
Opioid Risk:Benefit Issues U.S. Food and Drug Administration Anesthetic and Life Support Drugs...
35
Opioid Risk:Benefit Issues U.S. Food and Drug Administration Anesthetic and Life Support Drugs Advisory Committee Bethesda MD September 9. 2003 Arthur G. Lipman, PharmD Professor of Pharmacotherapy, College of Pharmacy Director of Clinical Pharmacology, Pain Management Center Pain Medicine & Palliative Care Advisory Group, Huntsman Cancer Institute
-
Upload
jane-marshall -
Category
Documents
-
view
220 -
download
0
Transcript of Opioid Risk:Benefit Issues U.S. Food and Drug Administration Anesthetic and Life Support Drugs...

Opioid Risk:Benefit IssuesU.S. Food and Drug Administration
Anesthetic and Life Support Drugs Advisory CommitteeBethesda MD
September 9. 2003
Arthur G. Lipman, PharmDProfessor of Pharmacotherapy, College of Pharmacy
Director of Clinical Pharmacology, Pain Management CenterPain Medicine & Palliative Care Advisory Group, Huntsman Cancer Institute
Investigator, Pharmacotherapy Outcomes Research and Pain Research Centers
University of Utah Health Sciences CenterEditor, Journal of Pharmaceutical Care in Pain & Symptom Control
Salt Lake City, Utah

We are appalled by the needless pain that plagues the people of the world -in rich and poor nations alike. By any reasonable code, freedom from pain should be a basic human right limited only by our ability to achieve it.
Liebeskind J, Melzack R. Pain 1987;30:1
U.S. News & World ReportMarch 17, 1997
Old Thinking
New Science

AHCPR Clinical Practice Guideline
Full Guideline Available
in searchable format
on the WWW at
www.ahrq.gov
1992

AHCPR Clinical Practice Guideline
Full Guideline Available
in searchable format
on the WWWat
www.ahrq.gov
1994

Released March 15, 2002
American Pain SocietyClinical Practice
Guideline
Available through the American Pain Society
Website
www.ampainsoc.org

Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain
Fifth Edition, 2003
Available from
American Pain Society4700 West Lake AvenueGlenview IL 60025-1485
Phone: 847 375-4715Fax: 847 375-6315E-mail: [email protected] Site:www.ampainsoc.org

Physiological Effects of Pain
increased catabolic demands poor wound healing, weakness, muscle breakdown
increased risk of thromboembolic event respiratory effects
shallow breathing, tachypnea (acutely), cough suppression increasing risk of atelectasis and pneumonia
increased sodium and water retention (renal) decreased gastrointestinal motility tachycardia and elevated blood pressure
sympathetic autonomic activation
AHCPR Acute & Cancer Pain Guidelines: www.ahrq.gov

Psychological Effects of Pain
negative emotionsanxiety
depression sleep deprivation existential suffering
may cause patients to seek end of life
AHCPR Acute & Cancer Pain Guidelines: www.ahrq.gov

Immunological Effects of Pain
impaired immune responsedecreased natural killer (NK)
cell count
AHCPR Acute & Cancer Pain Guidelines: www.ahrq.gov.Fakata KL, Lipman AG, Mullin S. APS Annual Meeting Abstracts, 2002.

Correlation of of Pain Intensity and Impact Activities Impaired by Increasing Pain on a Pain intensity Scale of 1-10
Relate
Walk Walk
Sleep Sleep Sleep
Active Active Active Active
Mood Mood Mood Mood
Work Work Work Work Work
Enjoy Enjoy Enjoy Enjoy Enjoy Enjoy
3 4 5 6 7 8 >>>>> >>>>> >>> Worst Pain Rating >>> >>>>> >>>>>
Cleeland CS, Ryan KM. Ann Acad Med Singapore. 1994;23:129-138.

Therapeutic Interventions Must Have Favorable Risk:Benefit Ratios
The risk of pain is >> than is generally appreciated– More aggressive analgesia often is needed
There is inherent risk in all pharmacotherapy– Every drug is a poison
Opioid risks must be contrasted to:– Risks of alternative pharmacotherapy– Risks of nonpharmacological therapy
Treatment Alternatives for Moderate –Severe Pain
Oral NSAIDs Oral Opioids Invasive procedures
– CNS stimulators– Spinal alnalgesia
NSAIDs
Over 125,000,000 NSAID prescriptions written in U.S. annually in 1998
Gastroduodenal and platelet effects problematic– Toxicities limit usefulness– Effects decrease adherence (compliance)

FDA NSAID Class Warning
“Risk of GI ulceration, bleeding, and perforation with NSAID: Serious GI toxicity such as bleeding, ulceration, and perforation can occur at any time, with or without warning symptoms, in patients treated chronically with NSAID…symptomatic upper GI ulcers, gross bleeding, or perforation appear to occur in approximately 1% of patients treated for 3–6 months and in about 2%–4% of patients treated for 1 year…”
NSAID Gastrointestinal ToxicityUlcers and Complications of Ulcers
107,000 hospitalizations and 16,500 deaths in U.S. reported in 1998
Endoscopically documented lesions
Over three-quarters of patients were asymptomatic prior to N+SAID-induced bleeds
COX-1 vs. COX-2
Singh G Recent considerations in nonsteroidal anti-inflammatory drug gastropathy.Am J Med. 1998 Jul 27;105(1B):31S-38S. 1998

Invasive Procedures
Generally not supported by evidence Very expensive
– highly profitable – seldom questioned by insurers
Often must be repeated Adverse sequelae

Opioid Concerns
physical dependence psychological dependence - addiction tolerance cognitive impairment respiratory depression psychomotor impairment legal sanction risks therapeutic efficacy

Opioid Addiction
Addiction in the context of pain treatment with opioids is characterized by a consistent pattern of dysfunctional opioid use that may involve:
adverse consequences associated with the use of opioids– loss of control over the use of opioids– preoccupation with obtaining opioids despite the presence of
adequate analgesiaAmerican Society of Addiction MedicinePublic Policy Statement, April, 1997

American Society of Addiction Medicine Public Policy Statement
“...Individuals who have severe, unrelieved pain may become intensely focused on finding relief for their pain. Sometimes, such patients may appear to observers to be preoccupied with obtaining opioids, but the preoccupation is with finding relief of pain, rather than using opioids, per se. This phenomenon has been termed ‘pseudoaddiction’…”
April, 1997

Distinct Types of Opioid Tolerance
Tolerance to Analgesia may occur in first days to weeks of therapy; rare after pain relief
achieved with consistent dosing without increasing or new pathology.
Tolerance to Respiratory Depression, Confusion, Sedation, and Nausea
predictable after 5-7 days of consistent opioid administration Tolerance to Constipation
does not occur; scheduled stimulating laxatives are indicated with regularly scheduled opioids
Lipman AG, Jackson KC. Opioids. In C. Warfield and Z Bajwa, Eds, Principles and Practice of Pain Management, 2nd edition, NY, McGraw Hill, 2003
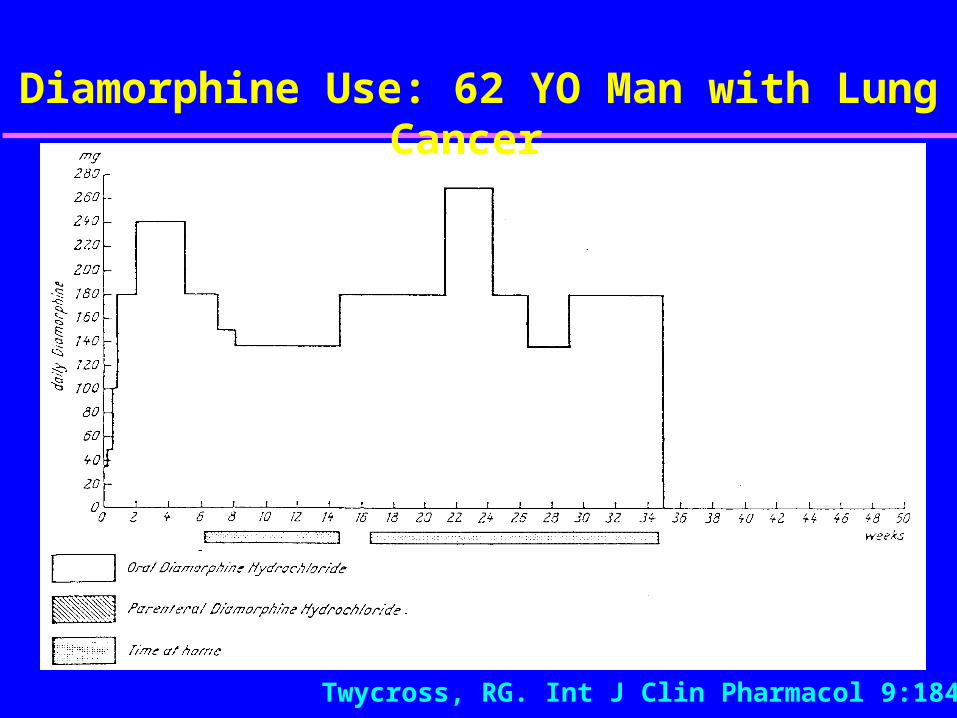
Diamorphine Use: 62 YO Man with Lung Cancer
Twycross, RG. Int J Clin Pharmacol 9:184-98

Myth: Opioids Always Depress Respiration
Acutely, opioids can be profound respiratory depressants
opioid-naïve patients After 5-7 days of continuous opioids, patients
predictably become tolerant to respiratory effects
opioid-tolerant patients pain is a powerful analeptic in awake patients

Myth: Patients in Pain Don’t Skip Analgesic Doses
Once pain is controlled for a few days, patients often skip doses, especially with short acting opioids that must be taken several times a day– fear of adverse drug effects– family and friends who fear drug effects
Long term compliance is aided by less frequent dosing

Physiological Responses to Repetitive Nociceptive Input
Winduphighly augmented response to repetitive afferent (C-fiber) input
Neuronal plasticity
changes in the CNS in response to repetitive afferent nociceptive input
Herrero JF et al. Wind-up of spinal cord neurons and pain sensation: much ado about something? Prog Neurobiol. 2000;61:1690203.
Mao J, Mayer DJ. Spinal cord neuroplasticity following repeated opioid exposure and its relation to pathological pain. Ann N Y Acad Sci. 2001;933:175-84.

Oral Long Acting Opioid Dosage Forms
Pharmacologically Long Acting
methadone levorphanol
Pharmaceutically
Long Acting morphine
– Oramorph SR, MS Contin, Kadian, Avinza Morphine ER
oxycodone – OxyContin

Methadone
Biphasic elimination– alpha (analgesic) T1/2 8-12 hours
– beta T1/2 24-36 hours - protects against withdrawal
Risk of accumulation toxicity

Methadone Biphasic Elimination
Lipman AG. Oncology. 1999;13:(9):1275-82
Therapeutic windowTherapeutic window
Analgesic onset ~ 1 hAnalgesic offset ~ 8 h

Plot of Methadone Accumulation(dosed q 8 h over 6 days)
Lipman AG. Oncology. 1999;13:(9):1275-82

Myth: Patients Taking Opioids Cannot Drive Safely
Opioids impair cognition and psychomotor coordination initially–patients should not drive for 5-7 days after starting
opioids or a dose increase After 5-7 days of continuous opioids, tolerance to
these effects develops predictably –studies show no increase in MVA in patients taking
chronic opioidsVainio A et al. Lancet 1995;346:667-70
Fishbain D et al. J Pain Palliative Care Pharmacotherap 2002;16(1):9-28.
Myth: Opioids Cause End Organ Toxicity
Respiratory and CNS toxicity do occur with
high opioid doses in opioid-naïve patients Long term opioid therapy does not produce
reported end-organ toxicity in patients who are titrated to response and monitored correctly– Long term NSAIDs may cause GI and renal toxicity – High acetaminophen doses can cause hepatotoxicity
Myth: Opioids Cause End Organ Toxicity
Respiratory and CNS toxicity have occurred with high opioid doses in opioid-naïve patients
Long term opioid therapy does not produce reported end-organ toxicity in patients who are titrated to response and monitored correctly– Long term NSAIDs may cause GI and renal toxicity – High acetaminophen doses can cause hepatotoxicity
Some Pain Management Guidelines and Statements that Advocate Opioids
for Safe and Effective Analgesia
AHCPR Acute Pain Guideline 1992 AHCPR Cancer Pain Guideline 1994 ASA Cancer Pain Guidelines 1996 AAPM-APS Opioids in Chronic Pain 1997 ASAM Public Policy Statement 1997 APS Sickle Cell Pain Guidelines 1999 APS OA and RA Pain Guideline 2001 AGS Persistent Pain in Elderly Guidelines 2002 APS Acute and Cancer Principles, 5th ed 2003

All this needless pain and suffering impoverishes the quality of life of those afflicted and their families; it may even shorten life by impairing recovery from surgery or disease. People suffering severe or unrelenting pain become depressed. They may lose their will to live and fail to take normal health preserving measures; some commit suicide.
Liebeskind J, Melzack R. Pain 1987;30:1


















