Old Order Amish
8
Am. J. Hum. Genet. 57:636-643, 1995 Linkage Analyses of Chromosome 18 Markers Do Not Identify a Major Susceptibility Locus for Bipolar Affective Disorder in the Old Order Amish David L. Pauls,' Jurg Ott,2 Steven M. Paul,3'4 Cleona R. Allen,5 Cathy S. J. Fann,2 John P. Carulli,6 Kathleen M. Falls,6 Christine A. Bouthillier,6 Thomas C. Gravius,6 Tim P. Keith,6 Janice A. Egeland,5 and Edward 1. Ginns3 'Child Study Center, Yale University School of Medicine, New Haven; 2Columbia University and New York State Psychiatric Institute, New York; 3Clinical Neuroscience Branch, IRP, National Institute of Mental Health, Bethesda; 4Lilly Research Laboratories, Indianapolis; -Department of Psychiatry, University of Miami, Miami; and 6Genome Therapeutics Corporation, Waltham Summary Previously reported linkage of bipolar affective disorder to DNA markers in the pericentromeric region of chro- mosome 18 was reexamined in a larger homogeneous sample of Old Order Amish families. Four markers (D18S21, D18S53, D18S44, and D18S40) were exam- ined in three kindreds containing 31 bipolar I (BP I) individuals. Although linkage findings were replicated in the one previously studied Amish pedigree containing four BP I individuals, linkage to this region was excluded in the larger sample. If a susceptibility locus for bipolar disorder is located in this region of chromosome 18, it is of minor significance in this population. Introduction A genetic etiology for bipolar affective disorder is strongly supported by family, twin, and adoption stud- ies. However, there is not consensus on the specific ge- netic mechanisms that account for the transmission of the illness within families. Several studies have suggested that some forms of bipolar affective disorder are X- linked (Risch et al. 1986; Pekkarinen et al. 1994). It is clear that not all bipolar illness is X-linked, because of the high rate of male-to-male transmission (Hebebrand and Hennighausen 1992). Early pedigree analyses of families collected through bipolar probands provided evidence for vertical transmission, although in general results were not consistent with single locus Mendelian inheritance (Leckman and Gershon 1977; Bucher and Elston, 1981; Bucher et al. 1981; Tsuang et al. 1985). More recent studies (Rice et al. 1987; Spence et al. 1993; Pauls et al., in press) suggest that the mode of transmis- Received January 18, 1995; accepted for publication May 31, 1995. Address for correspondence and reprints: Dr. David L. Pauls, Child Study Center, Yale University School of Medicine, 230 South Frontage Road, New Haven, CT 06510-8009. X 1995 by The American Society of Human Genetics. All rights reserved. 0002-9297/95/5703-0013$02.00 sion for bipolar I affective disorder (BP I) alone is consis- tent with an autosomal dominant mode of inheritance. Again, however, the findings are not consistent across all families studied (Sham et al. 1991). Despite difficulty in understanding the complex inher- itance patterns of bipolar disorder, a number of genetic linkage studies have attempted to identify a single gene of major effect (Nurnberger 1993). Initially, there were reports of linkage to markers near the color-blindness locus on the X chromosome (Risch et al. 1986). In 1987, Egeland and colleagues reported strong evidence for linkage of a susceptibility locus for bipolar disorder to markers on 11pl5 (Egeland et al. 1987). Unfortunately, there have been no replications of this finding in other pedigrees, and subsequent analyses of additional pedi- gree data from the Old Order Amish population sug- gested that, if there is a locus on 11p1S, it is not the only locus conferring risk for affective disorder in this population (Kelsoe et al. 1989). A number of other in- vestigators have reported negative results for other re- gions of the genome (Pauls et al. 1991; Ginns et al. 1992; Baron et al. 1993; Coon et al. 1993; Gejman et al. 1993). It is worth noting that each of these studies reported a few moderately positive lod scores for some markers, but none were statistically significant. Finally, a chromosome 21q22.3 locus has been suggested to be linked to bipolar affective disorder in one family (Straub et al. 1994), although no other studies have replicated that result. Recently, Berrettini et al. (1994) reported linkage of a bipolar susceptibility locus to a region near the centro- mere of chromosome 18, using 22 families ascertained through a bipolar proband. When all pedigrees were included in the estimation of the lod score, this region of chromosome 18 could be excluded, assuming either dominant or recessive inheritance. Although a test for heterogeneity was not significant, several of the kindreds showed positive scores to some, albeit different, markers in the pericentromeric region of 18. Using the affected sib-pair (ASP) and affected pedigree member (APM) 636
Transcript of Old Order Amish

Am. J. Hum. Genet. 57:636-643, 1995
Linkage Analyses of Chromosome 18 Markers Do Not Identify a
Major Susceptibility Locus for Bipolar Affective Disorder in theOld Order AmishDavid L. Pauls,' Jurg Ott,2 Steven M. Paul,3'4 Cleona R. Allen,5 Cathy S. J. Fann,2 John P. Carulli,6Kathleen M. Falls,6 Christine A. Bouthillier,6 Thomas C. Gravius,6 Tim P. Keith,6 Janice A. Egeland,5and Edward 1. Ginns3
'Child Study Center, Yale University School of Medicine, New Haven; 2Columbia University and New York State Psychiatric Institute, New York;3Clinical Neuroscience Branch, IRP, National Institute of Mental Health, Bethesda; 4Lilly Research Laboratories, Indianapolis; -Department ofPsychiatry, University of Miami, Miami; and 6Genome Therapeutics Corporation, Waltham
Summary
Previously reported linkage of bipolar affective disorderto DNA markers in the pericentromeric region of chro-mosome 18 was reexamined in a larger homogeneoussample of Old Order Amish families. Four markers(D18S21, D18S53, D18S44, and D18S40) were exam-ined in three kindreds containing 31 bipolar I (BP I)individuals. Although linkage findings were replicatedin the one previously studied Amish pedigree containingfour BP I individuals, linkage to this region was excludedin the larger sample. If a susceptibility locus for bipolardisorder is located in this region of chromosome 18, itis of minor significance in this population.
Introduction
A genetic etiology for bipolar affective disorder isstrongly supported by family, twin, and adoption stud-ies. However, there is not consensus on the specific ge-netic mechanisms that account for the transmission ofthe illness within families. Several studies have suggestedthat some forms of bipolar affective disorder are X-linked (Risch et al. 1986; Pekkarinen et al. 1994). It isclear that not all bipolar illness is X-linked, because ofthe high rate of male-to-male transmission (Hebebrandand Hennighausen 1992). Early pedigree analyses offamilies collected through bipolar probands providedevidence for vertical transmission, although in generalresults were not consistent with single locus Mendelianinheritance (Leckman and Gershon 1977; Bucher andElston, 1981; Bucher et al. 1981; Tsuang et al. 1985).More recent studies (Rice et al. 1987; Spence et al. 1993;Pauls et al., in press) suggest that the mode of transmis-
Received January 18, 1995; accepted for publication May 31, 1995.Address for correspondence and reprints: Dr. David L. Pauls, Child
Study Center, Yale University School of Medicine, 230 South FrontageRoad, New Haven, CT 06510-8009.X 1995 by The American Society of Human Genetics. All rights reserved.0002-9297/95/5703-0013$02.00
sion for bipolar I affective disorder (BP I) alone is consis-tent with an autosomal dominant mode of inheritance.Again, however, the findings are not consistent acrossall families studied (Sham et al. 1991).
Despite difficulty in understanding the complex inher-itance patterns of bipolar disorder, a number of geneticlinkage studies have attempted to identify a single geneof major effect (Nurnberger 1993). Initially, there werereports of linkage to markers near the color-blindnesslocus on the X chromosome (Risch et al. 1986). In 1987,Egeland and colleagues reported strong evidence forlinkage of a susceptibility locus for bipolar disorder tomarkers on 11pl5 (Egeland et al. 1987). Unfortunately,there have been no replications of this finding in otherpedigrees, and subsequent analyses of additional pedi-gree data from the Old Order Amish population sug-gested that, if there is a locus on 11p1S, it is not theonly locus conferring risk for affective disorder in thispopulation (Kelsoe et al. 1989). A number of other in-vestigators have reported negative results for other re-gions of the genome (Pauls et al. 1991; Ginns et al.1992; Baron et al. 1993; Coon et al. 1993; Gejman etal. 1993). It is worth noting that each of these studiesreported a few moderately positive lod scores for somemarkers, but none were statistically significant. Finally,a chromosome 21q22.3 locus has been suggested to belinked to bipolar affective disorder in one family (Straubet al. 1994), although no other studies have replicatedthat result.
Recently, Berrettini et al. (1994) reported linkage ofa bipolar susceptibility locus to a region near the centro-mere of chromosome 18, using 22 families ascertainedthrough a bipolar proband. When all pedigrees wereincluded in the estimation of the lod score, this regionof chromosome 18 could be excluded, assuming eitherdominant or recessive inheritance. Although a test forheterogeneity was not significant, several of the kindredsshowed positive scores to some, albeit different, markersin the pericentromeric region of 18. Using the affectedsib-pair (ASP) and affected pedigree member (APM)
636

Pauls et al.: Bipolar Disorder and Chromosome 18
methods, these investigators observed evidence for link-age to varying loci in this region. One of the kindredsthat showed a lod score >1.0 for a dominant modelwas the "right extension" of the large Old Order Amishkindred 110 (Kelsoe et al. 1989).We now report our effort to determine whether the
findings reported by Berrettini et al. could be extendedto the entire sample of Amish kindreds being used forsystematic mapping studies (Keith et al. 1991; Ginns etal. 1992). Our analyses of the right-extension pedigreeconfirmed the positive lod scores reported by Berrettiniet al. However, the lod scores in the larger sample ofAmish kindreds were all negative for markers in thisregion of chromosome 18, using both dominant andrecessive genetic models. Moreover, in contrast to thefamilies studied by Berrettini et al., neither ASP norAPM analyses of the entire Amish sample supportedthe presence of a susceptibility locus in this region ofchromosome 18.
Methodology
Clinical Evaluation and Description of FamiliesEach individual in the Old Order Amish pedigrees
was interviewed using the Schedule for Affective Disor-ders and Schizophrenia-Lifetime (SADS-L) (Endicottand Spitzer 1978). Hospital and outpatient office re-cords were obtained for patients. Family members andsignificant others were also interviewed about the pa-tient using the SADS-L (Egeland et al. 1990). After themedical records were abstracted and SADS-L interviewswere collated, the materials were reviewed by a diagnos-tic panel composed of four psychiatrists and a clinicalpsychologist who assigned diagnoses on the basis of re-search diagnostic criteria (RDC) (Spitzer et al. 1978).This board also provided a clinical consensus, using allsources of available information on patient cases (Hos-tetter et al. 1983). The diagnostic panel was kept blindwith respect to biological relationship and research sta-tus, including genotyping. Blindness is maintained bymixing community cases of mental illness with thosefrom the families being genotyped. All persons in thebipolar pedigrees used for this linkage study have beenfollowed annually. Updates on the clinical status of sub-jects have been processed using the same diagnostic pro-cedures described above.The diagnoses of the 205 individuals on whom geno-
typing is performed are shown in table 1. There are onlyfour BP I individuals in the right extension; the portionof Old Order Amish pedigree 110 included in the analy-ses of Berrettini et al. (1994). There are 27 BP I subjectsin the additional Amish pedigrees used in the currentanalyses. There is one individual in the right extensionwith a BP II diagnosis and seven in the expanded sample.Three individuals in the right extension have a diagnosis
of recurrent major depressive disorder (MDD), whilethere are 12 in the remaining linkage kindreds. Individu-als with single episodes ofMDD were treated as "pheno-type unknown," as were relatives with other psychiatricdisorders, minor spectrum illness, and those who wereunaffected.
Cell CollectionThe cell collection for the Amish Study is based pri-
marily at the National Cell Repository at the CoriellInstitute of Medical Research (CIMR) in Camden, NewJersey. The Old Order Amish pedigrees in these analysesinclude CIMR families 884/885 and 1075 and are de-scribed in detail in the CIMR catalogue (Egeland 1992).
GenotypingComplete genotypic data were collected from 205 in-
dividuals in the Amish pedigrees for three microsatellitemarkers (D18S40, D18S44, and D18S53) in the pericen-tromeric region of chromosome 18. An additionalVNTR marker, D18S21, was typed using standardSouthern blot techniques (Donis-Keller et al. 1987).
Protocols for the collection of genotypic data for themicrosatellite markers included end-labeling one of apair of primers with 33P using 0.75 gCi 33P, 50 U ofkinase, and 75 jiM primer in a 50 gl reaction volume.PCR for each marker was subsequently performed using50 ng genomic DNA, 200 jM dNTPs, 0.075 jM of the33P end-labeled primer, 0.2 jM of the unlabeled primer,0.5 U Taq polymerase, and 1.5 mM MgC12 in a buffercontaining 10 mM Tris-Cl, pH 8.3, 50 mM KCL, and0.001% gelatin. PCR products were separated on dou-ble-loaded 0.6% denaturing polyacrylamide gels thatwere exposed to x-ray film after electrophoresis.
Allele sizes for the microsatellite markers were deter-mined relative to a pUC18 sequencing ladder and forthe VNTR marker relative to molecular weight markers.In order to maintain allelic designations for future allelefrequency determinations, DNA from replicate individu-als were included both within and between gels. All filmswere scored independently by two individuals who hadno information regarding disease status. Data were en-tered into computer files for subsequent linkage analyseswith printouts of the data files checked with the originaldata score sheets, to ensure accuracy.
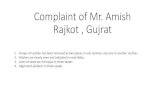
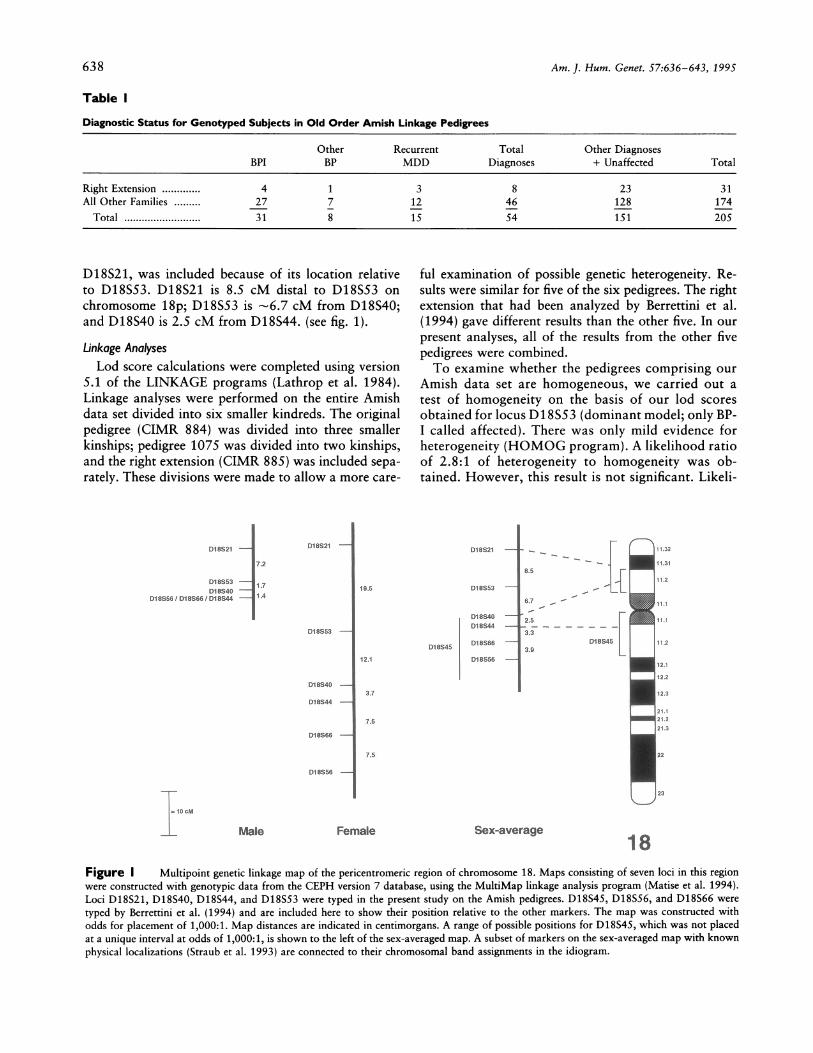
Berrettini et al. (1994) reported positive lod scoreswith markers D18S53, D18S40, D18S45, D18S44,D18S32, and D18S453. Two of these markers (D18S53and D18S45) gave lod scores >1.0 in the right extensionof Old Order Amish pedigree 110. D18S45 maps to thesame region as D18S40 and D18S44 (see fig. 1).We examined linkage to D18S53, D18S40, and
D18S44 and not D18S45, because D18S40 and D18S44are more likely to be heterozygous (.80 and .79, respec-tively) than D18S45 (.63). An additional marker,
637
Am. J. Hum. Genet. 57:636-643, 1995
Table I
Diagnostic Status for Genotyped Subjects in Old Order Amish Linkage Pedigrees
Other Recurrent Total Other DiagnosesBPI BP MDD Diagnoses + Unaffected Total
Right Extension ............. 4 1 3 8 23 31All Other Families ......... 27 7 12 46 128 174
Total .......................... 31 8 15 54 151205
D18S21, was included because of its location relativeto D18S53. D18S21 is 8.5 cM distal to D18S53 onchromosome 18p; D18S53 is -6.7 cM from D18S40;and D18S40 is 2.5 cM from D18S44. (see fig. 1).
Linkage AnalysesLod score calculations were completed using version
5.1 of the LINKAGE programs (Lathrop et al. 1984).Linkage analyses were performed on the entire Amishdata set divided into six smaller kindreds. The originalpedigree (CIMR 884) was divided into three smallerkinships; pedigree 1075 was divided into two kinships,and the right extension (CIMR 885) was included sepa-rately. These divisions were made to allow a more care-
92t-I72
UM 13D1_X ----E
Diem113 IADlOD8I9V
D1i21 -
DIEUs -
V18344-
_1SM
D_ _
Mie
ful examination of possible genetic heterogeneity. Re-sults were similar for five of the six pedigrees. The rightextension that had been analyzed by Berrettini et al.(1994) gave different results than the other five. In ourpresent analyses, all of the results from the other fivepedigrees were combined.To examine whether the pedigrees comprising our
Amish data set are homogeneous, we carried out atest of homogeneity on the basis of our lod scoresobtained for locus D18S53 (dominant model; only BP-I called affected). There was only mild evidence forheterogeneity (HOMOG program). A likelihood ratioof 2.8:1 of heterogeneity to homogeneity was ob-tained. However, this result is not significant. Likeli-
mo
1DA
Dvim"12.1
D1ve -
DMen -913344
M_ -
D6 ---
3.7
_a_
.72.53s52.0
- - - - - - -
maw
7?
7.
Sex
18Figure I Multipoint genetic linkage map of the pericentromeric region of chromosome 18. Maps consisting of seven loci in this regionwere constructed with genotypic data from the CEPH version 7 database, using the MultiMap linkage analysis program (Matise et al. 1994).Loci D18S21, D18S40, D18S44, and D18S53 were typed in the present study on the Amish pedigrees. D18S45, D18S56, and D18S66 weretyped by Berrettini et al. (1994) and are included here to show their position relative to the other markers. The map was constructed withodds for placement of 1,000:1. Map distances are indicated in centimorgans. A range of possible positions for D18S45, which was not placedat a unique interval at odds of 1,000:1, is shown to the left of the sex-averaged map. A subset of markers on the sex-averaged map with knownphysical localizations (Straub et al. 1993) are connected to their chromosomal band assignments in the idiogram.
638
0 ISOM
-L
Pauls et al.: Bipolar Disorder and Chromosome 18
hood ratios of 10:1 or higher are typically consideredsignificant.
Analyses were done using two diagnostic schemeswith affected individuals only. The first scheme includedonly individuals with an RDC diagnosis of BP I. Thesecond scheme included individuals with BP I, BP II, andrecurrent MDD. This second scheme was identical tothe affection status model II used by Berrettini et al.(1994). All other relatives in the kindreds were includedas phenotype unknown. Using affecteds-only in the anal-yses minimizes the chance of a spuriously high lod scorebeing obtained from unaffected individuals in the pedi-gree. Because BP I can have a relatively late age at onset,some unaffected individuals could subsequently becomeill. By using only affected individuals, the results are notas susceptible to new onsets. As has been demonstrated,new onsets of illness can have a dramatic effect on theevidence for linkage (Kelsoe et al. 1989; Egeland et al.1990).Autosomal dominant, additive, and recessive models
were used for each diagnostic scheme. For analyses in-cluding only BP I individuals, the dominant model in-cluded a maximum penetrance for the susceptibility ge-notypes of .50 with an allele frequency of .007; theadditive model included maximum penetrances of .54for the heterozygous susceptibility genotype and .99 forthe homozygous susceptibility genotype. The allele fre-quency for this model was .008. The recessive modelwas identical to that used by Berrettini et al. (1994).The maximum penetrance for the susceptibility geno-type was .85, and the allele frequency was .15. For thebroader diagnostic scheme, the same penetrances wereused, but the allele frequencies were increased. For thedominant and additive models the allele frequency was.025, and for the recessive model the allele frequencywas .20. The dominant model used for the broader diag-nostic scheme was the same as that used by Berrettiniet al. (1994). All models allowed for a population preva-lence of phenocopies of 10% and included age-depen-dent liability classes.The nonparametric ASP (BP I only) analyses were
completed using the SIBPAL program of the SAGE pack-age (Bailey-Wilson and Elston 1989); the same approachas that applied by Berrettini et al. (1994). Analyses weredone for all sib pairs in all families and were comparedwith the results reported by these investigators. Sib-pairanalyses examine whether ASPs share alleles at a givenmarker locus identical by descent (IBD) more often thanwould be expected by chance. In addition, APM analyses(Weeks and Lange 1988) were carried out for selectedmarkers in the region of interest. APM analyses are ex-tensions of ASP analyses to affected pairs of relativesother than siblings. Formal P-values are based on theasymptotic normal distribution of the APM test statis-tics. Marker allele frequencies used in all linkage analy-
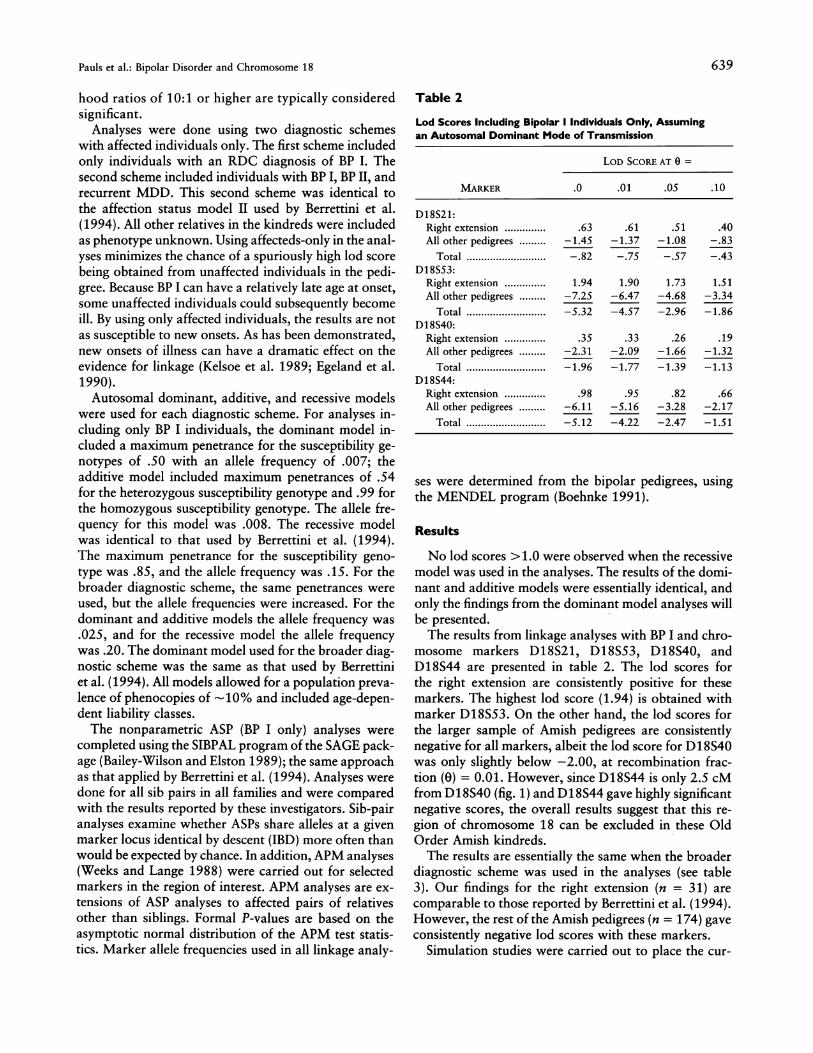
Table 2
Lod Scores Including Bipolar I Individuals Only, Assumingan Autosomal Dominant Mode of Transmission
LOD SCORE AT 0 =
MARKER .0 .01 .05 .10
D18S21:Right extension .............. .63 .61 .51 .40All other pedigrees ......... -1.45 -1.37 -1.08 -.83
Total .................. -.82 -.75 -.57 -.43D18S53:
Right extension .............. 1.94 1.90 1.73 1.51All other pedigrees ......... -7.25 -6.47 -4.68 -3.34
Total .................. -5.32 -4.57 -2.96 -1.86D18S40:
Right extension .............. .35 .33 .26 .19All other pedigrees ......... -2.31 -2.09 -1.66 -1.32
Total .................. -1.96 -1.77 -1.39 -1.13D18S44:
Right extension .............. .98 .95 .82 .66All other pedigrees ......... -6.11 -5.16 -3.28 -2.17
Total .................. -5.12 -4.22 -2.47 -1.51
ses were determined from the bipolar pedigrees, usingthe MENDEL program (Boehnke 1991).
Results
No lod scores > 1.0 were observed when the recessivemodel was used in the analyses. The results of the domi-nant and additive models were essentially identical, andonly the findings from the dominant model analyses willbe presented.The results from linkage analyses with BP I and chro-
mosome markers D18S21, D18S53, D18S40, andD18S44 are presented in table 2. The lod scores forthe right extension are consistently positive for thesemarkers. The highest lod score (1.94) is obtained withmarker D18S53. On the other hand, the lod scores forthe larger sample of Amish pedigrees are consistentlynegative for all markers, albeit the lod score for D18S40was only slightly below -2.00, at recombination frac-tion (0) = 0.01. However, since D18S44 is only 2.5 cMfrom D18S40 (fig. 1) and D18S44 gave highly significantnegative scores, the overall results suggest that this re-gion of chromosome 18 can be excluded in these OldOrder Amish kindreds.The results are essentially the same when the broader
diagnostic scheme was used in the analyses (see table3). Our findings for the right extension (n = 31) arecomparable to those reported by Berrettini et al. (1994).However, the rest of the Amish pedigrees (n = 174) gaveconsistently negative lod scores with these markers.
Simulation studies were carried out to place the cur-
639

Am. J. Hum. Genet. 57:636-643, 1995
Table 3 Table 4
Lod Scores Including BP 1, BP 11 and Recurrent MDDIndividuals, Assuming an Autosomal Dominant Modeof Transmission
LOD SCORE AT 0 =
MARKER .0 .01 .05 .10
D18S21:Right extension .............. .05 .09 .16 .18All other pedigrees ......... -.76 -.72 -.64 -.54
Total .................. -.70 -.64 -.48 -.36D18S53:
Right extension .............. 1.29 1.31 1.30 1.21All other pedigrees ......... -4.83 -4.59 -3.80 -3.02
Total .................. -3.54 -3.27 -2.50 -1.79D18S40:
Right extension .............. .55 .53 .45 .35All other pedigrees ......... -1.88 -1.81 -1.58 -1.34
Total .................. -1.33 -1.28 -1.13 -.99D18S44:
Right extension .............. .12 .15 .22 .22All other pedigrees ......... -5.26 -4.85 -3.74 -2.83
Total .................. -5.14 -4.70 -3.52 -2.61
rent results in proper perspective and to estimate theprobability of a false-positive linkage finding. All simu-lations were done using computer programs developedby Weeks et al. (1990). These simulations examined thepower to detect linkage in the Old Order Amish pedi-grees and estimated the probability of false-positive re-
sults (Type I error, with unlinked marker loci). Simula-tions were done on the six separate kinships describedpreviously, thus it was possible to examine results foreach "small" kinship as well as for the entire homoge-nous collection of families.
Simulations were done using identical diagnosticschemes described for the analyses of the real data. Fivehundred simulations were completed for each recombi-nation fraction. Data were generated simulating rela-tively tight linkage (0 = .01), looser linkage (0 = .05),and no linkage (0 = .50). The simulation results suggestthat the current linkage findings are within expectedranges. It is noteworthy that, when data were generatedsimulating no linkage, a lod score -1.0 occurred 2.6%of the time in the right-extension pedigree but only 0.6%of the time in the remaining five kindreds. This differ-ence is statistically significant (Fisher's exact test, P =
.01). Thus, the right extension yields significantly morefalse-positive linkage results than do the other Amishfamilies under study.The results of nonparametric analyses support the
findings from the parametric analyses. In the ASP analy-ses, Berrettini et al. (1994) reported one marker(D18S21) in the right extension for which the propor-
Affected Sib-Pair Analyses of Old Order Amish Pedigrees
ALL AMISHRIGHT EXTENSIONa FAMILIES
MARKER IBD P IBD P
D18S21 ......... .58 .0004 .52 .3741D18S53 ......... .54 .0530 .54 .3350D18S40 ......... .57 .0120 .71 .0048D18S44 ......... .48 1.0000 .63 .0657
NoTE.-Bipolar I individuals only; IBDidentical by descent.
a From table 2 in Berrettini et al. (1994).
= Proportion of alleles
tion of alleles IBD was greater (P < .001) than expectedby chance, and other markers (D18S62, D18S37, andD18S56) with suggestive P-values <.01. In our analysesof all Amish families, none of the markers showed sig-nificant (P < .001) evidence for linkage (table 4). Fur-thermore, in the regression analysis of squared sib differ-ences on the estimated proportion of alleles IBD, all P-values with positive slope were >.20.
In the APM analyses (table 5), none of the markersstudied showed significant results consistently. ForD18S53, high significance was obtained for the f(p)= 1/p weighting scheme, but no significance was ob-served for the other two weighting schemes (i.e., resultsfrom this marker depend strongly on allele frequencies).Furthermore, none of the weighting schemes resulted insignificant results for D18S21.
Discussion
Our reanalyses of the recently reported linkage of sev-eral pericentromeric chromosome 18 marker loci andbipolar affective disorder replicate the findings of Berret-tini et al. (1994) for the right extension of Old OrderAmish pedigree 110. However, these findings could not
Table 5
Affected Pedigree Member Analysis of Old Order AmishPedigrees
SIGNIFICANCE LEVELS FOR WEIGHTINGSCHEME
MARKER f(p) = 1 f(p) = Iv f(p) = 1/p
D18S53 .......... .6853 .0856 .0000D18S40 ......... .0526 .0201 .2766D18S44 ......... .3227 .3436 .5273
NoTE.-Bipolar I individuals only; p = marker allele frequency.
640

Pauls et al.: Bipolar Disorder and Chromosome 18
be extended to the larger sample of Amish kindreds.Using lod-score analyses and the same genetic modelsas Berrettini et al., this region was excluded by usingthe larger sample. Moreover, nonparametric ASP andAPM analyses suggested that none of the chromosome18 markers were significantly associated with bipolaraffective disorder in the larger sample. If there is a locusconferring susceptibility to bipolar affective disorder on
chromosome 18, it is neither a major locus nor the onlylocus in the Amish population.The results of Berrettini et al., as well as the reanaly-
sis of their findings reported here, are reminiscent ofour previously published findings for the two 11pl5markers HRAS and INS (Kelsoe et al. 1989). As we
emphasized in our earlier study, if homogeneity is as-
sumed, then the presence of a susceptibility locus inthis region of the genome can be excluded. However,there is still a portion of the Amish kindred that contin-ues to provide intriguing evidence for linkage to chro-mosome 11 markers HRAS (lod = 1.34) and INS (lod= 2.88). These findings were obtained using clinicaldiagnoses and a diagnostic hierarchy including BPI,BPII, and recurrent MDD. Given the likelihood of ge-
netic heterogeneity for this common disorder (Baron-des 1992) and the data that support the presence of a
11pl5 susceptibility locus in non-Amish patients (Mel-oni et al. 1993), it is possible that there are at least twoloci contributing to bipolar affective disorder in theAmish kindreds.
It is interesting that the linkage findings for chromo-somes 11 and 18 come from different sections of thelarger extended kindred and might provide evidencethat the illness in these two parts of the pedigree mayhave different ancestral pathways (Kelsoe et al. 1989).While tests for homogeneity did not provide statisticalevidence for heterogeneity, it is nevertheless importantto examine alternative hypotheses. Thus, two-locusanalyses will be applied to these data to examinewhether there is any evidence that both regions mightbe contributing to the expression of the illness in thispopulation. Clearly, multiple susceptibility loci couldcontribute to the inheritance of a complex trait suchas bipolar affective disorder, even in a genetic isolatesuch as the Old Order Amish. The latter would besimilar to other complex disorders such as type 1 insu-lin-dependent diabetes (Davies et al. 1994).An equally valid alternative to the possibility of hav-
ing two ancestral pathways for bipolar disorder amongthe Old Order Amish relates to the fact that the pres-
ently studied Amish families, including the right exten-sion, share several critical family funnels tracing to a
common progenitor. The common ancestor is the only1 of 26 pioneer couples for whom recurrent psychiatricdisorder can be shown among grandchildren and theearliest diagnosed BP I disorder can be identified. The
31 BP I subjects studied in this paper share this historicbipolar pathway and can be described in a single ex-tended pedigree. This suggests that a much higher de-gree of genetic homogeneity exists in this closed popu-lation when compared with other bipolar pedigreesamples.
Importantly, our data and those of Berrettini et al.(1994) should also be evaluated in light of our simula-tion data, which suggest that the right extension of pedi-gree 110 is more likely to yield false-positive lod scores>1.0 when compared with the other Amish kindreds inthis study. This is important, since it is standard practicein linkage studies of complex disorders to examine thepower of a sample of pedigrees to yield significant lodscores. However, the likelihood of false-positive linkageresults in any given sample is rarely considered, eventhough it is well known that the same critical lod scorein different families may be associated with differentP-values (Ott 1991). Our data suggest that the rightextension of pedigree 110 is significantly more likely toyield false-positive results (when the criterion is a lodscore >1.0) than all other Amish pedigrees combined.While this is not the case for more stringent criterion(i.e., lod score > 2.0), these findings should be consid-ered in evaluating reports of "linkage" when lod scoresare <2.0. Presumably, these observations also hold fornonparametric linkage (ASP) analyses.
These simulations underscore the importance of notselectively reporting positive findings in genetic linkagestudies. Berrettini et al. (1994) initially state that, if thereis genetic homogeneity, linkage of bipolar affective dis-order to this region of chromosome 18 can be excludedunder the assumptions of several different genetic mod-els. Although they state that there is no statistical evi-dence to support heterogeneity in their sample, theirreport emphasizes the several positive lod scores for se-lected pedigrees. To interpret such findings adequately,it would be important to have available the estimates offalse-positive findings for each of the pedigrees and foreach of the markers examined. The informativeness ofmarkers can vary considerably from pedigree to pedigreeand even within the same kindred. It has been shownthat such variability can have significant impact on theevidence for linkage (Egeland et al. 1990). We thereforeconclude, from the present data, that there is not a sig-nificant susceptibility locus for bipolar affective disorderin this region of chromosome 18 in the Old Order Amishpopulation.
AcknowledgmentsThis work supported in part by National Institute of Mental
Health grants MH-00508 (a Research Scientist Award toD.L.P.), MH44292 (to J.O.), and MH28287 (to J.A.E.). Theauthors thank Robert Long for technical assistance.
641

642 Am. J. Hum. Genet. 57:636-643, 1995
ReferencesBailey-Wilson JE, Elston RC (1989) SAGE: statistical analysis
for genetic epidemiology. Version 2.0. Louisiana State Uni-versity Medical Center, New Orleans
Baron M, Freimer NF, Risch N. Lerer B, Alexander JR, StraubRE, Asokan S. Das K, Peterson A, Amos J. et al (1993)Diminished support for linkage between manic depressiveillness and X-chromosome markers in three Israeli pedi-grees. Nat Genet 3:49-55
Barondes SH (1992) How genetically heterogeneous are themajor psychiatric disorders? J Psychiatr Res 26:299-303
Berrettini WH, Ferraro TN, Goldin LR, Weeks DE, Detera-Wadleigh S, Nurnberger JI, Gershon ES (1994) Chromo-some 18 DNA markers and manic-depressive illness: Evi-dence for a susceptibility locus. Proc Natl Acad Sci USA91:5918-5921
Boehnke M (1991) Allele frequency estimation from data onrelatives. Am J Hum Genet 48:22-25
Bucher KD, Elston RC (1981) The transmission of manic de-pressives illness. I. Theory, description of the model andsummary of results. J Psychiatr Res 16:53-63
Bucher KD, Elston RC, Green R, Whybrow P. Helzer J, ReichT, Clayton P. Winokur G (1981) The transmission of manicdepressive illness. II. Segregation analysis of three sets offamily data. J Psychiatr Res 16:65-78
Coon H, Jensen S. Hoff M, Holik J. Plaetke R. Reimherr F,Wender P, Leppert M, Byerley W (1993) A genome-widesearch for genes predisposing to manic-depression, assumingautosomal dominant inheritance. Am J Hum Genet52:1234-1249
Davies JL, Kawaguchi Y. Bennett ST, Copeman JB, CordellHJ, Pritchard LE, Reed PW, et al (1994) A genome-widesearch for human type 1 diabetes susceptibility genes. Na-ture 371:130-134
Donis-Keller H. Green P, Helms C, Cartinhour S, WeiffenbachB, Stephens K, Keith TP, et al (1987) A genetic linkage mapof the human genome. Cell 51:319-337
Egeland JA (1992) Amish major affective disorders pedigrees.In: US Department of Health and Human Services NationalInstitute of General Medical Sciences Human Genetic Mu-tant Cell Repository 1992-1993 catalog of cell lines. NIHpublication 93-2944. US Department of Health and Hu-man Services, Washington, pp. 386-405, 841-848
Egeland JA, Gerhard DS, Pauls DL, Sussex JN, Kidd KK, AllenCR, Hostetter AM, et al (1987) Bipolar affective disorderslinked to DNA markers on chromosome 11. Nature325:783-787
Egeland JA, Sussex JN, Endicott J, Hostetter AM, Offord DR,Schwab JJ, Pauls DL (1990) The impact of diagnoses ongenetic linkage study for bipolar affective disorders amongthe Amish. Psychiatr Genet 1:5-18
Endicott J, Spitzer RL (1978)A diagnostic interview: the sched-ule for affective disorders and schizophrenia. Arch Gen Psy-chiatry 35:837-844
Gejman PV, Martinez M, Cao Q, Friedman E, Berrettini WH,Goldin LR, Koroulakis P, et al (1993) Linkage analysis offifty-seven microsatellite loci to bipolar disorder. Neuropsy-chopharmacology 9:31-40
Ginns El, Egeland JA, Allen CR, Pauls DL, Falls K, Keith TP,
Paul SM (1992) Update on the search for DNA markerslinked to manic-depressive illness in the Old Order Amish.J Psychiatr Res 26:305-308
Hebebrand J, Hennighausen K (1992) A critical analysis ofdata presented in eight studies favoring X-linkage of bipolarillness with special emphasis on formal genetic aspects. HumGenet 90:289-293
Hostetter AM, Egeland JA, Endicott J (1983) Amish study II:consensus diagnoses and reliability results. Am J Psychiatry140:62-66
Keith T, Ginns El, Egeland JA, Falls K, Allen C, Long RT,Phipps P, Gravious T, et al (1991) Systematic search of thegenome for markers linked to bipolar affective disorder. AmJ Hum Genet Suppl 49:346
Kelsoe JR, Ginns El, Egeland JA, Gerhard DS, Goldstein AM,Bale SJ, Pauls DL, et al (1989) Reevaluation of the linkagerelationship between chromosome 1ip loci and the gene forbipolar affective disorder in the Old Order Amish. Nature342:238-243
Lathrop GM, Lalouel JM, Julier C, Ott J (1984) Strategies formultilocus linkage analysis in humans. Proc Natl Acad SciUSA 81:3443-3446
Leckman JF, Gershon ES (1977) Autosomal models of sexeffect in bipolar-related major affective illness. J PsychiatrRes 13:237-246
Matise TC, Perlin M, Chakravarti A (1994) Automated con-struction of genetic linkage maps using an expert system(MultiMap): a human genome linkage map. Nat Genet6:384-390
Meloni R. LeBoyer M, Campion D, Savoye C, Poirier M-F,Samolyk D, Malafosse A, et al (1993) Association of manicdepressive illness with the TH locus using microsatellitemarker localized in the tyrosine hydroxylase gene. PsychiatrGenet 3:121
Nurnberger J (1993) Genotyping status report for bipolar af-fective disorder. Psychiatr Genet 3:207-214
OttJ (1991) Analysis of human genetic linkage. Johns HopkinsUniversity Press, Baltimore
Pauls DL, Bailey JN, Carter AS, Allen CR, Egeland JA. Com-plex segregation analyses of Old Order Amish families ascer-tained through bipolar I individuals. Am J Med Genet (Neu-ropsychiatr Genet) (in press)
Pauls DL, Gerhard DS, Lacy LG, Hostetter AM, Allen CR,Bland SD, LaBuda MC, et al. (1991) Linkage of bipolaraffective disorders to markers on chromosome lip is ex-cluded in a second lateral extension of Amish pedigree 110.Genomics 11:730-736
Pekkarinen P, Bredbacka P-E, Terwilliger J, Hovatta I, Lonn-gvist J. Peltonen L (1994) Evidence for a susceptibility locusfor main-depressive disorder in Xq26. Am J Hum GenetSuppl 35:133
Rice J. Reich T. Andreasen NC, Endicott J, Van EerdeweghM, Fishman R. Hirschfeld RM, et al (1987) The familialtransmission of bipolar illness. Arch Gen Psychiatry44:441-447
Risch N. Baron M, Mendlewicz J (1986) Assessing the roleof X-linked inheritance in bipolar-related major affectivedisorder. J Psychiatr Res 20:275-288
Sham PC, Morton NE, Rice JP(1991) Segregation analysis of

Pauls et al.: Bipolar Disorder and Chromosome 18 643
the NIMH Collaborative Study family data on bipolar disor-der. Psychiatr Genet 2:175-184
Spence MA, Amali H, Sadovnik, AD, Remick RA, Bailey-Wil-son JA, Flodman P, Yee IML (1993) A single major locusis the best explanation for bipolar family data: results ofcomplex segregation analyses. Psychiatr Genet 3:143
Spitzer RL, Endicott J, Robins E (1978) Research diagnosticcriteria:rationale and reliability. Arch Gen Psychiatry35:773-782
Straub RE, Lehner T, Luo Y, Loth JE, Shao W, Sharpe L,Alexander JR, et al (1994) A possible vulnerability locusfor bipolar affective disorder on chromosome 21q22.3 NatGenet 8:291-296
Straub RE, Speer MC, Luo Y, Rojas K, Overhauser J, GilliamTC (1993) A microsatellite genetic linkage map of humanchromosome 18. Genomics 15:48-56
Tsuang MT, Bucher KD, Fleming JA, Faraone SV (1985)Transmission of affective disorders: an application of segre-gation analysis to blind family study data. J Psychiatr Res19:23-29
Weeks DE, Lange K (1988) The affected-pedigree-membermethod of linkage analysis. Am J Hum Genet 42:315-326
Weeks DE, Ott J, Lathrop GM (1990) SLINK: a general simu-lation program for linkage analysis. Am J Hum Genet Suppl47:204A