Opioids - PBworks
20
1 Opioids Dr. Majdi Bkhaitan Department of Pharmaceutical Chemistry. [email protected] www. http://medchem1432.pbworks.com Clinical Significance “Opioid agonists and partial agonist/antagonists generally act on δ, µ, and κ receptors. All of these receptors have subtypes that provide varying degrees of analgesia, euphoria or dysphoria, central nervous system depression, and perhaps, the potential for tolerance. By modifying their structures, proper ties can be changed to develop agents that require more or less hepatic metabolism and, thus, affect the duration of action and the bioavailability. Other changes in the chemical structures can yield agents with much higher affinity for analgesic receptors, which corresponds to more potency on a milligram-to-milligram basis. Other alterations of the chemical structures can lead to improved profiles regarding respiratory depression, emesis, tolerance, and allergenicity. By altering the affinities for some receptors more than others, the addictive proper ties also may be manipulated. Through an understanding of the relationship of chemical structures to biological activity, the clinician can improve the select ion of drug to the specific patient.” Jill T. Johnson, Pharm.D., BCPS, Associate Professor Department of Pharmacy Practice, College of Pharmacy, University of Arkansas for Medical Sciences
Transcript of Opioids - PBworks

1
Opioids
Dr. Majdi Bkhaitan
Department of Pharmaceutical Chemistry.
www. http://medchem1432.pbworks.com
Clinical Significance
“Opioid agonists and partial agonist/antagonists generally act on δ, µ, and
κ receptors. All of these receptors have subtypes that provide varying
degrees of analgesia, euphoria or dysphoria, central nervous system
depression, and perhaps, the potential for tolerance. By modifying their
structures, proper ties can be changed to develop agents that require more
or less hepatic metabolism and, thus, affect the duration of action and the
bioavailability. Other changes in the chemical structures can yield agents
with much higher affinity for analgesic receptors, which corresponds to
more potency on a milligram-to-milligram basis. Other alterations of the
chemical structures can lead to improved profiles regarding respiratory
depression, emesis, tolerance, and allergenicity. By altering the affinities for
some receptors more than others, the addictive proper ties also may be
manipulated. Through an understanding of the relationship of chemical
structures to biological activity, the clinician can improve the select ion of
drug to the specific patient.”
Jill T. Johnson, Pharm.D., BCPS, Associate Professor
Department of Pharmacy Practice, College of Pharmacy, University of Arkansas for Medical
Sciences

2
Analgesia/Analgesics • A number of classes of drugs that are used to relieve pain.
Are also called Anti-nociceptives:
• The non- steroidal anti-inflammatory agents have primarily a peripheral site of
action, are useful for mild to moderate pain, and often have an anti-inflammatory
effect associated with their pain-killing action.
• Local anesthetics inhibit pain transmission by inhibition of voltage- regulated
sodium channels. These agents often are highly toxic when used in
concentrations sufficient to relieve chronic or acute pain in ambulatory patients.
• Dissociative anesthetics (ketamine), and other compounds that act as inhibitors of
N-methyl -D-aspartate (NMDA)–activated glutamate receptors in the brain, are
effective antinociceptive agents when used alone or in combination with Opioids.
• Compounds, such as the anti-seizure drug Pregabulin, which inhibits voltage
regulated Ca2+ ion channels, are useful in treating neuropathic pain.
• Most central nervous system (CNS) depressants (e.g., ethanol, barbiturates, and
antipsychotics) will cause a decrease in pain perception
• Inhibitors of serotonin and nor epinephrine reuptake (i .e., antidepressant drugs)
are useful either alone and in combination with Opioids in treating certain cases
of chronic pain.
• Current research into the anti-nociceptive effects of centrally acting α-adrenergic,
cannabinoid, and nicotinic- receptor agonists may yield clinically useful
analgesics working by non-opioid mechanisms. Research in one or more of the
above areas may lead to new drugs, but at present, severe acute or chronic pain
generally is treated most effectively with opioid agents.
Opiates “opioids”
Until the 1980s, the term “Opiate” was used extensively to describe any natural or
synthetic agent that was derived from morphine. One could say an opiate was any
compound that was structurally related to morphine.
• In the mid-1970s, the discovery of peptides in the brain with pharmacological actions
similar to morphine prompted a change in nomenclature. The peptides were not easily

3
related to morphine structurally, yet their actions were like those produced by morphine.
At this time, the term “Opioid” meaning opium- or morphine-like in terms of
pharmacological action, was introduced.
• The broad group of opium alkaloids, synthetic derivatives related to the opium alkaloids,
and the many naturally occurring and synthetic peptides with morphine- like
pharmacological effects and are antagonized by an Opioid antagonist, such as Naloxone
are called Opioids.
• Receptors to which opioid agents bind and initiate biological responses are called opioid
receptors.
• Opioid systems are responsible for a variety of processes in organisms, the best
characterized of which is analgesia.
• Classical opiate pharmacology derives largely from the isolation and characterization of
alkaloids (including morphine) of the opium poppy plant “Papaver somniferu”.
Definitions
Analgesia Absence of pain without loss of consciousness
Opioid receptor agonists Drugs with morphine-like effects that bind to
opiate receptors
Opioid receptor antagonists Drugs that bind to opiate receptors and
prevent/antagonize effects of opioid agonists
Mixed agonists/antagonists Drugs with agonist and antagonist effects at
different opiate receptors; used as analgesics
Endorphins
The opioid peptides isolated from mammalian tissue are known collectively as endorphins, a
word that is derived from a combination of “endogenous” and “morphine”. The opioid alkaloids
and all of the synthetic opioid derivatives are exogenous opioids; the endogenous opioids exert
their analgesic action at spinal and supraspinal sites. They also produce analgesia by a peripheral
mechanism of action associated with the inflammatory process. In the CNS, opioids exert an
inhibitory neurotransmitter or neuromodulator action on afferent pain-signaling neurons in the
dorsal horn of the spinal cord and on interconnecting neuronal pathways for pain signals within
the brain. In the brain, the arcuate nucleus, periaqueductal gray, and the thalamic areas are
especially rich in opioid receptors and are sites at which opioids exert an analgesic action. In the
spinal cord, concentrations of endogenous opioids are high in laminae 1, laminae 2, and
trigeminal nucleus areas. All of the endogenous opioid peptides and the three major classes of
opioid receptors appear to be at least partially involved in the modulation of pain. The
endogenous opioids exert their analgesic action at spinal and supraspinal sites, Analgesia that
results from acupuncture or is self- induced by a placebo or biofeedback mechanisms is caused by

4
release of endogenous endorphins. Analgesia produced by these procedures can be prevented by
the previous dosage of a patient with an opioid antagonist.

5
Endorphin Analogues: Analogues which are stable to peptidases and which would be orally
active. This can be achieved through Replacement of non-essential amino acids with unnatural
AA’s or D-AA’s to make enkephalin unrecognisable to peptidase enzymes.
Opioid Receptors
There are the three major types of opioid receptors: µ, κ, and δ

6

7
Opioid Alkaloids
Opium contains numerous alkaloids (as Meconoate and sulfate salts) of which are therapeutically
most important:
• Morphine
• Codeine
• Noscapine
• Papaverine
• It also contains Thebaine that has convulsant properties.
In opium we can observe two types of basic structures:
• The phenanthrene type (as in morphine, codeine, thebaine)
• The benzylisoquoinoline type (as in Papaverine, Noscapine).
Biological effects of morphine:
• Increased tolerance to pain, Sleepy feeling, A sensation of
well-being, Lesser perception to external stimuli, Respiratory depression of
central origin, Tendency to cause addiction
N
CH3O
CH3O
CH2
OCH3
OCH3

8
Neurobiology of Drug Abuse and Addiction The factors that drive some individuals to abuse drugs, with resultant tolerance and psychological
and physical dependence, remains unknown. It has been proposed that a deficiency exists in the
opioid-mediated self- reward system of individuals who have a predisposition to abuse addictive
drugs.
Self-Reward Response
It is now evident that all forms of drug addiction are driven by the stimulation of the brain's self-
reward system, which originates in the ventral tegmental nucleus (VTN) and extends to the
nucleus accumbens (NAC) area of the midbrain, The µ opioid agonists work upstream in the
reward neuronal system by exerting an inhibitory action on GABAergic neurons, thus removing
the inhibitory GABAergic tonus on DA neurons and initiating the self- reward response. The κ
opioid agonists work at a site more downstream in the system and cause the opposite effect of the
µ agonists. The κ neurons synapse directly onto the DA nerve terminal in the NAC and exert an
inhibitory effect (negative tonus) on DA release. Thus, a µ agonist will cause a self- reward and
euphoric stimulus, and a κ agonist will cause an aversive and dysphoric stimulus. Alcohol
(ethanol) also causes a stimulation of the self- reward system, partially, by acting on the µ opioid
neurons to facilitate the release of endogenous opioids Thus, the common driving pathway in
drug addiction is the euphoria experienced when a drug is taken and the self -reward system is
activated by DA release. The self- reward response tends to be self- limiting, because feedback
(adaptive) mechanisms in the nerve cells attenuate the reward delivered after prolonged or
repeated activation of the system. Highly abused substances tend to have high potency, full
efficacy, and a fast onset of action so that the reward signal is initiated and fully activated before
the adaptive process can take effect. Factors that contribute to fast onset of action are high

9
lipophilicity of the drug and a dosing method that allows rapid distribution to the brain. Most
abused drugs are highly lipophilic so that they rapidly cross the blood-brain barrier. The dosage
routes preferred by drug addicts (smoking and intravenous injection) meet the criteria for fast
distribution to the brain.
Rehabilitation of Opioid Addiction The best-known treatment is the use of methadone maintenance in the rehabilitation of the opioid
addiction a well- run program, daily treatment with oral methadone maintains the addicted
(tolerant ) state while allowing minimal euphoric/aversive mood swings, attenuates drug craving,
decreases the spread of HIV (by decreasing needle sharing) , and minimizes the social destructive
behavior Other agents, such as the µ agonist L-α-acetylmethadol (levomethadyl ) and the partial µ
agonist buprenorphine, can be substituted for methadone and offer the advantage of dosing every
third day.
Evidence suggests that treatment of a detoxified opioid addict (i .e., an individual who has been
weaned from opioid dependence through a methadone or other treatment program) with a long-
acting opioid antagonist, such as naltrexone, can not only pharmacologically block readdiction
but also limit the addict 's drug-craving urge.
Morphine-like derivatives
First type of modifications brought about on morphine had the goal of separating the analgesic
effect from other types of side effects (side effects like addiction liability, respiratory depression,
GI disturbances, etc.)
These studies have focalized their attention upon modifying what are called “peripheral
groups”. Peripheral groups are:
1) Phenolic hydroxyl in position 3
2) Alcoholic
hydroxyl in
position 6.
3) Ether Bridge.
4) Alicyclic
unsaturated
linkage in position
7-8.
5) N-methyl group.
One of the more useful results in this stage was the synthesis of 5-methyl- dihydromorphinone.
This compound possesses addiction liability but it was found to be a very potent analgesic with a
minimum of other side effects like emesis and mental dullness. It was found that the methylation

10
of the alicyclic ring and its reduction (or both changes) and the absence of the alcoholic group in
position 6 brings about more active compounds. The most active compounds are the 14-hydroxy
and the dihydrodeoxy derivatives, these latter represent the most active derivatives of this series.
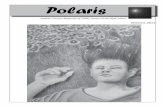
Rigid Opioids
Morphinan Derivatives
• (N-methylmorphinans): these compounds differ from
the morphine nucleus in the lack of the ether bridge
between C4-C5. This suggests the unessential nature
of the ether bridge.
SAR
• The 3-hydroxy derivative of Morphinan (levorphanol)
(the structure above) is the analgesically active one,
and it exceeds in analgesic activity that of morphine for eight times; because of a
OH
N
CH3
1
2
3 4 5 6
7
8
910
11
12 13
14
Opioids (Rigid & Non-Rigid)

11
major μ opioid receptor affinity and because of its major lipophilicity which
allows higher concentrations to reach the brain.
• The dextrorotatory derivative possesses
antitussive activity as the 3-methoxy derivative
(Dextromethorphan).
• It is essential to observe the importance of the
phenolic OH in position 3, in fact the OH in
other positions produces inactive compounds.
• The N-allyl derivative (levallorphan) is a potent
morphine antagonist. Also the N-cycloprpylmethyl
derivative (cyclorphan) is an antagonist at μ receptors
but it acts as agonist at κ (Kappa) receptors (partial
agonist), prducing analgesia with less addiction but with
other unfortunate side effects like depression caused by
the dysphoria produced from the stimulation of κ
(Kappa) receptors and also hallucination.
• The N-aralalkyl derivatives are markedly (10-20 times) more active than their
parent compounds, they are represented by ethylphenyl, p-amino ethyl phenyl,
and ethyl furyl morphinans in an increasing potency order.
Benzomorphans “Benzazocines”
• These are derivatives lacking both the ether bridge and the alicyclic ring which is
replaced by one or two methyl groups.
SAR:
• The trimethyl derivatives are more active than the dimethyl ones.
• The N-phenyl ethyl derivative (Phenazocine) is almost 20 times more active than
the corresponding N-methyl compounds.
• It was possible in some of the derivatives of this series to divorce the analgesic
activity from the addictive one. This to demonstrate the possibility of separating
the
analgesic
activity
from
undesired
side
effects.
R3
R2
OH
N
R1
R1 = CH2CH2
R2= R3 = CH3
Phenazocine
R1= CH2CH=C(CH3)2
CH3= R3R2= Pentazocine

12
• Partial antagonists with analgesic activity in the benzomorphan series were
prepared. The most prominent member is pentazocine and cyclozocine.
Pentazocine has antagonistic properties with much lower addiction liability than
morphine.
Metabolism of rigid opioids:
• Morphine is metabolized by conjugation
at the phenolic (OH). Metabolism occurs
in the liver, it occurs also in the
intestinal mucosa requiring the action of
sulfatransferase or glucuronidyl-
transferase enzymes.
• The 3-conjugates has low activity and
poor distribution. Conjugation at 6-OH
gives an active metabolite. Morphine is
also N-demethylated to nor-morphine,
which has decreased activity and
decreased bioavailability.
• Nor-Morphine undergoes N and O-
conjugation followed by excretion.
• Other rigid opioids (Morphinans,
Benzazocines) undergo similar routs of
metabolism of morphine. However
compounds with N-alkyl groups larger
than methyl get N-dealkylated as major
route of inactivation.
• Codeine in humans is 10% O-
demethylated to produce morphine that
plays an important role in its analgesic
effect
Non-Rigid Opioids
4-Phenyl Piperidine derivatives “Meperidine-like derivatives”
• Meperidine is a typical μ agonist with 1/5 of the activity of morphine.
Researchers who were trying to obtain an anti spasmodic agent discovered it
through the observation of typical side effect observed for morphine while testing
it upon test animals. It possesses an anti spasmodic activity but also analgesic,
morphine-like activity.
NCH3
R

13
SAR
• Replacement of the N-methyl group with other aralalkyl groups brings about
much more potent derivatives as in pheneridine and aniliridine.
• Structural modification of the 4-phenylpiperidine has led to the discovery of 4-
anilido piperidine derivatives or the Fentanyl group that is 50 times more potent
than morphine and Lofentanyl which is 8400 folds more potent than morphine.
These agents are used usually as anesthesia adjuncts.
• On the other hand replacing the N-methyl group with a very bulky group
produces inactive compounds as in the case of diphenoxylate and loperamide
(Imodium®), however used in the treatment of diarrhea as OTC in the case of
Loperamide.
Metabolism
• Mepiridine is considered to have a relatively short duration of action. This is due
to a rapid first pass metabolism in the liver.
NCH2
CH2R
N C
O
C2H5
Fentanyl: R=H Lofentanyl R= -COOCH3
NCH2
CH2 OH
Cl
C
CON
CH3
CH3
Loperamide
NCH3
C
O
O C2H5
MFO
EstersaeNCH3
C
O
O H
NH
C
O
O C2H5

14
• Methadone and Methadone-like derivatives • In this class of opioids we observe the disappearance of the piperidine ring; with
the tertiary amine group, in most of the members of this series, is acyclic. This to
demonstrate the unessential nature of a cyclic tertiary amine.
• Methadone, which is the principle element of this family, is twice as potent as
morphine, while its toxicity is three to ten times that of morphine, with high
addiction liability. It is used to alleviate pain and is also used to maintain addicts
in the rehabilitation of heroin addiction.
SAR:
• One of the most important derivatives of methadone is the acetyl prodrug of
Methadole, which is called L-α-acetylmethadol “LAAM”. This derivative is
characterized by longer duration of action than Methadone, due to its active
metabolites in vivo and the lack of the ketone group found in Methadone, which
is responsible for the relative rapid inactivation of it, in vivo. This allows a once
daily administration.
• R1 and R2 in all methadone
derivatives are represented by
phenyl rings.
• It is thought that one of the two
phenyl rings correspond to the
benzene found in all opioids.
Whilst the second is thought to
maintain the aliphatic chain in a
position relative to that of the
alicyclic ring found in morphine.
Therefore, any modification upon
these two phenyls will bring
about a decrease in activity.

15
Tramadol.HCl
Represents a fragment of codeine’s structure, consisting of
the phenyl and cyclohexane rings, the drug possesses opioid
activity, although it is thought to be attributed to the O-
demethylated metabolite regarding the opioid fraction of
activity. It is demonstrated that Tramadol possesses NE and
5HT reuptake inhibitory activity. Tramadol has been used in
Europe since the 1980s and was introduced to the U.S.
market in 1995. The drug is non-addicting and, thus, is not a
scheduled agent. In addition, tramadol does not cause respiratory depression or constipation
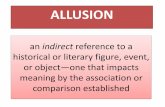
Morphine antagonists
• An N-aliphatic group instead of the usual N-methyl group characterizes the SAR
of Morphine antagonists. Examples of the aliphatic groups encountered are N-
cyclopropylmethyl (CPM), N-cyclobutyl methyl (CBM), N-allyl and N-
secpentenyl group.
• Examples of morphine derivative antagonists we can mention Naloxone,
naltrexone (considered as pure antagonists) Nalorphine and Nalbufine
(considered as partial antagonists )
• Examples of Morphinan derivative antagonists: we mention Levallorphan (as pure
antagonist),
cyclorphan and
Butorphanol
(considered partial
antagonists).
OOH
N
OH
CH2
OOH
N
OH
O
R
CH2 R=
R= CH2CH=CH2
Naltroxone
Naloxone
Nalbufine
OH
N
R
R= CH2
R= CH2
(Cyclorphan)
(Butorphanol)
R= CH2CH=CH2 (Levallorphan)

16
• Example of benzomorphan antagonists we can mention Pentazocine (considered as
partial antagonist).
Clinical uses of antagonists
Pure antagonists
• Are used as antidotes in overdose, they have the ability to reverse the respiratory
depression and deprive addicts from the euphorogenic effect of Heroine.
Some pure antagonists like Naloxone and more importantly Naltrexone are used in the
treatment of addiction in addicts.
Diagnostic test to determine narcotic addiction.
Partial antagonists:
Such as butorphanol and Pentazocine are used as:
True analgesics with less addiction liability with respect to pure agonists

17

18
μ receptor Binding Theories
1) Becket and Casey theory
2) Bimodal Binding Model theory

19
3) Enkephalin binding mode based theory

20
Antitussive agents • Cough is a protective, physiologic reflex that occurs in health as well as in
disease. Among the agents used in the symptomatic control of cough are those
that act by depressing the cough center located in the medulla. These have been
called anodynes, cough suppressants, and centrally acting antitussives. Until
recently, the only effective drugs in this area were members of the narcotic
analgesic agents.
• The more important and widely used ones were Morphine, hydromorphone,
codeine, hydrocodone, methadone, and levorphanol.
• In recent years, several compounds have been synthesized that possess
antitussive activity without the addiction liability of the narcotic agents. Some of
these new agents act in a similar manner through a central effect. It is suggested
that a bronchodilation is essential in cough relief.
• In addition to the primary antitussive agent. The more important ones include
antihistamines, sympathomimetics (bronchodilators) as ephedrine, phenylpropanolamine,
parasympatholytics and expectorants.
Codeine
• It occurs naturally, but is also produced in major quantities from morphine or even thebaine. It
is less effective orally than parenterally. It has one-tenth the potency of morphine as analgesic
due to the methylation of the phenolic hydroxyl. In high doses it can cause the same side
effects of morphine “respiratory depression, constipation, nausea, and such”. Codeine has the
reputation of being antitussive, depressing the cough reflex, and is used in many cough
preparations.
Dextromethorphan
• This drug is the O-methylated (+) form of racemorphan remaining after the resolution
necessary in the preparation of levorphanol. It possesses the antitussive properties of Codeine,
without the analgesic, addictive, central depressant, and constipating features. 10 mg are
suggested as being equivalent to 15mg of codeine as antitussive agent. This product has
replaced codeine and other older antitussive agents.
• Other antitussive agents are Noscapine, Benzonatate, Caramiphen, and carbetapentene.
References:
Foy’s: Principles of Medicinal Chemistry, Opioid Analgesics,Sixth edition,
David S. Fries, Chapter 24