Omphalocel PPT
23
Transcript of Omphalocel PPT

OMPHALOCELEGroup 4
BSN II-E
Mr. Knudson, Torvald P.
Ms. Guillen, Felomina
Ms. Mapa, Rachel
Mr. Loquite, Samuel, Jr.
Mr. Lizardo, John Keven


DEFINITIONProtrusion at birth of part of the intestine through a large defect in the abdominal wall at the umbilicus, the protruding bowel being covered only by a thin transparent membrane composed of amnion and peritoneum.ETIOLOGYUnknown, however omphaloceles are attributed to cases of Edward’s Syndrome (Trisomy 18) and Patau Syndrome (Trisomy 13), both genetic disorders.

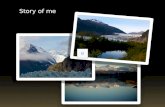
PathophysiologyBelieved to be genetic.Two typesFetal omphaloceleSmall abdominal defect < 4 cm wide with herniation of bowel into a sac of amnion that has the umbilicial vessels located at the apex of the sac. This is due to the failure in development of the periumbilical abdominal wall after the first 8 weeks of gestation.

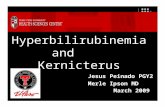
Embryonic omphaloceleUsually > 4 cm in width.Due to failure of abdominal wall closure in the
embryonic stage of development (before the 8th week).
Liver as well as bowel is herniated.Multiple anomalies are present in 50% of these
cases, such as;Congential heart defectsTrisomy 21Diaphragamatic herniaRenal anamolies

General Signs & SymptomsIn utero Alpha Fetal Protein is elevated (AFP) screening or fetal ultrasound at 16 and 32 weeks are early detection methods used.Delivery serves as visual confirmation of degree of problem.

ASSESSMENT *immediate newbornCues:-Herniated Liver-Herniated BowelsV/S; T 37.0 C, P 140, RR 40, BP 70/50, Wt 3.0 kg.

I. NURSING DXImpaired Skin Integiry; related to congenital birth defect, abdominal organ is outside abdominal wall.PLANNINGAfter 8 hours of nursing intervention the patient will have organs stabilized in position and protected from environment.

IMPLEMENTATIONNursing InterventionsWrap organ in wet sterile gauze.Rationale - Protects organ from drying.Position patient to maximize safety.Rationale - Neonate may need to have pillows or supports to minimize movement.

Monitor V/S.Rationale - Close monitoring of V/S T, P, RR, BP may indicate immediate change in health status.Prepare for immediate surgery.Rationale - Surgical intervention is indicated for small omphaloceles.Maintain asepsis.Rationale - Prevent infection.

EVALUATIONAfter 8 hours of nursing intervention, the patient will have organs stabilized in place and vital signs will be stable.

ASSESSMENTCues:-Herniated Liver-Herniated BowelsV/S; T 37.0 C, P 140, RR 40, BP 70/50, Wt 3.0 kg.

II.Nursing DXRisk for infection; related to internal organs being herniated from abdominal wall, secondary to congenital birth defect.PLANNINGAfter 8 hours of nursing intervention the patient will remain free of infection as evidenced by absence of purulent drainage from omphalocele site.

IMPLEMENTATIONNursing InterventionsIrrigate gauze and organ with room temperature saline.Rationale - Keeps gauze moist which in turn protects organ from drying.Demonstrate Wound care.Rationale - The abdomen is open and exposed to environmental pathogens.Use paper tape if needed.Rationale - Adhesive tape may be abrasive to fragile new born tissue.

Position infant in supine position.Rationale - Infant must be positioned to maximize protection of abdomen and exposed organs.Administer Antibiotics as ordered.Rationale - Antibiotic therapy to reduce risk of infection.

EVALUATIONAfter 8 hours of nursing intervention, the patient will be demonstrating no signs or symptoms indicating infection.

ASSESSMENTCues:-Herniated Liver-Herniated BowelsV/S; T 37.0 C, P 140, RR 40, BP 70/50, Wt 3.0 kg.

III. Nursing DXRisk for aspiration; related to presence of gastrointestinal tube.PLANNINGAfter 8 hours of nursing intervention the patient will experience no aspiration as evidenced by noiseless respirations, clear breath sounds, clear, odorless secrections.

IMPLEMENTATIONNursing InterventionsDetermine presence of other disorders.Rationale - Infants born with congenital defects are known to have multifactorial issues.Monitor use of oxygen tent/mask.Rationale - Neonate oxygen therapy only as needed.

Suction as needed.Rationale - To clear secretions while reducing potential for aspiration of secretions.Auscultate lung sounds frequently.Rationale - To determine presence of secretions or silent aspiration.Position infant or HOB to 30 degrees and position to right side if possible.Rationale - Upper airway patency is facilitated by upright position and turning to right side decreases likelihood of drainage into trachea.

EVALUATIONAfter 8 hours of nursing intervention demonstrate normal breathing pattern will demonstrate clear lung sounds from auscultation.

Embryonic Omphlocele

Fetal omphlocele