loading cycles are required.
• Cell processes cell membrane deform following loading, signals transducted via cell membranes to simulate 2nd messengers.
• These changes release molecules initiate osteogenic response such as ILs,nitric oxide, certain G.Fs.
• PH, oxygen, tension also affect osteogenic responses.
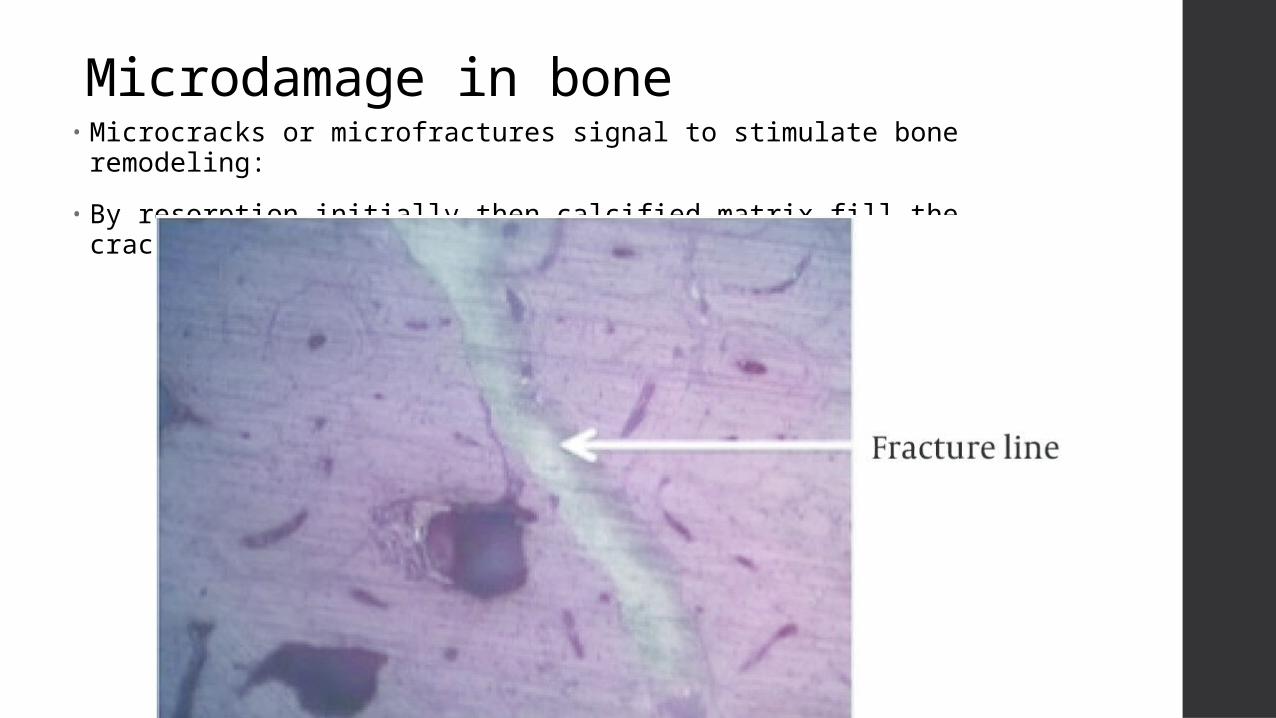
Microdamage in bone• Microcracks or microfractures signal to stimulate bone remodeling:
• By resorption initially then calcified matrix fill the cracks.

Sharpey fibers entering alveolar bone

Structural lines in bone
Scalloped reversal line: site of change from bone resorption to deposition.
Vertical resting lines: rhythmic bone deposition

Clinical considerations1. Resorption following extraction, bone tends to atrophy because tensile forces
decreases.
2. Ability of bone to remodel after orthodontic treatment.
3. Localized bone loss in periodontal diseases.
4. Osteopetrosis( deficiency in osteoclasts):
• Thick bone
• Difficulty in teeth extraction
• Prevent teeth from eruption
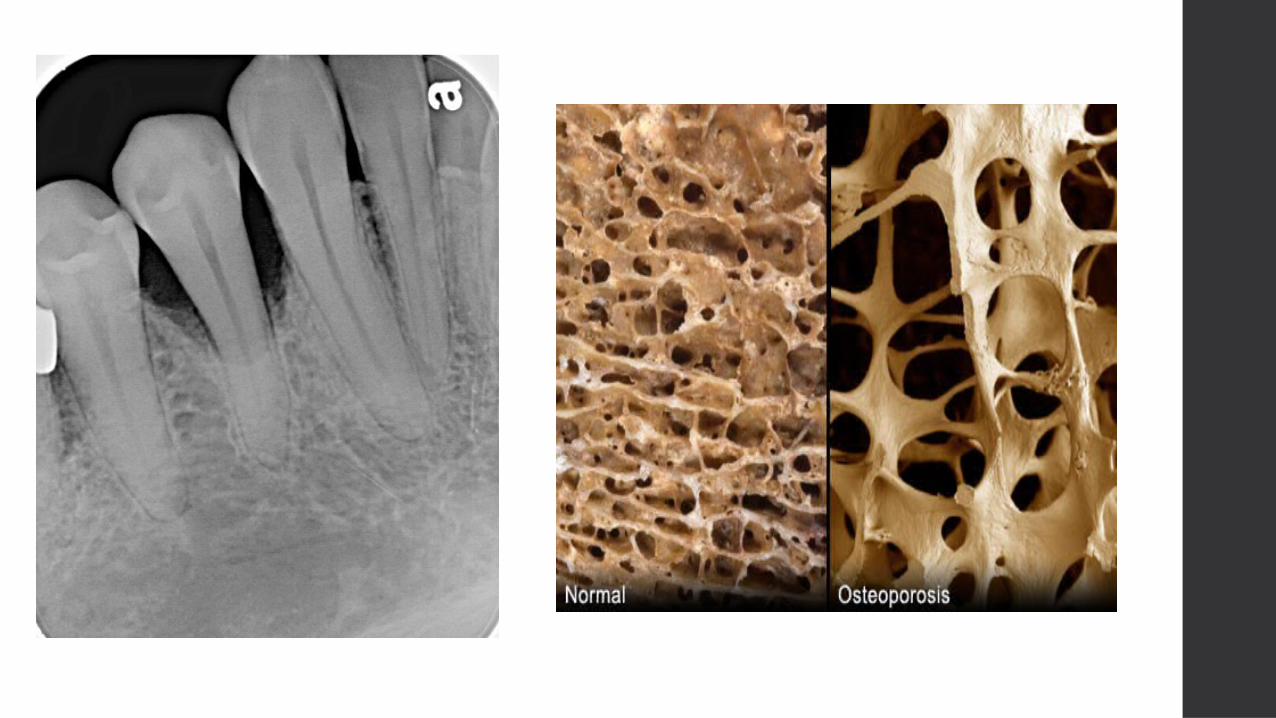
5. Osteoporosis:
• Low bone mass but normal constituents
• Affects trabecular bone ; neck of femur, lumbar vertebrae
• Age related
• Female more than male esp. after menopause


6.In implant dentistry
• osseointegration is important
• Materials commonly used are titanium/ aluminum vanadium alloys.
• Spontaneously formed metal oxide surfaces are critical for osseointegration.
• Narrow surface (20-40 nm) between bone-implant contains non-collagenous bone matrix proteins such as osteopontin, sialoprotein.
Successful retention of implant depends on:
1. Correct surgical technique to reduce trauma.
2. Absence of excessive micromotion following implantation.
3. Factors related to the implant such as shape, topography, stiffness, composition and surface chemistry.


7-Fractures involving face and jaw are common.
8-Trauma and malignant diseases:
Need for larger amount of bone.
Autogenous bone graft (from the same patient).
Allograft(from another person).
Xenograft(from other species).

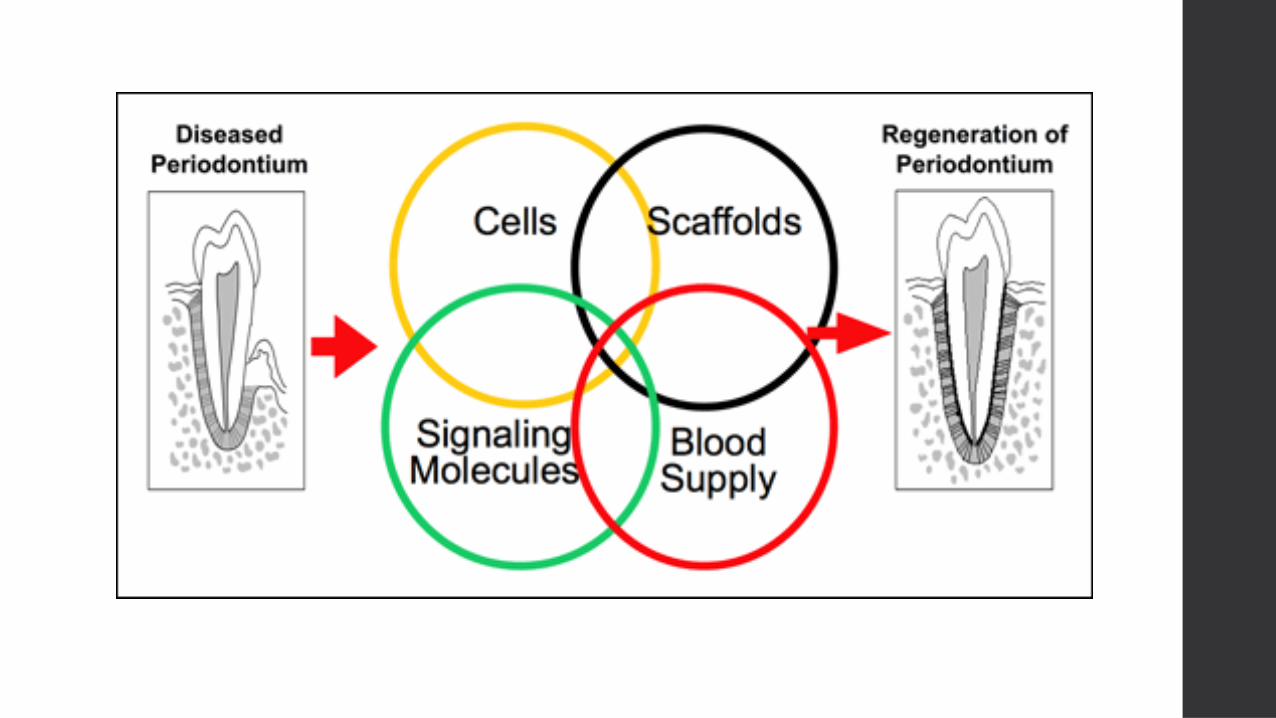
9-tissue engineering:
To substitute bone or provide scaffolds and stimuli to promote healing.
A-The scaffold
*Biocompatible.
*Allow cell migration and differentiation.
*Allow mineralization of the artificial matrix.
*Allow angiogenesis
B-The cells are stem cells
C-Additional molecules to drive osteogenesis ; cytokines and growth factors

B-The cells are stem cells
C-Additional molecules to drive osteogenesis ; cytokines and growth factors.
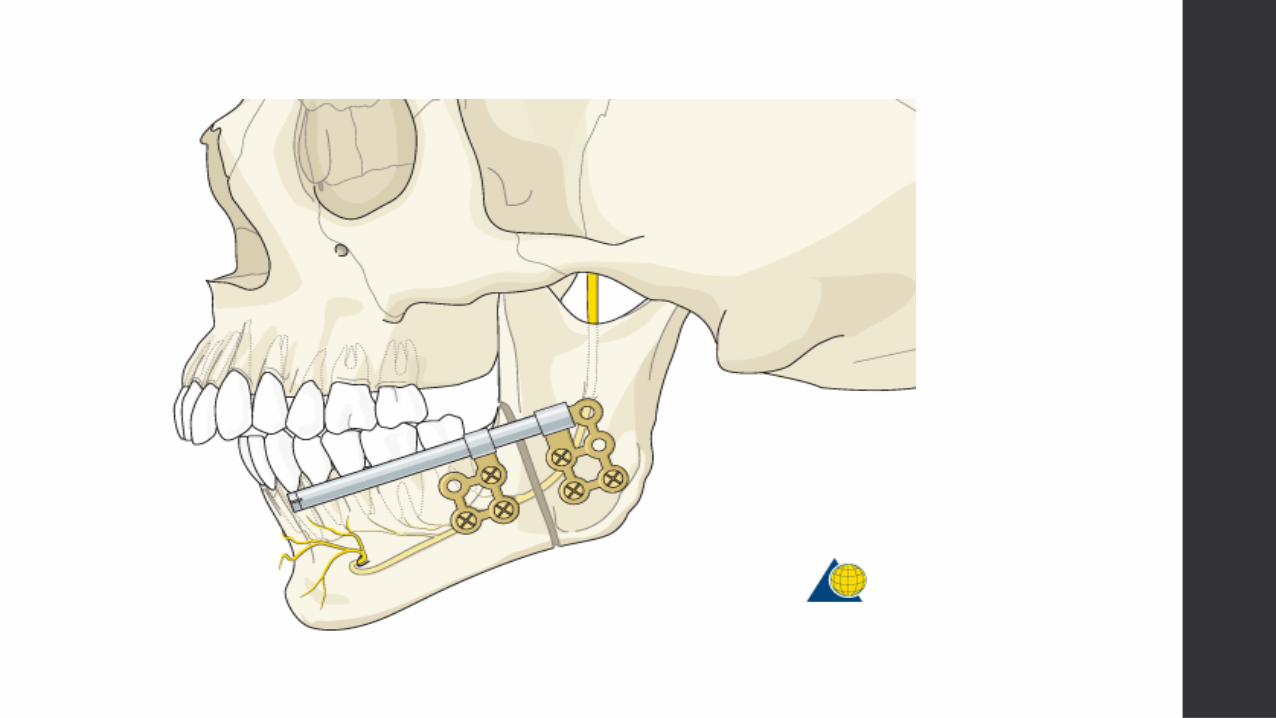
10-Distraction osteogenesis
Technique whereby a bone is sectioned (osteotomy) and after an initial interval of 5-7 days, a slow controlled separation (.5-1mm/day) of the two bone fragments is undertaken to allow length augmentation by the sustained addition of new woven bone at the fracture site formed by tension.
Allow woven bone callus to be reinforced and ultimately replaced by dense bone.
Uses of DO:
1. Increase length of long bone
2. Craniofacial underdevelopment (micrognathia).
3. After extraction, to render site suitable for implant.
Thank you

![Oral Histology Quiz_MCQ[AmCoFam]](https://static.fdocuments.net/doc/165x107/5525aecc4a7959da488b4d75/oral-histology-quizmcqamcofam.jpg)