
On the CUSP: Stop CAUTI in ICU National Content Webinar 1 Today’s Topic: Defining “Critically...
33
On the CUSP: Stop CAUTI in ICU National Content Webinar 1 Today’s Topic: Defining “Critically Ill” in the ICU; Alternatives to Catheters; Using the CUSP Staff Safety Assessment and the Learning from Defects Tools to Improve Safety Culture Access slides and the audio recording of today’s webinar on the national project website: http://www.onthecuspstophai.org/on-the-cuspstop- cauti/cohort-9-icu-initiative/
-
Upload
jacob-fleming -
Category
Documents
-
view
218 -
download
1
Transcript of On the CUSP: Stop CAUTI in ICU National Content Webinar 1 Today’s Topic: Defining “Critically...

On the CUSP: Stop CAUTI in ICU National Content Webinar
1
Today’s Topic:
Defining “Critically Ill” in the ICU; Alternatives to Catheters; Using the CUSP Staff Safety Assessment
and the Learning from Defects Tools to Improve Safety Culture
Access slides and the audio recording of today’s webinar on the national project website:
http://www.onthecuspstophai.org/on-the-cuspstop-cauti/cohort-9-icu-initiative/

Webinar Evaluation
2
Your feedback is important!Please take a moment to fill out an evaluation
of today’s webinar:
http://www.cvent.com/d/xrqmmq

Today’s Presenters
Randy Garnett Jr., MD
PCCM Physician, Sentara Medical Group
Chairman, Sentara Norfolk General Critical Care Committee
Medical Director, Sentara Lung Transplant Out Patient Program
Norfolk, Virginia
Sheryl Sheriff, RN
Greenville Hospital System
Greenville, South Carolina
Emily Pasola MSN, RN, CNL
Clinical Nurse Leader
Surgical Intensive Care Unit
Saint Joseph Mercy Hospital
Ann Arbor, Michigan3

INDWELLING URINARY CATHETER USE IN THE ICUCRITICALLY ILL PATIENTS
4
Randy Garnett Jr., MDPCCM Physician, Sentara Medical Group Chairman, Sentara Norfolk General Critical Care CommitteeMedical Director, Sentara Lung Transplant Out Patient ProgramNorfolk, Virginia

ICU Characteristics(Complex Interactions, May Effect indwelling urinary catheter
Utilization)
• Medical vs. Surgical• Acuity level of patients• Arena from which patient comes from to the ICU- OR, ED,
floor SNF• Who put the indwelling urinary catheter in?• ICU culture
– RN– MD– Leadership/admin support– Other

Potentially Critical Illness Clinical Observations
• Sweaty, anxious, pale• Agitated or confused• Responds to moderate stimulation only – loud voice,
physical prodding• Accessory muscle use and RR 20-30 or RR < 8• HR > 100• SBP < 90 • UO < 0.5 ml/kg/hr
The Critically Ill Patient Clinical Observations
• Looks ill – poorly perfused • Unresponsive or poorly responsive neurologically• Resp Rates < 8 or > 30 • HR < 50 or > 150• SBP < 60 to 70• Anuric or oliguric

Critically Ill
Surgical Patient Categories who will almost always need indwelling urinary catheters:• Post op patients with continued mechanical ventilation and sedation• CSICU- CVG, Valve surgery, transplant , aortic dissections • Major abdominal GI surgery- SBO, ischemic bowel, bowel perforations, liver transplant,
abdominal compartment syndrome • Major Vascular surgery- Ruptured AAA, retroperitoneal bleeds• Most GU surgeries • Hemodynamically unstable post op patients where UO guides therapy• Immobilized patients- trauma , fractures, TBI • Post operative co-morbid processes where accurate urine output is important to monitor -
acute and chronic renal failure, CHF/CMO or low Cardiac output states, DI • Post operative delirium, agitation, encephalopathy where incontinence has a detrimental
effect on optimal care – wounds , staff safety

Critically Ill
Medical Patient Categories who will almost always needs indwelling urinary catheters:• Respiratory failure on mechanical ventilation and significant sedation• Hemodynamic instability
– Sepsis and septic shock– Hemorrhagic Shock – GI bleed, trauma, post procedural – Cardiogenic Shock
• Unstable CHF patients undergoing aggressive diuresis• Severe neurologic impairment with altered mentation- CVA,ICH,SAH, SDH,TBI• Acute or chronic renal failure with obstruction/retention• Critical illness where voiding exacerbates the primary process – COPD or CHF on
NIV

Types Of TreatmentsRequiring Close UO Monitoring
• Bolus fluid resuscitation• Vasopressors• Inotropes• High dose diuretics• Hourly urine studies to measure life threatening
laboratory abnormalities

Case #1 Indwelling urinary catheter – Yes or No?
• 24 yo presents with acute SOB with history of asthma. Acutely ill. • BP 155/95• HR 124• RR 30• EXAM:
– Oriented x 3– 2 + accessory muscle use– Diffuse wheezing bilaterally, prolonged expiratory phase– Can move from stretcher to bed without significant change in status
• ABG on 2 LNC ---- PaO2 – 87; PCO2 - 46; pH 7.36

Case #2Indwelling urinary catheter – Yes or No?
• 72 yo male 48 hrs post CVG x 3 and MVR. Still on mechanical ventilator with moderate levels of sedation and RASS of -2
• Is on moderate doses of norepinephrine and epinephrine that are being adjusted for MAP of 65-70
• Remains on 55% FiO2 and 8 PEEP• EXAM:
– Opens eyes and follows simple commands before drifting off– Lung and cardiac exam are normal– Abd is benign and extremities feel perfused
• Labs and CXR s are not concerning

Case #3Indwelling urinary catheter – Yes or No?
• 83 yo male with BPH who is post op ruptured AAA returns to ICU for post op care.
• Is extubated 2 hrs post arrival in the ICU and has moderate abd pain. • Drips: low dose Neosynephrine • VS: HR 90, BP 140/85 , RR 17. Temp 95.4• EXAM:
– Lungs clear– Heart – RRR without murmer– Abd – moderately tender– Extremities perfused– Urine out put 50 -100 cc /hr since going to the OR
• When can the indwelling urinary catheter come out?

Case #4Indwelling urinary catheter – Yes or No?
• 65 yo with moderate to severe COPD presents with acute on chronic respiratory failure to the ICU from the ED and is placed on NIV . No cardiac history.
• VS: HR 110, RR 21 with 1 + accessory muscle use, BP 125/66 , afebrile
• EXAM: – Distant breath sounds with rare wheezing and prolonged expiratory phase – Cardiac exam pertinent only for tachycardia– Abdomen is benign and extremities are adequately perfused– He is oriented x 3 , moves around in bed
• He has been supported 3 times with short term NIV in the past year without needing intubation
• ABG in 40 % and NIV : PaO2 – 72 ; PCO2 - 52 ; pH – 7.35
Indwelling Urinary Catheter Removal Protocol
Sheryl Sheriff, RN
Greenville Hospital System
Greenville, South Carolina
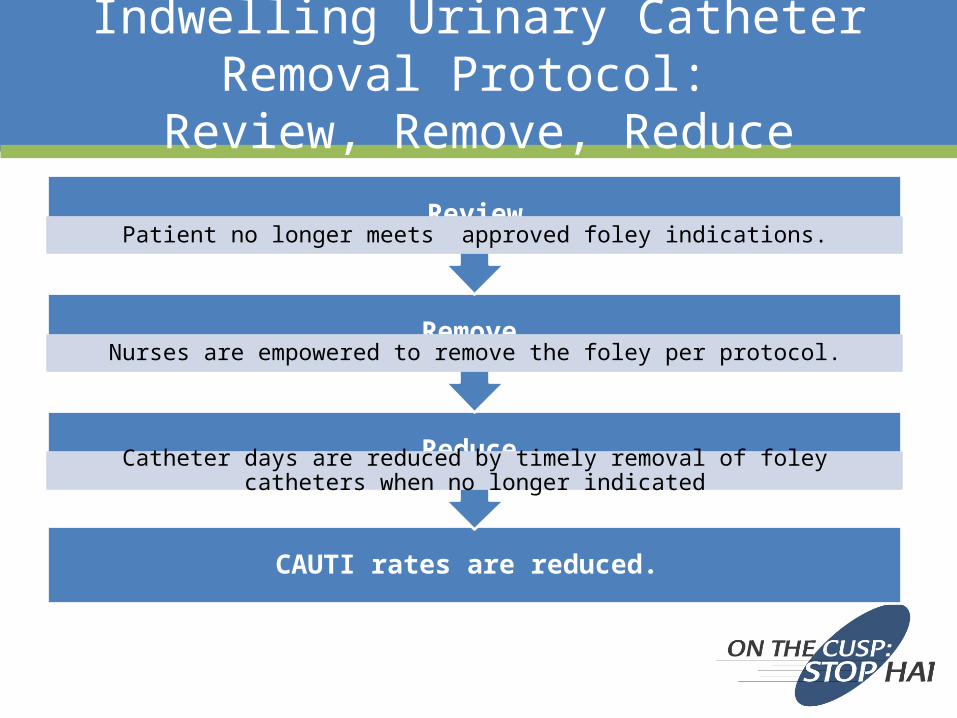
Indwelling Urinary Catheter Removal Protocol: Review, Remove, Reduce
CAUTI rates are reduced.
Reduce Catheter days are reduced by timely removal of foley catheters when no longer indicated
Remove Nurses are empowered to remove the foley per protocol.
ReviewPatient no longer meets approved foley indications.

Approved Indwelling Urinary Catheter Indications
• Ordered or placed peri-operatively for selected surgical procedures (i.e. Unstable Pelvic, Hip/Spine fracture, Renal/Urologic surgery, Gynecological Surgery, Perineal procedure)
• Accurate measurements of intake and urinary output in critically ill patients: Hemodynamic instability (requiring Pressors, shock), &/or Neuromuscular blockade (ventilated), &/or Deoxygenation with exertion or position changes (i.e. acute respiratory compromise, acute decompensated
CHF) • Epidural catheter in place for pain management and patient is unable to ambulate• Traumatic bladder and/or ureter • Acute urinary retention with failure of Urinary Retention Protocol • Bladder outlet obstruction • Gross hematuria/irrigation • Assistance in pressure ulcer healing for incontinent patients with stage 3 or 4 sacral ulcer or perineal
wound(s)• Comfort care (category 4)/hospice at patient/family request• Pre-existing Foley catheter upon admit and unable to verify Foley indication • Pre-existing Foley catheter upon admit with chronic Urological issues• Foley tagged with “yellow band” (NOTE: Yellow tag located around Foley tubing or at juncture of
tubing and bag. If Foley is tagged, do not remove without a physician’s order.)
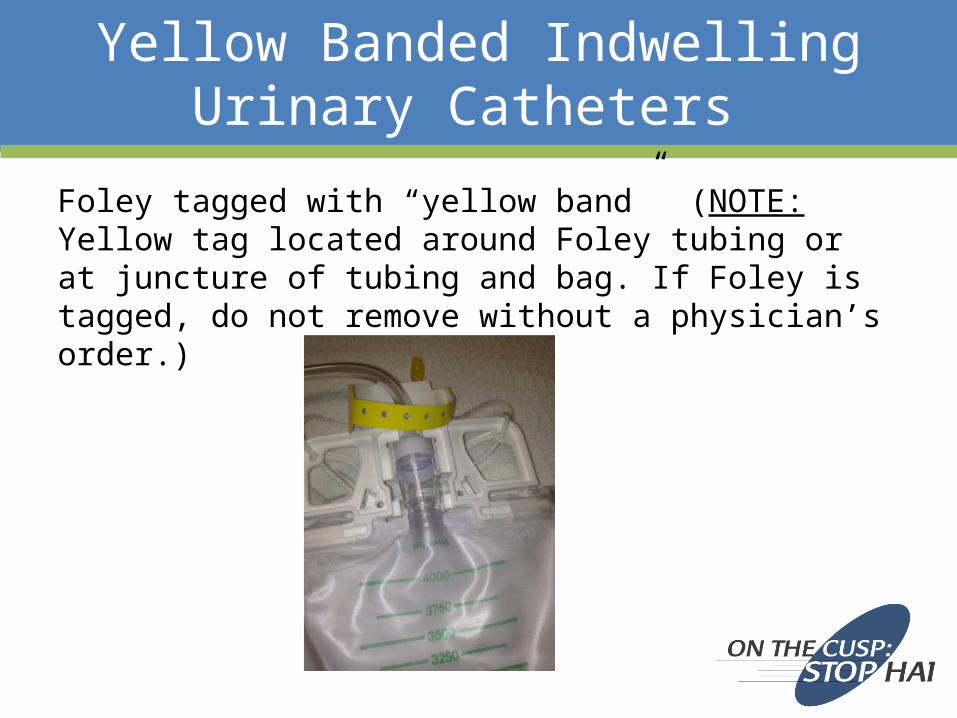
Yellow Banded Indwelling Urinary Catheters
Foley tagged with “yellow band” (NOTE: Yellow tag located around Foley tubing or at juncture of tubing and bag. If Foley is tagged, do not remove without a physician’s order.)

Fact or Fiction and Indwelling Urinary Catheters
Fiction: Any patient on Lasix or requiring accurate intake & output measurement require foley catheters – not true.
Fact: Lasix and I/O measurement are not approved indications for foleys.
• Follow the hospital approved foley indications. • Use alternatives to Foley for measurement of output.

Fact or Fiction and Indwelling Urinary Catheters in Critical Care
Fiction: All patients in critical care require a foley for accurate measurement of intake and output – not true.
Fact: Patients do not need foleys just because they are in a critical care bed.
Approved foley indications defines “Accurate measurements of intake and urinary output in critically ill patients” as:
• Hemodynamic instability (requiring pressors, shock)• Neuromuscular blockade (ventilated)• Deoxygenation with exertion or position changes (i.e. acute respiratory compromise and/or acute decompensated CHF)
Critical care patients admitted from the OR/PACU
do not automatically need a urinary catheter.

Identifying Defects andUsing the Learn From a Defect Tool
Emily Pasola MSN, RN, CNLClinical Nurse LeaderSurgical Intensive Care UnitSaint Joseph Mercy HospitalAnn Arbor, Michigan

Objectives
• Discuss strategies to identify defects• Review steps of Learn From a Defect Tool (LFD)• Discuss example using LFD
What is a defect?
HAPUSelf ExtubationInfection ControlCLABSI/CAUTI/VAEMedication ErrorRN Shift HandoffMissed DocumentationKnowledge GapEnvironmental Safety
Finding the Defects
25
• Staff feedback– Shift huddles, staff meetings
• Event reporting– Root Cause Analysis, hospital reporting system
• Quality and safety measures– Monthly data reports– Recurring gaps
• Staff Safety Assessment survey

13
Appendix C
STAFF SAFETY ASSESSMENT – CUSP
Please describe how you think the next patient in your unit/clinical area will be harmed.
Name (optional): Job Category: Date: Unit:
Please describe what you think can be done to prevent or minimize this harm.
Thank you for helping improve safety in your workplace!
Purpose of this form: The purpose of this form is to tap into your knowledge and experiences at the frontlines of patient care to find out what risks are present on your unit that have or could jeopardize patient safety. Who should complete this form: All health care providers. How to complete this form: Provide as much detail as possible when answering the 2 questions. Drop off your completed safety assessment form in the location designated by the CUSP improvement team with your job category, date and unit in the top box (name is optional). When to complete this form: Assessing safety should be considered an iterative process with no defined end (like a moving bicycle wheel). Thus, it can be filled out by any health care provider at any time. At the very least, all health care providers should complete this form semiannually.

Staff Safety Assessment
27
• What is it?
Two questions for bedside staff:– Please describe how you think the next patient in your unit/clinical area
will be harmed.– Please describe what you think can be done to prevent or minimize this
harm.• Why is it important?
– Staff engagement-driving change– Staff understanding their role in patient safety
• What should you do with the information?
– Be transparent– Identify theme– LEARN FROM IT

Learn From a Defect
Supporting a culture of safety• Easy to use
– efficient• Structured Method• Continuity• Non-punitive• Ownership
– collaborative, multidisciplinary• Improve Quality



Conclusion
• Easy, efficient & organized• Supports staff engagement
– Multidisciplinary approach to quality care• Provides transparency
– Staff want to know what we do.– Staff want to know that we listen.
• Provides structure & accountability• Tracks progress
Summary/Next Steps
• Understand the HICPAC indications for urinary catheter use, especially in the critically ill population
• Understand when catheters may be discontinued in critically ill patients
• Know what alternatives to indwelling urinary catheters are available in your organization
• Implement the Learning From Defects tool and staff safety assessment with your ICU team
Questions?
33
Your feedback is important!Please take a moment to fill out an evaluation
of today’s webinar:
http://www.cvent.com/d/xrqmmq


















