OR notes kim
12
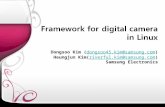
WHO Surgical Safety Checklist Prior to Induction of Anaesthesia Prior to Skin Incision Prior to patient leaving the operating theatre SIGN IN TIME OUT SIGN OUT Patient Confirmed - Identity - Site - Procedure - Consent Site marked/not applicable Anaesthesia safety check completed Pulse oximeter on patient and functioning Confirm all team members have introduced themselves by name and role Surgeon, Anaesthesia professional and nurse verbally confirm: - Patient - Site - Procedure - position anticipated critical events surgeon reviews: What are the critical or unexpected steps operative duration, anticipated blood loss? Anaesthesia team reviews: are there any patient- specific concerns? The name of the procedure recorded That instrument, sponge and needle counts are correct (or not applicable) How the specimen is labelled (including patient’s name) Whether there are any equipment problems to be addressed. Surgeon, anaesthesia professional and nurse concerns for recovery and management of this patient? Does patient have known allergy? _ Yes _ No Difficulty Antibiotic Prophylaxis given within the last 60 minutes? _ Yes _ Not applicable
-
Upload
kim-soriano -
Category
Documents
-
view
176 -
download
0
Transcript of OR notes kim

WHO Surgical Safety Checklist
Prior to Induction of Anaesthesia Prior to Skin Incision Prior to patient leaving the operating theatre
SIGN IN TIME OUT SIGN OUT Patient Confirmed
- Identity- Site- Procedure- Consent
Site marked/not applicable Anaesthesia safety check
completed Pulse oximeter on patient and
functioning
Confirm all team members have introduced themselves by name and role
Surgeon, Anaesthesia professional and nurse verbally confirm:- Patient- Site- Procedure- position
anticipated critical events surgeon reviews: What are the
critical or unexpected steps operative duration, anticipated blood loss?
Anaesthesia team reviews: are there any patient-specific concerns?
The name of the procedure recorded
That instrument, sponge and needle counts are correct (or not applicable)
How the specimen is labelled (including patient’s name)
Whether there are any equipment problems to be addressed.
Surgeon, anaesthesia professional and nurse concerns for recovery and management of this patient?
Does patient have known allergy?_ Yes_ No
Difficulty Airway/Aspiration Risks_ No_ Yes and Equitable_ Assistance Available
Risk of >500cc blood loss (7cc in children)_ Yes_ No
Antibiotic Prophylaxis given within the last 60 minutes?_ Yes_ Not applicable
Essential Imaging Displaced?_ Yes_ Not applicable_ Other Checks

PRAYER BEFORE A PROCEDURE
Heavenly Father, we believe that You are truly present in Your midst today. As we begin our work, make use of us as Your instrument of LOVE and HEALING to others. Guide us in all our decisions and actions especially in this particular operation. Bless (NAME OF PATIENT) so that whatever we do, in thought, word or action may bring about Your LOVE and HEALING to him/her for Your greater Honor and Glory. We ask You this through the intercession of Jesus, Your Son and the Blessed Virgin Mary, our Mother. Amen.
RESPONSIBILITIES OF A CIRCULATING NURSE
1. Functions as the overseer of the room during the procedure to maintain sterility.
2. Assists the entire team and the patient.
3. Send for patients at appropriate time.
4. Receives, greets, identifies the patient.
5. Checks chart for completeness.6. Assists patient in moving safely
to operating table.7. Assists the anaesthesiologist
when requested, stays with patient during induction.
8. Ties the scrubbed members’ gowns.
9. Checks operating room lights in advance for good working order, turns lights on at appropriate time and adjust when needed.
10.Prepares operative site.11.Connects catheter to drainage
bottle, or catheterize if desired by the surgeon.
12.Position the patient.13.Supplies foot stools if needed.14.Does the sponge count with the
scrub nurse.15.Watches forehead for
perspiration.16.Fills out required operative
records completely and legibly.17.Remains in the room as much as
possible to be constantly available.
18.Watches surgery, anticipates needs.
19.Sees that the surgical team is supplied with necessary item to perform the operation efficiently.
20.Uses equipment and supplies economically and conservatively.
21.Directs cleaning of the room and preparation for the next operation.
RESPONSIBILITIES OF A SCRUB NURSE
1. Sets up sterile supplies and instruments.
2. Assists the surgeon as needed throughout the surgery.
3. Assists in draping the patient in the field.
4. Assists in gowning and gloving.5. Hands instruments, sutures,
sponges, etc... as needed in efficient manner.
6. Keeps operative field tidy during case.
7. Wipes blood from instruments.8. Keeps close watch of needles,
instruments and sponges so that none will be misplaced or lost.
9. Keeps accurate instrument/needle count.
10.Supplies sterile dressing materials.

11.Discards soiled linens into hamper after checking it for instrument.
12.Cares for all instruments and supplies LEFT AFTER CASE.
PRINCIPLES OF ASEPTIC TECHNIQUE
1. All articles to be sterilize should be clean and free from foreign particles, hair, dust, dirt or discharge of any kind.
2. All materials must be sterile before it comes in contact with a sterile area. Sterilized articles become unsterile when they come in contact with any unsterile object or material.
3. Dressings and sponges once removed from the sterile container due considered contaminated.
4. Covers of containers corks from bottle etc... when removed and placed on an unsterile surface, should be placed with the sterile side up so as to prevent contamination from the unsterile surface. When held in, they should be held with the sterile side down. This helps to keep air contamination to a minimum.
5. If in doubt as to the sterility of an article, it should be considered unsterile.
a. If a sterile looking package is in a non-sterile area, it should be unsterile.
b. If the actual timing of an autoclaves lead is uncertain, it should be autoclaved and re-timed.
c. If an unsterile person brushes a sterile table, the table should be considered unsterile.
6. Wrappers on sterile packages should be of a double thickness and of sufficient size so that the package may be opened without contamination or contaminating rather any part of the contents of the package.
7. Sterile packages should have identification as to sterility and contents.
a. Sterile and unsterile articles should not be stored together.
b. Sterile packages should be dated on marked with a moist heat indicator to denote sterility.
8. The edges of anything that encloses sterile contents are considered unsterile.
a. In opening sterile packages, the ends of flaps are secured in the hand so they flaps are secured in the hand so they do not dangle loosely.
b. The last flap of a sterile package is pulled towards the person opening the package thereby exploring the package contents away from the non-sterile hand.
c. Flaps on peel-open packages should be pulled back not torn, to expose sterile contents.
d. If a sterile wrapper is used as a table cover, it amply covers the entire table surface, only the exterior and surface level of the cover are considered sterile.

OR STAFFBalisi M. Hamilig, RN, MSNSheila Paulasa, RNNelson B. Valdepenas, RN, MPARomeo A. Felipe, RNJayson Val A. Buduan, RNDebbie A. Taguba, RN, MSNRei Marc Cipriano, RNJalan Neil C. Moralit, RNJudy Heizel Asuncion, RNChristopher D. Javier, RNR-mie Mar De Laza, RNManuel S. Cortez III, RNJohn Paul Balisi, RNLionel Christian D. Gallibu, RNRichelle Lhyn I. Tallow, RNAbigail Ann R. Soriano, RNDel Marie Bautista, RN
URODr. Manuel David Hipolito
ANAESTHESIOLOGISTSDr. Visitacion D. PinsonDr. Eligio M. CapioDr. Ma. Angelicita D. CapioDr. Joan T. BaranganDr. Tarcila B. LagayanDr. Jennifer L. SaludezDr. Fe Angelica T. AlvarezDr. Reymundo M. BlancaflorDr. Edwin A. TaguinodDr. Cesar B. CatingDr. Marisa T. VerzosaDr. Maria Asucion R. HipolitoDr. Harold BanezDr. Rashelle LopezDr. Sherwin RebivezDr. Mirabelle M. Diaz
OBDr. German Tan – CardosoDr. Jose Dante MarcosDr. Grace Marie MarcosDr. Marivic TuddaoDr. Ma. Imelda Garbajal
Dr. Ellen Mary De GuzmanDr. Cristy CorpuzDr. Shahreza BaquiranDr. Criseline TolentinoDr. Maricel PalattaoDr. Claire GonzalesDr. Amelita MambaDr. Fritzie JosueDr. Lovela UsalDr. Divina Gracia ArellanoDr. Michelle SeraDr. Christiana CalaguiDr. Pua
SurgeryDr. Edwin BaguinonDr. Jherome PascualDr. Pinky d. BeranDr. Salvador BeranDr. Narciso ChanDr. Jose Alfredo FonacierDr. Sergio MambaDr. Jomar MarceloDr. Domingo MatammuDr. Rolando MesdeDr. Frederick PuaDr. Franco Rommel ReyesDr. Francis IgnacioDr. Dominadoe CentenoDr. Odessa B. TiangcoDr. Aziz Santican
EENTDr. Enouel Steve BattungDr. Dhelia Macaiba – BernaniDr. Lydia Chan – BinuluanDr. Rafael De GuzmanDr. Angelito Madrid
ORTHODr. Anthony AbogadoDr. Joegy LlanesDr. Nicolo MambaDr. Marc Paolo LasamDr. Angel Cayetano

ABBREVIATIONSROI – Removal of ImplantCSM – Cataract Senile MatureHCVD – Hypersensitive Cardiovascular Disease ITP – Idiopathic Thrombocytopenic PurpuraTURB – Transurethral Resection of the BladderTURP – Transurethral Resection of the ProstateECCE – Extracapsular Cataract ExtractionPCIOL – Posterior Chamber Intraocular LensPSARPT – Posterior Sagittal Anorectal Pull ThroughURS – UteroscopySBE – Stone Basket ExtractionBOO – Bladder Outlet ObstructionIOC – Intra Operative CholangiogramPOA – Post- Operative AdhesionsCLEA – Continuous Lumbar Epidural Anesthesia GETA – General Endotracheal AnesthesiaPHRA – Partial Hip Replacement ArthroplastyRMMA – Poly Methyl Metacrylic AcidFESS – Functional Endoscopic Sinus SurgerySAB – Subarachnoid BlockAPR – Abdomino Perineal ResectionCRD – Chronic Renal DiseaseTUI – Transurethral IncisionUVJ – Uretero – Vesicle JunctionPL – Peritoneal LavagePFC – Perineal Fluid CytologyPO – Partial OmentectomyBLND – Bilateral Lymph Node DissectionTBW – Tension Band WiringDJ Stenting – Double Junction StentingCAG – Colloid Adenomatous Goiter
TKR – Total Knee RepalcementPL – Peritoneal LavageIIH – Indirect Inguinal HerniaPL – direct LaryngoscopySSSI – Superficial Surgical Skin InfectonDMF – Distal Mucoid FistulaRGP – RetroGrade PyelographyPPUD – Perforated Peptic Ulcer DiseaseTIVA – Total Intravenous AnaesthesiaGALMA – General Anesthesia Laryngeal Mask AirwayLMA – Laryngeal Mask AirwayCHSF – Compression Hip Screw FixationAPR – Abdominoperineal ResectionR – rightL – leftS/P – status postT/C – to considerLSCS – Low Segment Caesarean SectionBTL – Bilateral Tubal Ligation“E” – EmergencyEL – Explore LaparotomyPUFT - TAHBSO – Total Abdominal Hysterectomy Bilateral Salphingo OophorectomyPEA – Polypectomy, Ethmoidectomy, ArthotomyCGO – Complete Gut ObstructionPGO – Partial Gut ObstructionAKA – Above the Knee AmputationBKA – Below the Knee AmputationCBDE – Common Bile Duct ExplorationIOC – Intra-Operative CholangiogramMPI – Multiple Physical InjuryBPA – Benign Prostatic HypertrophyICBC – Iliac Crest Bone GraftingTBW – Tension Band WiringESWL – Extra Corporeal Shock Wave Lithothripsy

RAEF – Roger Anderson External FixationORIF – Open Reduction Internal FixationMRM – Modified Radical MastectomyBPH – Benign Prostatic HypertrophyLap Chole – Laparoscopic CholecystectomyEL – Exploratory LaparotomyDL – Direct LaryngoscopySSSI – Superficial Surgical Skin InfectionDMF – Distal Mucoid Fistula
Ostomy – openingEctomy – removalPlasty – repairFE/SE – Stool Exam/ Fecal ExamUA/BUA – Uric AcidFBS – Fasting Blood SugarU/A – UrinalysisCTT – Chest Tube ThoracostomyUTZ – UltrasoundHBT – Hepatobillary TreeKUB – Kidney Urether Bladder (Full Bladder)BBL – Bone to Bone – LigamentMTB – Muscle to Bone - TendonIVP with contrast – KreatinineDecrease CBC – risk for bleedingIncrease WBC – infectionTotal Cholesterol Tryglyceride – NPO 6-8 hoursCholedochotomy – the opening of the common bile duct to remove stonesR Hemicolectomy – resection of the R half of the colon
LAYERS OF TISSUE/ABDOMEN Skin Subcutaneous Fascia Muscle Peritoneum
SURGICAL NEEDLESBy the Shaft:
Straight – used generally on the Skin
½ circle – mostly internal to skin 3/8 circle – skin, plastic surgery
By the eye: Eye present – will require
threading Lack of eye – the needle and
suture are one unit Note: either double arm-two needles, atraumatic or traumatic)
By the point: Cutting – spear or trocal Round – tapered point
OR INSTRUMENTS:
FORCEPS Mixter Kocher forcep (straight and
curve) Tissue forcep (with teeth) Thumb forcep ( without teeth) Russian tissue forcep (long and
short) Adson- with and without teeth Multiple teeth Single-tooth Ferris-Smith Forester sponge forcep
RETRACTORS Harrington retractor Army-navy retractor Deaver retractor Ribbon (malleable) retractor Richardson retractor (baby and
big) Weitlaner retractor Gelpi retractor

Beckman retractor Balfour abdominal retractor Spring wire retractor Vein retractor Mayo abdominal retractor Crile retractor Harrington retractor Non-self-retaining retractor
SCISSORS Thorek-Feldman scissors Suture scissors Mayo scissors (straight, curved,
long) Metzenbaum scissors (long,
curved, straight) Stitch scissors Steven tenotomy scissors Steven iris scissors Corneal scissors (left and right) Wescott scissors
CLAMPS Straight Glassman noncrushing
intestinal clamp Bobcock clamp Allis clamp Kocker (ochsner) clamp Backhaus towel clamp (large and
small) Mosquito (Halsted) clamp Kelly clamp (straight and curve) Crile clamp (straight and curve)
NEEDLE HOLDERS Webster needle holder
ACCESSORY INSTRUMENTS Frazier suction tip Buie probe, groove director
INSTRUMENTS FOR DILATATION AND CURRETAGE
Auvard vaginal speculum Jackson vaginal retractor Schroeder-braun uterine
tenaculum Schroeder uterine tenaculum Straight museux uterine
vulsellum forceps Goodell uterine dilator Sims uterine sound Curtic tissue forcep Bozeman uterine packing forceps Forester sponge forcep Fletcher-Van Doren uterine polyp
forcep Hank uterine dilator Hegar uterine dilator Pratt uterine dilator Sim sharo curette Heaney uterine curette Thomas dull uterine curette Kevorkian-Younge endocervical
curette
MINOR ORTHOPEDIC SURGERY INSTRUMENTS
Skin hooks Senn retractor Rake (Volkmann) retractor Meyerding finger retractors with
blade Inge lamina spreader Heiss retractor Freer elevator Key periosteal elevator Brun (Spratt) curette (size 3-0) Mouse curette (double ended) Maltz-lip sett nasal rasp Carroll tendon passing Kern bone-holders Hike osteotomes Zimmer stainless steel mallet Zimmer bone cutting forceps
(double action) Kleinert-Kutz rongeur (double
action)

INSTRUMENTS FOR MAJOR ORTHOPEDIC SURGERY
Sofield retractor Hibbs retractor Meyerding retractor Bennet bone elevator retractor Israel rake retractor Leksell bone rongeur Jansen-Zaufel bone rongeur Echlin bone rongeur Lowman bone holding clamp Bone hook Kep periosteal elevator Crego periosteal elevators Ferris – Smith tissue forcep Brun bone curette (straight and
angled) Hohmann retractor Bone chisel Smith-Peterson osteotomes
(curved and straight) Zimmer bone mallet Zuelzer awl Kiene bone tomp Maltz nasal rasp Universal file Kerrison cervical rongeurs Cushing pituitary rongeur
(straight and curve) Hand drill with Jacobs chuck key Zimmer drills bits Sadle – nosed pliers Standard pliers Vise-grip pliers Traction bow T-wrench Philips screw-driver Straight screwdriver Stille-Mosley bone cutting forceps Lane bone holding forcep Bishop bone clamp Wire cutter Multiaction pin cutter Solid Gigli saw handles with Gigli
saw blade
SUTURESAbsorbable Non-absorbable
Plain 2/0 Prolene 0Plain 3/0 Prolene 7-0PDS II 0 Prolene 3-0Chromic 2-0 Mersilk 0Chromic 1 Mersilk 3-0Chromic 0 Mersilk 2-0Chromic 3/0 Ethilon 10-0Chromic 4/0Vicryl 4-0Vicryl 5-0
SUTURE COLORSProlene – Blue Ethilon – GreenMersilk (Silk) – BlackVicyl – VioletPbs – All NylonChromic – BrownPlain – Monocryl – dark blue