Olfactory Neuroblastoma
6
OLFACTORY NEUROBLASTOMA A Clinical Analysis of 17 Cases SIDNEY KADISH, MD,* MAX GOODMAN, KID,+ AND C. C. ~YANG, MD~ Seventeen patients with olfactory neuroblastoma seen at the Massachusetts General Hospital and Massachusetts Eye and Ear Infirmary from 1941 to 1971 are presented. Data on age, sex, symptoms, physical, and roentgenographic findings, and therapeutic results are evaluated. A system of pretherapy staging is proposed in which for Group A, the tumor is limited to the nasal cavity; in group B, the tumor is localized to the nasal cavity and paranasal sinuses; and in group C, the tumor extends beyond the nasal cavity and paranasal sinuses. Olfactory neuroblastoma is a radioresponsive, and, to a limited extent, radiocurable tumor and varies in aggressiveness. Of I7 patients in this series, 13 or 76% were alive without disease following treatment by surgery, irradia- tion, and combination of these two methods. Uncontrolled primary lesions with or without metastases accounted for all therapeutic failures. A treatment policy lor this disease is presented. Cancer 37:1571-1576, 1976. HE SENbE OF SMELL IS LOCATED IN A SPE- T c i a1 ized sensory neuroepithelium which covers the superior nasal turbinates and the upper portion of the nasal septum, terminat- ing in nerve filaments that collect into bun- dles and pass the cribiform plate of the eth- moitl bone to synapse with neuronal processes of the olfactory bulb. Malignant tumors of this neuroepithelium rarely occur and the first tumors recogniietl as originating from this epithelium were termed “esthesioneuroepithe- lionie olfactil” by Berger, Luc, and Richard in 1924.3 The first report of this entity in the English language literature was by Schall and From the Departments of Radiation Medicine and Pathology, Massachusetts General Hospital and Massa- chwelts Eye arid Ear Infirmary, Boston, Massachusetts, :ind the Department of Radiation Therapy and Pa- thology, Harvard Medical School, Boston, Massa- ch use l t S. * Director of Radiation Oncology, St. Vincent Hos- pital, Worcester, Massachusetts. t Associate Pathologist, Massachusetts General Hos- pital, and Pathologist, Massachusetts Eye and Ear Infirmary. .4ssociate Professor of Pathology, Harvard bfedical School. t Radiotherapist and Head, Division of Clinical Services, Department of Radiation Medicine, hfassa- chuselts General Hospital. Professor of Radiation Therapy, Harvard Medical School. Address for reprints: Dr. C. C. Wang, Department of Radiation Medicine, Massachusetts General Hospital, Boston, MA 0211.1. Lineback’s at the hIassachusetts Eye and Ear Infirmary in 1951, when they described three cases of “primary intranasal neuroblastoma.” A total of 104 cases have been reported in the world’s literature. Owing to the rarity of this neoplasm, no single physician or institution has accumulated a broad experience in the therapeutic management of patients with this tumor. Histological criteria used to identify olfac- tory neuroblastoma from undifferentiated carcinoma and other intranasal malignancies are: neuroepithelial cells arranged in pseudo- rosettes; a surrounding stroma composed of undifferentiated nuclei and fibrillar cords; marked microvascularity, with palisading of neuroepithelial cells around blood vessels; a conspicuous absence of mitotic figures; oc- casional interstitial calcification; and finally, a basic similarity to adrenal or sympathetic ganglionic neuroblastoma and retinoblas- toma1.8.11 (Fig. 1). At the Massachusetts General Hospital and Massachusetts Eye and Ear Infirmary, 17 pa- tients with histologically proven olfactory neuroblastoma were seen between 1941 and 197 1. These cases, including the original three patients described by Schall and Lineback,l6 constitute the material of this report. This paper concerns a review of data on age, sex, symptomatology, physical and roent- genographic findings, and results of treatment 1571
-
Upload
talia-lizardi -
Category
Documents
-
view
3 -
download
0
description
A
Transcript of Olfactory Neuroblastoma

OLFACTORY NEUROBLASTOMA A Clinical Analysis of 17 Cases
SIDNEY KADISH, MD,* MAX GOODMAN, KID,+ AND C. C. ~ Y A N G , M D ~
Seventeen patients with olfactory neuroblastoma seen a t the Massachusetts General Hospital and Massachusetts Eye and Ear Infirmary from 1941 to 1971 are presented. Data on age, sex, symptoms, physical, and roentgenographic findings, a n d therapeutic results are evaluated. A system of pretherapy staging is proposed i n which for Group A, the tumor is limited to the nasal cavity; i n group B, the tumor is localized to the nasal cavity and paranasal sinuses; and in group C, the tumor extends beyond the nasal cavity and paranasal sinuses. Olfactory neuroblastoma is a radioresponsive, and, to a limited extent, radiocurable tumor and varies i n aggressiveness. Of I7 patients i n this series, 13 or 76% were alive without disease following treatment by surgery, irradia- tion, and combination of these two methods. Uncontrolled primary lesions with or without metastases accounted for all therapeutic failures. A treatment policy lor this disease is presented.
Cancer 37:1571-1576, 1976.
HE SENbE OF SMELL I S LOCATED IN A SPE-
T c i a 1 ized sensory neuroepithelium which covers the superior nasal turbinates and the upper portion of the nasal septum, terminat- ing in nerve filaments that collect into bun- dles and pass the cribiform plate of the eth- moitl bone to synapse with neuronal processes of the olfactory bulb. Malignant tumors of this neuroepithelium rarely occur and the first tumors recogniietl as originating from this epithelium were termed “esthesioneuroepithe- lionie olfactil” by Berger, Luc, and Richard i n 1924.3 The first report of this entity in the English language literature was by Schall and
From the Departments of Radiation Medicine and Pathology, Massachusetts General Hospital and Massa- chwelts Eye arid Ear Infirmary, Boston, Massachusetts, :ind the Department of Radiation Therapy and Pa- thology, Harvard Medical School, Boston, Massa- ch use l t S.
* Director of Radiation Oncology, St. Vincent Hos- pital, Worcester, Massachusetts.
t Associate Pathologist, Massachusetts General Hos- pital, and Pathologist, Massachusetts Eye and Ear Infirmary. .4ssociate Professor of Pathology, Harvard bfedical School.
t Radiotherapist and Head, Division of Clinical Services, Department of Radiation Medicine, hfassa- chuselts General Hospital. Professor of Radiation Therapy, Harvard Medical School.
Address for reprints: Dr. C. C. Wang, Department of Radiation Medicine, Massachusetts General Hospital, Boston, MA 0211.1.
Lineback’s at the hIassachusetts Eye and Ear Infirmary in 1951, when they described three cases of “primary intranasal neuroblastoma.” A total of 104 cases have been reported in the world’s literature. Owing to the rarity of this neoplasm, no single physician or institution has accumulated a broad experience in the therapeutic management of patients with this tumor.
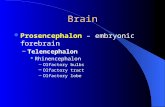
Histological criteria used to identify olfac- tory neuroblastoma from undifferentiated carcinoma and other intranasal malignancies are: neuroepithelial cells arranged in pseudo- rosettes; a surrounding stroma composed of undifferentiated nuclei and fibrillar cords; marked microvascularity, with palisading of neuroepithelial cells around blood vessels; a conspicuous absence of mitotic figures; oc- casional interstitial calcification; and finally, a basic similarity to adrenal or sympathetic ganglionic neuroblastoma and retinoblas- toma1.8.11 (Fig. 1).
At the Massachusetts General Hospital and Massachusetts Eye and Ear Infirmary, 17 pa- tients with histologically proven olfactory neuroblastoma were seen between 1941 and 197 1. These cases, including the original three patients described by Schall and Lineback,l6 constitute the material of this report.
This paper concerns a review of data on age, sex, symptomatology, physical and roent- genographic findings, and results of treatment
1571

1572 CANCER March 1976 VOl. 37
of the primary as well as the recurrent disease, with a minimum follow-up of 3 years.
Staging was made on clinical grounds, in- cluding presenting symptoms, physical find- ings, and roentgenographic changes. The le- sions were separated into three anatomic groups as follows: Group A, tumor confined to nasal cavity, seven patients; Group B, tu- mor involved nasal cavity and paranasal sinuses, five patients; and Group C, tumor spread beyond the nasal cavity and paranasal sinuses, five patients.
Seven patients were males (41y0) and 10 were females (59y0). Ages ranged from 3 years to 77 years, with a mean age of 41.4 years. For Group A patients, the mean age was 43.1 years; Group B, 49.8 years; and Group C, 30.4 years. The relative youth of the C Group ap- pears to be significant, suggesting a more virulent form of tumor in the younger age patients.
The presenting symptoms are common, non- specific indicators of intranasal neoplasms. The most frequent symptom was unilateral nasal obstruction, occurring in 12 of 17 pa- tients or 70y0. Seven patients (41Y0) had epistaxis, four of whom had an accompany- ing nasal obstruction. Other symptoms were rhinorrhea (two patients) and sinus pain (four patients). Many patients had several of these
FIG. 1 . Photomicro- graph of olfactory neuroblastoma show- ing vascularity and neuroblastoma cells (x370).
symptoms and Group A and Group B had similar symptomatology.
Orbital symptoms occurred in Group C patients and consisted of proptosis in one, retrobulbar pain in one, blurred vision in three, and sudden blindness in one. Symp- tomatic evidence of disease extending beyond the nasal cavity and paranasal sinuses were unilateral earache with tumor extension to the nasopharynx causing obstruction of the eustachian tube orifice in one, a palpable neck mass suspicious of cervical lymph node me- tastases in one, and a 30-pound weight loss in another.
Physical findings consisted of an intranasal mass in Group A and Group B patients. In Group C patients, in addition to intranasal masses, four of the five patients had orbital signs, three had sixth nerve palsy, and two had unilateral papilledema. Other findings in a single patient included partial third nerve palsy, optic nerve palsy, proptosis, nasopharyn- geal mass, and a palpable cervical node.
ROENTGENOGRAPHIC FINDINGS
Roentgenographic features of olfactory neuroblastoma are unilateral intranasal and paranasal soft tissue mass, with or without focal calcifications, mucosal thickening or

No. 3 OLFACTORY NEUROBLASTOMA * Kadish et al . 1573
opacity of the paranasal sinuses, and/or bone destruction of the nasoantral or orbital walls.
In 15 patients with roentgenographic find- ings recorded, a mass was seen within the nasal cavity. Two of these had focal calcifica- tions which were confirmed histologically. Findings suggestive of sinusitis were seen in patients from all three groups and did not correlate with symptoms of sinus pain.
Six patients in Groups B and C had soft tissue masses in the paranasal sinuses. T h e ethmoidal and maxillary sinuses were most frequently involved.
Bone destruction, best visualized in lanii- nograms, indicates the presence of extensive tumor. In Group B, two patients had erosion of the medial wall of the maxillary sinus, one with concomitant erosion of the anterior wall of the sphenoid sinus, and one with ethmoidal bone destruction. In Group C, four patients had bone destruction, including three with loss of the ethmoid orbital lamina and one with erosion of the sella turcica and sphe- noidal planum. All three patients with orbital signs and symptoms had roentgenographic evidence of bone destruction.
Selective arteriograms and C T scans (com- puted tomography) have been used recently and were found to be extremely useful in evaluating the possibility of intracranial ex- tension of tumor.
TREATMENT
Treatment of this group of patients varied, consisting of surgery, radiation therapy, and a combination of these two methods. Table 1 summarizes the treatment methods and the follow-up information of various groups of patients.
Radiotherapeutic methods and modalities used have varied over the past 30 years. Pa- tients treated by irradiation before the mid- 1950s received low doses of orthovoltage radia- tion or intracavitary radium packing. Patients after the mid-1950s were treated exclusively with megavoltage radiation using high doses and wedge and/or multiple portal techniques which were designed to deliver homogeneous irradiation.
Surgical procedures were lateral rhinotomy with tumor excision, ethmoidectomy, sphe- noidectomy, and subtotal maxillectomy de- pending upon the tumor extent. For maxil- lary lesions, a Caldwell-Luc procedure was commonly done to establish an oroantral
fistula to promote sinus drainage prior to radiation therapy.
RESULTS
T h e survival status is shown in Table 2. Of the entire group of 17 patients, 13 or 76q0 showed no evidence of disease for 3 or more years after therapy. Of seven patients having limited lesions within the nasal cavity (Group A), all survived without disease, five following surgery, one, irradiation, and one, combined radiotherapy a n d , surgery. Of five patients with lesions limited to the nasal cavity and paranasal sinuses (Group B), four were with- out disease, two following surgery and two following combined treatment; one died with uncontrolled primary disease. Of five patients with extensive disease, with tumor extending beyond the sinuses (Group C), only two sur- vived lor 3 or more years.
Recurrent disease at the primary site oc- curred in four of eight patients treated by surgery alone. Of these recurrences, two were subsequently salvaged by radiation therapy and two by lurther surgical resection. Four patients were treated exclusively by radiation therapy, three with extensive disease (Group C) and one belonging to Group A; only one survived without disease. Of the five patients treated by combined radiotherapy and sur- gery, four survived without disease, one of whom had local recurrence subsequently treated by further radiation therapy and was without disease for 3 or more years.
T h e time interval between the initial treat- ment and recurrences varied from 1 to 78 months, and the mean time for first recur- rence was 18 months. Of all the four ther- apeutic failures, all died with local, uncon- trolled primary, one patient also had distant metastases.
Only one patient developed a major radia- tion complication from high dose orthovolt- age irradiation to the eye which resulted in radiation phthisis bulbi which required enu- cleat ion.
DISCUSSION
The rarity of olfactory neuroblastoma pre- cludes prospective therapeutic trials, so that guidelines to its management can only be found in anecdotal case reports.
Seaman,I7 in 1951, reviewed 10 reported cases of olfactory neuroblastoma and pre-

1574 CANCER March 1976 VOl. 37
TABLE 1. Treatment and Survival Status of Olfactory Neuroblastoma Patients
Patient Ape Sex Primary therapy FoIIow-u~ Re marks
D.P.
’4.1..
l..D.
J.W.
E.N.
A.R.
F.G.
1.K.
M .w
V.D.
L.1..
F.N.
B.C. A . R .
D.ni
L.D.
I..C.
49
51
49
.z 8
3 6
57
22
20
75
39
77
38
-3 52
18
28
51
F
M
nf F
h l
F
F
F
F
M
F
F
hl M
M
F
F
Group A-Trimor Confined to Nasal Cavity
Group B-Tumor Involving Nasal Cavity and Paranasal Sinrises
9/71-Combined irradiation (5000 rads) and surgery 5/71--Radiation therapy (5300 rads) 7/70--Lateral rhinotomy and excision of tumor 3/7O--Lateral rhinotomy, excision, and subtotal maxillectomy
NED-31 yr
NED-31 yr
NED--4; yr
NED--4; yr
2j64-LateraI rhinotomy and excision of tumor 2/50-I.ateral rhinotomy and ethnioidectomy
2 /48--Ethnioidectomy
NED-61 yr
NED-32 yr after initial surgery, died of carcinoma of esophagus. NED---26 yr
No tumor in postirradiation specimen
6/71--Recurrence right medial orbit, treated by radiation therapy, 4500 rads, NED. In 1/74, developed massive R cervical metastases, treated by combined preoperative radiotherapy and neck dissection, as of 12/75 N E D
1,ocal reciirrence 5 months after surgery, treated by radium packing, -4000 mg/hr.
Had “some x-ray treatments cf unknown amount,” prior to surgery. Treatment did not help.
10/71--I..ateral rhinotomy and resection of tumor 5 / 7 1 -Combined preoperative irradiation (5000 rads) and lateral rhinotomy and maxillectomy 11/67-Combined lateral rhinotomy and resection of tumor and postoperative irradiation (6000 rads) 6/47--Lateral rhinotomy, Pthmoidectomy, and sphenoidec tomy 1 /41-Combined resection of tiimor, and postoperative radium packing and external radiation therapy (6000 rads given dose, 200 kV)
NED-3 yr
NED--3; yr
DOD-I yr
NED-I0 yr, died at age 87 of cerebral hemorrhage NED-22 yr, died of intercurrent disease
Group C-Tumor Extending Beyond Nasal Cavity and 5/7 1 -Radiation therapy 9/6CiCombined preoperative NED--8 yr Irradiation (2000 rads) and lateral rhinotomy with excision of tumor
DOD-I3 mo
7/6I--Lateral rhinotomy and NED--13 yr resection of tumor
6/59-External radiation Don-: yr therapy
1 /55--External radiation DOD-l/6 yr therapy
No residrial tiinior in post- radiation resected specimen
ITncontrolled local disease
Had local recurrence 6 f years after initial siirgery. Treated hy further excision through lateral rhinotomy. Reciirrence 1 years after initial treatment and received further external irradiation.
Paranasal Sinuses Primary lesion uncontrolled. 11/66--left radical neck dissection for metastases and external irradia- tion for metastases in left parotid and buccal areas. 6/67-right radical neck dissection for cervical metastases. 7/62-Fiirther resection for reciir- rence. 1966-Orbital exenteration for local recurrence. Had cervical nodal metastases. Died of uncontrolled primary and metastases. Primary trinior iincoiitrolled.
. _
Key: NED-No evidence of disease DOD-Died of disease (carcinoma).

No. 3 OLFACTORY NEUROBLASTOMA * Kadish et 01. 1575
‘r.4~1.z 2. Three-Year NED Following Treatment of Olfactory h’euroblastonu: MGH and MEEI Experience (1911-1971)
Combined irradia- Treatment methnd Surgery Irradiation tion & surgery TOTAI
Group A 5 / 5 * 111 111 717 (100%) Group B 2/2t - 2 13s 41s (80%) Group C 111’ 013 1/1 215 (40%)
‘rOTAL 8 / 8 (100%) 114 (25%) - 415 (80%) 13/17 (76%)
* Two recurrences, salvaged by irradiation. t One recurrence, salvaged by further surgery.
One recurrence, salvaged hy further irradiation.
5ented one of his own; he noted that each case had an excellent response to radiation therapy. Becker and Jacox2 reported five cases i n 1964, four of whom received radiation therapy with good results; they advocated high dose radiation therapy after surgical ex- cision of the tumor. Other a~thors~3.14 urging a similar treatment approach include Fitz- hugh et al.,5 Schenk and Ogura,’B Dibble and Brown,4 Ash et al.1 and Fruhling and Wild.6 MacComblO suggested treatment primarily by radiation therapy followed by limited surgery if necessary.
Fitzh~igh5 reported two patients without tumor regression after cancerocidal doses of megavoltage radiation therapy. Grahne7 re- ported one patient with slight tumor regres- \ion after irradiation and marked tumor re- gression after thioTEPA chemotherapy. Obertl’ reported eight cases of olfactory neu- roblastoma, seven of whom had documented recurrences following surgery and radiation therapy, although radiation techniques con- sisted of low dose kilovoltage or intracavitary radium. Lewis et al.9 commented on the vari- ability in radiosensitivity in the 18 cases they liad treated and suggested that neither radio- therapy nor surgery, nor their combination was successful in controlling this tumor.
T h e present review emphasizes the need for classification of lesions into various stages of disease progression. Such classification permits the original management decision to be based on a reasonable expectation of outcome. None of the previous published reports on this tumor endeavored to stage their reported cases and consequently, these reports failed to dis- tinguish between curative and palliative treat- ment regardless of modality. Because the most iavorable early cases have been traditionally managed by surgery, an inherent bias against the use of radiation therapy in the manage-
ment of olfactory neuroblastoina is quite evi- dent in the literature.
T h e efficacy of radiation therapy, however, in controlling olfactory neuroblastoma is be- yond doubt. T h e patients with tumors of limited extent in this series were in apparent remission following high close megavoltage irradiation alone and/or in combination with surgery. In addition, local recurrences follow- ing surgical treatment were effectively con- trolled by irradiation. Also, in two patients, the resected specimens showed no histologic evidence of residual tumor following a dose of 4500 rads. Our data, therefore, have con- firmed the radioresponsiveness and radio- curability of this tumor.
It is possible that tumor confined to the nasal cavity (Group A) may be to a large extent curable either by surgery or by radia- tion therapy. Following surgical resection, the local recurrence rate is high. Therefore, we recommend therapeutically for this disease a combined approach using radiation therapy and surgery. For lesions limited to the nasal cavity and/or paranasal sinuses (Groups A and B), preoperative radiation therapy of 5000-rad megavoltage radiation should be given in 5 to 6 weeks followed by surgical resection. Patients with tumor extending be- yond the nasal cavity and sinuses, i.e., Group C , often considered to be inoperable, should receive high dose radiation therapy of 6000 to 6500 rads in 7 weeks followed by surgical resection of residual disease if operable. Since the incidence of cervical lymph node metas- tases is low-3/17 or less than 20~o-elective neck irradiation or dissection does not appear to be indicated. T h e presence of cervical meta- static nodes, however, should be dealt with best by preoperative radiation therapy and neck dissection.

1576 CANCER Mnrch 1976
ADDENDUM
Since 1971, two addilional cases of olfactory neuroblastoma hare been seen. The first one was an 18-year-old femalc with a Group C tumor and extensive ipsilateral cervical lymph node metastases, unsuccessfully treated by radiation therapy, who succumbed to distant metastases to the liver and abdominal lymph nodes. The second case was a 65-year-old male, with a Group C lesion currently treated with radiation therapy.
Vol. 37
REFERENCES
1. Ash, J . E., Beck, M. R., and TVilkcs, J. D.: T u - mors of the upper respiratory tract and ear. In Atlas of Tumor Pathology, Sect. IV, Fasc. 12 and 13. Wash- ington, DC, Armed Forces Institute of Pathology,
2. Becker, M. H., and Jacox, H. \V.: Olfactory esthesioneurocpithelioma. Radiology 82:77-83, 1964.
3. Berger, L., Luc, and Richard.: L’esthesioneuro- cpitlieliome olfactif. Bull. Asoc. Franc. P o w I’Etride Cntrcer 13:41(1-420, 1924.
4. Dibble, P. A., and Brown, A. K.: Esthesioneuro- epithelioma. Lalyngoscope 71:192-199, 1965.
5 . Fitzliugh, G. S., Allen, M. S., Jr., Rucker, T . N., and Sprinkle, P. M.: Olfactory ncuroblastoma (esthesio- tieuroepithelioma). Arch. Otolatyiigol. 81: 161-168, 1965.
6. Fruhling, L., and Wild, C.: Olfactory esthesio- neuroepithelioma of Louis Berger. Arch. Ololaryngo!. 60:3748, 1954.
7. Grahne, B.: Olfactory neuroblastoma. Acta Oto- Inrytzgol. 60:37-48, 1954.
7. Grahne. B.: Olfactory neuroblastoma. Acta Oto- laryiigol. 59:55-64, 1965.
8. Hutter, R. V. P., Lewis, J. S., Foote, F. W., Jr., and Tollefsen, H. R.: Esthesioneuroblastoma-A clin- ical antl pathological study. Aii i . J. Surg. 106:748-753, 19ti3.
9. Lewis, J. S., Huttcr, R. V. P., Tollefsen, H. R.,
1964; p. 79.
antl Foote, 1;. W., Jr.: Nasal tumors of olfactory origin. Arclr . Otolaryngol. 81 :169-174, 1965.
10. MaComb, W. S.: Miscellancous tumors-Esthesio- neuroepithelioma. In Cancer of the Head and Neck. Chap. 15. Baltimore, Williams and Wilkins Co., 1967;
11. Mcndeloff, J.: T h e olfactory nenroepithelial tu- mors. Cancer 10944-956, 1957.
12. Obert, G. H., Devine, K. D., and McDonald. J. R.: Olfactory neuroblastomas. Cancer 13:205-215, 1960.
13. Riemcnschneider, P. 4 . , and Prior, J . T.: Neui-o- blastoma originating from olfactory epithelium (eathe- sioneuroblastoma). A m . J. Roentgeiiol. Radiuru T h e r . Nuc l . illed. 80:759-756, 1958.
14. Robinson, E., ant1 Solitare, G. B.: Olfactory neuroblastoma-Neurosurgical implications of an in- tranasal tumor. J . Neurosurg. 25:133-139, 1966.
15. Schall, L. A, , and Lineback, hl.: Primary intra- nasal neuroblastoina. Ann. Otolaryngol. 60:221-229, 1951.
16. Schenk, N. L., and Ogura, J. H.: Esthesioneuro- blastonia-An enigma in diagnosis, a dilemma in treat- ment. Arch. Otolaryngol. 96:322-324, 1972.
17. Seaman, W. B.: Olfactory esthesio-neuroepithe- liomas. Radiology 57:541-546, 1951.
pp. 447-451.