OPTIMISING DIAGNOSIS AND TREATMENT OF COAGULOPATHY … · OPTIMISING DIAGNOSIS AND TREATMENT OF...
238
OPTIMISING DIAGNOSIS AND TREATMENT OF COAGULOPATHY IN SEVERELY INJURED TRAUMA PATIENTS Kirsten Balvers
Transcript of OPTIMISING DIAGNOSIS AND TREATMENT OF COAGULOPATHY … · OPTIMISING DIAGNOSIS AND TREATMENT OF...
OPTIMISING DIAGNOSIS AND TREATMENT OF COAGULOPATHY IN SEVERELY INJURED
TRAUMA PATIENTS
Kirsten Balvers
OPTIMISING DIAGNOSIS AND TREATMENT OF COAGULOPATHY IN SEVERELY INJURED
TRAUMA PATIENTS
Kirsten Balvers
Optimising diagnosis and treatment of coagulopathy in severely injured trauma patientsThesis, University of Amsterdam, The Netherlands
Paranimfen: Susan Hatzmann, Monique Walenkamp, Elisa Ng, Sanne TaksISBN: 978-94-028-0202-3Cover design and layout: Susan HatzmannPrinted by: Ipskamp Printing
© K. Balvers, Amsterdam, The Netherlands, 2016The copyright of the published and accepted articles has been transferred to the respective publishers. No part of this thesis may be reproduced, stored or transmitted, in any form or by any means, without permission of the author.
The printing of this thesis was financially supported by: Tem International GmbH, CSL Behring, Nederlandse Vereniging voor Traumachirurgie, TraumaNet AMC, Wetenschappelijk Fonds Chirurgie AMC, Academisch Medisch Centrum (AMC), ABN AMRO, Chipsoft B.V.
OPTIMISING DIAGNOSIS AND TREATMENT OF COAGULOPATHY IN SEVERELY INJURED
TRAUMA PATIENTS
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor
aan de Universiteit van Amsterdam
op gezag van de Rector Magnificus
prof. dr. D.C. van den Boom
ten overstaan van een door het College voor Promoties ingestelde commissie,
in het openbaar te verdedigen in de Agnietenkapel
op vrijdag 24 juni 2016, te 14:00 uur
door Kirsten Balvers
geboren te Woerden
PROMOTIECOMMISSIE
Promotor: Prof. dr. J.C. Goslings Universiteit van Amsterdam
Co-promotor: Prof. dr. N.P. Juffermans Universiteit van Amsterdam
Overige leden: Prof. dr. C. Boer Vrije Universiteit Amsterdam Dr. S.S. Zeerleder Universiteit van Amsterdam Prof. dr. M.J. Schultz Universiteit van Amsterdam Prof. dr. L.P.H. Leenen Universiteit Utrecht Prof. dr. M.W. Hollmann Universiteit van Amsterdam Prof. dr. K. Brohi Queen Mary University of London
Faculteit der Geneeskunde
CONTENTS
General introduction and outline of the thesis
PART 1 DIAGNOSIS
Chapter 1 The utility of thromboelastometry (ROTEM®) and thromboelastography (TEG®) to detect coagulation disorders in non-bleeding ICU patients Chapter 2 Thromboelastometry and organ failure in trauma patients: a prospective cohort study Chapter 3 Haemoglobin level and neurologic outcome in patients with severe traumatic brain injury Chapter 4 Endogenous microparticles drive the pro-inflammatory host immune response in severely injured trauma patients
PART 2 TREATMENT
Chapter 5 Risk factors related to trauma-induced coagulopathy and resuscitation strategies for the development of multiple organ failure in severely injured trauma patients
Chapter 6 Is hypothermia at ICU admission an independent predictor of 28-days mortality? Chapter 7 Effects of implementation of a massive transfusion protocol on the usage of blood products and transfusion strategies Chapter 8 Are there any alternatives for transfusion of AB plasma as universal donor in an emergency release setting? Chapter 9 Therapeutic strategies associated with improved outcomes in bleeding trauma patients
Chapter 10 Transfusion strategy associated with correction of coagulopathy as detected by ROTEM® in bleeding trauma patients
9
23
35
51
63
77
103
119
135
149
169
Summary and future perspectivesSamenvatting en toekomstperspectievenResearch portfolioList of publicationsDankwoordCurriculum Vitae
195207221225229223


GENERAL INTRODUCTION AND OUTLINE OF THE THESIS

10 |
GENERAL INTRODUCTION
Trauma has a profound impact on public health around the world. Yearly approximately 5 million people die due to traumatic injury, which is 1 out of every 3 severely injured patients1. Therefore, improving survival after trauma is a major challenge in which timely therapy is of great importance. Although increased knowledge about the mechanisms and pathophysiology of traumatic injury to the human body have led to improved trauma care, surgical procedures, and critical care management over the last decades, still a large proportion of patients die after trauma. Better understanding of how the injury and treatment affect the outcome after trauma may result in a decreased mortality. However, in this field there is still a lot of work to do. In trauma patients, massive haemorrhage is one of the leading causes of mortality. Exsanguination accounts for more than 30% of mortality in trauma patients2. The main part of the treatment of massive haemorrhage is to stop the bleeding. However, the development of trauma-induced coagulopathy (TIC) hampers this and exacerbates the bleeding. Therefore, treatment of coagulopathy is a cornerstone in achieving haemostasis and in therapy of bleeding trauma patients.
COAGULOPATHY
Coagulopathy is a condition of the blood in which the blood`s ability to coagulate is impaired. However, the term coagulopathy can relate to several divers conditions. Intensivists associate coagulopathy with disseminated intravascular coagulopathy (DIC), which is characterized by an increased tendency of clotting of the blood, also known as hypercoagulopathy, which is thought to contribute to organ failure and late mortality. Trauma surgeons interpret coagulopathy as a diminished clotting function, also known as hypocoagulopathy, which is associated with early mortality. Additionally, several terms in literature are used to refer to the same condition. Terms such as acute traumatic coagulopathy (ATC), early coagulopathy of trauma (ECT), trauma-induced coagulopathy (TIC), and the acute coagulopathy of trauma-shock (ACoTS) are commonly used. Both the various interpretations and terms used for coagulopathy, illustrate the lack of knowledge on the dynamics of the coagulation process in trauma. In this thesis we will further discuss coagulopathy after trauma. The term in this thesis used for coagulopathy is trauma-induced coagulopathy (TIC) and refers to a diminished clotting function, also knowns as a hypocoagulable state, upon arrival at the Emergency Department.
| 11INTRODUCTION
TRAUMA-INDUCED COAGULOPATHY
Almost 25% of the severely injured trauma patients have developed hypocoagulopathy on arrival to the Emergency Department3, 4. Compared to trauma patients without coagulopathy, patients with TIC have a fourfold higher risk for mortality. Early mortality is determined by a hypocoagulable state and bleeding to death, whereas late mortality is determined by a hypercoagulable state and the development of multiple organ failure2, 5.
The hypocoagulable state increases the risk for bleeding and exacerbates blood loss. This early mortality by haemorrhage is one of the leading causes of death in trauma patients, but it is also the most preventable cause of death6-8. Treatment of coagulopathy is a cornerstone in achieving haemostasis and in therapy of bleeding trauma patients, as controlling the bleeding by a surgical procedure is not possible without a good functioning clotting system. However, overtreatment of TIC may result in a hypercoagulable state, which is associated with the development of multiple organ failure and late mortality. Therefore, to treat TIC adequately, knowledge about the pathophysiology and dynamics of coagulopathy in the course of severe trauma is required.
PATHOGENESIS OF TRAUMA-INDUCED COAGULOPATHY
Conventional theory holds that early TIC was caused by hypothermia, acidosis and dilution, also known as the lethal triad. Hypothermia and acidosis result in the dysfunction of clotting enzymes, whereas administration of resuscitation fluids dilutes the concentration of clotting factors in blood9, 10. TIC results in an increased blood loss with exacerbation of hypovolemic shock and concomitant decreased perfusion of organs, which leads to hypothermia, acidosis and subsequently death2-4, 11.
However, nowadays it is suggested that early development of TIC is caused by external factors, like hypothermia, dilution and acidosis, in combination with a response of the body to tissue injury. After tissue injury, endothelial cell activation results in the initiation of the pro-inflammatory response system and the triggering of thrombo-thrombomodulin complexes. These complexes activate protein C, also known as the protein C pathway. Activated protein C inhibits clotting factors V and VIII thereby reducing the clotting function. However, in trauma, the presence of shock and sustained hypoperfusion, causes an increased release of thrombo-thrombomodulin complexes, which results in a widespread protein C activation and an impaired clot formation. Additionally, besides the fact that clotting factor V and VIII are inhibited by activated protein C,
12 |
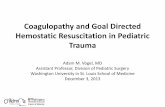
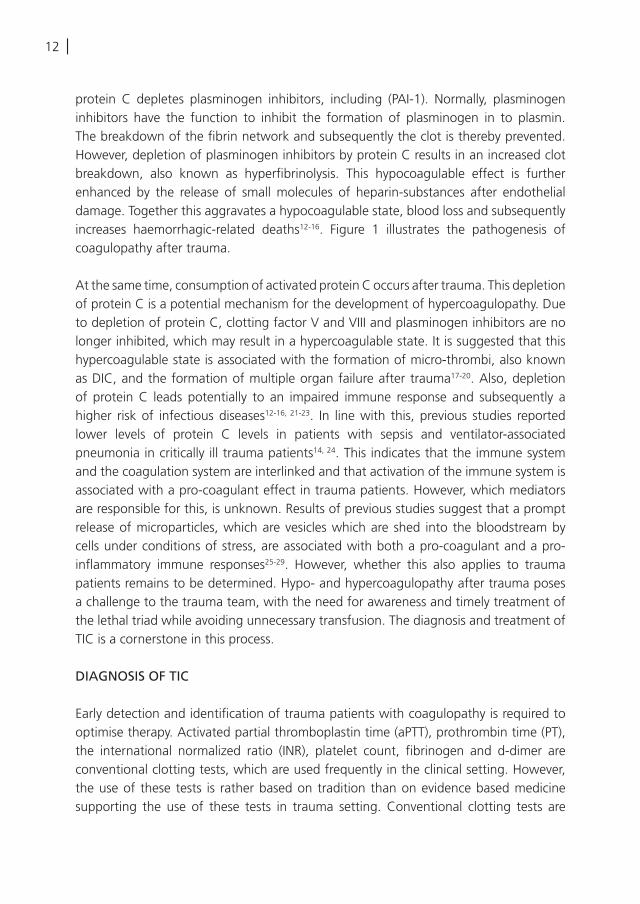
protein C depletes plasminogen inhibitors, including (PAI-1). Normally, plasminogen inhibitors have the function to inhibit the formation of plasminogen in to plasmin. The breakdown of the fibrin network and subsequently the clot is thereby prevented. However, depletion of plasminogen inhibitors by protein C results in an increased clot breakdown, also known as hyperfibrinolysis. This hypocoagulable effect is further enhanced by the release of small molecules of heparin-substances after endothelial damage. Together this aggravates a hypocoagulable state, blood loss and subsequently increases haemorrhagic-related deaths12-16. Figure 1 illustrates the pathogenesis of coagulopathy after trauma.
At the same time, consumption of activated protein C occurs after trauma. This depletion of protein C is a potential mechanism for the development of hypercoagulopathy. Due to depletion of protein C, clotting factor V and VIII and plasminogen inhibitors are no longer inhibited, which may result in a hypercoagulable state. It is suggested that this hypercoagulable state is associated with the formation of micro-thrombi, also known as DIC, and the formation of multiple organ failure after trauma17-20. Also, depletion of protein C leads potentially to an impaired immune response and subsequently a higher risk of infectious diseases12-16, 21-23. In line with this, previous studies reported lower levels of protein C levels in patients with sepsis and ventilator-associated pneumonia in critically ill trauma patients14, 24. This indicates that the immune system and the coagulation system are interlinked and that activation of the immune system is associated with a pro-coagulant effect in trauma patients. However, which mediators are responsible for this, is unknown. Results of previous studies suggest that a prompt release of microparticles, which are vesicles which are shed into the bloodstream by cells under conditions of stress, are associated with both a pro-coagulant and a pro-inflammatory immune responses25-29. However, whether this also applies to trauma patients remains to be determined. Hypo- and hypercoagulopathy after trauma poses a challenge to the trauma team, with the need for awareness and timely treatment of the lethal triad while avoiding unnecessary transfusion. The diagnosis and treatment of TIC is a cornerstone in this process.
DIAGNOSIS OF TIC
Early detection and identification of trauma patients with coagulopathy is required to optimise therapy. Activated partial thromboplastin time (aPTT), prothrombin time (PT), the international normalized ratio (INR), platelet count, fibrinogen and d-dimer are conventional clotting tests, which are used frequently in the clinical setting. However, the use of these tests is rather based on tradition than on evidence based medicine supporting the use of these tests in trauma setting. Conventional clotting tests are
| 13INTRODUCTION
FIG
UR
E 1:
Pat
hoge
nesi
s of
coa
gulo
path
y
14 |
very time-consuming as results become available after at least 40-60 minutes. Also, these tests reflect only a part of the clotting profile. Thereby, these tests have minimal impact on transfusion practice in bleeding trauma patients30-33. Although these tests are commonly used to evaluate and to predict bleeding, these tests are originally designed to diagnose coagulation disorders and to evaluate anticoagulant medication. Therefore, transfusion practice is currently more an empiric procedure than based upon adequate clotting tests. This is alarming, as conventional clotting tests do not allow for correct diagnosis of TIC and hence no targeted therapy is possible. In conclusion, no adequate diagnostic and monitoring tools for coagulopathy in trauma patients are available nowadays.
Viscoelatic Heamostatic Assays (VHA), like thromboelastometry (ROTEM®) and thromboelastography (TEG®), are rapid tests which reflect the whole coagulation status. Within 5-10 minutes a first impression of the clotting function is visualized. VHA tests provide an impression for global haemostasis, including the measurement of the total coagulation process from clot formation until clot breakdown. Therefore the use of these VHA assays may be a valuable alternative for diagnosing and monitoring of the effectivity of treatment of TIC in bleeding trauma patients33-38. However, clear reference values for coagulopathy in trauma patients still need to be determined, as the manufacturer has provided only general reference values. Furthermore, it is unknown what the monitoring capacity of these VHA assays is and whether implementation of these tests results in optimization of transfusion by avoiding transfusion unnecessary blood products and pro-coagulants. Additionally, it remains to be determined whether VHA assays can be used to provide targeted transfusion in trauma patients and what the triggers and targets are for transfusion. Currently, the suspicion of bleeding, hypovolemia and the haemoglobin level are frequently used as triggers for transfusion, however it is unknown whether these factors predict bleeding adequately and are able to use as a transfusion target. Therefore, adequate and rapid diagnostic tools for coagulopathy are required to optimise and monitor treatment of coagulopathic trauma patients.
TREATMENT OF TIC
Over the last decades, research efforts in the field of transfusion practice in trauma patients have been directed towards treatment of the principle drivers of the lethal triad, including hypothermia, acidosis and coagulopathy. Therefore, supportive care in trauma consists of prevention of hypothermia and the administration of fewer fluids. From this point of view, prevention of hypothermia and a restricted fluid policy have become part of standard trauma care. Additionally, transfusion practice has evolved from
| 15INTRODUCTION
A
B
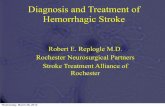
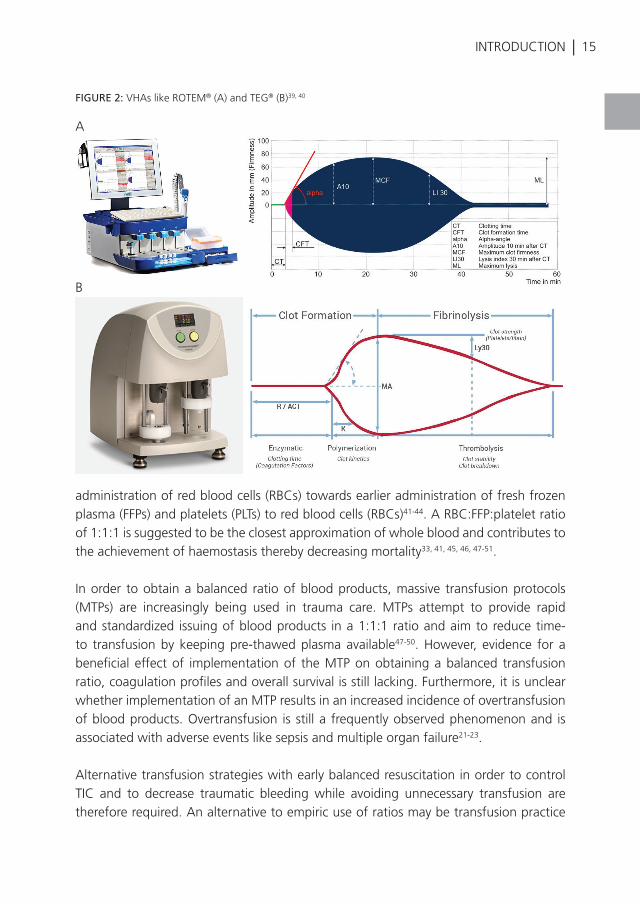
FIGURE 2: VHAs like ROTEM® (A) and TEG® (B)39, 40
administration of red blood cells (RBCs) towards earlier administration of fresh frozen plasma (FFPs) and platelets (PLTs) to red blood cells (RBCs)41-44. A RBC:FFP:platelet ratio of 1:1:1 is suggested to be the closest approximation of whole blood and contributes to the achievement of haemostasis thereby decreasing mortality33, 41, 45, 46, 47-51.
In order to obtain a balanced ratio of blood products, massive transfusion protocols (MTPs) are increasingly being used in trauma care. MTPs attempt to provide rapid and standardized issuing of blood products in a 1:1:1 ratio and aim to reduce time-to transfusion by keeping pre-thawed plasma available47-50. However, evidence for a beneficial effect of implementation of the MTP on obtaining a balanced transfusion ratio, coagulation profiles and overall survival is still lacking. Furthermore, it is unclear whether implementation of an MTP results in an increased incidence of overtransfusion of blood products. Overtransfusion is still a frequently observed phenomenon and is associated with adverse events like sepsis and multiple organ failure21-23.
Alternative transfusion strategies with early balanced resuscitation in order to control TIC and to decrease traumatic bleeding while avoiding unnecessary transfusion are therefore required. An alternative to empiric use of ratios may be transfusion practice
16 |
guided by VHA assays, as these tests are rapid and reflect the coagulation status adequately. Furthermore, these tests have shown promising results in their ability to detect and to monitor coagulopathy34, 37, 38. As results become available within 5-10 minutes after initiating the VHA assays, these tests may be used to guide transfusion of blood products, pro-coagulant and antifibrinolytic agents. Subsequently, VHA assays could be incorporated in a transfusion algorithm, which supports rapid clinical management of severely injured trauma patients. However, the additional value of the use of VHA assays in trauma resuscitation has to be determined.
AIM AND OUTLINE OF THE THESIS
This thesis focusses on knowledge gaps in the field of diagnosis and treatment of TIC in severely injured trauma patients. In order to explore potential diagnostic tools for TIC and to investigate potential strategies to optimise treatment of TIC, the Academic Medical Center of Amsterdam has been participating in the International Trauma Research Network (INTRN) since 2012. The INTRN is a consortium of 6 European Level-1 trauma centres, which received funding from the European Union Framework Programme 7 (FP7) to perform research in the field of coagulopathy after trauma. This thesis is partly established by collaboration with INTRN and by using a large database of trauma patients. The aim of this thesis is to evaluate diagnostic tools for TIC and to investigate which transfusion strategy is associated with the best outcome after trauma. The first part of this thesis focusses on optimising diagnosis of TIC, whereas the second part of this thesis focusses on optimising treatment of TIC.
PART 1 DIAGNOSIS OF COAGULOPATHY
• Chapter 1 provides a narrative review of the utility of ROTEM® and TEG® to detect coagulopathy in critically ill non-bleeding patients.
• Chapter 2 assesses the predictive value of hypercoagulopathy detected by ROTEM® for the development of multiple organ failure.
• Chapter 3 determines the association between the haemoglobin level and the neurologic outcome of patients after traumatic brain injury.
• Chapter 4 investigates the role of microparticles in mediating the immune response following trauma.
TREATMENT OF COAGULOPATHY
• Chapter 5 gives a systematic overview of the risk factors related to coagulopathy and transfusion practice for adverse outcome after major trauma.
| 17INTRODUCTION
• Chapter 6 emphasizes the detrimental effect of accidental hypothermia on mortality in coagulopathic trauma patients at admittance to the intensive care unit.
• Chapter 7 studies the effect of the introduction of an MTP on the use of blood products and transfusion ratios.
• Chapter 8 systematically determines alternatives for the transfusion of AB-plasma in massively bleeding patients
• Chapter 9 investigates which transfusion strategy is associated with best outcome in bleeding trauma patients
• Chapter 10 determines the response of ROTEM® to transfusion practice in bleeding trauma patients.
18 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
Haagsma JA, Graetz N, Bolliger I, Naghavi
M, Higashi H, Mullany EC, et al. The global
burden of injury: incidence, mortality,
disability-adjusted life years and time trends
from the Global Burden of Disease study
2013. Injury prevention : journal of the
International Society for Child and Adolescent
Injury Prevention. 2016;22(1):3-18.
Sauaia A, Moore FA, Moore EE, Moser KS,
Brennan R, Read RA, et al. Epidemiology of
trauma deaths: a reassessment. J Trauma.
1995;38(2):185-93.
Brohi K, Singh J, Heron M, Coats T.
Acute traumatic coagulopathy. J Trauma.
2003;54(6):1127-30.
MacLeod JB, Lynn M, McKenney MG, Cohn
SM, Murtha M. Early coagulopathy predicts
mortality in trauma. J Trauma. 2003;55(1):39-
44.
Krug EG, Sharma GK, Lozano R. The global
burden of injuries. Am J Public Health.
2000;90(4):523-6.
Bellamy RF. The causes of death in conventional
land warfare: implications for combat casualty
care research. Mil Med 1984;149(2):55-62.
Holcomb JB, McMullin NR, Pearse L, Caruso
J, Wade CE, Oetjen-Gerdes L, et al. Causes
of death in U.S. Special Operations Forces in
the global war on terrorism: 2001-2004. Ann
Surg 2007;245(6):986-91.
Esposito TJ, Sanddal ND, Hansen JD, Reynolds
S. Analysis of preventable trauma deaths and
inappropriate trauma care in a rural state. J
Trauma. 1995;39(5):955-62.
Maegele M, Lefering R, Yucel N, Tjardes T,
Rixen D, Paffrath T, et al. Early coagulopathy in
multiple injury: an analysis from the German
Trauma Registry on 8724 patients. Injury.
2007;38(3):298-304.
Wafaisade A, Wutzler S, Lefering R, Tjardes
T, Banerjee M, Paffrath T, et al. Drivers of
acute coagulopathy after severe trauma: a
multivariate analysis of 1987 patients. Emerg
Med J 2010;27(12):934-9.
Cosgriff N, Moore EE, Sauaia A, Kenny-
Moynihan M, Burch JM, Galloway B. Predicting
life-threatening coagulopathy in the massively
transfused trauma patient: hypothermia and
acidoses revisited. J Trauma. 1997;42(5):857-
61.
Maegele M, Schochl H, Cohen MJ. An update
on the coagulopathy of trauma. Shock.
2014;41 Suppl 1:21-5.
Brohi K, Cohen MJ, Ganter MT, Matthay
MA, Mackersie RC, Pittet JF. Acute traumatic
coagulopathy: initiated by hypoperfusion:
modulated through the protein C pathway?
Ann Surg 2007;245(5):812-8.
Cohen MJ, Call M, Nelson M, Calfee CS,
Esmon CT, Brohi K, et al. Critical role of
activated protein C in early coagulopathy
and later organ failure, infection and death in
trauma patients. Ann Surg 2012;255(2):379-
85.
Kutcher ME, Xu J, Vilardi RF, Ho C, Esmon
CT, Cohen MJ. Extracellular histone release in
response to traumatic injury: implications for
a compensatory role of activated protein C. J
Trauma Acute Care Surg 2012;73(6):1389-94.
Rehm M, Bruegger D, Christ F, Conzen P, Thiel
M, Jacob M, et al. Shedding of the endothelial
glycocalyx in patients undergoing major
vascular surgery with global and regional
ischemia. Circulation. 2007;116(17):1896-
906.
Gando S, Nakanishi Y, Tedo I. Cytokines
and plasminogen activator inhibitor-1 in
posttrauma disseminated intravascular
coagulation: relationship to multiple organ
dysfunction syndrome. Crit Care Med
1995;23(11):1835-42.
Gando S, Nakanishi Y, Kameue T, Nanzaki S.
Soluble thrombomodulin increases in patients
with disseminated intravascular coagulation
and in those with multiple organ dysfunction
syndrome after trauma: role of neutrophil
elastase. J Trauma. 1995;39(4):660-4.
Gando S, Nanzaki S, Kemmotsu O.
| 19
REFERENCES
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Disseminated intravascular coagulation and
sustained systemic inflammatory response
syndrome predict organ dysfunctions after
trauma: application of clinical decision
analysis. Ann Surg 1999;229(1):121-7.
Paffrath T, Wafaisade A, Lefering R, Simanski
C, Bouillon B, Spanholtz T, et al. Venous
thromboembolism after severe trauma:
incidence, risk factors and outcome. Injury.
2010;41(1):97-101.
Sauaia A, Moore FA, Moore EE, Haenel JB,
Read RA, Lezotte DC. Early predictors of
postinjury multiple organ failure. Arch Surg
1994;129(1):39-45.
Dewar DC, Tarrant SM, King KL, Balogh ZJ.
Changes in the epidemiology and prediction
of multiple-organ failure after injury. J Trauma
Acute Care Surg 2013;74(3):774-9.
Frohlich M, Lefering R, Probst C, Paffrath T,
Schneider MM, Maegele M, et al. Epidemiology
and risk factors of multiple-organ failure
after multiple trauma: an analysis of 31,154
patients from the TraumaRegister DGU. J
Trauma Acute Care Surg 2014;76(4):921-7.
Choi Q, Hong KH, Kim JE, Kim HK. Changes
in plasma levels of natural anticoagulants in
disseminated intravascular coagulation: high
prognostic value of antithrombin and protein
C in patients with underlying sepsis or severe
infection. Annals of laboratory medicine.
2014;34(2):85-91.
Fujimi S, Ogura H, Tanaka H, Koh T,
Hosotsubo H, Nakamori Y, et al. Increased
production of leukocyte microparticles with
enhanced expression of adhesion molecules
from activated polymorphonuclear leukocytes
in severely injured patients. J Trauma.
2003;54(1):114-9.
Mastronardi ML, Mostefai HA, Meziani F,
Martinez MC, Asfar P, Andriantsitohaina R.
Circulating microparticles from septic shock
patients exert differential tissue expression of
enzymes related to inflammation and oxidative
stress. Crit Care Med 2011;39(7):1739-48.
Morel O, Toti F, Hugel B, Bakouboula B,
Camoin-Jau L, Dignat-George F, et al.
Procoagulant microparticles: disrupting the
vascular homeostasis equation? Arterioscler
Thromb Vasc Biol 2006;26(12):2594-604.
Ogura H, Kawasaki T, Tanaka H, Koh T,
Tanaka R, Ozeki Y, et al. Activated platelets
enhance microparticle formation and platelet-
leukocyte interaction in severe trauma and
sepsis. J Trauma. 2001;50(5):801-9.
Ogura H, Tanaka H, Koh T, Fujita K, Fujimi
S, Nakamori Y, et al. Enhanced production
of endothelial microparticles with increased
binding to leukocytes in patients with severe
systemic inflammatory response syndrome. J
Trauma. 2004;56(4):823-30.
Holcomb JB, Minei KM, Scerbo ML, Radwan
ZA, Wade CE, Kozar RA, et al. Admission
rapid thrombelastography can replace
conventional coagulation tests in the
emergency department: experience with
1974 consecutive trauma patients. Annals of
surgery. 2012;256(3):476-86.
Dzik WH. Predicting hemorrhage using
preoperative coagulation screening assays.
Current hematology reports. 2004;3(5):324-
30.
Park MS, Martini WZ, Dubick MA,
Salinas J, Butenas S, Kheirabadi BS, et
al. Thromboelastography as a better
indicator of hypercoagulable state after
injury than prothrombin time or activated
partial thromboplastin time. J Trauma.
2009;67(2):266-75; discussion 75-6.
Davenport R, Manson J, De’Ath H, Platton
S, Coates A, Allard S, et al. Functional
definition and characterization of acute
traumatic coagulopathy. Crit Care Med
2011;39(12):2652-8.
Johansson PI, Stensballe J. Effect of Haemostatic
Control Resuscitation on mortality in massively
bleeding patients: a before and after study.
Vox Sang 2009;96(2):111-8.
Woolley T, Midwinter M, Spencer P, Watts
INTRODUCTION
20 |
REFERENCES
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
S, Doran C, Kirkman E. Utility of interim
ROTEM((R)) values of clot strength, A5
and A10, in predicting final assessment of
coagulation status in severely injured battle
patients. Injury. 2013;44(5):593-9.
Rugeri L, Levrat A, David JS, Delecroix E,
Floccard B, Gros A, et al. Diagnosis of early
coagulation abnormalities in trauma patients
by rotation thrombelastography. Journal
of thrombosis and haemostasis : JTH.
2007;5(2):289-95.
Schochl H, Nienaber U, Hofer G, Voelckel
W, Jambor C, Scharbert G, et al. Goal-
directed coagulation management of major
trauma patients using thromboelastometry
(ROTEM)-guided administration of fibrinogen
concentrate and prothrombin complex
concentrate. Crit Care. 2010;14(2):R55.
Schochl H, Nienaber U, Maegele M,
Hochleitner G, Primavesi F, Steitz B, et al.
Transfusion in trauma: thromboelastometry-
guided coagulation factor concentrate-based
therapy versus standard fresh frozen plasma-
based therapy. Crit Care. 2011;15(2):R83.
GmbH TI. Available from: https://www.rotem.
de.
Heamonetics. Available from: http://teg.
haemonetics.com/.
Holcomb JB, del Junco DJ, Fox EE, Wade
CE, Cohen MJ, Schreiber MA, et al. The
prospective, observational, multicenter,
major trauma transfusion (PROMMTT) study:
comparative effectiveness of a time-varying
treatment with competing risks. JAMA Surg
2013;148(2):127-36.
Kutcher ME, Kornblith LZ, Narayan R, Curd V,
Daley AT, Redick BJ, et al. A paradigm shift
in trauma resuscitation: evaluation of evolving
massive transfusion practices. JAMA Surg
2013;148(9):834-40.
Wafaisade A, Maegele M, Lefering R, Braun
M, Peiniger S, Neugebauer E, et al. High
plasma to red blood cell ratios are associated
with lower mortality rates in patients receiving
multiple transfusion (4</=red blood cell
units<10) during acute trauma resuscitation.
J Trauma. 2011;70(1):81-8.
Zink KA, Sambasivan CN, Holcomb JB,
Chisholm G, Schreiber MA. A high ratio of
plasma and platelets to packed red blood
cells in the first 6 hours of massive transfusion
improves outcomes in a large multicenter
study. Am J Surg 2009;197(5):565-70.
Holcomb JB, Jenkins D, Rhee P, Johannigman
J, Mahoney P, Mehta S, et al. Damage
control resuscitation: directly addressing the
early coagulopathy of trauma. J Trauma.
2007;62(2):307-10.
Holcomb JB, Tilley BC, Baraniuk S, Fox EE,
Wade CE, Podbielski JM, et al. Transfusion
of plasma, platelets, and red blood cells in a
1:1:1 vs a 1:1:2 ratio and mortality in patients
with severe trauma: the PROPPR randomized
clinical trial. JAMA. 2015;313(5):471-82.
Ball CG, Dente CJ, Shaz B, Wyrzykowski AD,
Nicholas JM, Kirkpatrick AW, et al. The impact
of a massive transfusion protocol (1:1:1)
on major hepatic injuries: does it increase
abdominal wall closure rates? Can J Surg
2013;56(5):E128-E34.
Khan S, Allard S, Weaver A, Barber C,
Davenport R, Brohi K. A major haemorrhage
protocol improves the delivery of blood
component therapy and reduces waste
in trauma massive transfusion. Injury.
2013;44(5):587-92.
McDaniel LM, Neal MD, Sperry JL, Alarcon
LH, Forsythe RM, Triulzi D, et al. Use of a
massive transfusion protocol in nontrauma
patients: activate away. J Am Coll Surg
2013;216(6):1103-9.
O’Keeffe T, Refaai M, Tchorz K, Forestner JE,
Sarode R. A massive transfusion protocol to
decrease blood component use and costs.
Arch Surg 2008;143(7):686-90.
Schuster KM, Davis KA, Lui FY, Maerz LL,
Kaplan LJ. The status of massive transfusion
protocols in United States trauma centers:

| 21
REFERENCES
massive transfusion or massive confusion?
Transfusion. 2010;50(7):1545-51.
INTRODUCTION
1K. Balvers, M.C.A. Muller, N.P. Juffermans
Annual Update in Intensive Care and Emergency Medicine 2014
THE UTILITY OF THROMBOELASTOMETRY (ROTEM®) OR THROMBOELASTOGRAPHY (TEG®) IN
NON-BLEEDING ICU PATIENTS
CHAPTER 124 |
INTRODUCTION
A hypocoagulable state is highly prevalent in critically ill patients. An INR of >1.5 occurs in 30% of patients, associated with increased mortality1. Also, of critically ill patients, up to 40% develops thrombocytopenia during their intensive care unit (ICU) stay2-4, associated with increased length of stay, need for transfusion of blood products and increased mortality5. A hypercoagulable state is also associated with adverse outcome, as well as with increased thrombo-embolic events6. Disseminated intravascular coagulation (DIC) develops in 10 to 20% of ICU patients. A hypercoagulable state contributes to organ failure and is associated with a high mortality, ranging from 45% to 78%7.
Coagulopathy is thought to result from an imbalance between activation of coagulation and impaired inhibition of coagulation and fibrinolysis. Activation is triggered by tissue factor, which is expressed in reaction to cytokines or endothelial damage. Impaired inhibition of coagulation is the consequence of reduced plasma levels of antithrombin (AT), depressed activity of the protein C system and decreased levels of tissue factor pathway inhibitor (TFPI). A decrease in the fibrinolytic system is due to increased levels of plasminogen activator inhibitor type 1 (PAI-1)8;9. This disturbance between components of the coagulation system leads to a variable clinical picture, ranging from patients with an increased bleeding tendency (hypocoagulable state) to those with DIC with (micro-) vascular thrombosis (hypercoagulable state).
Assessment of coagulation status in patients is complex. Global coagulation tests, including activated partial thromboplastin time (aPTT) and prothrombin time (PT), are used clinically. However, these tests are of limited value and their ability to accurately reflect in vivo hypocoagulable state is questioned10. Also, aPTT/PT reflects a part of the coagulation system and does not provide information on the full balance between coagulation, anti-coagulation and fibrinolysis. Hypercoagulable state can be assessed by increased levels of d-dimers, but specificity is limited10. Impaired function of the anticoagulant system can be diagnosed by measuring plasma levels of naturally occurring anticoagulant factors AT, protein C and TFPI. However, these are not readily available for clinical use. Apart from the DIC score, there are no diagnostic tests which evaluate a hypercoagulable state. Also, markers of the activity of the fibrinolytic system are not used at the bedside10.
TEG®/ROTEM® TESTS
Rotational thromboelastography (TEG®/ROTEM®) is a point of care test, which evaluates whole clot formation and degradation. The thromboelastogram arises through
| 25THE UTILITY OF ROTEM® OR TEG® IN NON-BLEEDING ICU PATIENTS
1
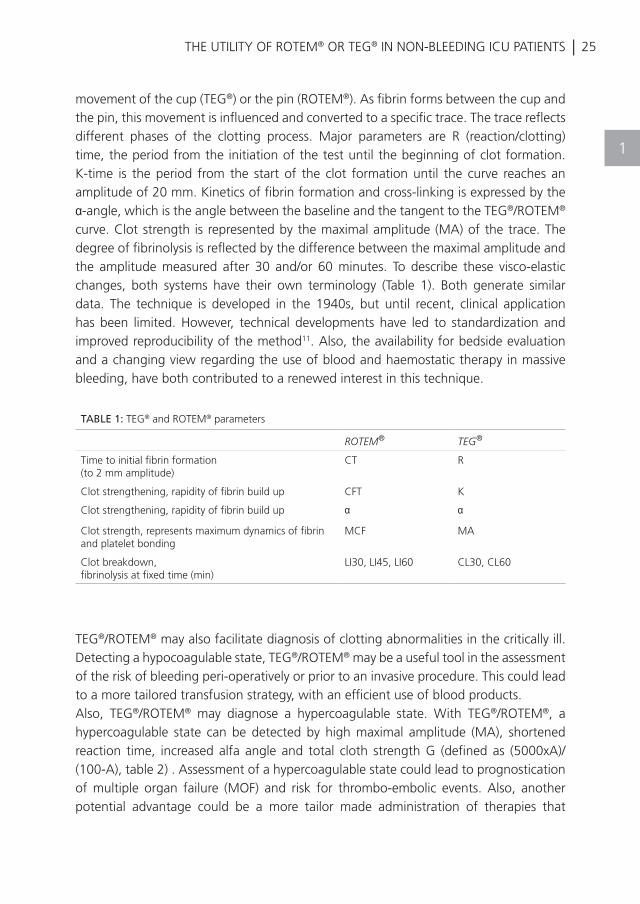
movement of the cup (TEG®) or the pin (ROTEM®). As fibrin forms between the cup and the pin, this movement is influenced and converted to a specific trace. The trace reflects different phases of the clotting process. Major parameters are R (reaction/clotting) time, the period from the initiation of the test until the beginning of clot formation. K-time is the period from the start of the clot formation until the curve reaches an amplitude of 20 mm. Kinetics of fibrin formation and cross-linking is expressed by the α-angle, which is the angle between the baseline and the tangent to the TEG®/ROTEM® curve. Clot strength is represented by the maximal amplitude (MA) of the trace. The degree of fibrinolysis is reflected by the difference between the maximal amplitude and the amplitude measured after 30 and/or 60 minutes. To describe these visco-elastic changes, both systems have their own terminology (Table 1). Both generate similar data. The technique is developed in the 1940s, but until recent, clinical application has been limited. However, technical developments have led to standardization and improved reproducibility of the method11. Also, the availability for bedside evaluation and a changing view regarding the use of blood and haemostatic therapy in massive bleeding, have both contributed to a renewed interest in this technique.
TEG®/ROTEM® may also facilitate diagnosis of clotting abnormalities in the critically ill. Detecting a hypocoagulable state, TEG®/ROTEM® may be a useful tool in the assessment of the risk of bleeding peri-operatively or prior to an invasive procedure. This could lead to a more tailored transfusion strategy, with an efficient use of blood products.Also, TEG®/ROTEM® may diagnose a hypercoagulable state. With TEG®/ROTEM®, a hypercoagulable state can be detected by high maximal amplitude (MA), shortened reaction time, increased alfa angle and total cloth strength G (defined as (5000xA)/(100-A), table 2) . Assessment of a hypercoagulable state could lead to prognostication of multiple organ failure (MOF) and risk for thrombo-embolic events. Also, another potential advantage could be a more tailor made administration of therapies that
TABLE 1: TEG® and ROTEM® parameters
ROTEM® TEG®
Time to initial fibrin formation (to 2 mm amplitude)
CT R
Clot strengthening, rapidity of fibrin build up CFT K
Clot strengthening, rapidity of fibrin build up α α
Clot strength, represents maximum dynamics of fibrin and platelet bonding
MCF MA
Clot breakdown, fibrinolysis at fixed time (min)
LI30, LI45, LI60 CL30, CL60
CHAPTER 126 |
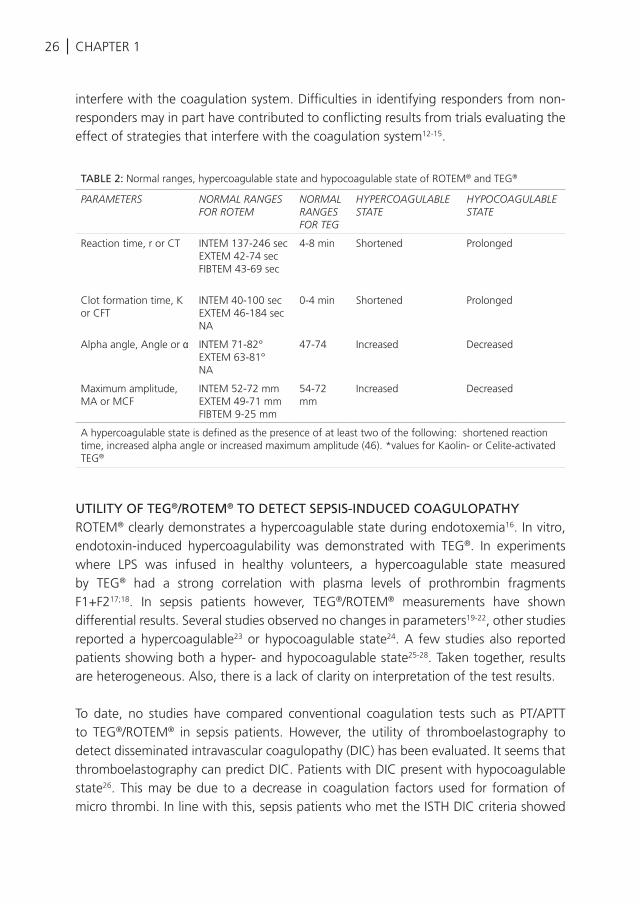
interfere with the coagulation system. Difficulties in identifying responders from non-responders may in part have contributed to conflicting results from trials evaluating the effect of strategies that interfere with the coagulation system12-15.
UTILITY OF TEG®/ROTEM® TO DETECT SEPSIS-INDUCED COAGULOPATHYROTEM® clearly demonstrates a hypercoagulable state during endotoxemia16. In vitro, endotoxin-induced hypercoagulability was demonstrated with TEG®. In experiments where LPS was infused in healthy volunteers, a hypercoagulable state measured by TEG® had a strong correlation with plasma levels of prothrombin fragments F1+F217;18. In sepsis patients however, TEG®/ROTEM® measurements have shown differential results. Several studies observed no changes in parameters19-22, other studies reported a hypercoagulable23 or hypocoagulable state24. A few studies also reported patients showing both a hyper- and hypocoagulable state25-28. Taken together, results are heterogeneous. Also, there is a lack of clarity on interpretation of the test results.
To date, no studies have compared conventional coagulation tests such as PT/APTT to TEG®/ROTEM® in sepsis patients. However, the utility of thromboelastography to detect disseminated intravascular coagulopathy (DIC) has been evaluated. It seems that thromboelastography can predict DIC. Patients with DIC present with hypocoagulable state26. This may be due to a decrease in coagulation factors used for formation of micro thrombi. In line with this, sepsis patients who met the ISTH DIC criteria showed
TABLE 2: Normal ranges, hypercoagulable state and hypocoagulable state of ROTEM® and TEG®
PARAMETERS NORMAL RANGES FOR ROTEM
NORMAL RANGES FOR TEG
HYPERCOAGULABLE STATE
HYPOCOAGULABLE STATE
Reaction time, r or CT INTEM 137-246 secEXTEM 42-74 secFIBTEM 43-69 sec
4-8 min Shortened Prolonged
Clot formation time, K or CFT
INTEM 40-100 secEXTEM 46-184 secNA
0-4 min Shortened Prolonged
Alpha angle, Angle or α INTEM 71-82°EXTEM 63-81°NA
47-74 Increased Decreased
Maximum amplitude, MA or MCF
INTEM 52-72 mmEXTEM 49-71 mmFIBTEM 9-25 mm
54-72 mm
Increased Decreased
A hypercoagulable state is defined as the presence of at least two of the following: shortened reaction time, increased alpha angle or increased maximum amplitude (46). *values for Kaolin- or Celite-activated TEG®
| 27THE UTILITY OF ROTEM® OR TEG® IN NON-BLEEDING ICU PATIENTS
1
a hypocoagulable state when compared to healthy controls, while patients without DIC showed a non-significant trend towards hypercoagulation25. Also, patients with an underlying disease known to be associated with DIC and ISTH DIC scores >5 had significantly prolonged reaction and K times and decreased alpha-angle and MA (signs of a hypocoagulable state) compared to patients with low ISTH DIC scores. The authors developed a score, defined as the total number of parameters (R, K, MA, and alfa) that were deranged in the direction of a hypocoagulable state. With this score, the discriminatory value of thromboelastometry to detect DIC improved29. Impaired fibrinolysis in sepsis may contribute to a hypercoagulable state. Inhibition of the fibrinolytic system was found to discriminate sepsis from postoperative controls19;28;30.
In terms of prognostication, a hypercoagulable state was not found to be a predictor of outcome. In contrast, the finding of a hypocoagulable state was repeatedly shown to be associated with a poor outcome. The TEG® MA value is an independent predictor for 28-day mortality on admission27. Hospital mortality was predicted by a hypocoagulable state due to a deficit in thrombin generation (30). A hypocoagulable state measured with TEG® is found to be associated with a pro-inflammatory response19;24. Also, the degree of a hypocoagulable state is associated with severity of organ failure in sepsis19;22.
Taken together, results are heterogeneous. Timing of measurements may be relevant to these observations, as a hypocoagulable state may be more outspoken in the acute phase of sepsis and return to normal values towards discharge of ICU, or even to enhanced clot formation.
USE OF TEG®/ROTEM® TO GUIDE ANTICOAGULANT TREATMENT IN SEPSIS PATIENTSIn sepsis, activation of coagulation is a crucial step in the pathophysiological cascade of sepsis, with concomitant low levels of circulating natural anticoagulants8;9. From thisperspective, various treatment modalities that interfere with the coagulation system have been studied (e.g. rhAPC, AT and heparin)12-15. However, efficacy has been questioned. It can be hypothesized that TEG®/ROTEM® may help to identify patients likely to respond to therapies that target coagulopathy. To date, there are no studies which have addressed this question. Only a few small patient series evaluated TEG®/ROTEM® measurement during anticoagulant medication. ROTEM® parameters did not change during anticoagulant medication. Also, treatment with antithrombin did not induce changes in the ROTEM® measurements23.
USE OF TEG®/ROTEM® IN PATIENTS WITH INDUCED HYPOTHERMIAInduced hypothermia is a common therapy in survivors of a cardiac arrest31-33. However, hypothermia is associated with coagulopathy, prolongation of aPTT and PT33;34 and
CHAPTER 128 |
an increased risk of bleeding35. A test that reliably detects hypothermia induced coagulopathy would be helpful in identifying patients who have an increased bleeding risk while being cooled and sedated. Unfortunately, little is known about the value of TEG®/ROTEM® in these patients. Spiel et al observed that ROTEM® measurements showed a prolonged CT at 1 hour after infusion of 4°C cold crystalloid solution. All other parameters remained within reference values. An important limitation of this study is that all measurements were performed at 37°C33. TEG® parameters were evaluated also in patients after cardiac arrest. On the contrary, the TEG® was performed at isothermal conditions and a hypocoagulable state was detected by TEG®36.
USE OF TEG®/ROTEM® IN PATIENTS WITH BRAIN INJURY
After severe traumatic brain injury and neurosurgery, up to 45% of patients develop acoagulopathy37-39. Given the serious consequences of intracranial bleeding, instant assessment of coagulation status is desirable. Two small trials have studied the value ofTEG® to detect coagulopathy in these patients, which mostly found test results within reference values. However, the functional response of platelets as measured in a platelet mapping™ (TEG®-PM) assay, was significantly lower in brain injury patients than in control groups, with a particular low response in those patients who developed bleeding complications40. Furthermore, a hypocoagulable state on admission to the ICU is associated with worse outcome in patients with traumatic brain injury and intracranial bleeding41.
UTILITY OF TEG® TO DETECT A HYPERCOAGULABLE STATE AND PROGNOSTICATE ORGAN FAILURE IN TRAUMA PATIENTS
Patients who survive the acute phase of trauma are prone to develop a hypercoagulablestate with increased risk for thrombo-embolic events and DIC1. Conventional coagulation tests are not able to detect such a hypercoagulable state. Also, there is debate as to whether the syndrome DIC is applicable to coagulation abnormalities in trauma. With TEG®/ROTEM®, a hypercoagulable state can be detected by high maximal amplitude (MA) and shortened reaction time (Table 1). Several reports demonstrate a hypercoagulable state in severely injured patients with TEG®/ROTEM®. In trauma and burn patients admitted to the ICU, TEG® was found to be more sensitive in detecting a hypercoagulable state than conventional clotting assays42;43. A high MA was found to be an independent contributor of mortality in multiple logistic regression analysis42. A hypercoagulable state measured by TEG® predicted the development of thrombo-embolic events in trauma patients44 although not all studies have confirmed this
| 29
1
THE UTILITY OF ROTEM® OR TEG® IN NON-BLEEDING ICU PATIENTS
finding45. It should be noted that the finding of a hypercoagulable state is not specific for DVT. A study on the use of ROTEM® to prognosticate the occurrence of multiple organ failure in a cohort of trauma patients is currently underway.
CONSIDERATIONS
In several non-bleeding critically ill patient populations, evidence supporting the use of TEG®/ROTEM® to diagnose a hypocoagulable or hypercagulable state is limited at this stage, mostly because of heterogeneity of the included studies in design, use of control groups and chosen endpoints. Heterogeneity of results can also be caused by differences in disease severity, as changes were more outspoken during severe illness. Timing of TEG®/ROTEM® measurements may greatly influence results, as coagulopathy is a dynamic process, eg. evolving from subtle activation of coagulation to overt DIC in sepsis and from a hypocoagulable to a hypercoagulable state in trauma. Performing sequential measurements will probably provide better insight in the development of coagulation derangements. Another important issue is that no uniform definitions exist of a hypocoagulable and a hypercoagulable state. Reference values for non-bleeding patients with disorders of coagulation are not widely assessed and cut off values are often not defined in studies. To compare patient categories and possibly investigate therapeutic interventions in the coagulation system, validated universal reference values and definitions are essential. A study on TEG® reference intervals has been recently completed (NCT01357928). Presumably, as patients groups are relatively small, evaluation of larger patient groups may yield more clear results.
CONCLUSION
TEG®/ROTEM® can detect coagulopathy in the critically ill. Whether these tests are useful as diagnostic tools remains to be investigated when reference values and clear definitions have been established. TEG®/ROTEM® may be useful for prognostication of outcome. A hypocoagulable status seems to be an independent predictor for organ failure and mortality in sepsis, also after correction for disease severity. In patients with brain injury, a hypocoagulable state on admission to the ICU is also associated with worse outcome. In patients who survive the acute phase of trauma, a hypercoagulable state as detected by TEG®/ROTEM® is a common finding. These tests could be helpful in identifying those patients at risk for thrombo-embolic complications, as a hypercoagulable state predicted the development of thrombo-embolic events in the majority of studies. Further research on this topic is forthcoming.
CHAPTER 130 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
Walsh TS, Stanworth SJ, Prescott RJ, Lee
RJ, Watson DM, Wyncoll D. Prevalence,
management, and outcomes of critically ill
patients with prothrombin time prolongation
in United Kingdom intensive care units. Crit
Care Med 2010 Oct;38(10):1939-46.
Crowther MA, Cook DJ, Meade MO, Griffith
LE, Guyatt GH, Arnold DM, Rabbat CG,
Geerts WH, Warkentin TE. Thrombocytopenia
in medical-surgical critically ill patients:
prevalence, incidence, and risk factors. J Crit
Care 2005 Dec;20(4):348-53.
Strauss R, Wehler M, Mehler K, Kreutzer D,
Koebnick C, Hahn EG. Thrombocytopenia
in patients in the medical intensive care
unit: bleeding prevalence, transfusion
requirements, and outcome. Crit Care Med
2002 Aug;30(8):1765-71.
Vanderschueren S, De WA, Malbrain M,
Vankersschaever D, Frans E, Wilmer A,
Bobbaers H. Thrombocytopenia and prognosis
in intensive care. Crit Care Med 2000
Jun;28(6):1871-6.
Hui P, Cook DJ, Lim W, Fraser GA, Arnold
DM. The frequency and clinical significance
of thrombocytopenia complicating critical
illness: a systematic review. Chest 2011
Feb;139(2):271-8.
Shackford SR, Davis JW, Hollingsworth-
Fridlund P, Brewer NS, Hoyt DB, Mackersie
RC. Venous thromboembolism in patients
with major trauma. Am J Surg 1990
Apr;159(4):365-9.
Singh B, Hanson AC, Alhurani R, Wang S,
Herasevich V, Cartin-Ceba R, Kor DJ, Gangat
N, Li G. Trends in the incidence and outcomes
of disseminated intravascular coagulation in
critically ill patients (2004-2010): a population-
based study. Chest 2013 May;143(5):
1235-42.
Dempfle CE. Coagulopathy of sepsis. Thromb
Haemost 2004 Feb;91(2):213-24.
Levi M, Ten CH. Disseminated intravascular
coagulation. N Engl J Med 1999
Aug 19;341(8):586-92.
Levi M, Meijers JC. DIC: which
laboratory tests are most useful.
Blood Rev 2011 Jan;25(1):33-7.
Reikvam H, Steien E, Hauge B, Liseth K, Hagen
KG, Storkson R, Hervig T. Thrombelastography.
Transfus Apher Sci 2009 Apr;40(2):119-23.
Bernard GR, Vincent JL, Laterre PF, LaRosa SP,
Dhainaut JF, Lopez-Rodriguez A, Steingrub
JS, Garber GE, Helterbrand JD, Ely EW, et al.
Efficacy and safety of recombinant human
activated protein C for severe sepsis. N Engl J
Med 2001 Mar 8;344(10):699-709.
Afshari A, Wetterslev J, Brok J, Moller A.
Antithrombin III in critically ill patients:
systematic review with meta-analysis and
trial sequential analysis. BMJ 2007 Dec
15;335(7632):1248-51.
Abraham E, Reinhart K, Opal S, Demeyer I, Doig
C, Rodriguez AL, Beale R, Svoboda P, Laterre PF,
Simon S, et al. Efficacy and safety of tifacogin
(recombinant tissue factor pathway inhibitor)
in severe sepsis: a randomized controlled trial.
JAMA 2003 Jul 9;290(2):238-47.
Jaimes F, De La Rosa G, Morales C, Fortich F,
Arango C, Aguirre D, Munoz A. Unfractioned
heparin for treatment of sepsis: A randomized
clinical trial (The HETRASE Study). Crit Care
Med 2009 Apr;37(4):1185-96.
Schochl H, Solomon C, Schulz A, Voelckel
W, Hanke A, Van GM, Redl H, Bahrami
S. Thromboelastometry (TEM) findings in
disseminated intravascular coagulation in a
pig model of endotoxinemia. Mol Med 2011
Mar;17(3-4):266-72.
Spiel AO, Mayr FB, Firbas C, Quehenberger
P, Jilma B. Validation of rotation
thrombelastography in a model of systemic
activation of fibrinolysis and coagulation
in humans. J Thromb Haemost 2006
Feb;4(2):411-6.
Zacharowski K, Sucker C, Zacharowski P,
Hartmann M. Thrombelastography for the
monitoring of lipopolysaccharide induced
| 31
REFERENCES
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
activation of coagulation. Thromb Haemost
2006 Mar;95(3):557-61.
Brenner T, Schmidt K, Delang M, Mehrabi A,
Bruckner T, Lichtenstern C, Martin E, Weigand
MA, Hofer S. Viscoelastic and aggregometric
point-of-care testing in patients with septic
shock - cross-links between inflammation and
haemostasis. Acta Anaesthesiol Scand 2012
Nov;56(10):1277-90.
Durila M, Kalincik T, Jurcenko S, Pelichovska
M, Hadacova I, Cvachovec K. Arteriovenous
differences of hematological and coagulation
parameters in patients with sepsis. Blood
Coagul Fibrinolysis 2010 Dec;21(8):770-4.
Altmann DR, Korte W, Maeder MT, Fehr T,
Haager P, Rickli H, Kleger GR, Rodriguez
R, Ammann P. Elevated cardiac troponin I
in sepsis and septic shock: no evidence for
thrombus associated myocardial necrosis.
PLoS One 2010;5(2):e9017.
Daudel F, Kessler U, Folly H, Lienert JS, Takala
J, Jakob SM. Thromboelastometry for the
assessment of coagulation abnormalities in
early and established adult sepsis: a prospective
cohort study. Crit Care 2009;13(2):R42.
Gonano C, Sitzwohl C, Meitner E, Weinstabl
C, Kettner SC. Four-day antithrombin therapy
does not seem to attenuate hypercoagulability
in patients suffering from sepsis. Crit Care
2006;10(6):R160.
Viljoen M, Roux LJ, Pretorius JP, Coetzee
IH, Viljoen E. Hemostatic competency and
elastase-alpha 1-proteinase inhibitor levels in
surgery, trauma, and sepsis. J Trauma 1995
Aug;39(2):381-5.
Sivula M, Pettila V, Niemi TT, Varpula M,
Kuitunen AH. Thromboelastometry in
patients with severe sepsis and disseminated
intravascular coagulation. Blood Coagul
Fibrinolysis 2009 Sep;20(6):419-26.
Collins PW, Macchiavello LI, Lewis SJ,
Macartney NJ, Saayman AG, Luddington
R, Baglin T, Findlay GP. Global tests of
haemostasis in critically ill patients with severe
sepsis syndrome compared to controls. Br J
Haematol 2006 Oct;135(2):220-7.
Ostrowski SR, Windelov NA, Ibsen M, Haase
N, Perner A, Johansson PI. Consecutive
thrombelastography clot strength profiles in
patients with severe sepsis and their association
with 28-day mortality: a prospective study. J
Crit Care 2013 Jun;28(3):317-11.
Adamzik M, Langemeier T, Frey UH, Gorlinger
K, Saner F, Eggebrecht H, Peters J, Hartmann
M. Comparison of thrombelastometry with
simplified acute physiology score II and
sequential organ failure assessment scores
for the prediction of 30-day survival: a cohort
study. Shock 2011 Apr;35(4):339-42.
Sharma P, Saxena R. A novel
thromboelastographic score to identify
overt disseminated intravascular coagulation
resulting in a hypocoagulable state. Am J Clin
Pathol 2010 Jul;134(1):97-102.
Massion PB, Peters P, Ledoux D, Zimermann
V, Canivet JL, Massion PP, Damas P, Gothot A.
Persistent hypocoagulability in patients with
septic shock predicts greater hospital mortality:
impact of impaired thrombin generation.
Intensive Care Med 2012 Aug;38(8):1326-35.
Mild therapeutic hypothermia to improve the
neurologic outcome after cardiac arrest. N
Engl J Med 2002 Feb 21;346(8):549-56.
Bernard SA, Gray TW, Buist MD, Jones BM,
Silvester W, Gutteridge G, Smith K. Treatment
of comatose survivors of out-of-hospital
cardiac arrest with induced hypothermia. N
Engl J Med 2002 Feb 21;346(8):557-63.
Spiel AO, Kliegel A, Janata A, Uray T, Mayr
FB, Laggner AN, Jilma B, Sterz F. Hemostasis
in cardiac arrest patients treated with
mild hypothermia initiated by cold fluids.
Resuscitation 2009 Jul;80(7):762-5.
Reed RL, Bracey AW, Jr., Hudson JD, Miller
TA, Fischer RP. Hypothermia and blood
coagulation: dissociation between enzyme
activity and clotting factor levels. Circ Shock
1990 Oct;32(2):141-52.
THE UTILITY OF ROTEM® OR TEG® IN NON-BLEEDING ICU PATIENTS
1
CHAPTER 132 |
REFERENCES
35
36
37
38
39
40
41
42
43
44
45
Nielsen N, Sunde K, Hovdenes J, Riker RR,
Rubertsson S, Stammet P, Nilsson F, Friberg H.
Adverse events and their relation to mortality
in out-of-hospital cardiac arrest patients
treated with therapeutic hypothermia. Crit
Care Med 2011 Jan;39(1):57-64.
Cundrle I, Jr., Sramek V, Pavlik M, Suk P,
Radouskova I, Zvonicek V. Temperature
corrected thromboelastography in
hypothermia: is it necessary? Eur J Anaesthesiol
2013 Feb;30(2):85-9.
Sun Y, Wang J, Wu X, Xi C, Gai Y, Liu H, Yuan
Q, Wang E, Gao L, Hu J, et al. Validating the
incidence of coagulopathy and disseminated
intravascular coagulation in patients with
traumatic brain injury--analysis of 242 cases.
Br J Neurosurg 2011 Jun;25(3):363-8.
Lustenberger T, Talving P, Kobayashi L, Inaba K,
Lam L, Plurad D, Demetriades D. Time course
of coagulopathy in isolated severe traumatic
brain injury. Injury 2010 Sep;41(9):924-8.
Stein SC, Smith DH. Coagulopathy in traumatic
brain injury. Neurocrit Care 2004;1(4):479-88.
Nekludov M, Bellander BM, Blomback
M, Wallen HN. Platelet dysfunction in
patients with severe traumatic brain injury. J
Neurotrauma 2007 Nov;24(11):1699-706.
Windelov NA, Welling KL, Ostrowski
SR, Johansson PI. The prognostic value
of thrombelastography in identifying
neurosurgical patients with worse prognosis.
Blood Coagul Fibrinolysis 2011 Jul;22(5):416-
9.
Park MS, Salinas J, Wade CE, Wang J, Martini
W, Pusateri AE, Merrill GA, Chung K, Wolf
SE, Holcomb JB. Combining early coagulation
and inflammatory status improves prediction
of mortality in burned and nonburned
trauma patients. J Trauma 2008 Feb;64(2
Suppl):S188-S194.
Gonzalez E, Kashuk JL, Moore EE, Silliman
CC. Differentiation of enzymatic from
platelet hypercoagulability using the novel
thrombelastography parameter delta (delta). J
Surg Res 2010 Sep;163(1):96-101.
Schreiber MA, Differding J, Thorborg P,
Mayberry JC, Mullins RJ. Hypercoagulability is
most prevalent early after injury and in female
patients. J Trauma 2005 Mar;58(3):475-80.
Park MS, Martini WZ, Dubick MA, Salinas
J, Butenas S, Kheirabadi BS, Pusateri
AE, Vos JA, Guymon CH, Wolf SE, et al.
Thromboelastography as a better indicator
of hypercoagulable state after injury than
prothrombin time or activated partial
thromboplastin time. J Trauma 2009
Aug;67(2):266-75.

| 33THE UTILITY OF ROTEM® OR TEG® IN NON-BLEEDING ICU PATIENTS
1
M.C.A. Müller, K. Balvers, J.M. Binnekade, N. Curry, S. Stanworth, C. Gaarder, K.M. Kolstadbraaten, C. Rourke, K. Brohi, J.C. Goslings, N.P. Juffermans
Critical Care 2014
THROMBOELASTOMETRY AND ORGAN FAILURE IN TRAUMA PATIENTS: A PROSPECTIVE COHORT STUDY
2
36 | CHAPTER 2
ABSTRACT
Introduction: Data on the incidence of a hypercoagulable state in trauma, as measured by thromboelastometry (ROTEM®), is limited and the prognostic value of hypercoagulability after trauma on outcome is unclear. We aimed to determine the incidence of hypercoagulability after trauma, and to assess whether early hypercoagulability has prognostic value on the occurrence of multiple organ failure (MOF) and mortality.
Methods: This was a prospective observational cohort study in trauma patients who met the highest trauma level team activation. Hypercoagulability was defined as a G value of ≥11.7 dynes/cm2 and hypocoagulability as a G value of <5.0 dynes/cm2. ROTEM® was performed on admission and 24 hours later.
Results: A total of 1,010 patients were enrolled and 948 patients were analysed. Median age was 38 (interquartile range (IQR) 26 to 53), 77% were male and median injury severity score was 13 (IQR 8 to 25). On admission, 7% of the patients were hypercoagulable and 8% were hypocoagulable. Altogether, 10% of patients showed hypercoagulability within the first 24 hours of trauma. Hypocoagulability, but not hypercoagulability, was associated with higher sequential organ failure assessment scores, indicating more severe MOF. Mortality in patients with hypercoagulability was 0%, compared to 7% in normocoagulable and 24% in hypocoagulable patients (P <0.001). EXTEM CT, alpha and G were predictors for occurrence of MOF and mortality.
Conclusion: The incidence of a hypercoagulable state after trauma is 10% up to 24 hours after admission, which is broadly comparable to the rate of hypocoagulability. Further work in larger studies should define the clinical consequences of identifying hypercoagulability and a possible role for very early, targeted use of anticoagulants.
| 37PREDICTIVE VALUE OF HYPERCOAGULOPATHY FOR MOF
2
INTRODUCTION
Major trauma is among the most common causes of death worldwide. Whereas uncontrolled bleeding accounts for 50 to 80% of mortality early following trauma1,2, multiple organ failure (MOF) is the most important cause of late mortality after trauma1,3. Traumatic injury induces a hypocoagulable state, as a result of acute traumatic coagulopathy (ATC) accompanied by loss, consumption and dilution of coagulation factors and fibrinolysis. Hypothermia, shock and acidosis further amplify the derangement of the coagulation system4. In addition to reduced haemostatic potential, trauma can also induce a hypercoagulable state5-7. Animal experiments have shown that hypercoagulability can arise within hours of the injury8, a phenomenon confirmed in humans5,9. However, uniform definitions of hypercoagulability are lacking and effects of this hypercoagulable state after trauma are not fully elucidated, with studies showing conflicting results. An association with adverse events such as an increased risk of venous thromboembolism has been reported7,10,11. However, early hypercoagulability has also been associated with decreased early mortality, which may suggest that hypercoagulability is a functional response in order to reduce blood loss9.In sepsis, it has been demonstrated that hypercoagulability, characterized by the formation of microthrombi with concurrent protein C deficiency and impaired fibrinolysis, contributes to MOF and adverse outcome12,13. Although sepsis and trauma are different entities, the accompanying coagulopathies show similarities and persistent protein C deficiency after trauma is also associated with occurrence of MOF14,15. Shock and hypoperfusion can induce activation of the endothelium and if the patient survives the initial bleeding episode, this can result in a procoagulant state. It is conceivable that therapy of ATC may add to this endogenous response, possibly resulting in an overshoot in coagulation over time, with subsequent enhancement of hypercoagulability and MOF.Diagnosing hypercoagulability is complex. Thrombin generation tests, or assessment of plasma levels of natural anticoagulants, as protein C, are not readily available for clinical use and not validated to detect hypercoagulability. Thromboelastometry (ROTEM®) provides real-time information on all aspects of the coagulation system, including the presence of hypercoagulability16,17. The use of thromboelastometry to diagnose hypocoagulability in trauma has frequently been explored in recent years18-21. However, reports on the use of ROTEM® to detect a hypercoagulable state are scarce.We aimed to study the incidence of early hypercoagulability in multiple trauma patients and to establish whether hypercoagulability is associated with the occurrence of MOF and mortality. In addition, as transfusion strategies have shifted, we assessed whether transfusion strategy influenced the occurrence of hypercoagulability.
38 | CHAPTER 2
METHODS
Study design and patientsA prospective observational cohort study was conducted in four level-1 trauma centres in London, Oxford, Oslo and Amsterdam. This study is part of the Activation of Coagulation and Inflammation in Trauma (ACIT) study, an ongoing prospective observational multicentre study in trauma patients. The ethics committees of the Academic Medical Center in Amsterdam, the Netherlands; of the Oslo University Hospital, Oslo, Norway; of the Royal London Hospital, London and of the John Radcliffe Hospital, Oxford, United Kingdom, all reviewed and approved the study. Written informed consent was obtained from all participating patients. All procedures have been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Between January 2008 and March 2013, all adult trauma patients (18 years and older) who met the local criteria for highest trauma team level activation were eligible for enrolment in the study. Patients were excluded if arrival at the emergency department (ED) was >2 hours following injury; >2,000 ml of intravenous fluid was administered before ED admission; they were transferred from another hospital or if they had burns covering >5% of total body surface area. Patients were retrospectively excluded if they declined to give consent to use data, were receiving anticoagulation (not including aspirin), or had moderate or severe liver disease or a known bleeding diathesis.
Data collectionData were prospectively collected on patient demographics, time from injury to arrival at the ED, mechanism of injury (blunt or penetrating), presence of traumatic brain injury, vital signs on arrival and 24 hours after injury and amount of fluid and blood products within the first 24 hours of injury. Trauma severity was assessed using the injury severity score (ISS)22. Furthermore, sequential organ failure assessment (SOFA) scores, with Glasgow coma scale to assess neurologic dysfunction, and mortality rates after 28 days were obtained.
ThromboelastometryThromboelastometric variables were measured with ROTEM (Tem International, Munich, Germany). Citrated blood samples were drawn within 1 hour after arrival in the ED and a second sample was collected 24 hours (±2 hours) after admission. All samples were processed within 1 hour. For EXTEM, 20 μL of 0.2 mol/L CaCl2 (star-tem™) and 20 μL of human recombinant tissue factor (r EXTEM™) were added to a test vial. Subsequently 300 μL of the citrated blood sample was added. For INTEM, 20 μL of 0.2 mol/L CaCl2 (star-tem™) and 20 μL of partial thromboplastin phospholipid
| 39PREDICTIVE VALUE OF HYPERCOAGULOPATHY FOR MOF
2
made of rabbit brain and ellagic acid (in-tem™) were added as activator to 300 μL of blood in the test cuvette. The electronic pipette program guided all test steps. For both assays, clotting time (CT), clot formation time (CFT), maximum clot firmness (MCF) and alpha angle were recorded. Total clot strength was assessed by G as calculated according to the formula: (5,000 × MCF)/100 - MCF and expressed as dynes/cm216. G has a curvilinear relation with MCF and reflects the contribution of enzymatic and platelet components to the hemostasis, hereby better reflecting haemostatic potential than individual thromboelastometry parameters7,23. G has been shown to be valuable in diagnosing hypo- and hypercoagulability7,16,23. Hypercoagulability was defined as a G value of ≥11.7 dynes/cm2 and hypocoagulability as a G value of <5.0 dynes/cm2 (values provided by manufacturer).
Outcome variablesPrimary outcome was the occurrence of MOF, assessed by the SOFA score, which reliably assesses organ failure in trauma patients24. The score awards 0 (normal) to 4 (most abnormal) points for each organ system. MOF was defined by a score of 3 points or more3. Secondary outcome was 28-day mortality. In addition, effect of transfusion strategy (ratio of red blood cells (RBC) to fresh frozen plasma (FFP)) on ROTEM® profile and occurrence of hypercoagulability was determined.
StatisticsContinuous normally distributed variables are expressed by their mean and standard deviation. Not normally distributed variables are expressed as medians and their interquartile (IQR) ranges and categorical variables are expressed as n (%). ISS was treated as a continuous variable. Groups are compared by using Student’s t test or Mann-Whitney U test in case of not normally distributed data.For comparison of categorical variables, the chi-square test or Fisher’s exact tests are used. The primary analysis focused on modelling the hypothesized relation between ROTEM-detected hypercoagulability, MOF and mortality in trauma patients. First, univariate logistic regression analysis was used to select independent factors achieving a P value ≤0.10, in addition to factors that were deemed clinically important (age, time to ED, presence of traumatic brain injury, injury mechanism, ISS, base excess, systolic blood pressure) in relation to the outcome variables. Subsequently, selected ROTEM® factors were entered in a multivariate logistic regression model. Patients who died on admission were not included in the analyses to assess the value of thromboelastometry to predict MOF, while patients who died later were included when a SOFA score was available. All deceased patients were included in the analyses to assess the value of ROTEM® to predict mortality.

40 | CHAPTER 2
To compare the effect of transfusion strategies, transfused patients were divided based on RBC:FFP ratio. Statistical significance was considered to be at P= 0.05. Analyses were performed using R (version 2.3; R Foundation for Statistical Computing, Vienna, Austria). Graphs were created with Prism 5.0 (GraphPad Software, San Diego, CA, USA).
RESULTS
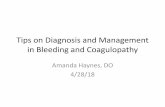
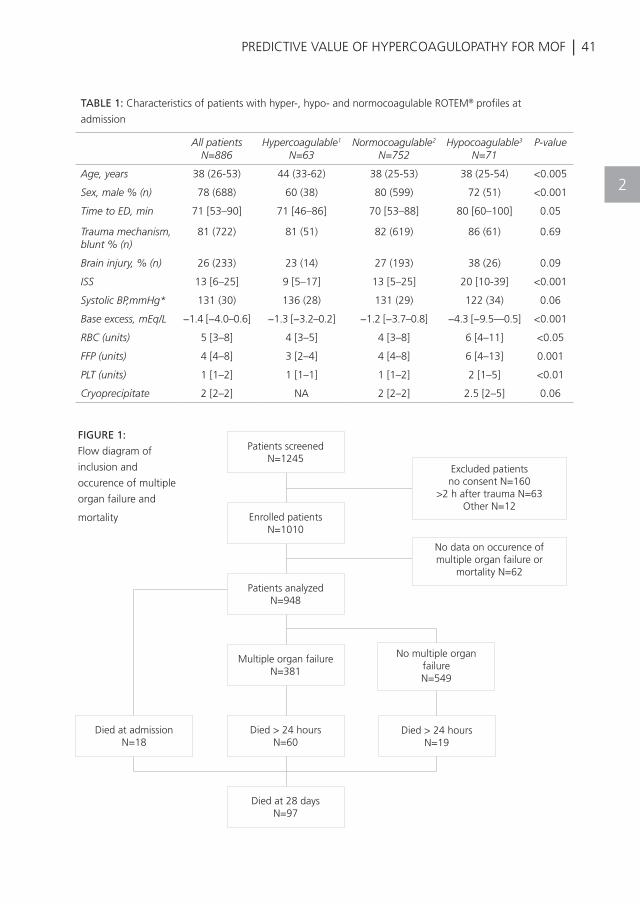
During the study period, 1,245 patients were screened and 1,010 patients were enrolled in the study (Figure 1). For 62 of the patients, no data were available on occurrence of MOF or mortality, therefore, analyses were performed in the remaining 948 patients.Of these, 776 patients were admitted to the hospital (intensive care unit: n = 318 and ward: n = 458) and 76 were discharged home. Patient characteristics are listed in Table 1. The majority of included patients were males experiencing blunt injury. Median age was 38 years and median ISS was 13 (IQR 8 to 25). Eighteen patients died at admission, nine of them had traumatic brain injury (TBI). Of those who died between 24 hours and 28 days, mortality was 21% in TBI and 3.4% in non-TBI patients.
ROTEM® profiles and hypercoagulability on admissionBaseline thromboelastometry data were available for 886 patients upon ED admission. On admission, the G value was increased in 63 (7%) of the patients, while 71 (8%) were hypocoagulable and the remaining 85% had normal clot strength according to the G value. Patients showing hypercoagulability on admission were more often female (40% vs. 28%, P <0.001), had lower ISS scores (9 vs. 20, P <0.001) and higher base excess values (−1.3 mEq/L vs. −4.3 mEq/L, P <0.001) compared to hypocoagulable patients. Also, they received less RBC, FFP and platelet transfusions compared to hypocoagulable patients. In addition, hypocoagulable patients had longer time to arrival at ED and a trend toward a higher incidence of TBI (Table 1).
ROTEM® profiles and hypercoagulability 24 hours after admissionTwenty-four hours after admission, for 451 out of 776 admitted patients, ROTEM® profiles were available, 26 (6%) patients were hypercoagulable and 35 (8%) were hypocoagulable (Figure S1 in Additional file 1). In accordance with the hypercoagulable patients at ED admission, the hypercoagulable patients 24 hours after admission had lower ISS scores (14 vs. 25, P = 0.04), higher base excess values (−1.4 mEq/L vs. −6.2 mEq/L, P <0.001) and received less RBC transfusions compared to the hypocoagulable patients. Amount of FFP and platelets transfused did not differ between hyper-, normo- and hypocoagulable patients.Altogether, during the first 24 hours after trauma, 88 (10%) patients were hypercoagulable at some point. Patients showing hypercoagulable ROTEM® profiles had higher platelet counts and fibrinogen levels.
| 41PREDICTIVE VALUE OF HYPERCOAGULOPATHY FOR MOF
2
FIGURE 1:
Flow diagram of
inclusion and
occurence of multiple
organ failure and
mortality
TABLE 1: Characteristics of patients with hyper-, hypo- and normocoagulable ROTEM® profiles at
admission
All patientsN=886
Hypercoagulable1
N=63Normocoagulable2
N=752Hypocoagulable3
N=71P-value
Age, years 38 (26-53) 44 (33-62) 38 (25-53) 38 (25-54) <0.005
Sex, male % (n) 78 (688) 60 (38) 80 (599) 72 (51) <0.001
Time to ED, min 71 [53–90] 71 [46–86] 70 [53–88] 80 [60–100] 0.05
Trauma mechanism, blunt % (n)
81 (722) 81 (51) 82 (619) 86 (61) 0.69
Brain injury, % (n) 26 (233) 23 (14) 27 (193) 38 (26) 0.09
ISS 13 [6–25] 9 [5–17] 13 [5–25] 20 [10-39] <0.001
Systolic BP,mmHg* 131 (30) 136 (28) 131 (29) 122 (34) 0.06
Base excess, mEq/L −1.4 [−4.0–0.6] −1.3 [−3.2–0.2] −1.2 [−3.7–0.8] −4.3 [−9.5—0.5] <0.001
RBC (units) 5 [3–8] 4 [3–5] 4 [3–8] 6 [4–11] <0.05
FFP (units) 4 [4–8] 3 [2–4] 4 [4–8] 6 [4–13] 0.001
PLT (units) 1 [1–2] 1 [1–1] 1 [1–2] 2 [1–5] <0.01
Cryoprecipitate 2 [2–2] NA 2 [2–2] 2.5 [2–5] 0.06
Patients screenedN=1245
Enrolled patientsN=1010
Patients analyzedN=948
Multiple organ failureN=381
Died > 24 hoursN=60
Died at 28 daysN=97
Excluded patientsno consent N=160
>2 h after trauma N=63Other N=12
No data on occurence of multiple organ failure or
mortality N=62
No multiple organ failureN=549
Died > 24 hoursN=19
Died at admissionN=18
42 | CHAPTER 2
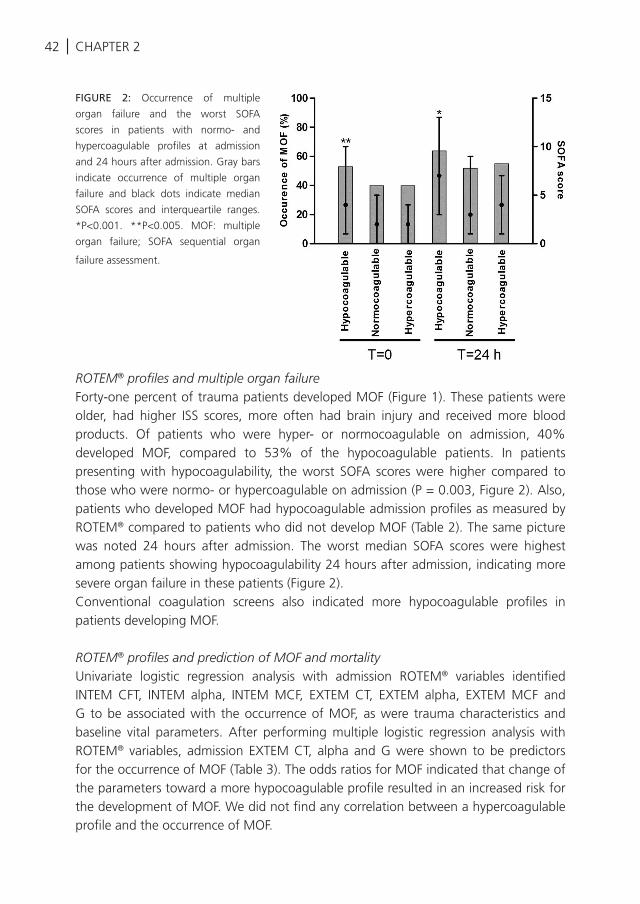
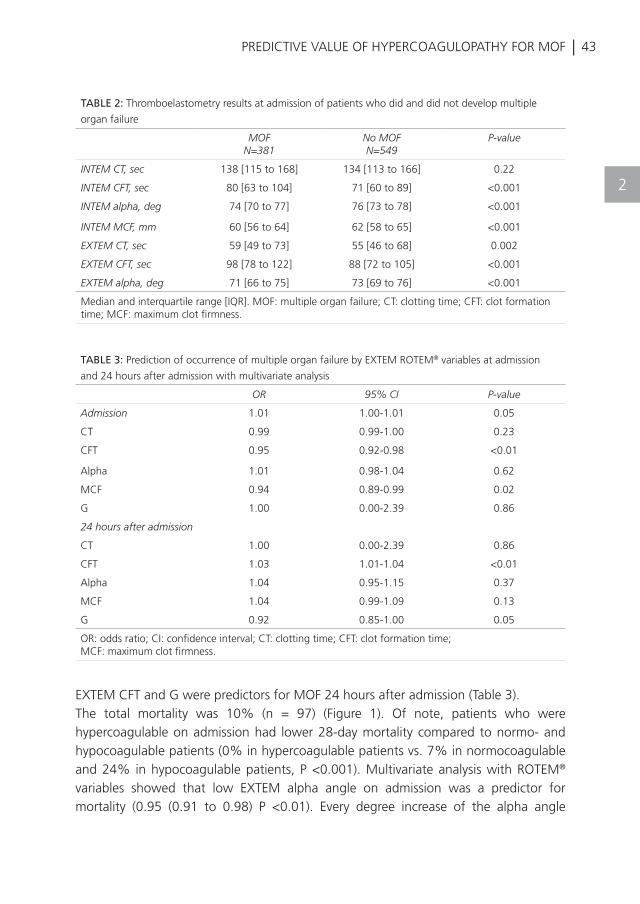
ROTEM® profiles and multiple organ failureForty-one percent of trauma patients developed MOF (Figure 1). These patients were older, had higher ISS scores, more often had brain injury and received more blood products. Of patients who were hyper- or normocoagulable on admission, 40% developed MOF, compared to 53% of the hypocoagulable patients. In patients presenting with hypocoagulability, the worst SOFA scores were higher compared to those who were normo- or hypercoagulable on admission (P = 0.003, Figure 2). Also, patients who developed MOF had hypocoagulable admission profiles as measured by ROTEM® compared to patients who did not develop MOF (Table 2). The same picture was noted 24 hours after admission. The worst median SOFA scores were highest among patients showing hypocoagulability 24 hours after admission, indicating more severe organ failure in these patients (Figure 2). Conventional coagulation screens also indicated more hypocoagulable profiles in patients developing MOF.
ROTEM® profiles and prediction of MOF and mortalityUnivariate logistic regression analysis with admission ROTEM® variables identified INTEM CFT, INTEM alpha, INTEM MCF, EXTEM CT, EXTEM alpha, EXTEM MCF and G to be associated with the occurrence of MOF, as were trauma characteristics and baseline vital parameters. After performing multiple logistic regression analysis with ROTEM® variables, admission EXTEM CT, alpha and G were shown to be predictors for the occurrence of MOF (Table 3). The odds ratios for MOF indicated that change of the parameters toward a more hypocoagulable profile resulted in an increased risk for the development of MOF. We did not find any correlation between a hypercoagulable profile and the occurrence of MOF.
FIGURE 2: Occurrence of multiple
organ failure and the worst SOFA
scores in patients with normo- and
hypercoagulable profiles at admission
and 24 hours after admission. Gray bars
indicate occurrence of multiple organ
failure and black dots indicate median
SOFA scores and interqueartile ranges.
*P<0.001. **P<0.005. MOF: multiple
organ failure; SOFA sequential organ
failure assessment.
| 43PREDICTIVE VALUE OF HYPERCOAGULOPATHY FOR MOF
2
EXTEM CFT and G were predictors for MOF 24 hours after admission (Table 3).The total mortality was 10% (n = 97) (Figure 1). Of note, patients who were hypercoagulable on admission had lower 28-day mortality compared to normo- and hypocoagulable patients (0% in hypercoagulable patients vs. 7% in normocoagulable and 24% in hypocoagulable patients, P <0.001). Multivariate analysis with ROTEM® variables showed that low EXTEM alpha angle on admission was a predictor for mortality (0.95 (0.91 to 0.98) P <0.01). Every degree increase of the alpha angle
TABLE 2: Thromboelastometry results at admission of patients who did and did not develop multiple
organ failure
MOFN=381
No MOFN=549
P-value
INTEM CT, sec 138 [115 to 168] 134 [113 to 166] 0.22
INTEM CFT, sec 80 [63 to 104] 71 [60 to 89] <0.001
INTEM alpha, deg 74 [70 to 77] 76 [73 to 78] <0.001
INTEM MCF, mm 60 [56 to 64] 62 [58 to 65] <0.001
EXTEM CT, sec 59 [49 to 73] 55 [46 to 68] 0.002
EXTEM CFT, sec 98 [78 to 122] 88 [72 to 105] <0.001
EXTEM alpha, deg 71 [66 to 75] 73 [69 to 76] <0.001
Median and interquartile range [IQR]. MOF: multiple organ failure; CT: clotting time; CFT: clot formation time; MCF: maximum clot firmness.
TABLE 3: Prediction of occurrence of multiple organ failure by EXTEM ROTEM® variables at admission
and 24 hours after admission with multivariate analysis
OR 95% CI P-value
Admission 1.01 1.00-1.01 0.05
CT 0.99 0.99-1.00 0.23
CFT 0.95 0.92-0.98 <0.01
Alpha 1.01 0.98-1.04 0.62
MCF 0.94 0.89-0.99 0.02
G 1.00 0.00-2.39 0.86
24 hours after admission
CT 1.00 0.00-2.39 0.86
CFT 1.03 1.01-1.04 <0.01
Alpha 1.04 0.95-1.15 0.37
MCF 1.04 0.99-1.09 0.13
G 0.92 0.85-1.00 0.05
OR: odds ratio; CI: confidence interval; CT: clotting time; CFT: clot formation time; MCF: maximum clot firmness.

44 | CHAPTER 2
results in a 0.95 reduction of mortality risk. In order to assess whether liberal use of FFP affected occurrence of hypercoagulability and subsequent MOF, we performed an additional sub analysis in patients transfused with RBC and FFP. Transfused patients were divided in one group with an RBC:FFP ratio of 1:1 (n = 35), one with a ratio of more than 1:1 (n = 115) and one with a ratio of less than 1:1 (n = 21). These three groups did not differ significantly with respect to baseline characteristics (data not shown) and platelet transfusions. ROTEM® EXTEM CT, CFT, MCF and alpha did not differ at baseline and after 24 hours, nor did G values (data not shown). After 24 hours, none of the patients transfused with a RBC:FFP ratio <1:1 showed hypercoagulability and of patients transfused with higher ratios of RBC:FFP, only two out of one hundred patients progressed from a normocoagulable to a hypercoagulable state.Occurrence of MOF was high in all groups, but did not differ between groups with different transfusion ratios (82% in patients with a ratio of 1:1 or higher, and 81% in patients with RBC:FFP <1:1 respectively, P = 0.99).
DISCUSSION
The current study shows that a hypercoagulable state as detected by thromboelastometry, occurred in 7% at admission and in 10% of patients within 24 hours after trauma. Characteristics associated with the presence of hypercoagulability included lower ISS, higher base excess values, female gender and shorter time to ED arrival. These rates were not that different to the detected incidence for hypocoagulability, which has been the focus of considerable research interest, as part of evolving concepts of ATC. In contrast to our hypothesis, hypercoagulability did not appear to predict the occurrence of MOF. Rather, severity of MOF after trauma was associated with a hypocoagulable state. Hypercoagulable patients at admission had lower mortality, consistent with lower ISS and more normal base excess values. High EXTEM CFT and low G values were predictive for the development of MOF and low EXTEM alpha was predictive for mortality.Hypercoagulability after trauma has been reported using a variety of thrombelastographic (TEG®) measurements5,7,9,25,26, however, whether TEG® and ROTEM® results are interchangeable is still under debate27,28. Reported incidences of hypercoagulability diagnosed by TEG® range from 11 to 80%5,7,9,10,26. This wide variation can be ascribed to use of different definitions of hypercoagulability, with studies using individual parameters of the thrombelastographic trace5,9,26, a combination of parameters6,10 or the use of G as a marker of whole clot strength7. Also injury severity and timing of measurements differed among these cohorts. Although our findings are in line with those previously reported in a smaller cohort of trauma patients26, our observed rates of hypercoagulability were lower compared to a recent evaluation of admission profiles
| 45PREDICTIVE VALUE OF HYPERCOAGULOPATHY FOR MOF
2
with TEG®, most likely due to the use of a more narrow definition of hypercoagulability in this study9. With respect to the observed rate of hypocoagulability, our numbers were in line with the previous mentioned TEG® study9, but lower than other reports from the ACIT cohort using ROTEM®29, because only patients needing more than four units of RBC were included.We hypothesized that occurrence of hypercoagulability was associated with MOF. However, we observed an opposite effect. Patients showing hypocoagulability within the first 24 hours of admission developed more severe organ failure and had an increased late mortality. This observation is in line with studies demonstrating that hypocoagulability is associated with adverse outcome after trauma and brain injury23,30,31. We showed that, in addition to individual parameters, G values on admission and 24 hours after admission are predictors for the occurrence of MOF. Of note, G is considered to better represent total clot strength than the individual thrombelastography parameters7,16,23. Previous studies on ROTEM® in trauma patients focused on diagnosing early coagulation abnormalities20,32, prediction of transfusion requirements21,33 and correction of hypocoagulability34,35. Our data indicate, contrary to our hypothesis, that hypocoagulability detected by ROTEM® also has an enhanced risk of adverse late outcome, which confirms previous observations in a smaller cohort 21.In the current study, patients with hypercoagulability had lower mortality and lower SOFA scores. A similar observation was recently reported in a smaller cohort of trauma patients9. Therefore, we hypothesize that early hypercoagulability after trauma is an evolutionary response to prevent exsanguination. Results do not point toward the hypothesis that early hypercoagulability after trauma resembles disseminated intravascular coagulation (DIC) with the formation of microthrombi, thereby contributing to organ failure15,36. The observation that early hypercoagulability after trauma is more prevalent in females is in line with a previous report5.Limitations of our study include that we did not systematically look for occurrence of venous thromboembolism as this is a complication of major interest in patients initially surviving major trauma. In addition, only the summary of the SOFA score was collected, hereby we cannot comment on SOFA subgroups. It is also not possible to rule out a contribution of late hypercoagulability to the development of organ failure, as we only assessed ROTEM® on admission and after 24 hours. Prolonged hypercoagulability has been linked to increased risk of thromboembolic complications7,10,11. Also, we did not assess d-dimers and hereby we were not able to correlate ROTEM® findings to DIC scores. However, a recent review of pathology samples obtained early after trauma failed to demonstrate microthrombi despite the clinical presence of increased DIC scores37. Furthermore, in 40% of admitted patients ROTEM® values were not available at 24 hours following trauma, attributed to logistic issues, which could have introduced recruitment bias and contributed to an underestimation of hypercoagulability at this
46 | CHAPTER 2
time point. Limited reports have described the coagulopathic changes over time in trauma and a recent small cohort study suggested that hypercoagulability after trauma occurs after 48 hours38. Therefore, further research should include serial measurements and a prospective standardized observation of complications after trauma. However, the current data suggest that early hypercoagulability after trauma not only reduces early mortality9, but also seems to be associated with lower occurrence and severity of MOF and 28-day mortality.Altogether, this study has identified a significant proportion of patients with hypercoagulability as defined by ROTEM® at admission. Further work in larger studies should define the clinical consequences and prognostic value of identifying hypercoagulability, specifically including thromboembolic events, and might assess a role for very early, targeted use of anticoagulants in selected patients. The role of plasma or other blood components in potentially exacerbating the consequences of hypercoagulability is also an area of further research. In this study, patients with hypocoagulability on admission mostly tended to regress to normal values over time and not to hypercoagulability, irrespective of blood product ratio. This is in contrast with studies showing an association between amount of blood products and MOF39, but is in line with other studies, which suggested that other fluids were more associated with MOF than blood products40,41. Also, there is experimental evidence that FFP preserves endothelial integrity in haemorrhagic shock42.
CONCLUSION
In a cohort of trauma patients, 10% shows a hypercoagulable state, as defined by ROTEM® G value, within the first 24 hours. Occurrence of early hypercoagulability is not associated with development of MOF, moreover it appears to protect against adverse outcome. Admission ROTEM® variables indicating hypocoagulability are predictive of the development of MOF and mortality. Liberal use of FFP is not associated with enhanced hypercoagulability.
| 47
REFERENCES
PREDICTIVE VALUE OF HYPERCOAGULOPATHY FOR MOF
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Sauaia A, Moore FA, Moore EE, Moser KS,
Brennan R, Read RA, Pons PT: Epidemiology
of trauma deaths: a reassessment. J Trauma.
1995, 38:185–193.
Hoyt DB, Bulger EM, Knudson MM, Morris
J, Ierardi R, Sugerman HJ, Shackford SR,
Landercasper J, Winchell RJ, Jurkovich G,
Coffey SC, Chang M, O’Malley KF, Lowry
J, Trevisani GT, Cogbill TH: Death in the
operating room: an analysis of a multi-center
experience. J Trauma. 1994, 37:426–432.
Ulvik A, Kvale R, Wentzel-Larsen T, Flaatten
H: Multiple organ failure after trauma affects
even long-term survival and functional status.
Crit Care. 2007, 11:R95.
Brohi K, Cohen MJ, Davenport RA: Acute
coagulopathy of trauma: mechanism,
identification and effect. Curr Opin Crit Care.
2007, 13:680–685.
Schreiber MA, Differding J, Thorborg P,
Mayberry JC, Mullins RJ: Hypercoagulability is
most prevalent early after injury and in female
patients. J Trauma. 2005, 58:475–480.
Kaufmann CR, Dwyer KM, Crews JD, Dols SJ,
Trask AL: Usefulness of thrombelastography in
assessment of trauma patient coagulation. J
Trauma. 1997, 42:716–720.
Kashuk JL, Moore EE, Sabel A, Barnett C, Haenel
J, Le T, Pezold M, Lawrence J, Biffl WL, Cothren
CC, Johnson JL: Rapid thrombelastography
(r-TEG) identifies hypercoagulability and
predicts thromboembolic events in surgical
patients. Surgery. 2009, 146:764–772.
Mulier KE, Greenberg JG, Beilman GJ:
Hypercoagulability in porcine hemorrhagic
shock is present early after trauma and
resuscitation. J Surg Res. 2012, 174:e31–e35.
Branco BC, Inaba K, Ives C, Okoye O, Shulman
I, David JS, Schochl H, Rhee P, Demetriades D:
Thromboelastogram evaluation of the impact
of hypercoagulability in trauma patients.
Shock. 2014, 41:200–207
Park MS, Martini WZ, Dubick MA, Salinas
J, Butenas S, Kheirabadi BS, Pusateri AE,
Vos JA, Guymon CH, Wolf SE, Mann KG,
Holcomb JB: Thromboelastography as a
better indicator of hypercoagulable state after
injury than prothrombin time or activated
partial thromboplastin time. J Trauma. 2009,
67:266–275.
Cotton BA, Minei KM, Radwan ZA, Matijevic
N, Pivalizza E, Podbielski J, Wade CE,
Kozar RA, Holcomb JB: Admission rapid
thrombelastography predicts development
of pulmonary embolism in trauma patients.
J Trauma Acute Care Surg. 2012, 72:1470–
1475.
Fourrier F, Chopin C, Goudemand J, Hendrycx
S, Caron C, Rime A, Marey A, Lestavel P:
Septic shock, multiple organ failure, and
disseminated intravascular coagulation.
Compared patterns of antithrombin III,
protein C, and protein S deficiencies. Chest.
1992, 101:816–823.
Yan SB, Helterbrand JD, Hartman DL, Wright
TJ, Bernard GR: Low levels of protein C are
associated with poor outcome in severe
sepsis. Chest. 2001, 120:915–922.
Cohen MJ, Call M, Nelson M, Calfee CS, Esmon
CT, Brohi K, Pittet JF: Critical role of activated
protein C in early coagulopathy and later
organ failure, infection and death in trauma
patients. Ann Surg. 2012, 255:379–385. 15.
Gando S, Kameue T, Matsuda N, Hayakawa
M, Ishitani T, Morimoto Y, Kemmotsu O:
Combined activation of coagulation and
inflammation has an important role in
multiple organ dysfunction and poor outcome
after severe trauma. Thromb Haemost. 2002,
88:943–949.
Taura P, Rivas E, Martinez-Palli G, Blasi A,
Holguera JC, Balust J, Delgado S, Lacy AM:
Clinical markers of the hypercoagulable state
by rotational thrombelastometry in obese
patients submitted to bariatric surgery. Surg
Endosc. 2014, 28:543–551.
Muller MC, Meijers JC, Vroom MB, Juffermans
NP: Utility of thromboelastography and/or
2
48 |
REFERENCES
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
thromboelastometry in adults with sepsis: a
systematic review. Crit Care. 2014, 18:R30.
Davenport R, Manson J, De’Ath H, Platton
S, Coates A, Allard S, Hart D, Pearse R, Pasi
KJ, MacCallum P, Stanworth S, Brohi K:
Functional definition and characterization of
acute traumatic coagulopathy. Crit Care Med.
2011, 39:2652–2658.
Schochl H, Solomon C, Traintinger S, Nienaber
U, Tacacs-Tolnai A, Windhofer C, Bahrami S,
Voelckel W: Thromboelastometric (ROTEM)
findings in patients suffering from isolated
severe traumatic brain injury. J Neurotrauma.
2011, 28:2033–2041.
Meyer AS, Meyer MA, Sorensen AM,
Rasmussen LS, Hansen MB, Holcomb JB,
Cotton BA, Wade CE, Ostrowski SR, Johansson
PI: Thrombelastography and rotational
thromboelastometry early amplitudes in 182
trauma patients with clinical suspicion of
severe injury. J Trauma Acute Care Surg. 2014,
76:682–690. 21.
Tauber H, Innerhofer P, Breitkopf R,
Westermann I, Beer R, El Attal R, Strasak
A, Mittermayr M: Prevalence and impact
of abnormal ROTEM(R) assays in severe
blunt trauma: results of the ‘Diagnosis and
Treatment of Trauma-Induced Coagulopathy
(DIA-TRE-TIC) study’. Br J Anaesth. 2011,
107:378–387.
Baker SP, O’Neill B, Haddon W Jr, Long
WB: The injury severity score: a method for
describing patients with multiple injuries and
evaluating emergency care. J Trauma. 1974,
14:187–196.
Kashuk JL, Moore EE, Wohlauer M, Johnson
JL, Pezold M, Lawrence J, Biffl WL, Burlew
CC, Barnett C, Sawyer M, Sauaia A: Initial
experiences with point-of-care rapid
thrombelastography for management of
lifethreatening postinjury coagulopathy.
Transfusion. 2012, 52:23–33.
Antonelli M, Moreno R, Vincent JL, Sprung
CL, Mendoca A, Passariello M, Riccioni L,
Osborn J: Application of SOFA score to trauma
patients. Sequential Organ Failure Assessment.
Intensive Care Med. 1999, 25:389–394.
Differding JA, Underwood SJ, Van PY, Khaki
RA, Spoerke NJ, Schreiber MA: Trauma
induces a hypercoagulable state that is
resistant to hypothermia as measured
by thrombelastogram. Am J Surg 2011,
201:587–591.
Ostrowski SR, Sorensen AM, Larsen CF,
Johansson PI: Thrombelastography and
biomarker profiles in acute coagulopathy of
trauma: a prospective study. Scand J Trauma
Resusc Emerg Med. 2011, 19:64.
Aleshnick M, Orfeo T, Brummel-Ziedins K,
Gissel M, Mann K:
Interchangeability of rotational elastographic
instruments and reagents. J Trauma Acute
Care Surg. 2014, 76:107–113.
Hagemo JS, Naess PA, Johansson P, Windelov
NA, Cohen MJ, Roislien J,
Brohi K, Heier HE, Hestnes M, Gaarder C:
Evaluation of TEG((R)) and RoTEM ((R)) inter-
changeability in trauma patients. Injury. 2013,
44:600–605.
Khan S, Brohi K, Chana M, Raza I, Stanworth
S, Gaarder C, Davenport R: Hemostatic
resuscitation is neither hemostatic nor
resuscitative in trauma hemorrhage. J Trauma
Acute Care Surg. 2014, 76:561–567.
Nystrup KB, Windelov NA, Thomsen AB,
Johansson PI: Reduced clot strength upon
admission, evaluated by thrombelastography
(TEG), in trauma patients is independently
associated with increased 30-day mortality.
Scand J Trauma Resusc Emerg Med. 2011,
19:52.
Kunio NR, Differding JA, Watson KM, Stucke
RS, Schreiber MA: Thrombelastography-
identified coagulopathy is associated with
increased morbidity and mortality after
traumatic brain injury. Am J Surg. 2012,
203:584–588.
Rugeri L, Levrat A, David JS, Delecroix
CHAPTER 2
| 49
REFERENCES
PREDICTIVE VALUE OF HYPERCOAGULOPATHY FOR MOF
33
34
35
36
37
38
39
40
41
42
E, Floccard B, Gros A, Allaouchiche B,
Negrier C: Diagnosis of early coagulation
abnormalities in trauma patients by rotation
thrombelastography. J Thromb Haemost.
2007, 5:289–295.
Schochl H, Cotton B, Inaba K, Nienaber U,
Fischer H, Voelckel W, Solomon C: FIBTEM
provides early prediction of massive transfusion
in trauma. Crit Care. 2011, 15:R265.
Schochl H, Nienaber U, Maegele M,
Hochleitner G, Primavesi F, Steitz B, Arndt C,
Hanke A, Voelckel W, Solomon C: Transfusion
in trauma:
thromboelastometry-guided coagulation
factor concentrate-based therapy versus
standard fresh frozen plasma-based therapy.
Crit Care. 2011, 15:R83.
Rourke C, Curry N, Khan S, Taylor R, Raza I,
Davenport R, Stanworth S, Brohi K: Fibrinogen
levels during trauma hemorrhage, response to
replacement therapy, and association with
patient outcomes. J Thromb Haemost. 2012,
10:1342–1351.
Gando S: Acute coagulopathy of trauma
shock and coagulopathy of trauma: a rebuttal.
You are now going down the wrong path. J
Trauma 2009, 67:381–383.
Rizoli S, Nascimento B Jr, Key N, Tien HC,
Muraca S, Pinto R, Khalifa M,
Plotkin A, Callum J: Disseminated intravascular
coagulopathy in the first 24 hours after
trauma: the association between ISTH score
and anatomopathologic evidence. J Trauma.
2011, 71:S441–S447.
Chapman BC, Moore EE, Barnett C, Stovall RT,
Biffl WL, Burlew CC, Bensard DD, Jurkovich
GJ, Pieracci FM: Hypercoagulability following
blunt solid abdominal organ injury: when to
initiate anticoagulation. Am J Surg. 2013,
206:917–923.
Johnson JL, Moore EE, Kashuk JL, Banerjee A,
Cothren CC, Biffl WL, Sauaia A: Effect of blood
products transfusion on the development of
postinjury multiple organ failure. Arch Surg.
2010, 145:973–977.
Park PK, Cannon JW, Ye W, Blackbourne
LH, Holcomb JB, Beninati W, Napolitano LM:
Transfusion strategies and development of
acute respiratory distress syndrome in combat
casualty care. J Trauma Acute Care Surg.
2013, 75:S238–S246.
Robinson BR, Cotton BA, Pritts TA, Branson
R, Holcomb JB, Muskat P, Fox EE, Wade CE,
del Junco DJ, Bulger EM, Cohen MJ, Schreiber
MA, Myers JG, Brasel KJ, Phelan HA, Alarcon
LH, Rahbar MH, Callcut RA, PROMMTT study
group: Application of the Berlin definition
in PROMMTT patients: the impact of
resuscitation on the incidence of hypoxemia.
J Trauma Acute Care Surg. 2013, 75:S61–S67.
Torres LN, Sondeen JL, Ji L, Dubick MA,
Filho IT: Evaluation of resuscitation fluids on
endothelial glycocalyx, venular blood flow,
and coagulation function after hemorrhagic
shock in rats. J Trauma Acute Care Surg.
2013, 75:759–766.
2
K. Balvers, M.R. Wirtz, C. Rourke, S. Eaglestone, K. Brohi, S. Stanworth, C. Gaarder, J.C. Goslings, N.P. Juffermans
Submitted
HAEMOGLOBIN LEVEL AND NEUROLOGIC OUTCOME IN PATIENTS WITH SEVERE TRAUMATIC BRAIN INJURY
3
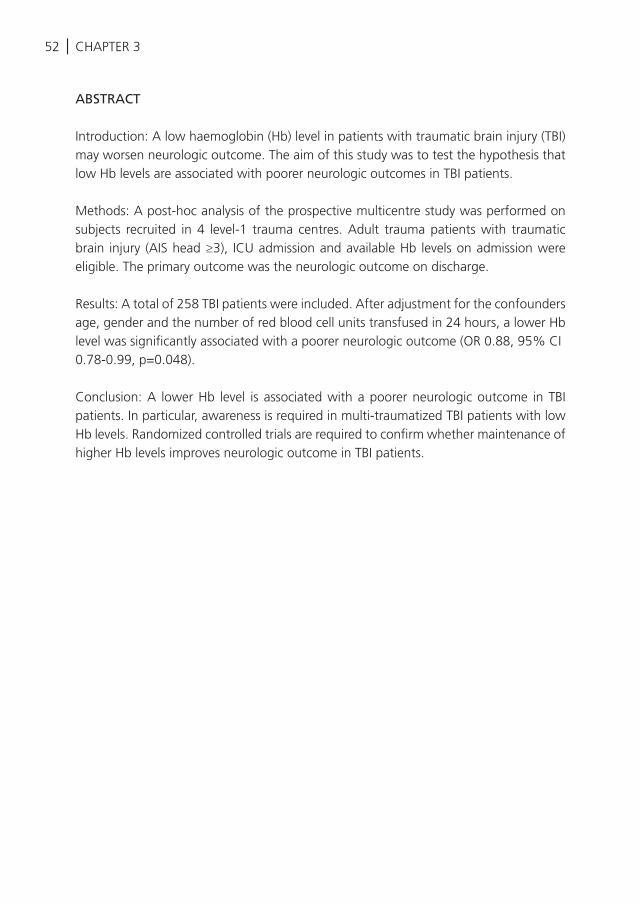
CHAPTER 352 |
ABSTRACT
Introduction: A low haemoglobin (Hb) level in patients with traumatic brain injury (TBI) may worsen neurologic outcome. The aim of this study was to test the hypothesis that low Hb levels are associated with poorer neurologic outcomes in TBI patients.
Methods: A post-hoc analysis of the prospective multicentre study was performed on subjects recruited in 4 level-1 trauma centres. Adult trauma patients with traumatic brain injury (AIS head ≥3), ICU admission and available Hb levels on admission were eligible. The primary outcome was the neurologic outcome on discharge.
Results: A total of 258 TBI patients were included. After adjustment for the confounders age, gender and the number of red blood cell units transfused in 24 hours, a lower Hb level was significantly associated with a poorer neurologic outcome (OR 0.88, 95% CI 0.78-0.99, p=0.048).
Conclusion: A lower Hb level is associated with a poorer neurologic outcome in TBI patients. In particular, awareness is required in multi-traumatized TBI patients with low Hb levels. Randomized controlled trials are required to confirm whether maintenance of higher Hb levels improves neurologic outcome in TBI patients.
HAEMOGLOBIN LEVEL AND NEUROLOGIC OUTCOME IN TBI
3
| 53
INTRODUCTION
Anaemia is frequently observed in patients with traumatic brain injury (TBI)1, 2 and is associated with an increased mortality1, 3-5. Anaemia hampers adequate cerebral oxygenation, which induce cerebral oedema and an increased intracranial pressure6-8. Transfusion of red blood cells (RBCs) is associated with increased haemoglobin (Hb) levels and an improved brain tissue oxygenation9, 10. Therefore, transfusion of RBCs may be appropriate in TBI patients in order to maintain higher Hb levels and to improve neurological outcome. However, transfusion of RBCs is also associated with adverse events11-13. Clear evidence for a beneficial effect of higher Hb levels on outcome in TBI patients is therefore required.
The majority of previous studies investigating the association between Hb levels and outcome in trauma patients have used mortality as a primary endpoint. Given the relation between anaemia and cerebral performance,9, 10 neurologic recovery may also be a relevant endpoint, and has indeed been used as primary outcome in a recent Hb threshold trial in TBI patients5. However, the number of studies investigating the association between Hb levels and neurologic outcome in TBI patients is small and studies have yielded contradicting results3, 5, 14-16. The aim of this study was to test the hypothesis that low Hb levels are associated with poorer neurologic outcomes in TBI patients.
MATERIALS AND METHODS
This study is a post-hoc analysis of the ongoing Activation of Coagulation and Inflammation in Trauma study (ACIT, United Kingdom Clinical Research Network Study Portfolio, ID: 5637), which is a prospective observational multicentre study on coagulopathy in trauma.
Subjects were recruited between January 2008 and December 2014 in 4 European level-1 trauma centres; London, Oxford, Oslo and Amsterdam. All adult trauma patients (age≥18 years) who met the local criteria for highest trauma team level activation were enrolled. Exclusion criteria of the ACIT study were age <18 years old, arrival in the emergency department more than 2 hours after injury as well as transfer from another hospital, transfusion of more than 2000 mL of intravenous fluids prior to Emergency Department (ED) arrival and burns covering more than 5% of the total body surface area. Patients were retrospectively excluded if they declined to give informed consent, were found to be taking anticoagulant medications other than aspirin (<650mg/day), or had moderate or severe liver disease (Child’s classification B or C3) or a known bleeding diathesis.
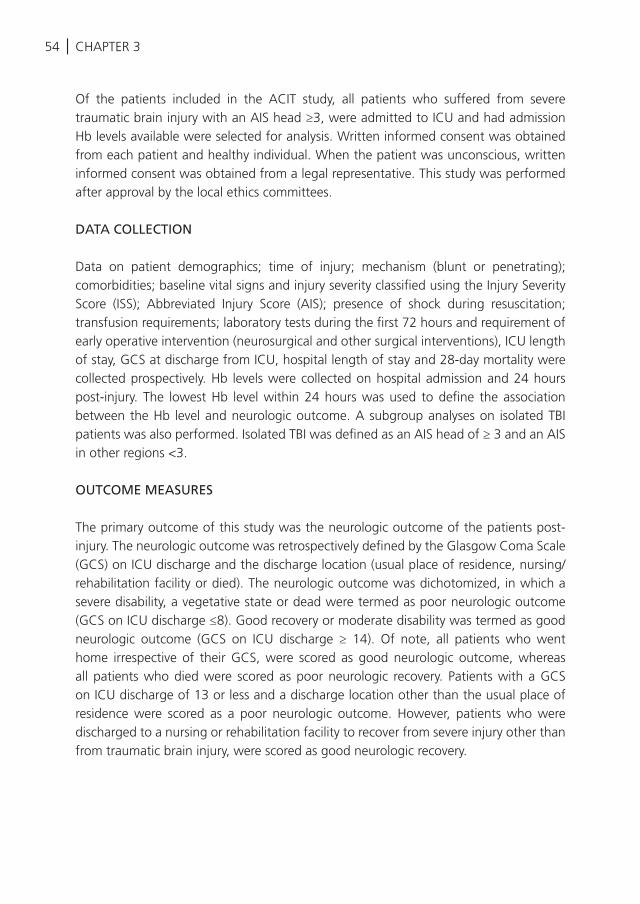
CHAPTER 354 |
Of the patients included in the ACIT study, all patients who suffered from severe traumatic brain injury with an AIS head ≥3, were admitted to ICU and had admission Hb levels available were selected for analysis. Written informed consent was obtained from each patient and healthy individual. When the patient was unconscious, written informed consent was obtained from a legal representative. This study was performed after approval by the local ethics committees.
DATA COLLECTION
Data on patient demographics; time of injury; mechanism (blunt or penetrating); comorbidities; baseline vital signs and injury severity classified using the Injury Severity Score (ISS); Abbreviated Injury Score (AIS); presence of shock during resuscitation; transfusion requirements; laboratory tests during the first 72 hours and requirement of early operative intervention (neurosurgical and other surgical interventions), ICU length of stay, GCS at discharge from ICU, hospital length of stay and 28-day mortality were collected prospectively. Hb levels were collected on hospital admission and 24 hours post-injury. The lowest Hb level within 24 hours was used to define the association between the Hb level and neurologic outcome. A subgroup analyses on isolated TBI patients was also performed. Isolated TBI was defined as an AIS head of ≥ 3 and an AIS in other regions <3.
OUTCOME MEASURES
The primary outcome of this study was the neurologic outcome of the patients post-injury. The neurologic outcome was retrospectively defined by the Glasgow Coma Scale (GCS) on ICU discharge and the discharge location (usual place of residence, nursing/rehabilitation facility or died). The neurologic outcome was dichotomized, in which a severe disability, a vegetative state or dead were termed as poor neurologic outcome (GCS on ICU discharge ≤8). Good recovery or moderate disability was termed as good neurologic outcome (GCS on ICU discharge ≥ 14). Of note, all patients who went home irrespective of their GCS, were scored as good neurologic outcome, whereas all patients who died were scored as poor neurologic recovery. Patients with a GCS on ICU discharge of 13 or less and a discharge location other than the usual place of residence were scored as a poor neurologic outcome. However, patients who were discharged to a nursing or rehabilitation facility to recover from severe injury other than from traumatic brain injury, were scored as good neurologic recovery.

HAEMOGLOBIN LEVEL AND NEUROLOGIC OUTCOME IN TBI
3
| 55
STATISTICAL ANALYSIS
Continuous normally distributed variables will be expressed by their mean and standard deviation or when not normally distributed as medians and their interquartile ranges. Categorical variables will be expressed as n (%). To test groups Student’s t-test will be used, if continuous data is not normally distributed the Mann-Whitney U test will be used. Categorical variables will be compared with the Chi-square test or Fisher’s exact tests.
The goal of the primary analysis was to quantify the relationship between Hb levels at admission on the emergency department and the neurologic outcomes in TBI patients, controlling for other variables17. We identified potential predictors of neurologic outcome by univariable logistic regression. From the univariate logistic regression, all potential confounders were selected that showed a p value of less or equal to 0.10 or where possibly otherwise clinically relevant to be included within the final multiple logistic regression model. Confounding was defined as ≥ 10% change in the coefficient of the central determinant (Hb level) as a consequence of adding a covariate. The added covariates in the final model were tested for linearity assumption18. Confounders included in the analyses were trauma mechanism, gender, age, intubation, AIS head/neck, systolic blood pressure (SBP) on ED, GCS on ED and the number of transfused red blood cells (RBCs) in 24 hours3, 15, 16. Statistical significance was considered to be a p< 0.05, whether appropriate statistical uncertainty was expressed by the 95% confidence levels. Statistical analyses were performed in SPSS version 21(IBM, Chicago, IL, USA).
RESULTS
In total 2760 severely injured trauma patients met the ACIT study inclusion criteria. Of these 2760 patients, 215 patients were excluded retrospectively as patients declined to give consent or due to retrospective exclusion criteria. Of the remaining 2545 patients, 258 patients suffered from severe traumatic brain injury with an AIS head ≥3, were admitted to ICU, had admission Hb levels available and were eligible for this study. A total of 112 patients (43%) were diagnosed with isolated TBI. The mean age was 43 ±19 years, of which the majority was male (74%). Patients were severely injured with an ISS of 30 (±12), a GCS on the ED of 7 (3-13) and a lowest Hb measured within 24 hours of 10.8 (±2.4) g/dL. The overall mortality on 28-days was 30% (Table 1).
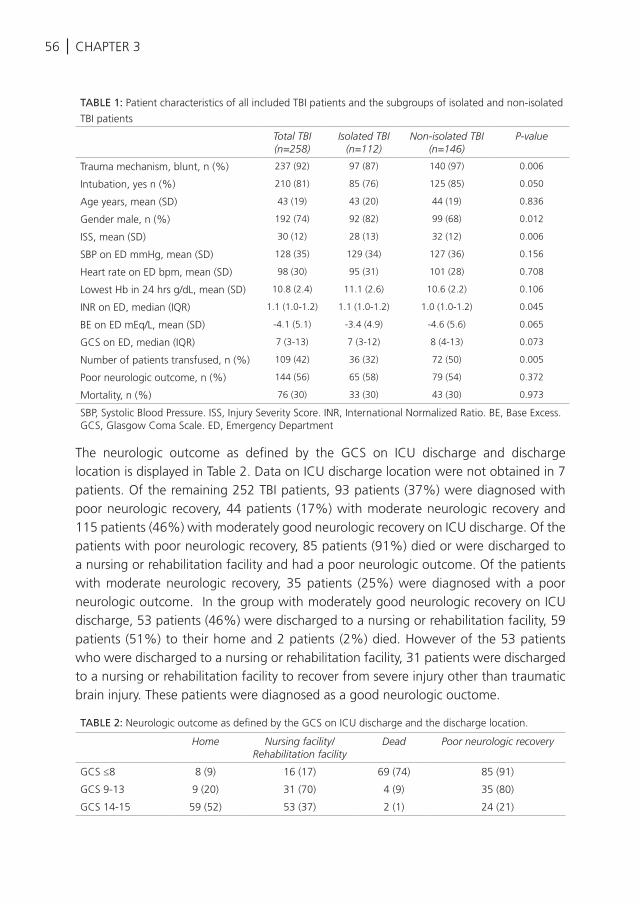
CHAPTER 356 |
The neurologic outcome as defined by the GCS on ICU discharge and discharge location is displayed in Table 2. Data on ICU discharge location were not obtained in 7 patients. Of the remaining 252 TBI patients, 93 patients (37%) were diagnosed with poor neurologic recovery, 44 patients (17%) with moderate neurologic recovery and 115 patients (46%) with moderately good neurologic recovery on ICU discharge. Of the patients with poor neurologic recovery, 85 patients (91%) died or were discharged to a nursing or rehabilitation facility and had a poor neurologic outcome. Of the patients with moderate neurologic recovery, 35 patients (25%) were diagnosed with a poor neurologic outcome. In the group with moderately good neurologic recovery on ICU discharge, 53 patients (46%) were discharged to a nursing or rehabilitation facility, 59 patients (51%) to their home and 2 patients (2%) died. However of the 53 patients who were discharged to a nursing or rehabilitation facility, 31 patients were discharged to a nursing or rehabilitation facility to recover from severe injury other than traumatic brain injury. These patients were diagnosed as a good neurologic ouctome.
TABLE 2: Neurologic outcome as defined by the GCS on ICU discharge and the discharge location.
Home Nursing facility/Rehabilitation facility
Dead Poor neurologic recovery
GCS ≤8 8 (9) 16 (17) 69 (74) 85 (91)
GCS 9-13 9 (20) 31 (70) 4 (9) 35 (80)
GCS 14-15 59 (52) 53 (37) 2 (1) 24 (21)
TABLE 1: Patient characteristics of all included TBI patients and the subgroups of isolated and non-isolated
TBI patients
Total TBI(n=258)
Isolated TBI(n=112)
Non-isolated TBI(n=146)
P-value
Trauma mechanism, blunt, n (%) 237 (92) 97 (87) 140 (97) 0.006
Intubation, yes n (%) 210 (81) 85 (76) 125 (85) 0.050
Age years, mean (SD) 43 (19) 43 (20) 44 (19) 0.836
Gender male, n (%) 192 (74) 92 (82) 99 (68) 0.012
ISS, mean (SD) 30 (12) 28 (13) 32 (12) 0.006
SBP on ED mmHg, mean (SD) 128 (35) 129 (34) 127 (36) 0.156
Heart rate on ED bpm, mean (SD) 98 (30) 95 (31) 101 (28) 0.708
Lowest Hb in 24 hrs g/dL, mean (SD) 10.8 (2.4) 11.1 (2.6) 10.6 (2.2) 0.106
INR on ED, median (IQR) 1.1 (1.0-1.2) 1.1 (1.0-1.2) 1.0 (1.0-1.2) 0.045
BE on ED mEq/L, mean (SD) -4.1 (5.1) -3.4 (4.9) -4.6 (5.6) 0.065
GCS on ED, median (IQR) 7 (3-13) 7 (3-12) 8 (4-13) 0.073
Number of patients transfused, n (%) 109 (42) 36 (32) 72 (50) 0.005
Poor neurologic outcome, n (%) 144 (56) 65 (58) 79 (54) 0.372
Mortality, n (%) 76 (30) 33 (30) 43 (30) 0.973
SBP, Systolic Blood Pressure. ISS, Injury Severity Score. INR, International Normalized Ratio. BE, Base Excess. GCS, Glasgow Coma Scale. ED, Emergency Department
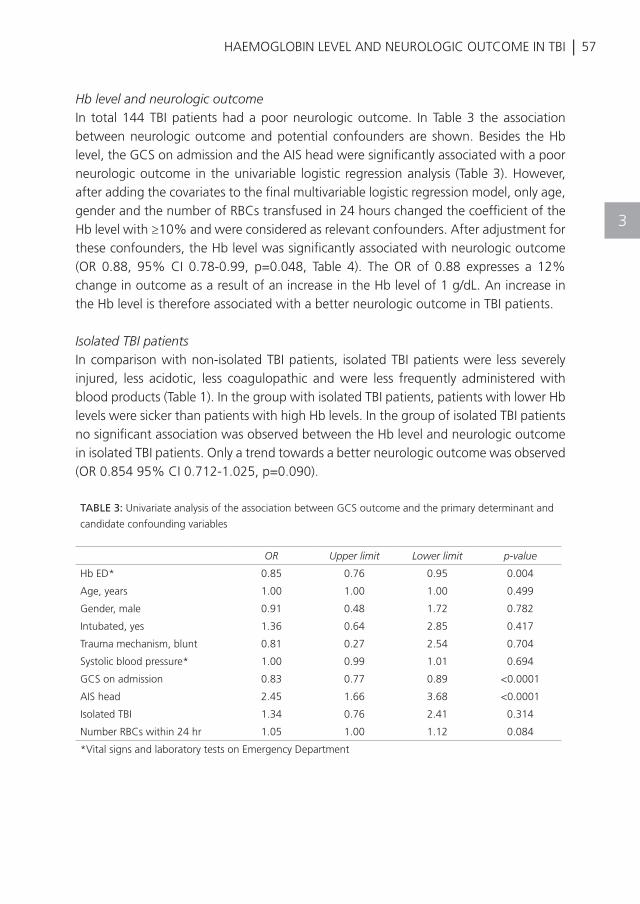
HAEMOGLOBIN LEVEL AND NEUROLOGIC OUTCOME IN TBI
3
| 57
Hb level and neurologic outcomeIn total 144 TBI patients had a poor neurologic outcome. In Table 3 the association between neurologic outcome and potential confounders are shown. Besides the Hb level, the GCS on admission and the AIS head were significantly associated with a poor neurologic outcome in the univariable logistic regression analysis (Table 3). However, after adding the covariates to the final multivariable logistic regression model, only age, gender and the number of RBCs transfused in 24 hours changed the coefficient of the Hb level with ≥10% and were considered as relevant confounders. After adjustment for these confounders, the Hb level was significantly associated with neurologic outcome (OR 0.88, 95% CI 0.78-0.99, p=0.048, Table 4). The OR of 0.88 expresses a 12% change in outcome as a result of an increase in the Hb level of 1 g/dL. An increase in the Hb level is therefore associated with a better neurologic outcome in TBI patients.
Isolated TBI patientsIn comparison with non-isolated TBI patients, isolated TBI patients were less severely injured, less acidotic, less coagulopathic and were less frequently administered with blood products (Table 1). In the group with isolated TBI patients, patients with lower Hb levels were sicker than patients with high Hb levels. In the group of isolated TBI patients no significant association was observed between the Hb level and neurologic outcome in isolated TBI patients. Only a trend towards a better neurologic outcome was observed (OR 0.854 95% CI 0.712-1.025, p=0.090).
TABLE 3: Univariate analysis of the association between GCS outcome and the primary determinant and
candidate confounding variables
OR Upper limit Lower limit p-value
Hb ED* 0.85 0.76 0.95 0.004
Age, years 1.00 1.00 1.00 0.499
Gender, male 0.91 0.48 1.72 0.782
Intubated, yes 1.36 0.64 2.85 0.417
Trauma mechanism, blunt 0.81 0.27 2.54 0.704
Systolic blood pressure* 1.00 0.99 1.01 0.694
GCS on admission 0.83 0.77 0.89 <0.0001
AIS head 2.45 1.66 3.68 <0.0001
Isolated TBI 1.34 0.76 2.41 0.314
Number RBCs within 24 hr 1.05 1.00 1.12 0.084
*Vital signs and laboratory tests on Emergency Department
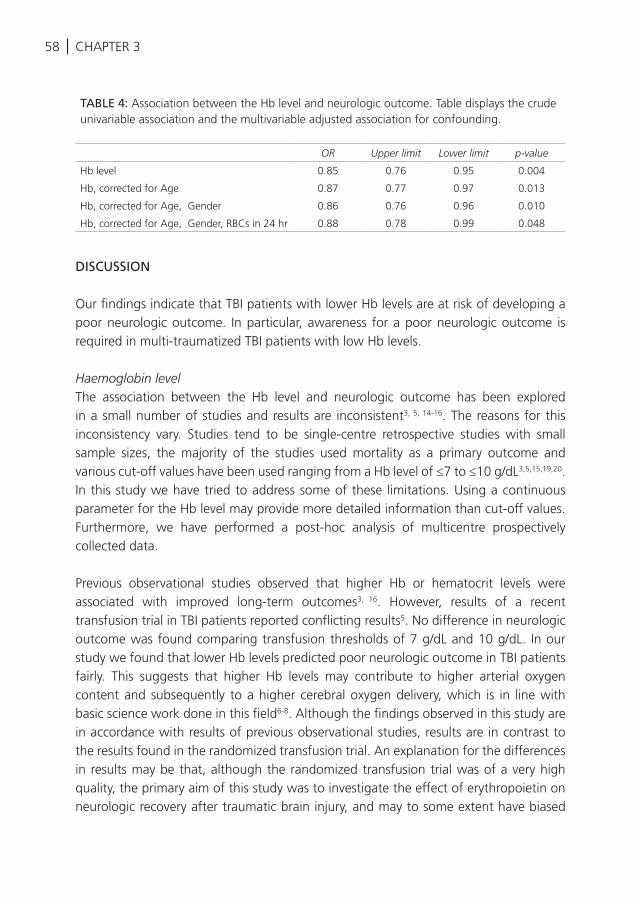
CHAPTER 358 |
DISCUSSION
Our findings indicate that TBI patients with lower Hb levels are at risk of developing a poor neurologic outcome. In particular, awareness for a poor neurologic outcome is required in multi-traumatized TBI patients with low Hb levels.
Haemoglobin levelThe association between the Hb level and neurologic outcome has been explored in a small number of studies and results are inconsistent3, 5, 14-16. The reasons for this inconsistency vary. Studies tend to be single-centre retrospective studies with small sample sizes, the majority of the studies used mortality as a primary outcome and various cut-off values have been used ranging from a Hb level of ≤7 to ≤10 g/dL3,5,15,19,20. In this study we have tried to address some of these limitations. Using a continuous parameter for the Hb level may provide more detailed information than cut-off values. Furthermore, we have performed a post-hoc analysis of multicentre prospectively collected data.
Previous observational studies observed that higher Hb or hematocrit levels were associated with improved long-term outcomes3, 16. However, results of a recent transfusion trial in TBI patients reported conflicting results5. No difference in neurologic outcome was found comparing transfusion thresholds of 7 g/dL and 10 g/dL. In our study we found that lower Hb levels predicted poor neurologic outcome in TBI patients fairly. This suggests that higher Hb levels may contribute to higher arterial oxygen content and subsequently to a higher cerebral oxygen delivery, which is in line with basic science work done in this field6-8. Although the findings observed in this study are in accordance with results of previous observational studies, results are in contrast to the results found in the randomized transfusion trial. An explanation for the differences in results may be that, although the randomized transfusion trial was of a very high quality, the primary aim of this study was to investigate the effect of erythropoietin on neurologic recovery after traumatic brain injury, and may to some extent have biased
TABLE 4: Association between the Hb level and neurologic outcome. Table displays the crude univariable association and the multivariable adjusted association for confounding.
OR Upper limit Lower limit p-value
Hb level 0.85 0.76 0.95 0.004
Hb, corrected for Age 0.87 0.77 0.97 0.013
Hb, corrected for Age, Gender 0.86 0.76 0.96 0.010
Hb, corrected for Age, Gender, RBCs in 24 hr 0.88 0.78 0.99 0.048
HAEMOGLOBIN LEVEL AND NEUROLOGIC OUTCOME IN TBI
3
| 59
the results of the effect of the Hb thresholds on the neurologic outcome. Additionally, Hb levels were relatively high and above transfusion thresholds.
We found no significant association between the Hb level and poor neurologic outcome in patients with isolated TBI. Isolated TBI patients were less injured than non-isolated TBI patients. Additionally, despite the fact that Hb levels were not significantly different between both groups, polytrauma patients with TBI received significantly more blood products than isolated TBI patients. This suggests that blood loss was more severe in multi-traumatized TBI patients, which resulted in a reduced cerebral oxygenation and a poorer neurologic outcome. However, large randomized controlled trials in TBI patients are required to further investigate the association between low Hb levels and neurologic outcome.
Limitations to this study should be acknowledged. A substantial proportion of patients in this study presented with multi-trauma and heterogeneity in our study population was therefore considerable. Furthermore, we used a retrospectively defined neurologic outcome as primary outcome and this post-hoc analysis of prospectively collected data may have missed confounders unaccounted for. Also, due to strict inclusion criteria, results do not hold for those patients on anticoagulation as these were excluded in this study and time of transfusion was not registered. Additionally, it was not feasible to investigate the association between Hb levels lower than 9 g/dL and neurologic outcome, as this was hampered by small patient numbers. Lastly, the cause of death was not documented systematically in this study.
In summary, we have documented the association between low Hb levels and poor neurologic outcome in TBI patients. In particular, awareness is required in multi-traumatized TBI patients with low Hb levels. Randomized controlled trials are needed to assess whether maintenance of higher Hb levels improve functional outcome in TBI patients.
60 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
Salim A, Hadjizacharia P, DuBose J, Brown
C, Inaba K, Chan L, et al. Role of anemia
in traumatic brain injury. J Am Coll Surg
2008;207(3):398-406.
Sekhon MS, McLean N, Henderson WR,
Chittock DR, Griesdale DE. Association of
hemoglobin concentration and mortality in
critically ill patients with severe traumatic
brain injury. Crit Care. 2012;16(4):R128.
Carlson AP, Schermer CR, Lu SW.
Retrospective evaluation of anemia and
transfusion in traumatic brain injury. J Trauma.
2006;61(3):567-71.
Hare GM, Mazer CD, Hutchison JS,
McLaren AT, Liu E, Rassouli A, et al. Severe
hemodilutional anemia increases cerebral
tissue injury following acute neurotrauma. J
Appl Physiol. 2007;103(3):1021-9.
Robertson CS, Hannay HJ, Yamal JM, Gopinath
S, Goodman JC, Tilley BC, et al. Effect of
erythropoietin and transfusion threshold on
neurological recovery after traumatic brain
injury: a randomized clinical trial. JAMA.
2014;312(1):36-47.
Chappell JE, Shackford SR, McBride WJ. Effect
of hemodilution with diaspirin cross-linked
hemoglobin on intracranial pressure, cerebral
perfusion pressure, and fluid requirements
after head injury and shock. J Neurosurg
1997;86(1):131-8.
Hare GM, Mazer CD, Hutchison JS,
McLaren AT, Liu E, Rassouli A, et al. Severe
hemodilutional anemia increases cerebral
tissue injury following acute neurotrauma.
Journal of applied physiology (Bethesda, Md
: 1985). 2007;103(3):1021-9.
Oddo M, Levine JM, Kumar M, Iglesias K,
Frangos S, Maloney-Wilensky E, et al. Anemia
and brain oxygen after severe traumatic brain
injury. Intensive Care Med. 2012;38(9):1497-
504.
Zygun DA, Nortje J, Hutchinson PJ, Timofeev I,
Menon DK, Gupta AK. The effect of red blood
cell transfusion on cerebral oxygenation and
metabolism after severe traumatic brain injury.
Crit Care Med 2009;37(3):1074-8.
Smith MJ, Stiefel MF, Magge S, Frangos S,
Bloom S, Gracias V, et al. Packed red blood
cell transfusion increases local cerebral
oxygenation. Crit Care Med 2005;33(5):1104-
8.
Claridge JA, Sawyer RG, Schulman AM,
McLemore EC, Young JS. Blood transfusions
correlate with infections in trauma patients
in a dose-dependent manner. Am Surg
2002;68(7):566-72.
Hill GE, Frawley WH, Griffith KE, Forestner
JE, Minei JP. Allogeneic blood transfusion
increases the risk of postoperative bacterial
infection: a meta-analysis. J Trauma.
2003;54(5):908-14.
Malone DL, Dunne J, Tracy JK, Putnam AT,
Scalea TM, Napolitano LM. Blood transfusion,
independent of shock severity, is associated
with worse outcome in trauma. J Trauma.
2003;54(5):898-905.
Elterman J, Brasel K, Brown S, Bulger E,
Christenson J, Kerby JD, et al. Transfusion of
red blood cells in patients with a prehospital
Glasgow Coma Scale score of 8 or less and
no evidence of shock is associated with
worse outcomes. J Trauma Acute Care Surg
2013;75(1):8-14.
Warner MA, O’Keeffe T, Bhavsar P, Shringer
R, Moore C, Harper C, et al. Transfusions and
long-term functional outcomes in traumatic
brain injury. J Neurosurg 2010;113(3):539-46.
Griesdale DE, Sekhon MS, Menon DK, Lavinio
A, Donnelly J, Robba C, et al. Hemoglobin Area
and Time Index Above 90 g/L are Associated
with Improved 6-Month Functional Outcomes
in Patients with Severe Traumatic Brain Injury.
Neurocrit Care. 2015;23(1):78-84.
David G. Kleinbaum LLK, Azhar Nizam, Keith E.
Muller Applied Refression Analysis And Other
Multivariate Methods: Brooks/Cole2008.
Hosmer DW LS. Applied Logistic Regression:
New York: Wiley1989.
CHAPTER 3

| 61
REFERENCES
HAEMOGLOBIN LEVEL AND NEUROLOGIC OUTCOME IN TBI
19
20
George ME, Skarda DE, Watts CR, Pham
HD, Beilman GJ. Aggressive red blood cell
transfusion: no association with improved
outcomes for victims of isolated traumatic
brain injury. Neurocrit Care. 2008;8(3):337-
43.
McIntyre LA, Fergusson DA, Hutchison JS,
Pagliarello G, Marshall JC, Yetisir E, et al.
Effect of a liberal versus restrictive transfusion
strategy on mortality in patients with
moderate to severe head injury. Neurocrit
Care. 2006;5(1):4-9.
3
K. Balvers, N. Curry, D.J.B. Kleinveld, A.N. Böing, R. Nieuwland, J.C. Goslings, and N.P. Juffermans
Shock 2015
ENDOGENOUS MICROPARTICLES DRIVE THE PROINFLAMMATORY HOST IMMUNE RESPONSE IN
SEVERELY INJURED TRAUMA PATIENTS
4
64 | CHAPTER 4
ABSTRACT
Introduction: Severe trauma affects the immune system, which in its turn is associated with poor outcome. The mediators driving the immune responses in trauma are largely unknown. The aim of this study was to investigate the role of endogenous microparticles (MPs) in mediating the immune response following severe trauma.
Methods: A prospective, observational substudy of the ACIT II (Activation of Coagulation and Inflammation in Trauma II) study was performed at our academic level I trauma centre. Adult multiple-trauma patients with an injury severity score of 15 or higher were included between May 2012 and June 2013. Ex vivo whole-blood stimulation with lipopolysaccharide was performed on aseptically collected patient plasma containing MPs and in plasma depleted of MPs. Flow cytometry and transmission electronic microscopy were performed on plasma samples to investigate the numbers and cellular origin of MPs. Healthy individuals served as a control group.
Results: Ten trauma patients and 10 control subjects were included. Trauma patients were significantly injured with a median injury severity score of 19 (range, 17-45). Patients were neither in shock nor bleeding. On admission to the hospital, the host response to bacterial stimulation was blunted in trauma patients compared with control subjects, as reflected by decreased production of interleukin 6 (IL-6), IL-10, and tumour necrosis factor α (P< 0.001). In trauma patients, MP-positive plasma was associated with a significantly higher synthesis of IL-6 and tumour necrosis factor α compared with plasma depleted from MPs (P = 0.047 and 0.002, respectively). Compared with control subjects, the number of circulating MPs was significantly decreased in trauma patients (P = 0.009). Most MPs originated from platelets. Multiple cellular protrusions, which result in MP formation, were observed in plasma from trauma patients, but not in control subjects.
Conclusions: On admission, trauma patients have a reduced immune response toward endotoxin challenge, which is, at least in part, mediated by MPs, which circulate in low numbers and in early stages. Most MPs originate from platelets, which indicates that these cells may be the most important source of MPs involved in initiating an inflammatory host response after injury.
| 65
4
MICROPARTICLES IN TRAUMA
INTRODUCTION
Traumatic injuries are responsible for a high morbidity and mortality worldwide 1. Multiple trauma affects the immune system in a complex way. Currently, it is thought that both hyperinflammation and immunosuppression can occur following severe trauma. On the one hand, hyperinflammation is associated with a cytokine storm causing a systematic inflammatory response syndrome (SIRS), which is strongly associated with the occurrence of multiple organ failure and mortality2-13. On the other hand, immunosuppression is an early event following trauma, characterized by a decreased ability of immune cells to respond to bacterial antigens and is associated with an enhanced risk of developing hospital-acquired infections and mortality3-5, 14-17. Therefore, understanding the immune response is important to improve outcome of trauma patients. However, mediators of host responses after injury are largely unknown.
Microparticles (MPs) are vesicles shed into the bloodstream by cells under conditions of stress. Microparticles can originate from various cells and are thought to play an important role in intercellular communication by activating circulating monocytes and leukocytes with subsequent production of inflammatory cytokines18-20. In line with this, previous studies have reported increased numbers of circulating MPs in patients with SIRS and sepsis7, 19, 21, 22. Also, increased numbers of MPs, mainly originating from platelets23, are observed in trauma patients with SIRS23-25. It is unknown whether increased numbers of circulating MPs are cause or effect of the host immune response after injury. If MPs mediate the immune response after injury, they could be useful biomarkers or therapeutic targets to influence the immune system and improve the long-term outcome of trauma patients.
The aim of this study was to investigate the role of MPs in mediating the immune response following trauma. We determined the numbers and cellular origin of MPs following severe trauma and investigated the role of MPs in the generation of a host immune response to a bacterial antigen.
MATERIALS AND METHODS
This study was a substudy of the ongoing Activation of Coagulation and Inflammation in Trauma II study (ACIT II, UKCRN ID: 5637), which is a prospective observational multicentre study on mechanisms of coagulopathy and inflammation in trauma patients. This substudy was performed at our academic level I trauma centre after approval by the local ethics committee.
66 | CHAPTER 4
Ten adult severely injured multiple-trauma patients with an injury severity score (ISS) of more than 15 who were admitted to the emergency department (ED) at the Academic Medical Center between May 2012 and June 2013 were studied. Patients who were transferred from other hospitals, who presented more than 2 h after injury on the ED, who were using anticoagulant medication, or for whom no informed consent was obtained were excluded. Patient demographics, mechanism of injury, prehospital fluids, Glasgow Coma Scale, injury severity score (ISS), systolic blood pressure, heart rate, haemoglobin, prothrombin time, platelet count, and leukocytes were recorded on the ED. Furthermore, data about the length of stay and in-hospital mortality were collected. Healthy volunteers of both sexes (aged 20-35 years) served as a control group. Written informed consent was obtained from each patient and control subject. When the patient was unconscious, written informed consent was obtained from a legal representative.
Blood samplesOn admission to the ED, blood samples were collected into buffered trisodium citrate vacutainer tubes (2.7 mL; Becton Dickinson, Plymouth, UK). Within 15 min after blood sampling, the collection tubes were centrifuged to prepare platelet-free plasma (1,750 RCF, 18°C, 10 min). The upper two-thirds of this plasma was collected and centrifuged again. The obtained platelet-free plasma was stored as 250 2L aliquots at -80°C until time of assay. Blood sampling procedures were identical for control subjects.
Cytokine production in response to lipopolysaccharide stimulationPrior to centrifugation, samples were thawed on melting ice for 1 h. Microparticles were pelleted by ultracentrifugation (50,000 revolutions/min, 20°C for 1h). After centrifugation, the MP-depleted (MP-) supernatant was removed and used as a control. The MP-containing pellet was used as MP-positive (MP+) samples.
To perform whole-blood stimulation, heparin-anticoagulated blood was collected from a healthy donor. To study the effect of MPs, 250 µL whole blood was 1:1 diluted with RPMI medium supplemented with glutamine 0.3 g/L to which either 50 µL trauma plasma containing MPs (MP+) or plasma depleted from MPs (MP-) pellet was added as well as 5 µL lipopolysaccharide (LPS) (1 ng/mL; Sigma-Aldrich, Steinheim, Germany) and incubated at 5% CO2 at 37°C for 24 h. In addition, whole blood was stimulated with LPS (1 ng/mL) only as a positive control (LPS) and with RPMI medium as a negative control (RPMI). In all stimulation assays, similar volumes were maintained. Whole-blood stimulation procedures were identical for control subjects.
After 24 h of incubation, blood samples were centrifuged (600 revolutions/min, 18°C, 10 min). The upper two-thirds of the plasma was collected and stored at -80°C. Interleukin 6 (IL-6), IL-10, and tumour necrosis factor-α (TNF-α) were measured in the
| 67
4
MICROPARTICLES IN TRAUMA
plasma samples by enzyme-linked immuno-sorbent assay, according to instructions of the manufacturer (R&D Systems, Abingdon, United Kingdom).
To examine the cytokine synthesis in plasma from trauma patients com-pared with control subjects, results from the whole-blood stimulation of MP+ and MP- samples were combined. Subsequently, to examine the effect of MPs on the cytokine synthesis in trauma patients or control subjects, MP+ samples were compared with MP- samples.
Number and origin of MPsFlow cytometry with cell-specific markers was used to determine the origin of MPs. Fluorescein isothiocyanate (FITC)-labelled CD144 (Enzo Life Science, Farmingdale, NY) was used to determine endothelial-derived MP, FITC-labelled anti-CD235a (Dako, Glostrup, Denmark) for MP derived from erythrocytes, phycoerythrin-labeled CD61 (Becton Dickinson, San Jose, Calif) for MP derived from platelets, and FITC-labelled CD62p (Beckman Coulter, Brea, Calif) for MP derived from activated platelets. As negative controls, immunoglobulin G1 (IgG1)-phycoerythrin (Becton Dickinson; control for CD61), IgG1-FITC (Becton Dickinson; control for CD235a and CD62p), and IgG-FITC (Immuno Quality Products, Groningen, The Netherlands; control for CD144-FITC) were used. Thawed plasma from patients and control subjects (5 µL) was added to phosphate-buffered saline/citrate buffer (35 µL) supplied with antibody (5 µL) against a cell-specific antigen. The mixture was incubated for 15 min at room temperature, in the dark. Then, phosphate-buffered saline/citrate buffer (900 µL) was added, and samples were analysed on a FACS (Fluorescence-Assisted Cell Sorting) Calibur (Cellquest version 4.02; Becton Dickinson) for 1 min. The number of MPs per millilitre was calculated with the formula: N * (total volume (950 µL) /volume used by FACS (60 µL)) x (1,000 / 5).
Morphology of MPsThe morphology of MPs was examined by transmission electron microscopy. Size exclusion chromatography was used to isolate MPs from plasma as described before26, and fractions 9 and 10 were used. Then, MPs were stained with anti-CD235a, anti-CD62p, anti-CD61, anti-CD142, anti-CD62p, or anti-CD42b as described before. In addition, MPs were stained with gold-labelled annexin V (gift from Alain Brisson, University of Bordeaux) as described before, but without the use of PPACK27.
Statistical analysisNormality for continuous variables was tested by visual inspection of histograms and by Kolmogorov-Smirnov test. Results are expressed as either mean T SD or as median T interquartile range (IQR), depending on the distribution of the variables. A Student t test was performed when normality assumption was obtained; otherwise, a Mann-Whitney U test was used to test for difference in cytokine synthesis between trauma
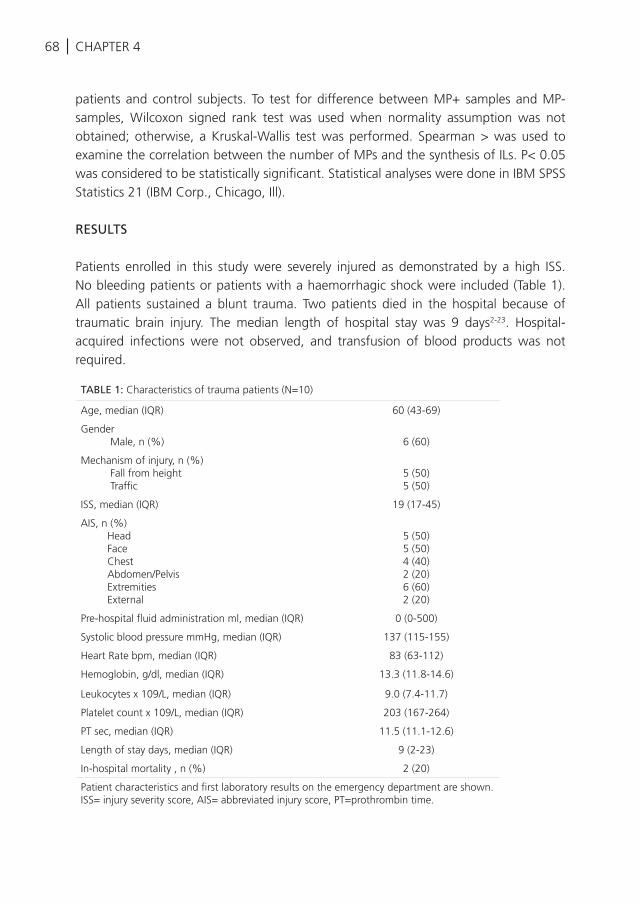
68 | CHAPTER 4
patients and control subjects. To test for difference between MP+ samples and MP- samples, Wilcoxon signed rank test was used when normality assumption was not obtained; otherwise, a Kruskal-Wallis test was performed. Spearman > was used to examine the correlation between the number of MPs and the synthesis of ILs. P< 0.05 was considered to be statistically significant. Statistical analyses were done in IBM SPSS Statistics 21 (IBM Corp., Chicago, Ill).
RESULTS
Patients enrolled in this study were severely injured as demonstrated by a high ISS. No bleeding patients or patients with a haemorrhagic shock were included (Table 1). All patients sustained a blunt trauma. Two patients died in the hospital because of traumatic brain injury. The median length of hospital stay was 9 days2-23. Hospital-acquired infections were not observed, and transfusion of blood products was not required.
TABLE 1: Characteristics of trauma patients (N=10)
Age, median (IQR) 60 (43-69)
Gender Male, n (%) 6 (60)
Mechanism of injury, n (%) Fall from height Traffic
5 (50)5 (50)
ISS, median (IQR) 19 (17-45)
AIS, n (%) Head Face Chest Abdomen/Pelvis Extremities External
5 (50)5 (50)4 (40)2 (20)6 (60)2 (20)
Pre-hospital fluid administration ml, median (IQR) 0 (0-500)
Systolic blood pressure mmHg, median (IQR) 137 (115-155)
Heart Rate bpm, median (IQR) 83 (63-112)
Hemoglobin, g/dl, median (IQR) 13.3 (11.8-14.6)
Leukocytes x 109/L, median (IQR) 9.0 (7.4-11.7)
Platelet count x 109/L, median (IQR) 203 (167-264)
PT sec, median (IQR) 11.5 (11.1-12.6)
Length of stay days, median (IQR) 9 (2-23)
In-hospital mortality , n (%) 2 (20)
Patient characteristics and first laboratory results on the emergency department are shown. ISS= injury severity score, AIS= abbreviated injury score, PT=prothrombin time.
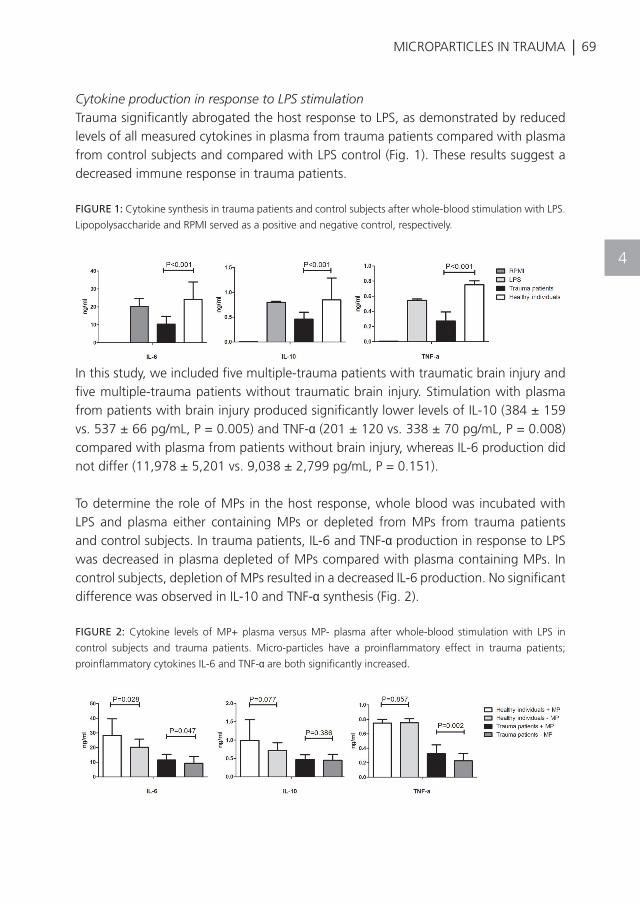
| 69
4
MICROPARTICLES IN TRAUMA
Cytokine production in response to LPS stimulationTrauma significantly abrogated the host response to LPS, as demonstrated by reduced levels of all measured cytokines in plasma from trauma patients compared with plasma from control subjects and compared with LPS control (Fig. 1). These results suggest a decreased immune response in trauma patients.
FIGURE 1: Cytokine synthesis in trauma patients and control subjects after whole-blood stimulation with LPS.
Lipopolysaccharide and RPMI served as a positive and negative control, respectively.
In this study, we included five multiple-trauma patients with traumatic brain injury and five multiple-trauma patients without traumatic brain injury. Stimulation with plasma from patients with brain injury produced significantly lower levels of IL-10 (384 ± 159 vs. 537 ± 66 pg/mL, P = 0.005) and TNF-α (201 ± 120 vs. 338 ± 70 pg/mL, P = 0.008) compared with plasma from patients without brain injury, whereas IL-6 production did not differ (11,978 ± 5,201 vs. 9,038 ± 2,799 pg/mL, P = 0.151).
To determine the role of MPs in the host response, whole blood was incubated with LPS and plasma either containing MPs or depleted from MPs from trauma patients and control subjects. In trauma patients, IL-6 and TNF-α production in response to LPS was decreased in plasma depleted of MPs compared with plasma containing MPs. In control subjects, depletion of MPs resulted in a decreased IL-6 production. No significant difference was observed in IL-10 and TNF-α synthesis (Fig. 2).
FIGURE 2: Cytokine levels of MP+ plasma versus MP- plasma after whole-blood stimulation with LPS in
control subjects and trauma patients. Micro-particles have a proinflammatory effect in trauma patients;
proinflammatory cytokines IL-6 and TNF-α are both significantly increased.
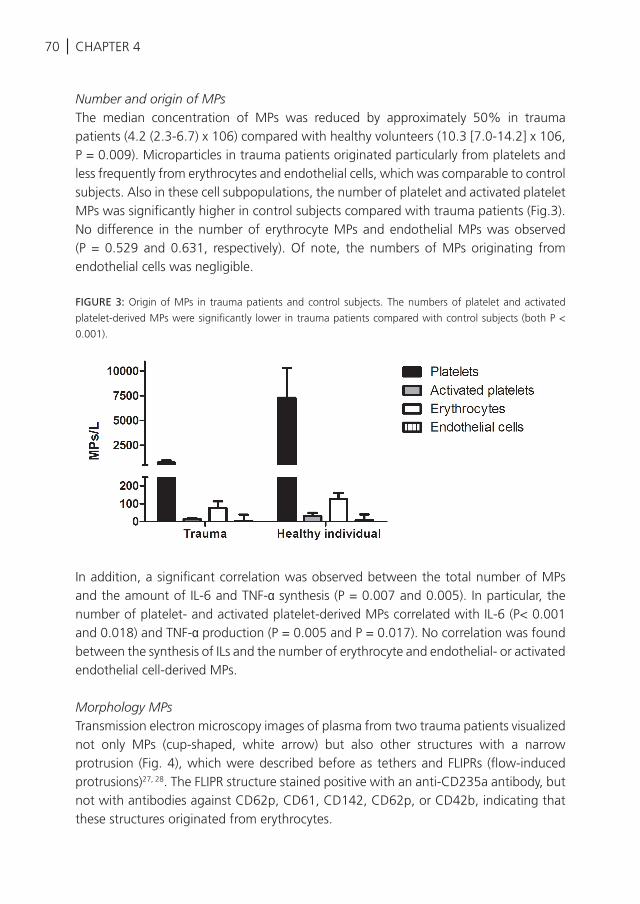
70 | CHAPTER 4
Number and origin of MPsThe median concentration of MPs was reduced by approximately 50% in trauma patients (4.2 (2.3-6.7) x 106) compared with healthy volunteers (10.3 [7.0-14.2] x 106, P = 0.009). Microparticles in trauma patients originated particularly from platelets and less frequently from erythrocytes and endothelial cells, which was comparable to control subjects. Also in these cell subpopulations, the number of platelet and activated platelet MPs was significantly higher in control subjects compared with trauma patients (Fig.3). No difference in the number of erythrocyte MPs and endothelial MPs was observed (P = 0.529 and 0.631, respectively). Of note, the numbers of MPs originating from endothelial cells was negligible.
FIGURE 3: Origin of MPs in trauma patients and control subjects. The numbers of platelet and activated
platelet-derived MPs were significantly lower in trauma patients compared with control subjects (both P <
0.001).
In addition, a significant correlation was observed between the total number of MPs and the amount of IL-6 and TNF-α synthesis (P = 0.007 and 0.005). In particular, the number of platelet- and activated platelet-derived MPs correlated with IL-6 (P< 0.001 and 0.018) and TNF-α production (P = 0.005 and P = 0.017). No correlation was found between the synthesis of ILs and the number of erythrocyte and endothelial- or activated endothelial cell-derived MPs.
Morphology MPsTransmission electron microscopy images of plasma from two trauma patients visualized not only MPs (cup-shaped, white arrow) but also other structures with a narrow protrusion (Fig. 4), which were described before as tethers and FLIPRs (flow-induced protrusions)27, 28. The FLIPR structure stained positive with an anti-CD235a antibody, but not with antibodies against CD62p, CD61, CD142, CD62p, or CD42b, indicating that these structures originated from erythrocytes.
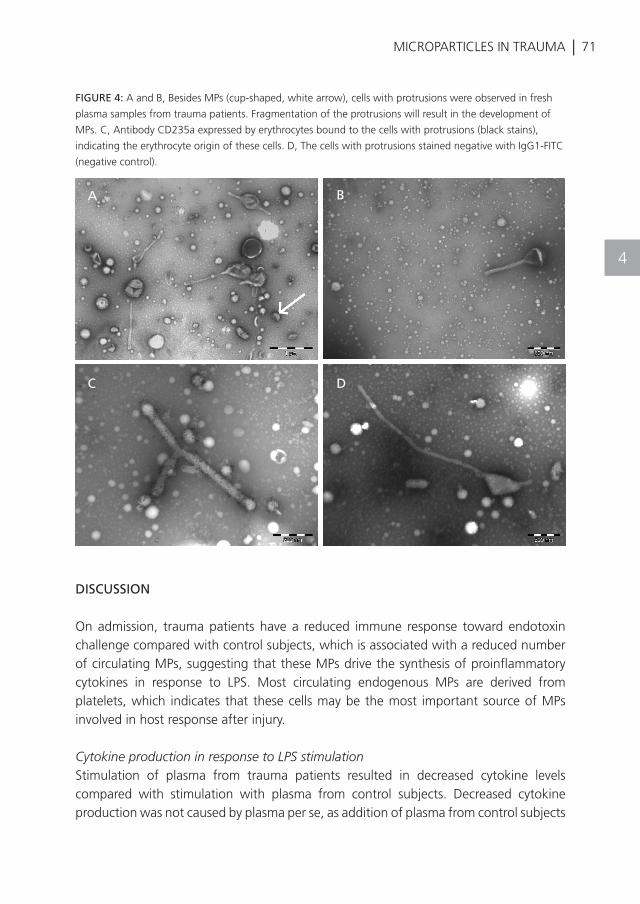
| 71
4
MICROPARTICLES IN TRAUMA
FIGURE 4: A and B, Besides MPs (cup-shaped, white arrow), cells with protrusions were observed in fresh
plasma samples from trauma patients. Fragmentation of the protrusions will result in the development of
MPs. C, Antibody CD235a expressed by erythrocytes bound to the cells with protrusions (black stains),
indicating the erythrocyte origin of these cells. D, The cells with protrusions stained negative with IgG1-FITC
(negative control).
DISCUSSION
On admission, trauma patients have a reduced immune response toward endotoxin challenge compared with control subjects, which is associated with a reduced number of circulating MPs, suggesting that these MPs drive the synthesis of proinflammatory cytokines in response to LPS. Most circulating endogenous MPs are derived from platelets, which indicates that these cells may be the most important source of MPs involved in host response after injury.
Cytokine production in response to LPS stimulationStimulation of plasma from trauma patients resulted in decreased cytokine levels compared with stimulation with plasma from control subjects. Decreased cytokine production was not caused by plasma per se, as addition of plasma from control subjects
A B
C D

72 | CHAPTER 4
to the assay rather seems to enhance cellular response. A reduced host response in trauma has been found before13. It is hypothesized that a reduced cellular immune response in trauma patients toward endotoxin challenge is caused by exhaustion of immune cells, termed immunoparalysis. This may hold in particular for traumatic brain injury patients. It is known that in these patients the systemic innate immune response is diminished14, 29, 30. This is confirmed by our results, which show that the host response is even more suppressed in patients with traumatic brain injury.
Mediators of the host response are unknown. We show here that in trauma, the immune response to LPS is, at least in part, mediated by endogenous MPs. This is in line with previous studies, in which it has been proposed that MPs derived from leukocytes circulate in low levels in control subjects and become up-regulated after systematic inflammation or in sepsis. Microparticles activate circulating cells and stimulate production of proinflammatory cytokines such as IL-1ß, IL-6, TNF-α, and IL-87,19-21,24,25,28,31. Of interest, our data suggest that the stimulating effect of MPs on immune cells is a physiological response, given that MPs derived from trauma patients as well as from control subjects stimulate cytokine production. Whether a persistent depletion of MPs contributes to an increased risk of nosocomial infection following trauma remains to be determined.
Number and origin of MPsThe number of circulating MPs in trauma was significantly decreased compared with control subjects. This is in contrast to previous studies, in which a higher number of circulating MPs was observed in trauma patients with SIRS compared with control subjects23, 24. A possible explanation for the decreased number of MPs in trauma patients may be activation of cells by MPs, resulting in the formation of complexes be-tween MPs and other cells. Complexes will not be diagnosed as MPs by flow cytometry, which may be a limitation of our study. Furthermore, the timing of blood draw in previous studies varied between 1 and 5 hospital days. As the turnover of MPs is highly dynamic, particularly following trauma, this may account for contrasting results between studies23-25.
Most MPs in the severely injured trauma patients included in this study were derived from platelets. This is similar to previous studies in trauma patients with SIRS or coagulopathy in which MPs also originated from platelets23, 32. Together, this suggests that platelet MPs may be the most important source of MPs involved in initiating an inflammatory host response after injury. Recently, in an ex vivo study, it was shown that activated platelets form protrusions (FLIPRs), which fragment resulting in platelet-derived MPs. These MPs could subsequently activate monocytes and neutrophils by
| 73
4
MICROPARTICLES IN TRAUMA
upregulation of adhesion molecules on the surface of endothelial cells, mediating a proinflammatory response28,33. In line with this, the number of platelet-derived MPs correlated with the host response in this study. Follow-up studies are required to investigate the immunoactivity of platelets following trauma in more detail.
Given that patients sustained severe trauma with tissue injury, we expected to also find endothelial-derived MPs. However, the numbers of endothelial-derived MPs were low. An explanation may be that patients in this study were not bleeding, and hence endothelium was not disrupted. It is possible that bleeding patients display another profile of endogenous MPs.
Morphology MPsWhen we investigated MP morphology in fresh plasma samples from trauma patients, we detected large numbers of cells with protrusions. These cells were not present in control subjects. The cells with protrusions in this study were derived from erythrocytes and could fragment into and thus are precursors of erythrocyte-derived MPs. We did not find platelet-derived protrusions at this time point. The consequence of finding large numbers of cells with protrusions cannot be dissected from our study, which is a limitation. We hypothesize that the development of an erythrocyte-derived MP storm may occur in time, with subsequent activation of leukocytes and monocytes with ensuing progression toward a proinflammatory response. However, this remains to be determined, as we did not measure host response at different time points.
Another limitation of this study is that flow cytometry detects only a minor fraction of all circulating extracellular vesicles such as MPs34. However, currently, flow cytometry is the standard method to detect single MPs. More sensitive technology may improve detection limits. Furthermore, we have investigated the role of MPs in mediating the immune response following trauma in a selected group of blunt trauma patients as patients had significant injury, but patients were neither in shock nor bleeding.
In conclusion, severely injured trauma patients have a reduced immune response toward endotoxin challenge on ad-mission, which is strongly associated with decreased levels of circulating MPs. In these patients, MPs are able to drive the synthesis of proinflammatory cytokines and could abrogate the immunoparalysis. Most MPs are derived from platelets, which indicates that these cells may be the most important source of MPs involved in the host response after injury.
74 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
Sauaia A, Moore FA, Moore EE, Moser KS,
Brennan R, Read RA, Pons PT: Epidemiology
of trauma deaths: a reassessment. J
Trauma:38(2):185-93,1995.
DeLong WG, Jr., Born CT: Cytokines in
patients with polytrauma. Clin Orthop Relat
Res:(422):57-65,2004.
Pape HC, Remmers D, Grotz M, Schedel I,
von GS, Oberbeck R, Dahlweit M, Tscherne H:
Levels of antibodies to endotoxin and cytokine
release in patients with severe trauma: does
posttraumatic dysergy contribute to organ
failure? J Trauma:46(5):907-13,1999.
Pape HC, Tsukamoto T, Kobbe P, Tarkin I,
Katsoulis S, Peitzman A: Assessment of the
clinical course with inflammatory parameters.
Injury:38(12):1358-64,2007.
Tschoeke SK, Ertel W: Immunoparalysis after
multiple trauma. Injury:38(12):1346-57,2007.
Flohe SB, Flohe S, Schade FU: Invited review:
deterioration of the immune system after
trauma: signals and cellular mechanisms.
Innate Immun:14(6):333-44,2008.
Reid VL, Webster NR: Role of microparticles in
sepsis. Br J Anaesth:109(4):503-13,2012.
Manson J, Thiemermann C, Brohi K: Trauma
alarmins as activators of damage-induced
inflammation. Br J Surg:99 Suppl 1:12-
20,2012.
Gando S, Kameue T, Nanzaki S, Hayakawa
T, Nakanishi Y: Participation of tissue
factor and thrombin in posttraumatic
systemic inflammatory syndrome. Crit Care
Med:25(11):1820-6,1997.
Gentile LF, Cuenca AG, Efron PA, Ang D,
Bihorac A, McKinley BA, Moldawer LL,
Moore FA: Persistent inflammation and
immunosuppression: a common syndrome
and new horizon for surgical intensive care.
J Trauma Acute Care Surg:72(6):1491-
501,2012.
Rittirsch D, Redl H, Huber-Lang M: Role of
complement in multiorgan failure. Clin Dev
Immunol:2012:962927,2012.
Faist E, Storck M, Hultner L, Redl H, Ertel W,
Walz A, Schildberg FW: Functional analysis
of monocyte activity through synthesis
patterns of proinflammatory cytokines and
neopterin in patients in surgical intensive care.
Surgery:112(3):562-72,1992.
Kirchhoff C, Biberthaler P, Mutschler WE, Faist
E, Jochum M, Zedler S: Early down-regulation
of the pro-inflammatory potential of
monocytes is correlated to organ dysfunction
in patients after severe multiple injury: a
cohort study. Crit Care:13(3):R88,2009.
Schwulst SJ, Trahanas DM, Saber R, Perlman
H: Traumatic brain injury-induced alterations
in peripheral immunity. J Trauma Acute Care
Surg:75(5):780-8,2013.
Hietbrink F, Koenderman L, Althuizen M, Pillay
J, Kamp V, Leenen LP: Kinetics of the innate
immune response after trauma: implications
for the development of late onset sepsis.
Shock:40(1):21-7,2013.
DiPiro JT, Howdieshell TR, Goddard JK,
Callaway DB, Hamilton RG, Mansberger AR,
Jr.: Association of interleukin-4 plasma levels
with traumatic injury and clinical course. Arch
Surg:130(11):1159-62,1995.
Keel M, Trentz O: Pathophysiology of
polytrauma. Injury:36(6):691-709,2005.
Lynch SF, Ludlam CA: Plasma
microparticles and vascular disorders. Br J
Haematol:137(1):36-48,2007.
Adib-Conquy M, Moine P, Asehnoune K,
Edouard A, Espevik T, Miyake K, Werts C,
Cavaillon JM: Toll-like receptor-mediated tumor
necrosis factor and interleukin-10 production
differ during systemic inflammation. Am J
Respir Crit Care Med:168(2):158-64,2003.
Thomas LM, Salter RD: Activation of
macrophages by P2X7-induced microvesicles
from myeloid cells is mediated by
phospholipids and is partially dependent on
TLR4. J Immunol:185(6):3740-9,2010.
Prakash PS, Caldwell CC, Lentsch AB, Pritts
TA, Robinson BR: Human microparticles
CHAPTER 4
| 75
REFERENCES
MICROPARTICLES IN TRAUMA
22
23
24
25
26
27
28
29
30
31
32
33
34
generated during sepsis in patients with
critical illness are neutrophil-derived and
modulate the immune response. J Trauma
Acute Care Surg:73(2):401-6,2012.
Meziani F, Delabranche X, Asfar P, Toti
F: Bench-to-bedside review: circulating
microparticles--a new player in sepsis? Crit
Care:14(5):236,2010.
Ogura H, Kawasaki T, Tanaka H, Koh T,
Tanaka R, Ozeki Y, Hosotsubo H, Kuwagata
Y, Shimazu T, Sugimoto H: Activated platelets
enhance microparticle formation and platelet-
leukocyte interaction in severe trauma and
sepsis. J Trauma:50(5):801-9,2001.
Ogura H, Tanaka H, Koh T, Fujita K, Fujimi
S, Nakamori Y, Hosotsubo H, Kuwagata Y,
Shimazu T, Sugimoto H: Enhanced production
of endothelial microparticles with increased
binding to leukocytes in patients with severe
systemic inflammatory response syndrome. J
Trauma:56(4):823-30,2004.
Fujimi S, Ogura H, Tanaka H, Koh T, Hosotsubo
H, Nakamori Y, Kuwagata Y, Shimazu T,
Sugimoto H: Increased production of leukocyte
microparticles with enhanced expression
of adhesion molecules from activated
polymorphonuclear leukocytes in severely
injured patients. J Trauma:54(1):114-9,2003.
Boing AN, van der Pol E, Grootemaat AE,
Coumans FA, Sturk A, Nieuwland R: Single-
step isolation of extracellular vesicles by
size-exclusion chromatography. J Extracell
Vesicles:3,2014.
Arraud N, Linares R, Tan S, Gounou
C, Pasquet JM, Mornet S, Brisson AR:
Extracellular vesicles from blood plasma:
determination of their morphology, size,
phenotype and concentration. J Thromb
Haemost:12(5):614-27,2014.
Tersteeg C, Heijnen HF, Eckly A, Pasterkamp
G, Urbanus RT, Maas C, Hoefer IE, Nieuwland
R, Farndale RW, Gachet C, de Groot PG, Roest
M: FLow-Induced PRotrusions (FLIPRs): A
Platelet-Derived Platform for the Retrieval of
Microparticles by Monocytes and Neutrophils.
Circ Res:2014.
Griffin GD: The injured brain: TBI, mTBI, the
immune system, and infection: connecting
the dots. Mil Med:176(4):364-8,2011.
Vermeij JD, Aslami H, Fluiter K, Roelofs JJ, van
den Bergh WM, Juffermans NP, Schultz MJ,
van der Sluijs K, van de Beek D, van Westerloo
DJ: Traumatic brain injury in rats induces lung
injury and systemic immune suppression. J
Neurotrauma:2013.
Deng ZB, Poliakov A, Hardy RW, Clements
R, Liu C, Liu Y, Wang J, Xiang X, Zhang S,
Zhuang X, Shah SV, Sun D, Michalek S, Grizzle
WE, Garvey T, Mobley J, Zhang HG: Adipose
tissue exosome-like vesicles mediate activation
of macrophage-induced insulin resistance.
Diabetes:58(11):2498-505,2009.
Matijevic N, Wang YW, Wade CE, Holcomb
JB, Cotton BA, Schreiber MA, Muskat P,
Fox EE, Del Junco DJ, Cardenas JC, Rahbar
MH, Cohen MJ: Cellular microparticle and
thrombogram phenotypes in the Prospective
Observational Multicenter Major Trauma
Transfusion (PROMMTT) study: correlation
with coagulopathy. Thromb Res:134(3):652-
8,2014.
Barry OP, Pratico D, Savani RC, FitzGerald
GA: Modulation of monocyte-endothelial cell
interactions by platelet microparticles. J Clin
Invest:102(1):136-44,1998.
van der Pol E, Coumans F, Varga Z, Krumrey
M, Nieuwland R: Innovation in detection
of microparticles and exosomes. J Thromb
Haemost:11 Suppl 1:36-45,2013.
4
K. Balvers, M.R. Wirtz, S. van DierenJ.C. Goslings, N.P. Juffermans
Frontiers in Medicine 2015
RISK FACTORS RELATED TO TIC AND RESUSCITATION STRATEGIES FOR THE DEVELOPMENT OF MULTIPLE
ORGAN FAILURE IN SEVERELY INJURED TRAUMA PATIENTS
5
78 | CHAPTER 5
ABSTRACT
Introduction: Both trauma-induced coagulopathy (TIC) and transfusion strategies influence early outcome in haemorrhagic trauma patients. Their impact on late outcome is less well characterized. This study systematically reviews risk factors for TIC- and transfusion-associated multiple organ failure (MOF) in severely injured trauma patients.
Methods: A systematic search was conducted in PubMed and Embase. Studies published from 1986 to 2013 on adult trauma patients with an Injury Severity Score ≥16, investigating TIC or transfusion strategies with MOF as primary or secondary outcome, were eligible for inclusion. Results of the included studies were evaluated with meta-analyses of pooled data.
Results: In total, 50 studies were included with a total sample size of 63,586 patients. Due to heterogeneity of the study populations and outcome measures, results from 7 studies allowed for pooling of data. Risk factors for TIC-associated MOF were hypocoagulopathy, haemorrhagic shock, activated protein C, increased histone levels, and increased levels of markers of fibrinolysis on admission. After at least 24 h after admission, the occurrence of thromboembolic events was associated with MOF. Risk factors for transfusion-associated MOF were the administration of fluids and red blood cell units within 24 h post-injury, the age of red blood cells (>14 days) and a ratio of FFP:RBC ≥ 1:1 (OR 1.11, 95% CI 1.04–1.19).
Conclusion: Risk factors for TIC-associated MOF in severely injured trauma patients are early hypocoagulopathy and haemorrhagic shock, while a hypercoagulable state with the occurrence of thromboembolic events later in the course of trauma predisposes to MOF.
| 79RISK FACTORS FOR MOF
5
INTRODUCTION
Despite advances in trauma care, multiple organ failure (MOF) still remains one of the leading causes of late mortality (occurring after more than 3 days) in trauma patients1,2. The incidence of MOF in severely injured trauma patients ranges from 15% up until 40%3–6, with an associated mortality rate that varies between 24%3 and 51%6. Even though MOF-related mortality has been shown to decrease over the last decades2,6, mortality is still 10 times higher in patients with MOF compared to patients without MOF4,5.
Over the last decade, trauma-induced coagulopathy (TIC) is increasingly recognized to contribute to adverse early outcome in trauma patients7–13. In recognition of that, transfusion strategies have changed toward more and earlier administration of plasma. This has led to a shift in the ratio of RBC:FFP to 1:1. Furthermore, fluid resuscitation with crystalloids has evolved from aggressive therapy to a minimal amount of crystalloid administration. More and earlier administration of plasma, combined with a restriction of crystalloid administration, has showed to reduce early mortality14–16. However, the impact of both TIC and changing transfusion strategies on the occurrence of MOF has not been systematically reviewed before. Therefore, the aim of this study was to summarize risk factors for TIC- and transfusion-associated MOF in severely injured trauma patients.
MATERIALS AND METHODS
The present study was reported according to the PRISMA guidelines (preferred reporting items for systematic reviews and meta-analyses)17.
Study selectionAn electronic search was conducted in PubMed and Embase for articles published from 1986 to 2013. In addition, we searched for ongoing trials on www.controlled-trials.com and www.clinicaltrials.gov.
The following subject headings and free text words were used: (“Blood Coagulation Disorders”[Mesh] OR “Blood Coagulation”[Mesh] OR Coagulation[tiab] OR coagulopa-thy[tiab] OR “Fibrinolysis”[Mesh] OR Fibrinolysis[tiab] OR hypofibrinolysis[tiab] OR hyperfibrinolysis[tiab]) OR (“Blood Transfusion”[Mesh] OR Transfusion[tiab] OR “Transfusion Med-icine”[Mesh] OR “Erythrocyte Transfusion”[Mesh] OR “Blood Component Transfusion”[Mesh]) AND (“Multiple Organ Fail-ure”[Mesh] OR multiple organ failure*[tiab] OR MOF[tiab] OR (infection*[tiab] AND trauma[tiab])) AND

80 | CHAPTER 5
(“Multiple Trauma”[Mesh] OR multiple trauma[tiab] OR “Wounds and Injuries”[Mesh] OR “Injury Severity Score”[Mesh] OR Injury Severity Score[tiab] OR ISS[tiab] (Table S2 in Supplementary Material).
Target population were trauma patients who suffered blunt or penetrating trauma, with a mean injury severity score (ISS) of ≥16 and an age of ≥16 years. Randomized controlled trials (RCTs) and observational studies investigating TIC or transfusion strategies with MOF as primary or secondary outcome were eligible for inclusion. Studies, which focused on patients with isolated traumatic brain injury or burn injury, were excluded. Both prospective and retrospective studies were included. Reviews, correspondences, case reports, expert opinions, and editorials were excluded. The search was conducted by two independent researchers (Kirsten Balvers and Mathijs R. Wirtz). Any discrepancies in the included studies were resolved by discussion between the reviewers. If necessary, an independent third reviewer was consulted. Only articles defining MOF according to the definition of the Denver18, Marshall18, 19, or SOFA20 score were included in this review. A Denver score of more than 3 and a Marshall score of more than 5, both for at least two consecutive days, were used to define MOF. Furthermore, MOF according to the SOFA score was defined as the simultaneous failure of two or more organ systems. Organ failure was defined as a total of more than two points in a single organ. Language was limited to English, Dutch, or German. We reviewed the bibliographies of the eligible studies for citations of additional suitable studies.
Data synthesisPrimary outcomes were risk factors for TIC- and transfusion-associated MOF. Since most of the studies in this field are observational studies, we performed a quality assessment according to the Newcastle-Ottawa Scale21. Characteristics of the studies examined included comparability of the study groups, methods used to select study participants and determination of outcome variables. The quality of selection of patients in the included studies was rated as good if they included severely injured trauma patients and the control group was drawn from the same community as the exposed cohort. The assessment of comparability of the studies was based on the design and/or analysis used in the studies. Quality of outcome variables was determined by follow-up period and <10% of patients lost-to-follow-up. The Cochrane Collaboration’s tool for assessing the risk of bias was used to assess the quality of RCTs22. This tool was used to evaluate RCTs on seven specific domains (sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias). If the results of studies were contradicting, the quality assessment was used to grade conclusions.

| 81RISK FACTORS FOR MOF
Review Manager (RevMan 5, The Nordic Cochrane Centre) was used to combine findings of studies in a meta-analysis. Studies were pooled if homogeneity was considered by assessing study population, intervention and outcome. RevMan was used to deter-mine homogeneity by the inverse variance method for a random or fixed effects model. If homogeneity was not obtained studies were excluded from meta-analysis. Heterogeneity was expressed by I2. An I2 of >75% was considered as substantial heterogeneity. Meta-analysis was performed on observational studies and RCTs, in which data from observational studies and RCTs were not combined in the same meta-analysis. For the outcome of interest, risk ratios and 95% confidence intervals were used.
RESULTS
We identified 476 articles (PubMed 320, Embase 156) meeting the inclusion criteria. Of these, seven duplicates were removed. Reviewing of the bibliographies resulted in 11 additional articles. The full texts of 114 articles were assessed for eligibility. An additional 64 reviews were excluded, bringing the total on 50 included articles with a total sample size of 63,586 patients (Figure 1). Of the 50 included studies, 46 studies were observational cohort studies and 4 were RCTs. The observational studies included 15 retrospective and 31 prospective studies. Sample size in these studies varied between 19 and 20,288 patients with a median of 384 (IQR 135–1217) patients. Two studies included a heterogeneous population of intensive care patients, all other studies were restricted to trauma patients. The score of the included studies on the Newcastle-Ottawa scale ranged from 6 to 8 with a median of 7. The score of the Cochrane Collaboration’s tool for assessing the risk of bias ranged from 8 to 9 (Tables 1 and 2; Table S1 in Appendixl).
Risk factors for TIC-associated MOFEighteen studies reported the effect of TIC on the development of MOF in trauma patients (Table 1). The presence of hypocoagulopathy on admission to the Emergency Department (ED) was an independent risk factor for MOF (26, 30, 33, 35–39); however, studies could not be pooled due to substantial heterogeneity (I2 = 90%, Figure 2). Hypocoagulopathy was defined by prolongation of coagulation parameters including PTT, INR, and APTT and a decreased platelet count 26. Four studies reported a decreased platelet count as an independent risk factor23, 26, 41, 72. Of note, hypocoagulopathy was rare in patients without persisting shock73. Other risk factors for TIC-associated MOF were activation of protein C, increased levels of fibrinolytic markers27, 36–39, and increased levels of extracellular histones37. Of note, these risk factors were reported in small study numbers.
5
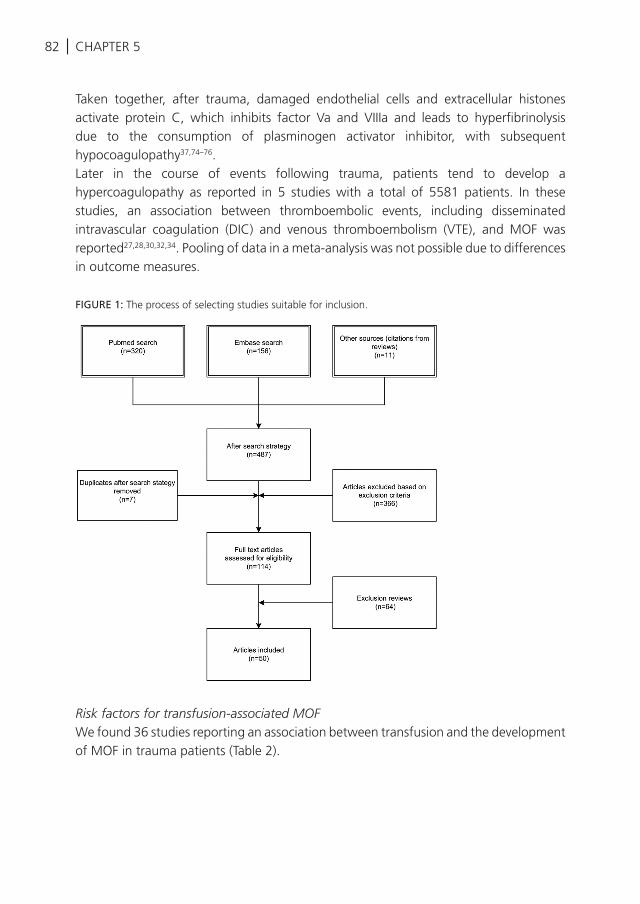
82 | CHAPTER 5
Taken together, after trauma, damaged endothelial cells and extracellular histones activate protein C, which inhibits factor Va and VIIIa and leads to hyperfibrinolysis due to the consumption of plasminogen activator inhibitor, with subsequent hypocoagulopathy37,74–76.Later in the course of events following trauma, patients tend to develop a hypercoagulopathy as reported in 5 studies with a total of 5581 patients. In these studies, an association between thromboembolic events, including disseminated intravascular coagulation (DIC) and venous thromboembolism (VTE), and MOF was reported27,28,30,32,34. Pooling of data in a meta-analysis was not possible due to differences in outcome measures.
FIGURE 1: The process of selecting studies suitable for inclusion.
Risk factors for transfusion-associated MOFWe found 36 studies reporting an association between transfusion and the development of MOF in trauma patients (Table 2).
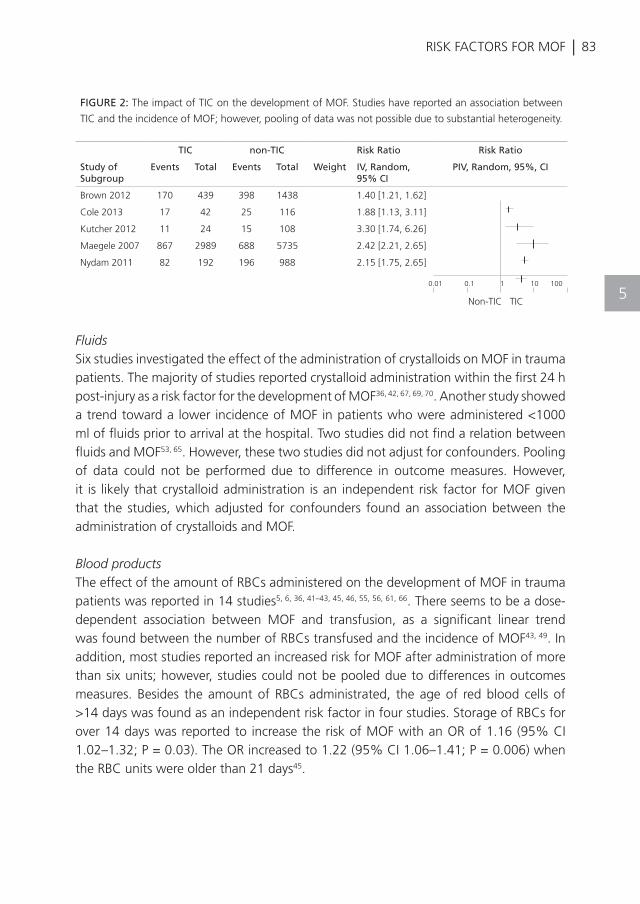
| 83RISK FACTORS FOR MOF
FluidsSix studies investigated the effect of the administration of crystalloids on MOF in trauma patients. The majority of studies reported crystalloid administration within the first 24 h post-injury as a risk factor for the development of MOF36, 42, 67, 69, 70. Another study showed a trend toward a lower incidence of MOF in patients who were administered <1000 ml of fluids prior to arrival at the hospital. Two studies did not find a relation between fluids and MOF53, 65. However, these two studies did not adjust for confounders. Pooling of data could not be performed due to difference in outcome measures. However, it is likely that crystalloid administration is an independent risk factor for MOF given that the studies, which adjusted for confounders found an association between the administration of crystalloids and MOF.
Blood productsThe effect of the amount of RBCs administered on the development of MOF in trauma patients was reported in 14 studies5, 6, 36, 41–43, 45, 46, 55, 56, 61, 66. There seems to be a dose-dependent association between MOF and transfusion, as a significant linear trend was found between the number of RBCs transfused and the incidence of MOF43, 49. In addition, most studies reported an increased risk for MOF after administration of more than six units; however, studies could not be pooled due to differences in outcomes measures. Besides the amount of RBCs administrated, the age of red blood cells of >14 days was found as an independent risk factor in four studies. Storage of RBCs for over 14 days was reported to increase the risk of MOF with an OR of 1.16 (95% CI 1.02–1.32; P = 0.03). The OR increased to 1.22 (95% CI 1.06–1.41; P = 0.006) when the RBC units were older than 21 days45.
FIGURE 2: The impact of TIC on the development of MOF. Studies have reported an association between
TIC and the incidence of MOF; however, pooling of data was not possible due to substantial heterogeneity.
TIC non-TIC Risk Ratio Risk Ratio
Study of Subgroup
Events Total Events Total Weight IV, Random, 95% CI
PIV, Random, 95%, CI
Brown 2012 170 439 398 1438 1.40 [1.21, 1.62]
Cole 2013 17 42 25 116 1.88 [1.13, 3.11]
Kutcher 2012 11 24 15 108 3.30 [1.74, 6.26]
Maegele 2007 867 2989 688 5735 2.42 [2.21, 2.65]
Nydam 2011 82 192 196 988 2.15 [1.75, 2.65]
0.01 0.1 1 10 100
Non-TIC TIC5
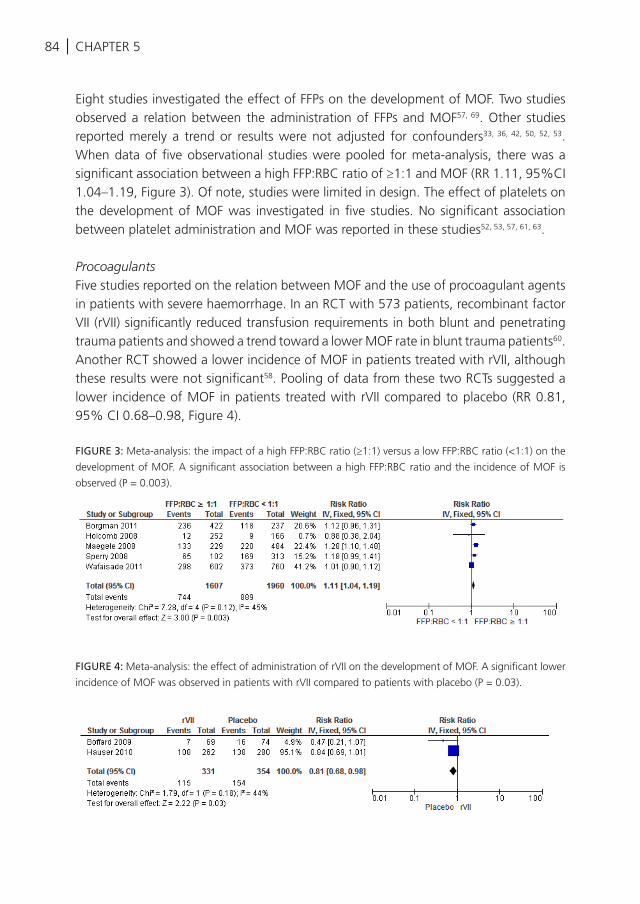
84 | CHAPTER 5
Eight studies investigated the effect of FFPs on the development of MOF. Two studies observed a relation between the administration of FFPs and MOF57, 69. Other studies reported merely a trend or results were not adjusted for confounders33, 36, 42, 50, 52, 53. When data of five observational studies were pooled for meta-analysis, there was a significant association between a high FFP:RBC ratio of ≥1:1 and MOF (RR 1.11, 95%CI 1.04–1.19, Figure 3). Of note, studies were limited in design. The effect of platelets on the development of MOF was investigated in five studies. No significant association between platelet administration and MOF was reported in these studies52, 53, 57, 61, 63.
ProcoagulantsFive studies reported on the relation between MOF and the use of procoagulant agents in patients with severe haemorrhage. In an RCT with 573 patients, recombinant factor VII (rVII) significantly reduced transfusion requirements in both blunt and penetrating trauma patients and showed a trend toward a lower MOF rate in blunt trauma patients60. Another RCT showed a lower incidence of MOF in patients treated with rVII, although these results were not significant58. Pooling of data from these two RCTs suggested a lower incidence of MOF in patients treated with rVII compared to placebo (RR 0.81, 95% CI 0.68–0.98, Figure 4).
FIGURE 3: Meta-analysis: the impact of a high FFP:RBC ratio (≥1:1) versus a low FFP:RBC ratio (<1:1) on the
development of MOF. A significant association between a high FFP:RBC ratio and the incidence of MOF is
observed (P = 0.003).
FIGURE 4: Meta-analysis: the effect of administration of rVII on the development of MOF. A significant lower
incidence of MOF was observed in patients with rVII compared to patients with placebo (P = 0.03).
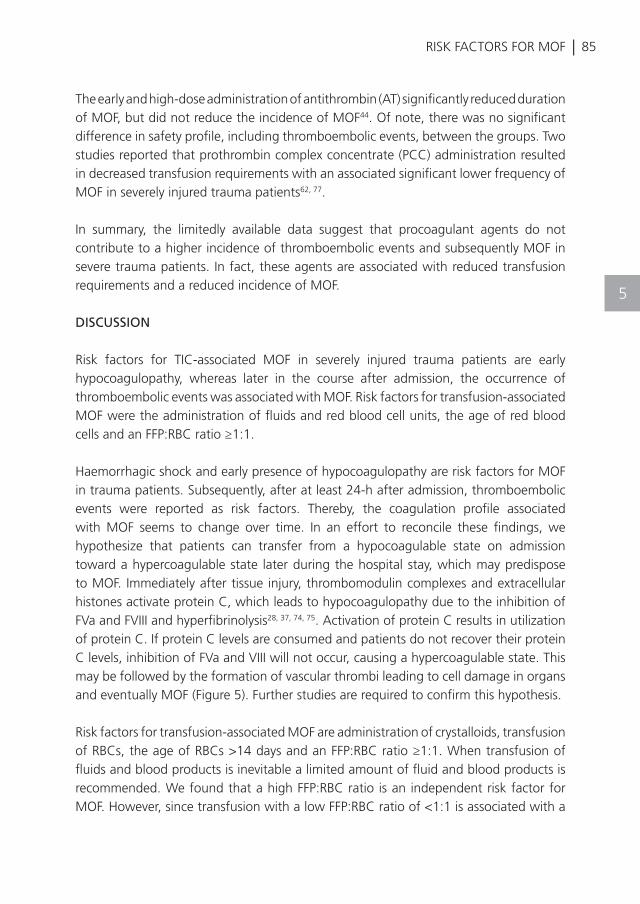
| 85RISK FACTORS FOR MOF
The early and high-dose administration of antithrombin (AT) significantly reduced duration of MOF, but did not reduce the incidence of MOF44. Of note, there was no significant difference in safety profile, including thromboembolic events, between the groups. Two studies reported that prothrombin complex concentrate (PCC) administration resulted in decreased transfusion requirements with an associated significant lower frequency of MOF in severely injured trauma patients62, 77.
In summary, the limitedly available data suggest that procoagulant agents do not contribute to a higher incidence of thromboembolic events and subsequently MOF in severe trauma patients. In fact, these agents are associated with reduced transfusion requirements and a reduced incidence of MOF.
DISCUSSION
Risk factors for TIC-associated MOF in severely injured trauma patients are early hypocoagulopathy, whereas later in the course after admission, the occurrence of thromboembolic events was associated with MOF. Risk factors for transfusion-associated MOF were the administration of fluids and red blood cell units, the age of red blood cells and an FFP:RBC ratio ≥1:1.
Haemorrhagic shock and early presence of hypocoagulopathy are risk factors for MOF in trauma patients. Subsequently, after at least 24-h after admission, thromboembolic events were reported as risk factors. Thereby, the coagulation profile associated with MOF seems to change over time. In an effort to reconcile these findings, we hypothesize that patients can transfer from a hypocoagulable state on admission toward a hypercoagulable state later during the hospital stay, which may predispose to MOF. Immediately after tissue injury, thrombomodulin complexes and extracellular histones activate protein C, which leads to hypocoagulopathy due to the inhibition of FVa and FVIII and hyperfibrinolysis28, 37, 74, 75. Activation of protein C results in utilization of protein C. If protein C levels are consumed and patients do not recover their protein C levels, inhibition of FVa and VIII will not occur, causing a hypercoagulable state. This may be followed by the formation of vascular thrombi leading to cell damage in organs and eventually MOF (Figure 5). Further studies are required to confirm this hypothesis.
Risk factors for transfusion-associated MOF are administration of crystalloids, transfusion of RBCs, the age of RBCs >14 days and an FFP:RBC ratio ≥1:1. When transfusion of fluids and blood products is inevitable a limited amount of fluid and blood products is recommended. We found that a high FFP:RBC ratio is an independent risk factor for MOF. However, since transfusion with a low FFP:RBC ratio of <1:1 is associated with a
5
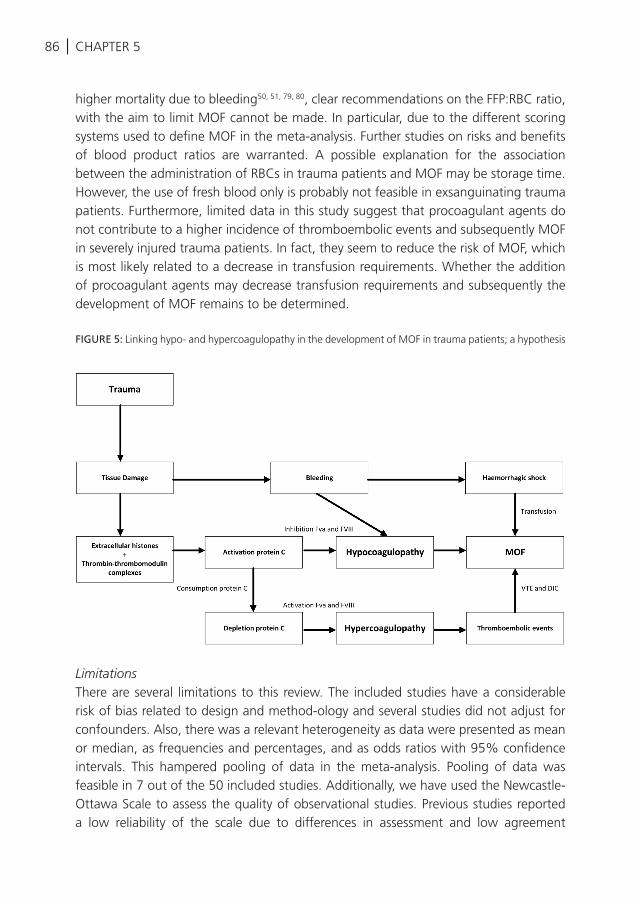
86 | CHAPTER 5
higher mortality due to bleeding50, 51, 79, 80, clear recommendations on the FFP:RBC ratio, with the aim to limit MOF cannot be made. In particular, due to the different scoring systems used to define MOF in the meta-analysis. Further studies on risks and benefits of blood product ratios are warranted. A possible explanation for the association between the administration of RBCs in trauma patients and MOF may be storage time. However, the use of fresh blood only is probably not feasible in exsanguinating trauma patients. Furthermore, limited data in this study suggest that procoagulant agents do not contribute to a higher incidence of thromboembolic events and subsequently MOF in severely injured trauma patients. In fact, they seem to reduce the risk of MOF, which is most likely related to a decrease in transfusion requirements. Whether the addition of procoagulant agents may decrease transfusion requirements and subsequently the development of MOF remains to be determined.
FIGURE 5: Linking hypo- and hypercoagulopathy in the development of MOF in trauma patients; a hypothesis
LimitationsThere are several limitations to this review. The included studies have a considerable risk of bias related to design and method-ology and several studies did not adjust for confounders. Also, there was a relevant heterogeneity as data were presented as mean or median, as frequencies and percentages, and as odds ratios with 95% confidence intervals. This hampered pooling of data in the meta-analysis. Pooling of data was feasible in 7 out of the 50 included studies. Additionally, we have used the Newcastle-Ottawa Scale to assess the quality of observational studies. Previous studies reported a low reliability of the scale due to differences in assessment and low agreement
| 87RISK FACTORS FOR MOF
between reviewers, which is a limitation of the scale and subsequently of this study81,82. However, despite these limitations, the Cochrane Collaboration recommends the Newcastle-Ottawa scale as the most useful tool for assessing the risk of bias in non-RCTs83. Furthermore, there is a lack of a uniform definition of MOF. The use of different scores of MOF hampers interpretation of the results of the meta-analyses and therefore no firm conclusions can be drawn. Additional studies are required to confirm the results of this study.
ConclusionIdentifying patients at high risk for MOF may guide the need for monitoring of organ failure and may provide avoidance of therapy, which can aggravate organ failure. Early hypocoagulopathy and shock are risk factors for TIC-associated MOF in severely injured trauma patients. Later in the course of trauma, a hypercoagulable state with the occurrence of thromboembolic events predisposes to MOF. Risk factors for transfusion-associated MOF include the administration of crystalloids and red blood cells and a prolonged storage time of red blood cells. However, pooling of data was hampered by heterogeneity of the study populations and out-come measures. Future prospective studies investigating TIC- and transfusion-associated risk factors on late outcome are required.
5
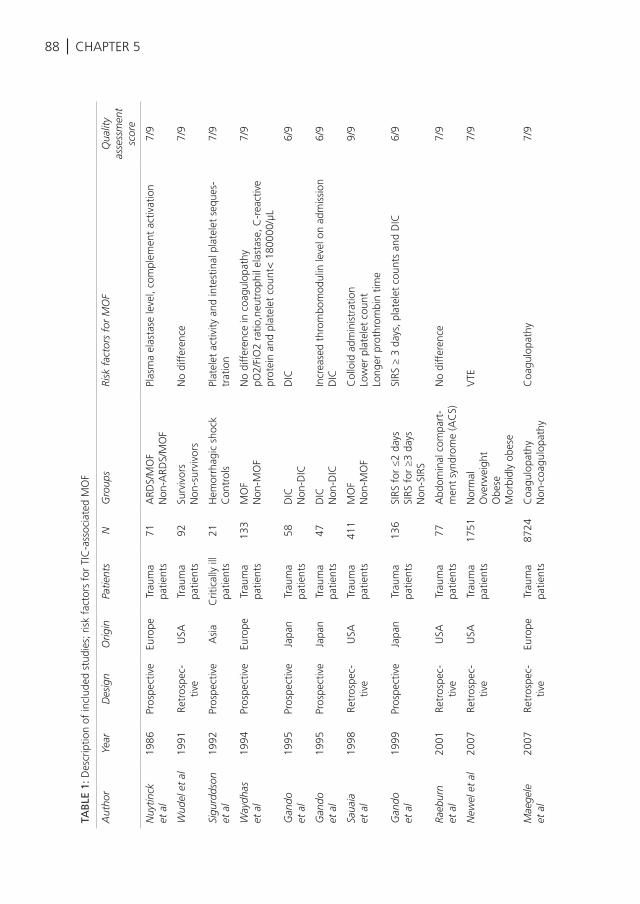
88 | CHAPTER 5
TAB
LE 1
: Des
crip
tion
of in
clud
ed s
tudi
es; r
isk
fact
ors
for
TIC
-ass
ocia
ted
MO
F
Aut
hor
Year
Des
ign
Orig
inPa
tient
sN
Gro
ups
Risk
fac
tors
for
MO
FQ
ualit
y as
sess
men
t sc
ore
Nuy
tinck
et
al
1986
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s71
ARD
S/M
OF
Non
-ARD
S/M
OF
Plas
ma
elas
tase
leve
l, co
mpl
emen
t ac
tivat
ion
7/9
Wud
el e
t al
1991
Retr
ospe
c-tiv
eU
SATr
aum
a pa
tient
s92
Surv
ivor
sN
on-s
urvi
vors
No
diff
eren
ce7/
9
Sigu
rdds
on
et a
l19
92Pr
ospe
ctiv
eA
sia
Crit
ical
ly il
l pa
tient
s21
Hem
orrh
agic
sho
ckC
ontr
ols
Plat
elet
act
ivity
and
inte
stin
al p
late
let
sequ
es-
trat
ion
7/9
Way
dhas
et
al
1994
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s13
3M
OF
Non
-MO
FN
o di
ffer
ence
in c
oagu
lopa
thy
pO2/
FiO
2 ra
tio,n
eutr
ophi
l ela
stas
e, C
-rea
ctiv
e pr
otei
n an
d pl
atel
et c
ount
< 1
8000
0/µL
7/9
Gan
do
et a
l19
95Pr
ospe
ctiv
eJa
pan
Trau
ma
patie
nts
58D
ICN
on-D
ICD
IC6/
9
Gan
do
et a
l19
95Pr
ospe
ctiv
eJa
pan
Trau
ma
patie
nts
47D
ICN
on-D
ICIn
crea
sed
thro
mbo
mod
ulin
leve
l on
adm
issi
onD
IC6/
9
Saua
ia
et a
l19
98Re
tros
pec-
tive
USA
Trau
ma
patie
nts
411
MO
FN
on-M
OF
Col
loid
adm
inis
trat
ion
Low
er p
late
let
coun
tLo
nger
pro
thro
mbi
n tim
e
9/9
Gan
do
et a
l19
99Pr
ospe
ctiv
eJa
pan
Trau
ma
patie
nts
136
SIRS
for
≤2
days
SIRS
for
≥3
days
Non
-SIR
S
SIRS
≥ 3
day
s, p
late
let
coun
ts a
nd D
IC6/
9
Raeb
urn
et a
l20
01Re
tros
pec-
tive
USA
Trau
ma
patie
nts
77A
bdom
inal
com
part
-m
ent
synd
rom
e (A
CS)
No
diff
eren
ce7/
9
New
el e
t al
2007
Retr
ospe
c-tiv
eU
SATr
aum
a pa
tient
s17
51N
orm
alO
verw
eigh
tO
bese
Mor
bidl
y ob
ese
VTE
7/9
Mae
gele
et
al
2007
Retr
ospe
c-tiv
eEu
rope
Trau
ma
patie
nts
8724
Coa
gulo
path
yN
on-c
oagu
lopa
thy
Coa
gulo
path
y7/
9
Paff
rath
et
al
2010
Retr
ospe
c-tiv
eEu
rope
Trau
ma
patie
nts
7937
VTE
Non
-VTE
VTE
7/9
Nyd
am
et a
l20
11Re
tros
pec-
tive
USA
Trau
ma
patie
nts
1415
Thro
mbo
cyto
peni
aN
on-t
hrom
bocy
tope
nia
Thro
mbo
cyto
peni
a 25
-48
hour
s po
st-in
jury
8/9
Brow
n et
al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
1877
Acu
te t
raum
atic
coa
gu-
lopa
thy
Non
acu
te t
raum
atic
co
agul
opat
hyM
ale
vs f
emal
e
Act
ivat
ion
of P
rote
in C
Acu
te c
oagu
lopa
thy
on a
rriv
alIn
crea
sed
tran
sfus
ion
requ
irem
ents
7/9
Kut
cher
et
al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
132
Hig
h hi
ston
e le
vels
Low
his
tone
leve
lsH
igh
hist
one
leve
l ass
ocia
ted
with
3,2
-fol
d hi
gher
inci
denc
e of
MO
F7/
9
Coh
en
et a
l20
12Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s20
3-
Hig
her
leve
ls o
f ac
tivat
ed P
rote
in C
upo
n ad
mis
sion
8/9
Col
e et
al
2013
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s15
8In
fect
ion
Non
-infe
ctio
nM
OF
rate
s in
crea
sed
with
PC
dep
letio
n of
PC
an
d ra
ised
PA
P le
vels
7/9
Tren
tzsc
h et
al
2014
Retr
ospe
c-tiv
eEu
rope
Trau
ma
patie
nts
2028
8M
ale
Fem
ale
No
diff
eren
ce in
coa
gulo
path
y be
twee
n gr
oups
8/9
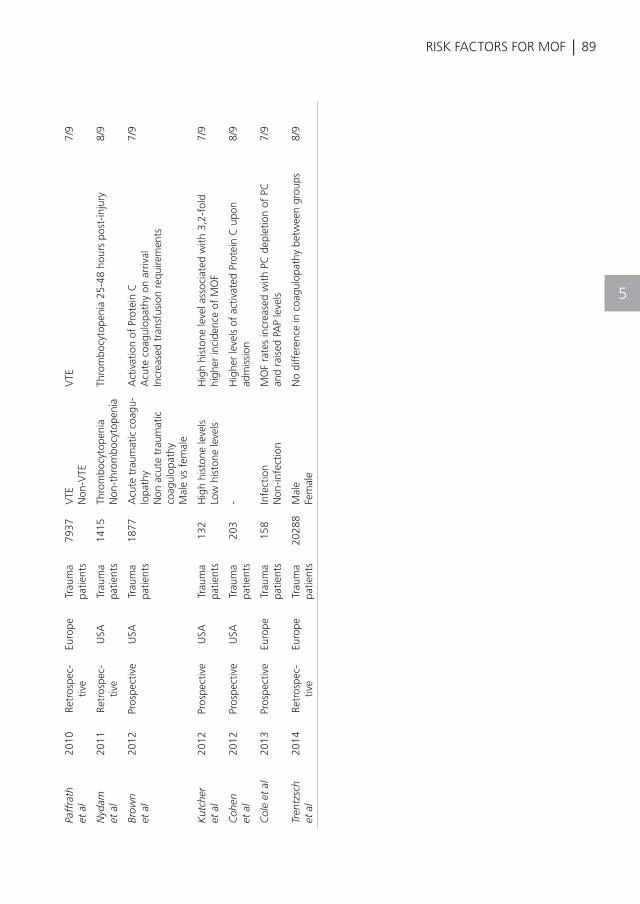
| 89
TAB
LE 1
: Des
crip
tion
of in
clud
ed s
tudi
es; r
isk
fact
ors
for
TIC
-ass
ocia
ted
MO
F
Aut
hor
Year
Des
ign
Orig
inPa
tient
sN
Gro
ups
Risk
fac
tors
for
MO
FQ
ualit
y as
sess
men
t sc
ore
Nuy
tinck
et
al
1986
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s71
ARD
S/M
OF
Non
-ARD
S/M
OF
Plas
ma
elas
tase
leve
l, co
mpl
emen
t ac
tivat
ion
7/9
Wud
el e
t al
1991
Retr
ospe
c-tiv
eU
SATr
aum
a pa
tient
s92
Surv
ivor
sN
on-s
urvi
vors
No
diff
eren
ce7/
9
Sigu
rdds
on
et a
l19
92Pr
ospe
ctiv
eA
sia
Crit
ical
ly il
l pa
tient
s21
Hem
orrh
agic
sho
ckC
ontr
ols
Plat
elet
act
ivity
and
inte
stin
al p
late
let
sequ
es-
trat
ion
7/9
Way
dhas
et
al
1994
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s13
3M
OF
Non
-MO
FN
o di
ffer
ence
in c
oagu
lopa
thy
pO2/
FiO
2 ra
tio,n
eutr
ophi
l ela
stas
e, C
-rea
ctiv
e pr
otei
n an
d pl
atel
et c
ount
< 1
8000
0/µL
7/9
Gan
do
et a
l19
95Pr
ospe
ctiv
eJa
pan
Trau
ma
patie
nts
58D
ICN
on-D
ICD
IC6/
9
Gan
do
et a
l19
95Pr
ospe
ctiv
eJa
pan
Trau
ma
patie
nts
47D
ICN
on-D
ICIn
crea
sed
thro
mbo
mod
ulin
leve
l on
adm
issi
onD
IC6/
9
Saua
ia
et a
l19
98Re
tros
pec-
tive
USA
Trau
ma
patie
nts
411
MO
FN
on-M
OF
Col
loid
adm
inis
trat
ion
Low
er p
late
let
coun
tLo
nger
pro
thro
mbi
n tim
e
9/9
Gan
do
et a
l19
99Pr
ospe
ctiv
eJa
pan
Trau
ma
patie
nts
136
SIRS
for
≤2
days
SIRS
for
≥3
days
Non
-SIR
S
SIRS
≥ 3
day
s, p
late
let
coun
ts a
nd D
IC6/
9
Raeb
urn
et a
l20
01Re
tros
pec-
tive
USA
Trau
ma
patie
nts
77A
bdom
inal
com
part
-m
ent
synd
rom
e (A
CS)
No
diff
eren
ce7/
9
New
el e
t al
2007
Retr
ospe
c-tiv
eU
SATr
aum
a pa
tient
s17
51N
orm
alO
verw
eigh
tO
bese
Mor
bidl
y ob
ese
VTE
7/9
Mae
gele
et
al
2007
Retr
ospe
c-tiv
eEu
rope
Trau
ma
patie
nts
8724
Coa
gulo
path
yN
on-c
oagu
lopa
thy
Coa
gulo
path
y7/
9
Paff
rath
et
al
2010
Retr
ospe
c-tiv
eEu
rope
Trau
ma
patie
nts
7937
VTE
Non
-VTE
VTE
7/9
Nyd
am
et a
l20
11Re
tros
pec-
tive
USA
Trau
ma
patie
nts
1415
Thro
mbo
cyto
peni
aN
on-t
hrom
bocy
tope
nia
Thro
mbo
cyto
peni
a 25
-48
hour
s po
st-in
jury
8/9
Brow
n et
al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
1877
Acu
te t
raum
atic
coa
gu-
lopa
thy
Non
acu
te t
raum
atic
co
agul
opat
hyM
ale
vs f
emal
e
Act
ivat
ion
of P
rote
in C
Acu
te c
oagu
lopa
thy
on a
rriv
alIn
crea
sed
tran
sfus
ion
requ
irem
ents
7/9
Kut
cher
et
al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
132
Hig
h hi
ston
e le
vels
Low
his
tone
leve
lsH
igh
hist
one
leve
l ass
ocia
ted
with
3,2
-fol
d hi
gher
inci
denc
e of
MO
F7/
9
Coh
en
et a
l20
12Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s20
3-
Hig
her
leve
ls o
f ac
tivat
ed P
rote
in C
upo
n ad
mis
sion
8/9
Col
e et
al
2013
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s15
8In
fect
ion
Non
-infe
ctio
nM
OF
rate
s in
crea
sed
with
PC
dep
letio
n of
PC
an
d ra
ised
PA
P le
vels
7/9
Tren
tzsc
h et
al
2014
Retr
ospe
c-tiv
eEu
rope
Trau
ma
patie
nts
2028
8M
ale
Fem
ale
No
diff
eren
ce in
coa
gulo
path
y be
twee
n gr
oups
8/9
RISK FACTORS FOR MOF
5
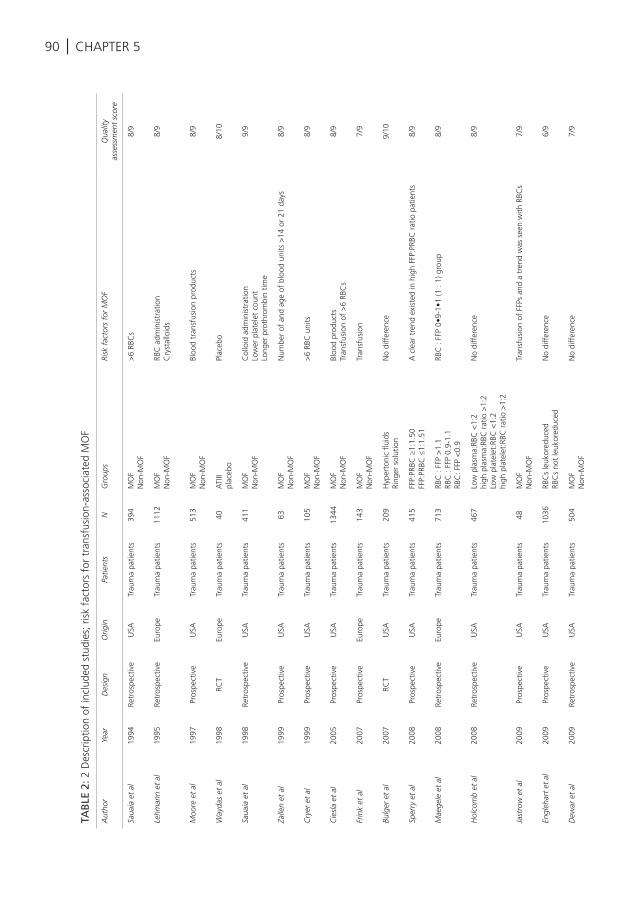
90 | CHAPTER 5
TAB
LE 2
: 2 D
escr
iptio
n of
incl
uded
stu
dies
; ris
k fa
ctor
s fo
r tr
ansf
usio
n-as
soci
ated
MO
F
Aut
hor
Year
Des
ign
Orig
inPa
tient
sN
Gro
ups
Risk
fac
tors
for
MO
FQ
ualit
y
asse
ssm
ent
scor
e
Saua
ia e
t al
1994
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s39
4M
OF
Non
-MO
F>
6 RB
Cs
8/9
Lehm
ann
et a
l19
95Re
tros
pect
ive
Euro
peTr
aum
a pa
tient
s11
12M
OF
Non
-MO
FRB
C a
dmin
istr
atio
nC
ryst
allo
ids
8/9
Moo
re e
t al
1997
Pros
pect
ive
USA
Trau
ma
patie
nts
513
MO
FN
on-M
OF
Bloo
d tr
ansf
usio
n pr
oduc
ts8/
9
Way
das
et a
l19
98RC
TEu
rope
Trau
ma
patie
nts
40A
TIII
plac
ebo
Plac
ebo
8/10
Saua
ia e
t al
1998
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s41
1M
OF
Non
-MO
FC
ollo
id a
dmin
istr
atio
nLo
wer
pla
tele
t co
unt
Long
er p
roth
rom
bin
time
9/9
Zalle
n et
al
1999
Pros
pect
ive
USA
Trau
ma
patie
nts
63M
OF
Non
-MO
FN
umbe
r of
and
age
of
bloo
d un
its >
14 o
r 21
day
s8/
9
Cry
er e
t al
1999
Pros
pect
ive
USA
Trau
ma
patie
nts
105
MO
FN
on-M
OF
>6
RBC
uni
ts8/
9
Cie
sla
et a
l20
05Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s13
44M
OF
Non
-MO
FBl
ood
prod
ucts
Tran
sfus
ion
of >
6 RB
Cs
8/9
Frin
k et
al
2007
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s14
3M
OF
Non
-MO
FTr
ansf
usio
n7/
9
Bulg
er e
t al
2007
RCT
USA
Trau
ma
patie
nts
209
Hyp
erto
nic
fluid
sRi
nger
sol
utio
nN
o di
ffer
ence
9/10
Sper
ry e
t al
2008
Pros
pect
ive
USA
Trau
ma
patie
nts
415
FFP:
PRBC
≥1:
1.50
FFP:
PRBC
≤1:
1.51
A c
lear
tre
nd e
xist
ed in
hig
h FF
P:PR
BC r
atio
pat
ient
s8/
9
Mae
gele
et
al20
08Re
tros
pect
ive
Euro
peTr
aum
a pa
tient
s71
3RB
C :
FFP
>1.
1RB
C :
FFP
0.9-
1.1
RBC
: FFP
<0.
9
RBC
: FF
P 0•
9-1•
1 (1
: 1)
gro
up8/
9
Hol
com
b et
al
2008
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s46
7Lo
w p
lasm
a:RB
C <
1:2
high
pla
sma:
RBC
rat
io >
1:2
Low
pla
tele
t:RB
C <
1:2
high
pla
tele
t:RB
C r
atio
>1:
2
No
diff
eren
ce8/
9
Jast
row
et
al20
09Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s48
MO
FN
on-M
OF
Tran
sfus
ion
of F
FPs
and
a tr
end
was
see
n w
ith R
BCs
7/9
Engl
ehar
t et
al
2009
Pros
pect
ive
USA
Trau
ma
patie
nts
1036
RBC
s le
ukor
educ
edRB
Cs
not
leuk
ored
uced
No
diff
eren
ce6/
9
Dew
ar e
t al
2009
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s50
4M
OF
Non
-MO
FN
o di
ffer
ence
7/9
Mah
ambr
ey e
t al
2009
Retr
ospe
ctiv
eC
anad
aTr
aum
a pa
tient
s26
0-
RBC
adm
inis
trat
ion
7/9
Wat
son
et a
l20
09Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s11
75H
igh
plas
ma
tran
sfus
ion
Low
pla
sma
tran
sfus
ion
FFP
and
cryo
prec
ipita
te a
dmin
istr
atio
n9/
9
Boff
ard
et a
l20
09RC
TA
fric
aTr
aum
a pa
tient
s30
1rV
IIaPl
aceb
orV
II gr
oup
low
er in
cide
nce
MO
F al
thou
gh n
ot
sign
ifica
nt8/
10
Cot
ton
et a
l20
09Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s26
6Pr
e-m
assi
ve t
rans
fusi
on p
roto
col
Mas
sive
tra
nsfu
sion
pro
toco
l Bl
ood
prod
uct
adm
inis
trat
ion
7/9
Hau
ser
et a
l20
10RC
TW
orld
wid
eTr
aum
a pa
tient
s57
3FV
IIaPl
aceb
oA
tre
nd is
obs
erve
d to
war
d de
crea
sed
MO
F in
rFV
IIa
grou
p9/
10
Paff
rath
et
al20
10Re
tros
pect
ive
Euro
peTr
aum
a pa
tient
s79
37V
TEN
on-V
TEV
TE7/
9
Brat
tstr
om e
t al
2010
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s16
4-
> 1
0 RB
C u
nits
8/9
John
son
et a
l20
10Re
tros
pect
ive
USA
Trau
ma
patie
nts
1440
MO
FN
on-M
OF
RBC
adm
inis
trat
ion
with
in 1
2 ho
urs
8/9
Nie
nabe
r et
al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
36FF
PC
oagu
latio
n fa
ctor
con
cent
rate
sPC
C t
reat
men
t as
soci
ated
with
red
uctio
n of
MO
F7/
9
Perk
ins
et a
l20
11Re
tros
pect
ive
USA
Trau
ma
patie
nts
369
Fres
h w
hole
blo
odA
pher
esis
pla
tele
tsN
o di
ffer
ence
7/9
Waf
aisa
de e
t al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
1362
FFP:
RBC
<1:
1FF
P:RB
C 1
:1FF
P:RB
C>
1:1
No
diff
eren
ce7/
9
Hus
sman
n et
al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
375
<10
00 m
l10
00-2
000
ml
2001
-300
0 m
l>
3000
ml
Cry
stal
loid
s <
100
0 m
l ass
ocia
ted
with
dec
reas
e in
M
OF
7/9
Brak
enrid
ge e
t al
2011
Pros
pect
ive
USA
Trau
ma
patie
nts
1366
->
10
RBC
uni
ts w
ithin
12
hour
s po
st-in
jury
7/9
Borg
man
et
al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
2474
Hig
h FF
P:RB
C >
1:2
Low
FFP
:RBC
<1:
2N
o di
ffer
ence
8/9
Brow
n et
al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
1877
Acu
te t
raum
atic
coa
gulo
path
yN
on a
cute
tra
umat
ic
coag
ulop
athy
Mal
e vs
fem
ale
Cry
stal
loid
, RBC
and
FFP
adm
inis
trat
ion
7/9
Inne
rhof
er e
t al
2012
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s14
4Fi
brin
ogen
and
/or
prot
hrom
bin
com
plex
con
cent
rate
alo
neA
dditi
onal
ly F
FP
FFP
adm
inis
trat
ion
8/9
Min
ei e
t al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
916
MO
FN
on-M
OF
FFP
adm
inis
trat
ion
with
in 1
2 ho
urs
post
-inju
ryC
ryst
allo
id a
dmin
istr
atio
n w
ithin
24
hour
s po
st-in
jury
9/9
Nea
l et
al20
12Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s45
2C
ryst
allo
id:R
BC r
atio
Cry
stal
loid
:RBC
rat
io >
1.5
:19/
9
Duc
hesn
e et
al
2012
Retr
ospe
ctiv
eTr
aum
a pa
tient
s18
83
perc
ent
hype
rton
ic s
olut
ion
Isot
onic
sol
utio
nIs
oton
ic s
olut
ion
7/9
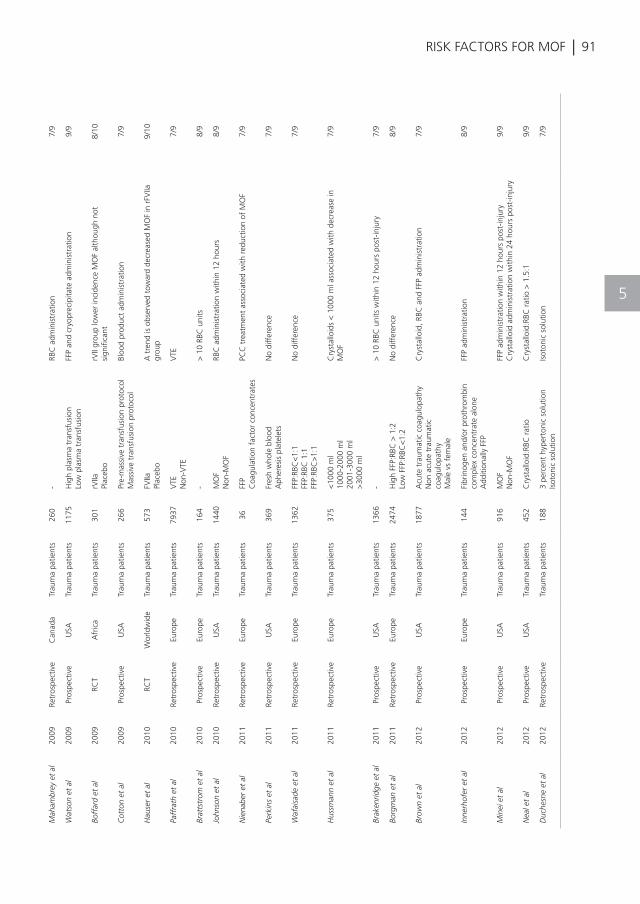
| 91RISK FACTORS FOR MOF
TAB
LE 2
: 2 D
escr
iptio
n of
incl
uded
stu
dies
; ris
k fa
ctor
s fo
r tr
ansf
usio
n-as
soci
ated
MO
F
Aut
hor
Year
Des
ign
Orig
inPa
tient
sN
Gro
ups
Risk
fac
tors
for
MO
FQ
ualit
y
asse
ssm
ent
scor
e
Saua
ia e
t al
1994
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s39
4M
OF
Non
-MO
F>
6 RB
Cs
8/9
Lehm
ann
et a
l19
95Re
tros
pect
ive
Euro
peTr
aum
a pa
tient
s11
12M
OF
Non
-MO
FRB
C a
dmin
istr
atio
nC
ryst
allo
ids
8/9
Moo
re e
t al
1997
Pros
pect
ive
USA
Trau
ma
patie
nts
513
MO
FN
on-M
OF
Bloo
d tr
ansf
usio
n pr
oduc
ts8/
9
Way
das
et a
l19
98RC
TEu
rope
Trau
ma
patie
nts
40A
TIII
plac
ebo
Plac
ebo
8/10
Saua
ia e
t al
1998
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s41
1M
OF
Non
-MO
FC
ollo
id a
dmin
istr
atio
nLo
wer
pla
tele
t co
unt
Long
er p
roth
rom
bin
time
9/9
Zalle
n et
al
1999
Pros
pect
ive
USA
Trau
ma
patie
nts
63M
OF
Non
-MO
FN
umbe
r of
and
age
of
bloo
d un
its >
14 o
r 21
day
s8/
9
Cry
er e
t al
1999
Pros
pect
ive
USA
Trau
ma
patie
nts
105
MO
FN
on-M
OF
>6
RBC
uni
ts8/
9
Cie
sla
et a
l20
05Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s13
44M
OF
Non
-MO
FBl
ood
prod
ucts
Tran
sfus
ion
of >
6 RB
Cs
8/9
Frin
k et
al
2007
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s14
3M
OF
Non
-MO
FTr
ansf
usio
n7/
9
Bulg
er e
t al
2007
RCT
USA
Trau
ma
patie
nts
209
Hyp
erto
nic
fluid
sRi
nger
sol
utio
nN
o di
ffer
ence
9/10
Sper
ry e
t al
2008
Pros
pect
ive
USA
Trau
ma
patie
nts
415
FFP:
PRBC
≥1:
1.50
FFP:
PRBC
≤1:
1.51
A c
lear
tre
nd e
xist
ed in
hig
h FF
P:PR
BC r
atio
pat
ient
s8/
9
Mae
gele
et
al20
08Re
tros
pect
ive
Euro
peTr
aum
a pa
tient
s71
3RB
C :
FFP
>1.
1RB
C :
FFP
0.9-
1.1
RBC
: FFP
<0.
9
RBC
: FF
P 0•
9-1•
1 (1
: 1)
gro
up8/
9
Hol
com
b et
al
2008
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s46
7Lo
w p
lasm
a:RB
C <
1:2
high
pla
sma:
RBC
rat
io >
1:2
Low
pla
tele
t:RB
C <
1:2
high
pla
tele
t:RB
C r
atio
>1:
2
No
diff
eren
ce8/
9
Jast
row
et
al20
09Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s48
MO
FN
on-M
OF
Tran
sfus
ion
of F
FPs
and
a tr
end
was
see
n w
ith R
BCs
7/9
Engl
ehar
t et
al
2009
Pros
pect
ive
USA
Trau
ma
patie
nts
1036
RBC
s le
ukor
educ
edRB
Cs
not
leuk
ored
uced
No
diff
eren
ce6/
9
Dew
ar e
t al
2009
Retr
ospe
ctiv
eU
SATr
aum
a pa
tient
s50
4M
OF
Non
-MO
FN
o di
ffer
ence
7/9
Mah
ambr
ey e
t al
2009
Retr
ospe
ctiv
eC
anad
aTr
aum
a pa
tient
s26
0-
RBC
adm
inis
trat
ion
7/9
Wat
son
et a
l20
09Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s11
75H
igh
plas
ma
tran
sfus
ion
Low
pla
sma
tran
sfus
ion
FFP
and
cryo
prec
ipita
te a
dmin
istr
atio
n9/
9
Boff
ard
et a
l20
09RC
TA
fric
aTr
aum
a pa
tient
s30
1rV
IIaPl
aceb
orV
II gr
oup
low
er in
cide
nce
MO
F al
thou
gh n
ot
sign
ifica
nt8/
10
Cot
ton
et a
l20
09Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s26
6Pr
e-m
assi
ve t
rans
fusi
on p
roto
col
Mas
sive
tra
nsfu
sion
pro
toco
l Bl
ood
prod
uct
adm
inis
trat
ion
7/9
Hau
ser
et a
l20
10RC
TW
orld
wid
eTr
aum
a pa
tient
s57
3FV
IIaPl
aceb
oA
tre
nd is
obs
erve
d to
war
d de
crea
sed
MO
F in
rFV
IIa
grou
p9/
10
Paff
rath
et
al20
10Re
tros
pect
ive
Euro
peTr
aum
a pa
tient
s79
37V
TEN
on-V
TEV
TE7/
9
Brat
tstr
om e
t al
2010
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s16
4-
> 1
0 RB
C u
nits
8/9
John
son
et a
l20
10Re
tros
pect
ive
USA
Trau
ma
patie
nts
1440
MO
FN
on-M
OF
RBC
adm
inis
trat
ion
with
in 1
2 ho
urs
8/9
Nie
nabe
r et
al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
36FF
PC
oagu
latio
n fa
ctor
con
cent
rate
sPC
C t
reat
men
t as
soci
ated
with
red
uctio
n of
MO
F7/
9
Perk
ins
et a
l20
11Re
tros
pect
ive
USA
Trau
ma
patie
nts
369
Fres
h w
hole
blo
odA
pher
esis
pla
tele
tsN
o di
ffer
ence
7/9
Waf
aisa
de e
t al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
1362
FFP:
RBC
<1:
1FF
P:RB
C 1
:1FF
P:RB
C>
1:1
No
diff
eren
ce7/
9
Hus
sman
n et
al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
375
<10
00 m
l10
00-2
000
ml
2001
-300
0 m
l>
3000
ml
Cry
stal
loid
s <
100
0 m
l ass
ocia
ted
with
dec
reas
e in
M
OF
7/9
Brak
enrid
ge e
t al
2011
Pros
pect
ive
USA
Trau
ma
patie
nts
1366
->
10
RBC
uni
ts w
ithin
12
hour
s po
st-in
jury
7/9
Borg
man
et
al
2011
Retr
ospe
ctiv
eEu
rope
Trau
ma
patie
nts
2474
Hig
h FF
P:RB
C >
1:2
Low
FFP
:RBC
<1:
2N
o di
ffer
ence
8/9
Brow
n et
al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
1877
Acu
te t
raum
atic
coa
gulo
path
yN
on a
cute
tra
umat
ic
coag
ulop
athy
Mal
e vs
fem
ale
Cry
stal
loid
, RBC
and
FFP
adm
inis
trat
ion
7/9
Inne
rhof
er e
t al
2012
Pros
pect
ive
Euro
peTr
aum
a pa
tient
s14
4Fi
brin
ogen
and
/or
prot
hrom
bin
com
plex
con
cent
rate
alo
neA
dditi
onal
ly F
FP
FFP
adm
inis
trat
ion
8/9
Min
ei e
t al
2012
Pros
pect
ive
USA
Trau
ma
patie
nts
916
MO
FN
on-M
OF
FFP
adm
inis
trat
ion
with
in 1
2 ho
urs
post
-inju
ryC
ryst
allo
id a
dmin
istr
atio
n w
ithin
24
hour
s po
st-in
jury
9/9
Nea
l et
al20
12Pr
ospe
ctiv
eU
SATr
aum
a pa
tient
s45
2C
ryst
allo
id:R
BC r
atio
Cry
stal
loid
:RBC
rat
io >
1.5
:19/
9
Duc
hesn
e et
al
2012
Retr
ospe
ctiv
eTr
aum
a pa
tient
s18
83
perc
ent
hype
rton
ic s
olut
ion
Isot
onic
sol
utio
nIs
oton
ic s
olut
ion
7/9
5
92 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
Sauaia A,Moore FA,Moore EE,Moser
KS,Brennan R,Read RA,et al.Epidemiology
of trauma deaths: are assessment. J Trauma
(1995) 38(2):185–93.doi:10.1097/00005373-
199502000-00006
Soreide K,Kruger AJ,Vardal AL,Ellingsen
CL,Soreide E,Lossius HM.Epidemiology and
contemporary patterns of trauma deaths:
changing place, similar pace,older face.
WorldJSurg (2007) 31(11):2092–103.
doi:10.1007/s00268-007-9226-9
DewarDC,TarrantSM,KingKL,BaloghZJ.
Changes in the epidemiology and prediction
of multiple organ failure after injury. J
Trauma Acute Care Surg (2013) 74(3):774–9.
doi:10.1097/TA.0b013e31827a6e69
Nast-Kolb D, Aufmkolk M, Rucholtz S,
Obertacke U, Waydhas C.Multiple organ
failure still a major cause of morbidity but not
mortality in blunt multiple trauma. J Trauma
(2001) 51(5):835–41.doi:10.1097/00005373-
200111000-00003
Brattstrom O, Granath F, Rossi P, Oldner A.
Early predictors of morbidity and mortality
in trauma patients treated in the intensive
care unit. Acta Anaesthesiol Scand (2010)
54 (8 ) : 1007–17 .do i : 10 .1111 / j . 1399 -
6576.2010.02266.x
Ciesla DJ, Moore EE, Johnson JL , Burch
JM, Cothren CC, Sauaia A. A 12-year
prospective study of post injury multiple
organ failure: has anything changed? Arch
Surg (2005) 140(5):432–8.doi:10.1001/
archsurg.140.5.432
Dunn EL, MooreEE, Breslich DJ, Galloway WB.
Acidosis-induced coagulopathy. Surg Forum
(1979) 30:471–3.
Schochl H, Frietsch T, Pavelka M, Jambor
C. Hyperfibrinolysis after major trauma:
differential diagnosis of lysis patterns and
prognostic value of thrombelastometry. J
Trauma (2009) 67(1):125–31.doi:10.1097/
TA.0b013e31818b2483
Johansson PI, Stensballe J, Rasmussen LS,
Ostrowski SR. A high admission syndecan-1
level, a marker of endothelial glycocalyx
degradation, is associated with inflammation,
protein C depletion, fibrinolysis, and increased
mortality in trauma patients. Ann Surg
(2011) 254(2):194–200.doi:10.1097/SLA.
0b013e318226113d
MacLeod JB, Lynn M, McKenney MG, Cohn
SM, Murtha M. Early coagulopathy predicts
mortality in trauma. J Trauma (2003) 55(1):39–
44.doi:10.1097/01.TA.0000075338.21177.EF
Hess JR, Lindell AL, Stansbury LG, Dutton
RP, Scalea TM. The prevalence of abnormal
results of conventional coagulation tests on
admission to a trauma center. Transfusion
(2009) 49(1):34–9.doi:10.1111/j.1537-
2995.2008.01944.x
Brohi K, Singh J, Heron M, Coats T.
Acute traumatic coagulopathy. J Trauma
(2003) 54(6):1127–30.doi:10.1097/01.
TA.0000069184.82147.06
Plotkin AJ, Wade CE, Jenkins DH, Smith KA,
Noe JC, Park MS, et al. A reduction in clot
formation rate and strength assessed by
thrombelastography is indicative of transfusion
requirements in patients with penetrating
injuries. J Trauma (2008) 64(2 Suppl):S64–8.
doi:10.1097/TA.0b013e318160772d
del Junco DJ, Holcomb JB, Fox EE, Brasel
KJ, Phelan HA, Bulger EM, et al. Resuscitate
early with plasma and platelets or balance
blood products gradually: findings from the
PROMMTT study. J Trauma Acute Care Surg
(2013) 75(1 Suppl1):S24–30.doi:10.1097/
TA.0b013e31828fa3b9
Brown LM, Aro SO, Cohen MJ, Holcomb JB,
Wade CE, Brasel KJ,et al. A high fresh frozen
plasma: packed red blood cell transfusion ratio
decreases mortality in all massively transfused
trauma patients regardless of admission
international normalized ratio. J Trauma
(2011) 71(2 Suppl3):S358–63.doi:10.1097/
TA.0b013e318227f152
Morrison CA, Carrick MM, Norman MA,
CHAPTER 5
| 93
REFERENCES
RISK FACTORS FOR MOF
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
Scott BG, Welsh FJ, Tsai P, et al. Hypotensive
resuscitation strategy reduces transfusion
requirements and severe postoperative
coagulopathy in trauma patients with
hemorrhagic shock: preliminary results of
a randomized controlled trial. J Trauma
(2011) 70(3):652–63.doi:10.1097/
TA.0b013e31820e77ea
Moher D, Liberati A,Tetzlaff J, Altman DG.
Preferred reporting items for systematic
reviews and meta-analyses: the PRISMA
statement. BMJ (2009) 339:b2535.
doi:10.1136/bmj.b2535
Sauaia A, Moore EE, Johnson JL, Ciesla
DJ, Biffl WL, Banerjee A. Validation of
post injury multiple organ failure scores.
Shock (2009) 31(5):438–47.doi:10.1097/
SHK.0b013e31818ba4c6
Grotz M, von GM, Stalp M, Kaufmann U,
Hildebrand F, Pape HC. [Scoring multiple
organ failure after severe trauma. Comparison
of the Goris, Marshall and Moore scores].
Chirurg (2001) 72(6):723–30.doi:10.1007/
s001040170130
Antonelli M, Moreno R, Vincent JL, Sprung
CL, Mendoca A, Passariello M, et al.
Application of SOFA score to trauma patients.
Sequential organ failure assessment. Intensive
Care Med (1999) 25(4):389–94.doi:10.1007/
s001340050863
Wells G, Shea B, O’Connel J. The Newcastle-
Ottawa Scale(NOS) for Assessing the Quality
of Nonrandomised Studies in Meta-Analysis
(2011). Available from: http://www.ohri.ca/
programs/clinical_epidemiology/oxford.asp
Higgins JPT, Altman DG. Chapter8: assessing
risk of bias in included studies. In: Higgins J,
Green S, editors. The Cochrane Collaboration,
5.0.1ed.Chichester: John Wiley&Sons,
Ltd(2008).
Nuytinck JK, Goris JA, Red lH, Schlag G,van
Munster PJ. Posttraumatic complications
and inflammatory mediators. Arch Surg
(1986) 121(8):886–90. doi:10.1001/
archsurg.1986.01400080028004
Wudel JH, Morris JAJr, YatesK, Wilson A, Bass
SM. Massive transfusion: Outcome in blunt
trauma patients. J Trauma (1991) 31(1):1–7.
doi:10.1097/00005373-199101000-00001
Sigurdsson GH, Christenson JT, El-Rakshy
MB, Sadek S. Intestinal platelet trapping after
traumatic and septic shock. An early sign of
sepsis and multi organ failure in critically ill
patients? Crit Care Med (1992) 20:458–67.
doi:10.1097/00003246-199204000-00005
Waydhas C, Nast-Kolb D, Kick M, Zett lR,
Wiesholler J, Trupka A, et al.[Operation
planning of secondary interventions after
polytrauma]. Unfallchirurg (1994) 97(5):244–
9.
Gando S, Nakanishi Y, TedoI. Cytokines
and plasminogen activator inhibitor-1 in
post trauma disseminated intravascular
coagulation: relationship to multiple organ
dysfunction syndrome. Crit Care Med (1995)
23(11):1835–42. doi:10.1097/00003246-
199511000-00009
Gando S, Nakanishi Y, Kameue T, Nanzaki S.
Soluble thrombomodulin increases in patients
with disseminated intravascular coagulation
and in those with multiple organ dysfunction
syndrome after trauma: role of neutrophil
elastase. J Trauma (1995) 39(4):660–4.
doi:10.1097/00005373-199510000-00007
Sauaia A, Moore FA, Moore EE, Norris JM,
Lezotte DC, Hamman RF. Multiple organ
failure can be predicted as early as 12 hours
after injury. J Trauma (1998) 45(2):291–301.
doi:10.1097/00005373-199808000-00014
Gando S, Nanzaki S, Kemmotsu O.
Disseminated intravascular coagulation and
sustained systemic inflammatory response
syndrome predict organ dysfunctions after
trauma: application of clinical decision
analysis. Ann Surg (1999) 229(1):121–7.
doi:10.1097/00000658-199901000-00016
Raeburn CD, Moore EE, Biffl WL, Johnson
JL, Meldrum DR, Offner PJ, et al. The
5
94 |
REFERENCES
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
abdominal compartment syndrome is a
morbid complication of postin-jury damage
control surgery. Am J Surg (2001) 182:542–6.
doi:10.1016/S0002-9610(01)00821-2
Newell MA, Bard MR, Goettler CE, Toschlog
EA, Schenarts PJ, Sagraves SG, et al. Bodymass
index and outcomes in critically injured
blunt trauma patients: weighing the impact.
J Am Coll Surg (2007) 204(5):1056–61.
doi:10.1016/j. jamcollsurg.2006.12.042
Maegele M, Lefering R, Yuce lN, Tjardes T,
Rixen D, Paffrath T, et al. Early coagulopathy
in multiple injury: an analysis from the
German trauma registry on 8724 patients.
Injury (2007) 38(3):298–304.doi:10.1016/j.
injury.2006.10.003
Paffrath T, Wafaisade A, Lefering R, Simanski C,
Bouillon B, Spanholtz T, et al. Venous thrombo
embolism after severe trauma: incidence, risk
factors and outcome. Injury (2010) 41(1):97–
101.doi:10.1016/j.injury.2009.06.010
Nydam TL, Kashuk JL, Moore EE, Johnson
JL, Burlew CC, Biffl WL, et al. Refractory
postinjury thrombocytopenia is associated
with multiple organ failure and adverse
outcomes. J Trauma (2011) 70(2):401–6.
doi:10.1097/TA. 0b013e31820b5c85
Brown JB, Cohen MJ, Minei JP, Maier RV,
West MA, Billiar TR, et al. Characterization of
acute coagulopathy and sexual dimorphism
after injury: females and coagulopathy
just do not mix. J Trauma Acute Care Surg
(2012) 73(6):1395–400. doi:10.1097/
TA.0b013e31825b9f05
Kutcher ME, Xu J, Vilardi RF, Ho C, Esmon
CT, Cohen MJ. Extracellular histone release in
response to traumatic injury: implications for
a compensatory role of activated protein C. J
Trauma Acute Care Surg (2012) 73(6):1389–
94. doi:10.1097/TA.0b013e318270d595
Cohen MJ, Call M, Nelson M, Calfee CS,
Esmon CT, Brohi K, et al. Critical role of
activated protein C in early coagulopathy
and later organ failure, infection and death in
trauma patients. Ann Surg (2012) 255(2):379–
85.doi:10.1097/SLA.0b013e318235d9e6
Cole E, Davenport R, De’Ath H, Manson J,
Brockamp T ,Brohi K. Coagulation system
changes associated with susceptibility to
infection in trauma patients. J Trauma Acute
Care Surg (2013) 74(1):51–7.doi:10.1097/
TA.0b013e3182788b0f
Trentzsch H, Nienaber U, Behnke M, Lefering R,
Piltz S. Female sex protects from organ failure
and sepsis after major trauma haemorrhage.
Injury (2014) 45(Suppl3):S20–8.doi:10.1016/j.
injury.2014.08.013
Sauaia A, Moore FA, Moore EE, Haene
lJB, Read RA, Lezotte DC. Early predictors
of post injury multiple organ failure. Arch
Surg (1994) 129(1):39–45. doi:10.1001/
archsurg.1994.01420250051006
Lehmann U, Grotz M, Regel G, Rudolph
S, Tscherne H. [Does initial management
of polytrauma patients have an effect on
the development of multiple organfailure?
Evaluation of preclinical and clinical data of
1,112 polytrauma patients]. Unfallchirurg
(1995) 98(8):442–6.
Moore FA, Moore EE, Sauaia A. Blood
transfusion. An independent risk factor
for post injury multiple organ failure. Arch
Surg (1997) 132(6):620–4. doi:10.1001/
archsurg.1997.01430300062013
Waydhas C, Nast-Kolb D, Gippner-Steppert
C, Trupka A, Pfundstein C, Schweiberer L,
et al. High-dose antithrombin III treatment
of severely injured patients: results of a
prospective study. J Trauma (1998) 45(5):931–
40.doi:10.1097/00005373-199811000-
00015
Zallen G, Offner PJ, Moore EE, Blackwell J,
Ciesla DJ, Gabriel J,et al. Age of transfused
blood is an independent risk factor for post
injury multiple organ failure. Am J Surg
(1999) 178(6):570–2.doi:10.1016/S0002-
9610(99)00239-1
Cryer HG, Leong K, McArthur DL, Demetriades
CHAPTER 5
| 95
REFERENCES
RISK FACTORS FOR MOF
47
48
49
50
51
52
53
54
55
56
57
58
59
60
D, Bongard FS, Fleming AW, et al.Multiple
organ failure: by the time you predict it, it’s
already there. J Trauma (1999) 46(4):597–604.
doi:10.1097/00005373-199904000-00007
Frink M, Pape HC, van Griensven M, Krettek
C, Chaudry IH, Hildebrand F. Influence of
sex and age on mods and cytokines after
multiple injuries. Shock (2007) 27:151–6.
doi:10.1097/01.shk.0000239767.64786
Bulger EM, Cuschieri J, Warner K, Maier
RV. Hypertonic resuscitation modulates the
inflammatory response in patients with
traumatic hemorrhagic shock. Ann Surg
(2007) 245(4):635–41. doi:10.1097/01.
sla.0000251367.44890.ae
Sperry JL, Nathens AB, Franke lHL, Vanek SL,
Moore EE, Maier RV, et al. Characterization
of the gender dimorphism after injury and
hemorrhagic shock: are hormonal differences
responsible? Crit Care Med (2008) 36(6):1838–
45.doi:10.1097/CCM.0b013e3181760c14
Sperry JL, Ochoa JB, Gunn SR, Alarcon LH,
Minei JP, Cuschieri J, et al. An FFP:PRBC
transfusion ratio >/=1:1.5 is associated
with a lower risk of mortality after massive
transfusion. J Trauma (2008) 65(5):986–93.
doi:10.1097/TA.0b013e3181878028
Maegele M, Lefering R, Paffrath T, Tjardes
T, Simanski C, Bouillon B. Red-bloodcell to
plasma ratios transfused during massive
transfusion are associated with mortality in
severe multiple injury: a retrospective analysis
from the trauma registry of the Deutsche
Gesellschaft fur Unfallchirurgie. VoxSang
(2008) 95(2):112–9.doi:10.1111/j.1423-
0410.2008.01074.x
Holcomb JB, Wade CE, Michalek JE,
Chisholm GB, Zarzabal LA, Schreiber MA,
et al. Increased plasma and platelet to red
blood cell ratios improves outcome in 466
massively transfused civilian trauma patients.
Ann Surg (2008) 248(3):447–58.doi:10.1097/
SLA.0b013e318185a9ad
Jastrow KMIII, Gonzalez EA,McGuire MF,
Suliburk JW, Kozar RA, Iyengar S, et al. Early
cytokine production risk stratifies trauma
patients for multiple organ failure. J Am Coll
Surg (2009) 209(3):320–31.doi:10.1016/j.
jamcollsurg.2009.05.002
Englehart MS, Cho SD, Morris MS, Gee
AC, Riha G, Underwood SJ, et al. Use
of leukoreduced blood does not reduce
infection, organ failure, or mortality following
trauma. World J Surg (2009) 33(8):1626–32.
doi:10.1007/s00268-009-0076-5
Dewar DC, Mackay P, Balogh Z. Epidemiology
of post-injury multiple organ failure in
an Australian trauma system. ANZ JSurg
(2009) 79(6):431–6. doi:10.1111/j.1445-
2197.2009.04968.x
Mahambrey TD, Fowler RA, Pinto R, Smith
TS, Callum JL, Pisani NS, et al. Early massive
transfusion in trauma patients: Canadian
single-centre retrospective cohort study. Can
J Anaesth (2009) 56(10):740–50.doi:10.1007/
s12630-009-9151-5
Watson GA, Sperry JL, Rosengart MR, Minei
JP, Harbrecht BG, Moore EE, et al. Fresh
frozen plasma is independently associated
with a higher risk of multiple organ failure
and acute respiratory distress syndrome. J
Trauma (2009) 67(2):221–7.doi:10.1097/
TA.0b013e3181ad5957
Boffard KD, Choong PI, Kluger Y, Riou B, Rizoli
SB, Rossaint R,et al. The treatment of bleeding
is to stop the bleeding! Treatment of trauma-
related hemorrhage. Transfusion (2009)
49(Suppl5):240S–7S.doi:10.1111/j.1537-
2995.2008.01987.x
Cotton BA, Au BK, Nunez TC, Gunter
OL, Robertson AM, Young PP. Predefined
massive transfusion protocols are associated
with a reduction in organ failure and
postinjury complications. J Trauma (2009)
66(1):41–8; discussion48–9.doi:10.1097/
TA.0b013e31819313bb
Hauser CJ, Boffard K, Dutton R, Bernard
GR, Croce MA, Holcomb JB, et al. Results
5
96 |
REFERENCES
61
62
63
64
65
66
67
68
69
70
71
72
of the CONTROL trial: efficacy and safety
of recombinant activated factor VII in
the management of refractory traumatic
hemorrhage. J Trauma (2010) 69(3):489–500.
doi:10.1097/TA.0b013e3181edf36e
Johnson JL, Moore EE, Kashuk JL, Banerjee A,
Cothren CC, Biffl WL, et al. Effect of blood
products transfusion on the development
of postinjury multiple organ failure. Arch
Surg (2010) 145(10):973–7.doi:10.1001/
archsurg.2010.216
Nienaber U, Innerhofer P, Westermann I,
Schochl H, Attal R, Breitkopf R, et al. The
impact of fresh frozen plasma vs coagulation
factor concentrates on morbidity and mortality
in trauma-associated haemorrhage and
massive transfusion.Injury (2011) 42(7):697–
701.doi:10.1016/j.injury.2010.12.015
Perkins JG, Cap AP, Spinella PC, Shorr AF,
Beekley AC, Grathwohl KW,et al. Comparison
of platelet transfusion as fresh whole blood
versus apheresis platelets for massively
transfused combat trauma patients(CME).
Transfusion (2011) 51(2):242–52.doi:10.1111/
j.1537-2995.2010.02818.x
Wafaisade A, Maegele M, Lefering R, Braun
M, Peiniger S, Neugebauer E, et al. High
plasma to red blood cell ratios are associated
with lower mortality rates in patients receiving
multiple transfusion (4≤red blood cell units
<10) during acute trauma resuscitation. J
Trauma (2011) 70(1):81–8; discussion88–9.
doi:10.1097/TA.0b013e3182032e0b
Hussmann B, Taeger G, Lefering R, Waydhas
C, Nast-Kolb D, Ruchholtz S, et al. [Lethality
and outcome in multiple injured patients after
severe abdominal and pelvic trauma. Influence
of preclinical volume replacement–ananalysis
of 604 patients from the trauma registry of
the DGU]. Unfallchirurg (2011) 114(8):705–
12.doi:10.1007/s00113-010-1842-4
Brakenridge SC, Phelan HA, Henley SS,
Golden RM, Kashner TM, Eastman AE, et al.
Early blood product and crystalloid volume
resuscitation: risk association with multiple
organ dysfunction after severe blunt traumatic
injury. J Trauma (2011) 71(2):299–305.
doi:10.1097/TA.0b013e318224d328
Borgman MA, Spinella PC, Holcomb JB,
Blackbourne LH, Wade CE, Lefering R, et
al. The effect of FFP:RBC ratio on morbidity
and mortality in trauma patients based
on transfusion prediction score. VoxSang
(2011) 101(1):44–54. doi:10.1111/j.1423-
0410.2011.01466.x
Innerhofer P, Westermann I, Tauber H,
Breitkopf R, Fries D, Kastenberger T, et al.
The exclusive use of coagulation factor
concentrates enables reversal of coagulopathy
and decreases transfusion rates in patients
with major blunt trauma. Injury (2013)
44:209–16. doi:10.1016/j.injury.2012.08.047
Minei JP, Cuschieri J, Sperry J, Moore EE,
West MA, Harbrecht BG, et al. The changing
pattern and implications of multiple organ
failure after blunt injury with hemorrhagic
shock. Crit Care Med (2012) 40(4):1129–35.
doi:10.1097/CCM.0b013e3182376e9f
Neal MD, Hoffman MK, Cuschieri J, Minei
JP, Maier RV, Harbrecht BG, et al. Crystalloid
to packed red blood cell transfusion ratio
in the massively transfused patient: when
a little goes a long way. J Trauma Acute
Care Surg (2012) 72(4):892–8.doi:10.1097/
TA.0b013e31823d84a7
Duchesne JC, Simms E, Guidry C, Duke
M, Beeson E, McSwain NE, et al. Damage
control immunoregulation: is there a role for
low-volume hypertonic saline resuscitation
in patients managed with damage control
surgery? Am Surg (2012) 78(9):962–8.
Pape HC,van GM, Rice J, Gansslen
A, Hildebrand F, Zech S, et al. Major
secondary surgery in blunt trauma patients
and perioperative cytokine liberation:
determination of the clinical relevance
of biochemical markers. J Trauma (2001)
50(6):989–1000.doi:10.1097/00005373-
CHAPTER 5
| 97
REFERENCES
73
74
75
76
77
78
79
80
81
82
83
200106000-00004
Frith D, Goslings JC, Gaarder C, Maegele
M, Cohen MJ, Allard S, et al. Definition and
drivers of acute traumatic coagulopathy:
clinical and experimental investigations.
J Thromb Haemost (2010) 8(9):1919–25.
doi:10.1111/j.1538-7836.2010.03945.x
Floccard B, Rugeri L, Faure A, Saint DM, Boyle
EM, Peguet O, et al. Early coagulopathy in
trauma patients: a non-scene and hospital
admission study. Injury (2012) 43(1):26–32.
doi:10.1016/j.injury.2010.11.003
RazaI, Davenport R, Rourke C, Platton S,
Manson J, Spoors C, et al. The incidence
and magnitude of fibrinolytic activation in
trauma patients. J Thromb Haemost (2013)
11(2):307–14.doi:10.1111/jth.12078
Nielsen VG. A comparison of the
thrombelastograph and the ROTEM. Blood
Coagul Fibrinolysis (2007) 18(3):247–52.
doi:10.1097/MBC.0b013e328092ee05
Innerhofer P, Westermann I, Tauber H,
Breitkopf R, Fries D, Kastenberger T, et al.
The exclusive use of coagulation factor
concentrates enables reversal of coagulopathy
and decreases transfusion rates in patients with
major blunt trauma. Injury (2013) 44(2):209–
16.doi:10.1016/j.injury.2012.08.047
Tomori T, Hupalo D, Teranishi K, Michaud
S, Hammett M, Freilich D, et al. Evaluation
of coagulation stages of haemorrhaged
swine: comparison of thromboelastography
and rotational elastometry. Blood Coagul
Fibrinolysis (2010) 21(1):20–7.doi:10.1097/
MBC.0b013e32833113e9
Zehtabchi S, Nishijima DK. Impact of
transfusion of fresh-frozen plasma and packed
red blood cells in a 1:1 ratio on survival of
emergency department patients with severe
trauma. Acad Emerg Med (2009) 16(5):371–
8.doi:10.1111/j.1553-2712.2009.00386.x
Holcomb JB, Tilley BC, Baraniuk S, Fox EE,
Wade CE, Podbielski JM, et al. Transfusion
of plasma, platelets, and red blood cells in a
1:1:1 vs a 1:1:2ratio and mortality in patients
with severe trauma: the PROPPR randomized
clinical trial. JAMA (2015) 313(5):471–82.
doi:10.1001/jama.2015.12
Lo CK, Mertz D, Loeb M. Newcastle-Ottawa
scale: comparing reviewers’ to authors’
assessments. BMC Med Res Methodol (2014)
14:45.doi:10.1186/1471-2288-14-45
Hartling L, Milne A, Hamm MP, Van der meer
B, Ansari M, Tsertsvadze A,et al. Testing
the Newcastle Ottawa scale showed low
reliability between individual reviewers. J Clin
Epidemiol (2013) 66(9):982–93.doi:10.1016/j.
jclinepi.2013.03.003
Higgins JPT, Green S.(editors).
Cochrane Handbook for Systematic
Reviews of Interventions Version 5.1.0.
TheCochraneCollaboration (2011). Available
from:http://www.cochrane-handbook.org
RISK FACTORS FOR MOF
5
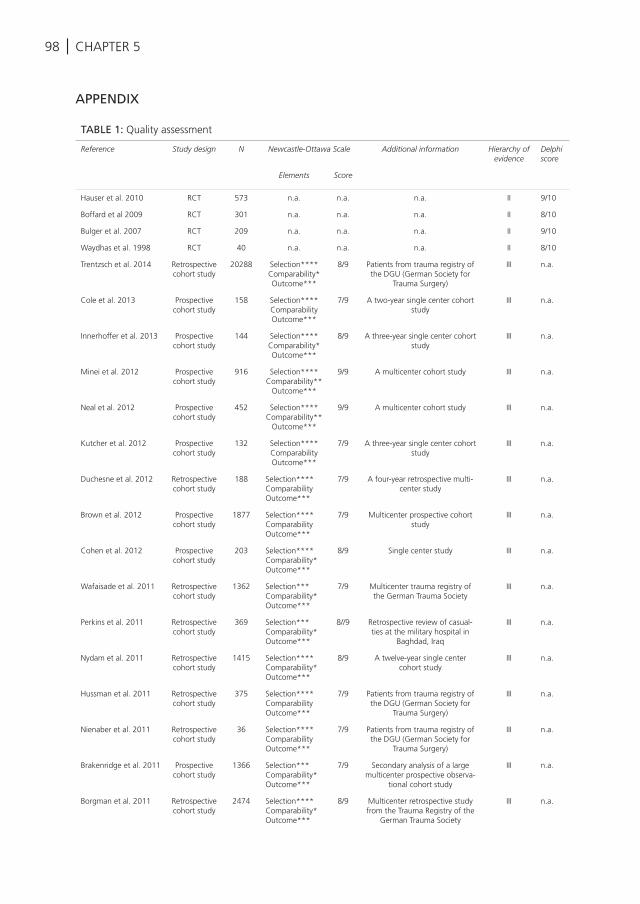
98 | CHAPTER 5
APPENDIX
TABLE 1: Quality assessment
Reference Study design N Newcastle-Ottawa Scale Additional information Hierarchy of evidence
Delphi score
Elements Score
Hauser et al. 2010 RCT 573 n.a. n.a. n.a. II 9/10
Boffard et al 2009 RCT 301 n.a. n.a. n.a. II 8/10
Bulger et al. 2007 RCT 209 n.a. n.a. n.a. II 9/10
Waydhas et al. 1998 RCT 40 n.a. n.a. n.a. II 8/10
Trentzsch et al. 2014 Retrospective cohort study
20288 Selection****Comparability*Outcome***
8/9 Patients from trauma registry of the DGU (German Society for
Trauma Surgery)
III n.a.
Cole et al. 2013 Prospective cohort study
158 Selection****ComparabilityOutcome***
7/9 A two-year single center cohort study
III n.a.
Innerhoffer et al. 2013 Prospective cohort study
144 Selection****Comparability*Outcome***
8/9 A three-year single center cohort study
III n.a.
Minei et al. 2012 Prospective cohort study
916 Selection****Comparability**
Outcome***
9/9 A multicenter cohort study III n.a.
Neal et al. 2012 Prospective cohort study
452 Selection****Comparability**
Outcome***
9/9 A multicenter cohort study III n.a.
Kutcher et al. 2012 Prospective cohort study
132 Selection****ComparabilityOutcome***
7/9 A three-year single center cohort study
III n.a.
Duchesne et al. 2012 Retrospective cohort study
188 Selection****ComparabilityOutcome***
7/9 A four-year retrospective multi-center study
III n.a.
Brown et al. 2012 Prospective cohort study
1877 Selection****ComparabilityOutcome***
7/9 Multicenter prospective cohort study
III n.a.
Cohen et al. 2012 Prospective cohort study
203 Selection****Comparability*Outcome***
8/9 Single center study III n.a.
Wafaisade et al. 2011 Retrospective cohort study
1362 Selection***Comparability*Outcome***
7/9 Multicenter trauma registry of the German Trauma Society
III n.a.
Perkins et al. 2011 Retrospective cohort study
369 Selection***Comparability*Outcome***
8//9 Retrospective review of casual-ties at the military hospital in
Baghdad, Iraq
III n.a.
Nydam et al. 2011 Retrospective cohort study
1415 Selection****Comparability*Outcome***
8/9 A twelve-year single center cohort study
III n.a.
Hussman et al. 2011 Retrospective cohort study
375 Selection****ComparabilityOutcome***
7/9 Patients from trauma registry of the DGU (German Society for
Trauma Surgery)
III n.a.
Nienaber et al. 2011 Retrospective cohort study
36 Selection****ComparabilityOutcome***
7/9 Patients from trauma registry of the DGU (German Society for
Trauma Surgery)
III n.a.
Brakenridge et al. 2011 Prospective cohort study
1366 Selection***Comparability*Outcome***
7/9 Secondary analysis of a large multicenter prospective observa-
tional cohort study
III n.a.
Borgman et al. 2011 Retrospective cohort study
2474 Selection****Comparability*Outcome***
8/9 Multicenter retrospective study from the Trauma Registry of the
German Trauma Society
III n.a.
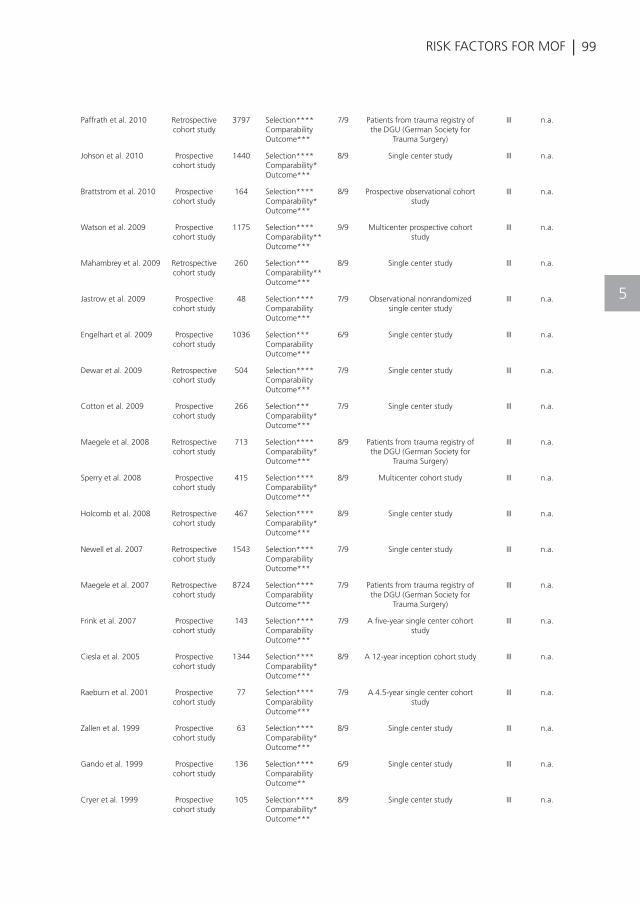
| 99RISK FACTORS FOR MOF
5
Paffrath et al. 2010 Retrospective cohort study
3797 Selection****ComparabilityOutcome***
7/9 Patients from trauma registry of the DGU (German Society for
Trauma Surgery)
III n.a.
Johson et al. 2010 Prospective cohort study
1440 Selection****Comparability*Outcome***
8/9 Single center study III n.a.
Brattstrom et al. 2010 Prospective cohort study
164 Selection****Comparability*Outcome***
8/9 Prospective observational cohort study
III n.a.
Watson et al. 2009 Prospective cohort study
1175 Selection****Comparability**Outcome***
9/9 Multicenter prospective cohort study
III n.a.
Mahambrey et al. 2009 Retrospective cohort study
260 Selection***Comparability**Outcome***
8/9 Single center study III n.a.
Jastrow et al. 2009 Prospective cohort study
48 Selection****ComparabilityOutcome***
7/9 Observational nonrandomized single center study
III n.a.
Engelhart et al. 2009 Prospective cohort study
1036 Selection***ComparabilityOutcome***
6/9 Single center study III n.a.
Dewar et al. 2009 Retrospective cohort study
504 Selection****ComparabilityOutcome***
7/9 Single center study III n.a.
Cotton et al. 2009 Prospective cohort study
266 Selection***Comparability*Outcome***
7/9 Single center study III n.a.
Maegele et al. 2008 Retrospective cohort study
713 Selection****Comparability*Outcome***
8/9 Patients from trauma registry of the DGU (German Society for
Trauma Surgery)
III n.a.
Sperry et al. 2008 Prospective cohort study
415 Selection****Comparability*Outcome***
8/9 Multicenter cohort study III n.a.
Holcomb et al. 2008 Retrospective cohort study
467 Selection****Comparability*Outcome***
8/9 Single center study III n.a.
Newell et al. 2007 Retrospective cohort study
1543 Selection****ComparabilityOutcome***
7/9 Single center study III n.a.
Maegele et al. 2007 Retrospective cohort study
8724 Selection****ComparabilityOutcome***
7/9 Patients from trauma registry of the DGU (German Society for
Trauma Surgery)
III n.a.
Frink et al. 2007 Prospective cohort study
143 Selection****ComparabilityOutcome***
7/9 A five-year single center cohort study
III n.a.
Ciesla et al. 2005 Prospective cohort study
1344 Selection****Comparability*Outcome***
8/9 A 12-year inception cohort study III n.a.
Raeburn et al. 2001 Prospective cohort study
77 Selection****ComparabilityOutcome***
7/9 A 4.5-year single center cohort study
III n.a.
Zallen et al. 1999 Prospective cohort study
63 Selection****Comparability*Outcome***
8/9 Single center study III n.a.
Gando et al. 1999 Prospective cohort study
136 Selection****ComparabilityOutcome**
6/9 Single center study III n.a.
Cryer et al. 1999 Prospective cohort study
105 Selection****Comparability*Outcome***
8/9 Single center study III n.a.
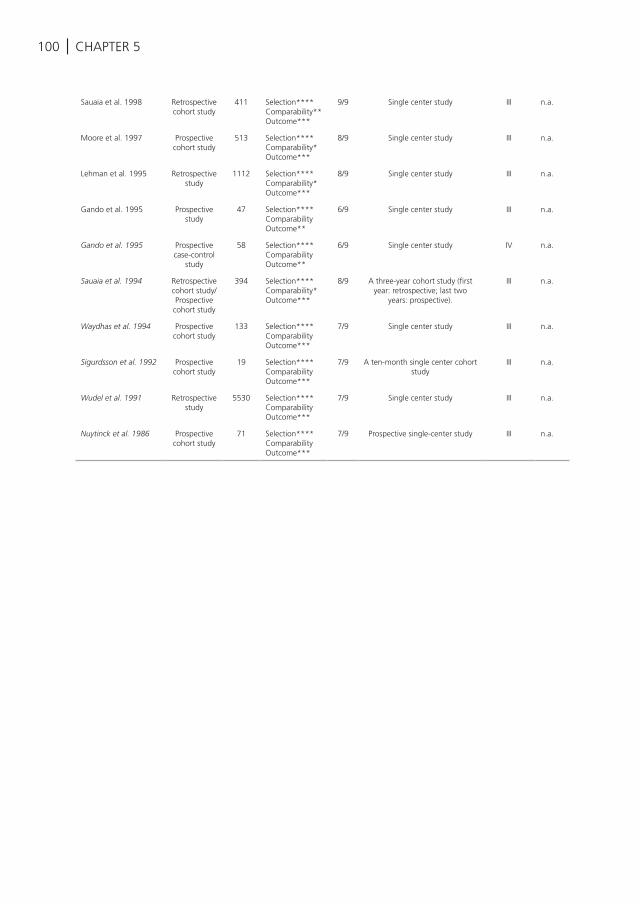
100 | CHAPTER 5
Sauaia et al. 1998 Retrospective cohort study
411 Selection**** Comparability**Outcome***
9/9 Single center study III n.a.
Moore et al. 1997 Prospective cohort study
513 Selection****Comparability*Outcome***
8/9 Single center study III n.a.
Lehman et al. 1995 Retrospective study
1112 Selection****Comparability*Outcome***
8/9 Single center study III n.a.
Gando et al. 1995 Prospective study
47 Selection****ComparabilityOutcome**
6/9 Single center study III n.a.
Gando et al. 1995 Prospective case-control
study
58 Selection****ComparabilityOutcome**
6/9 Single center study IV n.a.
Sauaia et al. 1994 Retrospective cohort study/ Prospective
cohort study
394 Selection****Comparability*Outcome***
8/9 A three-year cohort study (first year: retrospective; last two
years: prospective).
III n.a.
Waydhas et al. 1994 Prospective cohort study
133 Selection****ComparabilityOutcome***
7/9 Single center study III n.a.
Sigurdsson et al. 1992 Prospective cohort study
19 Selection****ComparabilityOutcome***
7/9 A ten-month single center cohort study
III n.a.
Wudel et al. 1991 Retrospective study
5530 Selection****ComparabilityOutcome***
7/9 Single center study III n.a.
Nuytinck et al. 1986 Prospective cohort study
71 Selection****ComparabilityOutcome***
7/9 Prospective single-center study III n.a.
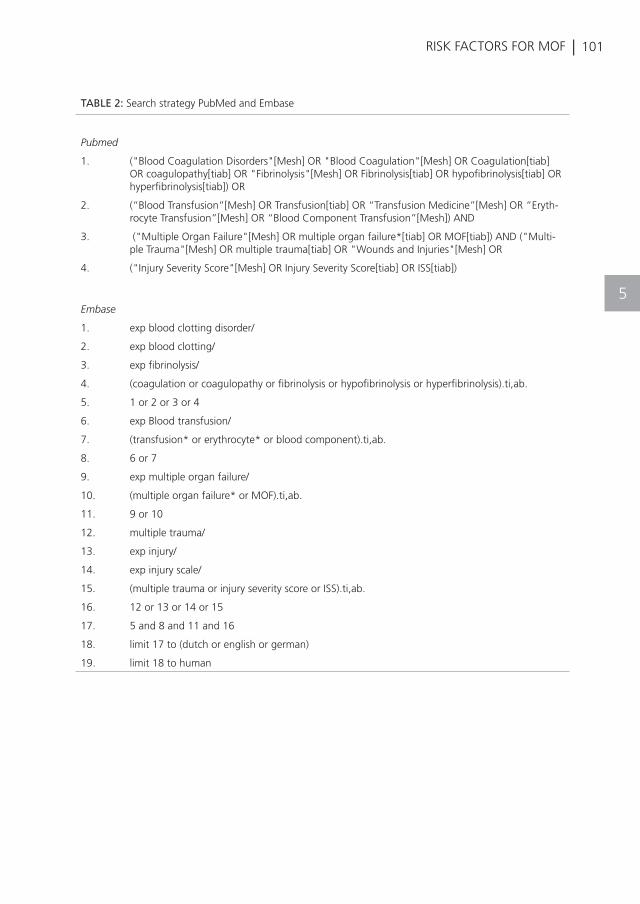
| 101RISK FACTORS FOR MOF
5
TABLE 2: Search strategy PubMed and Embase
Pubmed
1. ("Blood Coagulation Disorders"[Mesh] OR "Blood Coagulation"[Mesh] OR Coagulation[tiab] OR coagulopathy[tiab] OR "Fibrinolysis"[Mesh] OR Fibrinolysis[tiab] OR hypofibrinolysis[tiab] OR hyperfibrinolysis[tiab]) OR
2. (“Blood Transfusion”[Mesh] OR Transfusion[tiab] OR “Transfusion Medicine”[Mesh] OR “Eryth-rocyte Transfusion”[Mesh] OR “Blood Component Transfusion”[Mesh]) AND
3. ("Multiple Organ Failure"[Mesh] OR multiple organ failure*[tiab] OR MOF[tiab]) AND ("Multi-ple Trauma"[Mesh] OR multiple trauma[tiab] OR "Wounds and Injuries"[Mesh] OR
4. ("Injury Severity Score"[Mesh] OR Injury Severity Score[tiab] OR ISS[tiab])
Embase
1. exp blood clotting disorder/
2. exp blood clotting/
3. exp fibrinolysis/
4. (coagulation or coagulopathy or fibrinolysis or hypofibrinolysis or hyperfibrinolysis).ti,ab.
5. 1 or 2 or 3 or 4
6. exp Blood transfusion/
7. (transfusion* or erythrocyte* or blood component).ti,ab.
8. 6 or 7
9. exp multiple organ failure/
10. (multiple organ failure* or MOF).ti,ab.
11. 9 or 10
12. multiple trauma/
13. exp injury/
14. exp injury scale/
15. (multiple trauma or injury severity score or ISS).ti,ab.
16. 12 or 13 or 14 or 15
17. 5 and 8 and 11 and 16
18. limit 17 to (dutch or english or german)
19. limit 18 to human
K. Balvers, M. van der Horst, M. Graumans, C. Boer, J.M. Binnekade, J.C. Goslings, N.P. Juffermans
Journal of Emergencies, Trauma and Shock 2016
HYPOTHERMIA AS A PREDICTOR FOR MORTALITY IN TRAUMA PATIENTS AT ADMITTANCE TO THE
INTENSIVE CARE UNIT
6
104 | CHAPTER 6
ABSTRACT
Introduction: To study the impact of hypothermia upon admission to the Intensive Care Unit (ICU) on early and late mortality and to develop a prediction model for late mortality in severely injured trauma patients.
Methods: A multicenter retrospective cohort study was performed in adult trauma patients admitted to the ICU of two Level-1 trauma centers between 2007 and 2012. Hypothermia was defined as a core body temperature of ≤35° Celsius. Logistic regression analyses were performed to quantify the effect of hypothermia on 24-hour and 28-day mortality and to develop a prediction model.
Results: A total of 953 patients were included, of which 354 patients had hypothermia (37%) upon ICU admission. Patients were divided into a normothermic or hypothermic group. Hypothermia was associated with a significantly increased mortality at 24 hours and 28 days (OR 2.72 (1.18-6.29 and OR 2.82 (1.83-4.35) resp.). The variables included in the final prediction model were hypothermia, age, APACHE II score (corrected for temperature), INR, platelet count, traumatic brain injury and Injury Severity Score. The final prediction model discriminated between survivors and non-survivors with high accuracy (AUC=0.871, 95% CI 0.844-0.898).
Conclusion: Hypothermia, defined as a temperature ≤35° Celsius, is common in critically ill trauma patients and is one of the most important physiological predictors for early and late mortality in trauma patients. Trauma patients admitted to the ICU may be at high risk for late mortality if the patient is hypothermic, coagulopathic, severely injured and has traumatic brain injury or an advanced age.
| 105HYPOTHERMIA AS PREDICTOR FOR MORTALITY
INTRODUCTION
Accidental hypothermia on the Emergency Department (ED) is frequently observed in trauma patients and is associated with poor outcomes1-8, although not all studies provided consistent results9;1. Hypothermia in trauma patients is generally defined as a core body temperature of ≤35° C11. The association with early mortality4-8;12 is thought to occur via deterioration of coagulation abilities13, as hypothermia causes a decreased function of clotting factors and an impaired platelet function14 and is associated with increased blood loss and the transfusion of more blood products4;15. Between time of arrival on the ED and Intensive Care Unit (ICU) admission, stabilization efforts with trauma resuscitation, medication, coiling and damage control surgery may all influence temperature and subsequently may reverse accidental hypothermia. The impact of hypothermia present upon ICU admission on mortality occurring after stabilization efforts is not known. Of note, the occurrence of ‘indoor’ hypothermia was found to be associated with worse outcome than “outdoor” hypothermia in a small study in a medical ICU population16. Transient hypothermia might have a different etiology and outcome compared to persistent hypothermia or hypothermia which occurs during hospital stay. Furthermore, well known prediction models for mortality in trauma patients admitted to the ICU were developed in a non-trauma population or in non-intubated patients, which renders these models less suitable as prediction models for mortality in critically ill trauma patients17-19. Therefore, this study had 2 aims: first to study the incidence and impact of hypothermia on admission to the ICU on early and late mortality, controlling for variables that are associated with trauma-related mortality. Second, to develop a prediction model for late mortality in critically ill trauma patients.
MATERIALS AND METHODS
Study designThis study was a multicentre retrospective cohort study of adult trauma patients admitted to the ED and subsequently transferred to the ICU of two Level 1-trauma centres in Amsterdam, the Netherlands. Patients were recruited between January 2007 and December 2012. All adult trauma patients who were admitted to the ICU and with core temperature measurements available upon ICU admission were eligible. The Institutional Review Board approved the study and waived the need for informed consent.
6
106 | CHAPTER 6
Data collectionData on patient demographics, baseline vitals on ICU admission, injury severity as classified by the Injury Severity Score (ISS), laboratory tests, temperature on ICU admission, NICE score, ICU length of stay, 24-hour and 28-day mortality were collected retrospectively. Demographic data and measures of severity of illness were obtained from the NICE (National Intensive Care Evaluation) database and the electronic patient data management system. The NICE database contains continuous and complete recordings of patients demographics, vital signs, treatment and outcome data of patients who were admitted to the ICU in order to contribute to the quality of Intensive Care Medicine in the Netherlands20. Additionally, all participants of the NICE database are trained in collecting data accurately according to clear defined definitions (www.stichting-nice.nl). The ISS was obtained from the ED registry. Hypothermia was measured by nasopharynx or rectal thermistor temperature probes. Only temperature measurements which were validated by nurses were taken into account for analysis.
Hypothermia was defined as a core temperature of ≤35° C on ICU admission11. Management of hypothermia on the ICU consisted of a warm environment, blankets and active movement (if possible) if the temperature was between 32-35° Celsius. A temperature between 28-32 ° Celsius was managed by a bear hugger and warming of parenteral fluids using a fluido. Extracorporeal membrane oxygenation and cardiopulmonary bypass were added when patients had a temperature below 32° Celsius.
The primary outcome of this study was the mortality rate at 24 hours and 28 days.
Statistical analysisPatients were categorized into a normothermic or hypothermic group. Continuous normally distributed variables are expressed by their mean and standard deviation or when not normally distributed as median and their interquartile ranges. Categorical variables are expressed as n (%). To test group differences, the Students t-test was used, if continuous data are not normally distributed the Mann-Whitney U test was used. Categorical variables are compared with the Chi-square test.
Automatically multiple imputation by logistic regression of data was performed in order to handle missing values, with the exception of missing outcome variables. Reference distribution in the imputated dataset was set equal to the original dataset. Data are represented as pooled values of 10 imputations. The goal of the primary analysis (logistic regression) was to quantify the net effect of hypothermia at admission to the ICU on 24-hour and 28-day mortality, controlling for variables associated with trauma-
| 107HYPOTHERMIA AS PREDICTOR FOR MORTALITY
6
related mortality. Confounders were identified with univariable logistic regression models. Variables included in the univariable logistic regression models were: gender, age, weight, height, traumatic brain injury, ISS, Acute Physiology and Chronic Health Evaluation (APACHE) score corrected for temperature, mean arterial pressure (MAP), haemoglobin (Hb), pH, the total amount of blood products administered and platelet count. Furthermore, interaction terms were added to the logistic regression models to evaluate if hypothermia was a result of the injury mechanism (ISS, presence of head injury) or of resuscitation (the amount of allogeneic blood products transfused). Variables that are part of the APACHE II score were excluded to avoid redundancy in the analysis. Categorization of continuous potential confounders was used to examine linearity between these confounders and 24-hour and 28-day mortality. Square terms or log transformations were used to correct for non-linearity. A p-value of ≤0.2 in the univariable logistic regression models was considered as a relevant confounding effect. Variables with a relevant confounding effect were included in the multivariable logistic regression models as predictors for 24-hour and 28-day mortality by using backward selection. Only those variables with a significant association with mortality after backward selection were included in the final multivariable logistic regression models. A p-value of 0.05 was used as cut-off value for backward selection.
The final logistic regression model for 28-day mortality was used as a prediction model and to generate a formula to predict 28-day mortality. In this formula ß-coefficients of the logistic regression model were used to develop a weighted point system. The Area Under the Curve (AUC) of the Receiver Operating Characteristic (ROC) curve was used to evaluate the discrimination of the final model, the Hosmer-Lemeshow statistic was used to define goodness-of-fit of the model.
Statistical significance is considered to be p <0.05. Appropriate statistical uncertainty was expressed by the 95% confidence levels. Analysis was performed with SPSS Statistics 21 (IBM, Chicago, IL, USA). Methods and results were reported according to the “transparent reporting of a multivariable prediction model for individual prognosis or diagnosis” (TRIPOD) statement21.
RESULTS
Of a total of 953 patients admitted to the ICU, 354 (37%) patients had hypothermia. Table 1 describes the different demographic characteristics of the cohort for the hypothermic and normothermic group. The majority of the patient characteristics were different between both groups. The hypothermic group was more severely injured, coagulopathic, acidotic and had higher mortality rates. Almost 50% of the patients
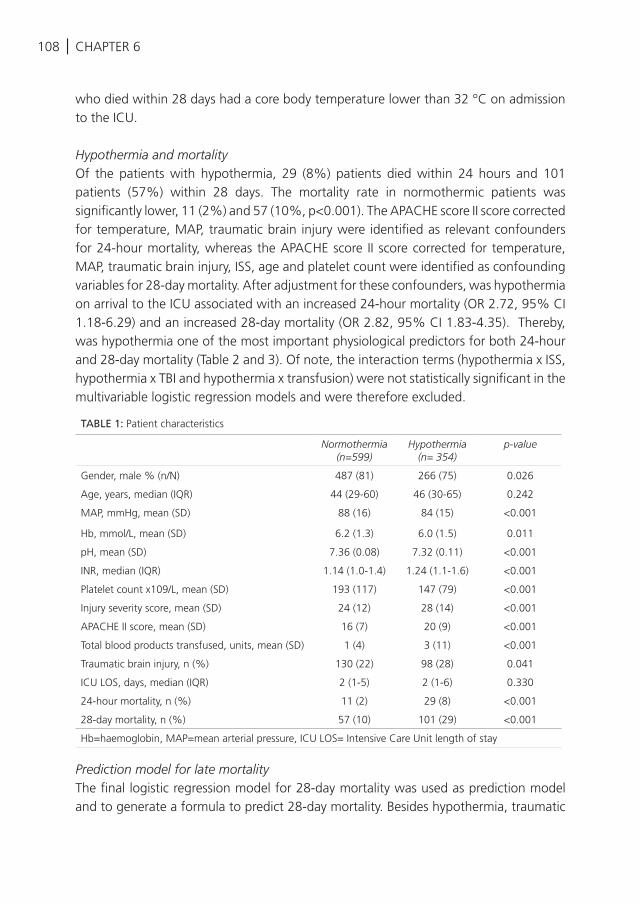
108 | CHAPTER 6
who died within 28 days had a core body temperature lower than 32 °C on admission to the ICU.
Hypothermia and mortalityOf the patients with hypothermia, 29 (8%) patients died within 24 hours and 101 patients (57%) within 28 days. The mortality rate in normothermic patients was significantly lower, 11 (2%) and 57 (10%, p<0.001). The APACHE score II score corrected for temperature, MAP, traumatic brain injury were identified as relevant confounders for 24-hour mortality, whereas the APACHE score II score corrected for temperature, MAP, traumatic brain injury, ISS, age and platelet count were identified as confounding variables for 28-day mortality. After adjustment for these confounders, was hypothermia on arrival to the ICU associated with an increased 24-hour mortality (OR 2.72, 95% CI 1.18-6.29) and an increased 28-day mortality (OR 2.82, 95% CI 1.83-4.35). Thereby, was hypothermia one of the most important physiological predictors for both 24-hour and 28-day mortality (Table 2 and 3). Of note, the interaction terms (hypothermia x ISS, hypothermia x TBI and hypothermia x transfusion) were not statistically significant in the multivariable logistic regression models and were therefore excluded.
Prediction model for late mortality The final logistic regression model for 28-day mortality was used as prediction model and to generate a formula to predict 28-day mortality. Besides hypothermia, traumatic
TABLE 1: Patient characteristics
Normothermia (n=599)
Hypothermia (n= 354)
p-value
Gender, male % (n/N) 487 (81) 266 (75) 0.026
Age, years, median (IQR) 44 (29-60) 46 (30-65) 0.242
MAP, mmHg, mean (SD) 88 (16) 84 (15) <0.001
Hb, mmol/L, mean (SD) 6.2 (1.3) 6.0 (1.5) 0.011
pH, mean (SD) 7.36 (0.08) 7.32 (0.11) <0.001
INR, median (IQR) 1.14 (1.0-1.4) 1.24 (1.1-1.6) <0.001
Platelet count x109/L, mean (SD) 193 (117) 147 (79) <0.001
Injury severity score, mean (SD) 24 (12) 28 (14) <0.001
APACHE II score, mean (SD) 16 (7) 20 (9) <0.001
Total blood products transfused, units, mean (SD) 1 (4) 3 (11) <0.001
Traumatic brain injury, n (%) 130 (22) 98 (28) 0.041
ICU LOS, days, median (IQR) 2 (1-5) 2 (1-6) 0.330
24-hour mortality, n (%) 11 (2) 29 (8) <0.001
28-day mortality, n (%) 57 (10) 101 (29) <0.001
Hb=haemoglobin, MAP=mean arterial pressure, ICU LOS= Intensive Care Unit length of stay
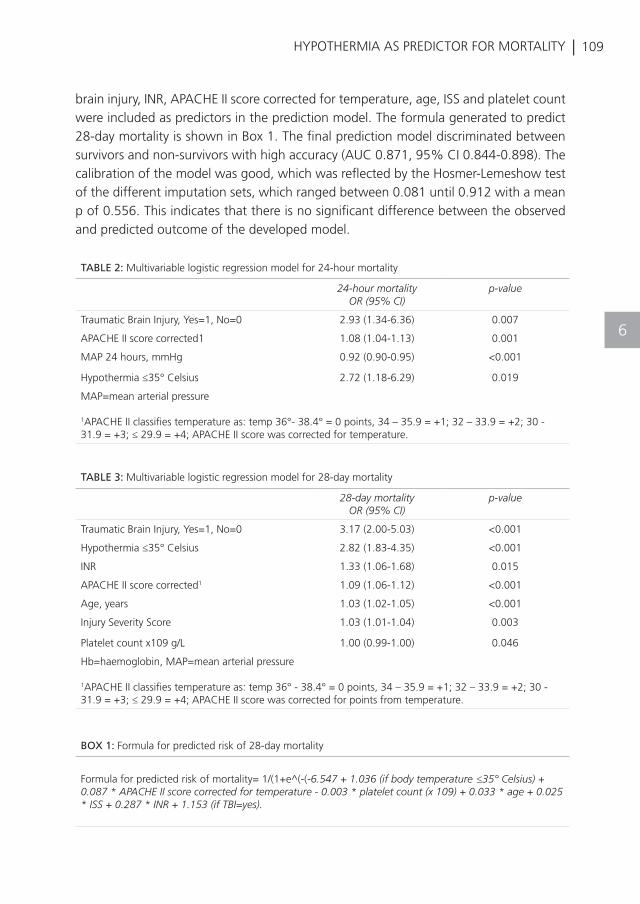
| 109HYPOTHERMIA AS PREDICTOR FOR MORTALITY
6
brain injury, INR, APACHE II score corrected for temperature, age, ISS and platelet count were included as predictors in the prediction model. The formula generated to predict 28-day mortality is shown in Box 1. The final prediction model discriminated between survivors and non-survivors with high accuracy (AUC 0.871, 95% CI 0.844-0.898). The calibration of the model was good, which was reflected by the Hosmer-Lemeshow test of the different imputation sets, which ranged between 0.081 until 0.912 with a mean p of 0.556. This indicates that there is no significant difference between the observed and predicted outcome of the developed model.
TABLE 2: Multivariable logistic regression model for 24-hour mortality
24-hour mortalityOR (95% CI)
p-value
Traumatic Brain Injury, Yes=1, No=0 2.93 (1.34-6.36) 0.007
APACHE II score corrected1 1.08 (1.04-1.13) 0.001
MAP 24 hours, mmHg 0.92 (0.90-0.95) <0.001
Hypothermia ≤35° Celsius 2.72 (1.18-6.29) 0.019
MAP=mean arterial pressure
1APACHE II classifies temperature as: temp 36°- 38.4° = 0 points, 34 – 35.9 = +1; 32 – 33.9 = +2; 30 - 31.9 = +3; ≤ 29.9 = +4; APACHE II score was corrected for temperature.
TABLE 3: Multivariable logistic regression model for 28-day mortality
28-day mortalityOR (95% CI)
p-value
Traumatic Brain Injury, Yes=1, No=0 3.17 (2.00-5.03) <0.001
Hypothermia ≤35° Celsius 2.82 (1.83-4.35) <0.001
INR 1.33 (1.06-1.68) 0.015
APACHE II score corrected1 1.09 (1.06-1.12) <0.001
Age, years 1.03 (1.02-1.05) <0.001
Injury Severity Score 1.03 (1.01-1.04) 0.003
Platelet count x109 g/L 1.00 (0.99-1.00) 0.046
Hb=haemoglobin, MAP=mean arterial pressure
1APACHE II classifies temperature as: temp 36° - 38.4° = 0 points, 34 – 35.9 = +1; 32 – 33.9 = +2; 30 - 31.9 = +3; ≤ 29.9 = +4; APACHE II score was corrected for points from temperature.
BOX 1: Formula for predicted risk of 28-day mortality
Formula for predicted risk of mortality= 1/(1+e^(-(-6.547 + 1.036 (if body temperature ≤35° Celsius) + 0.087 * APACHE II score corrected for temperature - 0.003 * platelet count (x 109) + 0.033 * age + 0.025 * ISS + 0.287 * INR + 1.153 (if TBI=yes).

110 | CHAPTER 6
DISCUSSION
This study shows that upon ICU admission following trauma, hypothermia is frequently present and is one of the most important physiological predictors for both early and late mortality in trauma patients. Other predictors for late mortality are age, APACHE II score corrected for temperature, INR, platelet count 109/L, traumatic brain injury and ISS. A prediction model, which combines these independent predictors, may be able to identify trauma patients at high risk for late mortality on ICU admission.
HypothermiaThe present study found that hypothermia on ICU admission is common in trauma patients. More than one third of the critically ill trauma patients in this study had hypothermia on arrival at the ICU. Similar results are found in studies investigating the incidence of hypothermia on the ED5;10. These findings suggest that therapy on the ED may not be focused on prevention or correction of hypothermia. Obviously, the focus of therapy in severely injured patients is on efforts to stop the bleeding and to protect the patient from further injury by failure of oxygenation of vital signs or central nervous system, which requires multiple actions and interventions. Hypothermia may aggravate bleeding and therefore management of body temperature is part of trauma management protocols22. However, body core temperature is collected in 30% -60%6;23;24 of the trauma patients upon admission to the ED. Thereby, screening of body core temperature may be regarded as less important in the care of trauma patients. An alternative explanation for the high incidence of hypothermia upon ICU admission may be that it is not feasible to correct core body temperature, as interventions may require that the patient is (partly) uncovered and that treatment and surgical procedures may further cool the patient25, even when devices with warm resuscitation fluids or other rewarming techniques are applied.
Hypothermia and mortalityWe have, in contrast to previous studies, examined accidental hypothermia upon admission to the ICU instead of on admission to the ED. The effect of accidental hypothermia at ICU admission on mortality is less well documented, and may be influenced by stabilization efforts during trauma resuscitation. Therefore the clinical significance of hypothermia may be different between these two time points. We found that hypothermia on ICU admission was associated with an increased mortality. This is in line with the results of two previous studies26;27]. Furthermore, we observed that hypothermia was more frequently observed in patients with TBI and in transfused patients, which suggests that hypothermia is merely a result of the injury severity, traumatic brain injury or transfusion of blood products than an independent predictor
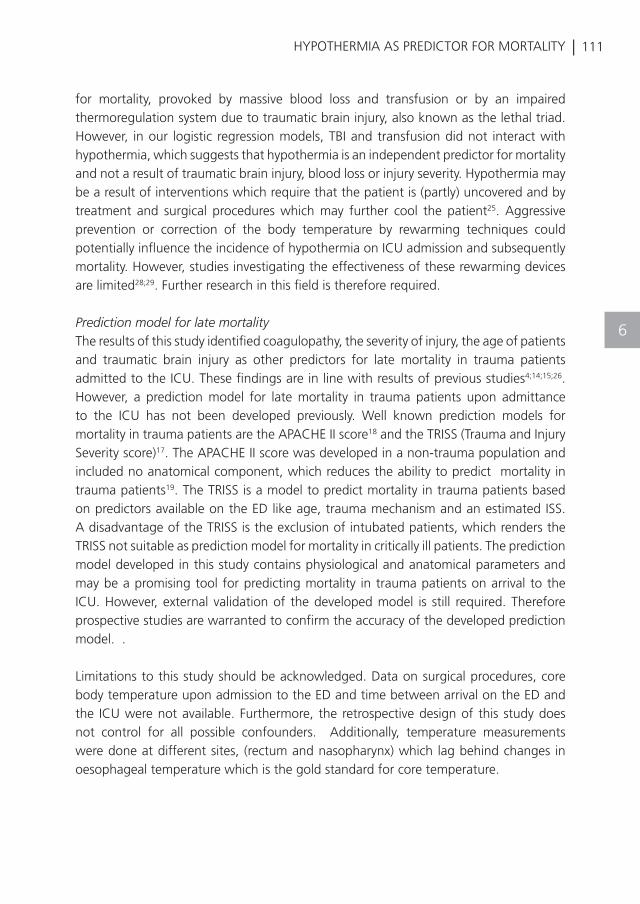
| 111HYPOTHERMIA AS PREDICTOR FOR MORTALITY
6
for mortality, provoked by massive blood loss and transfusion or by an impaired thermoregulation system due to traumatic brain injury, also known as the lethal triad. However, in our logistic regression models, TBI and transfusion did not interact with hypothermia, which suggests that hypothermia is an independent predictor for mortality and not a result of traumatic brain injury, blood loss or injury severity. Hypothermia may be a result of interventions which require that the patient is (partly) uncovered and by treatment and surgical procedures which may further cool the patient25. Aggressive prevention or correction of the body temperature by rewarming techniques could potentially influence the incidence of hypothermia on ICU admission and subsequently mortality. However, studies investigating the effectiveness of these rewarming devices are limited28;29. Further research in this field is therefore required.
Prediction model for late mortality The results of this study identified coagulopathy, the severity of injury, the age of patients and traumatic brain injury as other predictors for late mortality in trauma patients admitted to the ICU. These findings are in line with results of previous studies4;14;15;26. However, a prediction model for late mortality in trauma patients upon admittance to the ICU has not been developed previously. Well known prediction models for mortality in trauma patients are the APACHE II score18 and the TRISS (Trauma and Injury Severity score)17. The APACHE II score was developed in a non-trauma population and included no anatomical component, which reduces the ability to predict mortality in trauma patients19. The TRISS is a model to predict mortality in trauma patients based on predictors available on the ED like age, trauma mechanism and an estimated ISS. A disadvantage of the TRISS is the exclusion of intubated patients, which renders the TRISS not suitable as prediction model for mortality in critically ill patients. The prediction model developed in this study contains physiological and anatomical parameters and may be a promising tool for predicting mortality in trauma patients on arrival to the ICU. However, external validation of the developed model is still required. Therefore prospective studies are warranted to confirm the accuracy of the developed prediction model. .
Limitations to this study should be acknowledged. Data on surgical procedures, core body temperature upon admission to the ED and time between arrival on the ED and the ICU were not available. Furthermore, the retrospective design of this study does not control for all possible confounders. Additionally, temperature measurements were done at different sites, (rectum and nasopharynx) which lag behind changes in oesophageal temperature which is the gold standard for core temperature.

112 | CHAPTER 6
CONCLUSION
In conclusion, hypothermia, defined as a temperature ≤35°C, is common in trauma patients upon ICU admission and is associated with increased mortality. Hypothermic trauma patients admitted to the ICU may be at high risk for late mortality if the patient is also coagulopathic, severely injured, has traumatic brain injury or an advanced age.
| 113HYPOTHERMIA AS PREDICTOR FOR MORTALITY
6

114 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Reynolds BR, Forsythe RM, Harbrecht BG,
Cuschieri J, Minei JP, Maier RV, Moore EE,
Billiar EE, Peitzman AB, Sperry JL. Hypothermia
in massive transfusion: have we been paying
enough attention to it? J Trauma Acute Care
Surg.2012;73:486-91.
Beilman GJ, Blondet JJ, Nelson TR, Nathens
AB, Moore FA, Rhee P, Puyana JC, Moore EE,
Cohn SM. Early hypothermia in severely injured
trauma patients is a significant risk factor for
multiple organ dysfunction syndrome but not
mortality. Ann Surg.2009;249:845-50.
Rubiano AM, Sanchez AI, Estebanez G,
Peitzman A, Sperry J, Puyana JC. The effect
of admission spontaneous hypothermia on
patients with severe traumatic brain injury.
Injury.2013;44:1219-25.
Bukur M, Hadjibashi AA, Ley EJ, Malinoski D,
Singer M, Barmparas G, Margulies D, Salim
A. Impact of prehospital hypothermia on
transfusion requirements and outcomes. J
Trauma Acute Care Surg.2012;73:1195-201.
Ireland S, Endacott R, Cameron P, Fitzgerald
M, Paul E. The incidence and significance
of accidental hypothermia in major
trauma--a prospective observational study.
Resuscitation.2011;82:300-6.
Martin RS, Kilgo PD, Miller PR, Hoth JJ,
Meredith JW, Chang MC. Injury-associated
hypothermia: an analysis of the 2004 National
Trauma Data Bank. Shock.2005;24:114-8.
Shafi S, Elliott AC, Gentilello L. Is hypothermia
simply a marker of shock and injury severity
or an independent risk factor for mortality in
trauma patients? Analysis of a large national
trauma registry. J Trauma.2005;59:1081-5.
Wang HE, Callaway CW, Peitzman AB,
Tisherman SA. Admission hypothermia and
outcome after major trauma. Crit Care
Med.2005;33:1296-301.
van der Ploeg GJ, Goslings JC, Walpoth
BH, Bierens JJ. Accidental hypothermia:
rewarming treatments, complications and
outcomes from one university medical centre.
Resuscitation.2010;81:1550-5.
Mommsen P, Andruszkow H, Fromke C,
Zeckey C, Wagner U, van GM, Frink M,
Krettek C, Hildebrand F. Effects of accidental
hypothermia on posttraumatic complications
and outcome in multiple trauma patients.
Injury.2013;44:86-90.
Soar J, Perkins GD, Abbas G, Alfonzo A,
Barelli A, Bierens JJ, Brugger H, Deakin CD,
Dunning J, Georgiou M, Handley AJ, Lockey
DJ, Paal P, Sandroni C, Thies KC, Zideman
DA, Nolan JP. European Resuscitation
Council Guidelines for Resuscitation
2010 Section 8. Cardiac arrest in special
circumstances: Electrolyte abnormalities,
poisoning, drowning, accidental hypothermia,
hyperthermia, asthma, anaphylaxis, cardiac
surgery, trauma, pregnancy, electrocution.
Resuscitation.2010;81:1400-33.
Hildebrand F, Giannoudis PV, van GM, Chawda
M, Pape HC. Pathophysiologic changes
and effects of hypothermia on outcome in
elective surgery and trauma patients. Am J
Surg.2004;187:363-71.
Mikhail J. The trauma triad of death:
hypothermia, acidosis, and coagulopathy.
AACN Clin Issues.1999;10:85-94.
Zhang JN, Wood J, Bergeron AL, McBride L,
Ball C, Yu Q, Pusiteri AE, Holcomb JB, Dong
JF. Effects of low temperature on shear-
induced platelet aggregation and activation. J
Trauma.2004;57:216-23.
Rajagopalan S, Mascha E, Na J, Sessler DI.
The effects of mild perioperative hypothermia
on blood loss and transfusion requirement.
Anesthesiology.2008;108:71-7.
Megarbane B, Axler O, Chary I, Pompier R,
Brivet FG. Hypothermia with indoor occurrence
is associated with a worse outcome. Intensive
Care Med.2000;26:1843-9.
Boyd CR, Tolson MA, Copes WS. Evaluating
trauma care: the TRISS method. Trauma
Score and the Injury Severity Score. J
Trauma.1987;27:370-8.
CHAPTER 6
| 115
REFERENCES
HYPOTHERMIA AS PREDICTOR FOR MORTALITY
18
19
20
21
22
23
24
25
26
27
28
29
Knaus WA, Draper EA, Wagner DP,
Zimmerman JE. APACHE II: a severity of
disease classification system. Crit Care
Med.1985;13:818-29.
McAnena OJ, Moore FA, Moore EE, Mattox KL,
Marx JA, Pepe P. Invalidation of the APACHE II
scoring system for patients with acute trauma.
J Trauma.1992;33:504-6.
Arts D, de KN, Scheffer GJ, de JE. Quality
of data collected for severity of illness
scores in the Dutch National Intensive Care
Evaluation (NICE) registry. Intensive Care
Med.2002;28:656-9.
Collins G, Reitsma J, Altman D, Moons K.
Transparent Reporting of a Multivariable
Prediction Model for Individual Prognosis or
Diagnosis (TRIPOD): the TRIPOD statement.
BJOG.2015;122:434-43.
American College of Surgeons Committee
on Trauma. Advanced Trauma Life Support;
Student Course Manual. 9th ed. Chicago:
2012.
Trentzsch H, Huber-Wagner S, Hildebrand
F, Kanz KG, Faist E, Piltz S, Lefering R.
Hypothermia for prediction of death in
severely injured blunt trauma patients.
Shock.2012;37:131-9.
Langhelle A, Lockey D, Harris T, Davies G. Body
temperature of trauma patients on admission
to hospital: a comparison of anaesthetised
and non-anaesthetised patients. Emerg Med
J.2012;29:239-42.
Hirshberg A, Sheffer N, Barnea O.
Computer simulation of hypothermia during
“damage control” laparotomy. World J
Surg.1999;23:960-5.
Konstantinidis A, Inaba K, Dubose J, Barmparas
G, Talving P, David JS, Lam L, Demetriades D.
The impact of nontherapeutic hypothermia on
outcomes after severe traumatic brain injury. J
Trauma.2011;71:1627-31.
Rutherford EJ, Fusco MA, Nunn CR, Bass JG,
Eddy VA, Morris JA, Jr. Hypothermia in critically
ill trauma patients. Injury.1998;29:605-8.
Steele MT, Nelson MJ, Sessler DI, Fraker
L, Bunney B, Watson WA, Robinson WA.
Forced air speeds rewarming in accidental
hypothermia. Ann Emerg Med.1996;27:479-
84.
Gentilello LM, Jurkovich GJ, Stark MS,
Hassantash SA, O’Keefe GE. Is hypothermia
in the victim of major trauma protective or
harmful? A randomized, prospective study.
Ann Surg.1997;226:439-47.
6
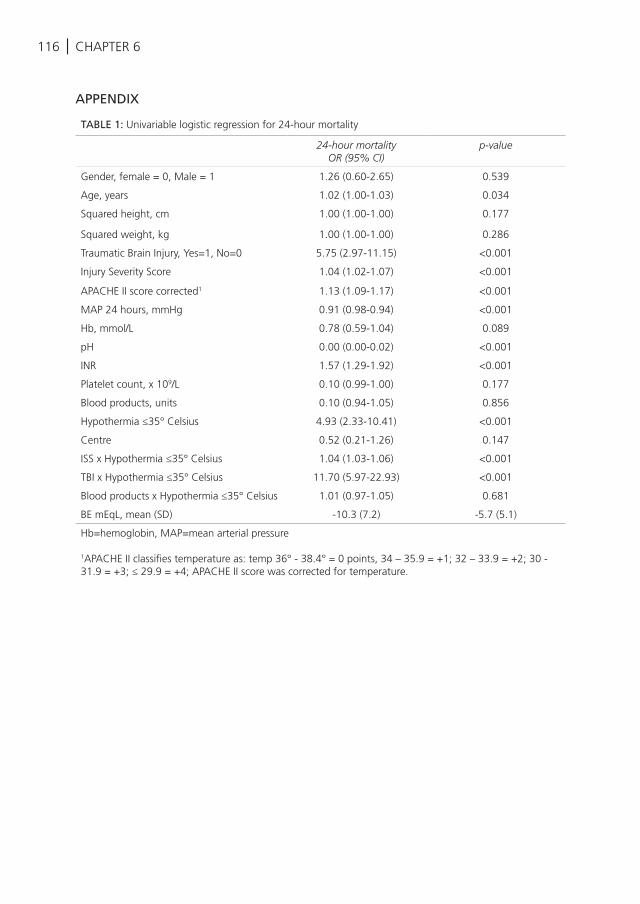
116 | CHAPTER 6
APPENDIX
TABLE 1: Univariable logistic regression for 24-hour mortality
24-hour mortalityOR (95% CI)
p-value
Gender, female = 0, Male = 1 1.26 (0.60-2.65) 0.539
Age, years 1.02 (1.00-1.03) 0.034
Squared height, cm 1.00 (1.00-1.00) 0.177
Squared weight, kg 1.00 (1.00-1.00) 0.286
Traumatic Brain Injury, Yes=1, No=0 5.75 (2.97-11.15) <0.001
Injury Severity Score 1.04 (1.02-1.07) <0.001
APACHE II score corrected1 1.13 (1.09-1.17) <0.001
MAP 24 hours, mmHg 0.91 (0.98-0.94) <0.001
Hb, mmol/L 0.78 (0.59-1.04) 0.089
pH 0.00 (0.00-0.02) <0.001
INR 1.57 (1.29-1.92) <0.001
Platelet count, x 109/L 0.10 (0.99-1.00) 0.177
Blood products, units 0.10 (0.94-1.05) 0.856
Hypothermia ≤35° Celsius 4.93 (2.33-10.41) <0.001
Centre 0.52 (0.21-1.26) 0.147
ISS x Hypothermia ≤35° Celsius 1.04 (1.03-1.06) <0.001
TBI x Hypothermia ≤35° Celsius 11.70 (5.97-22.93) <0.001
Blood products x Hypothermia ≤35° Celsius 1.01 (0.97-1.05) 0.681
BE mEqL, mean (SD) -10.3 (7.2) -5.7 (5.1)
Hb=hemoglobin, MAP=mean arterial pressure
1APACHE II classifies temperature as: temp 36° - 38.4° = 0 points, 34 – 35.9 = +1; 32 – 33.9 = +2; 30 - 31.9 = +3; ≤ 29.9 = +4; APACHE II score was corrected for temperature.
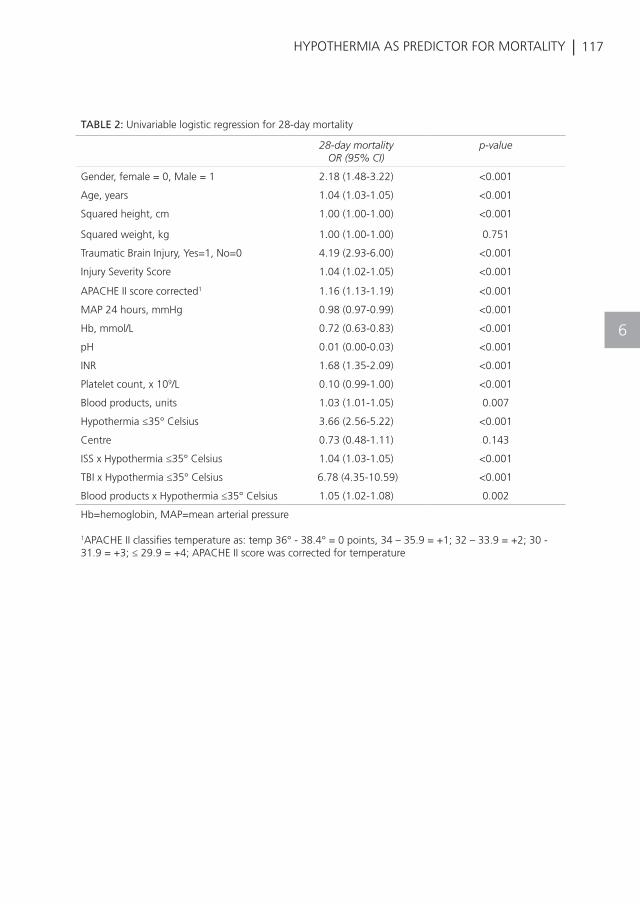
| 117HYPOTHERMIA AS PREDICTOR FOR MORTALITY
6
TABLE 2: Univariable logistic regression for 28-day mortality
28-day mortalityOR (95% CI)
p-value
Gender, female = 0, Male = 1 2.18 (1.48-3.22) <0.001
Age, years 1.04 (1.03-1.05) <0.001
Squared height, cm 1.00 (1.00-1.00) <0.001
Squared weight, kg 1.00 (1.00-1.00) 0.751
Traumatic Brain Injury, Yes=1, No=0 4.19 (2.93-6.00) <0.001
Injury Severity Score 1.04 (1.02-1.05) <0.001
APACHE II score corrected1 1.16 (1.13-1.19) <0.001
MAP 24 hours, mmHg 0.98 (0.97-0.99) <0.001
Hb, mmol/L 0.72 (0.63-0.83) <0.001
pH 0.01 (0.00-0.03) <0.001
INR 1.68 (1.35-2.09) <0.001
Platelet count, x 109/L 0.10 (0.99-1.00) <0.001
Blood products, units 1.03 (1.01-1.05) 0.007
Hypothermia ≤35° Celsius 3.66 (2.56-5.22) <0.001
Centre 0.73 (0.48-1.11) 0.143
ISS x Hypothermia ≤35° Celsius 1.04 (1.03-1.05) <0.001
TBI x Hypothermia ≤35° Celsius 6.78 (4.35-10.59) <0.001
Blood products x Hypothermia ≤35° Celsius 1.05 (1.02-1.08) 0.002
Hb=hemoglobin, MAP=mean arterial pressure
1APACHE II classifies temperature as: temp 36° - 38.4° = 0 points, 34 – 35.9 = +1; 32 – 33.9 = +2; 30 - 31.9 = +3; ≤ 29.9 = +4; APACHE II score was corrected for temperature
K. Balvers, M. Coppens, S. van Dieren, I.H.M. Rooyen van-Schreurs, J.H. Klinkspoor, S.S. Zeerleder, H.M. Baumann, J.C. Goslings, N.P. Juffermans
Journal of Emergencies, Trauma and Shock 2015
EFFECTS OF A HOSPITAL-WIDE INTRODUCTION OF A MASSIVE TRANSFUSION PROTOCOL ON BLOOD
PRODUCT RATIO AND BLOOD PRODUCT WASTE
7
120 | CHAPTER 7
ABSTRACT
Background: Massive transfusion protocols (MTPs) are increasingly used in the transfusion practice and are developed to provide the standardized and early delivery of blood products and procoagulant agents and to supply the transfusion of blood products in a well-balanced ratio. The aim of this study was to investigate the effect of a hospital-wide introduction of an MTP on blood product ratio and a waste of blood products.
Methods: A retrospective analysis was performed to compare the transfusion practice in massive bleeding patients before and after the introduction of an MTP and between the use of an MTP and transfusion off-protocol. Massive bleeding was defined as an administration of ≥5 units of red blood cells (RBCs) within 12 h.
Results: Of 547 massively transfused patients, 192 patients were included in the pre-MTP period and 355 patients in the MTP period. The ratio of RBC to fresh frozen plasma (FFP) and the platelets transfused shifted significantly toward 1:1:1 in the MTP period (P = 0.012). This was mainly caused by a shift in RBC: FFP ratio (P = 0.014). An increase in the waste of blood products was observed, most notably FFPs (P = 0.026). Extending the storage time after thawing reduced the waste of FFPs from 11% to 4%.
Conclusion: Hospital-wide introduction of an MTP is an adequate way to achieve a well-balanced transfusion ratio of 1:1:1. This comes at the cost of an increase in the waste of FFPs, which is lowered after extending the duration of storage time after thawing.
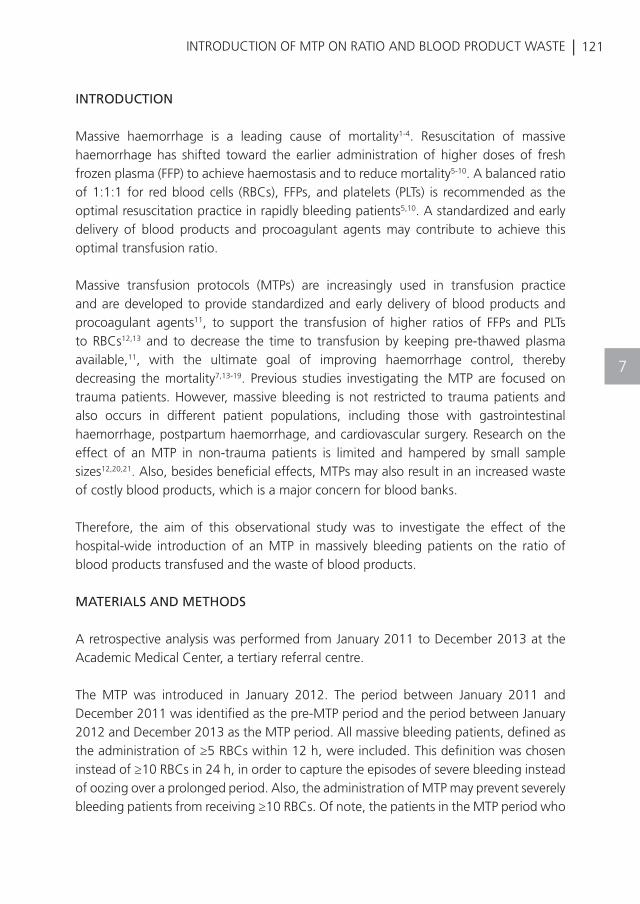
| 121INTRODUCTION OF MTP ON RATIO AND BLOOD PRODUCT WASTE
7
INTRODUCTION
Massive haemorrhage is a leading cause of mortality1-4. Resuscitation of massive haemorrhage has shifted toward the earlier administration of higher doses of fresh frozen plasma (FFP) to achieve haemostasis and to reduce mortality5-10. A balanced ratio of 1:1:1 for red blood cells (RBCs), FFPs, and platelets (PLTs) is recommended as the optimal resuscitation practice in rapidly bleeding patients5,10. A standardized and early delivery of blood products and procoagulant agents may contribute to achieve this optimal transfusion ratio.
Massive transfusion protocols (MTPs) are increasingly used in transfusion practice and are developed to provide standardized and early delivery of blood products and procoagulant agents11, to support the transfusion of higher ratios of FFPs and PLTs to RBCs12,13 and to decrease the time to transfusion by keeping pre-thawed plasma available,11, with the ultimate goal of improving haemorrhage control, thereby decreasing the mortality7,13-19. Previous studies investigating the MTP are focused on trauma patients. However, massive bleeding is not restricted to trauma patients and also occurs in different patient populations, including those with gastrointestinal haemorrhage, postpartum haemorrhage, and cardiovascular surgery. Research on the effect of an MTP in non-trauma patients is limited and hampered by small sample sizes12,20,21. Also, besides beneficial effects, MTPs may also result in an increased waste of costly blood products, which is a major concern for blood banks.
Therefore, the aim of this observational study was to investigate the effect of the hospital-wide introduction of an MTP in massively bleeding patients on the ratio of blood products transfused and the waste of blood products.
MATERIALS AND METHODS
A retrospective analysis was performed from January 2011 to December 2013 at the Academic Medical Center, a tertiary referral centre.
The MTP was introduced in January 2012. The period between January 2011 and December 2011 was identified as the pre-MTP period and the period between January 2012 and December 2013 as the MTP period. All massive bleeding patients, defined as the administration of ≥5 RBCs within 12 h, were included. This definition was chosen instead of ≥10 RBCs in 24 h, in order to capture the episodes of severe bleeding instead of oozing over a prolonged period. Also, the administration of MTP may prevent severely bleeding patients from receiving ≥10 RBCs. Of note, the patients in the MTP period who
122 | CHAPTER 7
were massive bleeding and required ≥5 RBCs, but for whom the MTP was not activated, were termed as massive transfusions off-protocol. Comparisons were made between the pre-MTP period and the MTP period, and between the use of MTP and transfusion off-protocol.
Transfusion strategiesIn the pre-MTP period, the patients with a suspected massive bleeding, with low haemoglobin levels (<8 g/dL) and in shock were transfused with leucoreduced RBCs, FFPs, PLTs, and procoagulant agents as deemed appropriate by the treating physician. FFPs were issued by the blood bank after the requested units were fully thawed. Recombinant factor VIIa (rVIIa) and fibrinogen were administered when a patient was still bleeding after gaining the surgical source control.
After the introduction, the MTP was activated for the patients with a systolic blood pressure <90 mmHg without the response to fluid administration and a suspicion of a massive bleeding due to any cause. Activation of the MTP provides an immediate delivery of 6 RBC units, 6 pre-thawed FFP units, and 2 PLT units (one unit is pooled from 5 donors) with the aim to administer blood products in a ratio of 1:1:1. Laboratory targets for resuscitation were a haemoglobin level of 8-10 g/dL, PT/APTT <1.5-fold extended, PLT count of 50-100 109/L, and a fibrinogen level >1.5 g/L. Additional treatment targets were normothermia (>35°C), pH level >7.25, oxygen saturation of 95% and normovolemia (base excess (BE) > −6, and a systolic blood pressure >90 mmHg). If a patient was still bleeding diffusely after gaining surgical source control while the temperature, pH, and BE were normal, rVIIa was administered together with PLTs and fibrinogen. Six units of FFPs were kept pre-thawed for 72 h, after which they were discarded if unused. Furthermore, RBCs units and thawed plasma were discarded when not returned to the blood bank within 8 h after MTP activation; PLTs were discarded when not returned within 2 h. Blood products were also discarded after exceeding the expiration date (RBC >35 days, PLT >7 days).
Data collectionA prospectively collected blood bank transfusion database was used to determine the frequency for all products issued, as well as the number of products transfused and wasted. Patient characteristics, comorbidities, the use of anticoagulant medication and the first laboratory tests, use of procoagulant agents, length of hospital stay, length of Intensive Care Unit stay, 24-h mortality, and 28-day mortality were collected from an electronic medical record. The primary outcome of this study was the ratio of blood products transfused (RBC: FFP:PLT). The secondary outcome was the waste of blood products.
| 123INTRODUCTION OF MTP ON RATIO AND BLOOD PRODUCT WASTE
7
Statistical analysisFor continuous variables, the normality assumption was tested by visually inspecting the histograms and using the Kolmogorov-Smirnov test. When the normality assumption was met, the Student’s t-tests were used. Otherwise Mann-Whitney U-test was applied to test for differences between the pre-MTP and the MTP group or between the use of MTP and transfusion off-protocol. Categorical variables were compared using the Chi-square test. To determine the waste of blood products following the introduction of the MTP, a subgroup analysis was performed on all the patients for whom the MTP was activated (whether massive bleeding or not).
RESULTS
A total of 639 patients were screened, of which 547 patients met the inclusion criteria, with 192 patients in the pre-MTP period and 355 patients in the MTP period. The majority of these included patients were non-trauma patients (91%). Of note, from the total of 207 MTP activations, 56% turned out to be massively bleeding [Figure 1]. Patient characteristics and first laboratory results after bleeding are shown in Table 1. Patients before and after MTP introduction did not differ in patient characteristics.
To further delineate effects of MTP, we also compared massively bleeding patients who were transfused according to the MTP with massive bleeding patients who were transfused off-protocol. Of the 447 patients in the MTP period, 240 patients received ≥5 RBCs off-protocol [Figure 1]. We were not able to retrieve the reasons why patients were transfused off-protocol. Of note, the patients for whom the MTP was activated were more acidotic compared to bleeding patients who were transfused off-protocol [Table 2].
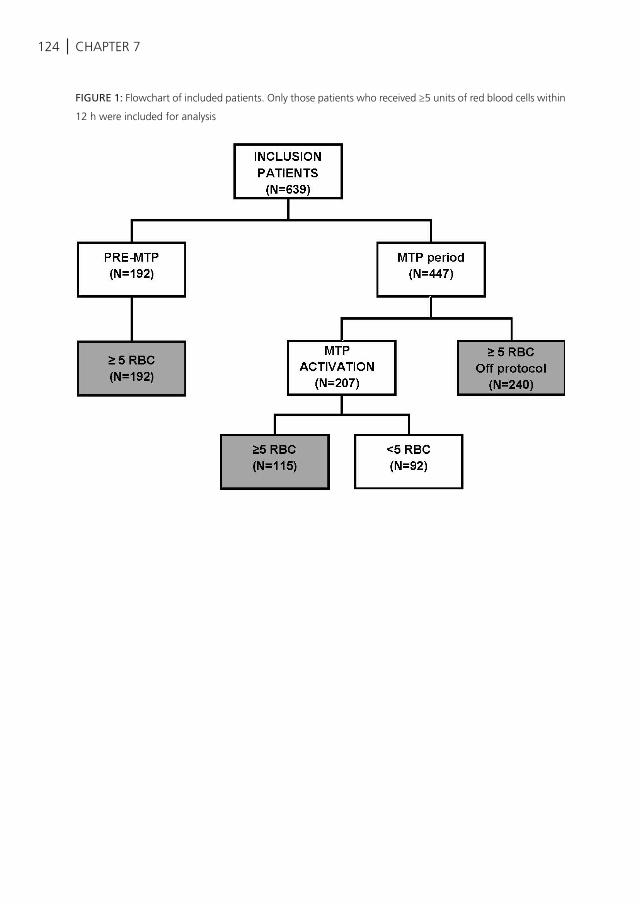
124 | CHAPTER 7
FIGURE 1: Flowchart of included patients. Only those patients who received ≥5 units of red blood cells within
12 h were included for analysis
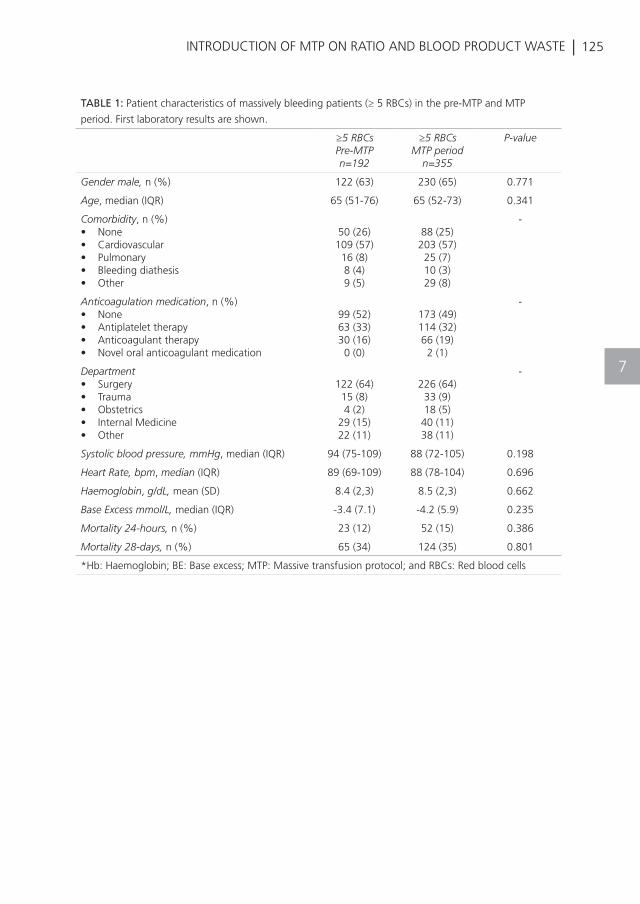
| 125INTRODUCTION OF MTP ON RATIO AND BLOOD PRODUCT WASTE
7
TABLE 1: Patient characteristics of massively bleeding patients (≥ 5 RBCs) in the pre-MTP and MTP
period. First laboratory results are shown.
≥5 RBCsPre-MTPn=192
≥5 RBCsMTP period
n=355
P-value
Gender male, n (%) 122 (63) 230 (65) 0.771
Age, median (IQR) 65 (51-76) 65 (52-73) 0.341
Comorbidity, n (%)• None• Cardiovascular• Pulmonary• Bleeding diathesis• Other
50 (26)109 (57)16 (8)8 (4)9 (5)
88 (25)203 (57)25 (7)10 (3)29 (8)
-
Anticoagulation medication, n (%)• None• Antiplatelet therapy• Anticoagulant therapy• Novel oral anticoagulant medication
99 (52)63 (33)30 (16)0 (0)
173 (49)114 (32)66 (19)2 (1)
-
Department • Surgery• Trauma• Obstetrics• Internal Medicine• Other
122 (64)15 (8)4 (2)
29 (15)22 (11)
226 (64)33 (9)18 (5)40 (11)38 (11)
-
Systolic blood pressure, mmHg, median (IQR) 94 (75-109) 88 (72-105) 0.198
Heart Rate, bpm, median (IQR) 89 (69-109) 88 (78-104) 0.696
Haemoglobin, g/dL, mean (SD) 8.4 (2,3) 8.5 (2,3) 0.662
Base Excess mmol/L, median (IQR) -3.4 (7.1) -4.2 (5.9) 0.235
Mortality 24-hours, n (%) 23 (12) 52 (15) 0.386
Mortality 28-days, n (%) 65 (34) 124 (35) 0.801
*Hb: Haemoglobin; BE: Base excess; MTP: Massive transfusion protocol; and RBCs: Red blood cells
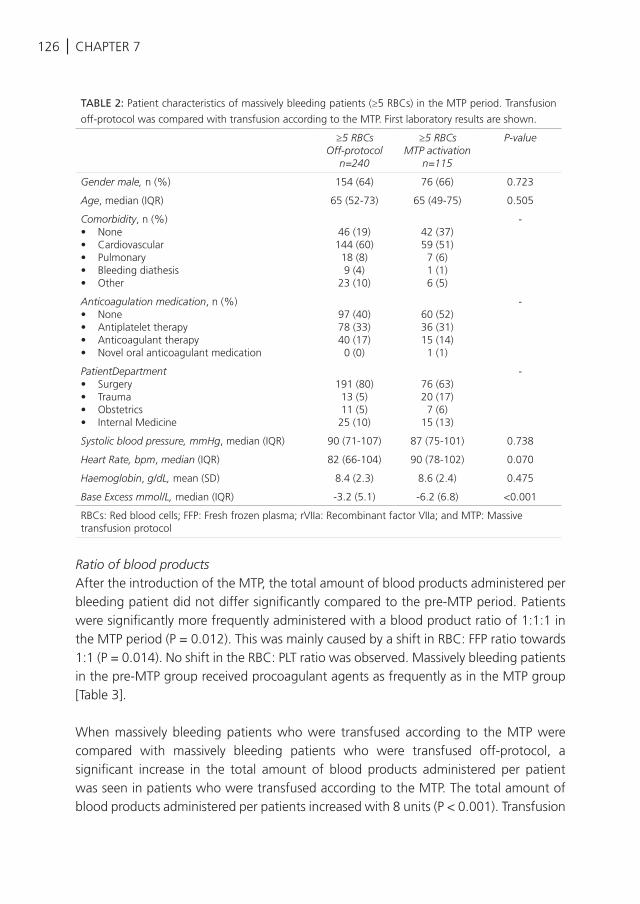
126 | CHAPTER 7
Ratio of blood productsAfter the introduction of the MTP, the total amount of blood products administered per bleeding patient did not differ significantly compared to the pre-MTP period. Patients were significantly more frequently administered with a blood product ratio of 1:1:1 in the MTP period (P = 0.012). This was mainly caused by a shift in RBC: FFP ratio towards 1:1 (P = 0.014). No shift in the RBC: PLT ratio was observed. Massively bleeding patients in the pre-MTP group received procoagulant agents as frequently as in the MTP group [Table 3].
When massively bleeding patients who were transfused according to the MTP were compared with massively bleeding patients who were transfused off-protocol, a significant increase in the total amount of blood products administered per patient was seen in patients who were transfused according to the MTP. The total amount of blood products administered per patients increased with 8 units (P < 0.001). Transfusion
TABLE 2: Patient characteristics of massively bleeding patients (≥5 RBCs) in the MTP period. Transfusion
off-protocol was compared with transfusion according to the MTP. First laboratory results are shown.
≥5 RBCsOff-protocol
n=240
≥5 RBCsMTP activation
n=115
P-value
Gender male, n (%) 154 (64) 76 (66) 0.723
Age, median (IQR) 65 (52-73) 65 (49-75) 0.505
Comorbidity, n (%)• None• Cardiovascular• Pulmonary• Bleeding diathesis• Other
46 (19)144 (60)18 (8)9 (4)
23 (10)
42 (37)59 (51)7 (6)1 (1)6 (5)
-
Anticoagulation medication, n (%)• None• Antiplatelet therapy• Anticoagulant therapy• Novel oral anticoagulant medication
97 (40)78 (33)40 (17)0 (0)
60 (52)36 (31)15 (14)1 (1)
-
PatientDepartment • Surgery• Trauma• Obstetrics• Internal Medicine
191 (80)13 (5)11 (5)25 (10)
76 (63)20 (17)7 (6)
15 (13)
-
Systolic blood pressure, mmHg, median (IQR) 90 (71-107) 87 (75-101) 0.738
Heart Rate, bpm, median (IQR) 82 (66-104) 90 (78-102) 0.070
Haemoglobin, g/dL, mean (SD) 8.4 (2.3) 8.6 (2.4) 0.475
Base Excess mmol/L, median (IQR) -3.2 (5.1) -6.2 (6.8) <0.001
RBCs: Red blood cells; FFP: Fresh frozen plasma; rVIIa: Recombinant factor VIIa; and MTP: Massive transfusion protocol
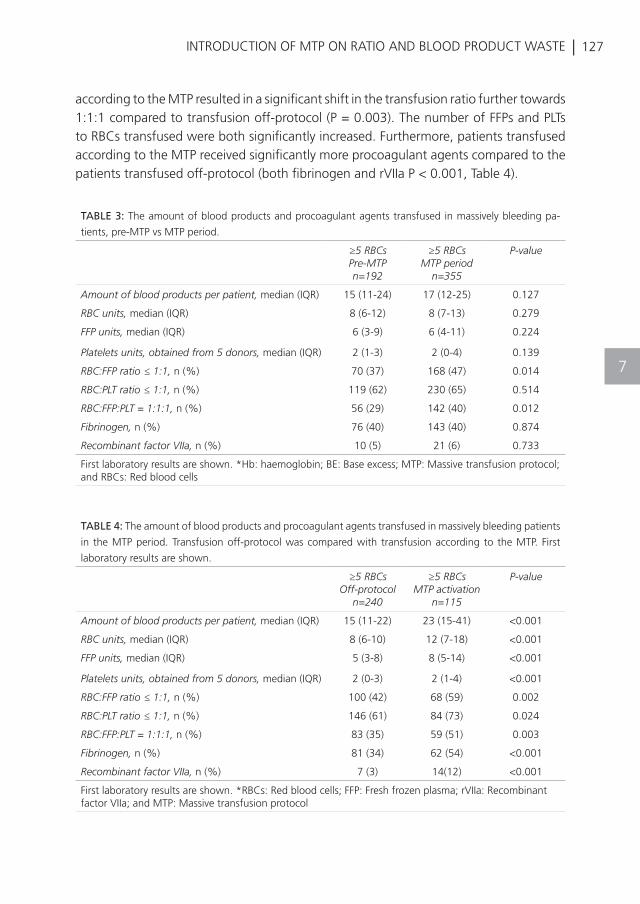
| 127INTRODUCTION OF MTP ON RATIO AND BLOOD PRODUCT WASTE
7
according to the MTP resulted in a significant shift in the transfusion ratio further towards 1:1:1 compared to transfusion off-protocol (P = 0.003). The number of FFPs and PLTs to RBCs transfused were both significantly increased. Furthermore, patients transfused according to the MTP received significantly more procoagulant agents compared to the patients transfused off-protocol (both fibrinogen and rVIIa P < 0.001, Table 4).
TABLE 3: The amount of blood products and procoagulant agents transfused in massively bleeding pa-
tients, pre-MTP vs MTP period.
≥5 RBCsPre-MTPn=192
≥5 RBCsMTP period
n=355
P-value
Amount of blood products per patient, median (IQR) 15 (11-24) 17 (12-25) 0.127
RBC units, median (IQR) 8 (6-12) 8 (7-13) 0.279
FFP units, median (IQR) 6 (3-9) 6 (4-11) 0.224
Platelets units, obtained from 5 donors, median (IQR) 2 (1-3) 2 (0-4) 0.139
RBC:FFP ratio ≤ 1:1, n (%) 70 (37) 168 (47) 0.014
RBC:PLT ratio ≤ 1:1, n (%) 119 (62) 230 (65) 0.514
RBC:FFP:PLT = 1:1:1, n (%) 56 (29) 142 (40) 0.012
Fibrinogen, n (%) 76 (40) 143 (40) 0.874
Recombinant factor VIIa, n (%) 10 (5) 21 (6) 0.733
First laboratory results are shown. *Hb: haemoglobin; BE: Base excess; MTP: Massive transfusion protocol; and RBCs: Red blood cells
TABLE 4: The amount of blood products and procoagulant agents transfused in massively bleeding patients
in the MTP period. Transfusion off-protocol was compared with transfusion according to the MTP. First
laboratory results are shown.
≥5 RBCsOff-protocol
n=240
≥5 RBCsMTP activation
n=115
P-value
Amount of blood products per patient, median (IQR) 15 (11-22) 23 (15-41) <0.001
RBC units, median (IQR) 8 (6-10) 12 (7-18) <0.001
FFP units, median (IQR) 5 (3-8) 8 (5-14) <0.001
Platelets units, obtained from 5 donors, median (IQR) 2 (0-3) 2 (1-4) <0.001
RBC:FFP ratio ≤ 1:1, n (%) 100 (42) 68 (59) 0.002
RBC:PLT ratio ≤ 1:1, n (%) 146 (61) 84 (73) 0.024
RBC:FFP:PLT = 1:1:1, n (%) 83 (35) 59 (51) 0.003
Fibrinogen, n (%) 81 (34) 62 (54) <0.001
Recombinant factor VIIa, n (%) 7 (3) 14(12) <0.001
First laboratory results are shown. *RBCs: Red blood cells; FFP: Fresh frozen plasma; rVIIa: Recombinant factor VIIa; and MTP: Massive transfusion protocol
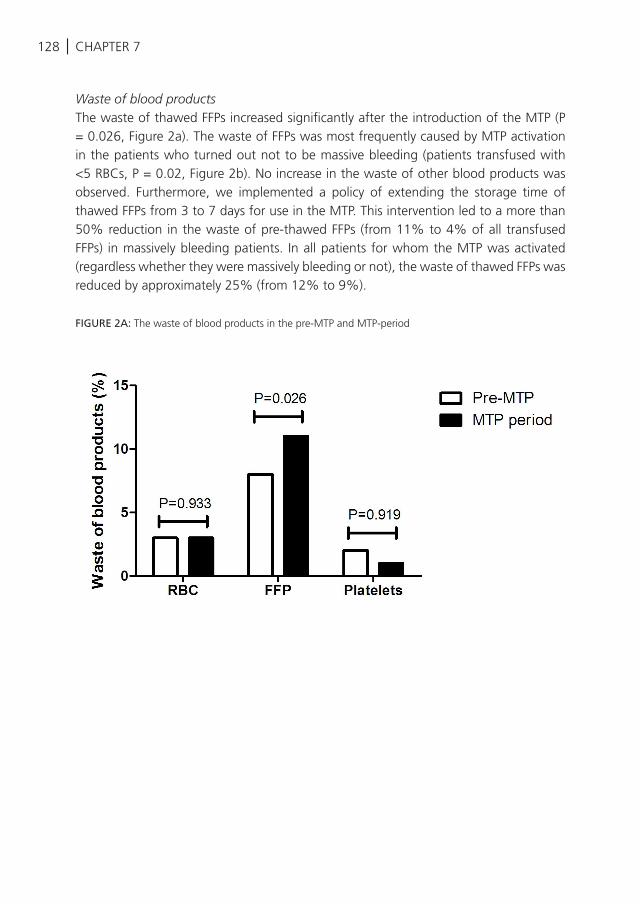
128 | CHAPTER 7
Waste of blood productsThe waste of thawed FFPs increased significantly after the introduction of the MTP (P = 0.026, Figure 2a). The waste of FFPs was most frequently caused by MTP activation in the patients who turned out not to be massive bleeding (patients transfused with <5 RBCs, P = 0.02, Figure 2b). No increase in the waste of other blood products was observed. Furthermore, we implemented a policy of extending the storage time of thawed FFPs from 3 to 7 days for use in the MTP. This intervention led to a more than 50% reduction in the waste of pre-thawed FFPs (from 11% to 4% of all transfused FFPs) in massively bleeding patients. In all patients for whom the MTP was activated (regardless whether they were massively bleeding or not), the waste of thawed FFPs was reduced by approximately 25% (from 12% to 9%).
FIGURE 2A: The waste of blood products in the pre-MTP and MTP-period
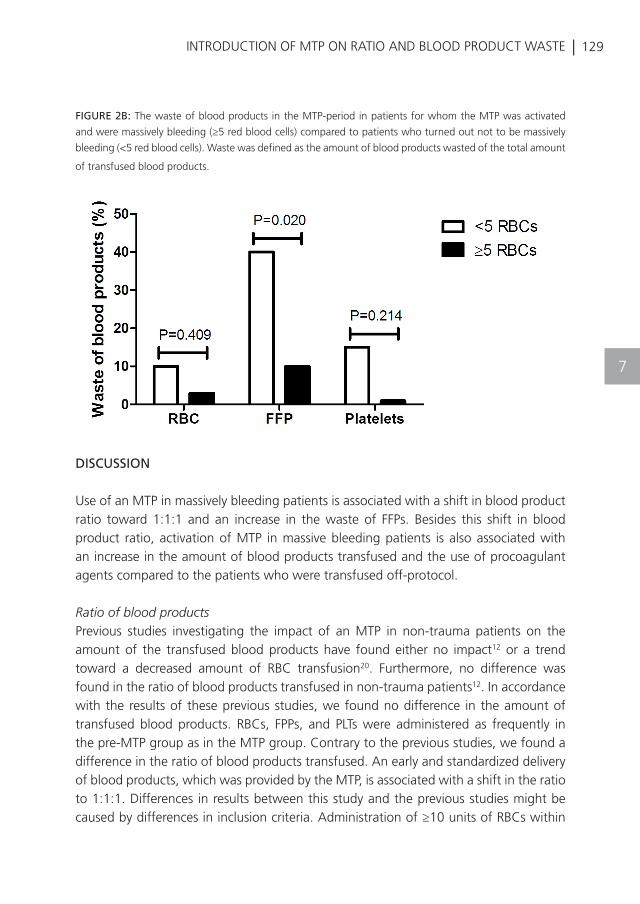
| 129INTRODUCTION OF MTP ON RATIO AND BLOOD PRODUCT WASTE
7
FIGURE 2B: The waste of blood products in the MTP-period in patients for whom the MTP was activated
and were massively bleeding (≥5 red blood cells) compared to patients who turned out not to be massively
bleeding (<5 red blood cells). Waste was defined as the amount of blood products wasted of the total amount
of transfused blood products.
DISCUSSION
Use of an MTP in massively bleeding patients is associated with a shift in blood product ratio toward 1:1:1 and an increase in the waste of FFPs. Besides this shift in blood product ratio, activation of MTP in massive bleeding patients is also associated with an increase in the amount of blood products transfused and the use of procoagulant agents compared to the patients who were transfused off-protocol.
Ratio of blood productsPrevious studies investigating the impact of an MTP in non-trauma patients on the amount of the transfused blood products have found either no impact12 or a trend toward a decreased amount of RBC transfusion20. Furthermore, no difference was found in the ratio of blood products transfused in non-trauma patients12. In accordance with the results of these previous studies, we found no difference in the amount of transfused blood products. RBCs, FPPs, and PLTs were administered as frequently in the pre-MTP group as in the MTP group. Contrary to the previous studies, we found a difference in the ratio of blood products transfused. An early and standardized delivery of blood products, which was provided by the MTP, is associated with a shift in the ratio to 1:1:1. Differences in results between this study and the previous studies might be caused by differences in inclusion criteria. Administration of ≥10 units of RBCs within
130 | CHAPTER 7
24 h is a generally accepted definition for massive bleeding and is frequently used in the previous studies. However, in this study the administration of ≥5 RBCs within 12 h was defined as massive bleeding and represented the inclusion criteria. This definition was chosen instead of ≥10 RBCs in 24 h, in order to capture the episodes of severe bleeding instead of oozing over a prolonged period. Also, the administration of MTP may prevent severely bleeding patients from receiving ≥10 RBCs.
We did not find an effect on survival rate after implementation of an MTP. Data from the Pragmatic, Randomized Optimal Platelet and Plasma Ratios trial10 and the Prospective Observational Multicentre Major Trauma Transfusion trial5 investigated the use of a 1:1:1 transfusion ratio in massively bleeding trauma patients and show that early administration of blood products in a 1:1:1 ratio was associated with more patients achieving haemostasis, but 24-h and 30-day mortality rate was unaffected. Death by haemorrhage occurs within the first 3 h after admission to the emergency room5,10. This may hamper the ability to detect a difference in mortality within 24-h or 28-day in previous studies but also in this study. Alternatively, the effect of the transfusion ratio on mortality might be less evident in non-trauma patients, which in this study the majority of patients are. Regardless the effect of the transfusion ratio on mortality, we observed in this study that introduction of the MTP is an adequate way to achieve a well-balanced transfusion ratio of blood products. This was confirmed by the comparison between patients who were transfused according to the MTP protocol and massive bleeding patients who were transfused off-protocol. Also, a significant shift was observed in RBC: FFP:PLT ratio towards 1:1:1 was observed in the MTP group. However, the comparison of patients who were transfused according to the MTP with massively bleeding patients who were transfused off-protocol is limited by a possible indication bias. The off-protocol patients might be healthier overall, which is indicated by less acidotic patients and less transfused blood products in this group. Also, a number of procoagulant agents in this group was lower. Therefore, it is likely that off-protocol patients did not have the same physiological measures that would have warranted an activation of the MTP.
Waste of blood products In this study, we found an increase in the waste of FFPs following the introduction of an MTP as observed in previous studies in trauma patients12. After obtaining these results, we implemented a policy of extending the storage time of thawed FFPs from 3 to 7 days for use in the MTP. This intervention led to a more than 50% reduction in the waste of pre-thawed FFPs in massively bleeding patients and a 25% reduction in all patients for whom the MTP was activated, massive bleeding or not. Of note, an extension of the storage time from 3 to 7 days will not influence the quality of clotting factors22,23. The waste of FFPs was 4 times higher in the patients for whom the MTP was activated
| 131INTRODUCTION OF MTP ON RATIO AND BLOOD PRODUCT WASTE
7
but who turned out not to be massive bleeding. Over-activation of an MTP is common and varies between 54% and 84%12,20,21, as specific criteria for massive bleeding in non-trauma patients are lacking. Activation criteria for the MTP are currently based on studies in trauma patients only24-26. Therefore, studies are required to identify predictors for massive bleeding in non-trauma patients. In the meantime, the feedback to the trauma team with the instructions to return products to the blood bank when not used may limit the FFP wastage.
There are several limitations to this study. It is a single centre study, time to transfusion was not reported and the definition for massive bleeding patients, which we used in this study, does not control for deceased patients who were massively bleeding, but died before they could have been administered with ≥5 RBCs within 12 h. Furthermore, we have defined massive bleeding as the administration of ≥5 RBCs in 12 h instead of ≥10 RBCs in 24 h, which is a more generally accepted definition. This may hamper comparability of results.
CONCLUSION
A hospital-wide introduction of an MTP leads to a shift in blood product ratio toward a 1:1:1 in massively bleeding patients. Furthermore, the introduction of an MTP comes with an increase in a waste of FFPs, which is lowered after extending the duration of storage time after thawing.
132 |
REFERENCES
Sauaia A, Moore FA, Moore EE, Moser KS,
Brennan R, Read RA, Pons PT. Epidemiology
of trauma deaths: a reassessment. J.Trauma
1995 Feb;38(2):185-93.
Evans JA, van Wessem KJ, McDougall D,
Lee KA, Lyons T, Balogh ZJ. Epidemiology of
traumatic deaths: comprehensive population-
based assessment. World J.Surg. 2010
Jan;34(1):158-63.
Ljubicic N, Budimir I, Pavic T, Biscanin A,
Puljiz Z, Bratanic A, Troskot B, Zekanovic D.
Mortality in high-risk patients with bleeding
Mallory-Weiss syndrome is similar to that of
peptic ulcer bleeding. Results of a prospective
database study. Scand.J.Gastroenterol. 2014
Apr;49(4):458-64.
Berg CJ, Callaghan WM, Syverson C,
Henderson Z. Pregnancy-related mortality
in the United States, 1998 to 2005. Obstet.
Gynecol. 2010 Dec;116(6):1302-9.
Holcomb JB, Del Junco DJ, Fox EE, Wade CE,
Cohen MJ, Schreiber MA, Alarcon LH, Bai Y,
Brasel KJ, Bulger EM, et al. The prospective,
observational, multicenter, major trauma
transfusion (PROMMTT) study: comparative
effectiveness of a time-varying treatment
with competing risks. JAMA Surg. 2013
Feb;148(2):127-36.
Kutcher ME, Kornblith LZ, Narayan R, Curd
V, Daley AT, Redick BJ, Nelson MF, Fiebig
EW, Cohen MJ. A paradigm shift in trauma
resuscitation: evaluation of evolving massive
transfusion practices. JAMA Surg. 2013
Sep;148(9):834-40.
Wafaisade A, Maegele M, Lefering R, Braun
M, Peiniger S, Neugebauer E, Bouillon B. High
plasma to red blood cell ratios are associated
with lower mortality rates in patients receiving
multiple transfusion (4</=red blood cell
units<10) during acute trauma resuscitation.
J.Trauma 2011 Jan;70(1):81-8.
Zink KA, Sambasivan CN, Holcomb JB,
Chisholm G, Schreiber MA. A high ratio of
plasma and platelets to packed red blood
cells in the first 6 hours of massive transfusion
improves outcomes in a large multicenter
study. Am.J.Surg. 2009 May;197(5):565-70.
Sperry JL, Ochoa JB, Gunn SR, Alarcon LH,
Minei JP, Cuschieri J, Rosengart MR, Maier
RV, Billiar TR, Peitzman AB, et al. An FFP:PRBC
transfusion ratio >/=1:1.5 is associated
with a lower risk of mortality after massive
transfusion. J.Trauma 2008 Nov;65(5):986-93.
Holcomb JB, Tilley BC, Baraniuk S, Fox EE,
Wade CE, Podbielski JM, Del Junco DJ, Brasel
KJ, Bulger EM, Callcut RA, et al. Transfusion
of plasma, platelets, and red blood cells in a
1:1:1 vs a 1:1:2 ratio and mortality in patients
with severe trauma: the PROPPR randomized
clinical trial. JAMA 2015 Feb 3;313(5):471-82.
Khan S, Allard S, Weaver A, Barber C,
Davenport R, Brohi K. A major haemorrhage
protocol improves the delivery of blood
component therapy and reduces waste in
trauma massive transfusion. Injury 2013
May;44(5):587-92.
McDaniel LM, Neal MD, Sperry JL, Alarcon
LH, Forsythe RM, Triulzi D, Peitzman AB, Raval
JS. Use of a massive transfusion protocol in
nontrauma patients: activate away. J.Am.Coll.
Surg. 2013 Jun;216(6):1103-9.
Schuster KM, Davis KA, Lui FY, Maerz LL,
Kaplan LJ. The status of massive transfusion
protocols in United States trauma centers:
massive transfusion or massive confusion?
Transfusion 2010 Jul;50(7):1545-51.
Ball CG, Dente CJ, Shaz B, Wyrzykowski
AD, Nicholas JM, Kirkpatrick AW, Feliciano
DV. The impact of a massive transfusion
protocol (1:1:1) on major hepatic injuries:
does it increase abdominal wall closure rates?
Can.J.Surg. 2013 Oct;56(5):E128-E134.
Dente CJ, Shaz BH, Nicholas JM, Harris
RS, Wyrzykowski AD, Patel S, Shah A,
Vercruysse GA, Feliciano DV, Rozycki GS,
et al. Improvements in early mortality and
coagulopathy are sustained better in patients
with blunt trauma after institution of a massive
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
CHAPTER 7
| 133
REFERENCES
INTRODUCTION OF MTP ON RATIO AND BLOOD PRODUCT WASTE
16
17
18
19
20
21
22
23
24
25
26
transfusion protocol in a civilian level I trauma
center. J.Trauma 2009 Jun;66(6):1616-24.
O’Keeffe T, Refaai M, Tchorz K, Forestner JE,
Sarode R. A massive transfusion protocol to
decrease blood component use and costs.
Arch.Surg. 2008 Jul;143(7):686-90.
Morse BC, Dente CJ, Hodgman EI, Shaz BH,
Nicholas JM, Wyrzykowski AD, Salomone JP,
Vercruysse GA, Rozycki GS, Feliciano DV. The
effects of protocolized use of recombinant
factor VIIa within a massive transfusion
protocol in a civilian level I trauma center.
Am.Surg. 2011 Aug;77(8):1043-9.
Cotton BA, Gunter OL, Isbell J, Au BK,
Robertson AM, Morris JA, Jr., St JP, Young PP.
Damage control hematology: the impact of a
trauma exsanguination protocol on survival
and blood product utilization. J.Trauma 2008
May;64(5):1177-82.
Riskin DJ, Tsai TC, Riskin L, Hernandez-
Boussard T, Purtill M, Maggio PM, Spain DA,
Brundage SI. Massive transfusion protocols:
the role of aggressive resuscitation versus
product ratio in mortality reduction. J.Am.
Coll.Surg. 2009 Aug;209(2):198-205.
Baumann Kreuziger LM, Morton CT,
Subramanian AT, Anderson CP, Dries DJ.
Not only in trauma patients: hospital-wide
implementation of a massive transfusion
protocol. Transfus.Med. 2013 Dec 26.
Morse BC, Dente CJ, Hodgman EI, Shaz BH,
Winkler A, Nicholas JM, Wyrzykowski AD,
Rozycki GS, Feliciano DV. Outcomes after
massive transfusion in nontrauma patients
in the era of damage control resuscitation.
Am.Surg. 2012 Jun;78(6):679-84.
Tholpady A, Monson J, Radovancevic R, Klein
K, Bracey A. Analysis of prolonged storage
on coagulation Factor (F)V, FVII, and FVIII
in thawed plasma: is it time to extend the
expiration date beyond 5 days? Transfusion
2013 Mar;53(3):645-50.
Wang Z, Du X, Li C, Ma L, Sun P, Cao H,
Lin F, Ye S, Xiao X. Coagulation factors and
inhibitors in thawed plasma stored at 1-6
degrees C for 5 days in China. Transfus.Apher.
Sci. 2014 Apr;50(2):274-80.
Nunez TC, Voskresensky IV, Dossett LA, Shinall
R, Dutton WD, Cotton BA. Early prediction of
massive transfusion in trauma: simple as ABC
(assessment of blood consumption)? J.Trauma
2009 Feb;66(2):346-52.
Ogura T, Nakamura Y, Nakano M, Izawa
Y, Nakamura M, Fujizuka K, Suzukawa M,
Lefor AT. Predicting the need for massive
transfusion in trauma patients: The Traumatic
Bleeding Severity Score. J.Trauma Acute.Care
Surg. 2014 May;76(5):1243-50.
Olaussen A, Blackburn T, Mitra B, Fitzgerald
M. Review article: Shock Index for prediction
of critical bleeding post-trauma: A systematic
review. Emerg Med.Australas. 2014 Apr 8.
7
K. Balvers, S. Saleh, S.S. Zeerleder, J.H. Klinkspoor, J.C. Goslings, N.P. Juffermans
Transfusion 2016
ARE THERE ANY ALTERNATIVES FOR TRANSFUSION OF AB PLASMA AS UNIVERSAL DONOR IN AN
EMERGENCY RELEASE SETTING?
8

136 | CHAPTER 8
ABSTRACT
Introduction: AB plasma is used as the universal donor plasma product in patients requiring massive transfusion. However, currently it is a recommended policy to transfuse plasma derived from male donors only as transfusion of plasma from HLA antibody-positive female donors is associated with an increased risk for transfusion-related acute lung injury (TRALI). As a result, due to high demands, supplies of blood banks may run out of AB plasma, calling for alternatives. Therefore, the aim of this review was to investigate alternatives for emergency release of AB plasma as the universal donor.
Methods: A systematic search was conducted in Embase and Pubmed. Studies on adult patients, who were transfused with at least one unit of plasma investigating the incidence of transfusion-related complications or mortality in patients transfused with ABO identical plasma, ABO compatible or ABO incompatible plasma, were eligible for inclusion. The primary outcomes were the incidence of transfusion-related complications and mortality.
Results: In total 6 studies were included. Transfusion of ABO compatible plasma was associated with an increased incidence of lung injury and mortality (OR 1.10, 95% CI 1.04-1.15 p=0.0003) compared to transfusion of ABO identical plasma. No significant differences were observed regarding transfusion-related complications and mortality between patients transfused with ABO compatible or ABO incompatible plasma.
Conclusion: Studies are insufficient to formulate advices about alternatives for transfusion of AB plasma as universal donor plasma in the emergency setting due to the small number of studies. The results of this review underline the need for further research.
| 137ALTERNATIVES FOR AB PLASMA
8
INTRODUCTION
Massive hemorrhage is a leading cause of mortality1-3. Resuscitation of massive hemorrhage has shifted towards earlier administration of plasma to reduce mortality4-7. Ideally, blood products from the same blood group as the recipient are transfused. However, blood group determination delays time until administration of blood products in massively bleeding patients and is therefore not practical8. Transfusion of ABO non-identical plasma may increase the risk for transfusion-related complications caused by anti-A, anti-B and anti-A,B antibodies of the donor that bind to host erythrocytes9. AB plasma does not contain anti-A and anti-B antibodies, and is compatible with A, B, AB and O blood groups. Thereby, AB plasma is frequently used as the universal donor plasma product. However, blood group AB is less prevalent than other blood groups10. Also, policies to mitigate the risk of transfusion-related acute lung injury (TRALI) by deferral of donors with a high risk of carrying HLA antibodies may further hamper supply of a specific blood type of plasma11-15. As a result, supplies of blood banks may run out of AB plasma. Alternatives for AB plasma are ABO identical plasma and ABO-non-identical plasma, of which ABO non-identical plasma can be divided in ABO compatible and ABO incompatible plasma. However, it is unknown whether these alternatives are associated with an increased incidence of transfusion-related complications and mortality. Therefore, the aim of this review was to determine the incidences of transfusion-related complications and mortality in patients transfused with either ABO identical, ABO compatible or ABO incompatible plasma.
MATERIAL AND METHODS
The present review was reported according to the PRISMA guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses)16.
STUDY SELECTION
An electronic search was performed in Embase and Pubmed. The following search strategy was used: (“Plasma”[Mesh] OR “ABO Blood-Group System”[MeSH Terms] OR plasma[tiab] OR ABO[tiab]) AND (mismatch [tiab] OR “Blood Group Incompatibility”[Mesh] OR incompat*[tiab] OR compat*[tiab]) AND (“Blood Component Transfusion “[Mesh] OR “Transfusion Medicine”[Mesh] OR transfusion[tiab] OR haemorrhage [tiab] OR hemorrhage[tiab] OR bleeding[tiab]) AND (complication*[tiab] OR adverse outcome*[tiab] OR TRALI [tiab] OR adverse effect*[tiab] OR “adverse effects” [Subheading] OR “mortality” [Subheading] OR “Mortality”[Mesh] OR “complications” [Subheading] OR “Respiratory Distress Syndrome, Adult”[Mesh] OR “Sepsis”[Mesh] OR
138 | CHAPTER 8
Sepsis[tiab]) NOT (animal [mh] NOT human [mh]). No restriction on publication date was performed. Additionally, we have assessed all citations of the studies included for full text screening. After the search, duplicates were removed and studies were assessed for eligibility.
Studies on adult patients who were transfused with at least one unit of plasma investigating the incidence of transfusion-related complications and mortality in patients transfused with ABO identical, ABO compatible or ABO incompatible plasma in an emergency setting, were eligible for inclusion. All observational studies and randomized controlled trials with adult patients (≥18 years) and transfusion-related complications or mortality as primary or secondary outcome, were eligible. Exclusion criteria were animal studies, reviews, letters to the editors, case reports and editorials. The search was conducted by two independent researchers (SS and KB). Language was limited to English, German and Dutch. The primary outcome of this analysis was the incidences of mortality and transfusion-related complications like hemolytic reactions, transfusion-related acute lung injury (TRALI), adult respiratory distress syndrome (ARDS), acute renal failure (ARF), acute liver failure and thromboembolic events.
In order to assess the risk of bias of the included studies, the Newcastle Ottawa scale17 was used, since most of the studies were observational cohort studies. Studies were scored on different categories, i.e. comparability, methods used to select study participants and determination of outcome variables. The maximum score per item within the categories was two, the maximum score overall was 10.
Review Manager (RevMan 5, The Nordic Cochrane Centre) was used to pool data from different studies in a meta-analysis. Pooling of studies was performed if homogeneity was sufficient after assessment of study population, intervention, and outcome. The Inverse Variance method was used to test for homogeneity, which was expressed by an I2 lower than 75%. Randomized controlled studies and observational studies were not combined in the same meta-analysis. Results of meta-analyses were expressed by odds ratios and 95% confidence intervals.
RESULTS
In total, 1761 studies were screened and assessed for eligibility on abstract and title. Six studies were included after applying the inclusion and exclusion criteria, with in total 88,160 patients. Of these 6 studies, 5 studies were retrospective cohort studies and 1 study was a sub study of a randomized controlled transfusion trial. Figure 1 illustrates the flowchart of the inclusion process and Table 1 the characteristics of the included
| 139ALTERNATIVES FOR AB PLASMA
8
studies. Two studies compared the use of ABO identical plasma with ABO compatible plasma, whereas the other 4 studies compared the use of ABO compatible with ABO incompatible plasma in an emergency release setting. Risk for bias was moderate as scores on the Newcastle Ottawa Scale varied between the 5-8 points. The number of studies included in this study, which examined alternatives for AB plasma in the emergency setting, was insufficient. Therefore results are reported narratively rather than systematically.
Transfusion of ABO identical vs ABO compatible plasmaTwo retrospective single center studies8, 18 investigated the effect of ABO compatible plasma and ABO identical plasma on the incidence of transfusion-related adverse events. The first registry study18 was conducted in Sweden and included a large number of patients (n=86082). All patients transfused with at least one plasma unit were included. The incidence of transfusion-related complications was not determined, however a trend was observed towards a higher 14-days post transfusion mortality rate in patients transfused with ABO plasma (RR 1.06, 95% CI 0.997-1.13, p=0.006). This risk was most apparent in those patients who received large numbers of ABO compatible plasma. Of note, data in this study are obtained from a blood bank registry, with limited data on patient characteristics. Therefore, differences in patient characteristics between groups were unaccounted for in this study. The second study8 was limited to trauma patients who were matched for patient characteristics in order to adjust for confounders. Although mortality rates were similar in both groups, a significant dose dependent increase in ARDS was observed in patients receiving ABO compatible plasma compared to patients receiving ABO identical plasma. Patients receiving 4 to 6 units of ABO compatible plasma had a 3-fold higher risk of ARDS than patients receiving ABO identical plasma. Patients receiving ≥6 units ABO compatible plasma had a 4-fold higher risk than patients receiving ABO identical plasma. This increase in ARDS was most apparent in patients with blood group O (17.4% vs 7.8%, P<0.001). An explanation may be that patients with blood type O may have higher titers of anti-A and anti-B antibodies resulting in higher numbers of circulating immune complexes. However, patients with blood type A and B were underpowered in this study and data to support this hypothesis are not available.
Pooling of data from these two above mentioned studies for transfusion-related complications was not feasible due to a lack of documentation. However, pooling of data for mortality was feasible and resulted in a significant increased risk for mortality in patients transfused with ABO compatible plasma compared to ABO identical plasma (Figure 2, OR 1.10, 95% CI 1.04-1.15, p=0.0003).
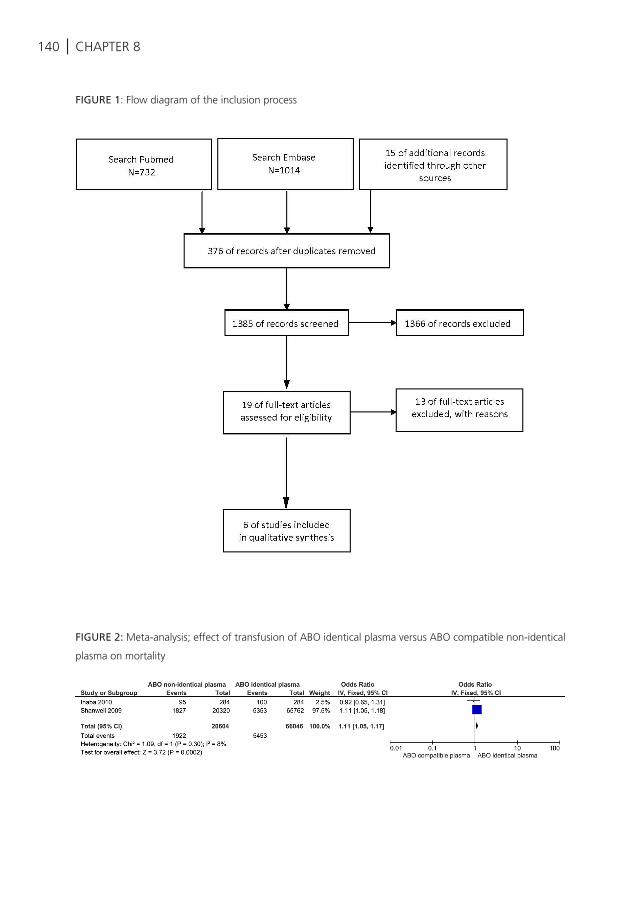
140 | CHAPTER 8
FIGURE 1: Flow diagram of the inclusion process
FIGURE 2: Meta-analysis; effect of transfusion of ABO identical plasma versus ABO compatible non-identical
plasma on mortality
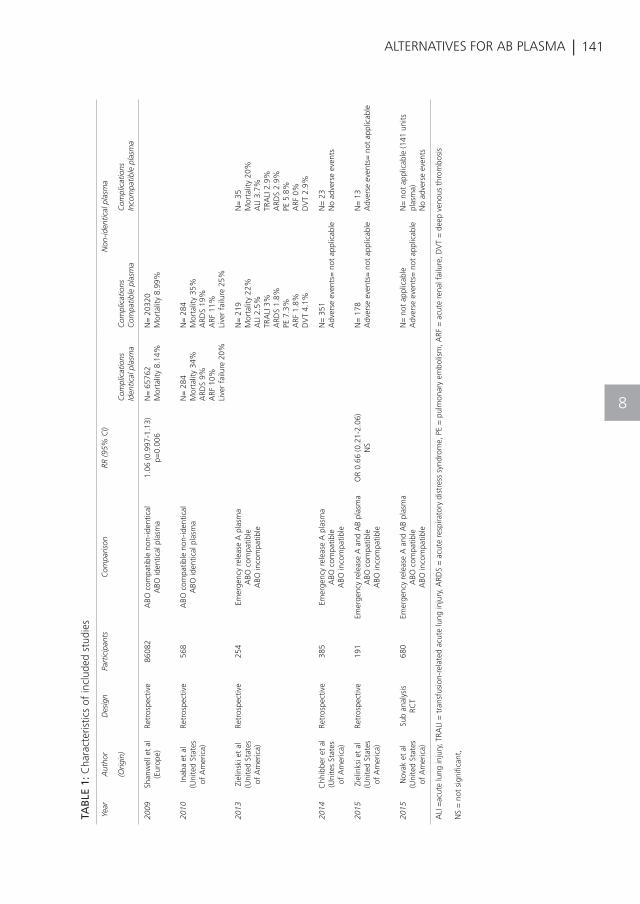
| 141ALTERNATIVES FOR AB PLASMA
8
TAB
LE 1
: Cha
ract
eris
tics
of in
clud
ed s
tudi
es
Year
Aut
hor
Des
ign
Part
icip
ants
Com
paris
onRR
(95%
CI)
Non
-iden
tical
pla
sma
(Orig
in)
Com
plic
atio
nsId
entic
al p
lasm
aC
ompl
icat
ions
Com
patib
le p
lasm
aC
ompl
icat
ions
Inco
mpa
tible
pla
sma
2009
Shan
wel
l et
al(E
urop
e)Re
tros
pect
ive
8608
2A
BO c
ompa
tible
non
-iden
tical
A
BO id
entic
al p
lasm
a1.
06 (0
.997
-1.1
3)
p=0.
006
N=
657
62M
orta
lity
8.14
%N
= 2
0320
M
orta
lity
8.99
%
2010
Inab
a et
al
(Uni
ted
Stat
es
of A
mer
ica)
Retr
ospe
ctiv
e56
8A
BO c
ompa
tible
non
-iden
tical
A
BO id
entic
al p
lasm
aN
= 2
84M
orta
lity
34%
ARD
S 9%
ARF
10%
Live
r fa
ilure
20%
N=
284
Mor
talit
y 35
%A
RDS
19%
ARF
11%
Live
r fa
ilure
25%
2013
Ziel
insk
i et
al(U
nite
d St
ates
of
Am
eric
a)
Retr
ospe
ctiv
e25
4Em
erge
ncy
rele
ase
A p
lasm
aA
BO c
ompa
tible
A
BO in
com
patib
le
N=
219
Mor
talit
y 22
%A
LI 2
.5%
TRA
LI 3
%A
RDS
1.8%
PE 7
.3%
ARF
1.8
%D
VT
4.1%
N=
35
Mor
talit
y 20
%A
LI 3
.7%
TRA
LI 2
.9%
ARD
S 2.
9%PE
5.8
%A
RF 0
%D
VT
2.9%
2014
Chh
ibbe
r et
al
(Uni
tes
Stat
es
of A
mer
ica)
Retr
ospe
ctiv
e38
5Em
erge
ncy
rele
ase
A p
lasm
aA
BO c
ompa
tible
A
BO in
com
patib
le
N=
351
Adv
erse
eve
nts=
not
app
licab
leN
= 2
3 N
o ad
vers
e ev
ents
2015
Ziel
inks
i et
al(U
nite
d St
ates
of
Am
eric
a)
Retr
ospe
ctiv
e19
1Em
erge
ncy
rele
ase
A a
nd A
B pl
asm
aA
BO c
ompa
tible
ABO
inco
mpa
tible
OR
0.66
(0.2
1-2.
06)
NS
N=
178
A
dver
se e
vent
s= n
ot a
pplic
able
N=
13
Adv
erse
eve
nts=
not
app
licab
le
2015
Nov
ak e
t al
(Uni
ted
Stat
es
of A
mer
ica)
Sub
anal
ysis
RC
T68
0Em
erge
ncy
rele
ase
A a
nd A
B pl
asm
aA
BO c
ompa
tible
ABO
inco
mpa
tible
N=
not
app
licab
le
A
dver
se e
vent
s= n
ot a
pplic
able
N=
not
app
licab
le (1
41 u
nits
pl
asm
a)N
o ad
vers
e ev
ents
ALI
=ac
ute
lung
inju
ry, T
RALI
= t
rans
fusi
on-r
elat
ed a
cute
lung
inju
ry, A
RDS
= a
cute
res
pira
tory
dis
tres
s sy
ndro
me,
PE
= p
ulm
onar
y em
bolis
m, A
RF =
acu
te r
enal
fai
lure
, DV
T =
dee
p ve
nous
thr
ombo
sis
NS
= n
ot s
igni
fican
t,

142 | CHAPTER 8
Transfusion of ABO compatible vs ABO incompatible plasmaOf the 6 studies in this analysis, 4 studies10, 19-21 investigated the effect of ABO compatible plasma with ABO incompatible plasma on transfusion-related complications and mortality. The first study19 was a retrospective single centre study conducted in England and included 385 patients, for whom type A plasma was issued. Of these, 325 patients had blood group A or O and therefore received compatible plasma, 11 patients did not receive any blood products or died from exsanguination and 26 patients with blood group B were not exposed to A plasma. The remaining 23 patients received ABO incompatible A plasma. In these patients, no transfusion-related complications or other adverse outcomes were observed.
The second20 study was a retrospective single center study conducted in all transfused trauma patients, who received at least one emergency release A plasma unit. In total, data from 254 patients were analyzed, of which 35 patients received incompatible plasma. No differences in the incidence of ALI, TRALI, ARDS, deep venous thrombosis (DVT), pulmonary embolism (PE), ARF and mortality were observed. However, adjustment for confounders was not performed.
A retrospective multicentre cohort study10 from the same research group as the previous study included 191 bleeding trauma patients. Emergency release of A plasma (n=115) was compared to emergency release of AB plasma (n=76). Patients receiving AB plasma were more severely injured and were transfused with more blood products. The incidence of transfusion-related complications like ARF, DVT, PE and mortality appeared to be higher in the AB plasma group. However, after adjustment for confounders, no difference was observed in the incidence of mortality between both groups. Controlling for confounders was not performed for other transfusion-related complications.
A sub study21 of the randomized controlled Pragmatic Randomized Optimal Platelets and Plasma ratios (PROPPR) trial included in total 680 bleeding trauma patients in 12 different hospitals. Emergency plasma blood type A, blood group A with low-titer anti-B and blood group AB were used. No transfusion-related complications were observed. The incidence of transfusion reactions in the other groups was not mentioned. However, data of this study were briefly presented.
Pooling of data of these 4 studies in a meta-analysis was not possible due to heterogeneity of the studies.
| 143ALTERNATIVES FOR AB PLASMA
8
DISCUSSION
The results of this review suggest that transfusion of ABO compatible plasma is associated with an increased incidence of lung injury and mortality compared to transfusion of ABO identical plasma. However, in an emergency setting when ABO identical plasma is not available, it appears that compatibility does not affect the outcome. Nevertheless, interpretations of results found in this review are hampered by small study numbers, design, heterogeneity in patient populations and incomplete documentation.
Ideally, blood group determination is performed before transfusion in order to reduce the risk for transfusion-related complications. Previous studies observed higher incidences of hemolytic reactions after transfusion of red blood cells when no compatibility between blood groups of donor and recipient was obtained22-25. In plasma units, high levels of antibodies can be detected26; however, whether the same assumption between donor and recipient as in red blood cells holds for the transfusion of plasma, is unknown. The findings of this review suggest that transfusion of ABO compatible plasma is actually associated with an increased risk for ARDS and mortality. However, these results are based on a very small number of studies18, 22, which were conducted in different patient populations (trauma vs all recipients). In particular, the study which suggested an increased risk of ARDS after transfusion of compatible ABO plasma compared to ABO identical plasma did not report differences in population in terms of plasma donor gender. Actually, 5 of the 6 studies in this review did not document sex of plasma donors. Furthermore, this study was performed before TRALI mitigation, which hampers the interpretation of these results.
Regarding transfusion of ABO non-identical plasma, no differences in the incidence of transfusion-related complications between ABO compatible and incompatible plasma were observed. All studies issued AB or A plasma in the emergency setting. Two studies reported not even one adverse event in the A plasma group. This suggests that transfusion of A plasma is potentially as safe as AB plasma and might be used as a universal donor in the emergency setting. However, the evidence found in this review for this hypothesis was very limited. The number of studies was small, designs of studies did not always control for potential confounders and different patient populations were used, which hampered pooling and interpretation of results. Additionally, low rates of incompatible transfusions were observed in the studies. This makes it impossible to draw definite conclusions.
Observational data are required comparing the incidence of transfusion-related complications and mortality in patients transfused with ABO-identical, ABO compatible

144 | CHAPTER 8
and ABO incompatible plasma. In the meantime, we recommend issuing AB plasma as universal donor plasma product initially when the blood group is unknown and switch to ABO identical plasma once the blood group has been determined. If AB plasma is not available, transfusion of A plasma seems to be a safe option and is preferable above B or O plasma as it appears that A plasma does not increase the incidence of transfusion-related complications10, 19-21 and is more common than B plasma10. O plasma is unsuitable as this plasma carries both anti-A and anti-B antibodies.
CONCLUSION
Presently it is unclear whether there are safe alternatives for transfusion of AB plasma as universal donor in the emergency setting. The small number of available studies in this review may suggest that ABO compatible plasma increases the risk for lung injury and mortality compared to ABO identical plasma. However, in an emergency setting when ABO identical plasma is not available, it appears that compatibility does not affect the outcome. However, interpretation of results is hampered by small study numbers, design, heterogeneity in patient populations, and incomplete documentation.

| 145ALTERNATIVES FOR AB PLASMA
8
146 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
CHAPTER 8
Evans JA, van Wessem KJ, McDougall D,
et al. Epidemiology of traumatic deaths:
comprehensive population-based assessment.
World J Surg 2010;34(1):158-63.
Sauaia A, Moore FA, Moore EE, et
al. Epidemiology of trauma deaths: a
reassessment. J Trauma. 1995;38(2):185-93.
Ljubicic N, Budimir I, Pavic T, et al. Mortality in
high-risk patients with bleeding Mallory-Weiss
syndrome is similar to that of peptic ulcer
bleeding. Results of a prospective database
study. Scand J Gastroenterol 2014;49(4):458-
64.
Holcomb JB, Del Junco DJ, Fox EE, et al.
The prospective, observational, multicenter,
major trauma transfusion (PROMMTT) study:
comparative effectiveness of a time-varying
treatment with competing risks. JAMA Surg
2013;148(2):127-36.
Holcomb JB, Tilley BC, Baraniuk S, et al.
Transfusion of plasma, platelets, and red
blood cells in a 1:1:1 vs a 1:1:2 ratio and
mortality in patients with severe trauma:
the PROPPR randomized clinical trial. JAMA.
2015;313(5):471-82.
Kutcher ME, Kornblith LZ, Narayan R, et al.
A paradigm shift in trauma resuscitation:
evaluation of evolving massive transfusion
practices. JAMA Surg 2013;148(9):834-40.
Sperry JL, Ochoa JB, Gunn SR, et al. An
FFP:PRBC transfusion ratio >/=1:1.5 is
associated with a lower risk of mortality
after massive transfusion. J Trauma.
2008;65(5):986-93.
Inaba K, Branco BC, Rhee P, et al. Impact
of ABO-identical vs ABO-compatible
nonidentical plasma transfusion in trauma
patients. Archives of surgery (Chicago, Ill :
1960). 2010;145(9):899-906.
Beauregard P, Blajchman MA. Hemolytic
and pseudo-hemolytic transfusion reactions:
an overview of the hemolytic transfusion
reactions and the clinical conditions that mimic
them. Transfus Med Rev. 1994;8(3):184-99.
Zielinski MD, Schrager JJ, Johnson P, et al.
Multicenter comparison of emergency release
group A versus AB plasma in blunt-injured
trauma patients. Clinical and translational
science. 2015;8(1):43-7.
Standards for Blood Banks and Transfusion
Services. 29th edition ed2014.
Beckers EAM, Van Stein D, Porcelijn L, et al.
Trali reports in the Netherlands: Evaluation
before and after the introduction of male-only
plasma. Vox Sanguinis. 2010;99:453.
Wiersum-Osselton JC, Middelburg RA, Beckers
EA, et al. Male-only fresh-frozen plasma
for transfusion-related acute lung injury
prevention: before-and-after comparative
cohort study. Transfusion. 2011;51(6):1278-
83.
Wiersum-Osselton JC, Middelburg RA, Van
Der Bom JG, et al. Effect of using male-only
fresh frozen plasma for TRALI prevention in
the Netherlands. Vox Sanguinis. 2010;99:457.
Eder AF, Herron RM, Jr., Strupp A, et al.
Effective reduction of transfusion-related
acute lung injury risk with male-predominant
plasma strategy in the American Red Cross
(2006-2008). Transfusion. 2010;50(8):1732-
42.
Moher D, Liberati A, Tetzlaff J, et al. Preferred
reporting items for systematic reviews and
meta-analyses: the PRISMA statement. BMJ.
2009;339:b2535.
G W, B S, J OC. The Newcastle-Ottawa
Scale (NOS) for assessing the quality of
nonrandomised studies in meta-analysis.
2011.
Shanwell A, Andersson TML, Rostgaard K, et
al. Post-transfusion mortality among recipients
of ABO-compatible but non-identical plasma.
Vox Sanguinis. 2009;96(4):316-23.
Chhibber V, Greene M, Vauthrin M, et al. Is
group A thawed plasma suitable as the first
option for emergency release transfusion?
(CME). Transfusion. 2014;54(7):1751-5; quiz
0.
| 147
REFERENCES
ALTERNATIVES FOR AB PLASMA
20
21
22
23
24
25
26
Zielinski MD, Johnson PM, Jenkins D, et al.
Emergency use of prethawed Group A plasma
in trauma patients. The journal of trauma
and acute care surgery. 2013;74(1):69-74;
discussion -5.
Novak DJ, Bai Y, Cooke RK, et al. Making
thawed universal donor plasma available
rapidly for massively bleeding trauma patients:
experience from the Pragmatic, Randomized
Optimal Platelets and Plasma Ratios (PROPPR)
trial. Transfusion. 2015;55(6):1331-9.
Inaba K, Teixeira PG, Shulman I, et al. The
impact of uncross-matched blood transfusion
on the need for massive transfusion and
mortality: analysis of 5,166 uncross-
matched units. The Journal of trauma.
2008;65(6):1222-6.
Benhamou D, Lienhart A, Auroy Y, et al.
Accidents by ABO incompatibility and
other main complications related to blood
transfusion in surgical patients: data from the
French national survey on anaesthesia-related
deaths. Transfus Clin Biol. 2005;12(5):389-90.
Janatpour KA, Kalmin ND, Jensen HM, et
al. Clinical outcomes of ABO-incompatible
RBC transfusions. Am J Clin Pathol.
2008;129(2):276-81.
Bryan S. Hemolytic transfusion reaction:
safeguards for practice. Journal of
perianesthesia nursing : official journal of the
American Society of PeriAnesthesia Nurses /
American Society of PeriAnesthesia Nurses.
2002;17(6):399-403.
Siani B, Willimann K, Wymann S, et al. Donor
screening reduces the isoagglutinin titer
in immunoglobulin products. Transfusion.
2015;55 Suppl 2:S95-7.
8

K. Balvers, S. van Dieren, K. Baksaas-Aasen, C. Gaarder, K. Brohi, S. Eaglestone, S. Stanworth, P.I. Johansson, S.R. Ostrowski, J. Stensballe, M. Maegele, J.C.
Goslings, N.P. Juffermans, TACTIC partners
Submitted
THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING TRAUMA PATIENTS
9
150 | CHAPTER 9
ABSTRACT
Introduction: The effect of a combined approach of balanced transfusion ratios, pro-coagulant and anti-fibrinolytic therapies on trauma-induced exsanguination is not known. The aim of this study was to investigate the effect of transfusion ratios, tranexamic acid (TXA) and products containing fibrinogen on outcome of bleeding trauma patients.
Methods: A prospective multicentre observational study was performed in 6 Level-1 trauma centres. Trauma patients who received at least 4 red blood cells (RBCs) were analysed (n=385) and divided into groups with low (<1:1) or high (≥1:1) ratios of plasma and platelets (PLTs) to RBCs, receiving TXA and fibrinogen products (fibrinogen concentrates or cryoprecipitate) or not. Logistic regression models were performed to assess the effect of transfusion strategies on the outcomes ‘alive and free of massive transfusion’ (≥10 RBCs in 24 hours) and early ‘normalization of coagulopathy’ (INR ≤1.2).
Results: A high PLT:RBC ratio and TXA were independently associated with an increased number of patients alive and free of massive transfusion (OR 2.8, 95% CI 1.3-6.0, p<0.01 and OR 2.2, 95% CI 1.0-4.9, p=0.04 resp.) A trend was observed for patients receiving a high ratio of plasma to RBCs (OR 2.0, 95% CI 1.0-3.9, p=0.052). Ratio, TXA and fibrinogen products were not associated with correction of coagulopathy.
Conclusion: A high PLT:RBC ratio and TXA are associated with a decreased need of massive transfusion and an increased survival in bleeding trauma patients. No effect on the early correction of coagulopathy, as defined by prolonged INR, was seen for transfusion ratio, TXA and fibrinogen products.
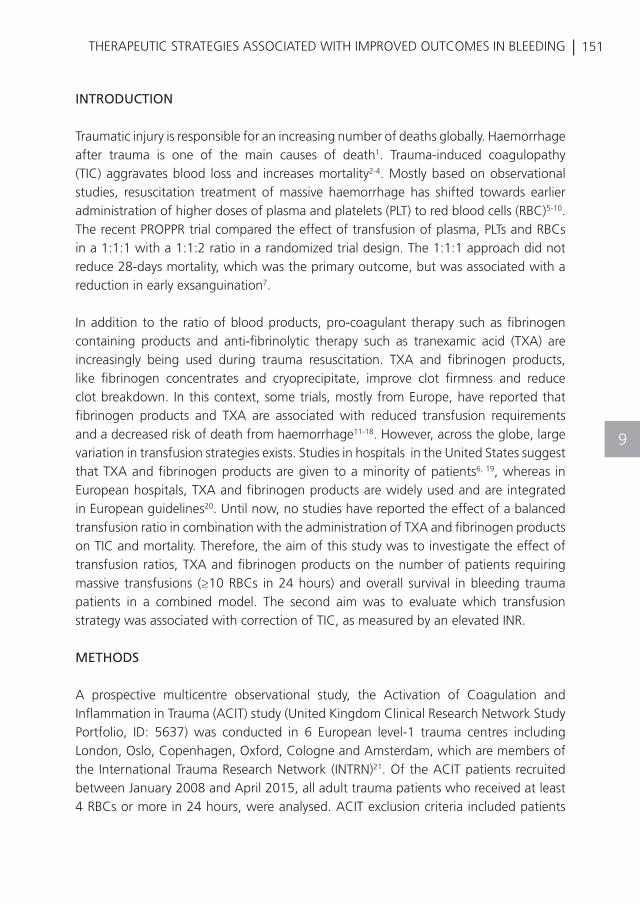
| 151THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
INTRODUCTION
Traumatic injury is responsible for an increasing number of deaths globally. Haemorrhage after trauma is one of the main causes of death1. Trauma-induced coagulopathy (TIC) aggravates blood loss and increases mortality2-4. Mostly based on observational studies, resuscitation treatment of massive haemorrhage has shifted towards earlier administration of higher doses of plasma and platelets (PLT) to red blood cells (RBC)5-10. The recent PROPPR trial compared the effect of transfusion of plasma, PLTs and RBCs in a 1:1:1 with a 1:1:2 ratio in a randomized trial design. The 1:1:1 approach did not reduce 28-days mortality, which was the primary outcome, but was associated with a reduction in early exsanguination7.
In addition to the ratio of blood products, pro-coagulant therapy such as fibrinogen containing products and anti-fibrinolytic therapy such as tranexamic acid (TXA) are increasingly being used during trauma resuscitation. TXA and fibrinogen products, like fibrinogen concentrates and cryoprecipitate, improve clot firmness and reduce clot breakdown. In this context, some trials, mostly from Europe, have reported that fibrinogen products and TXA are associated with reduced transfusion requirements and a decreased risk of death from haemorrhage11-18. However, across the globe, large variation in transfusion strategies exists. Studies in hospitals in the United States suggest that TXA and fibrinogen products are given to a minority of patients6, 19, whereas in European hospitals, TXA and fibrinogen products are widely used and are integrated in European guidelines20. Until now, no studies have reported the effect of a balanced transfusion ratio in combination with the administration of TXA and fibrinogen products on TIC and mortality. Therefore, the aim of this study was to investigate the effect of transfusion ratios, TXA and fibrinogen products on the number of patients requiring massive transfusions (≥10 RBCs in 24 hours) and overall survival in bleeding trauma patients in a combined model. The second aim was to evaluate which transfusion strategy was associated with correction of TIC, as measured by an elevated INR.
METHODS
A prospective multicentre observational study, the Activation of Coagulation and Inflammation in Trauma (ACIT) study (United Kingdom Clinical Research Network Study Portfolio, ID: 5637) was conducted in 6 European level-1 trauma centres including London, Oslo, Copenhagen, Oxford, Cologne and Amsterdam, which are members of the International Trauma Research Network (INTRN)21. Of the ACIT patients recruited between January 2008 and April 2015, all adult trauma patients who received at least 4 RBCs or more in 24 hours, were analysed. ACIT exclusion criteria included patients

152 | CHAPTER 9
who received >2 L intravenous fluids pre-hospital, who arrived >2 hours after injury in the Emergency Department (ED), who were transferred from other hospitals, who had burns covering >5% of the total body surface area, who had a known bleeding diathesis, who were taking anticoagulant medications other than aspirin (<650mg/day) or who declined to give informed consent, were excluded. Written informed consent was obtained from each patient or next of kin. This study was performed after approval by the local ethics committees and according to the declaration of Helsinki.
TRANSFUSION STRATEGY
Issuing of blood products, TXA and fibrinogen products by the blood bank was performed through locally implemented massive transfusion protocols (MTP) in all centres. The MTP was activated in most centres by physicians for patients with a systolic blood pressure <90 mmHg with an inadequate response to fluid administration and suspicion of ongoing bleeding. The applied ratio of blood products between hospitals ranged from 1:1:2 to 1:1:1. Oxford, Oslo and Amsterdam also used Octaplas®. Cryoprecipitate was used in London, Oxford and Copenhagen, whereas Amsterdam, Oslo and Cologne used fibrinogen concentrates. The trigger for fibrinogen administration differed between centres from a fibrinogen level ≤1.0 g/L to a fibrinogen level ≤1.5 g/L or was based on visco-elastic testing. TXA was a principal component in the MTPs of all hospitals. In London, Oxford, Oslo and Amsterdam, transfusion of blood products was monitored by conventional coagulation tests. In Copenhagen and Cologne, transfusion was guided by visco-elastic tests.
DATA COLLECTION
Research personnel screened and enrolled patients. The following data were collected prospectively in a centralized database: data on hospital, patient demographics, time of injury, mechanism (blunt or penetrating), comorbidities, vital signs and laboratory tests up to 24 hours post-injury, injury severity classified using the Abbreviated Injury Scale Score (AIS) and Injury Severity Score (ISS), requirement of surgical procedures, 24-hours mortality, total fluids (crystalloids, colloids, hypertonic saline), blood products (plasma, PLTs and RBCs), TXA, fibrinogen concentrates and cryoprecipitate administered within 24 hours.
To determine the effect of the transfusion strategy on the outcome, the following transfusion strategies were compared; high (≥1:1) and low (<1:1) ratios of plasma and PLTs to RBCs, the administration of TXA (yes/no) and fibrinogen products (fibrinogen concentrates and cryoprecipitate) (yes/no) within 24 hours. The number of PLT units was

| 153THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
corrected for the number of pooled donors.
The outcome of interest was the incidence of patients alive and free of massive transfusion within 24 hours. Massive transfusion was defined as the administration of ≥10 RBCs within 24 hours. Correction of TIC was defined as an INR ≤1.2 within 24 hours post injury. Of note, correction of coagulopathy was determined only in those patients who were still alive after 24 hours.
STATISTICS
In order to handle the problem of missing values, multiple imputation was performed, with the exception of missing outcome variables and variables with more than 50% missing. The mean predictive value was used to impute ten different datasets. The distribution of the original data was used to define constraints. Data were tested for distribution before multiple imputation. Skewed distribution of the original data was corrected with square root terms and log transformations. To test for differences in patient characteristics between the ratio, TXA and fibrinogen product groups, linear and logistic regression analyses were used. Furthermore, univariate logistic regression analyses were used to define possible confounders for the primary and secondary outcomes. Variables tested for a possible confounding effect were: age, gender, trauma mechanism, ISS, vital signs and laboratory tests in the ED, fluid administration, number of blood products transfused in 24 hours, surgical procedure and severe chest, limb or head injury (Appendix Table 1 and 2). Variables with a p-value of <0.20 were determined as having a relevant confounding effect and were included in the multivariable logistic regression models. Only those variables with a significant association with the primary and secondary outcomes after backward selection were included in the final multivariable logistic regression models. Subsequently, in a multilevel mixed effect logistic regression model, patients were clustered within each hospital. Multiple imputation was performed in R (an environment for statistical computing, R version 3.1.2 with R studio 0.98), further statistical analyses in SPSS version 21 (IBM, Chicago, IL, USA). A p-value <0.05 was considered to be statistically significant.
RESULTS
In total, 385 bleeding patients were included. The majority of the patients was male, suffered from blunt injury and was severely injured with a mean ISS of 31. Of the 385 bleeding patients, 216 patients (56%) received high plasma to RBC ratios and 150 patients (39%) received high PLT to RBC ratios. Additionally, 126 patients (34%) received TXA and 138 patients (36%) received fibrinogen products. Patients were coagulopathic with a mean initial INR of 1.3 and received a mean of 10 RBCs within 24 hours.
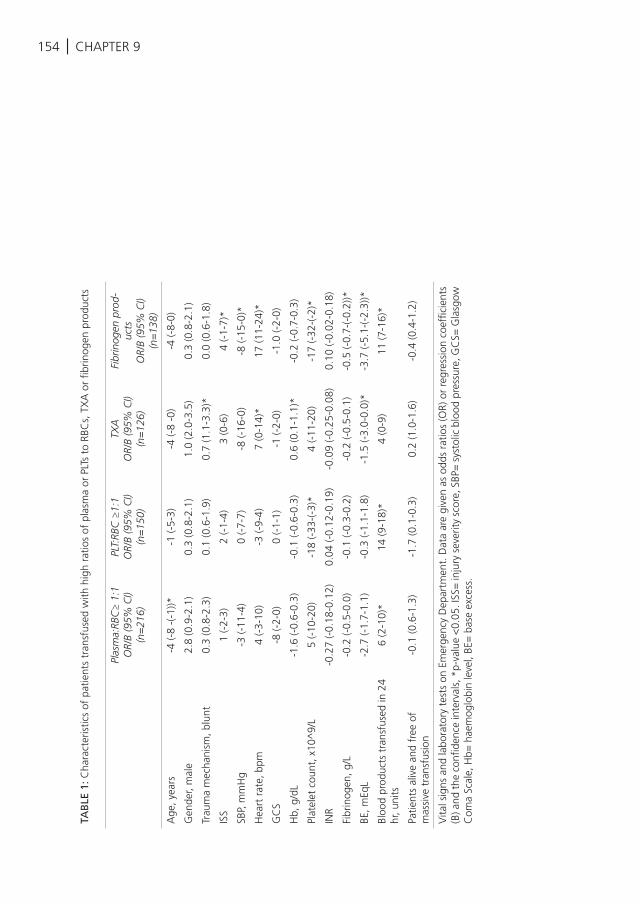
154 | CHAPTER 9
TAB
LE 1
: Cha
ract
eris
tics
of p
atie
nts
tran
sfus
ed w
ith h
igh
ratio
s of
pla
sma
or P
LTs
to R
BCs,
TX
A o
r fib
rinog
en p
rodu
cts
Plas
ma:
RBC
≥ 1
:1O
R/B
(95%
CI)
(n=
216)
PLT:
RBC
≥1:
1O
R/B
(95%
CI)
(n=
150)
TXA
OR/
B (9
5% C
I)(n
=12
6)
Fibr
inog
en p
rod-
ucts
OR/
B (9
5% C
I)(n
=13
8)
Age
, yea
rs-4
(-8
-(-1
))*-1
(-5-
3)-4
(-8
-0)
-4 (-
8-0)
Gen
der,
mal
e2.
8 (0
.9-2
.1)
0.3
(0.8
-2.1
)1.
0 (2
.0-3
.5)
0.3
(0.8
-2.1
)
Trau
ma
mec
hani
sm, b
lunt
0.3
(0.8
-2.3
)0.
1 (0
.6-1
.9)
0.7
(1.1
-3.3
)*0.
0 (0
.6-1
.8)
ISS
1 (-
2-3)
2 (-
1-4)
3 (0
-6)
4 (-
1-7)
*
SBP,
mm
Hg
-3 (-
11-4
)0
(-7-
7)-8
(-16
-0)
-8 (-
15-0
)*
Hea
rt r
ate,
bpm
4 (-
3-10
)-3
(-9-
4)7
(0-1
4)*
17 (1
1-24
)*
GC
S-8
(-2-
0)0
(-1-
1)-1
(-2-
0)-1
.0 (-
2-0)
Hb,
g/d
L-1
.6 (-
0.6-
0.3)
-0.1
(-0.
6-0.
3)0.
6 (0
.1-1
.1)*
-0.2
(-0.
7-0.
3)
Plat
elet
cou
nt, x
10^
9/L
5 (-
10-2
0)-1
8 (-
33-(
-3)*
4 (-
11-2
0)-1
7 (-
32-(
-2)*
INR
-0.2
7 (-
0.18
-0.1
2)0.
04 (-
0.12
-0.1
9)-0
.09
(-0.
25-0
.08)
0.10
(-0.
02-0
.18)
Fibr
inog
en, g
/L-0
.2 (-
0.5-
0.0)
-0.1
(-0.
3-0.
2)-0
.2 (-
0.5-
0.1)
-0.5
(-0.
7-(-
0.2)
)*
BE, m
EqL
-2.7
(-1.
7-1.
1)-0
.3 (-
1.1-
1.8)
-1.5
(-3.
0-0.
0)*
-3.7
(-5.
1-(-
2.3)
)*
Bloo
d pr
oduc
ts t
rans
fuse
d in
24
hr, u
nits
6 (2
-10)
*14
(9-1
8)*
4 (0
-9)
11 (7
-16)
*
Patie
nts
aliv
e an
d fr
ee o
f m
assi
ve t
rans
fusi
on-0
.1 (0
.6-1
.3)
-1.7
(0.1
-0.3
)0.
2 (1
.0-1
.6)
-0.4
(0.4
-1.2
)
Vita
l sig
ns a
nd la
bora
tory
tes
ts o
n Em
erge
ncy
Dep
artm
ent.
Dat
a ar
e gi
ven
as o
dds
ratio
s (O
R) o
r re
gres
sion
coe
ffici
ents
(B
) and
the
con
fiden
ce in
terv
als,
*p-
valu
e <
0.05
. ISS
= in
jury
sev
erity
sco
re, S
BP=
sys
tolic
blo
od p
ress
ure,
GC
S= G
lasg
ow
Com
a Sc
ale,
Hb=
hae
mog
lobi
n le
vel,
BE=
bas
e ex
cess
.
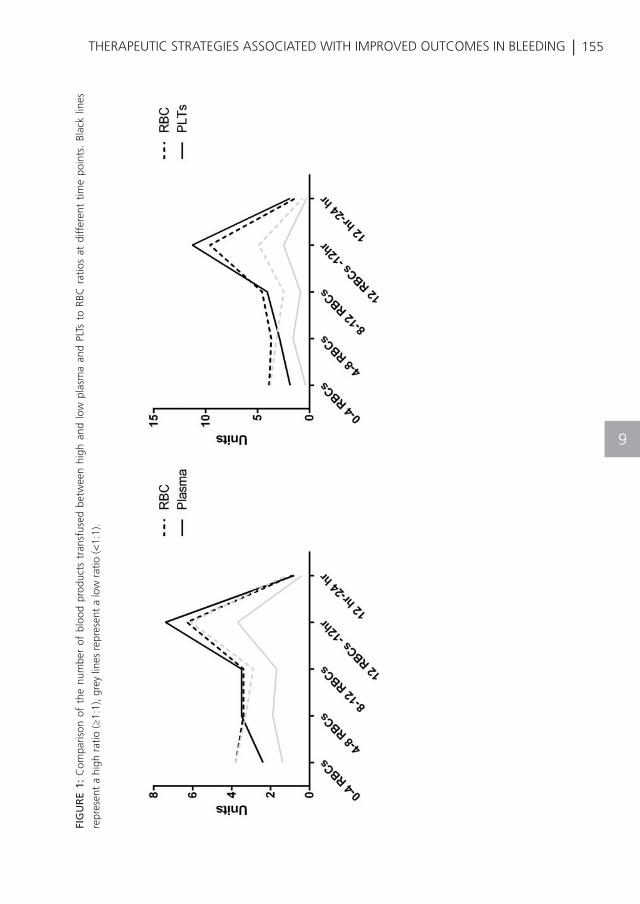
| 155THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
FIG
UR
E 1:
Com
paris
on o
f th
e nu
mbe
r of
blo
od p
rodu
cts
tran
sfus
ed b
etw
een
high
and
low
pla
sma
and
PLTs
to
RBC
rat
ios
at d
iffer
ent
time
poin
ts.
Blac
k lin
es
repr
esen
t a
high
rat
io (≥
1:1)
, gre
y lin
es r
epre
sent
a lo
w r
atio
(<1:
1).
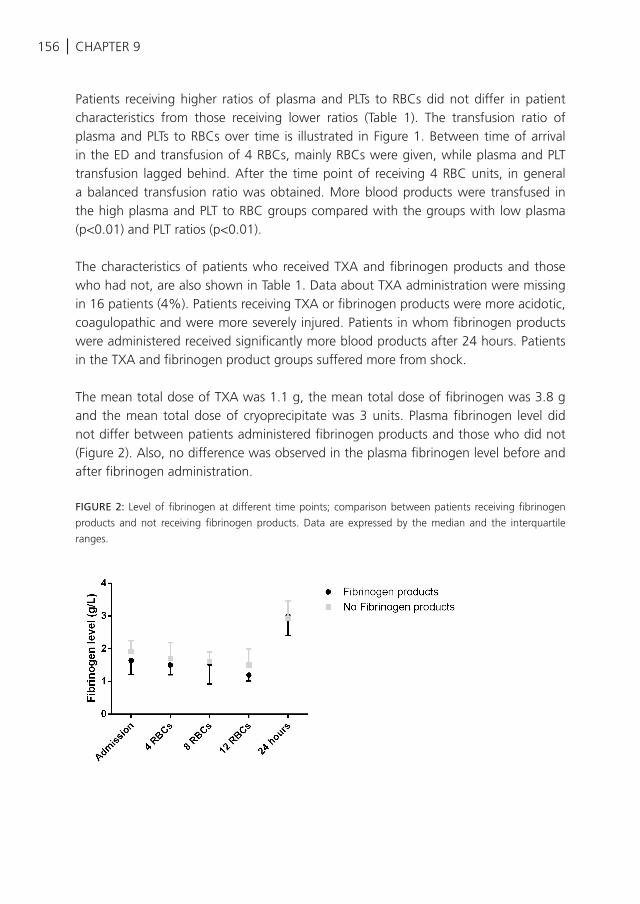
156 | CHAPTER 9
Patients receiving higher ratios of plasma and PLTs to RBCs did not differ in patient characteristics from those receiving lower ratios (Table 1). The transfusion ratio of plasma and PLTs to RBCs over time is illustrated in Figure 1. Between time of arrival in the ED and transfusion of 4 RBCs, mainly RBCs were given, while plasma and PLT transfusion lagged behind. After the time point of receiving 4 RBC units, in general a balanced transfusion ratio was obtained. More blood products were transfused in the high plasma and PLT to RBC groups compared with the groups with low plasma (p<0.01) and PLT ratios (p<0.01).
The characteristics of patients who received TXA and fibrinogen products and those who had not, are also shown in Table 1. Data about TXA administration were missing in 16 patients (4%). Patients receiving TXA or fibrinogen products were more acidotic, coagulopathic and were more severely injured. Patients in whom fibrinogen products were administered received significantly more blood products after 24 hours. Patients in the TXA and fibrinogen product groups suffered more from shock.
The mean total dose of TXA was 1.1 g, the mean total dose of fibrinogen was 3.8 g and the mean total dose of cryoprecipitate was 3 units. Plasma fibrinogen level did not differ between patients administered fibrinogen products and those who did not (Figure 2). Also, no difference was observed in the plasma fibrinogen level before and after fibrinogen administration.
FIGURE 2: Level of fibrinogen at different time points; comparison between patients receiving fibrinogen
products and not receiving fibrinogen products. Data are expressed by the median and the interquartile
ranges.
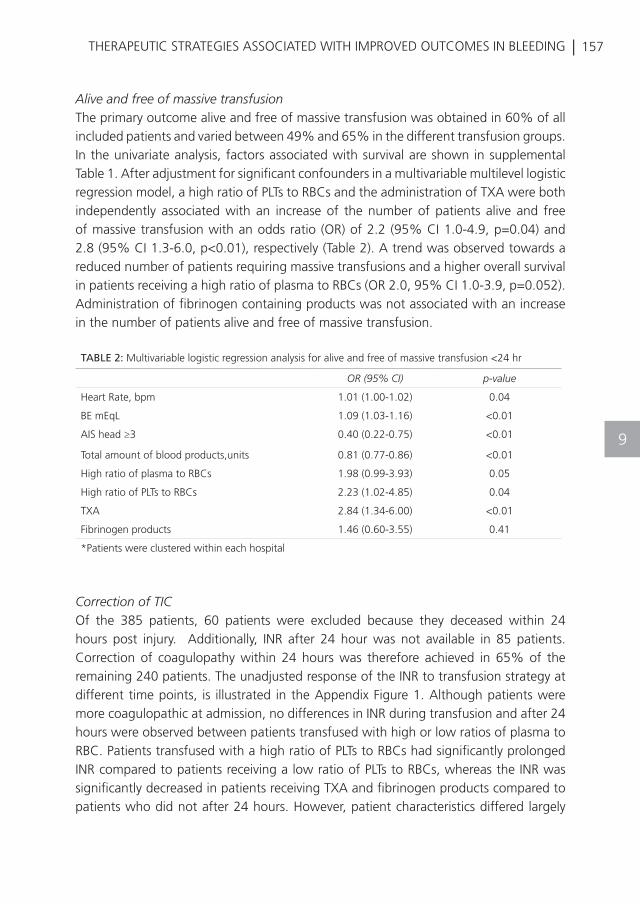
| 157THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
Alive and free of massive transfusionThe primary outcome alive and free of massive transfusion was obtained in 60% of all included patients and varied between 49% and 65% in the different transfusion groups. In the univariate analysis, factors associated with survival are shown in supplemental Table 1. After adjustment for significant confounders in a multivariable multilevel logistic regression model, a high ratio of PLTs to RBCs and the administration of TXA were both independently associated with an increase of the number of patients alive and free of massive transfusion with an odds ratio (OR) of 2.2 (95% CI 1.0-4.9, p=0.04) and 2.8 (95% CI 1.3-6.0, p<0.01), respectively (Table 2). A trend was observed towards a reduced number of patients requiring massive transfusions and a higher overall survival in patients receiving a high ratio of plasma to RBCs (OR 2.0, 95% CI 1.0-3.9, p=0.052). Administration of fibrinogen containing products was not associated with an increase in the number of patients alive and free of massive transfusion.
Correction of TICOf the 385 patients, 60 patients were excluded because they deceased within 24 hours post injury. Additionally, INR after 24 hour was not available in 85 patients. Correction of coagulopathy within 24 hours was therefore achieved in 65% of the remaining 240 patients. The unadjusted response of the INR to transfusion strategy at different time points, is illustrated in the Appendix Figure 1. Although patients were more coagulopathic at admission, no differences in INR during transfusion and after 24 hours were observed between patients transfused with high or low ratios of plasma to RBC. Patients transfused with a high ratio of PLTs to RBCs had significantly prolonged INR compared to patients receiving a low ratio of PLTs to RBCs, whereas the INR was significantly decreased in patients receiving TXA and fibrinogen products compared to patients who did not after 24 hours. However, patient characteristics differed largely
TABLE 2: Multivariable logistic regression analysis for alive and free of massive transfusion <24 hr
OR (95% CI) p-value
Heart Rate, bpm 1.01 (1.00-1.02) 0.04
BE mEqL 1.09 (1.03-1.16) <0.01
AIS head ≥3 0.40 (0.22-0.75) <0.01
Total amount of blood products,units 0.81 (0.77-0.86) <0.01
High ratio of plasma to RBCs 1.98 (0.99-3.93) 0.05
High ratio of PLTs to RBCs 2.23 (1.02-4.85) 0.04
TXA 2.84 (1.34-6.00) <0.01
Fibrinogen products 1.46 (0.60-3.55) 0.41
*Patients were clustered within each hospital
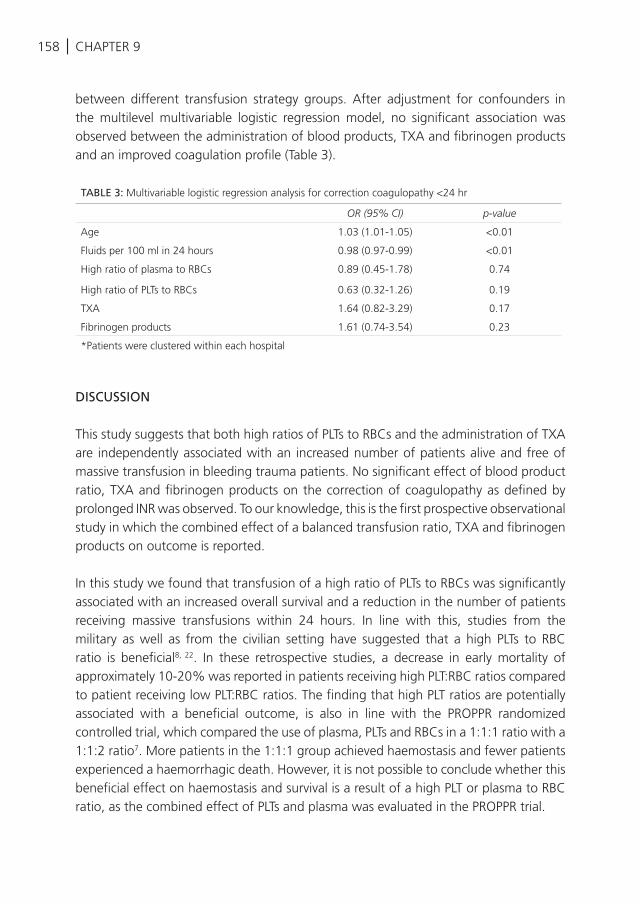
158 | CHAPTER 9
between different transfusion strategy groups. After adjustment for confounders in the multilevel multivariable logistic regression model, no significant association was observed between the administration of blood products, TXA and fibrinogen products and an improved coagulation profile (Table 3).
DISCUSSION
This study suggests that both high ratios of PLTs to RBCs and the administration of TXA are independently associated with an increased number of patients alive and free of massive transfusion in bleeding trauma patients. No significant effect of blood product ratio, TXA and fibrinogen products on the correction of coagulopathy as defined by prolonged INR was observed. To our knowledge, this is the first prospective observational study in which the combined effect of a balanced transfusion ratio, TXA and fibrinogen products on outcome is reported.
In this study we found that transfusion of a high ratio of PLTs to RBCs was significantly associated with an increased overall survival and a reduction in the number of patients receiving massive transfusions within 24 hours. In line with this, studies from the military as well as from the civilian setting have suggested that a high PLTs to RBC ratio is beneficial8, 22. In these retrospective studies, a decrease in early mortality of approximately 10-20% was reported in patients receiving high PLT:RBC ratios compared to patient receiving low PLT:RBC ratios. The finding that high PLT ratios are potentially associated with a beneficial outcome, is also in line with the PROPPR randomized controlled trial, which compared the use of plasma, PLTs and RBCs in a 1:1:1 ratio with a 1:1:2 ratio7. More patients in the 1:1:1 group achieved haemostasis and fewer patients experienced a haemorrhagic death. However, it is not possible to conclude whether this beneficial effect on haemostasis and survival is a result of a high PLT or plasma to RBC ratio, as the combined effect of PLTs and plasma was evaluated in the PROPPR trial.
TABLE 3: Multivariable logistic regression analysis for correction coagulopathy <24 hr
OR (95% CI) p-value
Age 1.03 (1.01-1.05) <0.01
Fluids per 100 ml in 24 hours 0.98 (0.97-0.99) <0.01
High ratio of plasma to RBCs 0.89 (0.45-1.78) 0.74
High ratio of PLTs to RBCs 0.63 (0.32-1.26) 0.19
TXA 1.64 (0.82-3.29) 0.17
Fibrinogen products 1.61 (0.74-3.54) 0.23
*Patients were clustered within each hospital
| 159THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
We found a less strong effect of transfusion of high plasma to RBCs ratio on outcome. No significant association, but only a trend, was found between a high plasma to RBC ratio and improved survival. This is in apparent contrast with the PROPPR trial. There may be several explanations. The PROPPR trial investigated the effect of a balanced transfusion ratio, whereas we investigated the combined effect of blood product ratio, TXA and fibrinogen products. In the PROPPR trial, TXA and fibrinogen containing products were given to a minority of patients, whereas in this study 54% of the patients received either TXA or fibrinogen products. We hypothesize that the effect of TXA partly outweighs the benefit of an increased plasma to RBC ratio. In line with this, TXA had a strong effect on survival in this study, even though patients in the TXA group were more severely ill, as demonstrated by a higher heart rate and base excess level at baseline. Alternatively, differences between the studies may be due to differences in outcome parameters and sample sizes. We have combined haemostasis and mortality in the primary outcome “alive and free of massive transfusion” because transfusion strategy is in the first place targeted on bleeding control and secondly on decreasing mortality. Previous studies have determined these outcome measures separately5-8, 10.
Administration of TXA was associated with increased survival of patients alive and free of massive transfusion. These findings are in accordance with the CRASH-II trial, which showed that TXA was able to reduce the risk of death from traumatic bleeding when TXA was administered within 3 hours post injury17.
Somewhat surprisingly, no effect of fibrinogen products on outcome was found, even though the mean fibrinogen level in these bleeding patients was below 2 g/L. An explanation may be that the level of fibrinogen did not increase over time in patients administered fibrinogen products compared to patients who did not receive any fibrinogen products in addition to plasma. This may indicate that the dose of fibrinogen substitution may have been too low to have an effect and that higher dosages are required to achieve a therapeutic effect. This hypothesis is in accordance with the guidelines in which amounts of 4-8 g are recommended for severe bleeding patients23. Whether fibrinogen products are beneficial in a setting in which balanced resuscitation is practiced, requires a randomized trial with a sufficient dose.
Limitations of this study are that we included patients who were administered with at least 4 units of RBCs, whereas the majority of the previous studies examined transfusion strategies in massively transfused patients (≥10 RBCs within 24 hours) or transfused patients (≥1 RBC transfused), which hampers the comparability of this study. However, we have chosen to use the definition of at least 4 RBCs transfused in order to include patients with a relevant bleeding but with a possibility that an optimal transfusion
160 | CHAPTER 9
strategy might also prevent patients from massive transfusion. Furthermore, prolonged INR was used to define coagulopathy which has not been validated for monitoring coagulopathy24-27. The INR represents a part of the coagulation profile and is not able to visualize the complete coagulation process, including clot formation, clot firmness and clot breakdown. However, although the INR as predictor for coagulopathy has not been validated, it is generally used as reference for the definition of trauma-induced coagulopathy. Furthermore, INR is frequently used in clinical practice and is a good prognosticator of outcome in massive haemorrhage28-30. Moreover, adverse events such as thromboembolism or organ failure were not recorded in this study, limiting a risk-benefit analysis of any transfusion strategy. This study also has strengths. We combined all transfusion strategies into one model, which is a better reflection of the fact that all treatment interventions interact with outcome.
CONCLUSION
High PLT to RBC ratio and TXA are associated with an increased number of patients alive and free of massive transfusion. Blood product ratio, TXA and fibrinogen products did not correct coagulopathy as defined by prolonged INR. Fibrinogen products did not affect outcome, however under-dosing may have influenced the outcome. These findings may offer guidance for designing a randomized controlled trial, in which the effect of the addition of TXA and fibrinogen products to a balanced resuscitation is investigated.

| 161THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
162 |
REFERENCES
CHAPTER 9
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
US Centers for Disease Control and
Prevention. Injury prevention and control:
data and statistics, 2012. 2014.
Brohi K, Singh J, Heron M, Coats T.
Acute traumatic coagulopathy. J Trauma.
2003;54(6):1127-30.
MacLeod JB, Lynn M, McKenney MG, Cohn
SM, Murtha M. Early coagulopathy predicts
mortality in trauma. J Trauma. 2003;55(1):39-
44.
Davenport R, Manson J, De’Ath H, Platton
S, Coates A, Allard S, et al. Functional
definition and characterization of acute
traumatic coagulopathy. Crit Care Med
2011;39(12):2652-8.
Borgman MA, Spinella PC, Perkins JG,
Grathwohl KW, Repine T, Beekley AC, et
al. The ratio of blood products transfused
affects mortality in patients receiving massive
transfusions at a combat support hospital. J
Trauma. 2007;63(4):805-13.
Holcomb JB, del Junco DJ, Fox EE, Wade
CE, Cohen MJ, Schreiber MA, et al. The
prospective, observational, multicenter,
major trauma transfusion (PROMMTT) study:
comparative effectiveness of a time-varying
treatment with competing risks. JAMA Surg
2013;148(2):127-36.
Holcomb JB, Tilley BC, Baraniuk S, Fox EE,
Wade CE, Podbielski JM, et al. Transfusion
of plasma, platelets, and red blood cells in a
1:1:1 vs a 1:1:2 ratio and mortality in patients
with severe trauma: the PROPPR randomized
clinical trial. JAMA. 2015;313(5):471-82.
Holcomb JB, Zarzabal LA, Michalek JE, Kozar
RA, Spinella PC, Perkins JG, et al. Increased
platelet:RBC ratios are associated with
improved survival after massive transfusion. J
Trauma. 2011;71(2 Suppl 3):S318-28.
Johansson PI, Oliveri RS, Ostrowski SR.
Hemostatic resuscitation with plasma and
platelets in trauma. J Emerg Trauma Shock.
2012;5(2):120-5.
Holcomb JB, Jenkins D, Rhee P, Johannigman
J, Mahoney P, Mehta S, et al. Damage
control resuscitation: directly addressing the
early coagulopathy of trauma. J Trauma.
2007;62(2):307-10.
Fenger-Eriksen C, Lindberg-Larsen M,
Christensen AQ, Ingerslev J, Sorensen B.
Fibrinogen concentrate substitution therapy
in patients with massive haemorrhage and
low plasma fibrinogen concentrations. British
journal of anaesthesia. 2008;101(6):769-73.
Fries D. The early use of fibrinogen,
prothrombin complex concentrate, and
recombinant-activated factor VIIa in massive
bleeding. Transfusion. 2013;53 Suppl 1:91s-
5s.
Stinger HK, Spinella PC, Perkins JG,
Grathwohl KW, Salinas J, Martini WZ, et al.
The ratio of fibrinogen to red cells transfused
affects survival in casualties receiving massive
transfusions at an army combat support
hospital. J Trauma. 2008;64(2 Suppl):S79-85;
discussion S.
Morrison JJ, Dubose JJ, Rasmussen TE,
Midwinter MJ. Military Application of
Tranexamic Acid in Trauma Emergency
Resuscitation (MATTERs) Study. Arch Surg
2012;147(2):113-9.
Morrison JJ, Ross JD, Dubose JJ, Jansen JO,
Midwinter MJ, Rasmussen TE. Association
of cryoprecipitate and tranexamic acid with
improved survival following wartime injury:
findings from the MATTERs II Study. JAMA
Surg. 2013;148(3):218-25.
Porta CR, Nelson D, McVay D, Salgar S, Eckert
M, Izenberg S, et al. The effects of tranexamic
acid and prothrombin complex concentrate
on the coagulopathy of trauma: an in vitro
analysis of the impact of severe acidosis. J
Trauma Acute Care Surg 2013;75(6):954-60.
Shakur H, Roberts I, Bautista R, Caballero J,
Coats T, Dewan Y, et al. Effects of tranexamic
acid on death, vascular occlusive events,
and blood transfusion in trauma patients
with significant haemorrhage (CRASH-2): a
| 163
REFERENCES
THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
18
19
20
21
22
23
24
25
26
27
28
29
30
randomised, placebo-controlled trial. Lancet.
2010;376(9734):23-32.
Cole E, Davenport R, Willett K, Brohi K.
Tranexamic acid use in severely injured civilian
patients and the effects on outcomes: a
prospective cohort study. Annals of surgery.
2015;261(2):390-4.
Holcomb JB, Fox EE, Zhang X, White N, Wade
CE, Cotton BA, et al. Cryoprecipitate use in
the PROMMTT study. J Trauma Acute Care
Surg. 2013;75(1 Suppl 1):S31-9.
Spahn DR, Bouillon B, Cerny V, Coats TJ,
Duranteau J, Fernandez-Mondejar E, et al.
Management of bleeding and coagulopathy
following major trauma: an updated European
guideline. Crit Care. 2013;17(2):R76.
Schafer N, Driessen A, Frohlich M, Sturmer EK,
Maegele M. Diversity in clinical management
and protocols for the treatment of major
bleeding trauma patients across European
level I Trauma Centres. Scand J Trauma Resusc
Emerg Med. 2015;23(1):74.
Perkins JG, Cap AP, Spinella PC, Blackbourne
LH, Grathwohl KW, Repine TB, et al. An
evaluation of the impact of apheresis platelets
used in the setting of massively transfused
trauma patients. J Trauma. 2009;66(4
Suppl):S77-84; discussion S-5.
Summary of Product Characteristics (SPC)
Haemocomplettan.
McCully SP, Fabricant LJ, Kunio NR, Groat
TL, Watson KM, Differding JA, et al. The
International Normalized Ratio overestimates
coagulopathy in stable trauma and surgical
patients. J Trauma Acute Care Surg.
2013;75(6):947-53.
Haas T, Spielmann N, Mauch J, Madjdpour
C, Speer O, Schmugge M, et al. Comparison
of thromboelastometry (ROTEM(R)) with
standard plasmatic coagulation testing
in paediatric surgery. British journal of
anaesthesia. 2012;108(1):36-41.
Hagemo JS, Christiaans SC, Stanworth SJ,
Brohi K, Johansson PI, Goslings JC, et al.
Detection of acute traumatic coagulopathy
and massive transfusion requirements by
means of rotational thromboelastometry: an
international prospective validation study. Crit
Care. 2015;19:97.
Holcomb JB, Minei KM, Scerbo ML, Radwan
ZA, Wade CE, Kozar RA, et al. Admission
rapid thrombelastography can replace
conventional coagulation tests in the
emergency department: experience with
1974 consecutive trauma patients. Annals of
surgery. 2012;256(3):476-86.
Hsu JM, Hitos K, Fletcher JP. Identifying the
bleeding trauma patient: predictive factors
for massive transfusion in an Australasian
trauma population. J Trauma Acute Care Surg.
2013;75(3):359-64.
Callcut RA, Cotton BA, Muskat P, Fox EE,
Wade CE, Holcomb JB, et al. Defining when to
initiate massive transfusion: a validation study
of individual massive transfusion triggers in
PROMMTT patients. J Trauma Acute Care
Surg. 2013;74(1):59-65, 7-8; discussion 6-7.
Goodman MD, Makley AT, Hanseman DJ, Pritts
TA, Robinson BR. All the bang without the
bucks: Defining essential point-of-care testing
for traumatic coagulopathy. J Trauma Acute
Care Surg. 2015;79(1):117-24; discussion 24.
9
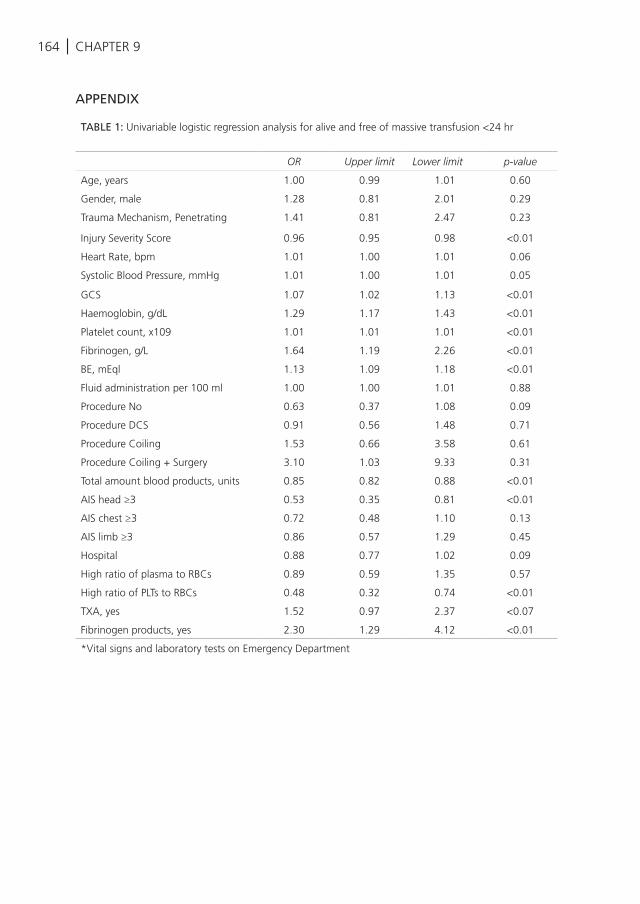
164 | CHAPTER 9
APPENDIX
TABLE 1: Univariable logistic regression analysis for alive and free of massive transfusion <24 hr
OR Upper limit Lower limit p-value
Age, years 1.00 0.99 1.01 0.60
Gender, male 1.28 0.81 2.01 0.29
Trauma Mechanism, Penetrating 1.41 0.81 2.47 0.23
Injury Severity Score 0.96 0.95 0.98 <0.01
Heart Rate, bpm 1.01 1.00 1.01 0.06
Systolic Blood Pressure, mmHg 1.01 1.00 1.01 0.05
GCS 1.07 1.02 1.13 <0.01
Haemoglobin, g/dL 1.29 1.17 1.43 <0.01
Platelet count, x109 1.01 1.01 1.01 <0.01
Fibrinogen, g/L 1.64 1.19 2.26 <0.01
BE, mEql 1.13 1.09 1.18 <0.01
Fluid administration per 100 ml 1.00 1.00 1.01 0.88
Procedure No 0.63 0.37 1.08 0.09
Procedure DCS 0.91 0.56 1.48 0.71
Procedure Coiling 1.53 0.66 3.58 0.61
Procedure Coiling + Surgery 3.10 1.03 9.33 0.31
Total amount blood products, units 0.85 0.82 0.88 <0.01
AIS head ≥3 0.53 0.35 0.81 <0.01
AIS chest ≥3 0.72 0.48 1.10 0.13
AIS limb ≥3 0.86 0.57 1.29 0.45
Hospital 0.88 0.77 1.02 0.09
High ratio of plasma to RBCs 0.89 0.59 1.35 0.57
High ratio of PLTs to RBCs 0.48 0.32 0.74 <0.01
TXA, yes 1.52 0.97 2.37 <0.07
Fibrinogen products, yes 2.30 1.29 4.12 <0.01
*Vital signs and laboratory tests on Emergency Department
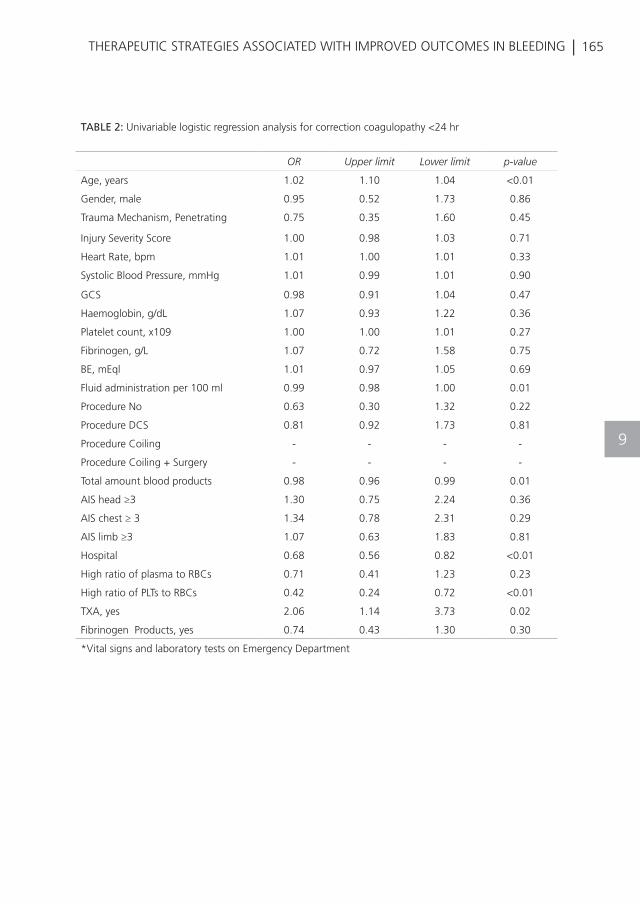
| 165THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
TABLE 2: Univariable logistic regression analysis for correction coagulopathy <24 hr
OR Upper limit Lower limit p-value
Age, years 1.02 1.10 1.04 <0.01
Gender, male 0.95 0.52 1.73 0.86
Trauma Mechanism, Penetrating 0.75 0.35 1.60 0.45
Injury Severity Score 1.00 0.98 1.03 0.71
Heart Rate, bpm 1.01 1.00 1.01 0.33
Systolic Blood Pressure, mmHg 1.01 0.99 1.01 0.90
GCS 0.98 0.91 1.04 0.47
Haemoglobin, g/dL 1.07 0.93 1.22 0.36
Platelet count, x109 1.00 1.00 1.01 0.27
Fibrinogen, g/L 1.07 0.72 1.58 0.75
BE, mEql 1.01 0.97 1.05 0.69
Fluid administration per 100 ml 0.99 0.98 1.00 0.01
Procedure No 0.63 0.30 1.32 0.22
Procedure DCS 0.81 0.92 1.73 0.81
Procedure Coiling - - - -
Procedure Coiling + Surgery - - - -
Total amount blood products 0.98 0.96 0.99 0.01
AIS head ≥3 1.30 0.75 2.24 0.36
AIS chest ≥ 3 1.34 0.78 2.31 0.29
AIS limb ≥3 1.07 0.63 1.83 0.81
Hospital 0.68 0.56 0.82 <0.01
High ratio of plasma to RBCs 0.71 0.41 1.23 0.23
High ratio of PLTs to RBCs 0.42 0.24 0.72 <0.01
TXA, yes 2.06 1.14 3.73 0.02
Fibrinogen Products, yes 0.74 0.43 1.30 0.30
*Vital signs and laboratory tests on Emergency Department
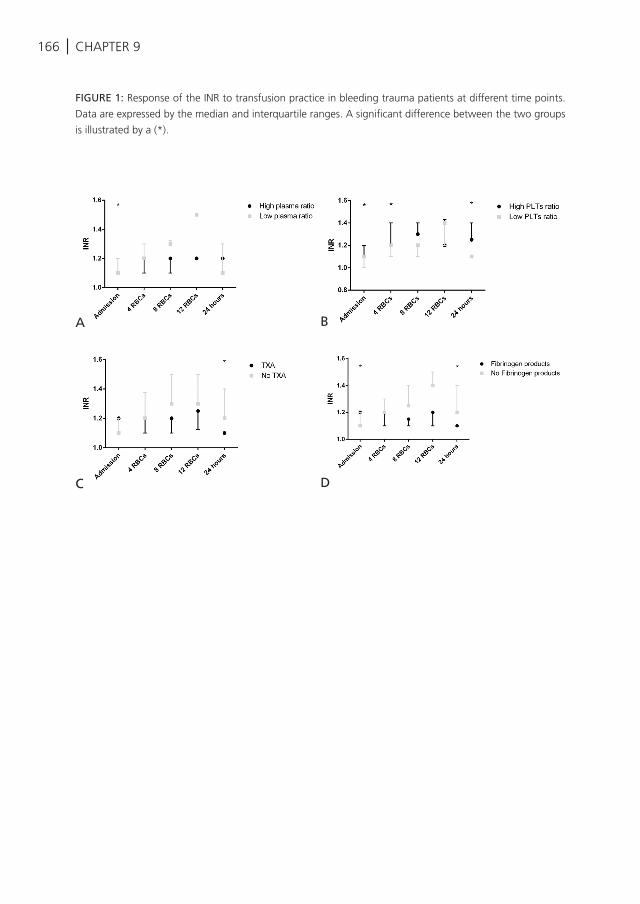
166 | CHAPTER 9
FIGURE 1: Response of the INR to transfusion practice in bleeding trauma patients at different time points.
Data are expressed by the median and interquartile ranges. A significant difference between the two groups
is illustrated by a (*).
A B
C D

| 167THERAPEUTIC STRATEGIES ASSOCIATED WITH IMPROVED OUTCOMES IN BLEEDING
9
K. Balvers, S. van Dieren, K. Baksaas-Aasen, C. Gaarder, K. Brohi, S. Eaglestone, S. Stanworth, P.I. Johansson, S.R. Ostrowski, J. Stensballe,
M. Maegele, J.C. Goslings, N.P. Juffermans, TACTIC partners
Submitted
TRANSFUSION STRATEGY ASSOCIATED WITH CORRECTION OF COAGULOPATHY AS DETECTED BY
ROTEM® IN BLEEDING TRAUMA PATIENTS
10
170 | CHAPTER 10
ABSTRACT
Introduction: Viscoelastic Heamostatic Assays, like Rotational Thromboelastometry (ROTEM®) have shown promising results in their ability to identify trauma-induced coagulopathy. However, the response of ROTEM® to blood products, anti-fibrinolytic and pro-coagulant therapy is unknown. Knowledge on the ROTEM® response to therapy can be used to construct ROTEM®-based algorithms which monitor transfusion therapy. The aim of this study was to determine which transfusion strategy is associated with normalization of deranged VHA profiles measured by ROTEM®. In addition, differences in responses to therapy between specific trauma patient groups were analysed.
Methods: In this prospective multicentre observational study, all adult trauma patients who received at least 4 red blood cell units (RBCs) and who were alive 24 hours post injury, were recruited. Blood was drawn on arrival in the Emergency Department, and after administration of 4, 8 and 12 RBCs. Follow-up samples were taken 24 and 72 hours post injury. The response of consecutive ROTEM® assays (EXTEM and FIBTEM) to transfusion with low (<1:1) and high (≥1:1) ratios of plasma and platelets (PLTs) to red blood cells (RBCs) as well as to the administration of tranexamic acid (TXA) or fibrinogen products (cryoprecipitate and fibrinogen concentrates) was evaluated. Linear regression analyses were used to relate therapy to changes in ROTEM® tracings. Subgroup analyses were performed on age, shock and traumatic brain injury.
Results: In total, 309 bleeding patients were included. Transfusion of high plasma to RBC ratios was associated with a decrease in EXTEM CT of 23 (-45 to 1) seconds compared to transfusion of a low plasma ratio, but did not influence other ROTEM® values. A high PLT to RBC ratio was also associated with a decrease in EXTEM CT of 35 (-58 to -12) seconds. In addition, high PLT to RBC ratio also increased EXTEM CA5, MCF, CA10, alpha angle, FIBTEM CA5, CA10 and MCF compared to transfusion with low RBC to PLT ratios. Administration of TXA and fibrinogen products was associated with an increased FIBTEM CA5, CA10, alpha angle and MCF. Additionally, EXTEM and FIBITEM Li30 were reduced by TXA. Subgroup analyses indicated that improvement of VHA assays after transfusion of a high PLT to RBC ratio and fibrinogen concentrates was present in younger patients and in patients with TBI but not in elderly patients and those without TBI. TXA was associated with a reduced fibrinolysis in patients with shock.
Conclusion: A high PLT to RBC ratio is associated with a more profound correction of CT than high plasma to RBC ratio, as well as by improvement of a multitude of ROTEM® parameters of clot formation, suggesting that platelets play an important role in trauma-
| 171CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
related coagulopathy. TXA reduced fibrinolysis and fibrinogen products improved clot formation and firmness. Whether a transfusion therapy aimed at correction of ROTEM® parameters results in improved outcome in trauma requires further study. Additionally, our data suggest that transfusion therapy in trauma patients with the aim to correct coagulopathy should be personalized.
172 | CHAPTER 10
INTRODUCTION
Trauma-induced coagulopathy (TIC) develops in up to 25% of severely injured trauma patients, which aggravates massive haemorrhage and is associated with increased mortality1, 2. Recent data suggest that bleeding trauma patients should empirically be transfused in a balanced resuscitation approach, which includes a 1:1:1 ratio of blood products, in order to reduce the incidence of TIC and mortality3-5. However, transfusion is also associated with adverse outcome, including infections6, acute respiratory distress syndrome (ARDS)7, 8 and the development of multiple organ failure9-12. Together, the outcome of traumatic bleeding is optimal with control of TIC with early balanced resuscitation while avoiding unnecessary transfusion.
Monitoring of haemostasis is essential in achieving a balance between correction of TIC and overtransfusion. Conventional clotting tests, like prothrombin time (PT), activated partial thromboplastin time (APTT), International Normalized Ratio (INR), platelet count, fibrinogen and D-dimer levels, only partly reflect in vivo haemostatic potential and are too time-consuming, which renders them useless in guiding resuscitation strategy13-15.
Viscoelastic Heamostatic Assays (VHA), like Rotational Thromboelastometry (ROTEM®, trademark of TEM international GmbH, Munich, Germany: www.ROTEM®.de), are rapid tests and have shown promising results in their ability to identify TIC in trauma patients16-18. Previous observational studies suggest that the use of VHA targeted haemostatic resuscitation is associated with an improved outcome in trauma patients19-22.As a result, treatment algorithms using VHA tests have been published, even though data on the response of ROTEM® parameters to specific ratio therapy or anti-fibrinolytic and pro-coagulant therapy are largely absent.
Currently, all trauma patients are transfused in the same fashion. However, coagulation abnormalities may differ between patient populations, indicating that a personalized transfusion strategy may improve outcome after trauma.
The aim of this study was to determine which transfusion strategy was associated with normalization of TIC as assessed by ROTEM®. In this analysis, we determined whether specific patient populations respond differently to transfusion therapy in terms of normalization of ROTEM® parameters.
METHODS
As part of a prospective multicentre observational study, named the Activation of
| 173CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
Coagulation and Inflammation in Trauma (ACIT) study (United Kingdom Clinical Research Network Study Portfolio, ID: 5637), this study was performed in 6 European level-1 trauma centres; London, Oslo, Copenhagen, Oxford, Cologne and Amsterdam, which are members of the International Trauma Research Network (INTRN). All adult trauma patients (age ≥18 years) who required a full trauma team activation, who received at least 4 units of RBCs within 24 hours and who were still alive after 24 hours, were recruited between January 2008 and April 2015. Patients who received >2 L intravenous fluids pre-hospital, who arrived >2 hours after injury in the Emergency Department (ED), who were transferred from other hospitals and patients who had burns covering more than 5% of the total body surface area, were not eligible. Patients were retrospectively excluded if they declined to give informed consent, were taking anticoagulant medications other than aspirin (<650mg/day), had moderate or severe liver disease (Child’s classification B or C3) , had a known bleeding diathesis, had no ROTEM® measurements available or died within 24 hours post-injury.
Written informed consent was obtained from each patient. When the patient was unconscious, written informed consent was obtained from a legal representative. This study was conducted according to the Statement of the Declaration of Helsinki and performed after approval by the local ethics committees.
BLOOD SAMPLING AND ROTEM® ASSAYS
Blood was drawn and collected in citrated tubes immediately on arrival in the ED and after 24 and 72 hours post injury. Additionally, blood samples were drawn after administration of 4, 8 and 12 RBCs. Two ROTEM® assays (EXTEM and FIBTEM) were performed by trained personnel within half an hour after blood samples were taken. Within each assay 6 ROTEM® parameters were analysed; the clotting time (CT), the clot amplitude after 5 minutes (CA5), the clot amplitude after 10 minutes (CA10), the angle of tangent at 2 mm amplitude (alpha angle), the maximum clot firmness (MCF) and the lysis index of the clot after 30 minutes (Li30).
TRANSFUSION STRATEGY
In all trauma centres, issuing of blood products, anti-fibrinolytic and pro-coagulant agents by the blood bank was performed through locally implemented massive transfusion protocols (MTP). In most centres, the MTP was activated for patients with a systolic blood pressure <90 mmHg with inadequate response to fluid administration and suspicion of an ongoing bleeding. All centres intended to apply blood products in a ratio ranged from 1:1:2 to 1:1:1. Tranexamic acid (TXA) was used as a principle

174 | CHAPTER 10
component of the MTP in all centres. Cryoprecipitate was used in London, Oxford and Copenhagen, whereas Oslo, Cologne and Amsterdam used fibrinogen concentrates. The trigger for fibrinogen products differed between centres from a fibrinogen level ≤1.0 g/L in London to a fibrinogen level ≤2.0 g/L in Oslo.
DATA COLLECTION
The following data were collected prospectively to a centralized database: data on patient demographics, time of injury, trauma mechanism, vital signs and laboratory tests up to 72 hours post-injury, Injury Severity Score (ISS), Abbreviated Injury Scale Score (AIS), 24-hours and 28-day mortality, total fluids (crystalloids, colloids, hypertonic saline), blood products (RBCs, plasma and PLTs), anti-fibrinolytic (TXA) and pro-coagulant agents (fibrinogen concentrates, cryoprecipitate). To define the effect of transfusion practice on outcome, the following transfusion strategies were compared; high (≥1:1) and low (<1:1) ratios of plasma and PLTs to RBCs, receiving TXA or not and receiving fibrinogen products or not. Fibrinogen products included fibrinogen concentrates and cryoprecipitate. The number of PLT units was corrected for the number of pooled donors.
The effect of the use of different ratios of blood products on ROTEM® parameters was also analysed by relating the therapy given within a time interval to changes in ROTEM® results in the following consecutive time interval. The delta changes in VHA profiles between T=0 and T=RBC 4, between T=RBC 4 and T=RBC 8, between T=RBC 8 and T=RBC12, between T=RBC 12 and T=24 and between T=24 and T=72 were linked to the transfusion therapy given in the time interval which lies before, i.e. time between arrival in the ED and transfusion of 4 RBCs, transfusion of 4 and 8 RBCs, transfusion of 8 and 12 RBCs, transfusion of 12 RBCs and 24 hours post injury (Figure 1). This approach was chosen because VHA parameters change rapidly in response to blood products. To describe the effect of TXA and fibrinogen products on ROTEM® VHA profiles, the delta between T=0 and T=24 was used.
STATISTICS
Multiple imputation was performed in order to handle the problem of missing values. Predictive mean matching was performed to construct 10 different datasets. Skewed distribution of the original data was corrected with square root terms and log transformations. Outcome variables and variables with more than 50% missing were not imputed.
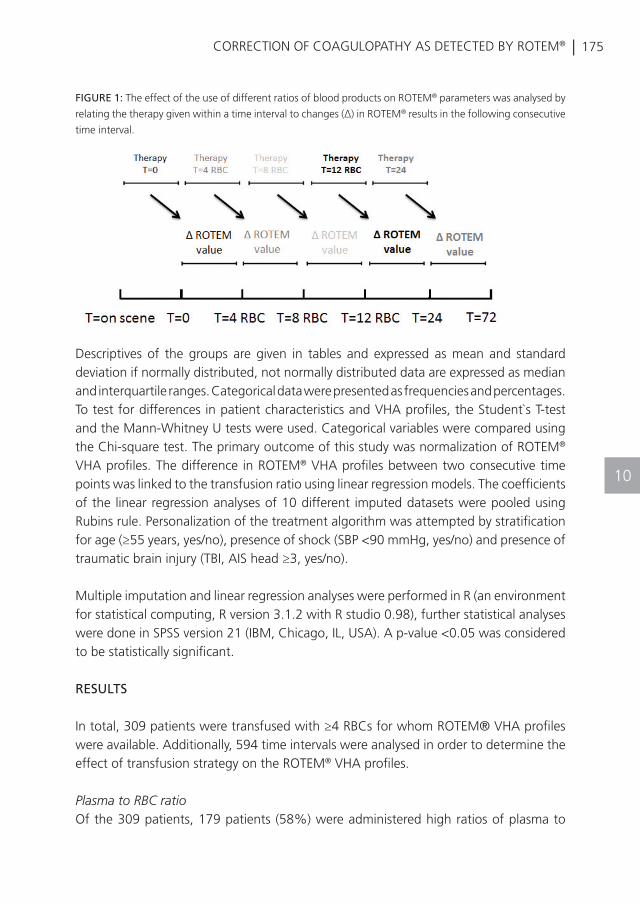
| 175CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
Descriptives of the groups are given in tables and expressed as mean and standard deviation if normally distributed, not normally distributed data are expressed as median and interquartile ranges. Categorical data were presented as frequencies and percentages. To test for differences in patient characteristics and VHA profiles, the Student`s T-test and the Mann-Whitney U tests were used. Categorical variables were compared using the Chi-square test. The primary outcome of this study was normalization of ROTEM® VHA profiles. The difference in ROTEM® VHA profiles between two consecutive time points was linked to the transfusion ratio using linear regression models. The coefficients of the linear regression analyses of 10 different imputed datasets were pooled using Rubins rule. Personalization of the treatment algorithm was attempted by stratification for age (≥55 years, yes/no), presence of shock (SBP <90 mmHg, yes/no) and presence of traumatic brain injury (TBI, AIS head ≥3, yes/no).
Multiple imputation and linear regression analyses were performed in R (an environment for statistical computing, R version 3.1.2 with R studio 0.98), further statistical analyses were done in SPSS version 21 (IBM, Chicago, IL, USA). A p-value <0.05 was considered to be statistically significant.
RESULTS
In total, 309 patients were transfused with ≥4 RBCs for whom ROTEM® VHA profiles were available. Additionally, 594 time intervals were analysed in order to determine the effect of transfusion strategy on the ROTEM® VHA profiles.
Plasma to RBC ratioOf the 309 patients, 179 patients (58%) were administered high ratios of plasma to
FIGURE 1: The effect of the use of different ratios of blood products on ROTEM® parameters was analysed by
relating the therapy given within a time interval to changes (Δ) in ROTEM® results in the following consecutive
time interval.
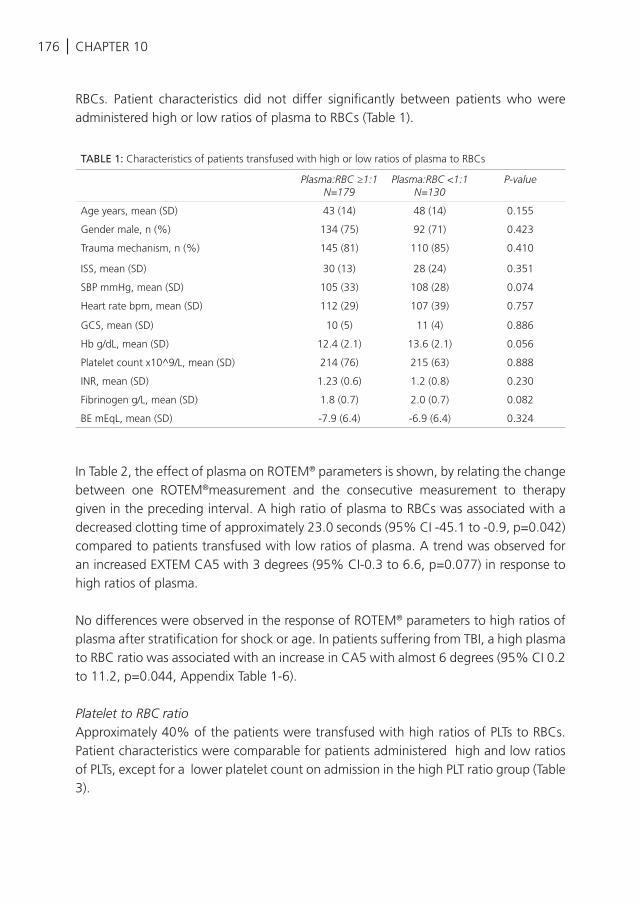
176 | CHAPTER 10
RBCs. Patient characteristics did not differ significantly between patients who were administered high or low ratios of plasma to RBCs (Table 1).
In Table 2, the effect of plasma on ROTEM® parameters is shown, by relating the change between one ROTEM®measurement and the consecutive measurement to therapy given in the preceding interval. A high ratio of plasma to RBCs was associated with a decreased clotting time of approximately 23.0 seconds (95% CI -45.1 to -0.9, p=0.042) compared to patients transfused with low ratios of plasma. A trend was observed for an increased EXTEM CA5 with 3 degrees (95% CI-0.3 to 6.6, p=0.077) in response to high ratios of plasma.
No differences were observed in the response of ROTEM® parameters to high ratios of plasma after stratification for shock or age. In patients suffering from TBI, a high plasma to RBC ratio was associated with an increase in CA5 with almost 6 degrees (95% CI 0.2 to 11.2, p=0.044, Appendix Table 1-6).
Platelet to RBC ratioApproximately 40% of the patients were transfused with high ratios of PLTs to RBCs. Patient characteristics were comparable for patients administered high and low ratios of PLTs, except for a lower platelet count on admission in the high PLT ratio group (Table 3).
TABLE 1: Characteristics of patients transfused with high or low ratios of plasma to RBCs
Plasma:RBC ≥1:1N=179
Plasma:RBC <1:1N=130
P-value
Age years, mean (SD) 43 (14) 48 (14) 0.155
Gender male, n (%) 134 (75) 92 (71) 0.423
Trauma mechanism, n (%) 145 (81) 110 (85) 0.410
ISS, mean (SD) 30 (13) 28 (24) 0.351
SBP mmHg, mean (SD) 105 (33) 108 (28) 0.074
Heart rate bpm, mean (SD) 112 (29) 107 (39) 0.757
GCS, mean (SD) 10 (5) 11 (4) 0.886
Hb g/dL, mean (SD) 12.4 (2.1) 13.6 (2.1) 0.056
Platelet count x10^9/L, mean (SD) 214 (76) 215 (63) 0.888
INR, mean (SD) 1.23 (0.6) 1.2 (0.8) 0.230
Fibrinogen g/L, mean (SD) 1.8 (0.7) 2.0 (0.7) 0.082
BE mEqL, mean (SD) -7.9 (6.4) -6.9 (6.4) 0.324
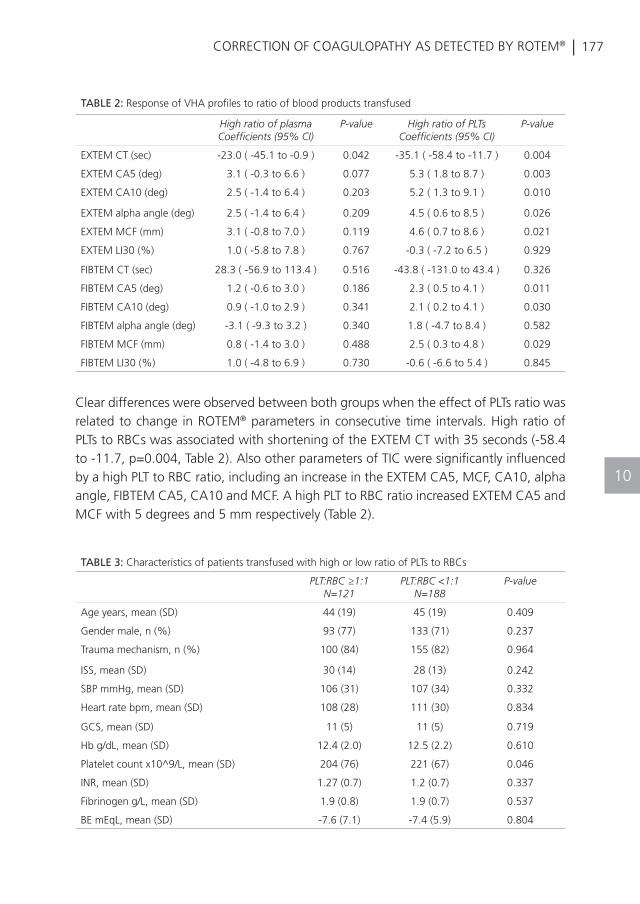
| 177CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
Clear differences were observed between both groups when the effect of PLTs ratio was related to change in ROTEM® parameters in consecutive time intervals. High ratio of PLTs to RBCs was associated with shortening of the EXTEM CT with 35 seconds (-58.4 to -11.7, p=0.004, Table 2). Also other parameters of TIC were significantly influenced by a high PLT to RBC ratio, including an increase in the EXTEM CA5, MCF, CA10, alpha angle, FIBTEM CA5, CA10 and MCF. A high PLT to RBC ratio increased EXTEM CA5 and MCF with 5 degrees and 5 mm respectively (Table 2).
TABLE 2: Response of VHA profiles to ratio of blood products transfused
High ratio of plasma Coefficients (95% CI)
P-value High ratio of PLTs Coefficients (95% CI)
P-value
EXTEM CT (sec) -23.0 ( -45.1 to -0.9 ) 0.042 -35.1 ( -58.4 to -11.7 ) 0.004
EXTEM CA5 (deg) 3.1 ( -0.3 to 6.6 ) 0.077 5.3 ( 1.8 to 8.7 ) 0.003
EXTEM CA10 (deg) 2.5 ( -1.4 to 6.4 ) 0.203 5.2 ( 1.3 to 9.1 ) 0.010
EXTEM alpha angle (deg) 2.5 ( -1.4 to 6.4 ) 0.209 4.5 ( 0.6 to 8.5 ) 0.026
EXTEM MCF (mm) 3.1 ( -0.8 to 7.0 ) 0.119 4.6 ( 0.7 to 8.6 ) 0.021
EXTEM LI30 (%) 1.0 ( -5.8 to 7.8 ) 0.767 -0.3 ( -7.2 to 6.5 ) 0.929
FIBTEM CT (sec) 28.3 ( -56.9 to 113.4 ) 0.516 -43.8 ( -131.0 to 43.4 ) 0.326
FIBTEM CA5 (deg) 1.2 ( -0.6 to 3.0 ) 0.186 2.3 ( 0.5 to 4.1 ) 0.011
FIBTEM CA10 (deg) 0.9 ( -1.0 to 2.9 ) 0.341 2.1 ( 0.2 to 4.1 ) 0.030
FIBTEM alpha angle (deg) -3.1 ( -9.3 to 3.2 ) 0.340 1.8 ( -4.7 to 8.4 ) 0.582
FIBTEM MCF (mm) 0.8 ( -1.4 to 3.0 ) 0.488 2.5 ( 0.3 to 4.8 ) 0.029
FIBTEM LI30 (%) 1.0 ( -4.8 to 6.9 ) 0.730 -0.6 ( -6.6 to 5.4 ) 0.845
TABLE 3: Characteristics of patients transfused with high or low ratio of PLTs to RBCs PLT:RBC ≥1:1
N=121PLT:RBC <1:1
N=188P-value
Age years, mean (SD) 44 (19) 45 (19) 0.409
Gender male, n (%) 93 (77) 133 (71) 0.237
Trauma mechanism, n (%) 100 (84) 155 (82) 0.964
ISS, mean (SD) 30 (14) 28 (13) 0.242
SBP mmHg, mean (SD) 106 (31) 107 (34) 0.332
Heart rate bpm, mean (SD) 108 (28) 111 (30) 0.834
GCS, mean (SD) 11 (5) 11 (5) 0.719
Hb g/dL, mean (SD) 12.4 (2.0) 12.5 (2.2) 0.610
Platelet count x10^9/L, mean (SD) 204 (76) 221 (67) 0.046
INR, mean (SD) 1.27 (0.7) 1.2 (0.7) 0.337
Fibrinogen g/L, mean (SD) 1.9 (0.8) 1.9 (0.7) 0.537
BE mEqL, mean (SD) -7.6 (7.1) -7.4 (5.9) 0.804
178 | CHAPTER 10
In response to a high PLT to RBC ratio, patients without shock showed a more profound correction of ROTEM® parameters than patients in shock. An improvement of EXTEM CT, CA5, CA10, alpha angle, MCF and FIBTEM CA5, CA10 and MCF was observed in patients without shock.
In both older and younger patients, the clotting time decreased in response to high ratios of PLTs to RBCs. However, the effect was more evident in older patients, as the EXTEM CT decreased with 80 seconds (95% CI -149.9 to -10.8) in patients transfused with high PLT to RBC ratios, whereas the decrease in clotting time was 24 seconds (95% CI-43.9 to -4.6) in younger patients. A high PLT to RBC ratio was also more effective in improving clot firmness in younger patients.
The response of ROTEM® parameters to a high PLT to RBC ratio was significantly different between TBI and non-TBI patients. In TBI patients, a high ratio of PLTs was associated with improved ROTEM® parameters, expressed by an increase in EXTEM CA5, CA10 and shortening of EXTEM CT, whereas no significant effect was observed in patients without TBI (Appendix Table 1-6, Figure 2).
Tranexamic acidTXA was not registered in 19 patients. Of the remaining 290 patients, 112 patients (39%) received TXA. Patients receiving TXA were significantly more severely injured, coagulopathic, had a higher incidence of shock and suffered more often from penetrating injury. Thereby, these groups were not balanced (Table 4).
In consecutive time intervals, TXA was associated with marked changes in ROTEM® parameters including an increased FIBTEM CA5, CA10, alpha angle and MCF (Table 5). Additionally, TXA was associated with a more profound inhibition of fibrinolysis as indicated by a reduced EXTEM Li30.
In response to TXA, patients with shock showed a reduced fibrinolysis and an improved fibrin clot formation in comparison to patients without shock (Figure 2). Fibrin clot formation was more pronounced in younger patients and patients without TBI than in older or TBI patients. However, TXA reduced fibrinolysis significantly more effective in patients with TBI compared to patients without TBI (Appendix Table 7-12, Table 2).
Fibrinogen productsOf the 309 patients, 119 patients (39%) received fibrinogen products. Patients administered fibrinogen products were more hypo-coagulopathic, severely injured and acidotic and suffered more often from TBI (Table 6).
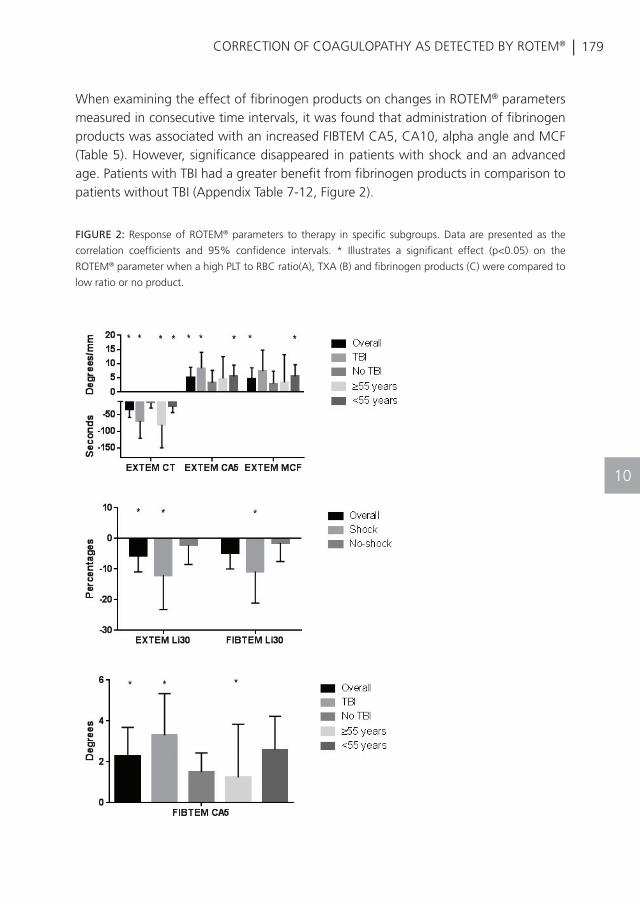
| 179CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
When examining the effect of fibrinogen products on changes in ROTEM® parameters measured in consecutive time intervals, it was found that administration of fibrinogen products was associated with an increased FIBTEM CA5, CA10, alpha angle and MCF (Table 5). However, significance disappeared in patients with shock and an advanced age. Patients with TBI had a greater benefit from fibrinogen products in comparison to patients without TBI (Appendix Table 7-12, Figure 2).
FIGURE 2: Response of ROTEM® parameters to therapy in specific subgroups. Data are presented as the
correlation coefficients and 95% confidence intervals. * Illustrates a significant effect (p<0.05) on the
ROTEM® parameter when a high PLT to RBC ratio(A), TXA (B) and fibrinogen products (C) were compared to
low ratio or no product.
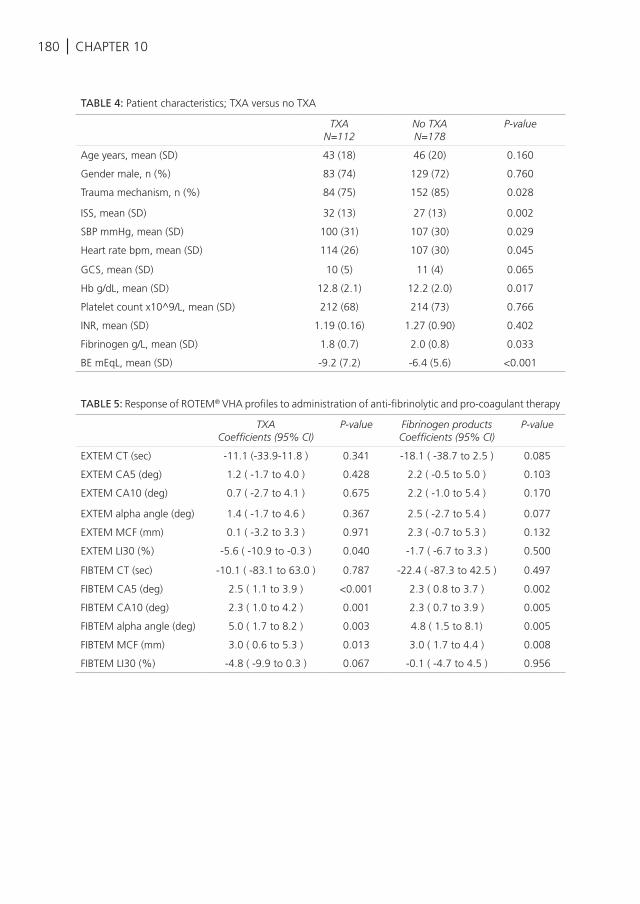
180 | CHAPTER 10
TABLE 4: Patient characteristics; TXA versus no TXA
TXAN=112
No TXAN=178
P-value
Age years, mean (SD) 43 (18) 46 (20) 0.160
Gender male, n (%) 83 (74) 129 (72) 0.760
Trauma mechanism, n (%) 84 (75) 152 (85) 0.028
ISS, mean (SD) 32 (13) 27 (13) 0.002
SBP mmHg, mean (SD) 100 (31) 107 (30) 0.029
Heart rate bpm, mean (SD) 114 (26) 107 (30) 0.045
GCS, mean (SD) 10 (5) 11 (4) 0.065
Hb g/dL, mean (SD) 12.8 (2.1) 12.2 (2.0) 0.017
Platelet count x10^9/L, mean (SD) 212 (68) 214 (73) 0.766
INR, mean (SD) 1.19 (0.16) 1.27 (0.90) 0.402
Fibrinogen g/L, mean (SD) 1.8 (0.7) 2.0 (0.8) 0.033
BE mEqL, mean (SD) -9.2 (7.2) -6.4 (5.6) <0.001
TABLE 5: Response of ROTEM® VHA profiles to administration of anti-fibrinolytic and pro-coagulant therapy
TXACoefficients (95% CI)
P-value Fibrinogen productsCoefficients (95% CI)
P-value
EXTEM CT (sec) -11.1 (-33.9-11.8 ) 0.341 -18.1 ( -38.7 to 2.5 ) 0.085
EXTEM CA5 (deg) 1.2 ( -1.7 to 4.0 ) 0.428 2.2 ( -0.5 to 5.0 ) 0.103
EXTEM CA10 (deg) 0.7 ( -2.7 to 4.1 ) 0.675 2.2 ( -1.0 to 5.4 ) 0.170
EXTEM alpha angle (deg) 1.4 ( -1.7 to 4.6 ) 0.367 2.5 ( -2.7 to 5.4 ) 0.077
EXTEM MCF (mm) 0.1 ( -3.2 to 3.3 ) 0.971 2.3 ( -0.7 to 5.3 ) 0.132
EXTEM LI30 (%) -5.6 ( -10.9 to -0.3 ) 0.040 -1.7 ( -6.7 to 3.3 ) 0.500
FIBTEM CT (sec) -10.1 ( -83.1 to 63.0 ) 0.787 -22.4 ( -87.3 to 42.5 ) 0.497
FIBTEM CA5 (deg) 2.5 ( 1.1 to 3.9 ) <0.001 2.3 ( 0.8 to 3.7 ) 0.002
FIBTEM CA10 (deg) 2.3 ( 1.0 to 4.2 ) 0.001 2.3 ( 0.7 to 3.9 ) 0.005
FIBTEM alpha angle (deg) 5.0 ( 1.7 to 8.2 ) 0.003 4.8 ( 1.5 to 8.1) 0.005
FIBTEM MCF (mm) 3.0 ( 0.6 to 5.3 ) 0.013 3.0 ( 1.7 to 4.4 ) 0.008
FIBTEM LI30 (%) -4.8 ( -9.9 to 0.3 ) 0.067 -0.1 ( -4.7 to 4.5 ) 0.956
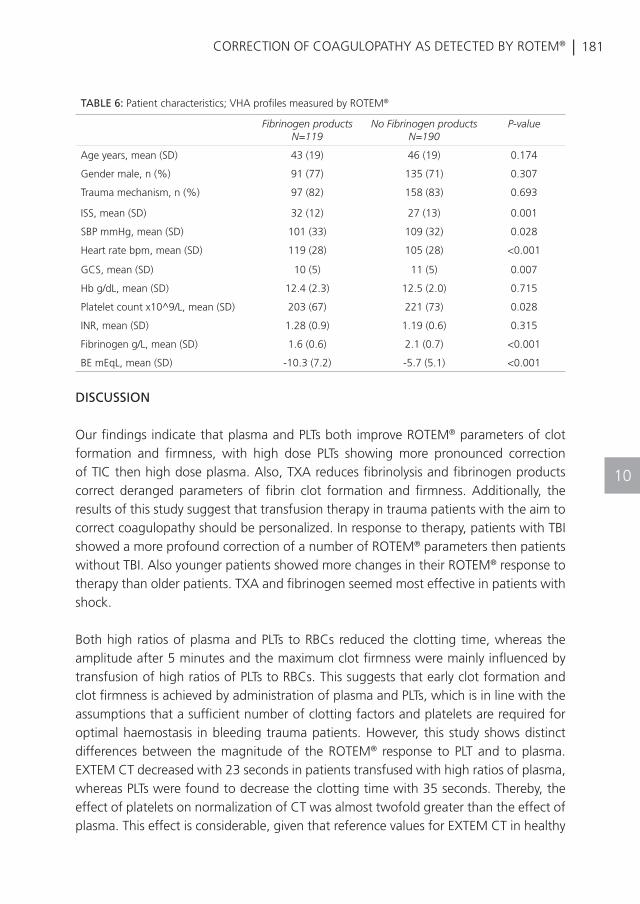
| 181CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
DISCUSSION
Our findings indicate that plasma and PLTs both improve ROTEM® parameters of clot formation and firmness, with high dose PLTs showing more pronounced correction of TIC then high dose plasma. Also, TXA reduces fibrinolysis and fibrinogen products correct deranged parameters of fibrin clot formation and firmness. Additionally, the results of this study suggest that transfusion therapy in trauma patients with the aim to correct coagulopathy should be personalized. In response to therapy, patients with TBI showed a more profound correction of a number of ROTEM® parameters then patients without TBI. Also younger patients showed more changes in their ROTEM® response to therapy than older patients. TXA and fibrinogen seemed most effective in patients with shock.
Both high ratios of plasma and PLTs to RBCs reduced the clotting time, whereas the amplitude after 5 minutes and the maximum clot firmness were mainly influenced by transfusion of high ratios of PLTs to RBCs. This suggests that early clot formation and clot firmness is achieved by administration of plasma and PLTs, which is in line with the assumptions that a sufficient number of clotting factors and platelets are required for optimal haemostasis in bleeding trauma patients. However, this study shows distinct differences between the magnitude of the ROTEM® response to PLT and to plasma. EXTEM CT decreased with 23 seconds in patients transfused with high ratios of plasma, whereas PLTs were found to decrease the clotting time with 35 seconds. Thereby, the effect of platelets on normalization of CT was almost twofold greater than the effect of plasma. This effect is considerable, given that reference values for EXTEM CT in healthy
TABLE 6: Patient characteristics; VHA profiles measured by ROTEM®
Fibrinogen productsN=119
No Fibrinogen productsN=190
P-value
Age years, mean (SD) 43 (19) 46 (19) 0.174
Gender male, n (%) 91 (77) 135 (71) 0.307
Trauma mechanism, n (%) 97 (82) 158 (83) 0.693
ISS, mean (SD) 32 (12) 27 (13) 0.001
SBP mmHg, mean (SD) 101 (33) 109 (32) 0.028
Heart rate bpm, mean (SD) 119 (28) 105 (28) <0.001
GCS, mean (SD) 10 (5) 11 (5) 0.007
Hb g/dL, mean (SD) 12.4 (2.3) 12.5 (2.0) 0.715
Platelet count x10^9/L, mean (SD) 203 (67) 221 (73) 0.028
INR, mean (SD) 1.28 (0.9) 1.19 (0.6) 0.315
Fibrinogen g/L, mean (SD) 1.6 (0.6) 2.1 (0.7) <0.001
BE mEqL, mean (SD) -10.3 (7.2) -5.7 (5.1) <0.001
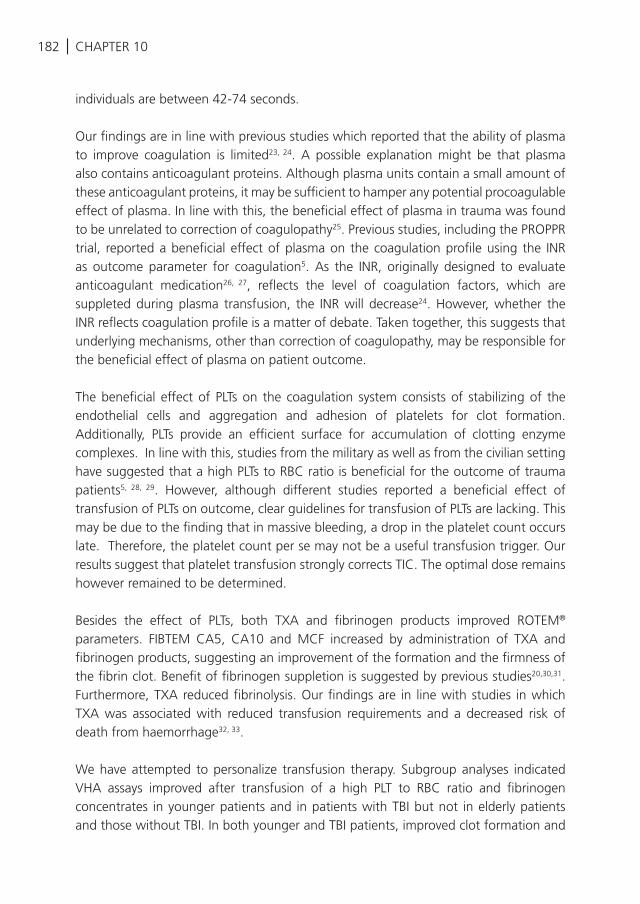
182 | CHAPTER 10
individuals are between 42-74 seconds.
Our findings are in line with previous studies which reported that the ability of plasma to improve coagulation is limited23, 24. A possible explanation might be that plasma also contains anticoagulant proteins. Although plasma units contain a small amount of these anticoagulant proteins, it may be sufficient to hamper any potential procoagulable effect of plasma. In line with this, the beneficial effect of plasma in trauma was found to be unrelated to correction of coagulopathy25. Previous studies, including the PROPPR trial, reported a beneficial effect of plasma on the coagulation profile using the INR as outcome parameter for coagulation5. As the INR, originally designed to evaluate anticoagulant medication26, 27, reflects the level of coagulation factors, which are suppleted during plasma transfusion, the INR will decrease24. However, whether the INR reflects coagulation profile is a matter of debate. Taken together, this suggests that underlying mechanisms, other than correction of coagulopathy, may be responsible for the beneficial effect of plasma on patient outcome.
The beneficial effect of PLTs on the coagulation system consists of stabilizing of the endothelial cells and aggregation and adhesion of platelets for clot formation. Additionally, PLTs provide an efficient surface for accumulation of clotting enzyme complexes. In line with this, studies from the military as well as from the civilian setting have suggested that a high PLTs to RBC ratio is beneficial for the outcome of trauma patients5, 28, 29. However, although different studies reported a beneficial effect of transfusion of PLTs on outcome, clear guidelines for transfusion of PLTs are lacking. This may be due to the finding that in massive bleeding, a drop in the platelet count occurs late. Therefore, the platelet count per se may not be a useful transfusion trigger. Our results suggest that platelet transfusion strongly corrects TIC. The optimal dose remains however remained to be determined.
Besides the effect of PLTs, both TXA and fibrinogen products improved ROTEM®
parameters. FIBTEM CA5, CA10 and MCF increased by administration of TXA and fibrinogen products, suggesting an improvement of the formation and the firmness of the fibrin clot. Benefit of fibrinogen suppletion is suggested by previous studies20,30,31. Furthermore, TXA reduced fibrinolysis. Our findings are in line with studies in which TXA was associated with reduced transfusion requirements and a decreased risk of death from haemorrhage32, 33.
We have attempted to personalize transfusion therapy. Subgroup analyses indicated VHA assays improved after transfusion of a high PLT to RBC ratio and fibrinogen concentrates in younger patients and in patients with TBI but not in elderly patients and those without TBI. In both younger and TBI patients, improved clot formation and
| 183CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
clot firmness was observed after transfusion of a high PLT to RBC ratio. Furthermore in these groups, a more pronounced improvement of the fibrin clot formation was seen after administration of fibrinogen products. Additionally, TXA seemed more beneficial in patients with shock than in patients without shock. Taken together, these findings suggest that the response of VHA profiles to transfusion differs between patient populations. Thereby, a personalized transfusion therapy may improve outcome after trauma, while minimizing transfusion in those subjects who do not need it to correct TIC. Our data suggest that transfusion with higher amounts of PLTs and fibrinogen products may be recommended in TBI and younger patients, whereas a higher dose of TXA may improve TIC in patients with shock. However, whether differential transfusion strategies guided by ROTEM® improve outcome in specific patient populations needs to be further studied.
Limitations to this study should be acknowledged. Initial ROTEM® measurements were missing in 10% of the patients transfused with ≥4 RBCs, for which multiple imputation was performed, which may cause bias. However, imputation may cause less bias then not accounting for missing values. Another important limitation is that we were not able to report on optimal dosing of anti-fibrinolytic or pro-coagulant agents. This remains an area which needs to be explored. Also, adjustment for confounders was not done in the model. However, no baseline differences in patient characteristics were found between the plasma and PLTs groups which may have affected outcome. Differences in patient characteristics were observed between patients receiving TXA or fibrinogen products and those who did not, with more significant injury in patients receiving therapy. However, although these patients were more severely injured, a beneficial effect of TXA on TIC was observed in patients with shock. Additionally, to overcome the limitation of no adjustment for confounders, stratifications for age, shock and TBI was performed, although subgroups were small. Furthermore, the sample size of 309 patients appears small. However, this is the largest prospective observational study to date in which the effect of therapy on ROTEM® profiles was investigated.
CONCLUSION
Administration of a high ratio of PLTs to RBCs has a more profound effect on improving clot formation than high plasma to RBC ratio. Also, our data suggest that TBI and younger patients show a greater response to PLTs and fibrinogen in terms of correction of TIC when compared to other patient populations. Additionally, patients with shock benefit more from TXA than patients without shock. These results suggest that a personalized therapy may improve the coagulation profile and outcome of trauma patients. Results can be used to develop treatment algorithms which aim at improvement of TIC as assessed by ROTEM®.
184 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Brohi K, Singh J, Heron M, Coats T.
Acute traumatic coagulopathy. J Trauma.
2003;54(6):1127-30.
MacLeod JB, Lynn M, McKenney MG, Cohn
SM, Murtha M. Early coagulopathy predicts
mortality in trauma. J Trauma. 2003;55(1):39-
44.
Johansson PI, Oliveri RS, Ostrowski SR.
Hemostatic resuscitation with plasma and
platelets in trauma. J Emerg Trauma Shock.
2012;5(2):120-5.
Holcomb JB, del Junco DJ, Fox EE, Wade
CE, Cohen MJ, Schreiber MA, et al. The
prospective, observational, multicenter,
major trauma transfusion (PROMMTT) study:
comparative effectiveness of a time-varying
treatment with competing risks. JAMA Surg
2013;148(2):127-36.
Holcomb JB, Tilley BC, Baraniuk S, Fox EE,
Wade CE, Podbielski JM, et al. Transfusion
of plasma, platelets, and red blood cells in a
1:1:1 vs a 1:1:2 ratio and mortality in patients
with severe trauma: the PROPPR randomized
clinical trial. JAMA. 2015;313(5):471-82.
Juffermans NP, Vlaar AP, Prins DJ, Goslings
JC, Binnekade JM. The age of red blood
cells is associated with bacterial infections in
critically ill trauma patients. Blood transfusion
= Trasfusione del sangue. 2012;10(3):290-5.
Chaiwat O, Lang JD, Vavilala MS, Wang
J, MacKenzie EJ, Jurkovich GJ, et al. Early
packed red blood cell transfusion and acute
respiratory distress syndrome after trauma.
Anesthesiology. 2009;110(2):351-60.
Plurad D, Martin M, Green D, Salim A, Inaba
K, Belzberg H, et al. The decreasing incidence
of late posttraumatic acute respiratory distress
syndrome: the potential role of lung protective
ventilation and conservative transfusion
practice. J Trauma. 2007;63(1):1-7; discussion
8.
Ciesla DJ, Moore EE, Johnson JL, Burch
JM, Cothren CC, Sauaia A. A 12-year
prospective study of postinjury multiple organ
failure: has anything changed? Arch Surg
2005;140(5):432-8.
Johnson JL, Moore EE, Kashuk JL, Banerjee A,
Cothren CC, Biffl WL, et al. Effect of blood
products transfusion on the development of
postinjury multiple organ failure. Arch Surg
2010;145(10):973-7.
Moore FA, Moore EE, Sauaia A. Blood
transfusion. An independent risk factor for
postinjury multiple organ failure. Arch Surg
1997;132(6):620-4.
Sauaia A, Moore FA, Moore EE, Haenel JB,
Read RA, Lezotte DC. Early predictors of
postinjury multiple organ failure. Arch Surg
1994;129(1):39-45.
Holcomb JB, Minei KM, Scerbo ML, Radwan
ZA, Wade CE, Kozar RA, et al. Admission
rapid thrombelastography can replace
conventional coagulation tests in the
emergency department: experience with
1974 consecutive trauma patients. Annals of
surgery. 2012;256(3):476-86.
Dzik WH. Predicting hemorrhage using
preoperative coagulation screening assays.
Current hematology reports. 2004;3(5):324-
30.
Park MS, Martini WZ, Dubick MA,
Salinas J, Butenas S, Kheirabadi BS, et
al. Thromboelastography as a better
indicator of hypercoagulable state after
injury than prothrombin time or activated
partial thromboplastin time. J Trauma.
2009;67(2):266-75; discussion 75-6.
Davenport R, Manson J, De’Ath H, Platton
S, Coates A, Allard S, et al. Functional
definition and characterization of acute
traumatic coagulopathy. Crit Care Med
2011;39(12):2652-8.
Woolley T, Midwinter M, Spencer P, Watts
S, Doran C, Kirkman E. Utility of interim
ROTEM((R)) values of clot strength, A5
and A10, in predicting final assessment of
coagulation status in severely injured battle
patients. Injury. 2013;44(5):593-9.
CHAPTER 10
| 185
REFERENCES
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
Rugeri L, Levrat A, David JS, Delecroix E,
Floccard B, Gros A, et al. Diagnosis of early
coagulation abnormalities in trauma patients
by rotation thrombelastography. Journal
of thrombosis and haemostasis : JTH.
2007;5(2):289-95.
Johansson PI, Stensballe J. Effect of Haemostatic
Control Resuscitation on mortality in massively
bleeding patients: a before and after study.
Vox Sang 2009;96(2):111-8.
Schochl H, Nienaber U, Hofer G, Voelckel
W, Jambor C, Scharbert G, et al. Goal-
directed coagulation management of major
trauma patients using thromboelastometry
(ROTEM)-guided administration of fibrinogen
concentrate and prothrombin complex
concentrate. Crit Care. 2010;14(2):R55.
Schochl H, Nienaber U, Maegele M,
Hochleitner G, Primavesi F, Steitz B, et al.
Transfusion in trauma: thromboelastometry-
guided coagulation factor concentrate-based
therapy versus standard fresh frozen plasma-
based therapy. Crit Care. 2011;15(2):R83.
Tapia NM, Chang A, Norman M, Welsh F, Scott
B, Wall MJ, Jr., et al. TEG-guided resuscitation
is superior to standardized MTP resuscitation
in massively transfused penetrating trauma
patients. J Trauma Acute Care Surg.
2013;74(2):378-85; discussion 85-6.
Hyytiainen S, Syrjala M, Fellman V, Heikinheimo
M, Petaja J. Fresh frozen plasma reduces
thrombin formation in newborn infants.
Journal of thrombosis and haemostasis : JTH.
2003;1(6):1189-94.
Muller MC, Straat M, Meijers JC, Klinkspoor
JH, de Jonge E, Arbous MS, et al. Fresh frozen
plasma transfusion fails to influence the
hemostatic balance in critically ill patients with
a coagulopathy. Journal of thrombosis and
haemostasis : JTH. 2015;13(6):989-97.
Khan S, Davenport R, Raza I, Glasgow S,
De’Ath HD, Johansson PI, et al. Damage
control resuscitation using blood component
therapy in standard doses has a limited effect
on coagulopathy during trauma hemorrhage.
Intensive Care Med 2015;41(2):239-47.
McCully SP, Fabricant LJ, Kunio NR, Groat
TL, Watson KM, Differding JA, et al. The
International Normalized Ratio overestimates
coagulopathy in stable trauma and surgical
patients. J Trauma Acute Care Surg.
2013;75(6):947-53.
Mitra B, O’Reilly G, Collecutt M, Cameron
PA, Phillips L, Davis A. Prospective
comparison of point-of-care international
normalised ratio measurement versus plasma
international normalised ratio for acute
traumatic coagulopathy. Emergency medicine
Australasia : EMA. 2012;24(4):363-8.
Holcomb JB, Zarzabal LA, Michalek JE, Kozar
RA, Spinella PC, Perkins JG, et al. Increased
platelet:RBC ratios are associated with
improved survival after massive transfusion. J
Trauma. 2011;71(2 Suppl 3):S318-28.
Perkins JG, Cap AP, Spinella PC, Blackbourne
LH, Grathwohl KW, Repine TB, et al. An
evaluation of the impact of apheresis platelets
used in the setting of massively transfused
trauma patients. J Trauma. 2009;66(4
Suppl):S77-84; discussion S-5.
Schochl H, Forster L, Woidke R,
Solomon C, Voelckel W. Use of rotation
thromboelastometry (ROTEM) to achieve
successful treatment of polytrauma with
fibrinogen concentrate and prothrombin
complex concentrate. Anaesthesia.
2010;65(2):199-203.
Fries D. The early use of fibrinogen,
prothrombin complex concentrate, and
recombinant-activated factor VIIa in massive
bleeding. Transfusion. 2013;53 Suppl 1:91s-
5s.
Shakur H, Roberts I, Bautista R, Caballero J,
Coats T, Dewan Y, et al. Effects of tranexamic
acid on death, vascular occlusive events,
and blood transfusion in trauma patients
with significant haemorrhage (CRASH-2): a
randomised, placebo-controlled trial. Lancet.
CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
186 |
REFERENCES
33
2010;376(9734):23-32.
Morrison JJ, Dubose JJ, Rasmussen TE,
Midwinter MJ. Military Application of
Tranexamic Acid in Trauma Emergency
Resuscitation (MATTERs) Study. Arch Surg
2012;147(2):113-9.
CHAPTER 10

| 187CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
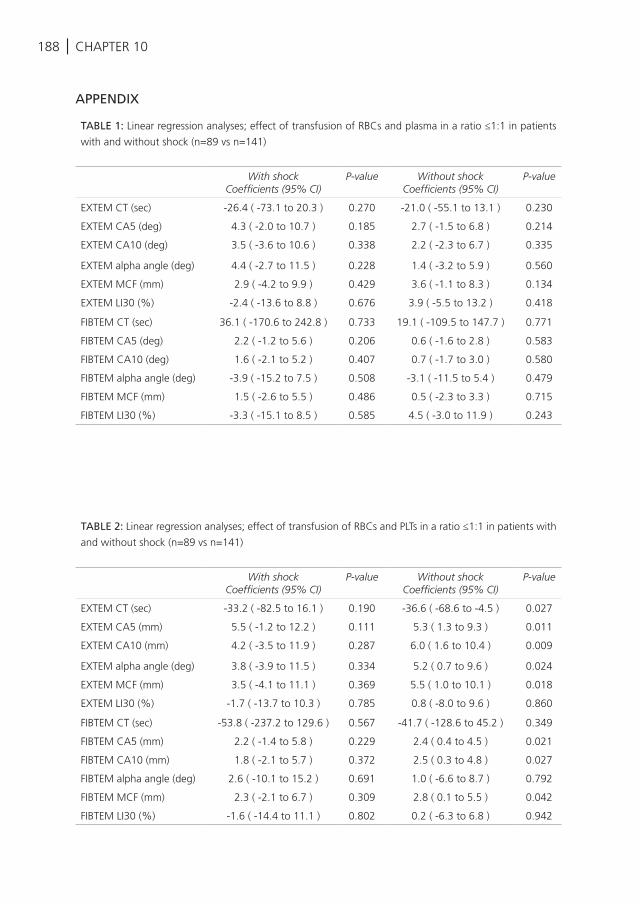
188 | CHAPTER 10
APPENDIX
TABLE 1: Linear regression analyses; effect of transfusion of RBCs and plasma in a ratio ≤1:1 in patients
with and without shock (n=89 vs n=141)
With shockCoefficients (95% CI)
P-value Without shockCoefficients (95% CI)
P-value
EXTEM CT (sec) -26.4 ( -73.1 to 20.3 ) 0.270 -21.0 ( -55.1 to 13.1 ) 0.230
EXTEM CA5 (deg) 4.3 ( -2.0 to 10.7 ) 0.185 2.7 ( -1.5 to 6.8 ) 0.214
EXTEM CA10 (deg) 3.5 ( -3.6 to 10.6 ) 0.338 2.2 ( -2.3 to 6.7 ) 0.335
EXTEM alpha angle (deg) 4.4 ( -2.7 to 11.5 ) 0.228 1.4 ( -3.2 to 5.9 ) 0.560
EXTEM MCF (mm) 2.9 ( -4.2 to 9.9 ) 0.429 3.6 ( -1.1 to 8.3 ) 0.134
EXTEM LI30 (%) -2.4 ( -13.6 to 8.8 ) 0.676 3.9 ( -5.5 to 13.2 ) 0.418
FIBTEM CT (sec) 36.1 ( -170.6 to 242.8 ) 0.733 19.1 ( -109.5 to 147.7 ) 0.771
FIBTEM CA5 (deg) 2.2 ( -1.2 to 5.6 ) 0.206 0.6 ( -1.6 to 2.8 ) 0.583
FIBTEM CA10 (deg) 1.6 ( -2.1 to 5.2 ) 0.407 0.7 ( -1.7 to 3.0 ) 0.580
FIBTEM alpha angle (deg) -3.9 ( -15.2 to 7.5 ) 0.508 -3.1 ( -11.5 to 5.4 ) 0.479
FIBTEM MCF (mm) 1.5 ( -2.6 to 5.5 ) 0.486 0.5 ( -2.3 to 3.3 ) 0.715
FIBTEM LI30 (%) -3.3 ( -15.1 to 8.5 ) 0.585 4.5 ( -3.0 to 11.9 ) 0.243
TABLE 2: Linear regression analyses; effect of transfusion of RBCs and PLTs in a ratio ≤1:1 in patients with
and without shock (n=89 vs n=141)
With shockCoefficients (95% CI)
P-value Without shockCoefficients (95% CI)
P-value
EXTEM CT (sec) -33.2 ( -82.5 to 16.1 ) 0.190 -36.6 ( -68.6 to -4.5 ) 0.027
EXTEM CA5 (mm) 5.5 ( -1.2 to 12.2 ) 0.111 5.3 ( 1.3 to 9.3 ) 0.011
EXTEM CA10 (mm) 4.2 ( -3.5 to 11.9 ) 0.287 6.0 ( 1.6 to 10.4 ) 0.009
EXTEM alpha angle (deg) 3.8 ( -3.9 to 11.5 ) 0.334 5.2 ( 0.7 to 9.6 ) 0.024
EXTEM MCF (mm) 3.5 ( -4.1 to 11.1 ) 0.369 5.5 ( 1.0 to 10.1 ) 0.018
EXTEM LI30 (%) -1.7 ( -13.7 to 10.3 ) 0.785 0.8 ( -8.0 to 9.6 ) 0.860
FIBTEM CT (sec) -53.8 ( -237.2 to 129.6 ) 0.567 -41.7 ( -128.6 to 45.2 ) 0.349
FIBTEM CA5 (mm) 2.2 ( -1.4 to 5.8 ) 0.229 2.4 ( 0.4 to 4.5 ) 0.021
FIBTEM CA10 (mm) 1.8 ( -2.1 to 5.7 ) 0.372 2.5 ( 0.3 to 4.8 ) 0.027
FIBTEM alpha angle (deg) 2.6 ( -10.1 to 15.2 ) 0.691 1.0 ( -6.6 to 8.7 ) 0.792
FIBTEM MCF (mm) 2.3 ( -2.1 to 6.7 ) 0.309 2.8 ( 0.1 to 5.5 ) 0.042
FIBTEM LI30 (%) -1.6 ( -14.4 to 11.1 ) 0.802 0.2 ( -6.3 to 6.8 ) 0.942
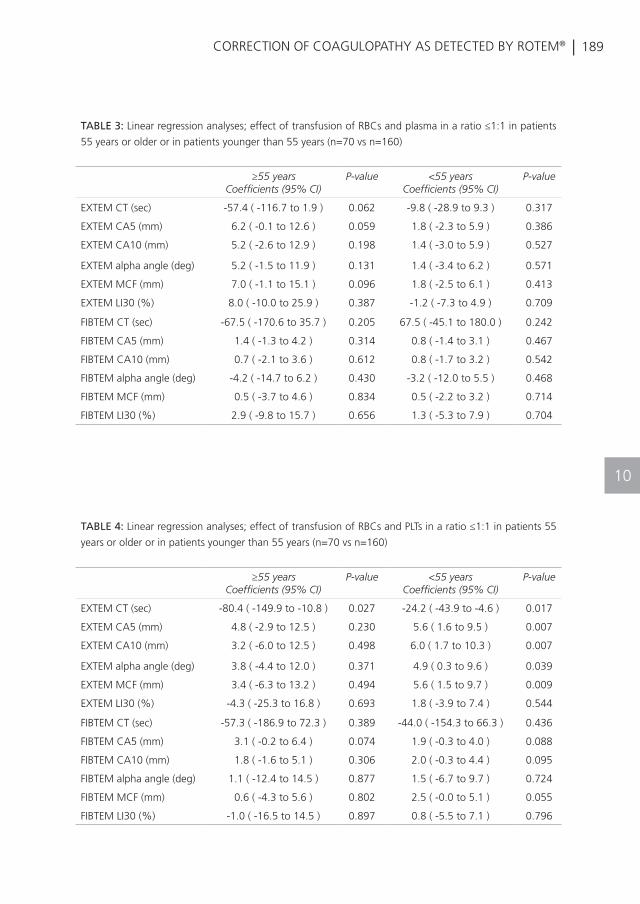
| 189CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
TABLE 3: Linear regression analyses; effect of transfusion of RBCs and plasma in a ratio ≤1:1 in patients
55 years or older or in patients younger than 55 years (n=70 vs n=160)
≥55 yearsCoefficients (95% CI)
P-value <55 yearsCoefficients (95% CI)
P-value
EXTEM CT (sec) -57.4 ( -116.7 to 1.9 ) 0.062 -9.8 ( -28.9 to 9.3 ) 0.317
EXTEM CA5 (mm) 6.2 ( -0.1 to 12.6 ) 0.059 1.8 ( -2.3 to 5.9 ) 0.386
EXTEM CA10 (mm) 5.2 ( -2.6 to 12.9 ) 0.198 1.4 ( -3.0 to 5.9 ) 0.527
EXTEM alpha angle (deg) 5.2 ( -1.5 to 11.9 ) 0.131 1.4 ( -3.4 to 6.2 ) 0.571
EXTEM MCF (mm) 7.0 ( -1.1 to 15.1 ) 0.096 1.8 ( -2.5 to 6.1 ) 0.413
EXTEM LI30 (%) 8.0 ( -10.0 to 25.9 ) 0.387 -1.2 ( -7.3 to 4.9 ) 0.709
FIBTEM CT (sec) -67.5 ( -170.6 to 35.7 ) 0.205 67.5 ( -45.1 to 180.0 ) 0.242
FIBTEM CA5 (mm) 1.4 ( -1.3 to 4.2 ) 0.314 0.8 ( -1.4 to 3.1 ) 0.467
FIBTEM CA10 (mm) 0.7 ( -2.1 to 3.6 ) 0.612 0.8 ( -1.7 to 3.2 ) 0.542
FIBTEM alpha angle (deg) -4.2 ( -14.7 to 6.2 ) 0.430 -3.2 ( -12.0 to 5.5 ) 0.468
FIBTEM MCF (mm) 0.5 ( -3.7 to 4.6 ) 0.834 0.5 ( -2.2 to 3.2 ) 0.714
FIBTEM LI30 (%) 2.9 ( -9.8 to 15.7 ) 0.656 1.3 ( -5.3 to 7.9 ) 0.704
TABLE 4: Linear regression analyses; effect of transfusion of RBCs and PLTs in a ratio ≤1:1 in patients 55
years or older or in patients younger than 55 years (n=70 vs n=160)
≥55 yearsCoefficients (95% CI)
P-value <55 yearsCoefficients (95% CI)
P-value
EXTEM CT (sec) -80.4 ( -149.9 to -10.8 ) 0.027 -24.2 ( -43.9 to -4.6 ) 0.017
EXTEM CA5 (mm) 4.8 ( -2.9 to 12.5 ) 0.230 5.6 ( 1.6 to 9.5 ) 0.007
EXTEM CA10 (mm) 3.2 ( -6.0 to 12.5 ) 0.498 6.0 ( 1.7 to 10.3 ) 0.007
EXTEM alpha angle (deg) 3.8 ( -4.4 to 12.0 ) 0.371 4.9 ( 0.3 to 9.6 ) 0.039
EXTEM MCF (mm) 3.4 ( -6.3 to 13.2 ) 0.494 5.6 ( 1.5 to 9.7 ) 0.009
EXTEM LI30 (%) -4.3 ( -25.3 to 16.8 ) 0.693 1.8 ( -3.9 to 7.4 ) 0.544
FIBTEM CT (sec) -57.3 ( -186.9 to 72.3 ) 0.389 -44.0 ( -154.3 to 66.3 ) 0.436
FIBTEM CA5 (mm) 3.1 ( -0.2 to 6.4 ) 0.074 1.9 ( -0.3 to 4.0 ) 0.088
FIBTEM CA10 (mm) 1.8 ( -1.6 to 5.1 ) 0.306 2.0 ( -0.3 to 4.4 ) 0.095
FIBTEM alpha angle (deg) 1.1 ( -12.4 to 14.5 ) 0.877 1.5 ( -6.7 to 9.7 ) 0.724
FIBTEM MCF (mm) 0.6 ( -4.3 to 5.6 ) 0.802 2.5 ( -0.0 to 5.1 ) 0.055
FIBTEM LI30 (%) -1.0 ( -16.5 to 14.5 ) 0.897 0.8 ( -5.5 to 7.1 ) 0.796
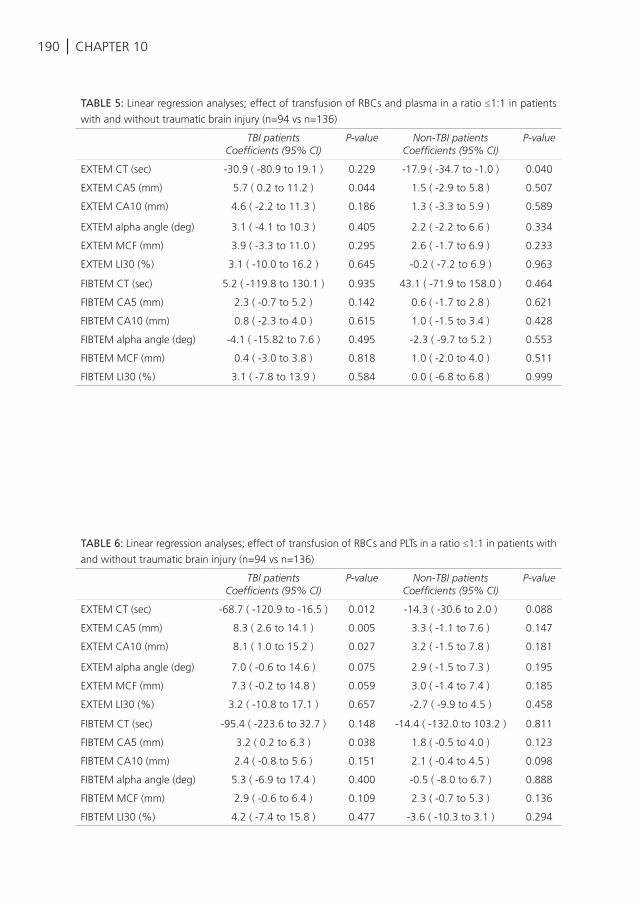
190 | CHAPTER 10
TABLE 5: Linear regression analyses; effect of transfusion of RBCs and plasma in a ratio ≤1:1 in patients
with and without traumatic brain injury (n=94 vs n=136)
TBI patientsCoefficients (95% CI)
P-value Non-TBI patientsCoefficients (95% CI)
P-value
EXTEM CT (sec) -30.9 ( -80.9 to 19.1 ) 0.229 -17.9 ( -34.7 to -1.0 ) 0.040
EXTEM CA5 (mm) 5.7 ( 0.2 to 11.2 ) 0.044 1.5 ( -2.9 to 5.8 ) 0.507
EXTEM CA10 (mm) 4.6 ( -2.2 to 11.3 ) 0.186 1.3 ( -3.3 to 5.9 ) 0.589
EXTEM alpha angle (deg) 3.1 ( -4.1 to 10.3 ) 0.405 2.2 ( -2.2 to 6.6 ) 0.334
EXTEM MCF (mm) 3.9 ( -3.3 to 11.0 ) 0.295 2.6 ( -1.7 to 6.9 ) 0.233
EXTEM LI30 (%) 3.1 ( -10.0 to 16.2 ) 0.645 -0.2 ( -7.2 to 6.9 ) 0.963
FIBTEM CT (sec) 5.2 ( -119.8 to 130.1 ) 0.935 43.1 ( -71.9 to 158.0 ) 0.464
FIBTEM CA5 (mm) 2.3 ( -0.7 to 5.2 ) 0.142 0.6 ( -1.7 to 2.8 ) 0.621
FIBTEM CA10 (mm) 0.8 ( -2.3 to 4.0 ) 0.615 1.0 ( -1.5 to 3.4 ) 0.428
FIBTEM alpha angle (deg) -4.1 ( -15.82 to 7.6 ) 0.495 -2.3 ( -9.7 to 5.2 ) 0.553
FIBTEM MCF (mm) 0.4 ( -3.0 to 3.8 ) 0.818 1.0 ( -2.0 to 4.0 ) 0.511
FIBTEM LI30 (%) 3.1 ( -7.8 to 13.9 ) 0.584 0.0 ( -6.8 to 6.8 ) 0.999
TABLE 6: Linear regression analyses; effect of transfusion of RBCs and PLTs in a ratio ≤1:1 in patients with
and without traumatic brain injury (n=94 vs n=136)
TBI patientsCoefficients (95% CI)
P-value Non-TBI patientsCoefficients (95% CI)
P-value
EXTEM CT (sec) -68.7 ( -120.9 to -16.5 ) 0.012 -14.3 ( -30.6 to 2.0 ) 0.088
EXTEM CA5 (mm) 8.3 ( 2.6 to 14.1 ) 0.005 3.3 ( -1.1 to 7.6 ) 0.147
EXTEM CA10 (mm) 8.1 ( 1.0 to 15.2 ) 0.027 3.2 ( -1.5 to 7.8 ) 0.181
EXTEM alpha angle (deg) 7.0 ( -0.6 to 14.6 ) 0.075 2.9 ( -1.5 to 7.3 ) 0.195
EXTEM MCF (mm) 7.3 ( -0.2 to 14.8 ) 0.059 3.0 ( -1.4 to 7.4 ) 0.185
EXTEM LI30 (%) 3.2 ( -10.8 to 17.1 ) 0.657 -2.7 ( -9.9 to 4.5 ) 0.458
FIBTEM CT (sec) -95.4 ( -223.6 to 32.7 ) 0.148 -14.4 ( -132.0 to 103.2 ) 0.811
FIBTEM CA5 (mm) 3.2 ( 0.2 to 6.3 ) 0.038 1.8 ( -0.5 to 4.0 ) 0.123
FIBTEM CA10 (mm) 2.4 ( -0.8 to 5.6 ) 0.151 2.1 ( -0.4 to 4.5 ) 0.098
FIBTEM alpha angle (deg) 5.3 ( -6.9 to 17.4 ) 0.400 -0.5 ( -8.0 to 6.7 ) 0.888
FIBTEM MCF (mm) 2.9 ( -0.6 to 6.4 ) 0.109 2.3 ( -0.7 to 5.3 ) 0.136
FIBTEM LI30 (%) 4.2 ( -7.4 to 15.8 ) 0.477 -3.6 ( -10.3 to 3.1 ) 0.294
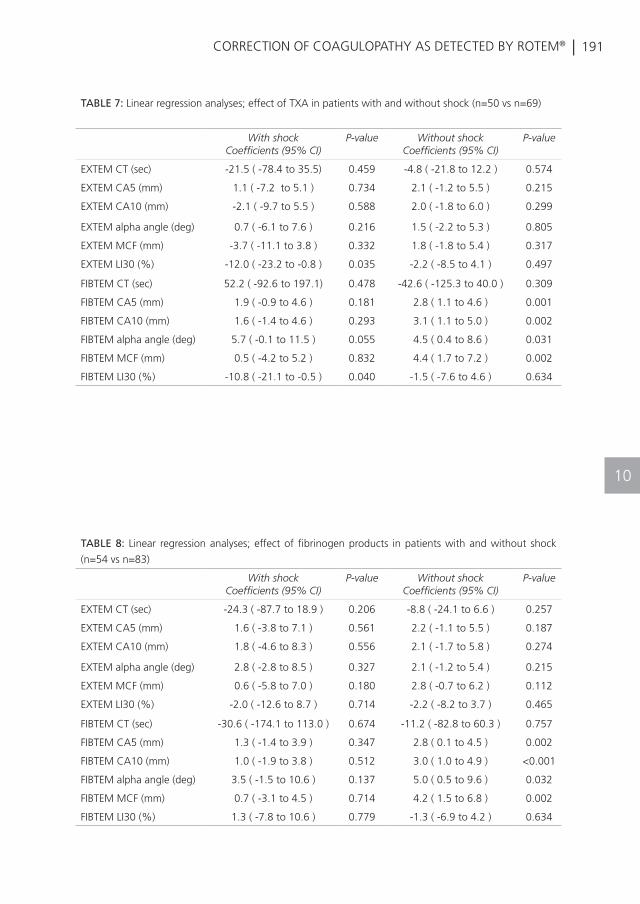
| 191CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
TABLE 7: Linear regression analyses; effect of TXA in patients with and without shock (n=50 vs n=69)
With shockCoefficients (95% CI)
P-value Without shockCoefficients (95% CI)
P-value
EXTEM CT (sec) -21.5 ( -78.4 to 35.5) 0.459 -4.8 ( -21.8 to 12.2 ) 0.574
EXTEM CA5 (mm) 1.1 ( -7.2 to 5.1 ) 0.734 2.1 ( -1.2 to 5.5 ) 0.215
EXTEM CA10 (mm) -2.1 ( -9.7 to 5.5 ) 0.588 2.0 ( -1.8 to 6.0 ) 0.299
EXTEM alpha angle (deg) 0.7 ( -6.1 to 7.6 ) 0.216 1.5 ( -2.2 to 5.3 ) 0.805
EXTEM MCF (mm) -3.7 ( -11.1 to 3.8 ) 0.332 1.8 ( -1.8 to 5.4 ) 0.317
EXTEM LI30 (%) -12.0 ( -23.2 to -0.8 ) 0.035 -2.2 ( -8.5 to 4.1 ) 0.497
FIBTEM CT (sec) 52.2 ( -92.6 to 197.1) 0.478 -42.6 ( -125.3 to 40.0 ) 0.309
FIBTEM CA5 (mm) 1.9 ( -0.9 to 4.6 ) 0.181 2.8 ( 1.1 to 4.6 ) 0.001
FIBTEM CA10 (mm) 1.6 ( -1.4 to 4.6 ) 0.293 3.1 ( 1.1 to 5.0 ) 0.002
FIBTEM alpha angle (deg) 5.7 ( -0.1 to 11.5 ) 0.055 4.5 ( 0.4 to 8.6 ) 0.031
FIBTEM MCF (mm) 0.5 ( -4.2 to 5.2 ) 0.832 4.4 ( 1.7 to 7.2 ) 0.002
FIBTEM LI30 (%) -10.8 ( -21.1 to -0.5 ) 0.040 -1.5 ( -7.6 to 4.6 ) 0.634
TABLE 8: Linear regression analyses; effect of fibrinogen products in patients with and without shock
(n=54 vs n=83)
With shockCoefficients (95% CI)
P-value Without shockCoefficients (95% CI)
P-value
EXTEM CT (sec) -24.3 ( -87.7 to 18.9 ) 0.206 -8.8 ( -24.1 to 6.6 ) 0.257
EXTEM CA5 (mm) 1.6 ( -3.8 to 7.1 ) 0.561 2.2 ( -1.1 to 5.5 ) 0.187
EXTEM CA10 (mm) 1.8 ( -4.6 to 8.3 ) 0.556 2.1 ( -1.7 to 5.8 ) 0.274
EXTEM alpha angle (deg) 2.8 ( -2.8 to 8.5 ) 0.327 2.1 ( -1.2 to 5.4 ) 0.215
EXTEM MCF (mm) 0.6 ( -5.8 to 7.0 ) 0.180 2.8 ( -0.7 to 6.2 ) 0.112
EXTEM LI30 (%) -2.0 ( -12.6 to 8.7 ) 0.714 -2.2 ( -8.2 to 3.7 ) 0.465
FIBTEM CT (sec) -30.6 ( -174.1 to 113.0 ) 0.674 -11.2 ( -82.8 to 60.3 ) 0.757
FIBTEM CA5 (mm) 1.3 ( -1.4 to 3.9 ) 0.347 2.8 ( 0.1 to 4.5 ) 0.002
FIBTEM CA10 (mm) 1.0 ( -1.9 to 3.8 ) 0.512 3.0 ( 1.0 to 4.9 ) <0.001
FIBTEM alpha angle (deg) 3.5 ( -1.5 to 10.6 ) 0.137 5.0 ( 0.5 to 9.6 ) 0.032
FIBTEM MCF (mm) 0.7 ( -3.1 to 4.5 ) 0.714 4.2 ( 1.5 to 6.8 ) 0.002
FIBTEM LI30 (%) 1.3 ( -7.8 to 10.6 ) 0.779 -1.3 ( -6.9 to 4.2 ) 0.634
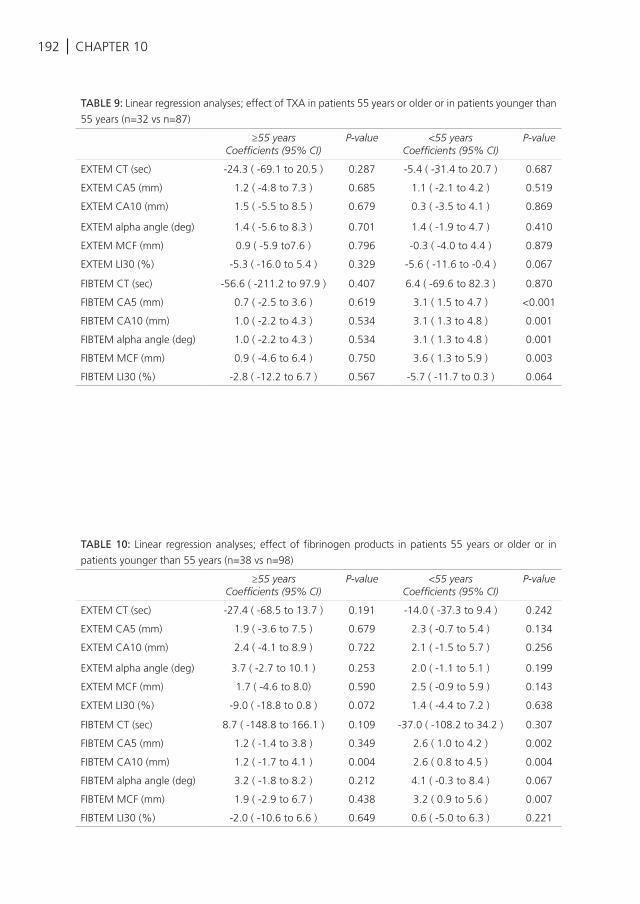
192 | CHAPTER 10
TABLE 9: Linear regression analyses; effect of TXA in patients 55 years or older or in patients younger than
55 years (n=32 vs n=87)
≥55 yearsCoefficients (95% CI)
P-value <55 yearsCoefficients (95% CI)
P-value
EXTEM CT (sec) -24.3 ( -69.1 to 20.5 ) 0.287 -5.4 ( -31.4 to 20.7 ) 0.687
EXTEM CA5 (mm) 1.2 ( -4.8 to 7.3 ) 0.685 1.1 ( -2.1 to 4.2 ) 0.519
EXTEM CA10 (mm) 1.5 ( -5.5 to 8.5 ) 0.679 0.3 ( -3.5 to 4.1 ) 0.869
EXTEM alpha angle (deg) 1.4 ( -5.6 to 8.3 ) 0.701 1.4 ( -1.9 to 4.7 ) 0.410
EXTEM MCF (mm) 0.9 ( -5.9 to7.6 ) 0.796 -0.3 ( -4.0 to 4.4 ) 0.879
EXTEM LI30 (%) -5.3 ( -16.0 to 5.4 ) 0.329 -5.6 ( -11.6 to -0.4 ) 0.067
FIBTEM CT (sec) -56.6 ( -211.2 to 97.9 ) 0.407 6.4 ( -69.6 to 82.3 ) 0.870
FIBTEM CA5 (mm) 0.7 ( -2.5 to 3.6 ) 0.619 3.1 ( 1.5 to 4.7 ) <0.001
FIBTEM CA10 (mm) 1.0 ( -2.2 to 4.3 ) 0.534 3.1 ( 1.3 to 4.8 ) 0.001
FIBTEM alpha angle (deg) 1.0 ( -2.2 to 4.3 ) 0.534 3.1 ( 1.3 to 4.8 ) 0.001
FIBTEM MCF (mm) 0.9 ( -4.6 to 6.4 ) 0.750 3.6 ( 1.3 to 5.9 ) 0.003
FIBTEM LI30 (%) -2.8 ( -12.2 to 6.7 ) 0.567 -5.7 ( -11.7 to 0.3 ) 0.064
TABLE 10: Linear regression analyses; effect of fibrinogen products in patients 55 years or older or in
patients younger than 55 years (n=38 vs n=98)
≥55 yearsCoefficients (95% CI)
P-value <55 yearsCoefficients (95% CI)
P-value
EXTEM CT (sec) -27.4 ( -68.5 to 13.7 ) 0.191 -14.0 ( -37.3 to 9.4 ) 0.242
EXTEM CA5 (mm) 1.9 ( -3.6 to 7.5 ) 0.679 2.3 ( -0.7 to 5.4 ) 0.134
EXTEM CA10 (mm) 2.4 ( -4.1 to 8.9 ) 0.722 2.1 ( -1.5 to 5.7 ) 0.256
EXTEM alpha angle (deg) 3.7 ( -2.7 to 10.1 ) 0.253 2.0 ( -1.1 to 5.1 ) 0.199
EXTEM MCF (mm) 1.7 ( -4.6 to 8.0) 0.590 2.5 ( -0.9 to 5.9 ) 0.143
EXTEM LI30 (%) -9.0 ( -18.8 to 0.8 ) 0.072 1.4 ( -4.4 to 7.2 ) 0.638
FIBTEM CT (sec) 8.7 ( -148.8 to 166.1 ) 0.109 -37.0 ( -108.2 to 34.2 ) 0.307
FIBTEM CA5 (mm) 1.2 ( -1.4 to 3.8 ) 0.349 2.6 ( 1.0 to 4.2 ) 0.002
FIBTEM CA10 (mm) 1.2 ( -1.7 to 4.1 ) 0.004 2.6 ( 0.8 to 4.5 ) 0.004
FIBTEM alpha angle (deg) 3.2 ( -1.8 to 8.2 ) 0.212 4.1 ( -0.3 to 8.4 ) 0.067
FIBTEM MCF (mm) 1.9 ( -2.9 to 6.7 ) 0.438 3.2 ( 0.9 to 5.6 ) 0.007
FIBTEM LI30 (%) -2.0 ( -10.6 to 6.6 ) 0.649 0.6 ( -5.0 to 6.3 ) 0.221
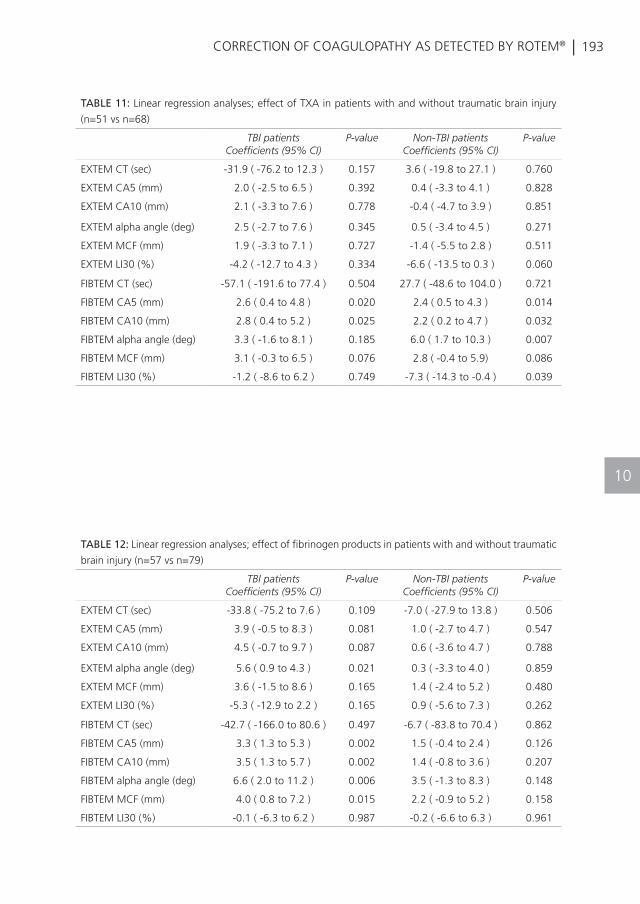
| 193CORRECTION OF COAGULOPATHY AS DETECTED BY ROTEM®
10
TABLE 11: Linear regression analyses; effect of TXA in patients with and without traumatic brain injury
(n=51 vs n=68)
TBI patientsCoefficients (95% CI)
P-value Non-TBI patientsCoefficients (95% CI)
P-value
EXTEM CT (sec) -31.9 ( -76.2 to 12.3 ) 0.157 3.6 ( -19.8 to 27.1 ) 0.760
EXTEM CA5 (mm) 2.0 ( -2.5 to 6.5 ) 0.392 0.4 ( -3.3 to 4.1 ) 0.828
EXTEM CA10 (mm) 2.1 ( -3.3 to 7.6 ) 0.778 -0.4 ( -4.7 to 3.9 ) 0.851
EXTEM alpha angle (deg) 2.5 ( -2.7 to 7.6 ) 0.345 0.5 ( -3.4 to 4.5 ) 0.271
EXTEM MCF (mm) 1.9 ( -3.3 to 7.1 ) 0.727 -1.4 ( -5.5 to 2.8 ) 0.511
EXTEM LI30 (%) -4.2 ( -12.7 to 4.3 ) 0.334 -6.6 ( -13.5 to 0.3 ) 0.060
FIBTEM CT (sec) -57.1 ( -191.6 to 77.4 ) 0.504 27.7 ( -48.6 to 104.0 ) 0.721
FIBTEM CA5 (mm) 2.6 ( 0.4 to 4.8 ) 0.020 2.4 ( 0.5 to 4.3 ) 0.014
FIBTEM CA10 (mm) 2.8 ( 0.4 to 5.2 ) 0.025 2.2 ( 0.2 to 4.7 ) 0.032
FIBTEM alpha angle (deg) 3.3 ( -1.6 to 8.1 ) 0.185 6.0 ( 1.7 to 10.3 ) 0.007
FIBTEM MCF (mm) 3.1 ( -0.3 to 6.5 ) 0.076 2.8 ( -0.4 to 5.9) 0.086
FIBTEM LI30 (%) -1.2 ( -8.6 to 6.2 ) 0.749 -7.3 ( -14.3 to -0.4 ) 0.039
TABLE 12: Linear regression analyses; effect of fibrinogen products in patients with and without traumatic
brain injury (n=57 vs n=79)
TBI patientsCoefficients (95% CI)
P-value Non-TBI patientsCoefficients (95% CI)
P-value
EXTEM CT (sec) -33.8 ( -75.2 to 7.6 ) 0.109 -7.0 ( -27.9 to 13.8 ) 0.506
EXTEM CA5 (mm) 3.9 ( -0.5 to 8.3 ) 0.081 1.0 ( -2.7 to 4.7 ) 0.547
EXTEM CA10 (mm) 4.5 ( -0.7 to 9.7 ) 0.087 0.6 ( -3.6 to 4.7 ) 0.788
EXTEM alpha angle (deg) 5.6 ( 0.9 to 4.3 ) 0.021 0.3 ( -3.3 to 4.0 ) 0.859
EXTEM MCF (mm) 3.6 ( -1.5 to 8.6 ) 0.165 1.4 ( -2.4 to 5.2 ) 0.480
EXTEM LI30 (%) -5.3 ( -12.9 to 2.2 ) 0.165 0.9 ( -5.6 to 7.3 ) 0.262
FIBTEM CT (sec) -42.7 ( -166.0 to 80.6 ) 0.497 -6.7 ( -83.8 to 70.4 ) 0.862
FIBTEM CA5 (mm) 3.3 ( 1.3 to 5.3 ) 0.002 1.5 ( -0.4 to 2.4 ) 0.126
FIBTEM CA10 (mm) 3.5 ( 1.3 to 5.7 ) 0.002 1.4 ( -0.8 to 3.6 ) 0.207
FIBTEM alpha angle (deg) 6.6 ( 2.0 to 11.2 ) 0.006 3.5 ( -1.3 to 8.3 ) 0.148
FIBTEM MCF (mm) 4.0 ( 0.8 to 7.2 ) 0.015 2.2 ( -0.9 to 5.2 ) 0.158
FIBTEM LI30 (%) -0.1 ( -6.3 to 6.2 ) 0.987 -0.2 ( -6.6 to 6.3 ) 0.961
SUMMARY AND FUTURE PERSPECTIVES

196 |
SUMMARY
In trauma patients, massive haemorrhage is the leading cause of mortality. Exsanguination accounts for more than 30% of mortality in trauma patients1. The main part of the treatment of massive haemorrhage is to stop the bleeding. However, the development of trauma-induced coagulopathy (TIC) hampers this and exacerbates the bleeding. Therefore, treatment of TIC is a cornerstone in achieving haemostasis and the therapy of bleeding trauma patients. Controlling the bleeding by a surgical procedure is not possible without a good functioning clotting system. However, adequate diagnosis and treatment of TIC remain major challenges to physicians. Therefore, more knowledge about coagulopathy and bleeding in trauma patients is required to improve outcome. For example, identifying trauma patients who are at high risk for coagulopathy might result in an increased survival. The first important question is: how are we able to diagnose TIC rapidly and accurately and how do we treat trauma patients with a diminished clotting ability? Nowadays, we use conventional clotting tests to diagnose coagulopathy, however these tests are time-consuming and useless in the treatment of coagulopathy2-5. Results become available when the bleeding trauma patient is already exsanguinated or transferred to the operating theatre or the intensive care unit. Currently, there is no accurate diagnostic and monitoring tool for TIC. Transfusion of blood products is therefore empirical rather than based upon precise laboratory tests. Viscoelastic Heamostatic Assays (VHAs) have shown promising results in their ability to identify TIC in trauma patients6-10. However, these tests have not yet been validated in trauma patients and it is unknown which threshold values are applicable to trauma patients. Furthermore, if a coagulopathic trauma patient has been identified, it is undetermined which transfusion therapy is associated with normalization of the clotting system and the best outcome.
While TIC needs prompt treatment, overtransfusion should be avoided, as there is a clear correlation between blood transfusion and adverse outcome. There is a knowledge gap also in determining who does NOT need aggressive correction of TIC with transfusion therapy. In treating trauma patients, the second question is: how are we able to succeed in achieving timely transfusion, while avoiding unnecessary transfusion of blood product?
This thesis focussed on some of these specific knowledge gaps in the field of diagnosis and treatment of TIC in severely injured trauma patients. The first part of thesis discussed the diagnosis and the second part the treatment of TIC.
| 197SUMMARY AND FUTURE PERSPECTIVES
SUMMARY OF RESULTS
PART 1
Diagnosis of TICConventional clotting tests reflect only a part of the coagulation status and are time-consuming. Therefore alternatives for diagnosing coagulopathy in trauma patients are warranted. Thromboelastometry (ROTEM®) and thromboelastography (TEG®) are point-of-care devices, which are able to detect the coagulation status throughout the process of clot formation until clot breakdown. However, whether these tools are also valuable in the prediction of outcome remains to be determined. An increasing amount of attention for VHAs is being observed, although studies in this field are limited. In the narrative review in Chapter 1 an overview is given of the utility of the ROTEM® and TEG® to detect coagulopathy in critically ill non-bleeding patients. In sepsis patients it appeared that hypocoagulopathy was associated with multiple organ failure, also known as disseminated intravascular coagulation (DIC). However, in contrast to these findings, in trauma patients a hypercoagulable state as measured by VHA predicted the development of thrombo-embolic events, although not all studies confirmed this finding. Due to heterogeneity of study designs and control groups, lack of reference standards and variability of chosen endpoints, it was not possible to draw definite conclusions.
Chapter 2 aimed to further determine the association between coagulopathy and multiple organ failure. This chapter focused on the predictive ability of hypercoagulopathy detected by ROTEM® for the development of multiple organ failure. Multiple organ failure is the main cause of late mortality among trauma patients. Early detection of multiple organ failure may provide opportunities for prevention of MOF, e.g. by interfering with coagulation status. However, in contrast to the hypothesis of this study, hypocoagulopathy instead of hypercoagulopathy on arrival to the Emergency Department, was associated with the development of MOF. I suspect that a hypocoagulable state on admission transfers towards a hypercoagulable state later during hospital stay, which may predispose to MOF. The consumption of protein C may be paramount in this process. This is further elaborated in chapter 5, in which we reviewed risk factors for MOF in trauma. This will be discussed under the heading treatment of TIC.
Currently, the suspicion of bleeding, hypovolemia and the haemoglobin level are frequently used as triggers for transfusion. However, it is unknown whether these factors predict bleeding adequately and are able to use as a transfusion target. Additionally,

198 |
these triggers may differ between specific patient populations. For example, in patients suffering from traumatic brain injury (TBI), it was shown that the injured brain may not tolerate lower haemoglobin (Hb) levels in an effort to maintain adequate cerebral oxygenation in order to prevent secondary ischemic injury to neuronal tissue. At the same time, there is an association between transfusion and adverse outcome of TBI. Therefore, early diagnosis and treatment of coagulopathy and bleeding may improve survival in these patients. However, the effect of a low Hb level on the neurologic outcome is less well determined. Therefore, the association between a low Hb level and neurologic outcome in critically ill traumatic brain injury patients was determined in Chapter 3. As hypothesized, a low Hb level was associated with a poor neurologic outcome in traumatic brain injury patients. In particular, multi-traumatized TBI patients were at high risk for a reduced neurologic recovery. Multi-traumatized TBI patients received more blood products, which suggest that blood loss was more pronounced in multi-traumatized TBI patients, which may result in a reduced cerebral oxygenation and a poorer neurologic outcome. Large randomized controlled trials in TBI patients are required to further investigate the association between low Hb levels and neurologic outcome and to investigate whether maintenance of higher Hb levels improve functional outcome in TBI patients.
Previous studies have reported that microparticles (MPs) have an important role in activating the coagulation system after trauma. As the coagulation system and the immune system are integrated, it is likely that MPs could also mediate the immune response after trauma. Therefore, the role of endogenous MPs in mediating the immune response after trauma was investigated in Chapter 4. Results indicated that severely injured trauma patients have a reduced immune response, which was strongly associated with a decreased number of circulating endogenous MPs. In particular, MPs derived from platelets, were able to drive the synthesis of proinflammatory cytokines, thereby contributing to host response and abrogating immunoparalysis. This begs the question as to whether MPs may be used in future studies as an interventional target. Furthermore, given the association between MPs and the coagulation ability, the question is whether transfusion with blood products containing exogenous MPs contribute to the improvement of the inflammatory status and improve TIC.
PART 2
Treatment of TICElaborating on the findings of Chapter 1 and 2, in which the role of TIC as a driver of early and late outcome of trauma was identified, risk factors associated with TIC and transfusion practice for the development of multiple organ failure after trauma were
| 199SUMMARY AND FUTURE PERSPECTIVES
assessed in Chapter 5. According to the results of Chapter 2, not hypercoagulopathy but hypocoagulopathy on arrival to the Emergency Department was found to be associated with the development of multiple organ failure. We hypothesized that later during hospital stay, the coagulation profile shifts from a hypocoagulable state towards a hypercoagulable state, which may predispose to multiple organ failure. The consumption of activated protein C results in a decreased inhibition of clotting factor V and VIII, causing a hypercoagulable state. However, future studies are required to confirm this hypothesis. Additionally, risk factors related to transfusion practice for multiple organ failure were determined. The administration of crystalloids, transfusion of red blood cells and a prolonged storage time of red blood cells seemed to increase the incidence of multiple organ failure. Procoagulant therapy was not identified as a risk factor, which indicates that procoagulant therapy has an acceptable safety profile and may be integrated in transfusion practice in order to limit blood loss and transfusion of unnecessary blood products.
Although emphasis has been on transfusion therapy in trauma, the impact of accidental hypothermia on mortality is also high. This may be related to the lethal triad, which include hypothermia, acidosis and coagulopathy. In Chapter 6, the effect of hypothermia upon arrival to the Intensive Care Unit on mortality was assessed. Hypothermia occurred in more than 30% of the patients admitted to an Intensive Care Unit and was identified as an independent predictor for early and late mortality. Other risk factors identified for late mortality include coagulopathy, a high injury severity score, traumatic brain injury and an advanced age.
Massive Transfusion Protocols (MTPs) have been institutionalized in order to provide rapid treatment with plasma. As part of these MTPs, plasma is kept thawed for this purpose. In Chapter 7 we demonstrated that a hospital-wide introduction of an MTP ensures a well-balanced transfusion ratio of red blood cells, plasma and platelets of 1:1:1. However, the group transfused with a balanced transfusion ratio received more blood products, which might be a disadvantage, as transfusion of blood products is also associated with adverse outcomes including infections, acute respiratory distress syndrome and the development of multiple organ failure. Another important finding of the study was that an MTP comes at the cost of an increased waste of fresh frozen plasma, which is caused by keeping pre-thawed plasma available. The waste of blood products was lowered after extending the duration of storage time from 3 to 5 days after thawing.
As a consequence of early plasma transfusion/use of MTP, the use of AB plasma as the universal donor of plasma has been increased. AB plasma does not contain
200 |
anti-A and anti-B antibodies and is thought to be safe to administer prior to cross matching. However, blood type AB is less common than other blood types. Also, in the Netherlands, there is a policy of limiting donation of plasma to males, as transfusion of female plasma is associated with the occurrence of transfusion-related acute lung injury . Therefore, blood banks are running out of their AB plasma supplies and call for alternatives. Chapter 8 systematically reviews papers that have examined alternatives for transfusion of AB plasma in massively bleeding patients. The findings of this study suggest that additional research is required as studies in this field are limited. In the meantime, it is recommended to transfuse type-specific plasma. However, in an emergency release setting, when type specific plasma is too time-consuming and AB plasma is not available, A plasma seems to be the best alternative.
In addition to the ratio of blood products, pro-coagulant therapy such as fibrinogen containing products and anti-fibrinolytic therapy such as tranexamic acid (TXA) are increasingly being used during trauma resuscitation. However, until now, no studies have reported the effect of a balanced transfusion ratio in combination with the administration of TXA and fibrinogen products on TIC and mortality. Therefore, the aim of Chapter 9 was to investigate the effect of transfusion ratios, TXA and fibrinogen products on the number of patients requiring massive transfusions (≥10 RBCs in 24 hours) and overall survival in bleeding trauma patients, in a combined model. The second aim was to evaluate which transfusion strategy was associated with correction of TIC, as measured by an elevated INR. We observed that TXA and a high platelet to RBC ratio were associated with an increased number of patients alive and free of massive transfusion. Blood product ratio, TXA and fibrinogen products did not correct coagulopathy as defined by a prolonged INR. Fibrinogen products did not affect outcome, however under-dosing may have influenced the outcome. Of note, the effect of plasma was less apparent. These findings may offer guidance for designing a randomized controlled trial, in which the effect of the addition of TXA and fibrinogen products to a balanced resuscitation will be investigated.
Monitoring of the effect of therapy on TIC is vital in order to treat TIC but avoid overtransfusion. However, the response of ROTEM® to transfusion practice is largely unknown. Therefore, Chapter 10 determined which transfusion strategy was associated with normalization of deranged VHA profiles measured by ROTEM®. The findings of this study indicated that administration of a high ratio of platelets to RBCs was most effective in improving clot formation. The beneficial effect of platelets on the coagulation system may consist of stabilizing of the endothelial cells and aggregation and adhesion of platelets for clot formation. Additionally, platelets provide an efficient surface for accumulation of clotting enzyme complexes. A beneficial effect on normalization of
| 201SUMMARY AND FUTURE PERSPECTIVES
deranged ROTEM® parameters of clotting was also observed for a high plasma to RBC ratio, however less pronounced. This is surprising, as previous studies including the PROPPR trial, reported a beneficial effect of plasma on the coagulation profile11. A possible explanation might be that plasma also contains anticoagulant proteins, which may hamper any potential pro-coagulable effect of plasma. Furthermore, we found differential effects in various patient populations. This suggests that a more personalized treatment is associated with improved coagulation profiles. Thereby, this study is the first attempt towards personalization of transfusion therapy. In theory, such an approach would result in transfusion in those who need it and no transfusion in those who do not, thereby decreasing amounts of unneccesary transfusion with improved outcome and less waste. However, future studies are required to determine whether a targeted, personalized transfusion therapy results in improved outcome and more efficient resuscitation.
GENERAL DISCUSSION AND FUTURE PERSPECTIVES
Diagnosis of TICPrompt and adequate identifying of patients with a high bleeding risk prevents massive blood loss and subsequently haemorrhagic shock-related death. Although conventional clotting tests, like activated partial thromboplastin time (aPTT), prothrombin time (PT), the international normalized ratio (INR), platelet count, fibrinogen and d-dimer are frequently used, these tests are useless in guiding transfusion2-5.
These conventional tests are time-consuming and not adequate in identifying patients with TIC. The impact of these tests on transfusion practice is therefore limited. Until now, transfusion practice has been guided by either empirical ratios or by clinical judgement. This is a major problem, leaving the trauma team at a loss of how to monitor major bleeding. Point-of-care diagnostics like VHA assays may be a valuable alternative for conventional clotting test. However, a recent meta-analysis stated that due to a lack of data, VHA guided treatment should be done in research settings only12. Despite these limitations, VHAs like ROTEM® and TEG® are increasingly being used in daily practice and in different patient populations, including trauma patients, without Level-1 evidence. This is alarming, as reference values are lacking and VHAs are not actually validated in trauma patients. More research is required to provide definite recommendations in this field. Furthermore, although the principles of ROTEM® and TEG® are similar, interpretation of the two tests are not interchangeable. Only a small number of studies have compared both tests and the majority of these studies were not performed in trauma patients. Therefore, future studies are required to investigate the comparability of ROTEM® and TEG® in trauma patients.
202 |
As part of INTRN and the Activation of Coagulation and Inflammation in Trauma study (ACIT, UKCRN ID: 5637), and by using a large database of trauma patients, this thesis focussed on some of the specific knowledge gaps in the field of diagnosis and treatment of TIC in severely injured trauma patients. This thesis showed that VHAs are promising tools for diagnosis and monitoring of TIC in trauma patients on account of their ability to reflect the whole coagulation profile, from clot formation until clot breakdown. Furthermore, these test accurately and rapidly identify coagulopathy in trauma patients. Results of this thesis pave the way for a trial which will investigate monitoring of TIC with VHAs.
Therefore, these tests are useful for guidance of transfusion practice. These assays make it feasible to shift from a one-size-fits-all empirical treatment towards a tailor made treatment. Currently, a randomized controlled trial, named the Targeted Action for Curing Trauma Induced Coagulopathy, will compare empirical administration of blood product ratios with patient-matched targeted transfusion policy guided by VHAs. This will be the first randomized controlled trial to compare the effectiveness of different transfusion practices across Europe. Based upon the results of this trial, universal guidelines will be delivered for how coagulopathy should be monitored and treated in trauma patients.
Treatment of TIC Throughout the last decades, an increasing number of studies have investigated transfusion practice in trauma patients. However, mortality associated with massive blood loss is still high. In order to reduce haemorrhagic deaths in severely injured trauma patients, it is important to treat TIC. Various actions have been implemented to prevent and treat TIC. However, which transfusion strategy is associated with best outcome in trauma patients, is still unknown.
The introduction of a massive transfusion protocol based on an empirical ratio approach is an adequate way to achieve transfusion of blood products in a 1:1:1 ratio. However, although time to transfusion is reduced by keeping pre-thawed plasma available, clear evidence for the beneficial effect of the implementation of a balanced transfusion ratio on the correction of TIC and mortality is still lacking. In particular in the context of pro-coagulant and anti-fibrinolytic agents, which are increasingly being used. This thesis showed that pro-coagulant and anti-fibrinolytic agents have a considerable effect on coagulopathy and may to some extent be superior to ratio of blood products in terms of correction of coagulopathy. However, although promising, beneficial effects of these agents have been reported in only a small number of studies and the majority of these studies are conflicting. Furthermore, across the globe, a large variation in transfusion
| 203SUMMARY AND FUTURE PERSPECTIVES
strategies exists. Studies in hospitals in the United States suggest that pro-coagulant and anti-fibrinolytic agents are given to a minority of patients11, 13, whereas in European hospitals these agents are widely used and are integrated in European guidelines14, 15. Also, the effect of pro-coagulant agents on the occurrence of thromboembolic events is still poorly studied.
Another downside of the implementation of empirical massive transfusion protocols and the administration of blood products in a balanced transfusion ratio, is the waste of pre-thawed plasma, which is remarkably high. Alternatives like freeze dried plasma may decrease the waste of pre-thawed plasma units. However, there is limited experience with free dried plasma in clinical settings.
A better alternative might be personalized transfusion of blood products and pro-coagulant agents by monitoring the coagulation profile by VHAs, thereby avoiding unnecessary transfusion of blood products and pro-coagulant agents. Therefore, we have tried to investigate the response of VHA assays to transfusion of blood products and pro-coagulant agents. Our data suggest that administration of a high ratio of platelets to RBCs has a more profound effect on improving clot formation than a high plasma to RBC ratio. This is innovative as previous studies reported that in particular transfusion of a high ratio of plasma was associated with an improved outcome in critically injured trauma patients. Also, our data suggest that a personalized therapy may improve the coagulation profile and outcome of trauma patients as the response of VHAs to therapy differed between specific patient populations. However, future randomized controlled transfusion trials are required to test whether personalised transfusion may improve outcome after trauma. Currently, a transfusion trial is being conducted, which will compare existing transfusion practice with a targeted treatment of TIC by using ROTEM® and TEG®. This Targeted Action for Curing Trauma Induced Coagulopathy (TACTIC) trial will deliver guidelines and support clinical management of coagulopathic bleeding.
204 |
REFERENCES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
Sauaia A, Moore FA, Moore EE, Moser KS,
Brennan R, Read RA, et al. Epidemiology of
trauma deaths: a reassessment. J Trauma.
1995;38(2):185-93.
Holcomb JB, Minei KM, Scerbo ML, Radwan
ZA, Wade CE, Kozar RA, et al. Admission
rapid thrombelastography can replace
conventional coagulation tests in the
emergency department: experience with
1974 consecutive trauma patients. Annals of
surgery. 2012;256(3):476-86.
Dzik WH. Predicting hemorrhage using
preoperative coagulation screening assays.
Current hematology reports. 2004;3(5):324-
30.
Park MS, Martini WZ, Dubick MA,
Salinas J, Butenas S, Kheirabadi BS, et
al. Thromboelastography as a better
indicator of hypercoagulable state after
injury than prothrombin time or activated
partial thromboplastin time. J Trauma.
2009;67(2):266-75; discussion 75-6.
Davenport R, Manson J, De’Ath H, Platton
S, Coates A, Allard S, et al. Functional
definition and characterization of acute
traumatic coagulopathy. Crit Care Med
2011;39(12):2652-8.
Hagemo JS, Christiaans SC, Stanworth SJ,
Brohi K, Johansson PI, Goslings JC, et al.
Detection of acute traumatic coagulopathy
and massive transfusion requirements by
means of rotational thromboelastometry: an
international prospective validation study. Crit
Care. 2015;19:97.
Schochl H, Forster L, Woidke R,
Solomon C, Voelckel W. Use of rotation
thromboelastometry (ROTEM) to achieve
successful treatment of polytrauma with
fibrinogen concentrate and prothrombin
complex concentrate. Anaesthesia.
2010;65(2):199-203.
Schochl H, Nienaber U, Hofer G, Voelckel
W, Jambor C, Scharbert G, et al. Goal-
directed coagulation management of major
trauma patients using thromboelastometry
(ROTEM)-guided administration of fibrinogen
concentrate and prothrombin complex
concentrate. Crit Care. 2010;14(2):R55.
Tauber H, Innerhofer P, Breitkopf R,
Westermann I, Beer R, El Attal R, et al.
Prevalence and impact of abnormal ROTEM(R)
assays in severe blunt trauma: results of the
‘Diagnosis and Treatment of Trauma-Induced
Coagulopathy (DIA-TRE-TIC) study’. British
journal of anaesthesia. 2011;107(3):378-87.
Johansson PI, Sorensen AM, Larsen CF,
Windelov NA, Stensballe J, Perner A, et
al. Low hemorrhage-related mortality in
trauma patients in a Level I trauma center
employing transfusion packages and early
thromboelastography-directed hemostatic
resuscitation with plasma and platelets.
Transfusion. 2013;53(12):3088-99.
Holcomb JB, Tilley BC, Baraniuk S, Fox EE,
Wade CE, Podbielski JM, et al. Transfusion
of plasma, platelets, and red blood cells in a
1:1:1 vs a 1:1:2 ratio and mortality in patients
with severe trauma: the PROPPR randomized
clinical trial. JAMA. 2015;313(5):471-82.
Hunt H, Stanworth S, Curry N, Woolley
T, Cooper C, Ukoumunne O, et al.
Thromboelastography (TEG) and rotational
thromboelastometry (ROTEM) for trauma
induced coagulopathy in adult trauma patients
with bleeding. The Cochrane database of
systematic reviews. 2015;2:Cd010438.
Holcomb JB, del Junco DJ, Fox EE, Wade
CE, Cohen MJ, Schreiber MA, et al. The
prospective, observational, multicenter,
major trauma transfusion (PROMMTT) study:
comparative effectiveness of a time-varying
treatment with competing risks. JAMA Surg
2013;148(2):127-36.
Maegele M, Inaba K, Rizoli S, Veigas P, Callum
J, Davenport R, et al. [Early viscoelasticity-
based coagulation therapy for severely injured
bleeding patients : Report of the consensus
group on the consensus conference 2014 for

| 205
REFERENCES
SUMMARY AND FUTURE PERSPECTIVES
15
formulation of S2k guidelines]. Anaesthesist.
2015.
Spahn DR, Bouillon B, Cerny V, Coats TJ,
Duranteau J, Fernandez-Mondejar E, et al.
Management of bleeding and coagulopathy
following major trauma: an updated European
guideline. Crit Care. 2013;17(2):R76.
SAMENVATTING EN TOEKOMSTPERSPECTIEVEN
208 |
SAMENVATTING
Massale bloeding is met 30% de belangrijkste oorzaak voor mortaliteit bij trauma patienten1. Het belangrijkste onderdeel in de behandeling van een massale bloeding is het stoppen van de bloeding. Echter, door het optreden van trauma-geïnduceerde coagulopatphie (TIC) wordt dit proces verhindert en verergert de bloeding. De behandeling van TIC is daarom een belangrijk onderdeel in het creëren van hemostase en in de behandeling van massaal bloedende trauma patiënten. Het controleren van een bloeding door een chirurgische interventie is niet mogelijk zonder een goed functionerend stollingssysteem. Toch blijft het adequaat diagnosticeren en behandelen van TIC een enorme uitdaging voor specialisten. Meer kennis over coagulopathie en massale bloedingen in trauma patiënten is derhalve noodzakelijk om de uitkomst van deze patienten te verbeteren. Het eerder identificeren van trauma patiënten die een hoog risico lopen om coagulopathie te ontwikkelen kan bijvoorbeeld zorgen voor een verhoogde kans op overleving. Daarbij zijn de eerste belangrijke vragen: hoe kan TIC snel en adequaat gediagnosticeerd worden en hoe moeten patiënten behandeld worden met een verminderde stollingsneiging? Tegenwoordig gebruiken we conventionele stollingstesten om coagulopathie te diagnosticeren. Echter deze testen zijn tijdrovend en daardoor niet bruikbaar om coagulopathie goed te behandelen en te monitoren2-5. Resultaten zijn vaak pas beschikbaar als de patiënt al is overleden of overgeplaatst is naar de operatiekamer of de Intensive Care. Daarom zijn er tot op heden geen accurate testen om coagulopathie te diagnosticeren en te monitoren. Transfusie van bloedproducten is daarom meer empirisch geleid dan gebaseerd op specifieke stollingstesten. Visco-elastische testen (VHAs) zijn snelle stollingstesten welke veelbelovende resultaten laten zien in hun mogelijkheid om TIC in trauma patiënten te diagnosticeren6-10. Echter zijn deze testen nog niet gevalideerd en is het onbekend welke referentiewaarden van toepassing zijn op trauma patiënten. Daarnaast is het onbekend welk transfusiebeleid geassocieerd is met het normaliseren van de stolling en de beste uitkomst.
Naast dat TIC een snelle behandeling behoeft moet over-transfusie vermeden worden, aangezien er een duidelijke relatie bestaat tussen bloedtransfusie en nadelige uitkomsten. Verder bestaat er een hiaat in kennis als het gaat over welke patiënt wel een agressieve behandeling van TIC nodig heeft en welke patiënt juist niet. Daarom is de tweede belangrijke vraag in de behandeling van trauma patiënten: Hoe zijn we in staat om tijdig te starten met transfunderen, terwijl de transfusie van onnodige bloedproducten voorkomen wordt?

| 209SAMENVATTING EN TOEKOMSTPERSPECTIEVEN
Dit proefschrift tracht een aantal van deze hiaten in kennis op het gebied van diagnose en behandeling van TIC op te vullen. Het eerste gedeelte van dit proefschrift gaat over het optimaliseren van het diagnosticeren en het tweede gedeelte over de behandeling van TIC bij trauma patiënten.
SAMENVATTING VAN DE RESULTATEN
DEEL 1
Optimaliseren van het diagnosticeren van TICConventionele stolllingstesten geven slechts een gedeelte van het stollingsprofiel weer en zijn tijdrovend. Er is daarom behoefte aan alternatieve testen voor de diagnostiek van coagulopathie. Thromboelastometrie (ROTEM®) en thromboelastographie (TEG®) zijn point-of-care testen die in staat zijn om het gehele stollingsprofiel van stolselvorming tot aan stolselafbraak in kaart brengen. Of deze testen bruikbaar zijn in het voorspellen van de uitkomst in patiënten is onbekend. Een toenemende mate van interesse voor VHAs wordt gezien, maar het aantal onderzoeken op dit gebied is nog beperkt. De beschrijvende review van Hoofdstuk 1 geeft een overzicht van het gebruik van ROTEM® en TEG® in het diagnosticeren van coagulopathie in ernstig zieke patiënten. In sepsispatiënten lijkt het erop dat hypocoagulabiliteit geassocieerd is met multi-orgaan falen (MOF). In tegenstelling tot deze bevindingen in sepsispatiënten, is hypercoagulabiliteit in trauma patiënten geassocieerd met het ontstaan van trombo-embolische complicaties. Hoewel, niet alle studies waren eenduidig in hun bevindingen. Door zowel heterogeniteit in studieopzet en controlegroepen, als een gebrek aan referentiewaarden en variabiliteit in de gekozen uitkomstmaten, was het niet mogelijk om duidelijke conclusies te trekken.
In Hoofdstuk 2 is er getracht om de associatie tussen coagulopathie en MOF verder uit te zoeken. Dit hoofdstuk richt zich op de voorspellende waarde van hypercoagulabiliteit gedetecteerd met ROTEM® voor het ontstaan van MOF. MOF is de nummer 1 oorzaak voor late mortaliteit bij trauma patiënten. Het vroeg detecteren kan MOF voorkomen, bijvoorbeeld door coagulopathie eerder te behandelen. Maar in tegenstelling tot de hypothese van deze studie, was juist hypocoagulabiliteit in plaats van hypercoagulabiliteit bij aankomst op de Spoedeisende Hulp geassocieerd met het ontstaan van MOF. Mogelijk vindt er een verschuiving plaats van hypocoagulabiliteit bij binnenkomst op de Spoedeisende Hulp naar hypercoagulabiliteit tijdens opname in het ziekenhuis. Deze verschuiving in het stollingsprofiel is mogelijk verantwoordelijk voor het ontstaan van MOF. Het verbruik van proteïne C zou hier aan ten grondslag liggen. Deze hypothese wordt verder onderzocht in hoofdstuk 5, waarin wordt ingegaan op
210 |
de risicofactoren voor het ontstaan van MOF. Hoofdstuk 6 zal besproken worden onder het kopje: ‘‘behandeling van TIC’’.
Momenteel worden hypovolemie en een laag hemoglobinegehalte (Hb) vaak gebruikt als indicaties voor transfusie, maar het is niet bekend of deze factoren een massale bloeding daadwerkelijk adequaat voorspellen. Bovendien kunnen afkapwaarden verschillen tussen specifieke patiëntengroepen. Zo werd bijvoorbeeld bij patiënten met traumatisch hersenletsel (TBI) aangetoond dat beschadigd hersenweefsel een lager Hb niet goed tolereert, omdat er onvoldoende hersenoxygenatie plaatsvindt om secundair ischemische schade te voorkomen. Maar aan de andere kant bestaat er ook een relatie tussen transfusie en een negatieve uitkomst bij TBI patiënten. Daarom kan het vroeg diagnosticeren en behandelen van zowel de coagulopathie als de bloeding bij deze patiënten de overlevingskans verbeteren. Echter, het effect van een laag Hb op de neurologische uitkomst is nog niet goed onderzocht. Daarom is de associatie tussen een laag Hb en de neurologische uitkomst bij ernstig zieke TBI patiënten verder uitgediept in Hoofdstuk 3. Zoals gesteld in de hypothese, werd een laag Hb in verband gebracht met een slechte neurologische uitkomst bij TBI patiënten. Met name multi-trauma TBI patiënten hebben een hoger risico op een verminderde neurologische uitkomst. De multi-trauma TBI patiënten ontvingen ook meer bloedproducten, wat suggereert dat bloedverlies meer uitgesproken was in deze groep, waardoor een verminderde cerebrale oxygenatie mogelijk plaatsvindt en een slechtere neurologische uitkomst gezien werd. Grote RCT’s bij TBI patiënten zijn nodig om de associatie tussen een laag Hb en de neurologische uitkomst verder te evalueren en om te onderzoeken of het in stand houden van hoger Hb de functionele uitkomst in TBI patiënten verbetert.
Eerdere studies hebben laten zien dat micropartikels (MPs) een belangrijke rol spelen bij het activeren van het stollingssysteem na trauma. Aangezien het stollingssysteem en het immuunsysteem aan elkaar verbonden zijn, is het waarschijnlijk dat MPs ook een rol spelen in het activeren van de immuunrespons na een trauma. Daarom is de rol van endogene MPs bij het mediëren van de immuunrespons na trauma onderzocht in Hoofdstuk 4. De resultaten wezen erop dat ernstig gewonde trauma patiënten een verminderde immuunrespons hebben, welke sterk geassocieerd is met een verminderd aantal circulerende endogene MPs. Vooral MPs afkomstig van trombocyten kunnen de synthese van pro-inflammatoire cytokines aanwakkeren en de immuunparalyse opheffen. Dit roept de vraag op of MPs gebruikt kunnen worden als een aangrijpingspunt voor interventies in toekomstige studies. Verder, gegeven het feit dat er een associatie tussen MPs en het stollingssysteem bestaat, zou de transfusie van bloedproducten met exogene MPs mogelijk kunnen bijdragen aan het verbeteren van de immuunrespons en het opheffen van TIC.
| 211SAMENVATTING EN TOEKOMSTPERSPECTIEVEN
DEEL 2
Optimaliseren van de behandeling van TICVoortbordurend op de bevindingen van hoofdstuk 1 en 2, waarin het effect van TIC op de vroege en late uitkomst na trauma werd onderzocht, werd er in Hoofdstuk 5 verder ingegaan op risicofactoren die geassocieerd zijn met TIC en het transfusiebeleid voor het ontwikkelen van MOF. Volgens de resultaten van hoofdstuk 2, bleek niet hypercoaguloabuliteit maar hypocoaguloabiliteit bij aankomst op de Spoedeisende Hulp een relatie te hebben met de ontwikkeling van MOF. Op basis van deze bevindingen is het mogelijk dat het stollingsprofiel verschuift van een hypocoagulopathie naar een hypercoagulopathie gedurende opname in het ziekenhuis en dat deze verschuiving in het stollingsprofiel kan leiden tot het ontstaan van MOF. Daarbij is de gedachtegang dat het verbruik van geactiveerd proteïne C leidt tot een verminderde inhibitie van stollingsfactor V en VIII, waardoor een hypercoagulopathie ontstaat. Echter, toekomstige studies zijn nodig om deze hypothese te bevestigen. Verder werd er ook gekeken naar risicofactoren voor MOF welke geassocieerd zijn met het transfusiebeleid. Het toedienen van kristalloïden, de transfusie van rode bloedcelzakken (RBCs) en een verlengde bewaartijd van RBCs werden als risicofactoren voor MOF geïdentificeerd. Opvallend was dat het toedienen van procoagulantia niet werd geïdentificeerd als een risicofactor voor MOF. Dit doet veronderstellen dat procoagulantia een aanvaardbaar risicoprofiel hebben en geïntegreerd kunnen worden in het transfusiebeleid om zo bloedverlies te verminderen en de transfusie van onnodige bloedproducten te voorkomen.
Hoewel de nadruk ligt op het transfusiebeleid bij trauma patiënten, kunnen de gevolgen van accidentele hypothermie op de uitkomst na een trauma ook groot zijn. Hypothermie is samen met acidose en coagulopathie onderdeel van de dodelijke trias. In Hoofdstuk 6 wordt het effect van hypothermie bij aankomst op de Intensive Care op de mortaliteit beschreven. Hypothermie treedt op in meer dan 30% van de patiënten bij aankomst op de Intensive Care en werd geïdentificeerd als een onafhankelijke voorspeller voor vroege en late mortaliteit. Andere risicofactoren voor late mortaliteit waren coagulopathie, een hoge Injury Severity Score (ISS), traumatisch hersenletsel en een leeftijd ouder dan 55 jaar.
Massale Transfusie Protocollen (MTP) worden gebruikt om een snellere toediening van plasma te bewerkstelligen. Als onderdeel van het MTP wordt plasma hiervoor ontdooid bewaard. In Hoofdstuk 7 wordt aangetoond dat invoering van een MTP ziekenhuisbreed een goede manier is om een transfusieverhouding van erytrocyten, plasma en trombocyten in een 1:1:1 ratio te bewerkstelligen. Echter, de groep die getransfundeerd werd met een 1:1:1 ratio kreeg meer bloedproducten toegediend
212 |
wat een nadeel zou kunnen zijn, aangezien de transfusie van bloedproducten ook geassocieerd is met een toegenomen risico op infecties, Acute Respiratory Distress Syndrome (ARDS) en de ontwikkeling van MOF. Een andere belangrijke bevinding van deze studie is dat de invoering van een MTP geassocieerd is met een toegenomen verspilling van plasma, welke veroorzaakt wordt door plasma ontdooid te bewaren. Echter, de verspilling van plasma kan teruggedrongen worden door de bewaartijd van plasma te verlengen.
Als gevolg van het vroeg transfunderen van plasma en het invoeren van een MTP is het gebruik van AB plasma als universele donor voor plasma toegenomen. AB plasma bevat namelijk geen anti-A en anti-B-antilichamen en is daardoor veilig toe te dienen voordat de bloedgroep bepaald is middels kruisbloed. Echter, bloedgroep AB komt minder vaak voor dan andere bloedgroepen. Ook wordt er in Nederland een beleid gehanteerd waarin het toedienen van plasma beperkt is tot plasma afkomstig van mannen. Transfusie van plasma afkomstig van vrouwen wordt namelijk geassocieerd met het optreden van transfusie-gerelateerde acute longschade. Daarom raken de plasmavoorraden van bloedbanken op en is men op zoek naar alternatieven voor AB plasma. In Hoofdstuk 8 is er systematisch gezocht naar alternatieven voor de transfusie van AB-plasma in massaal bloedende patiënten. De resultaten van deze studie suggereren dat verder onderzoek op dit gebied noodzakelijk is, aangezien het aantal onderzoeken op dit gebied beperkt is. In de tussentijd blijft het raadzaam om type-specifiek plasma te transfunderen. Echter, in noodsituaties, wanneer type-specifiek plasma te tijdrovend is en AB plasma niet beschikbaar, lijkt het transfunderen van A plasma een goed alternatief.
Naast de ratio van bloedproducten worden procoagulantia, zoals fibrinogeen bevattende producten en antifibrinolytica, zoals tranexaminezuur (TXA), steeds vaker gebruikt tijdens traumaopvang. Echter, tot nu toe zijn er geen studies die het effect van een gebalanceerde transfusieverhouding in combinatie met de toediening van TXA en fibrinogeen bevattende producten op TIC en de mortaliteit onderzocht hebben. Daarom was het doel van Hoofdstuk 9 om het effect van de transfusieratio in combinatie met TXA en fibrinogeen bevattende producten op het aantal patiënten die een massale transfusie (≥10 RBCs in 24 uur) ontvangen en de overleving bij bloedende traumapatiënten in een gecombineerd model te onderzoeken. Het tweede doel van de studie was om te evalueren welke transfusiestrategie geassocieerd was met de correctie van TIC, zoals gemeten met de INR. Resultaten laten zien dat een hoge trombocyten:RBC ratio en TXA geassocieerd zijn met een verhoogde overleving en een kleiner aantal patiënten die een massale transfusie ontvangen. De ratio van bloedproducten, TXA en fibrinogeen bevattende producten waren niet geassocieerd met de correctie van coagulopathie.
| 213SAMENVATTING EN TOEKOMSTPERSPECTIEVEN
Fibrinogeen bevattende producten hadden geen invloed op de primaire en secundaire uitkomstmaten, maar onder-dosering kan de uitkomst beïnvloed hebben. Belangrijk om daarnaast te noemen is dat het positieve effect van plasma minder duidelijk naar voren kwam. De bevindingen van deze studie kunnen gebruikt worden voor het ontwerpen van een RCT, waarin het effect van de ratio van bloedproducten gecombineerd met het effect van TXA en fibrinogeen bevattende producten onderzocht wordt.
Het monitoren van het effect van het transfusiebeleid op TIC is belangrijk om TIC goed te kunnen behandelen en om over-transfusie te voorkomen. Echter is de respons van ROTEM® op het transfusiebeleid grotendeels onbekend. Daarom werd in Hoofdstuk 10 bepaald welke transfusiestrategie geassocieerd is met de normalisering van coagulopathie gemeten door ROTEM®. De resultaten van deze studie tonen aan dat de toediening van een hoge verhouding van trombocyten ten opzichte van RBCs het meest effectief was in het verbeteren van de stollingsvorming. Het positieve effect van trombocyten op de stolling kan ten eerste verklaard worden door het effect dat trombocyten hebben op het stabiliseren van de endotheelcellen. Daarnaast is aggregatie en adhesie van trombocyten noodzakelijk voor de stolselvorming. Verder kunnen stollingsenzymen zich hechten aan trombocyten. Een gunstig effect op de normalisatie van gestoorde ROTEM® parameters werd ook waargenomen na toediening van een hoge plasma:RBC verhouding, maar dit was echter minder uitgesproken. Dit is opvallend, zeker aangezien eerdere studies, waaronder de PROPPR studie, lieten zien dat plasma een positief effect heeft op de stolling. Een mogelijke verklaring hiervoor is dat plasma ook anti-coagulante eiwitten bevat, welke een procoagulant effect van plasma verhinderen. Verder werd er gevonden dat het effect van therapie op ROTEM® parameters varieerde tussen verschillende patiëntengroepen. Deze bevindingen suggereren dat een meer gepersonaliseerde transfusiestrategie geassocieerd is met een verbetering van het stollingsprofiel. Daarmee is dit de eerste poging in de richting van het personaliseren van het transfusiebeleid. In theorie zou een dergelijke aanpak leiden tot transfusie bij de patiënten die het nodig hebben en het voorkomen van onnodige transfusie bij de patiënten die het niet nodig hebben. Daarmee zou mogelijk het aantal onnodige transfusies voorkomen kunnen worden, de uitkomst in trauma patiënten verbeteren en de verspilling van bloedproducten afnemen. Echter, toekomstige studies zijn nodig om te bepalen of een gerichte transfusiebeleid daadwerkelijk resulteert in een betere uitkomst en het efficiënter transfunderen.
ALGEMENE DISCUSSIE EN TOEKOMSTPERSPECTIEVEN
Optimaliseren van het diagnosticeren van TICHet snel en adequaat identificeren van patiënten met een hoog bloedingsrisico
214 |
voorkomt massaal bloedverlies en vermindert de mortaliteit geassocieerd aan een hemorragische-shock. Hoewel conventionele stollingstesten, zoals geactiveerde partiële tromboplastinetijd (aPTT), protrombinetijd (PT), de internationale genormaliseerde ratio (INR), trombocyten, fibrinogeen en d-dimeer vaak worden gebruikt, zijn deze testen niet bruikbaar in het begeleiden van transfusie2-5.
Deze conventionele testen zijn namelijk tijdrovend en inadequaat in het identificeren van patiënten met TIC. De impact van deze testen op het transfusiebeleid is daardoor beperkt. Dit is een groot probleem, aangezien dit ervoor zorgt dat het traumateam aan zijn lot wordt overgelaten in het monitoren en het behandelen van een massale bloeding. Point-of-care testen zoals VHAs kunnen een waardevol alternatief zijn voor de conventionele stollingstesten. Echter, een recente meta-analyse geeft als aanbeveling dat wegens een gebrek aan goede onderzoeken VHA geleide transfusie alleen uitgevoerd mag worden voor onderzoekdoeleinden12. Ondanks deze aanbeveling, worden VHAs zoals ROTEM® en TEG® steeds vaker gebruikt in de dagelijkse praktijk en in verschillende patiëntenpopulaties, waaronder trauma patiënten, zonder duidelijk Level 1-bewijs . Dit is zorgwekkend, omdat referentiewaarden ontbreken en VHAs niet gevalideerd zijn bij trauma patiënten. Meer onderzoek is daarom nodig om definitieve aanbevelingen te kunnen doen op dit gebied. Bovendien, hoewel de principes van ROTEM® en TEG® vergelijkbaar zijn, zijn de interpretaties van de twee testen niet uitwisselbaar. Slechts een klein aantal studies heeft beide testen vergeleken en de meerderheid van deze studies zijn niet uitgevoerd bij trauma patiënten. Daarom zijn toekomstige studies nodig om de vergelijkbaarheid van ROTEM® en TEG® te onderzoeken in traumapatiënten.
Als onderdeel van the International Trauma Research Network (INTRN) en the Activation of Coagulation and Inflammation in Trauma studie (ACIT, UKCRN ID: 5637) en met behulp van een grote database, heeft dit proefschrift zich gericht op een aantal specifieke hiaten in de kennis op het gebied van het diagnosticeren en het behandelen van TIC bij ernstig gewonde trauma patiënten. Dit proefschrift toont aan dat VHAs veelbelovende testen zijn voor het diagnosticeren en monitoren van TIC bij trauma patiënten. VHAs zijn namelijk in staat om het gehele stollingsproces te weerspiegelen van stolselvorming tot aan stolselafbraak. Bovendien zijn deze testen snel en nauwkeurig in het identificeren van coagulopathie. Daarom zijn deze testen nuttig in het begeleiden van het transfusiebeleid. Deze testen maken het mogelijk om van een one-size-fits-all empirische behandeling over te kunnen gaan naar een transfusiebeleid op maat.
Het optimaliseren van de behandeling van TICIn de afgelopen jaren is er steeds meer onderzoek gedaan naar het transfusiebeleid bij trauma patiënten. Echter, de sterfte veroorzaakt door massaal bloedverlies is nog
| 215SAMENVATTING EN TOEKOMSTPERSPECTIEVEN
steeds hoog. Om deze mortaliteit bij ernstig gewonde traumapatiënten te kunnen verminderen, is het van belang TIC te behandelen. Diverse maatregelen zijn genomen om TIC te voorkomen en te behandelen. Echter, welke transfusiestrategie geassocieerd is met de beste uitkomst bij trauma patiënten is nog onbekend.
De invoering van een MTP is een adequate manier om transfusie van bloedproducten in een 1:1:1 ratio te bereiken. Hoewel de tijd tot transfusie wordt verminderd door het beschikbaar houden van ontdooid plasma, ontbreekt een duidelijk bewijs nog voor het gunstige effect van een 1:1:1 ratio op de correctie van TIC en mortaliteit. Met name in de context van procoagulantia en antifibrinolytica die tegenwoordig in toenemende mate worden gebruikt. Dit proefschrift laat zien dat procoagulantia en antifibrinolytica een aanzienlijk effect hebben op de correctie van TIC. Ondanks veelbelovende resultaten, zijn de gunstige effecten van deze producten gemeld in slechts een klein aantal studies en de meerderheid van deze studies rapporteren tegenstrijdige resultaten. Bovendien bestaat over de hele wereld een grote variatie in transfusiestrategieën. Studies in ziekenhuizen in de Verenigde Staten suggereren dat procoagulantia en antifibrinolytica aan een klein deel van de patiënten gegeven wordt11-13, terwijl in Europese ziekenhuizen deze producten veel worden gebruikt en geïntegreerd zijn in Europese richtlijnen14,15. Daarnaast is het effect van procoagulantia op het optreden van trombo-embolische complicaties nog onvoldoende onderzocht.
Een ander nadeel van de invoering van een MTP en het toedienen van bloedproducten in een evenwichtige verhouding is de opmerkelijk hoge verspilling van ontdooid plasma. Alternatieven zoals gevriesdroogd plasma kunnen de verspilling van ontdooid plasma mogelijk verlagen. Echter, er is er maar weinig ervaring met het gebruik van gedroogd plasma in de kliniek.
Een beter alternatief zou een gepersonaliseerd transfusiebeleid van bloedproducten, procoagulantia en antifibrinolytica zijn, welke mogelijk gemaakt kan worden door het monitoren van de stolling met VHAs. Hierdoor kan onnodige transfusie vermeden worden. Daarom is er geprobeerd om het effect van het transfunderen van bloedproducten, procoagulantia en antifibrinolytica op VHAs te onderzoeken. Onze gegevens suggereren dat de toediening van een hoge verhouding van trombocyten ten opzichte van RBCs een groter effect heeft op het verbeteren van stolling dan een hoge plasma ten opzichte van RBCs ratio. Daarnaast lieten onze data zien dat een gepersonaliseerd transfusiebeleid het stollingsprofiel en de uitkomst van trauma patiënten kan verbeteren, aangezien het effect van het transfusiebeleid op VHAs varieerde tussen verschillende patientengroepen. Toekomstige RCT’s zijn nodig om te testen of deze nieuwe manier van transfunderen de uitkomst na een trauma kan

216 |
verbeteren. Op dit moment, zal een RCT, de Targeted Action for Curing Trauma Induced Coagulopathy (TACTIC) studie, het empirisch toedienen van bloedproducten vergelijken met een op de patiënt aangepast transfusiebeleid, welke bepaald wordt op basis van VHAs. Dit zal de eerste RCT in Europa zijn waarin de effectiviteit van verschillende transfusiestrategieën vergeleken wordt. Op basis van de resultaten van deze studie kunnen universele richtlijnen worden geleverd voor het monitoren en behandelen van TIC.

| 217SAMENVATTING EN TOEKOMSTPERSPECTIEVEN
218 |
REFERENTIES
1
2
3
4
5
6
7
8
9
10
11
12
13
14
Sauaia A, Moore FA, Moore EE, Moser KS,
Brennan R, Read RA, et al. Epidemiology of
trauma deaths: a reassessment. J Trauma.
1995;38(2):185-93.
Holcomb JB, Minei KM, Scerbo ML, Radwan
ZA, Wade CE, Kozar RA, et al. Admission
rapid thrombelastography can replace
conventional coagulation tests in the
emergency department: experience with
1974 consecutive trauma patients. Annals of
surgery. 2012;256(3):476-86.
Dzik WH. Predicting hemorrhage using
preoperative coagulation screening assays.
Current hematology reports. 2004;3(5):324-
30.
Park MS, Martini WZ, Dubick MA,
Salinas J, Butenas S, Kheirabadi BS, et
al. Thromboelastography as a better
indicator of hypercoagulable state after
injury than prothrombin time or activated
partial thromboplastin time. J Trauma.
2009;67(2):266-75; discussion 75-6.
Davenport R, Manson J, De’Ath H, Platton
S, Coates A, Allard S, et al. Functional
definition and characterization of acute
traumatic coagulopathy. Crit Care Med
2011;39(12):2652-8.
Hagemo JS, Christiaans SC, Stanworth SJ,
Brohi K, Johansson PI, Goslings JC, et al.
Detection of acute traumatic coagulopathy
and massive transfusion requirements by
means of rotational thromboelastometry: an
international prospective validation study. Crit
Care. 2015;19:97.
Schochl H, Forster L, Woidke R,
Solomon C, Voelckel W. Use of rotation
thromboelastometry (ROTEM) to achieve
successful treatment of polytrauma with
fibrinogen concentrate and prothrombin
complex concentrate. Anaesthesia.
2010;65(2):199-203.
Schochl H, Nienaber U, Hofer G, Voelckel
W, Jambor C, Scharbert G, et al. Goal-
directed coagulation management of major
trauma patients using thromboelastometry
(ROTEM)-guided administration of fibrinogen
concentrate and prothrombin complex
concentrate. Crit Care. 2010;14(2):R55.
Tauber H, Innerhofer P, Breitkopf R,
Westermann I, Beer R, El Attal R, et al.
Prevalence and impact of abnormal ROTEM(R)
assays in severe blunt trauma: results of the
‘Diagnosis and Treatment of Trauma-Induced
Coagulopathy (DIA-TRE-TIC) study’. British
journal of anaesthesia. 2011;107(3):378-87.
Johansson PI, Sorensen AM, Larsen CF,
Windelov NA, Stensballe J, Perner A, et
al. Low hemorrhage-related mortality in
trauma patients in a Level I trauma center
employing transfusion packages and early
thromboelastography-directed hemostatic
resuscitation with plasma and platelets.
Transfusion. 2013;53(12):3088-99.
Holcomb JB, Tilley BC, Baraniuk S, Fox EE,
Wade CE, Podbielski JM, et al. Transfusion
of plasma, platelets, and red blood cells in a
1:1:1 vs a 1:1:2 ratio and mortality in patients
with severe trauma: the PROPPR randomized
clinical trial. JAMA. 2015;313(5):471-82.
Hunt H, Stanworth S, Curry N, Woolley
T, Cooper C, Ukoumunne O, et al.
Thromboelastography (TEG) and rotational
thromboelastometry (ROTEM) for trauma
induced coagulopathy in adult trauma patients
with bleeding. The Cochrane database of
systematic reviews. 2015;2:Cd010438.
Holcomb JB, del Junco DJ, Fox EE, Wade
CE, Cohen MJ, Schreiber MA, et al. The
prospective, observational, multicenter,
major trauma transfusion (PROMMTT) study:
comparative effectiveness of a time-varying
treatment with competing risks. JAMA Surg
2013;148(2):127-36.
Maegele M, Inaba K, Rizoli S, Veigas P, Callum
J, Davenport R, et al. [Early viscoelasticity-
based coagulation therapy for severely injured
bleeding patients : Report of the consensus
group on the consensus conference 2014 for

| 219SAMENVATTING EN TOEKOMSTPERSPECTIEVEN
REFERENTIES
15
formulation of S2k guidelines]. Anaesthesist.
2015.
Spahn DR, Bouillon B, Cerny V, Coats TJ,
Duranteau J, Fernandez-Mondejar E, et al.
Management of bleeding and coagulopathy
following major trauma: an updated European
guideline. Crit Care. 2013;17(2):R76.
RESEARCH PORTFOLIO
222 |
RESEARCH PORTFOLIO
Name PhD student: K. BalversPhD period: January 2013-December 2015Name PhD supervisors: prof. dr. J.C. Goslings and prof. dr. N.P. Juffermans
1. PHD TRAININGYear Workload
(Hours/ECTS)
General courses
Practical Biostatistics Clinical Data ManagementBROK (Basiscursus Regelgeving Klinisch Onderzoek)Scientific Writing in English for publication
2013201320132013
1.10.30.91.5
Seminars, workshops and master classes
Weekly department seminarsJournal club
2013-20152013-2014
21
2. PRESENTATIONS
Oral presentations
Endogenous microparticles drive the pro-inflammatory host immune response in severely injured trauma patients NVT Assistentensymposium, SoestduinenEuropean Congress of Trauma & Emergency Surgery, Frankfurt
20132014
0.50.5
Het gebruik van tranexaminezuur bij trauma patiënten Symposium TraumaNet, Amsterdam
2014 0.5
Effects of implementation of a massive transfusion protocol on the usage of blood products and transfusion strategiesTraumadagen, Amsterdam 2014 0.5
Is hypothermia at ICU admission an independent predictor of 28-days mortality European Congress of Trauma & Emergency Surgery, Amsterdam 2015 0.5
Haemoglobin level and neurologic outcome in patients with severe traumatic brain injury (presented by M.R. Wirtz) Chirurgendagen
2015 0.5
Poster presentations
Risk factors related to TIC and resuscitation strategies for the Development multiple organ failure in severely injured trauma patients. Traumadagen , Amsterdam 2013 0.5
| 223RESEARCH PORTFOLIO
Effects of implementation of a massive transfusion protocol on the usage of blood products and transfusion strategies The International Symposium on Intensive Care Medicine, Brussel 2014 0.5
Is hypothermia at ICU admission an independent predictor of 28-days mortality. The International Symposium on Intensive Care Medicine, Brussel 2015 0.5
Endogenous microparticles drive the pro-inflammatory host immune response in severely injured trauma patientsThe International Symposium on Intensive Care Medicine, Brussel 2015 0.5
(Inter)national conferences
Assistentensymposium traumachirurgie, SoestduinenChirurgendagen, VeldhovenTraumadagen, AmsterdamChirurgendagen, VeldhovenThe International Symposium on Intensive Care Medicine, BrusselEuropean Congress of Trauma & Emergency Surgery, FrankfurtTraumadagen, AmsterdamThe International Symposium on Intensive Care Medicine, BrusselChirurgendagen, VeldhovenEuropean Congress of Trauma & Emergency Surgery, AmsterdamTraumadagen, Amsterdam
2013201320132013
201420142014
20152015
20152015
0.250.50.750.5
0.750.750.75
0.750.5
0.750.75
3. TEACHING
Tutoring and supervising medical students in executing a scientific project
B.W. HuismanD.J.B. KleinveldM.R. WirtzI.M. LokL. BosB. Van t` LandK. PrinsA. SmitsS. SalehManagement and training of student team (n=15, 7 days a week)
20132013
2013-2014201320132014201420142015
Jan 2013- Aug 2014
1.01.02.01.01.02.01.01.01.010
4. PARAMETERS OF ESTEEM
Grants
WBSO 2014
LIST OF PUBLICATIONS
226 |
LIST OF PUBLICATIONS
K. Balvers, M.R. Wirtz, C. Rourke, S. Eaglestone, K. Brohi, S. Stanworth, C. Gaarder, J.C. Goslings, N.P. Juffermans. Haemoglobin level and neurologic outcome in patients with severe traumatic brain injury. Submitted
K. Balvers, V. Viersen C.Gaarder, K. Brohi, S. Eaglestone, S. Stanworth, P.I. Johansson, S.R. Ostrowski, J. Stensballe, M. Maegele, J.C. Goslings, N.P. Juffermans, TACTIC group.Hyperfibrinolysis in trauma patients detected by the lysis onset time. Submitted
K. Balvers, S. van Dieren, K. Baksaas-Aasen, C. Gaarder, K. Brohi, S. Eaglestone, S. Stanworth, P.I. Johansson, S.R. Ostrowski, J. Stensballe, M. Maegele, J.C. Goslings, N.P. Juffermans, TACTIC partners. Therapeutic Strategies Associated with Improved Outcomes in Bleeding Trauma Patients. Submitted
K. Balvers, S. van Dieren, K. Baksaas-Aasen, C. Gaarder, K. Brohi, S. Eaglestone, S. Stanworth, P.I. Johansson, S.R. Ostrowski, J. Stensballe, M. Maegele, J.C. Goslings, N.P. Juffermans, TACTIC partners. Transfusion strategy associated with correction of coagulopathy as detected by ROTEM® in bleeding trauma patients . Submitted
K. Baksaas-Aasen, S. van Dieren, K. Balvers, N.P. Juffermans, P.A. Næss, K. Brohi, S. Eaglestone, S. Stanworth, P.I. Johansson, S.R. Ostrowski, M. Maegele, J.C. Goslings, C. Gaarder, TACTIC partners. Rubust threshold values for TEG and ROTEM trauma algorithms-results from a large multicentre observational trial. Submitted
K. Balvers, J.M. Binnekade, J.C. Goslings, N.P. Juffermans. Is hypothermia at ICU admission an independent predictor of 28-days mortality. J Emerg Trauma Shock. 2016
K. Balvers, M.C.A. Muller, N.P. Juffermans. The utility of ROTEM to detect coagulation disorders in non-bleeding ICU patients. Annual Update in Intensive Care and Emergency Medicine 2014
M.C.A. Müller, K. Balvers, J.M. Binnekade, N. Curry, S. Stanworth, C. Gaarder, K.M. Kolstadbraaten, C. Rourke, K. Brohi, J.C. Goslings, N.P. Juffermans. The predictive value of hypercoagulability detected by ROTEM for the development of multiple organ failure in trauma. Crit Care. 2014 Dec 25;18(6):687
K. Balvers, N. Curry, D.J.B. Kleinveld, A.N. Boing, R. Nieuwland, J.C. Goslings, N.P.
| 227LIST OF PUBLICATIONS
Juffermans. Endogenous microparticles drive the pro-inflammatory host immune response in severely injured trauma patients. Shock. 2015 Apr;43(4):317-21
K. Balvers, M.R. Wirtz, J.C. Goslings, N.P. Juffermans. Risk factors related to TIC and resuscitation strategies for the development of multiple organ failure in severely injured trauma patients. Front Med (Lausanne). 2015 Apr 24;2:24
A. Driessen, N. Schäfer, V. Albrecht, M. Schenk, M. Fröhlich, E.K. Stürmer, M. Maegele; TACTIC partners. Infrastructure and clinical practice for the detection and management of trauma-associated haemorrhage and coagulopathy. Eur J Trauma Emerg Surg. 2015 Aug;41(4):413-20
N. Schäfer, A. Driessen, M Fröhlich, E.K. Stürmer,M Maegele,TACTIC partners. Diversity in clinical management and protocols for the treatment of major bleeding trauma patients across European level I Trauma Centres. Scand J Trauma Resusc Emerg Med. 2015 Oct 1;23:74
K. Balvers, M. Coppens, S. van Dieren, I.H.M. Rooyen van-Schreurs, S.S. Zeerleder, J.C. Goslings, N.P. Juffermans. Effects of implementation of a massive transfusion protocol on the usage of blood products and transfusion strategies. J Emerg Trauma Shock. 2015 Oct-Dec;8(4):199-204
K. Balvers, S. Saleh, S. Zeerleder, H. Klinkspoor, J.C. Goslings, N.P. Juffermans. Are there any alternatives for AB plasma as the universal donor in massive bleeding patients? Transfusion. 2016 Feb 25. doi: 10.1111/trf.13527
DANKWOORD
230 |
DANKWOORD
Fris en fruitig startte ik drie jaar geleden mijn promotietraject. Een leerzame periode wordt met dit proefschrift afgerond. Maar zonder een aantal mensen was dit traject een stuk moeilijker verlopen. Kort en krachtig wil ik daarom via deze weg iedereen bedanken die een bijdrage hebben geleverd. Een aantal mensen in het bijzonder.
Ten eerste mijn promotor Prof. dr. J.C. Goslings, beste Carel. De eerste keer toen ik op jouw kamer kwam, heb ik uit zenuwen je kast omver gegooid omdat het traumasein voor de eerste keer afging. Foto`s met je kinderen en bekers van TraumaNet lagen op de grond. Ondanks dat je me op dat moment waarschijnlijk het liefst zo snel mogelijk uit je kamer wilde hebben, heb je het aangedurfd om mij later toch weer in je kamer toe te laten en mij drie jaar lang te begeleiden. Of het nu een zondag was of een doordeweekse dinsdagochtend, nakijken van stukken gebeurde op ieder moment van de dag en de week. Korte maar effectieve overlegmomenten inspireerden mij om weer aan de slag te gaan. Carel, ontzettend bedankt voor je kritische blik en je steun in de afgelopen jaren.
Natuurlijk ook mijn co-promotor prof. dr. N.P. Juffermans. Beste Nicole, met jou heb ik het meest intensieve emailverkeer gehad tijdens mijn promotietraject. Ontzettend veel respect heb ik voor de manier waarop jij je klinische werk combineert met de wetenschap en het begeleiden van vele promovendi. Altijd stond je deur open en kon ik langslopen voor vragen. Ik heb het ongelooflijk getroffen met een co-promotor die zo makkelijk benaderbaar is. Jij hebt mij onder andere geleerd om de onderzoeksresultaten in een breder perspectief te zien, heel erg bedankt hiervoor.
Dank aan alle mede-auteurs die hebben meegeschreven aan de artikelen uit dit proefschrift.
Prof. dr. M.J. Schultz, prof. dr. M.W. Hollmann, prof. dr. C Boer, dr. S.S. Zeerleder, prof. dr. L.P.H. Leenen en prof. dr. K. Brohi bedankt dat u plaats wilt nemen in mijn promotiecommissie en mijn proefschrift wilt beoordelen.
Dear TACTIC partners thank you all for your efforts and for adding such value to this thesis.
Mijn voorganger Marcella Muller. Bedankt voor het opzetten van de ACIT studie waardoor ik kon instappen op een rijdende trein.
| 231DANKWOORD
Dank aan alle studenten die in de avonden en de weekenden klaar stonden om trauma patiënten te includeren.
Alle collega-onderzoekers van de IC, bedankt. Zonder al jullie tips en tricks had ik zeker nog veel meer uren achter mijn computer zwoegend moeten doorbrengen.
Jacqueline, Joke, Els, Indra, Fenne, Ingrid en Coos zonder jullie zou G4 een grote chaos zijn. En Jacq, de moeder van de trauma-onderzoekers, zonder jou zou dit proefschrift niet tot stand zijn gekomen. Bedankt voor je steun. Ik ben blij in jou ook een tikkel-liefhebber gevonden te hebben.
G4 onderzoekers wat ben ik blij dat ik jullie om me heen heb gehad afgelopen 3 jaar. Zonder jullie was het promoveren een stuk minder gezellig geweest. Zeg maar rustig, heel saai. Door jullie enthousiasme ging ik altijd met plezier naar mijn werk toe.
Dank aan de trauma-collega`s Kaij, Dominique, Robert-Jan, Manouk, Siem, Marjolein en Matthijs. Promoveren zonder de koffiebar bij Kaij was onmogelijk geweest voor mij. Gelachen maar ook stoom afgeblazen, alles kon onder het genot van een heerlijke “echte” kop koffie. Jouw verwilderde haren verklapten wanneer je weer met SPSS aan het stoeien was en zorgde voor een glimlach op mijn gezicht. Robert-Jan en Manouk, wat super fijn dat ik ook nu in het OLVG West weer met jullie mag samenwerken en bedankt dat jullie mij bij de hand wilden nemen in de “nieuwe” wereld van het dokteren. Dominique wat leuk dat we zowel samen mochten onderzoeken als zaaldokteren. Siem en Marjo, waar lawaai en gelach is, zijn jullie te vinden. Heerlijke sfeermakers zijn jullie voor G4! En Matthijs, die bijna vanaf de eerste dag betrokken is geweest bij de ACIT studie, eerst als student, later als collega-onderzoeker. Aan zo`n betrokken iemand als jij laat ik de studie met veel vertrouwen achter. En al helemaal met Guido aan je zijde. Guido geeft een nieuwe dimensie aan de traumachirurgie door het delen van updates en beeldmateriaal van AT5. Bedankt allemaal!
Joline, Saloomeh en Monique, wat een ontzettend gezellige tijd heb ik met jullie gehad. Sallie wat vind ik jou als persoon fantastisch. Zo lekker relaxt en een lach die zo aanstekelijk is dat ik me altijd vrolijk voel bij jou. Jo, altijd sta je klaar voor iedereen. Mensen met zo`n gouden hart en zo`n luisterend oor zijn maar op 1 hand te tellen. Mo, promoveren met jou bij de trauma was in een woord fantastisch. Ongelooflijk hoe wij zo dicht naar elkaar zijn toegegroeid in zo`n korte tijd. Volgens mij is er niets wat wij niet besproken hebben onder het genot van een cappuccino. Zo jammer dat ik jullie niet elke dag om mee heen heb! Echte vriendinnetjes heb ik in jullie gevonden!
232 |
De chirurgen en assistenten uit het OLVG West. Ik ben heel blij dat ik bij jullie mag leren om een dokter te zijn. Bedankt voor al het gezelligs tot nu toe en de gezelligheid die nog moet komen.
Pap, mam, Tijmen en Rogier, bedankt voor jullie onvoorwaardelijke liefde, belangstelling en steun. Heerlijk om zo`n fijne thuishaven te hebben.
Al mijn vrienden die ik niet een voor een zal noemen, maar waar ik ontzettend veel steun aan heb gehad tijdens mijn promotie. Biertjes, theetjes, diners, lunchen, lachen, sporten, shoppen en goede gesprekken voeren. Heerlijk om bij jullie te kunnen ontspannen.
Lidwine, Reinier, Feline en Michiel wat leuk om bij jullie in de familie te zijn gekomen. Altijd even attent en vriendelijk. Echt een warm bad.
Paranimfen Sanne, Elisa, Monique en Susan wat leuk om jullie aan mijn zijde te hebben op deze belangrijke dag. Ik voel me vereerd dat jullie mijn paranimfen willen zijn. Suus in het bijzonder. Wat een tijd heb jij besteed aan het in elkaar zetten van mijn proefschrift! Eeuwige dank hiervoor!
En natuurlijk lieve Wout bedankt voor je geduld, je liefde, je muzikaliteit en je vrolijkheid. Heerlijk om samen met jou aan onze toekomst te werken.

| 233DANKWOORD
CURRICULUM VITAE
236 |
CURRICULUM VITAE
Kirsten Balvers was born on the 5th of June 1987 in Woerden, The Netherlands. In 2005 she graduated from secondary school at the Stedelijk Gymnasium in Apeldoorn. She moved to Groningen to study Human Movement Sciences at the University of Groningen. After finishing her propaedeutic examination, she started her medical training at the same university and obtained her medical degree in 2013. She worked in the Sint Elisabeth Hospitaal in Curaçao for one year as part of clinical rotations.
In January 2013 she started her PhD project at the Trauma Unit and the Department of Intensive Care Medicine, under supervision of prof. dr. J.C. Goslings and prof. dr. N.P. Juffermans. During her PhD research she was part of the International Trauma Research Network (INTRN), in which 6 European Level-1 trauma centres are involved. The INTRN was funded by the European Union Framework Programme 7 (FP7) to better understand coagulopathy and to obtain more knowledge about transfusion practice in trauma patients. Kirsten was involved in two large trials which were initiated by INTRN. The first one was the prospective multicentre observational study named Activation of Coagulation and Inflammation after Trauma (ACIT) study. This thesis is partly established by using this large database of trauma patients. Furthermore, results from the ACIT study were used to develop the second trial, which is a multicentre randomised controlled transfusion trial, named the Targeted Action for Curing Trauma-Induced Coagulopathy (TACTIC) trial, which has been started in January 2016.
After three years, her work in the field of trauma-induced coagulopathy resulted in her dissertation title “Optimising diagnosis and treatment of coagulopathy in severely injured trauma patients”. At the end of her PhD project she participated in an exchange program and gained research experience in the Royal London Hospital under supervision of prof. dr. K. Brohi. Currently, Kirsten is working in the Onze Lieve Vrouwe Gasthuis (OLVG) West in Amsterdam as a surgical resident (ANIOS), under the supervision of dr. Vrouenraets.

| 237CURRICULUM VITAE