Oral epithelia - WordPress.comOral epithelia Layers in the oral epithelia (from apical to basal)...
43
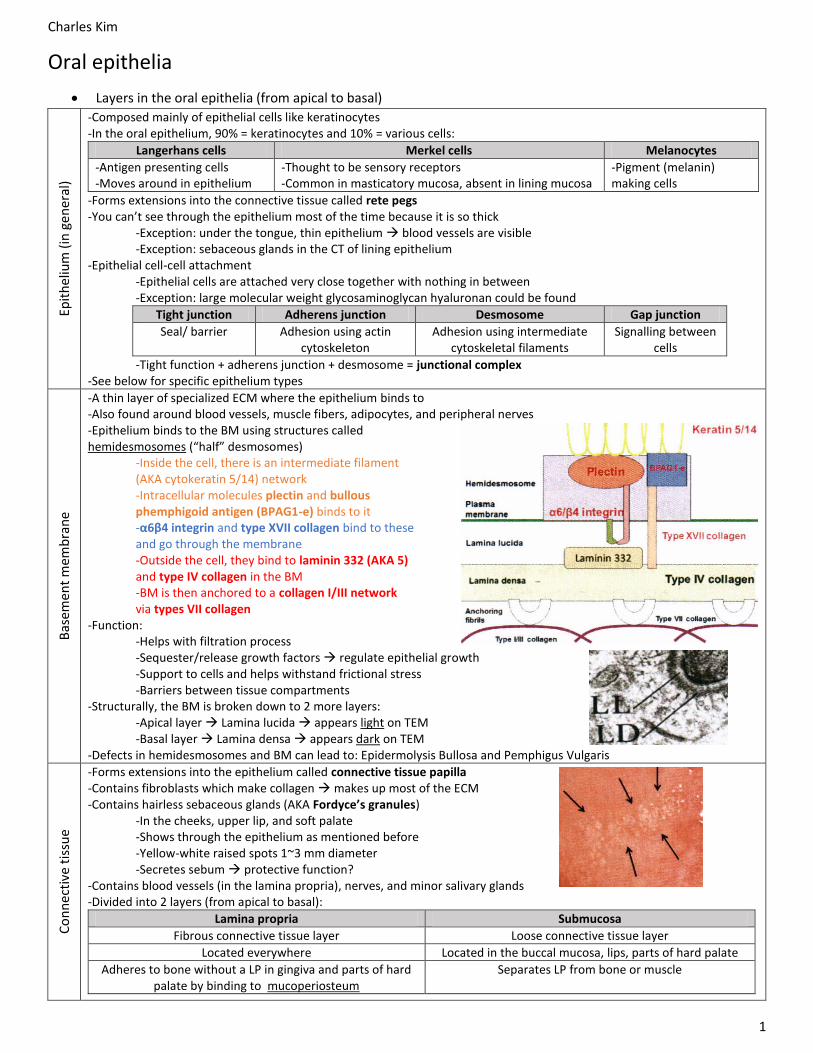
Charles Kim 1 Oral epithelia Layers in the oral epithelia (from apical to basal) Epithelium (in general) -Composed mainly of epithelial cells like keratinocytes -In the oral epithelium, 90% = keratinocytes and 10% = various cells: Langerhans cells Merkel cells Melanocytes -Antigen presenting cells -Moves around in epithelium -Thought to be sensory receptors -Common in masticatory mucosa, absent in lining mucosa -Pigment (melanin) making cells -Forms extensions into the connective tissue called rete pegs -You can’t see through the epithelium most of the time because it is so thick -Exception: under the tongue, thin epithelium blood vessels are visible -Exception: sebaceous glands in the CT of lining epithelium -Epithelial cell-cell attachment -Epithelial cells are attached very close together with nothing in between -Exception: large molecular weight glycosaminoglycan hyaluronan could be found Tight junction Adherens junction Desmosome Gap junction Seal/ barrier Adhesion using actin cytoskeleton Adhesion using intermediate cytoskeletal filaments Signalling between cells -Tight function + adherens junction + desmosome = junctional complex -See below for specific epithelium types Basement membrane -A thin layer of specialized ECM where the epithelium binds to -Also found around blood vessels, muscle fibers, adipocytes, and peripheral nerves -Epithelium binds to the BM using structures called hemidesmosomes (“half” desmosomes) -Inside the cell, there is an intermediate filament (AKA cytokeratin 5/14) network -Intracellular molecules plectin and bullous phemphigoid antigen (BPAG1-e) binds to it -α6β4 integrin and type XVII collagen bind to these and go through the membrane -Outside the cell, they bind to laminin 332 (AKA 5) and type IV collagen in the BM -BM is then anchored to a collagen I/III network via types VII collagen -Function: -Helps with filtration process -Sequester/release growth factors regulate epithelial growth -Support to cells and helps withstand frictional stress -Barriers between tissue compartments -Structurally, the BM is broken down to 2 more layers: -Apical layer Lamina lucida appears light on TEM -Basal layer Lamina densa appears dark on TEM -Defects in hemidesmosomes and BM can lead to: Epidermolysis Bullosa and Pemphigus Vulgaris Connective tissue -Forms extensions into the epithelium called connective tissue papilla -Contains fibroblasts which make collagen makes up most of the ECM -Contains hairless sebaceous glands (AKA Fordyce’s granules) -In the cheeks, upper lip, and soft palate -Shows through the epithelium as mentioned before -Yellow-white raised spots 1~3 mm diameter -Secretes sebum protective function? -Contains blood vessels (in the lamina propria), nerves, and minor salivary glands -Divided into 2 layers (from apical to basal): Lamina propria Submucosa Fibrous connective tissue layer Loose connective tissue layer Located everywhere Located in the buccal mucosa, lips, parts of hard palate Adheres to bone without a LP in gingiva and parts of hard palate by binding to mucoperiosteum Separates LP from bone or muscle
Transcript of Oral epithelia - WordPress.comOral epithelia Layers in the oral epithelia (from apical to basal)...
Charles Kim
1
Oral epithelia
Layers in the oral epithelia (from apical to basal)
Epit
hel
ium
(in
gen
eral
)
-Composed mainly of epithelial cells like keratinocytes -In the oral epithelium, 90% = keratinocytes and 10% = various cells:
Langerhans cells Merkel cells Melanocytes
-Antigen presenting cells -Moves around in epithelium
-Thought to be sensory receptors -Common in masticatory mucosa, absent in lining mucosa
-Pigment (melanin) making cells
-Forms extensions into the connective tissue called rete pegs -You can’t see through the epithelium most of the time because it is so thick -Exception: under the tongue, thin epithelium blood vessels are visible -Exception: sebaceous glands in the CT of lining epithelium -Epithelial cell-cell attachment -Epithelial cells are attached very close together with nothing in between -Exception: large molecular weight glycosaminoglycan hyaluronan could be found
Tight junction Adherens junction Desmosome Gap junction
Seal/ barrier Adhesion using actin cytoskeleton
Adhesion using intermediate cytoskeletal filaments
Signalling between cells
-Tight function + adherens junction + desmosome = junctional complex -See below for specific epithelium types
Bas
emen
t m
emb
ran
e
-A thin layer of specialized ECM where the epithelium binds to -Also found around blood vessels, muscle fibers, adipocytes, and peripheral nerves -Epithelium binds to the BM using structures called hemidesmosomes (“half” desmosomes) -Inside the cell, there is an intermediate filament (AKA cytokeratin 5/14) network -Intracellular molecules plectin and bullous phemphigoid antigen (BPAG1-e) binds to it -α6β4 integrin and type XVII collagen bind to these and go through the membrane -Outside the cell, they bind to laminin 332 (AKA 5) and type IV collagen in the BM -BM is then anchored to a collagen I/III network via types VII collagen -Function: -Helps with filtration process -Sequester/release growth factors regulate epithelial growth -Support to cells and helps withstand frictional stress -Barriers between tissue compartments -Structurally, the BM is broken down to 2 more layers: -Apical layer Lamina lucida appears light on TEM -Basal layer Lamina densa appears dark on TEM -Defects in hemidesmosomes and BM can lead to: Epidermolysis Bullosa and Pemphigus Vulgaris
Co
nn
ecti
ve t
issu
e
-Forms extensions into the epithelium called connective tissue papilla -Contains fibroblasts which make collagen makes up most of the ECM -Contains hairless sebaceous glands (AKA Fordyce’s granules) -In the cheeks, upper lip, and soft palate -Shows through the epithelium as mentioned before -Yellow-white raised spots 1~3 mm diameter -Secretes sebum protective function? -Contains blood vessels (in the lamina propria), nerves, and minor salivary glands -Divided into 2 layers (from apical to basal):
Lamina propria Submucosa
Fibrous connective tissue layer Loose connective tissue layer
Located everywhere Located in the buccal mucosa, lips, parts of hard palate
Adheres to bone without a LP in gingiva and parts of hard palate by binding to mucoperiosteum
Separates LP from bone or muscle

Charles Kim
2
Oral mucosa
Masticatory mucosa Lining mucosa Specialized mucosa
Epithelial traits
-Keratinized (tonofilaments + filagrin) -Fairly thin due to protection
-Non keratinized -Thicker (possibly due to lack of keratin?)
Lips -Keratin to no keratin (moving out to in)
Gustatory -Masticatory but with papillae for taste buds
Submucosal traits
-Lamina propria present -Submucosa mostly absent -Deep rete pegs + papilla
-Lamina propria present -Submucosa varies -Flat/fewer rete pegs + papilla
-Deeper rete pegs than skin
-LP only, no SM -Deep rete pegs and papillae
Characteristic
-Firmly attached to underlying bone -Not mobile -Resists mechanical compression and friction
-Flexible, distensible, compressible
-CT is rich in blood vessels colours the lips “red” called the vermillion border -Has minor salivary glands
-Has taste buds which are involved in taste sensation
Areas covered
-Gingiva (up to the muco gingival junction) -Hard palate
-Everywhere else (cheeks, vestibule, floor, ventral tongue, soft palate) -Alveolar mucosa (below MGJ)
-Lips -Dorsal tongue
Structures
Why does oral mucosa look different in certain areas?
Disease -Inflammation, disease process
Degree of pigmentation -Due to varying melanocyte activity
Specialized structures -Examples: Fordyce’s granules, papillae on tongue, lingual tonsils
Density of blood vessels
Presence of keratin -Keratinized areas like gingiva whitish appearance -Linea alba (white line) formation due to induced keratinisation of buccal mucosa
Thickness of epithelium -Buccal mucosa is much thicker than floor of the mouth
Charles Kim
3
Oral mucosa is unique. It is the transition between skin and the GI tract
o Therefore, it has traits from each area and also some unique traits on its own
Similar to GI tract Similar to skin Distinct from skin
-Moist and bathed in fluid -High rate of tissue turnover
-Keratinized stratified squamous epithelium exists -Basement membrane linking epidermis to CT -Fibrous CT exists under epithelium -Physically stron bg, distensible, and flexible
-Oral mucosa is thicker, but 10x more permeable -Turnover is 1~3 wks (4~10 wks in skin) -Longer rete pegs/papillae than skin -No hair follicles or sweat glands -Minor salivary glands exist
Epithelia in general
o Types of epithelium
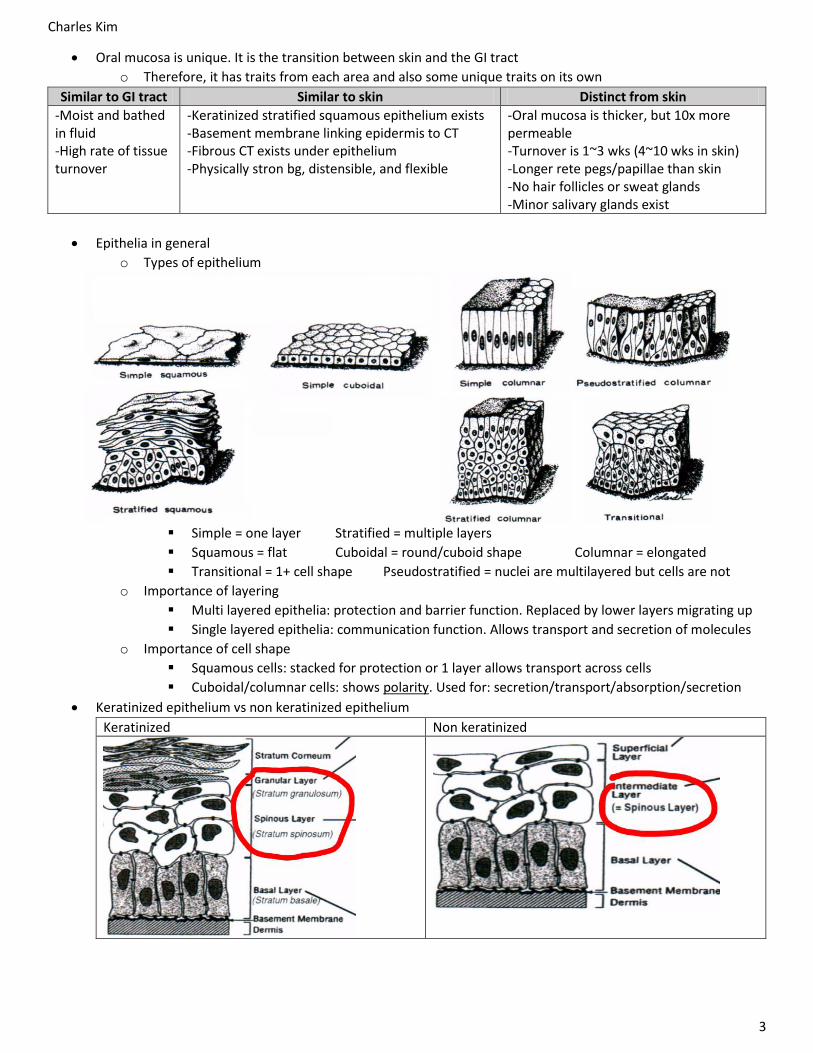
Simple = one layer Stratified = multiple layers
Squamous = flat Cuboidal = round/cuboid shape Columnar = elongated
Transitional = 1+ cell shape Pseudostratified = nuclei are multilayered but cells are not
o Importance of layering
Multi layered epithelia: protection and barrier function. Replaced by lower layers migrating up
Single layered epithelia: communication function. Allows transport and secretion of molecules
o Importance of cell shape
Squamous cells: stacked for protection or 1 layer allows transport across cells
Cuboidal/columnar cells: shows polarity. Used for: secretion/transport/absorption/secretion
Keratinized epithelium vs non keratinized epithelium
Keratinized Non keratinized
Charles Kim
4
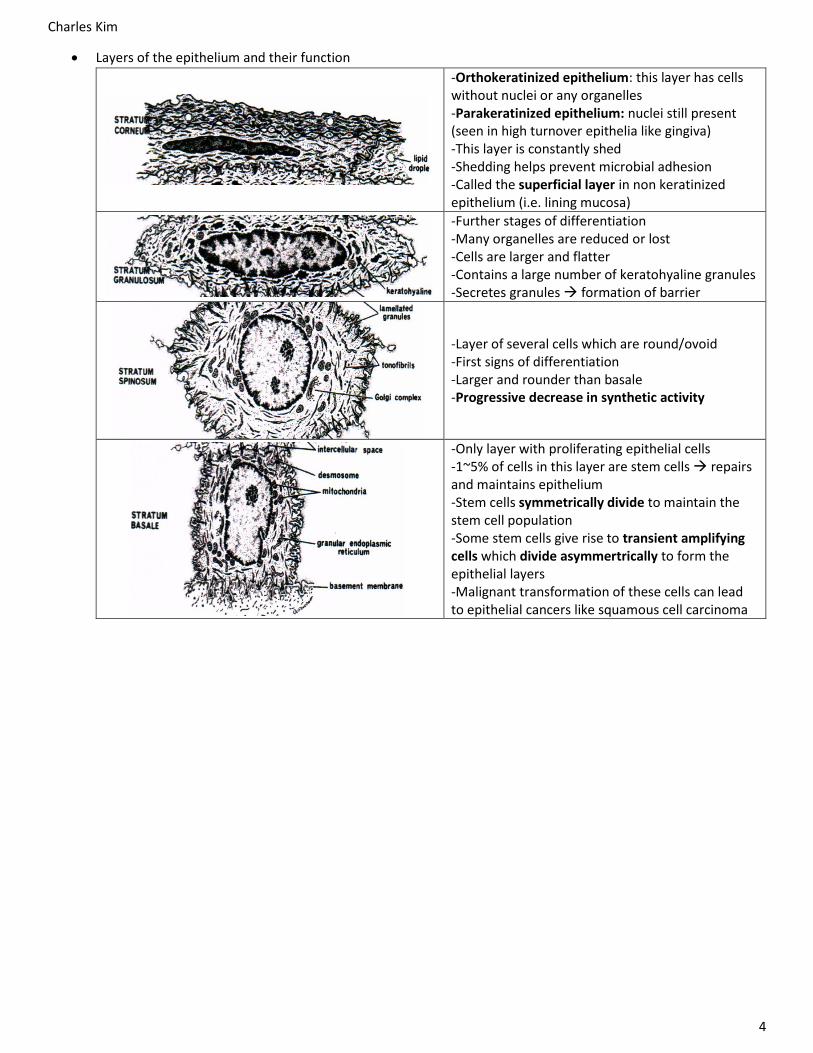
Layers of the epithelium and their function
-Orthokeratinized epithelium: this layer has cells without nuclei or any organelles -Parakeratinized epithelium: nuclei still present (seen in high turnover epithelia like gingiva) -This layer is constantly shed -Shedding helps prevent microbial adhesion -Called the superficial layer in non keratinized epithelium (i.e. lining mucosa)
-Further stages of differentiation -Many organelles are reduced or lost -Cells are larger and flatter -Contains a large number of keratohyaline granules -Secretes granules formation of barrier
-Layer of several cells which are round/ovoid -First signs of differentiation -Larger and rounder than basale -Progressive decrease in synthetic activity
-Only layer with proliferating epithelial cells -1~5% of cells in this layer are stem cells repairs and maintains epithelium -Stem cells symmetrically divide to maintain the stem cell population -Some stem cells give rise to transient amplifying cells which divide asymmertrically to form the epithelial layers -Malignant transformation of these cells can lead to epithelial cancers like squamous cell carcinoma

Charles Kim
5
Saliva
Components and function
o Volume: 600~1000mL/day (>90% water)
o Contains ions: Na, Ca, Mg, K, Cl, HCO3, HPO4, SCN, F
o Contains proteins: mucins, serum albumin
o Contains basic molecules: glucose, amino acids, lipids
o Contains immune proteins: IgA, IgM, IgG, lysozyme, defensins, lactoferrin, peroxidase, SLPI
o Contains epidermal growth factor
Function Component
Tissue repair Growth factors
-Maintains the taste buds Taste
Water Lubrication
Mucins -Family of ~20 genes -Codes for highly glycosylated glycoproteins. Glycosylation is mainly oligosaccharides (negatively charged!) -Packed in golgi released by secretion rheological action (attracts water) hydrates expansion -Functions: traps bacteria, ↓ dessication -Size: cross links to multimers (20~40 MDa)
Digestion
Amylase: Digests starch molecules into sugar monomers Lipase: Digests triglycerides into fatty acids + glycerol
Antimicrobial Lysozyme -Released by macrophages
Other proteins -Lactoferrin (depletes iron) -IgA/M/G, defensins, peroxidase -Secretory leukocyte protease inhibitor
Tooth integrity
Basic molecules: -Calcium -Phosphate -Fluoride
Pellicle proteins -1st stage (10~20nm): statherin, histatins, acidic proline rich proteins stick to the enamel -2nd stage (100-1000nm): knotted and globular like structures aggregate -Prevents Ca and PO from diffusing out -Also has carbonic anhydrase
Buffering Basic molecules: bicarbonate, urea, ammonia, phosphate Basic proteins .
Production of saliva
o Minor glands
Constitutively makes mucous-like saliva all over the submucosa (600~1000 in the mouth!)
In the submucosal layer except for the gingiva or the hard palate
o Major glands
Parotid gland Submandibular gland Sublingual gland Combined
Resting flow rate
0.04 0.1 0.2-0.4
Stimulated flow rate
1-2 0.8 2-5
pH 6.0~7.8 6.7~7.4
Type of saliva
Serous Mixed Mucous

Charles Kim
6
Structure of the salivary gland
o There are 3 types of end pieces: SEROUS ONLY, MUCOUS ONLY, MUCOUS W. SEROUS DEMILUNE
o Myoepithelial cells constrict and release the secretions
o Striated duct cells are intercalated cuboidal cells which modify the saliva. They also act as stem cells
How do striated duct cells modify saliva?
o Ionic exchange:
Na and Cl are taken out
H and HCO3 are added
Saliva is hypotonic
o Due to this intensive transport system, SD cells
have a ton of mitochondria and tight junctions
o Other additions:
Lysozymes and lactoferrin
Staining properties
o Hematoxylin: appears dark blue and binds to acidic/negative structures like DNA/RNA
o Eosin: appears pink and binds to basic/positive structures like most proteins
o Formalin: cell slides are treated with this to cross-link proteins (including collagen). However,
polysaccharides will dissolve away and appear as blank in slides
o H&E staining is the most common but others exist (PAS, alcian blue, toluidine blue, etc)
Mucous glands Serous glands
Stained with PAS + AB
PAS + AB bind Dark blue
PAS only binds Pink
Stained with H&E
Washed out
Stained

Charles Kim
7
Embryonic development (head)
Introduction
o Human development is divided into 2 main stages: embryo and fetus
o Embryo consists of the first 56 days of development
o Embryo is further divided into 23 stages
The face is formed in stages 17/18/19 (days 42-51)
o Not required to know all the stages in detail
Certain stages of development have a risk of anomalies (Moore and Persaud 6th edition)
Placental structures
o The fetus makes projections called chorionic villi (derived from chorion) full of fetal blood
o The mother’s decidua basalis allows nutrient/waste transport with the chorionic villi
Time What happens Clinical side note
Day
1-2
-Starts with fertilization and progresses down the fallopian tubes to implant into the uterus
2/4/8 cell stage -The cells are totipotent (can be differentiate into any cell) -Relevant to stem cell therapy -Not existent in adult humans
Morula cell stage -Cells are pluripotent (can almost differentiate into every cell)
Day
3-5
-Formation of the blastula -Embryo is now ready to implant on the mother’s uterus
Blastocyst cell stage -Only the embryoblast is pluripotent -First stage where cells start “deciding” what to be (trophoblast or embryoblast)

Charles Kim
8
Time What happens Clinical side note D
ay 6
-14
Implantation happens -Embryo needs to form a blood system for nutrients -Accomplished by implantation into the uterine lining Cell structures -Embryoblast epiblast + hypoblast -Trophoblast syncitio + cyto trophoblasts (embeds into uterus) Formation of extraembryonic membranes -Function: protects and nourishes the embryo. Does not end up being part of the embryo’s body
EEM Derived from Function
Chorion Tropho blast Forms the fetal placenta
Yolk sac Hypo blast Mainly for egg laying animals
Amnion Epi blast Contains amniotic fluid
More about the amnion: -Forms innermost fetal membrane -Fuses with chorion in week 8 -Eventually covers the entire embryo
Mechanism behind twins Fraternal twins: 2 eggs Identical twins: 1 egg. However, the 1 egg can take 3 different paths: A) 2 cell embryo splits right away -Each cell makes its own fetus -Most common mechanism -Forms 2 chorions and 2 amnions B) Embryo splits in the blastocoel -Trophoblast turns into 1 chorion -2 embryoblasts in 1 chorion -Rarer -Could cause uneven nutrient sharing -Forms 1 chorion but 2 amnions C) Embryo splits after amnion formed -Much much rarer -Resources are severely limited -Forms 1 chorion and 1 amnion
Day
14
-16
Gastrulation happens -Hensen’s node travels up, creating a primitive streak in the epiblast -Epiblast cells invade into the streak towards the endo/hypoblast -Endo/hypoblast disappears as the epiblast replaces it -First “wave” of migrating epiblast forms the definitive endoderm -Second “wave” of migrating epiblast forms the mesoderm -Epiblast on the top is now called the ectoderm
Body axes are formed Embryo How it relates on body
Primitive streak
Forms midline
Node -Right/left symmetry (important for liver, heart, etc orientation) -Cranio-caudal axis
Ectoderm side
Dorsal axis of the body (and hence ventral axis)
Endoderm forms the… -Alveolar, thyroid, and pancreas -Mainly “inside” -Endodermal epithelium
Mesoderm forms the… -Muscles, kidney tubules, RBC
Ectoderm forms the… -Mainly “outside” -Ectodermal epithelium (inc. skin) -Neurons, pigment cells, etc

Charles Kim
9
Time What happens Clinical side note W
eek
3
Neurulation -The diagram on the above ONLY shows the ectoderm -The ectoderm folds on itself to form the neural tube -The point where the tube pinches off called neural crest -Neural crest cells are thought to be a fourth germ layer -Bundle of neural crest cells part of the mesenchyme
Somite formation -Next to the neural tube, paired blocks of mesoderm form -Mesoderm develops into the dermatome, myotome, and sclerotome -Sclerotome is under the myotome (not seen above) -Dermatome: forms the dermis and the subcutaneous tissue -Myotome: forms the muscles -Sclerotome: turns into mesenchymal cells forms osteo cells, chondroblasts, and fibroblasts -The somites also start forming the vertebrae
Specifically in the head region -Rather than somites, there is a paraxial mesoderm next to the tube -There are also invading facial neural crest cells -Mesoderm makes head muscles and dorsal/inferior parts of skull -The ectodermal neural crest cells migrate to make the mandible, maxilla, eyes, and facial midline respectively -Trunk neural crest cells can make glial cells, smooth muscle cells, pigment cells, and neuronal cells. Cranial NCC’s are special because they can also turn into chondrocytes and osteoblasts!! Overview of the types of cells -Now, there are 2 main bodies of cells: epithelium and mesenchyme -Mesenchyme: neural crest derived and mesoderm derived -Epithelium: endoderm derived and ectoderm derived
The “folding” of the ectoderm doesn’t happen at the same on the whole embryo -It folds more like a “zipper” -Failure of anterior neural tube closure anencephaly (no cortex) -Failure of posterior neural tube closure spina bifida
Deficiency in neural crest cells -A huge portion of the face is made from cranial NCC’s
-Diagram above = all the cranial NCC bodies in the embryo -Diagram below = what could happen to the skull if NCC’s were deficient
-Defective upper jaw -TMJ problems, lack of TMJ, deafness

Charles Kim
10
Time What happens Clinical side note W
eek
4 –
Ph
aryn
geal
reg
ion
Pharyngeal arches, pouches and clefts -In the head region, pharyngeal arches start to be visible -Each arch has: ectoderm, endoderm, mesenchyme -Core of the arch: paraxial mesoderm forms muscles -Periphery of the arch: NCC’s connective tissue, cartilage, bone -When looking from the outside, there are clefts between arches -When looking from the inside, there are pouches
Arch Pouch Cleft
1 Tongue body, outer ear, and mandible
Auditory tube Eustachian tube
2 Outer ear Palatine tonsil Cleft 2, 3, 4 all merge to form the cervical sinus
3 Palatine tonsils and tongue root
Thymus and inferior parathyroid
4 Epiglottis Superior parathyroid and ultimobrachial body
Tongue innervation Nerve Innervates
CNV (lingual
branch of mandibular division)
Mucosa anterior 2/3 sensory
Mastication muscles
CNVII (chora typani branch)
Most taste buds Anterior 2/3 sensory
CNIX
Mucosa posterior 1/3 sensory
Circumvallate papillae, anterior 2/3 of tongue
XII Tongue muscles
Ear deformations could hint at mandibular defects -Because arch 1+2 forms these structures
Wee
k 5
– Se
nso
ry r
egio
ns
Placode formation -Placodes are embryonic structures which give rise to specialized structures -Olfactory placodes form at the borders of the frontonasal prominence -Neural crest cells (mesenchymal) are inside these layers making all these structures -#1,2,3,4 signifies the arches -Primitive mouth called the stomodeum is not yet connected to the GIT

Charles Kim
11
Time What happens W
eek
4-8
– F
acia
l reg
ion
The 5 facial prominences -Basic structures which will move and fuse to form the face
-Frontonasal prominence – gives rise to the nasal prominences -Medial nasal prominence (mammals) – Makes philtrum, nasal septum, intermaxillary segment, premaxilla, incisors -Maxillary prominence – Makes maxilla, palatine bones, upper teeth -Lateral nasal prominence – Makes nasal passages -Mandibular prominence – Makes lower jaw, parts of TMJ, bones of middle ear
Step 1 2 3 4 5
What happens
Outgrowth and contact of prominences
Formation of bilayered epithelial seam
Removal of the seam + epithelium
Replacement by mesenchyme (mesenchymal bridge)
Smoothing of grooves by proliferation of mesenchyme
Structure involved
-MNP -MP -LNP
.
. . .
-Note: if LNP and MP do not fuse correctly, the tear duct will be open in the fetus -Note: eyes start on the sides of the face and migrate forward
Wee
k 6
-9 –
Pal
atal
reg
ion
Secondary palate development happens after lip fusion (above) is complete
-Works by having the palatal shelf go from lateral to horizontal -Happens in a “zipper” fashion starting from the incisor area -“So much to do with so much to do right” prof’s reasoning for why cleft lip+palate defects are so common

Charles Kim
12
Enamel and dentin
Overview of the supporting structures of the tooth
o Note: Enamel is unique – no collagen!
Enamel Dentin Cementum Bone Periodontal ligament Sub epithelial matrix
Enamel Mineralized collagen Collagen, elastin, proteoglycans
Tooth function is influenced by
o Gross tooth morphology – cracks, crevices
o Microscopic tooth morphology – organization and integration of dentin tubules, DEJ
o Material properties – composition of sub layers in the tooth
Enamel and dentin
Enamel Dentin
Background
-Cannot be replaced -Can be repaired (remineralized) if less than 1/3 of the enamel is damaged -Evolved from fish scales -Complex gene organization still not well understood -Hardest substance in the body
-Is a living structure – has tubules with cell processes and nerves -Made by odontoblasts -Mechanically anisotropic (strength depends on direction of force applied) -2x more resistant to cracks if force is applied parallel to the tubules -Architecture, mineral composition, fiber organization are likely contributors to mechanics
Function -Protects the dentin -Supports the enamel
Composition -96% mineral, 4% organic -Made of interlocking rods
-67% mineral, 20% organic, 10% water -Dentin matrix with tubules of cellular processes
Appearance
-White and translucent -Opaque in less mineralized areas (i.e. white spot lesions) -Thickest at the crown (↑ stress)
-Darker than enamel -Varies (mantle, primary, circumpulpal, pre, intertubular, peritubular, secondary, and tertiary dentin)
Clinical abnormalities
Tooth agenesis -Mutations in WNT signalling molecule -Affects epithelial layer -No teeth formed Amelogenesis imperfecta -Commonly autosomal dominant -Gene responsible is not yet known -Could be due to amelogenin Neonatal line -Enlarged striae of Retzius -Due to illnesses like fevers or famines in early childhood -Will smooth out over time Caries predisposition -Due to mutated enamel genes -Studies still ongoing – not confirmed
Tooth agenesis -Mutations in MSX-1 signalling molecule -Affects mesenchyme layer -No teeth formed Dentinogenesis imperfecta -DGI type I: mutation in type 1 collagen which causes osteogenesis imperfecta. DGI-I is the oral manifestation of OGI -DGI type I/II: due to mutation in dentin sialophosphoprotein (DSPP). It is the one that initiates mineralization

Charles Kim
13
Enamel Dentin
Embryonic origin
-Enamel epithelium (inner, outer, stellate reticulum) are derived from the ectoderm
-Pretty much all other tooth structures (odontoblasts, bone sockets, periodontal ligament, etc) are from neural crest
Note: Neural crest cells also give rise to craniofacial cartilage + bone, bones of middle ear, smooth muscles, peripheral/enteric neurons, thymus, some heart structures, and pericytes on blood vessels,
Development and formation that enamel and dentin both share
-Maxillary, mandibular, and medial nasal processes come together to form the odontogenic epithelium -This epithelium gives rise to the teeth
-Epithelium thickens and forms a pouch -Blue = inner enamel epithelium -Dark pink = becomes outer enamel epithelium -Light pink area (including dental papilla) is where the odontoblasts + pulp will form (i.e. mesenchyme)
-Oral epithelial cells and mesenchyme cells signal each other to induce the differentiation of each other -Basal lamina (pink) dissolves to allow greater signalling -This process is called reciprocol induction -Epithelium ameloblasts, mesenchyme odontoblasts
-The mesenchyme becomes odontoblasts (elongates) -The pouch closes to form the basic tooth forming organ -Blue = inner enamel epithelium becomes ameloblasts -Pouch outline = outer enamel epithelium -Between inner/outer = stellate reticulum + stratum int. -Papilla gives rise to pulp and odontoblasts -Purple = dentin formed by underlying odontoblasts -The structure wraps around to form a tooth shape
-Mantle dentin (in blue) is made first -It is not very mineralized, mostly just collagen -Mantle dentin has no dentinal tubules -Pre-dentin is formed later and contains dentinal tubules. This is what will mineralize into dentin -Ameloblasts will make enamel downwards -Odontoblasts will make dentin on the ameloblast side, while keeping the pre-dentin layer right next to it Note: pre-dentin is also called smear dentin

Charles Kim
14
Enamel Dentin
Unique development traits of enamel and dentin
-Enamel formation can be broken down into 2 main steps: A) Secretory phase: a full thickness layer (mostly mineral and 30% protein) is made as a “scaffold” -Ameloblasts secrete matrix proteins and proteases which organizes tissues for crystal / prism alignment
Amelogenin (25 kDa)
-Most abundant. Establishes space occupied by enamel -Self aggregating “jelly” -Non homologous genes on X and Y chromosomes high level of heterogenicity -Mutations hypoplastic enamel (lacks rods)
Ameloblastin (70 kDa)
-Cell-matrix interaction and enamel synthesis -Mutations ameloblasts detach and enamel organ regression
Enamelin -Regulates crystal formation and elongation
-Ameloblasts also take ions (F, Ca, PO4, OH, CO3, Mg) from the blood into the enamel forming site -Stellate reticulum cells help pump more ions so that the concentration can be higher -By using bicarbonate to change the pH, ions and soluble proteins precipitate crystals form -Hydroxyapatite crystals nucleate at the DEJ and grow outwards (away from dentin) B) Maturation phase: proteins, organic material, and water are removed and replaced to end up with 95% mineralization -Stratum intermedium cells secretes alkaline phosphatase precipitates Ca and PO4 -Ameloblast cells secrete processing proteins:
Enamelysin MMP20
-Proteinase that removes amelogenins in mature enamel -Mutations thin, poorly structured enamel
Kallikrein 4 -Cleaves enamel proteins
-Cyclic release of bicarbonate cyclic alteration of pH cyclic release of calcium progressive mineralization
-Dentin formation starts at the apex of each cusp and progresses down to the roots -Problem: enamel doesn’t continue all the way to the root of the tooth. However, dentin does.
-How will odontoblasts form if there are no ameloblasts in the root to recipricolly induce? -Solution: Hertwig’s epithelial root sheath induces pulp to turn into odontoblasts without the need for ameloblasts (like in the crown area)
-Root dentin formation happens for 18~36 months after eruption -Dentin formation can be broken down into 2 main steps: A) Synthesis of collagen -Proline α chains are synthesized in the golgi/ER -Lys and Pro become hydroxylated (enzyme that does this step needs Vitamin C to revert back to its original conformation and continue functioning. Otherwise, it’s a 1-use enzyme) -Hydroxylysines then become glycosylated -3x chains make a triple helix procollagen -Procollagen gets secreted -Propeptides are cleaved forms collagen -Matrix is formed with collagen and proteoglycan B) Mineralization -Controlled by cell membrane processes called “matrix vesicles” coated with enzymes -Proteoglycans between collagen take up space they are removed by proteoglycanases -Phosphoproteins replace the proteoglycans -Osteoblasts, ameloblasts, odontoblasts secrete alkaline phosphatase and pyrophosphatase liberates PO4 from phosphoproteins -Calcium is brought by osteocalcin + sialoproteins -CaPO4 crystallizes and replaced proteoglycans -Matures into hydroxyapatite (Ca10(PO4)6(OH)2)
Layers formed (from out to in)
-Stellate reticulum -Stratum intermedium -Ameloblast body -Tomes processes + rods + interrods -DEJ
-DEJ -Dentin (peritubular and intertubular) -Predentin (collagen high, less mineralized) -Odontoblast body -Pulp
Charles Kim
15
Enamel Dentin
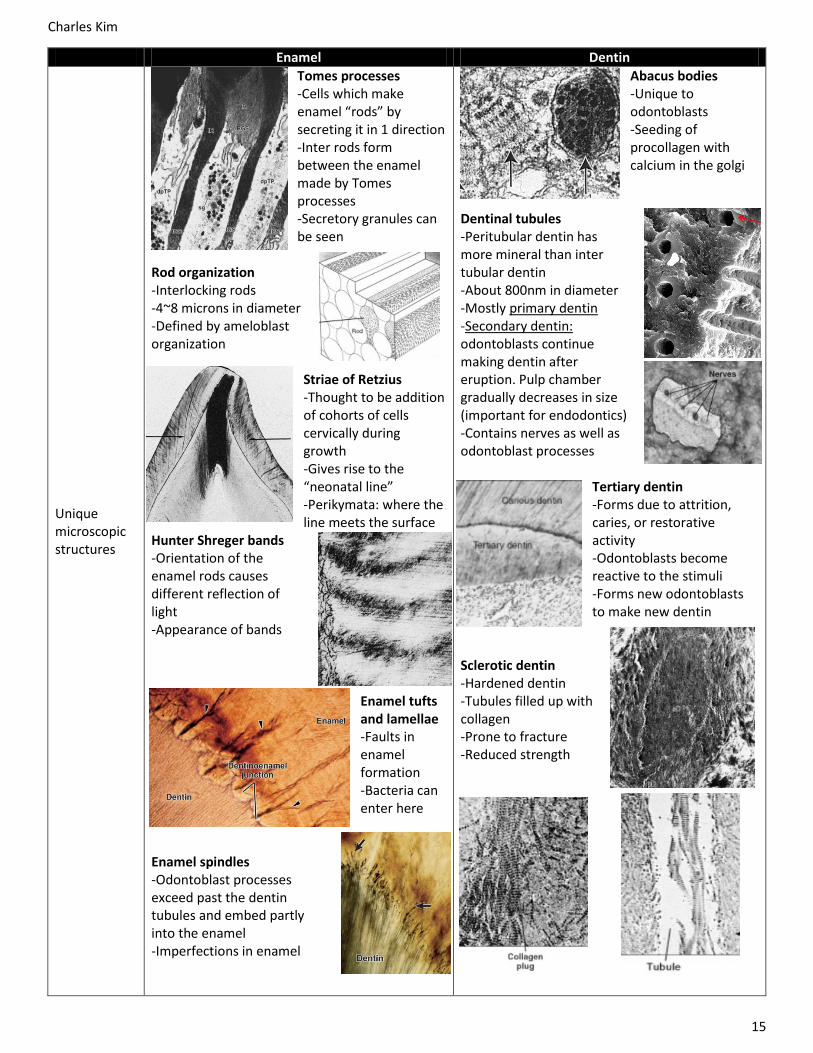
Unique microscopic structures
Tomes processes -Cells which make enamel “rods” by secreting it in 1 direction -Inter rods form between the enamel made by Tomes processes -Secretory granules can be seen
Rod organization -Interlocking rods -4~8 microns in diameter -Defined by ameloblast organization
Striae of Retzius -Thought to be addition of cohorts of cells cervically during growth -Gives rise to the “neonatal line” -Perikymata: where the line meets the surface
Hunter Shreger bands -Orientation of the enamel rods causes different reflection of light -Appearance of bands
Enamel tufts and lamellae -Faults in enamel formation -Bacteria can enter here
Enamel spindles -Odontoblast processes exceed past the dentin tubules and embed partly into the enamel -Imperfections in enamel
Abacus bodies -Unique to odontoblasts -Seeding of procollagen with calcium in the golgi
Dentinal tubules -Peritubular dentin has more mineral than inter tubular dentin -About 800nm in diameter -Mostly primary dentin -Secondary dentin: odontoblasts continue making dentin after eruption. Pulp chamber gradually decreases in size (important for endodontics) -Contains nerves as well as odontoblast processes
Tertiary dentin -Forms due to attrition, caries, or restorative activity -Odontoblasts become reactive to the stimuli -Forms new odontoblasts to make new dentin
Sclerotic dentin -Hardened dentin -Tubules filled up with collagen -Prone to fracture -Reduced strength

Charles Kim
16
Cementum and bone
Resembles bone and dentin (have a collagenous scaffold made by mesenchyme Bone Cementum Dentin
Hydroxyapatite 50-60% 45-50% 67%
Collagen Type I Type I and III Type I
Cells (scaffolding and maintenance)
Osteoblasts Osteocytes
Cementoblasts Cementocytes
Odontoblasts
Turnover Constant (due to osteoclast activity)
Minimal Minimal
Other proteins Bone sialoprotein Bone sialoprotein Dentin matrix proteins DSP (?)
Bone sialoprotein Dentin matrix proteins DSP (?)
Cementum structure o Covers the part of the dentin where enamel doesn’t (in the root)
In some cases, the cementum doesn’t fully cover the root
and some dentin is exposed o Cementum is thicker at the apex o Cementoblasts make the cementum o Cementocytes (stellate cells) are within the cementum
Cementum properties o ↓ Mineral and ↑ porosity compared to bone
o Contains more type 3 collagen (fibril-like) than bone
o Very slowly remodelled, if at all
o Very slow accumulation with age
o Characterized as cellular or acellular
Bone
o A dynamic structure of bone synthesis and degradation
o Osteoblasts = make bone, osteoclasts = destroy bone
o Regulating activity and generation of these cells controls bone
o Human periodontal disease: degradation of bone secondary to local inflammation
Caries
When caries reaches the DEJ, it spreads laterally and then forms another cone of invasion into the dentin
Bacteria can be seen in dentinal tubules (below)

Charles Kim
17
Embryonic tooth development
Teeth growth patterns
o Humans: 2 generations of teeth
1st generation (deciduous/baby/primary teeth): 2 molars, 1 canine, 2 incisors. 20 total
2nd generation (permanent teeth): 3 molars, 2 premolars, 1 canine, 2 incisors. 32 total
o Mouse: 1 continuous generation
3 molars and 1 incisor (16 total) that continuously grow
Embryonic origins of teeth
o Review: ectoderm folds on itself to form the neural tube. In the pinching process, the neural crest is
also made, which forms the mesenchyme
The ectoderm gives rise to 2 structures: ectodermal epithelium and neural crest mesenchyme
These 2 structures are responsible for forming all teeth
Note: facial and dental mesenchyme comes from neural crest, no mesodermal mesenchyme
o Review: In week 4-8, the facial prominences form and begin to fuse.
Each prominence is responsible for making different teeth
Medial nasal process: maxillary incisors
Maxillary process: rest of the maxillary teeth
Mandibular process (not labeled here): all mandibular teeth
Lateral nasal process: none
o Ectoderm derived structures: enamel and tiny part of cementum
o Mesenchyme derived structures: dentin, cementum, pulp, periodontal ligament
Stages of tooth development
o Overview: it is broken
down into 4 steps
Step What happens Diagrams
1 –
Init
iati
on
-Ectodermal epithelium and underlying mesenchyme interact with each other -Epithelium tells mesenchyme to make teeth at a particular spot to form a row of teeth -Epithelium differentiates slightly to form the odontogenic band (AKA marginal band)
-The odontogenic band thickens to form the dental lamina which follows the teeth arc -During this step, the mesenchyme is also busy differentiating (not seen in picture) -Placodes form where the teeth will be (so there will be 20 placodes in a human embryo) -“Beads on a string”
.
Side note: -In snakes: 2 rows of teeth on upper jaw! (premaxilla + maxilla odontogenic bands make the outer/marginal row of teeth. Pterygoid + palatine bands make the inner/palatine row of teeth) -In non mammals/birds/reptiles: animals have the ability to make odontogenic bands in the pharynx. This means they have 1 set of oral teeth and 1 set of pharyngeal teeth -In other tissues: this epithelial-mesenchymal interaction is also used to form other structures like hair, mammary glands, and feathers

Charles Kim
18
Step What happens Diagrams 2
– B
ud
din
g /
mo
rph
oge
nes
is
-Bud stage: First stage where tooth can be recognized in tissue sections -Special mesenchyme called odontogenic mesenchyme “gather/condense” around the dental lamina -The other mesenchyme is the jaw mesenchyme -This special mesenchyme sends a signal which causes the overlying dental lamine to invaginate -The enamel knot starts to form, leading to the next stage
-Cap stage: formation of enamel organ + primary knot -An “enamel knot” forms in the center of the inner enamel epithelium -It has 2 functions: A) Determine where cusps will form B) Signal/secrete proteins directs growth -The knot signals the mesenchyme below to form into the dental papilla -The bud closes off apically to also form the enamel organ -In the cap stage and early bell stage, the enamel organ can be seen as 3 layers: IEE, OEE, and SR
EK = enamel knot DE = dental epithelium DP = dental papilla IEE = internal enamel epi. OEE = external enamel epi. SR = stellate reticulum
-Bell stage: up until now, all teeth have looked the same under the microscope. Now it will differentiate -Humans are heterodonts (has different types of teeth) -The odontogenic mesenchyme determines how many enamel knots (which turn into cusps) will form in a tooth -Unicuspids = 1 knot, molars/premolars = 2+ knots -To accommodate this, 2ᵒ knots form. 1ᵒ knots will make buccal cusps whereas 2ᵒ makes the rest -Primary knot makes the buccal cusp only -In late bell stage, enamel organ has 4 layers: IEE, OEE, SR and now SI (stratum intermedium)
Side note – opossums: -There is a delay between primary (buccal) and secondary (lingual) knot formation -This gives the buccal cusp more time to make enamel so that it can be thicker -If the delay was small, buccal and lingual cusps would be similar size
Side note – tooth succession: -In the bell stage of primary teeth, there is a small pouch that forms on the outer enamel epithelium, called the successional lamina. This is the structure which develops into the permanent tooth -SL forms on the lingual side of the primary tooth
Primary tooth Gives rise to
Incisors x 2 Incisors x 2
Canines x 1 Canines x 1
Molars x 2 Premolars x 2
Side note – permanent molar formation: -It is not succession because permanent molars are not second generation teeth. They don’t replace any teeth when they erupt! -Unlike succession which has teeth come in lingually, molar formation happens distal to the previous molar -First molar (M1) has a distal M2 bud M2 has a distal M3 bud -If a 2ᵒ primary molar did not form, it may signal dental lamina damage so permanent molar may not form

Charles Kim
19
Step What happens Diagrams 3
– H
isto
dif
fere
nti
atio
n a
nd
min
eral
izat
ion
Late bell stage: -Note: shape of tooth is fully established at this point -Enamel organ induces odontoblast differentiation -Odontoblasts then induces ameloblast differentiation -Basement membrane between amelo and odontoblast disappears direct contact between cells -Amelo and odontoblasts polarize -Ameloblast and odontoblasts secrete enamel and dentin respectively which causes them to migrate away -Dentin forms slightly ahead of enamel
Side note – tooth development and caries: -Enamel-dentin interface determines how caries will spread in a tooth -Restorative techniques (i.e. dentinal etching) depends on formation of enamel and dentin
4 –
Ro
ot
form
atio
n a
nd
eru
pti
on
This step is part of histodifferentiation (but classified as its own stage in prof’s notes??)
Root formation -The OEE and IEE come together to form cervical loops under the tooth’s crown -Loops form Hertwig’s epithelial root sheaths @ the tips -HERS establishes the number, shape, and length of roots
Cementum formation
Cellular cementum Acellular cementum -Absent in single rooted teeth -Present in apical 1/3 and inter-radicular region of molars -Mostly made by neural crest, some by HERS
-Formed when HERS breaks down + deposits a lot of cementum -When HERS dies off, the surrounding mesenchyme forms a dental follicle
Dental follicle formation -Forms when the HERS breaks down -Made of mesenchymal cells surrounding the tooth -Forms the tooth attachment site (periodontal ligament, cementum, and induces bone formation) -Note: if there are no teeth no follicle no induction of bone formation no alveolar process (the thick ridge of bone that has the bone sockets)
Tooth eruption -The follicle causes deposition and resorption of bone by attracting osteoclasts -This rearranges the bone to erupt the tooth -Root formation is not required for eruption. Just the crown or even a non-tooth object will erupt as long as the follicle is intact
Metal object that replaced a tooth was able to erupt
.

Charles Kim
20
Disturbances in tooth formation
Disturbance Diagram Explanation
Nu
mb
er o
f te
eth
Hypodontia – tooth loss except in 3rd molars. 2~10% freq. Due to MSX1 or PAX9
.
-Lack of growth signal (like WNT10A [most common]) due to genetics -No placodes -Absent 1ᵒ tooth no SL -Present 1ᵒ tooth but SL fails to form -Present 1ᵒ tooth + SL but growth inhibited
Oligodontia – 6+ teeth missing except in 3rd molars. 0.1~1% freq. Due to MSX1, PAX9, or AXIN2
Anodontia – All teeth missing. Very rare
Supernumary teeth
. -Dental lamina grows very distally causes set of 4th molars -Bicuspids and incisors ?? -May appear normal without X ray
Mo
rph
oge
ne
sis
Extra lingual cusp on incisors (AKA Talon cusps)
. -Cusp is its own organ (has pulp!) -Caused by evagination of IEE and mesenchyme into its own organ during early tooth development
Extra central cusp on bicuspid
Conical teeth
.
Fused primary teeth
-Placodes started out too close together?
His
tod
iffe
ren
tiat
ion
(m
iner
aliz
atio
n)
Amelogenesis imperfecta – USA 1 : 14,000 Sweden 1 : 700 Turkey 1 : 232 Argentina 1: 1,000 Israel 1 : 8,000
.
-Discoloration, sensitive, prone to disintegration (pre/post eruption) -Highly genetic Can be due to: -Any stage of enamel making -Extrinsic disorders during development -Dental fluorosis -Enamel hypoplasia -Molar incisor hypomineralization
Dentinogenesis imperfecta – 1 : 6,000~8,000
.
-Primary and permanent dentition turns translucent, discolours, brittle -Enamel shears off exposed dentin -Autosomal dominant (50:50)
Enamel hypoplasia -If not all the teeth are affected or pattern is asymmetrical, it is likely an environmental cause -Environmental examples: tetracyclines, fluoride, trauma, high fever, infection, radiation
Explanation for pic 1: -Hypoplasia on both sides (bilateral). Likely due to systemic exposure -Probably due to tetracyclines and fluoride. Which tooth is affected depends on time of exposure Explanation for pic 2: -Asymmetrical so likely local insult -Primary tooth was abscessed so it was extracted. This affected the growth of the permanent premolar

Charles Kim
21
Pulp-dentin complex https://secure.dentistry.ubc.ca/intranet/Visuendo-svn/m1/index.html
Methods of bacterial entry into pulp
o Caries (cavitation or on the surface)
o Leakage
o Lateral canal, dentinal tubules which act as canals
o Deep pocket (of alveolar bone?) which allows entry via root apex
o Bacteremia
o Trauma exposes pulp
o Cracked tooth, Vertical root fracture, hairline fracture on crown
o Invagination (tooth folds while developing, causing a part of a tooth to be inside the main tooth)
o Evagination (tooth has a process coming out. This process contains pulp, so needs to be removed and
sealed before it becomes a problem)
Pulp stones
o Calcified bodies which form inside pulp chamber
o Previously thought to be harmful, but nowadays it is left alone if it’s not problematic
Properties of dentin
o By weight: 70% inorganic 20% organic 10% water
o By volume: 45% inorganic 33% organic 22% water
o Organic portion of the dentin
90% of it is type 1 collagen (and very small amount of type 3 + 5 collagen)
Type 1 collagen has a 9:26 ratio of hydroxylated lysine : lysine
What does this mean? higher cross linking than bone
Other 10%: dentin phosphoprotein, dentin sialoprotein, dentin matrix protein 1, osteonectin,
osteocalcin, bone sialoprotein, osteopontin, and some serum proteins
o Inorganic (mineralized) portion of the dentin
Average mineral size: 20 x 4 nm (enamel is 130 x 30 nm)
Dentin apatite is non homogenous and non stoichiometric
Normal HA has a 1.67 ratio of calcium : phosphorous. Dentin’s ratio is 1.62 (less calcium)
Dentin has higher Mg2+ and CO32- concentration ↓ sized crystals, ↑ solubility than enamel
o Types: primary, secondary, tertiary reactionary (1ᵒ odontoblasts) and tertiary reparative (2ᵒ odontoblasts)
Dentin components
o Phosphophoryn
Family of unique phosphorylated proteins in the dentin ECM
One of the major non-collagen proteins
Rich in serine, aspartic acid, and phosphorylations ↑ negative charge ↑ Ca2+ affinity
Key molecules driving dentin mineralization
o Matrix vesicles
Vesicles which are budded off by chondrocytes, osteoblasts, and odontoblasts
Structure: 100 nM diameter vesicles wrapped in a membrane
Contains: apatite crystals, phosphatases (alkaline phosphatase, adenosine triphosphatase,
pyrophosphatase), calcium binding molecules (annexin I, phosphatidyl serine)
Function: released into developing matrix to start calcification
Mechanism
Phase 1: all the enzymes (on/near vesicle membrane) are released to help crystallization
Phase 2: crystal release through MV membrane. ECM has enough Ca + PO4 to continue
crystal growth on the initial crystal nucleus
MV’s can cause pathologic calcification leading to osteoarthritis, atherosclerosis, and crystal
deposition arthritis

Charles Kim
22
Pulp composition
Cellular Extracellular
-Structural: odontoblasts, fibroblasts, blood vessels -Immune: macrophages, lymphocytes, dendritic cells, mast cells -Other: nerve cells, stem cells
-Ground substance: Proteoglycans, hyaluronic acid, dermatan sulfate, heparin sulfate, chondroitin sulfate -Connective tissue: Collagen type 1, elastin
Use of pulpal stem cells
o Physiologically
Source of cells to replace when damaged
Stem cells in PDL and roots can help with growth
o In research
Good source of stem cells because they can be obtained so easily
Used in pulp restoration due to infxn, PDL damage, generation of tooth structures for implants
J Endod 2008: Stem cells from baby teeth can be used for dental pulp tissue engineering
Implanted cells into a mouse and showed that growth was viable
Dental pluripotent stem cells + collagen scaffold + Dentin Matrix Protein 1 can induce
organized matrix formation similar to pulpal tissue
Dental stem cells are similar to mesenchymal stem cells could possible treat mesenchymal
related disorders like Parkinson’s disease
Pulp nerves
o 1000~4000 nerves enter the pulp. It is broken down to efferent and afferent
Aα fibers Aβ fibers Aδ fibers C fibers
Myelinated Myelinated Myelinated Unmyelinated (pain)
12~20 um 5~12 um 1~5 um 0.4~1 um
70~120 m/sec 30~70 m/sec 6~30 m/sec 0.5~2 m/sec
Efferent Afferent Afferent Afferent
Muscles Pressure, touch Pain, temp, touch Dull pain

Charles Kim
23
Muscle and nerve
Cells called Schwann cells make a myelin sheath to increase speed of
conduction of the nerve
o Myelin is composed of: Galactocebroside (glycolipid),
Sphingomyelin, Myelin basic protein, and Cholesterol
o Myelinated nerves travel faster and have greater sensitivity to
anesthesia
How do nerves function?
At rest
-Uneven distribution of ions across the membrane -Cell has a resting potential of -70 mV
Intracellular Extracellular
Potassium 148 mM 5 mM
Sodium 10 mM 142 mM
Calcium <0.01 mM 5 mM
- charged macromolecules 100 mM -
Receiving a signal
-Neurotransmitters from the previous neuron is released to the dendrite -Calcium enters the presynaptic neuron -The presynaptic neuron has neurotransmitter stored in vesicles -Vesicles fuse and release neurotransmitter contents (toxins can interfere here) -Neurotransmitters bind to transmitter gated ion channels and depolarize the dendrite -With Ach, Ach-esterase degrades Ach to prevent continued depolarization -Venoms/pesticides/poisons can target Ach-esterase prolonged action potential
Voltage gated ion channels Sodium, potassium, calcium channels
Transmitter gated ion channels
Excitatory Ach/serotonin gated cation channel Glutamate gated Ca channel
Inhibitory GABA/glycine gated Cl channel
-CNS drugs (psychoactive) target transmitter gated ion channels -Prozac (fluoxetine) prevents serotonin reuptake more activation of channel -Barbiturates and tranquilizers bind GABA channels more easily activated -Includes other anxiety, depression, and schizophrenic drugs
Propagation of action potential
-Voltage gated ion (Na, K, Ca) channels line the cell membrane -On the neuron axon, depolarization travels down the sheath in 1 direction -This is possible because sodium channels have a refractory period -One channel will activate the next channel, but it cannot go backwards
-Local anesthetics work by inhibiting ion transport on these channels -Lipid soluble and weak base. This means they can cross the lipid rich neuron membrane -Metabolized by liver (lidocaine) or hydrolyzing ester groups by cholinesterase (cocaine)
Charles Kim
24
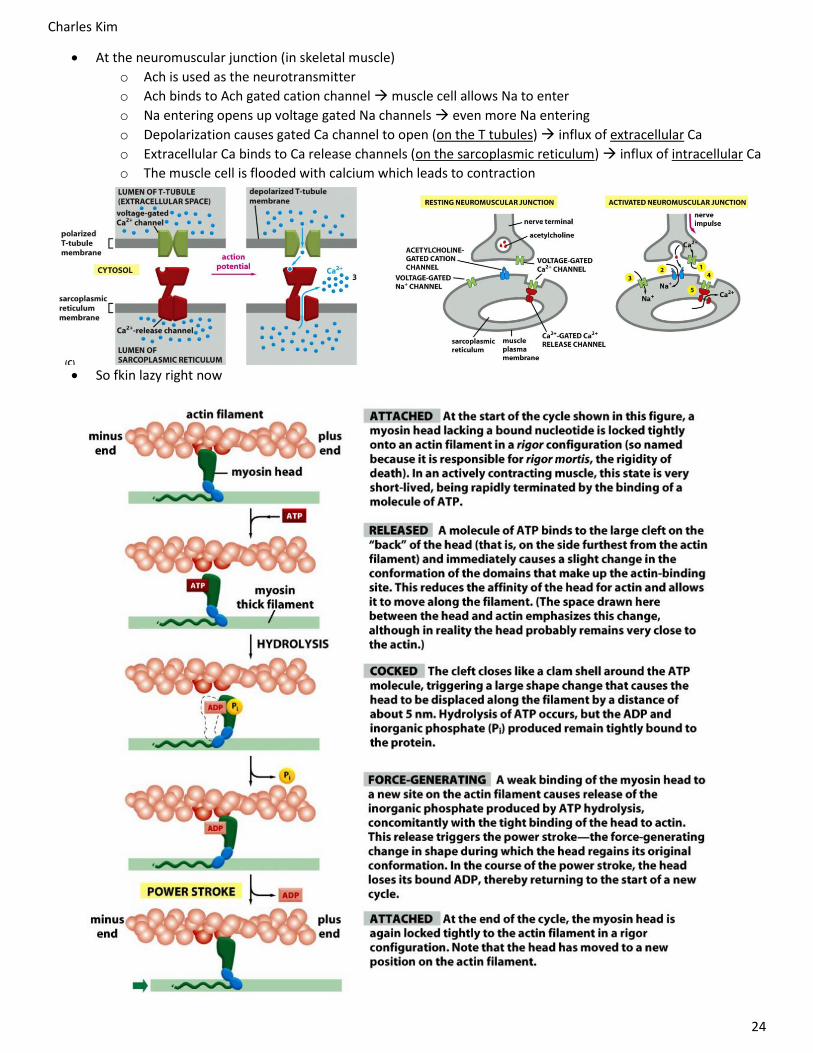
At the neuromuscular junction (in skeletal muscle)
o Ach is used as the neurotransmitter
o Ach binds to Ach gated cation channel muscle cell allows Na to enter
o Na entering opens up voltage gated Na channels even more Na entering
o Depolarization causes gated Ca channel to open (on the T tubules) influx of extracellular Ca
o Extracellular Ca binds to Ca release channels (on the sarcoplasmic reticulum) influx of intracellular Ca
o The muscle cell is flooded with calcium which leads to contraction
So fkin lazy right now
Charles Kim
25
Typical cell’s cytoskeleton
o 5nm actin filaments
Motility (can polymerise and depolymerise), tension, structure
Cell division, polarity secretion, endocytosis
o 10nm intermediate filaments
Attaches to desmosomes (e.g. keratin in epithelial cells)
o 25nm microtubules
Stable structures which can also polymerise/depolymerise
Cell division, transport of vesicles or organelles, can be organized into flagella
o Myosins, kinesins, dyneins
Motor proteins
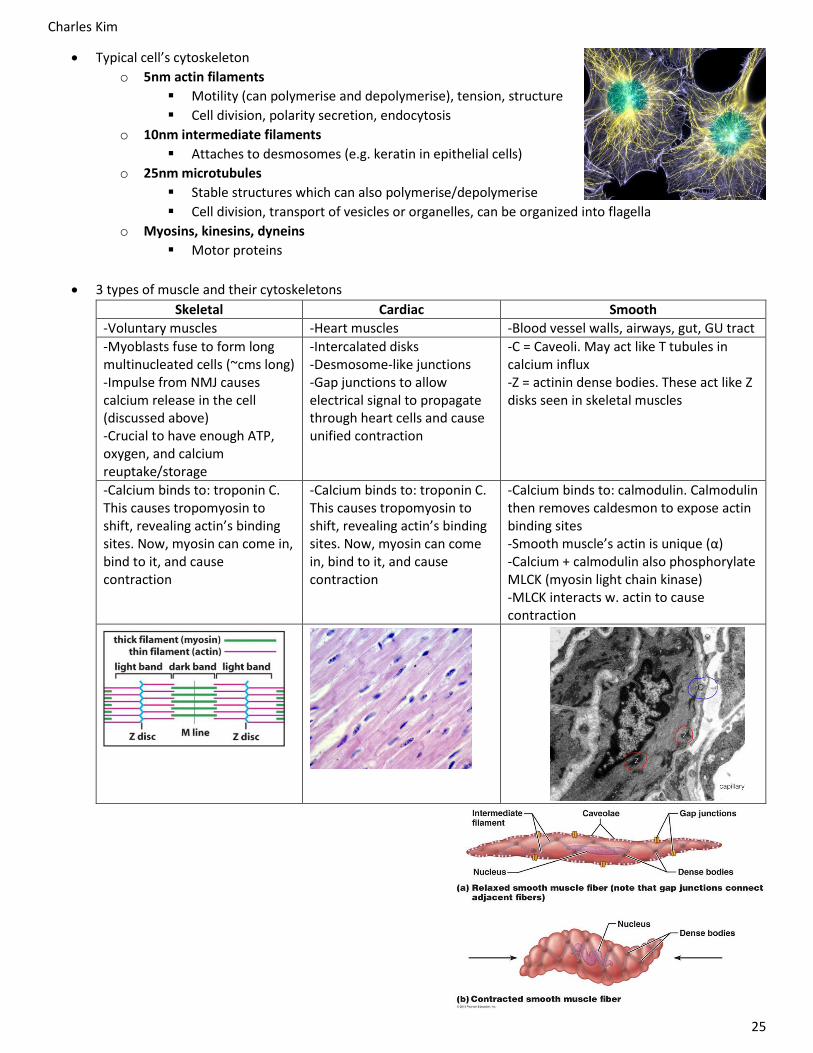
3 types of muscle and their cytoskeletons
Skeletal Cardiac Smooth
-Voluntary muscles -Heart muscles -Blood vessel walls, airways, gut, GU tract
-Myoblasts fuse to form long multinucleated cells (~cms long) -Impulse from NMJ causes calcium release in the cell (discussed above) -Crucial to have enough ATP, oxygen, and calcium reuptake/storage
-Intercalated disks -Desmosome-like junctions -Gap junctions to allow electrical signal to propagate through heart cells and cause unified contraction
-C = Caveoli. May act like T tubules in calcium influx -Z = actinin dense bodies. These act like Z disks seen in skeletal muscles
-Calcium binds to: troponin C. This causes tropomyosin to shift, revealing actin’s binding sites. Now, myosin can come in, bind to it, and cause contraction
-Calcium binds to: troponin C. This causes tropomyosin to shift, revealing actin’s binding sites. Now, myosin can come in, bind to it, and cause contraction
-Calcium binds to: calmodulin. Calmodulin then removes caldesmon to expose actin binding sites -Smooth muscle’s actin is unique (α) -Calcium + calmodulin also phosphorylate MLCK (myosin light chain kinase) -MLCK interacts w. actin to cause contraction

Charles Kim
26
Craniofacial development
Distinguish bones of the skull that are neural crest versus
mesodermal in origin
Neural crest: front of skull
Mesoderm: rest of the skull + musculature
Skull formation
o Before any bone forms, a primitive skull called the chondrocranium forms
The chondrocranium is made of cartilage (nc, cb, occ, mc)
o Function: it holds the skull together while bone develops around it. It does
not turn into bone. (see next objective)
o Surrounds sensory capsules (orbital, nasal, auditory) but not brain
o This primitive skull doesn’t surround the brain area
Surrounds sensory capsules
Time Palate Chondrocranium Body posture
7 weeks
-Secondary palate closure is starting
-Already well-present before palate closure -Meckel’s cartilage (which will turn into the mandible) starts to grow -Genioglossus muscle attaches to the rostral (front) part of the MC -MC meets at the midline
-Head is tucked -Mandible growth is difficult
9 weeks
-Secondary palate closure is complete, with the soft palate finishing up last
-Huge growth in Meckel’s cartilage (blue triangle). It outgrows the maxillary part of the jaw -Genioglossus muscle (brown) can be seen
-Head slowly angles up (until week 12) -Allows ↑ development to happen in the mouth
Meckel’s cartilage also gives rise to ear structures
o Pharyngeal arch 1: gives rise to Meckel’s cartilage,
which then extends caudally to form part of the
malleus and incus
o Pharyngeal arch 2: gives rise to the rest of the
malleus and incus, as well as all of the stapes
Mandible gives rise to secondary cartilages
o 2ᵒary cartilage develops adjacent to intramembranous bone at sites of
muscle attachments and articulations
o Condylar: will turn into part of mandible that articulates with the skull
o Angular: sharp corner at the inferior-posterior part of mandible

Charles Kim
27
Describe the steps leading to intramembranous bone formation going from the condensation phase to differentiation
Neural crest and mesodermal derived mesenchyme both have the ability to make bone. Bone can be formed in
2 ways, and both (NC/mesodermal) tissues can do both ways
Intramembranous ossification Endochondral ossification
-Direct conversion of mesenchymal tissue into bone -Mesenchymal tissue differentiates into cartilage cartilage gets replaced by bone
-Occurs primarily in bones of the skull -Around the chondrocranium
-Primarily in long bones -In head: condylar cartilage and occipital bones
Intramembranous ossification
o Which bones undergo IMO?
Most facial skull and bones
Teeth as well
Note in diagram: tb = tooth bud
o Mechanism
Mesenchymal cells turn into osteoblasts
Osteoblasts deposit osteoid matrix
Osteoblasts become arrayed on matrix
Trapped osteoblasts turn into osteocytes
o Initiation of ossification
Happens on sites called ossification centers
There are multiple ossification centers. For example, the maxillary
bone has 2 on each side, the premaxillary bone also has multiple
In calvaria (skull plates): frontal bone (NCC derived) has a
ossification center, and the parietal bone (mesoderm derived) has one as well
But macroscopically, they look the same despite the different origins. (exam question)
Understand the mechanisms of suture formation
Ossifying bones grow and touch each other Forms a suture. Some sutures are kept separated until after birth
o Why? To allow the head to fit through the birth canal
o How? There is undifferentiated mesenchyme between 2
bone fronts. These cells express Twist1 which prevents
differentiation. In contrast, bone cells don’t express Twist 1,
they express Bone sialoprotein
If there’s a defect in Twist1 fuse early and cause craniosynostosis
Pharaoh of Egypt had early mid-sagittal suture closure elongated head
o Note: signals from the dura mater layer are also needed to keep the sutures open
Suture closure
o How? fibroblast growth factor signalling pathway
Bone Coronal Sagittal Lambdoid Metopic Mid palatal
Time of fusion 22~39 years 3~9 months 11 years +
Understand the formation of the alveolar bone and tooth crypts
Tooth follicles induce alveolar bone to be formed around it
This forms bone with crypts for the teeth
Tooth crypts enlarge (inciso-gingivally and bucco-lingually) during week
12~19
By late fetal development, upper and lower jaws are established

Charles Kim
28
Connective tissue
Connective tissue cells
o Responsible for assembling the matrix (of collagen or other fibers) and maintaining it
Connective tissue is always in a balance of synthesis and degradation
o Examples: fibroblasts, osteoblasts/cytes (in bone), chondrocytes (in cartilage), adipocytes (in fat),
smooth muscle cells
o When matrix is damaged: causes stress and release of signalling molecules gene expression is
changed in the CT cells CT cells will increase matrix turnover
o What do cells use to interact with the matrix?
Integrins
Cell surface receptors which are high affinity adhesion to the matrix
Has alpha and beta subunits - # of these subunits will determine specificity and ligation
Forms the part of the hemidesmosome which goes from inside to outside the cell
Binds to intermediate filaments intracellularly, and basal lamina (collagens, laminin,
matrix glycoproteins) extracellularly
Sensors for mechanical stress on the matrix
Hyaluronan receptor (CD44)
Cell surface receptors which are used for cell migration and low affinity adhesion
Used in ↑ proteoglycan environments like development, nervous system, inflammation
Example: macrophages use this to migrate during inflammation
Example: nerve cells use this to migrate during development
Overview of molecules of the matrix
o Mechanical:
Collagen – provides tensile strength
Elastin – provides elasticity
Proteoglycans – provides resistance to
compression (cartilage)
o Non mechanical:
Adhesive glycoproteins – sticks matrix to
matrix, matrix to cell, and cell to cells
Proteoglycans – sticks to other matrix
molecules, bind signalling molecules (chemokines), modulates cell-matrix adherence
Collagen
Used in -Scaffold for soft tissues: gingival CT, blood vessels, basal lamina, parts of pulp -Scaffold for hard tissues: bone, dentin, cementum, cartilage
Structure -3 peptide chains that wind around each other -Peptide chain is made of repeating (G – X – Y)n
G X Y AA Glycine Usually proline Usually
hydroxyproline
Purpose Only AA which can occupy the tight space in the middle of collagen fiber
Has a 5 membered ring which kinks the chain
Same as proline, but the hydroxy group ↑ hydro-philicity and holds chain together
-Note: hydroxyl-lysine is also common in collagen (they are essential for glycosylation of hydroxyl-lysine crosslinks) -Since every 1/3 AA is glycine, any mutation to glycine will mess up the helix -If Y is not hydroxylated no H bonds w. surroundings fibrils unstable/unfolds at body temp

Charles Kim
29
Synthesis
2. Vitamin C recycles the enzyme that does this step 3. Glycosylation of hydroxyl-lysine helps with cross linking 4. Chain association and disulfide bonding is required for this step 5. Chaperones facilitate folding of collagen chains to its energetically stable form 7. Before they are deposited, the collagen undergoes post-translational modification (removal of the pro-peptides and glycosylation on the helix)
Variability -Collagen can be mineralized or unmineralized -Black layer between cementum and Sharpey’s fibers calcified hydroxyapatite -Collagen is broken down into types (>28 types!) -Type 1 found in bone, dentin, cementum, skin -Type 2 found in cartilage -Type 3 found in skin, blood vessels -Type 4 found in basal laminae -Collagen is also broken down by macroscopic structure
Fibril forming -Type 1, 2, 3, 5, 11 -Forms in quarter staggered fibrils
Fibril associated -Type 12, 16, 9 -Fibrils with some interruptions in the triple helix -Type 9 acts as a spacer here
Sheet forming -Type 4, 8 -Sheet forming “chicken wire”(i.e. BL uses type 4 collagen)
Collagen break-down
-Collagenase cleaves Gly-Ile bond at AA 777/1014 -Triple helix denatures to form “gelatin” -Protein denatures by many proteases

Charles Kim
30
Related diseases
Genetic defect of collagen genes -Not required to know all the collagenopathies -Usually involves mutation on glycine -Examples: osteogenesis imperfecta, dermatosparaxis, skin
Acquired collagen defect: Scurvy -Symptoms: bleeding gums, loss of teeth, unexplained bruising, weakness, inability to stand -Picture: 10 days of treatment of vitamin C -Mechanism: no vitamin C nothing will reduce the iron in the proline hydroxylase no recycling of enzyme -Historical relevance: -1535 – 25% of Jacques Cartier died -1735 – James Lind realized that eating fresh fruit and veggies prevented disease -1785 – Royal navy acted on Lind’s recommendations -1912 – Something about Antarctica Acquired collagen defect: Bone growth -Picture: Bone growth abnormality, fixed with Vit C x6 months

Charles Kim
31
Elastin
Background -Periodontal ligament has elastin as well as collagen -Cows have one large elastin molecule on the back of their necks to hold it while ruminating
Properties -Biological “rubber” material -Very hydrophobic (insoluble): Pro, Val, Ala, Gly -Gene sequence: codes for lots of hydrophobic and cross linking modules
Synthesis -Scaffold of fibrillin (a protein) is laid out -Elastin is deposited on this scaffold -Extensive cross linking happens by lysyl oxidase -72 kDa protein
Related diseases
Marfan’s syndrome -Defect in fibrillin gene elastin is laid down on a defective scaffold mechanical failure of elastic structures (i.e. aorta) and unusually long bones -Incidence of 1/5000 Menkes’ disease (not required to know) -Defect in copper transport/metabolism lysyl oxidase affected defective cross linking of elastin presents as aterial rupture and emphysema -Incidence of 1/30,000 ~ 1/250,000 (X linked recessive)
Elastin Breakdown
-Due to extensive cross linking, few cleavages little difference to the network -Sensitive to proteinases like cathepsins L, G, and neutrophil elastase -Elastase inhibitor: alpha 1 antitrypsin deficiency in this enzyme means elastin will not be broken down leads to emphysema (destruction of elastin in lungs), especially smokers
Proteoglycans
Background -Proteoglycans are glycoproteins which contain glycosaminoglycans (lol this sentence…) -Key concept: glycosaminoglycans are negatively charged -Found in cartilage, developing bone, blood vessels, matrix of nervous system, all soft CT like gingiva, pulp cavity
Structure Proteoglycan is the whole structure -Includes a “protein core” which is seen in the middle -GAG’s are attached as branches from the core -In this example, chondroitin is the GAG -The GAG has a huge negative charge -This causes sodium to come in and neutralize the charge -Water follows, due to osmotic pressure -This swells the proteoglycan increase in size -When loaded, water escapes
Proteoglycan responsible for cartilage is aggrecan -Each monomer has a 250 kDa core protein and 2mDa of glycosylations (mostly chondroitin) -Monomers polymers by aggregation with hyaluronan and link proteins -All of this is “wrapped” in type 2 collagen -Defects in cartilage altered skeletal development, altered joint function, altered resp. function
PG breakdown
-Seen in osteoarthritis -Degradation leads to changes in mechanics and decomposition of the structure

Charles Kim
32
Bone
Collagen and proteoglycans are able to become mineralized by Ca and PO4
Just like collagen, bone cells can detect changes/stress in the environment using integrins
o Remodelling happens as well, to respond to stress
o Bone is in a balance between synthesis and degradation
Terminology
o Axial skeleton: head, neck, trunk
o Appendicular skeleton: limbs
o Skeleton: encompasses cartilage and bone. It is surrounded by perichondrium and periosteum
o Bone is formed in 2 ways
Endochondral ossification: cartilage is made first and then bone infiltrates it
Intramembranous ossification: directly formed bone during embryonic/prenatal periods
o Gross appearance: bone is flat (skull, pelvis, scapula) or long (axial skeleton)
o Compact bone: mature, flat bones, shaft of long bones (weight bearing)
o Spongy bone: embryonic, insides of long bones, cancellous, trabecular
o Diaphysis: shaft of long bone
o Metaphysis: shaft near growth plate
o Epiphysis: ends of long bone
o Osteoid: type 1 collagen rich matrix, not yet mineralized
(analogous to pre dentin!)
Osteoblasts
o Connects to other cells using gap junctions on the ends of
cytoplasmic processes
o Makes collagen
o Deposits minerals (calcium and phosphate) into the ¼ gaps
between collagen fibers
o Mineralization (same steps as dentin, cartilage, and
cementum formation)
Osteo/odonto/ameloblast secretes alkaline
phosphatase + pyrophosphatase
Phosphate is liberated
Calcium is in high levels locally
Ca and phosphate containing proteins are brought to
the space between collagen fibers
Crystallization happens
This process is controlled by the release of matrix
vesicles (containing alkaline phosphatase)
Other control proteins exist (i.e. sialoproteins),
but not fully understood
Osteoclasts
o Derived from mononuclear cells, but they have multiple nuclei
o Has a ruffled border (RB) where lysosomes (low pH +
lysosomal proteinases) are released
Low pH = dissolves the CaPO4
Lysosomal proteinases = degrades collagen
o Lysosomes have ATP dependent proton pump
o Forms a “cleared zone” (CZ) once bone has been resorbed
Charles Kim
33
Osteocytes
o Cells which used to be osteoblasts, but got stuck in bone matrix during
formation
o Act as mechanical sensors in bone. Can make collagen as well
Appearance of bone is different depending on age
o Shows that bone is constantly undergoing remodelling
o Older bone is organized into and has structures called osteons
Bone macroscopic structure
o Bone is a collagen meshwork mineralized with calcium phosphate
o Center part spongy high turnover cellular part
o Outer part compact low turnover structural rigidity
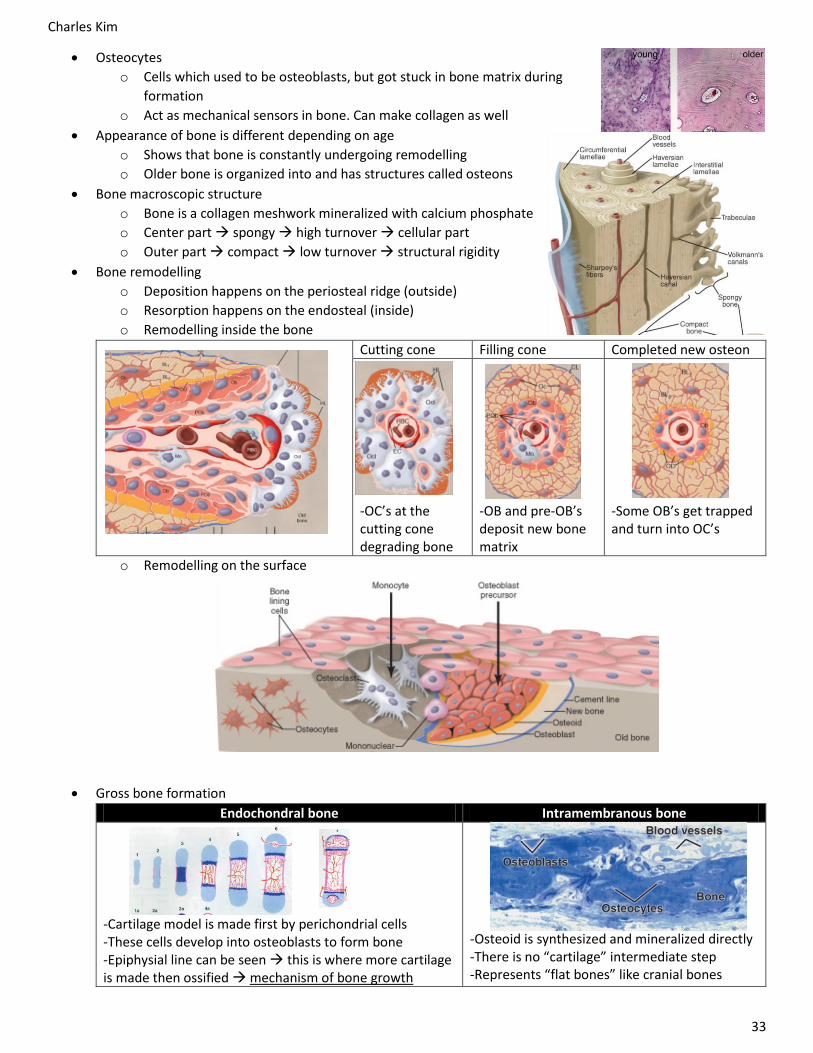
Bone remodelling
o Deposition happens on the periosteal ridge (outside)
o Resorption happens on the endosteal (inside)
o Remodelling inside the bone
Cutting cone Filling cone Completed new osteon
-OC’s at the cutting cone degrading bone
-OB and pre-OB’s deposit new bone matrix
-Some OB’s get trapped and turn into OC’s
o Remodelling on the surface
Gross bone formation
Endochondral bone Intramembranous bone
-Cartilage model is made first by perichondrial cells -These cells develop into osteoblasts to form bone -Epiphysial line can be seen this is where more cartilage is made then ossified mechanism of bone growth
-Osteoid is synthesized and mineralized directly -There is no “cartilage” intermediate step -Represents “flat bones” like cranial bones

Charles Kim
34
More bone terminology
Gross appearance
Flat Skull, pelvis, scapula
Long Axial skeleton
Macroscopic appearance
Compact Mature bones. Flat bones and shaft of long bones
Spongy/trabecular Embryonic bones. Inside long bones
Development/ formation
Intramembranous Direct formation of bone
Endochondral From cartilage model
Regions Diaphysis Shaft of long bone
Metaphysis Shaft near growth plate
Epiphysis Ends of long bones
Microstructure Embryonic/woven Irregular collagen network
Lamellar Collagen in concentric layers
Disposition of lamellae
Circumferential On periosteal and endosteal surfaces
Osteonic Concentric lamellae form osteons
Interstitial Residual zones between osteons
Mandible example
Trabecular part Compact part
-Rapidly remodelled -Can act as calcium storage
-Remodelled slowly -Biomechanical strength
Bone metabolism
o Regulated by cell interactions: cell-cell signalling, mechanical effects through integrins
o Regulated systemically: by hormones, estrogen, androgens, leptin, and others

Charles Kim
35
Bone synthesis Bone degradation
Cell responsible Osteoblast Osteoclast
Signal used -Osteoprotegerin (OPG) – released by OB’s. Binds to RANKL so that it can’t bind to clasts -TGFβ – released by the matrix in the clasts
-M-CSF and TNF11 (RANKL) – Binds to RANK receptors and activates + proliferates osteoclasts
Parathyroid is secreted when [Ca] is low. Why?
-PTH decreases OPG production by osteoblasts RANKL can bind to osteoclasts
-PTH increases RANKL production activates osteoclast activity
Too much can lead to…
-Osteopetrosis -Osteoporosis -Inflammation driven bone resorption
Biphosphonates -Kills/inhibits osteoclasts
Inflammation driven bone resorption
o Human periodontal disease
Chronic local inflammation
Death of bone cells in the alveolar bone
Degradation of bone
o Arthritis
Years of inflammation leading to bone deformation
Cartilage + subchondral bone is degraded
Blue = cartilage, white = bone
o How does inflammation ↑ bone degradation?
Tumor necrosis factor (TNF) is released in inflammation
TNF is synergistic with RANKL and not inhibited by OPG
Causes degradation to happen even with inhibiting mechanisms
TNF also inhibits osteoblast formation and activity
More information about TNFα
o Cytotoxin made by monocytes can trigger the death receptor
o Used for cell-cell contact mediated apoptosis
o Physiologically: used for tumor regression (hence the name), fever, and cachexia (muscle wasting)
o Remicade (infliximab) antibody which binds and inhibits TNFα
Other bone disorders
o Osteogenesis imperfects/brittle bone disease
Mutation in collagen type 1. Range of severity. Can affect the teeth
Has blue sclera
We did our case on this – refer to that
o Paget’s disease
Can be due to constitutive activation of RANK ↑ clast activity + number
Can be due to osteoprotegerin deficiency ↓ RANKL inhibition ↑ clast activity + number

Charles Kim
36
Genetics
What is DNA?
o Genetic information packaged in the nucleus of cells
o Made of units called adenine/thymine/cytosine/guanine with a phosphate backbone
Bases are named based on where they came from (i.e. guanine from guano)
o Can be interpreted as 4 terms: base pairs, gene, chromosome, genome
Central dogma
o DNA is kept in the nucleus where it duplicates itself (semi-conservatively)
o DNA transcribed RNA translated protein
o However, there are lots of exceptions to this rule (prions, ribozymes, etc)
Chromosomes
o Not visible until the cell is undergoing replication
o Can be in the condensed form (characteristic X) before cell division or in loose chromatin
o There are 2 arms coming out of the centromere
P = petite arm = shorter arm
Q = longer arm (comes after P). Always seen on the bottom when drawing chromosomes
o Centromere = in the center or off center. Acts as the “navigator” for the cell
In the center = metacentric
Off the center = acrocentric. Includes 13, 14, 15, 21, 22 (they can do Robertsonian translocation). These
chromosomes have redundant ribosomal DNA on the P arm. OK to lose.
o Telomere = on the ends of chromosomes. They protect the ends of chromosomes
o In humans, they are linear. This is because recombination needs to happen (harder in circular DNA)
Also, humans have 23 pairs. They are numbered 1~22 (based on size) and X/Y
o We get 2 copies of each – 1 from mom and 1 from dad
o “Bands” can be seen. However, 1 band does not mean 1 gene
Chromosome band nomenclature example: locate Xp11.23
o Xp = chromosome X’s p arm
o 11 = does not mean band eleven, it is band one one = first band of that first band
o 2 = second band of the first band of the first band
o 3 = third band of the second band of the first band of the first band
o Done because not everyone is able to see to the same resolution as others. This keeps it simple
Chromosome dosage
o Trisomy = 3 copies of 1 chromosome. Lethal unless it is 13, 18, 21
o Monosomy = 1 copy of 1 chromosome. Lethal unless it is monosomy X (Turner’s syndrome)
o Aneuploiy = any disturbance of chromosomes. Very common in cancer cells
o Triploidy = 3 copies of EVERY gene. Lethal in humans
Nature vs nurture?
o AIDS: thought to be fully environmental, but some genetic mutations can allow immunity to it
o Cystic fibrosis: thought to be fully genetic, but environment (treatment) can influence prognosis
o Heart disease, diabetes, etc: no idea but both play a role
Genomics
o Genome: all of the DNA. Includes nuclear, mitochondrial, etc
o Genomics: study of genes and their functions, and related techniques
Includes inter-relationships with genes and environment to study their combined influence
Pharmacogenomics
o Knowing the genetic background of a patient will allow giving correct dose to the patient
o CYP2C9*2/*3/*5/*6 slow/ultra slow metabolizers. Give these patients a lower dose
Other impacts on practice
o Being given genetic results we may know information (like risk of cancer) before the patient does
o Angelina Jolie effect lots of patients want double mastectomies even though they’re not at risk of having breast
cancer in both breasts
o People can order individual genome testing 23 and me shows risk of each condition. Patients will come and ask
for solutions or preventative measures because they will know their risk for every disease

Charles Kim
37
Karyotype exercises
Question Conclusion
45 X -Turner’s syndrome. Does not have 2 sex chromosomes
Appear clinically female but with no reproductive organs
47 XY + 13 -Male with extra chromosome 13
Not normal
46 XX del(9)(q22,q24) -Female with deleted long arm of chromosome 9
Probably not normal
46 XY r(5)(p14,q33) -R stands for ring -Ends of chromosome gets cut off -Chromosome then forms a ring
Not suitable for meiosis and life
45 X / 46 XY -2 cell lines in 1 person. Some cells are 45X, some are 46XY -Normal depends on the ratio and location of cells that are 45X and 46XY -If the person has 99% of one, and 1% of the other, they will likely be fine -Can be mosaic derived from conception -Can be chimeric acquired after conception (like transplants, twins eating twins in placenta)
Depends on ratio and location
45 XY i(21)(q10) -“i" = iso. Can also be written as i(21,21)(q10,q10) -q10 = right at the beginning of the arm, closest to the centromere
Person would be normal but problematic in their children
46 XX t(1,6)(p35,p23) -T = balanced translocation -Chromosomes 1 and 6 will exchange material -“p35 of chromosome 1 is removed” -“p23 of chromosome 6 is removed” -All the info is there, just in new homes
Normal, but could be problematic in their children
46 XX t(3,7)(p13,q12) -Chromosomes 3 and 7 will exchange material -“p13 of chromosome 3 is removed” -“q12 of chromosome 7 is removed”
Normal, but could be problematic in their children
46 XX der(3) t(3,7)(p13,q12) -t(3,7)(p13,q12) the karyotype of the mother -Chromosome 3: the mother has a normal set and a “der” set -Chromosome 7: the mother has a normal set and a “der” set -Only one copy of the 3 and one copy of the 7 will be passed down to child -der(3) the part passed down to the egg -Chromosome 3: could receive normal or “der” set. Received “der” -Chromosome 7: could receive normal or “der” set. Received normal -If we’re asking what the child will be, assume the father is normal
Assuming normal father, the child formed from this egg + normal sperm will not be normal. -Extra set of 7q -Lacking set of 3p
46 XY der(7) t(7,8)(p22,q12) -t(7,8)(p22,q12) the karyotype of the father -der(7) the part passed down to the sperm cell
Assuming normal mother -Extra set of 8q -Lacking set of 7p
45 XY der(13,14)(q10,q10) -This type of notation Robertsonian translocation -Only happens to chromosomes with very small P arms -13, 14, 15, 21, 22 -Q arms of these chromosomes combine -P arms get lost, but it’s OK because P arms of these chromosomes contain redundant ribosomal DNA genes. There are TONS of copies of these genes so it’s OK to lose some
-Can survive, but child may or may not survive (see below)

Charles Kim
38
What are the 4 most likely karyotypes of a person’s egg who is 46 XX t(9,13)(q32,q22)?
Depends on which version of 9 and 13 are passed down
What are the 6 most likely karyotypes of gametes for Robertsonian translocation of 13 and 21?
Depends on which version of 13 and 21 are passed down
Will a person have a normal child if their karyotype is XY 45 t(15,15)?
Child will not be normal. Will either have monosomy or trisomy of 15
Aneuploidies: abnormalities in chromosome number
o Anaphase lag
When the cell is about to divide, all the chromosomes have to line up
If there’s a lag in the lining up process, some chromosomes may end up absent in the daughter cell
There is a high chance of this happening for the Y chromosome leads to only X Turner’s syndrome
o Nondisjunction
Chromosomes line up properly, but they fail to separate
Can happen to chromosomes in Meiosis 1 or chromatids in Meiosis 2 + Mitosis
Normal Error in M1 Error in M2
1 chromosome to each cell 2 cells = nothing 2 cells = 2 different (A,B) chromosomes
1 cell = nothing 2 cells = normal 1 cell = 2 same chromosomes
Nondisjunction exercises: where did the extra chromosome come from in this child with Down Syndrome? A marker on
chromosome 21 gave the following results:
Mom Dad Child Explanation
A/B C/D A/B/C -A/B from mom, C from dad. Mom had nondisjunction in M1
C/C A/D A/A/C -C from mom. Dad gave A/A because of nondisjunction in M2
A/A C/D A/A/D -A/A from mom, D from dad. Can’t determine if it was M1 or M2
A/B A/A A/A/A -A from mom, A from dad. Third A = could be due to M2 in mom or M1/M2 in dad
A/C D/D A/C/D -A/C from mom, D from dad. Mom had nondisjunction in M1
A/A C/C A/A/B -B came out of nowhere non paternity (oh shiiiiiiiiit) 15% of cases

Charles Kim
39
Mutations
Definitions
o Locus: physical location on a chromosome
o Gene: stretch of DNA that encodes a functional product. Traditionally called “unit of hereditary”
o Allele: version of a gene. Every person has 2 alleles (can be homozygous or heterozygous)
We are used to genes having 2 alleles, but more than 2 is possible (i.e. blood type ABO)
New alleles can be formed via a change in DNA sequence (like mutation)
o Genotype: genetic information
o Phenotype: physical manifestation of that genotype
Types of gene mutations
o Point mutation: one base is changed (C often changes with T)
o Deletion: 1+ base is removed
o Insertion: 1+ base is added
Types of chromosomal mutations: Deletions, Duplications
Impact of mutations
o Silent: protein not affected. Mutation is not in the coding region or new code is still same AA
o Neutral: AA changes to something familiar, so function is the same
o Missense: AA changes and alters function
o Nonsense: mutation makes a stop codon protein ends early
o Frameshift: insertion or deletion causes codons to shift positions
Impact of mutations on function
o Loss of function: ends up being a recessive trait because you can’t do what you used to do
Loss of function on 1 allele is OK as long as the other one is fine (> 50%)
However, if there’s loss of function on both alleles (< 50%) then it is not fine
o Addition of function: ends up being a dominant trait
If the new mutation gives 100% function and used to be 0%, then now you’re at 50% which is OK
o Dominant negative: turn on in a new time + place, and influences function of their surroundings
Shows up earlier and with more problems. Extreme version of dominant disorder
DN osteogenesis imperfecta: on top of normal symptoms of OI, it harms other systems
Goes down to 50% at a new time and place and in the process brings something else below 50%
o Reverse mutation: restores function
o Lethal mutation: kills the cell or organism. Genetically, lethal mutation means not able to reproduce
Example: duchenne muscular dystrophy males cannot live to reproduce
Somatic mutations
o Mutations that are acquired during life (replication errors, DNA repair errors, mutagens, aging)
o Not all the cells in your body are identical. There’s a mosaic of slightly different cells due to mutations
Germline mutations
o Present in every cell. This is because it was passed down from the parent
Mutation patterns
Dominant inheritance Recessive inheritance X linked recessive Mitochondrial inheritance
-Aa -Every generation affected -Affected person usually has an affected parent
-aa -Not usually in every generation -Affected usually has unaffected parents
-Caused by mutations in X chromosome -Males more frequently affected -No male-male transmission
-Only eggs contribute mitochondrial DNA -Mutations only in the mother will be passed down

Charles Kim
40
Population carrier frequency
o Follows Hardy Weinberg’s law of equilibrium: p + q = 1, and p2 + 2pq + q2 = 1
o Applied to genetics, we get AA + 2Aa + aa = 1
o Example: Cystic fibrosis affects 1/2500 births
This means aa = 1/2500 a = 1/50 A = 1 – (1/50) A = 49/50 A ≈ 1
Since A ≈ 1 and a = 1/50, the frequency of carriers (2Aa) is 2 * 1 * 1/50 = 1/25 4% carriers
Lethal X linked recessive conditions
o The mutation must be replaced to maintain the disease frequency, or else everyone with the disease will
die and the mutation itself will die out
o 1/3 mutant alleles are in affected males and they will be lost because they will die
o 2/3 sporadic cases will have a carrier mother (see X linked lethal cases below for understanding)
o 1/3 sporadic cases will be new
Mutations exercises
-Double line = consanguinity -Parents are carriers and children have it -Must be autosomal recessive
-Recessive because upper generations don’t have it -Could be autosomal or X linked -Or a brand new dominant mutation. Not likely recessive mutation
because that would mean 2 same mutations happened which is highly unlikely
-Male to male = not X linked -Every generation has it -Dominant -Autosomal dominant
-Only affects males -Goes through an unaffected woman -X linked recessive most likely -No partner = assume normal partner, just not drawn in
Question Discussion A woman has been diagnosed as having retinitis pigmentosa, an etiologically heterogeneous disease that leads to blindness. Her sister received a similar diagnosis last year but her other sister has normal eye exams. Her dad and one of her dad’s two brothers have retinitis pigmentosa but her dad’s sister is unaffected. Her dad’s father also had the disease. What is the risk of retinitis pigmentosa developing in her children? Her husband has normal vision and a negative family history for vision problems.
-Draw out a pedigree -Mode of inheritance: autosomal dominant (male to male so it can’t be X linked, and dominant because it is in every generation) -Her genotype: her dad had both affected and non-affected children. That means the dad has to be heterozygous (Aa). Assuming mom is (aa), she has to be (Aa) and cannot be (AA) -Child’s risk: Punnet square shows risk of (Aa) is 50%
Autosomal recessive 1. Risk of being affected? 2. Risk of being a carrier?
-Since it is recessive, II-1 has to be (aa) -Parents have to be (Aa). If they were (aa) they would be affected. If any of them were (AA), child wouldn’t have it -Punnett square to see risk of child II-2 -Risk = 1/4

Charles Kim
41
Autosomal recessive 1. Risk of being affected? 2. Risk of being a carrier? 3. Risk of II-2 being a carrier?
1. Same case as last question, parents have to be (Aa). Therefore, Punnett square shows that risk is 1/4 2. Use Punnett square again, risk is 1/2 3. The son is normal, so the son cannot be (aa). So, the son can be (AA), (Aa), or (Aa). The risk of being a carrier is 2/3. Not 2/4, exclude (aa)!!
Carrier risk? -Female affected and not continuous in generation autosomal recessive -First find the genotypes of every person -The parents in the top generation can be Aa x Aa, but none of the children have the disease, so assume the parent is normal whenever you can (AA x Aa)
-So according to the Punnett square, carrier risk (Aa) = 1/2
Carrier risk? Assume autosomal recessive -III-2 -III-3
-Start with II-2 because they are for sure (aa)
-Assume II-2 has child with normal partner -Risk of III-2 being a carrier = 100% -Top generation has to be Aa x Aa because they have an affected child -Punnett square parents -II-3 has 2/3 carrier chance
-Assume II-4 is normal
[2
3 𝐴𝑎 (𝐼𝐼3)] ∗ [
1
2𝐴𝑎 (𝐼𝐼𝐼3)] =
1
3 chance
Carrier risk? Assume autosomal recessive
-Start with III-1 -II-1 has to be (Aa) because he doesn’t have the disease but has a child that does -Parents could be Aa x Aa but assume Aa x AA because they only have unaffected children (always assume normal) -This means 50% chance of II-2 being a carrier -Punnett square / cross this with normal (AA) partner -50% II-2 being (Aa) * 50% III-3 being (Aa) 25%
PKU is an autosomal recessive disease. A regular man who has a child with PKU by a previous marriage marries his first cousin. 1. What is the probability that their first child will have PKU? 2. If their first child has PKU, what is the probability that their second child will also be affected?
Assuming X linked lethal, what is the risk of the fetus being affected?
-Chance that the mom is a carrier is NOT 100%. The chance is 2/3. There is 1/3 chance that the first child’s mutation was sporadic -According to Punnet square, there’s a 1/4 chance that the child is affected -However, there’s also 2/3 chance she is a carrier -2/3 * 1/4 = 2/12 = 1/6 -If we KNEW it was a boy, then the chances would be 2/3 * 1/2 = 1/3

Charles Kim
42
Assuming X linked lethal, what is the risk of the fetus being affected?
-Deceased male means the X was lethal mutated -It is for sure not an isolated sporadic case because the deceased person was affected -Chance of child being affected = 1/4 according to Punnett square
Assuming X linked lethal, what is the risk of the fetus being affected?
-The son is affected with genotype X*Y -However, this may be an isolated case. So, there is only a 2/3 chance of the mom being X*X -Mom + dad have a daughter. She can be XX or X*X. There is a 1/2 chance that she is X*X -That daughter has a child with a XY male -According to Punnett square (XY x X*X), 1/4 chance that the child is affected and male -(2/3) x (1/2) x (1/4) = 1/12
Duchenne Muscular dystrophy is an X-linked disorder that usually affects only boys. Those affected beome progressively weaker, starting early in their lives. 1. If your father’s brother had the disease but your father doesn’t, what what is the probability that you carry the allele? If you are a woman? If you are a man? 2. If a girl is diagnosed as having Duchenne muscular dystrophy, what are some possible explanations for this diagnosis?
1. -No chance that I have it, regardless of being a man or a woman. This is because the father has to be XY, they cannot be X*Y otherwise they would be affected. So since my parents are XY and XX, there is no chance that I can acquire the X* gene, male/female regardless
2. For a girl to have DMD (lol), her genotype has to be X*X* -That means mother has to be X*X (or X*X*) -Father has to be X*Y -This means the father fertilized the egg when he was really young… -Mom is either a pedophile or a XY female
Beyond single gene disorders
Cancer is not purely genetic, it can also be caused by infections
o Example: HPV can cause oropharyngeal cancers
o The cell has to be affected in multiple ways to turn into a cancer cell
Cancer genetics
o 2 genes. Both of these genes are given in its inactivated form. You can’t inherit the activated form
because if it was activated, the offspring would die in development
o Oncogene
Gain of function mutations, therefore probably dominant
Example: Philadelphia chromosome (translocation of 22:9) creates a hybrid protein bcr-abl
Causes cells to grow uncontrollably. Often found in CML (type of Leukemia)
o Tumour suppressor gene
Regulates cell cycle and DNA growth
Loss of function mutation, therefore probably recessive
If you have 2 normal copies, you will be fine. If you have 1 mutated copy, you will be at 50%
function but it is still OK. However, it does not take much environmental influence to mutate the
second copy (for example, like staying out in the sun).
Example: BRCA1. There is a 50% chance you will get cancer by age 50 if you only have 1 normal
copy of the tumour suppressor gene

Charles Kim
43
Multifactorial inheritance
o Most traits (like heart disease) are a mix of genetics
and environment. MANY FACTORS
o Can be represented as a “load”
o The red is the threshold
o If you go above the threshold, you will get the
condition/disease
o Example: The “load” for heart disease is 10. Person A has a genetic load of 8. They only need an
environmental load of 2 to be pushed over the threshold and get the disease
The higher your genetic load, the more you want to lower your environmental load
o Example (real one): cleft lip. Girls have a higher threshold than boys. It takes more load for girls to get
cleft palate. The less affected sex brings more genetic load (took them more to reach the threshold)
o Inheritance patterns: unlike single gene disorders (which goes ½ ¼ etc), the risk drops much faster
the further you are away from that relative. For example, if person A has it, it doesn’t mean their cousin
is in risk
Epigenetics
o Keeping information on your DNA without changing its sequence (methylation, histone modifications
which influence DNA packing, replication timing, position in the nucleus)
o “An epigenetic trait is a stably heritable phenotype resulting from changes in a chromosome without
alterations in the DNA sequence”
o Epigenetics keeps your liver genes turned off in your eyes so your eyes don’t make liver proteins
X inactivation – example of epigenetics
o Dosage compensation
o X chromosome has 2,000 genes critical for cell function
o Since females have 2 X chromosomes, they would have twice as much X product than males
o To compensate, females turn off one X chromosome (down to only 10~15% of total function)
o Daughter cells will have the same X inactivated as the parent cell. Really apparent in calico cats
X inactivation – physical trait in calico cats
o Black and orange colour of the fur is determined by the X chromosome
o Orange comes from 1X, black comes from 1X
o Early on (blastocyst stage), a cell chooses randomly which X to inactivate and
which one to keep
o All the daughter cells from that 1 parent will keep that same X inactivated
o As replication happens, all the daughter cells will make the colour from whichever X is activated
Are male calico cats possible?
o Yes, if they have XXY chromosomes. You always need more than 1X to be a calico cat
o Although it is possible, this male will not be fertile
Calico cat cloning
o Rainbow (original calico cat) had orange and black spots
o This cat was cloned (copy cat). X inactivation was reset this cat turned out to be all black
Influencing genes
o It’s possible through environment + epigenetics to change how genes are expressed
o Epigenetics is involved in creating and maintaining expression patterns of genes
o It does not mean re-wiring of genetics and their sequence