Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative€¦ · Annual Report: August 1,...
51
Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative Annual Report: August 1, 2012 to July 31, 2013 SAMHSA Grant # 5U79SM060428-02 Prepared by Ohio Suicide Prevention Foundation Carolyn Givens, Executive Director Cheryl Holton, GLS Project Director Evaluator, Jane Timmons-Mitchell, Ph.D., Case Western Reserve University Submitted October 29, 2013
Transcript of Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative€¦ · Annual Report: August 1,...

Ohio’s Campaign for Hope:
Youth Suicide Prevention Initiative
Annual Report: August 1, 2012 to July 31, 2013
SAMHSA Grant # 5U79SM060428-02
Prepared by Ohio Suicide Prevention Foundation Carolyn Givens, Executive Director
Cheryl Holton, GLS Project Director
Evaluator, Jane Timmons-Mitchell, Ph.D., Case Western Reserve University
Submitted October 29, 2013

1
Table of Contents
Executive Summary …………… 2
Evaluation Introduction ……………. 6
Evaluation Implementation ……………. 7
Evaluation Methods ……………. 8
Demographics ……………. 10
Youth Screening
Gatekeeper Training
Professional Training
Outcomes ……………. 15
Youth Screening
Gatekeeper Training
Professional Training
Youth Risk Behavior Survey Scales
National Violent Death Reporting System
Next Steps ……………. 47
References ……………. 50

2
Executive Summary
Ohio Suicide Prevention Foundation (OSPF) Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative
SAMHSA Grant # 5U79SM060428-02 Annual Report August 1, 2012---July 31, 2013
Campaign of Hope Goals, Objectives: The Ohio Suicide Prevention Foundation (OSPF) is pleased to present Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative developed in response to SAMHSA’s State/Tribal Youth Suicide Prevention Cooperative Agreements. The Ohio Campaign for Hope: Youth Suicide Prevention Initiative is a multi-pronged approach for addressing at-risk youth ages10-24 and adults who serve them. Sadly, Ohio has rates of youth suicide that exceed the national average; suicide is the third leading cause of death for the targeted age population. At risk youth include: youth residing in Counties with higher than National or State averages for youth suicides, military families, youth involved in the foster care, LGBTQ youth and youth in the juvenile justice system. OSPF mobilized the statewide network of 85 County Suicide Prevention Coalitions, OSPF staff GLS Project Director, Cheryl Holton, Mentor programs (former GLS sub grantees) and OSPF Community Liaisons to promote and implement evidence-based practices including:
• Kognito’s “At Risk” for High School Educators and Military Families, an on-line, Gatekeeper Training,
• Assessing and Managing Suicide Risk, a professional development program for mental health professionals
• Mental Health Check-Ups for Youth--using suicide risk assessment tools - TeenScreen and Signs of Suicide.
• OSPF promotion of the National Suicide Prevention Lifeline 1-800 273-TALK (8255)
Progress Made on Grant Activities and Accomplishments Ohio’s Campaign for Hope has seen progress in a number of important areas; health promotion, National Suicide Prevention Lifeline promotion and suicide prevention awareness to name a few. Continuous updates to the OSPF Website www.ohiospf.org have allowed Ohioans and others to gain greater knowledge of the National Suicide Prevention Lifeline number 1-800 273-TALK (8255) as well as providing a quick overview of Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative and the strategies that are being used to implement the GLS Grant. OSPF’s quarterly E-newsletters have served as an additional vehicle to help educate Ohioans on the opportunities connected to the Campaign. These efforts have reached approximately 70,000 individuals per month (OSPF website average number of hits per month) and 1,000 Ohioans per quarterly via our E-newsletters. Progress at the community level has been realized by utilizing evidence-based practices which form the core components of the initiatives; specifically the evidence-based program created by Kognito Interactive - an online Gatekeeper Training for High Schools and adults serving youth. Ohio has also elected to use both Teen Screen and Signs of Suicide as a part of the Mental Health Check-Ups for Youth programming. OSPF with the support from SAMHSA GLS funding contracted with two persons to act as Community Liaisons for specific portions of the Campaign for Hope grant. One Liaison provides County Coalitions and schools guidance and encouragement on the Kognito, “At Risk” online Gatekeeper Training for

3
high school staff/administrators and adults serving youth. The other Liaison works with two former GLS grantees (from 2006) that are acting as Mentor Programs for the expressed purpose of providing guidance, encouragement and lessons learned to 10 mental health providers that were selected by OSPF to provide Mental Health Check-Ups for Youth programming in the higher risk Counties. As a result of Ohio’s Campaign for Hope GLS grant the two Mentor programs are continuing to offer Mental Health Check-Ups for Youth in their communities. The first year of Ohio’s Campaign for Hope, 941 youth were screened in schools, using the TeenScreen and Signs of Suicide;138 youth screened positive; 56 were referred for follow-up. In the second year (current report),1730 youth participated in education about suicide prevention; 1305 youth were screened in schools with parental consent and reported; 207 youth screened positive and 117 were referred for follow-up. OSPF awarded 15 high risk County Suicide Prevention Coalitions mini-grant funding to promote the Kognito At-Risk online Gatekeeper Training to Ohio high Schools in year one and 18 mini-grants to County Suicide Prevention Coalitions in year two. In the first year, 41 Ohio high schools registered or opened an account for their school, 228 total individual users registered to take the training and 195 individual users or adults completed the online training. In the second year (current report), a total of 92 schools have opened an account for their school, 1444 total individual users have registered to take the training and 1280 individual users or adults completed the online training this year. OSPF has encouraged the Coalitions to mobilize and engage High School Superintendents, High School Administrators, parents and community stakeholders to better understand the issues of depression, addiction and suicide ideation impacting Ohio high school students. 56 individuals also participated in the Kognito Family of Heroes on-line training for those working with veterans. Along with engaging schools, community stakeholder, parents and students OSPF had a specific focus on utilizing Assessing and Managing Suicidal Risk (AMSR) Training for Mental Health Professionals. Four trainings were provided to 182 Mental Health Professionals during the first year of the Campaign for Hope. During the second year (current report), two trainings were provided to 98 Mental Health Professionals. Challenges and Lessons Learned Ohio like many States is in the process of transition. Following the recession which created job loss, home foreclosures and economic loss; many programs have been is impacted at the community level and rebuilding is taking place. The State Departments of Mental Health and Alcohol and Drug Addiction Services are integrating or merging into one agency. This is not a bad thing; but with this type of change to a system that for the past 50 years has been State Administered and County operated some of the dust has yet to settle. Treatment capacity is decreasing, managed care has been introduced on public sector benefits and Medicaid has been elevated to the single State Agency for Medicaid. OSPF has worked to create collaborative partnerships with State Agencies: Mental Health, Alcohol and Drug Addition Services, Department of Health as well as the Department of Education each experiencing transition, change and budget cuts. With the goal in mind that the State Agencies can help promote the Ohio Campaign for Hope: Youth Suicide Prevention Imitative as a positive vehicle for wellness and restoration of hope for Ohio’s youth at the community level. OSPF has encountered the challenge of community partners, schools, mental health providers, parents, students and local governing authorities feeling overwhelmed. Not wanting to take on additional liability or work. There is fear that if you screen for distressed youth and there is not treatment capacity to treat the youth it creates an even more strained system. We have provided

4
AMSR training to help increase their treatment capacity and comfort levels. In working with the Suicide Prevention Coalitions in Ohio to promote Kognito online Gatekeeper Training, high schools had a hard time believing that the Training was FREE. These challenges have not been insurmountable. They have required additional time at the community level to help reassure local partners that not only does Ohio’s Campaign of Hope offer positive opportunity; but being proactive with youth suicide prevention is moving the conversation up stream to help attract greater support from local and state policy makers and the business community. OSPF and the SAMHSA GLS grant are a complimentary package of prevention/intervention benefits that many communities in Ohio are starting to embrace. The lesson for OSPF has been to increase face-to-face time and attention with communities. This is necessary to create change and increased participation. OSPF has also come to understand some regions of Ohio have greater denial and stigma attached to the issues of depression, addiction and suicide ideation. That even if you share the data with the community they don’t want to believe that represents their area or community. OSPF has supported the Coalitions in their effort to be innovative. There have been breakfast meetings, and after school events held for high school administrators, town hall meetings and presentations on the Ohio Campaign for Hope and gift cards and pizza parties to the schools that had the most adults complete the Kognito At-Risk online training. Creating fun and completion has increased local participation--and thinking outside the box is a must. In the current report, challenges regarding implementation of the expanded youth screening procedure are discussed. While the expansion did occur, with the number of counties and especially high risk counties in which youth were screened increasing, the expansion did not occur as rapidly or serve as many youth as we had anticipated. In the third year of the grant, lessons learned from experience will be included in procedures to facilitate increasing the number of youth screened. Major Budgetary and Personnel Adjustments With permission from our Project Officer, we contracted with two experienced individuals for field assistance with the Kognito At-Risk Gatekeeper program and the Youth Mental Health Checkups and eliminated the Program Coordinator position. Having people in the field to travel to coalition, agency and school locations provided excellent service for the dollars expended and we were able to work closely with schools, coalitions and agencies. We continued to contract with two mentor agencies, who delivered Youth Mental Health Check-ups and provided planning, training and mentoring for the 10 new agencies providing youth mental health check-ups. In Ohio we have found that relationship development is constantly needed for good program implementation and reporting and OSPF is committed to providing excellent outcomes.

5
Local Evaluation
Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative
Garrett Lee Smith Suicide Prevention Grant -- Cohort 6, Year Two
Ohio Suicide Prevention Foundation
Jane Timmons-Mitchell, Ph.D., Rodney Thomas, M.A.,
and Yingge Lin, Ph.D.
Begun Center for Violence Prevention Research and Education
Jack, Joseph and Morton Mandel
School of Applied Social Sciences
Case Western Reserve University

6
Introduction Ohio’s Campaign for Hope: Youth Suicide Prevention Initiative is a 3 year youth suicide prevention
campaign funded by SAMHSA (Substance Abuse and Mental Health Services Administration). The
campaign focuses on youth age 15 to 24 statewide and aims to expand suicide prevention awareness
and education. The targets of the campaign include: educators, youth, mental health providers and
others working with high risk youth populations, including youth in foster care and youth in the
juvenile justice system, as well as military families. The campaign mobilizes the Ohio Suicide
Prevention Network of 85 suicide prevention coalitions to promote and implement programming in the
26 highest risk Ohio counties, counties with suicide rates above the national average.
The primary ways in which Ohio’s Campaign for Hope proposes to achieve these aims include:
promoting use of the National Suicide Prevention Lifelines; engaging and mentoring local mental
health organizations in providing school-based youth suicide prevention using the Columbia
TeenScreen and Signs of Suicide programs; providing training to mental health professionals in
Assessing and Managing Suicide Risk (AMSR); and providing Kognito’s At-Risk for High School
Educators for all schools in Ohio.
The output measures for Ohio’s Campaign for Hope include achieving the following over the three
years of the grant:
• 20,000 educators across the state will participate in gatekeeper training
• 450 professionals will participate in AMSR training
• 8,000 youth will be screened using Columbia TeenScreen or Signs of Suicide
• 750 youth will receive follow-up by local mental health providers
• Increased use of the National Lifeline website
First year totals ( ) are presented below, and second year (current report) totals are presented in bold:
(228) 1444 gatekeepers participated in Kognito gatekeeper training
(182) 98 mental health professionals were trained with the Assessing and Managing Suicide Risk
(AMSR) program
(941) 1305 youth were screened in schools, using the TeenScreen and Signs of Suicide programs
(138) 207 youth screened positive; (56) 117 were referred for follow-up 56 people participated in Kognito Family of Heroes training for those who work with veterans

7
Evaluation Implementation As could be seen in the Year One Evaluation Report, the plan for evaluation changed substantially
from the initial proposal to what was carried out last year. An ambitious plan to link youth screening
with gatekeeper training in schools, showing an increase in identification of at-risk youth in high risk
counties that participated in the Kognito At-Risk for High School Educators program could not be
carried out while respecting the requirements of the SAMHSA grant. Fidelity monitoring for all of the
evidence-based programs was also planned. Fidelity is maintained for the Kognito program, since no
alteration to administration is possible for a computer-generated approach. Investigation found that,
although fidelity monitoring tools had been developed for TeenScreen, they were not widely
implemented. Signs of Suicide and Assessing and Managing Suicide Risk did not have fidelity tools
that could be discovered on inquiry.
In the second year of Ohio’s Campaign for Hope,
• Youth screening continued to occur conducted by the two mentor agencies, and also by 10
additional agencies who were contracted to begin screening in high-risk counties. As can be
seen by the maps on pages 16 and 18, expansion of youth both geographically and numerically
did occur. It did not occur at the anticipated rate, which may be due to a number of factors
relating to implementing a program in a new area. To find out more about this from the
agencies, a survey was constructed on Qualtrics and the link was sent to them. Results from
participants are summarized beginning on page 22.
• Kognito At-Risk for High School Educators continued and expanded. The process for
expansion had been worked out in the first year, and the Liaison was able to continue to build
number of schools participating and participants within the schools.
• Kognito Family of Heroes began.
• Assessing and Managing Suicide Risk (AMSR) continued to be administered as it was in Year
One.

8
Evaluation Methods
Youth Screening Youth, ages 15 and up, in secondary schools in Ohio form the potential participant pool.
Letters are sent home to parents, notifying them that the screening will occur at school and asking
them to return a consent form if they would like to have their child screened.
On the day of screening, mental health professionals from local agencies meet at the school to proctor
the screenings during designated class times. One of two screening procedures is used. In the
TeenScreen procedure, the Columbia Health Screen is employed to ask about a range of health issues,
including depression and suicidal feelings. In the Signs of Suicide (SOS) procedure, the Brief Screen
for Adolescent Depression is administered, asking seven questions related to depression and
suicidality. Screening is begun early in the day so that the mental health professionals can score the
screenings and flag those that require an interview. Students who score above a designated cut-off are
asked to meet with a mental health professional to explore their level of suicide potential. Students
may also ask to talk with a mental health professional whether they score above the cut-off or not.
Based on the interview, a number of outcome paths are possible. Students who indicate to the mental
health professional that they are in emotional distress are presented appropriate options, which may
range from emergency hospitalization to referral for outpatient mental health counseling or a referral
to a school counselor. Many students who score above the cut-off indicate that they are already
attending counseling to address their suicidal feelings. Results of the screening interviews are
communicated to parents, especially if an additional referral is indicated.
During the course of the year, a series of messages were communicated regarding the use of
TeenScreen. In the fall of 2012, users were told that they would need to cease use by the end of the
calendar year. Then, they were told that they could use TeenScreen through the end of the academic
year (2012-2013). For agencies beginning the process of discussing with schools to conduct
screening, this confusion created a difficulty. This was also a difficulty for the evaluation, since one
of the things that could still be compared in the first year of the grant was data resulting from youth
screens conducted using TeenScreen with data resulting from Signs of Suicide screening. Due to the
changes in procedure, this comparison became less meaningful: only three sites continued to use
TeenScreen.
Cross-Site Evaluation: ICF International
The mandatory cross-site evaluation is being conducted by ICF International, working with SAMHSA
contractually. The areas of interface between the Local Evaluation and the Cross-Site Evaluation
center on two reporting forms: the EIRF (Early Identification, Referral and Follow-Up), both
Individual and Aggregate forms, and the TES (Training Exit Survey)-Cover Page.
The EIRF tracks the school-based youth screening process, described above. Youth who screen
positive on the initial measure are further screened; some are referred for services, and parents are

9
involved in the process. Attendance at a first scheduled appointment is reported. Data are submitted
by mental health agencies to the evaluator, who submits the data to the ICF web-based server.
The TES-Cover Page reports the number of gatekeepers and mental health providers trained at an
individual training (AMSR) or for a report period (Kognito). Progress to date on the Cross-Site Evaluation includes:
• Data have been entered on the ICF web-based server (the Suicide Prevention Data Center) for
all quarters to date. The data were accepted by ICF and transmitted to SAMHSA.
• In order to enter EIRF data, an 8-digit individual identified must be used. The first four digits
of the identifier are expected to be the unique school code; this mirrors the procedure of the
Columbia TeenScreen program. Unfortunately, with the disappearance of TeenScreen,
assigning school codes fell to the evaluator, using procedure that TeenScreen had previously
shared. In the coming year, it will be easier to assign school codes and share them with sites at
or near the time of screening.
• A uniform data collection spreadsheet, developed to reflect the required elements for the EIRF,
was distributed to sites, and a codebook for spreadsheet variables developed. During the first
year of the expansion, as could be anticipated, there was unease and unfamiliarity with using
the data file. Somewhat problematically, sites put off sharing data until close to the end of the
year, which created a backlog; however, once the data file was sent by a given site, and the
process completed, it seemed to get easier.
Gatekeeper Training:
Local evaluation data for the Kognito At-Risk for High School Educators program includes reporting
demographics of the gatekeepers, as well as reporting pre-post data supplied by the gatekeepers, and
post-training completion of surveys. The results of the Ohio gatekeepers are compared with results
from the National Study (2011).
Mental Health Professional Training
Local evaluation data for the AMSR training includes reporting demographics, as well as a thorough
reporting of survey data supplied by the Suicide Prevention Resource Center, based on post-training
on-line evaluations. These evaluations are not mandatory; not all AMSR trainees completed the
surveys, though most did. Since data for some of the AMSR trainees are not available, data for the
current year are combined with those from the first year of the grant.
Youth Risk Behavior Survey Scales:
Data for the YRBSS, available from the CDC website, are reported for Ohio over time. It was our
hope that we could disaggregate the YRBSS data by county. While we were able to obtain a complete
clean data file from the CDC, Ohio’s data are not kept nor sent by county. Therefore, the goal of
disaggregating by county could not be achieved.

10
Demographics Youth Screening
A primary activity of the Garrett Lee Smith Suicide Prevention Grant is the screening of youth in
schools. During the first year of the grant, a total of 941 youth were screened; of these, 138 screened
positive. 56 were referred for additional services. More female youth than male youth were screened
(57% to 43%), and most youth screened were white (73%).
In the second year of the grant, a total of 1305 youth were screening; of these, 207 screened positive
and 117 were referred for additional services. More female youth than male youth were screened
(55% to 45%) and most youth screened were white (77%).
Figure 1: Gender of youth screened

11
Figure. 2: Ethnicity of youth screened
Age of students screened
Arriving at a consensus definition of age has been a task across the sites. From a previous grant cycle,
some agencies had been reporting grade as a proxy for student age. During the year, the uniform data
file was developed and distributed. Age in years will be reported for all youth screened in Year Three
of the grant.

12
Gatekeeper Training
A total of 228 gatekeepers participated in At-Risk for High School Educators (Kognito, 2011) during
the period August 1, 2011 through July 31, 2012. The demographics of the gatekeepers are
summarized below. Most gatekeepers were female (58%), white (94%), and had worked as teachers
(65%) for more than ten years (57%).
During the second year of the grant, a total of 1444 gatekeepers participated. Of these, 64% were
female and 36% were male. Just over 50% had worked with high school students for over ten years.
Figure 3: Gender of Gatekeepers

13
Figure 4: Ethnicity of Gatekeepers
Figure 5: Tenure of Gatekeepers, in years

14
Assessing and Managing Suicidal Risk (AMSR) Participants
98 mental health professionals attended two trainings for AMSR this year. Data are presented from
the combined 149 trainees who have completed the on-line evaluation in the two years of the grant.
Most are social workers (54%) who had worked in the profession for a number of years distributed
throughout a career (range= student through more than 20 years).
Table 1. Which best describes your profession: Aggregate
Response Percent Response Count
(N=132) Psychologist 2.0% 3
Psychiatrist 0.0% 0
Psychiatric nurse 0.7% 1
Clinical social worker 54.4% 81
Marriage and family therapist 0.7% 1
Substance abuse counselor 1.3% 2
Pastoral counselor 0.0% 0
Licensed professional counselor 17.4% 26
Student 0.0% 0
Other: 23.5% 35
Table 2. Number of years in practice: Aggregate
Response Percent Response Count
(N=132)
Student 1.3% 2
<1-5 years 31.5% 47
6-10 years 21.5% 32
11-20 years 22.1% 33
20+ years
23.5% 35

15
Kognito Family of Heroes Gatekeeper Training
56 people have logged onto the Family of Heroes program designed to aid people who work with
veterans to recognize signs of suicidal ideation and behavior. As the program is just being rolled out,
the number of participants to date is small. Demographics of participants are tabled below.
Table 3. Demographics of Family of Heroes Participants
Role Number of users
Veteran 4
Active Duty 2
Friends of Veteran 3
Family of Veteran 10
Work for a government agency that
Works with veterans
18
None of the above 19
Outcomes
Youth Screening
During the second year of Ohio’s Campaign for Hope, a total of 1305 youth were screened in schools
and 207 screened positive. Maps below show expansion of screening, and a listing of expansion in
high-risk counties. Whereas a single county, Champaign, participated in screening in year one, in year
two, 9 high-risk counties conducted screenings.

16
Figure 6. Map of Ohio’s High-Risk counties
Figure 7. Map showing Youth Screening and Kognito
FirstYear

17
Year 1 GLS Grant OSPF
Counties with Kognito 22 High risk Counties: 7
Allen Muskingham Highest Risk
Ashtabula High Risk Summit
Auglaize Warren
Champaign High Risk Williams
Clark
Clinton
Columbiana
Cuyahoga
Defiance High Risk
Guernsey Highest Risk
Hamilton
Hardin
Lake
Logan
Lorain
Mercer High Risk
Monroe Highest Risk
Montgomery
Counties doing youth screening
Logan
Champaign High Risk Trumbull
Mahoning
Bold = high risk county with both Kognito and Youth Screening
Year 1: 1 county (Champaign)

18
Figure 8. Map showing expansion of Youth Screening and Kognito, Year Two
Year 2 GLS Grant OSPF
Counties with Kognito (all in year one plus:) 23 new
Lucas
Geauga
Franklin
Tuscarawas
Clermont
Putnam
Hancock
Van Wert
Stark
Trumbull
Henry
Mahoning
Putnam
Warren

19
Morgan
Wood
Wayne High Risk
Ottawa
Fulton
Butler
Marion
Erie
Fairfield
Kognito High Risk counties Year 2: 8 (+1 from Year 1)
Counties with Youth Screening
Richland High Risk
Crawford
Jefferson Highest Risk
Defiance High Risk Henry
Fulton
Williams
Ashtabula High Risk
Wayne High Risk Holmes
Mercer High Risk Brown High Risk
Coshocton
Guernsey Highest Risk Morgan
Muskingham Highest Risk Logan
Champaign
Trumbull
Mahoning
Year 2: 7 counties, including 2 Highest Risk counties (+6 from Year 1)
Increase in youth screenings: 20 versus 4 (+16)
Increase in screenings in High Risk counties: 9 versus 1 (+8)

20
Results from youth who screened positive (N=207), for whom individual level data were available, are
reported below. Most youth who screened positive were female (68%), white (60 %) and were
referred to community outpatient mental health facilities (60%). This represents a change from year
one, when most youth were referred to school-based services and may reflect different service
utilization in the expansion counties.
Figure 9: Gender of Youth Screening Positive
Figure 10: Ethnicity of Youth Screening Positive

21
Case Vignettes
1. One young man screened positive (very high) on his SOS (Signs of Suicide) screen. When the
social worker spoke with him, he said “I’m not suicidal. I’m just a large black boy living in (a
small rural town in Ohio) with nothing to do; how the hell do you think I’m doing?” He went
on to share that his mom has been gone for years due to drugs and that his dad struggles with
Heroin. After much discussion with the young man and a call to his dad, we were able to re-
connect the young man to his church (minister and youth minister) and his dad to the
suboxone clinic (which is a program at the agency conducting school screening). The young
man and his dad are both doing very well. We would not have met this family without the
SOS screens.
2. A young lady screened positive (very high) on her SOS (Signs of Suicide) screen. Her mom had
been out of the home for months, dad had multiple mental health issues, and the family was
literally buried in their own home. The young lady had significant hygiene concerns. The
family had over 20 cats in the home and 5 dogs, most of which were soiling the house. The
daughter reported very little room to walk in her home due to “stuff” dad and the rest of the
family were hoarding. We were able to connect the young lady to counseling and both
parents were re-engaged with counseling. The entire family was referred to the Family and
Child First Council which approved a trash dumpster and a family YMCA membership so the
family could do something positive and healthy together. Today, six months later, this family
is doing remarkably better. The young lady is in school daily, showering, and doing her school
work. She is eligible for sports again since her grades have improved so much. Mom and dad
are still coming for counseling and are doing better. There are only 3 cats in the home now
and all dogs are outside. The home is looking much better than it did when we first started
working with this family. The young lady said, “We can actually eat in the dining room now
because we can get into that room again.” She reports, “I haven’t been this good in a long
time and my family is better too – we are not perfect, but better.” Without the SOS screen,
this child and her family would have been missed.
Implementation Survey
In order to gather additional information about reported challenges experienced by the
expansion sites for youth screening (see chart), a very brief survey was generated on Qualtrics. The
link was sent to key informants at the mental health agencies conducting the screening in 10 counties.
Thirteen people gave anonymous survey responses. The participants can be summarized as
follows:

22
• All are white; none are black or Hispanic/Latino.
• 8 are female; 3 are male. None are transgender and two did not report.
• Age:
o 1 is 20-29
o 5 are 30-39
o 2 are 40-49
o 3 are 50-59
o 2 did not report age
Information about their communities and work settings is as follows:
• 11 rural, 1 suburban, 1 urban
• Time worked at current agency:
o 1 years: 3
o 2-5 years: 1
o 6-10 years: 2
o 11-19 years: 3
o >20 years: 2
o 2 did not report
Information about how many years worked with youth in career:
• 1-5 years: 2
• 6-10 years: 2
• 11-19 years: 4
• >20 years: 4
• 1 did not report
Survey Results
We were interested in learning how the sites assessed their own progress toward their screening goals
and what, if anything, may have interfered with meeting the goals. Results are summarized below:
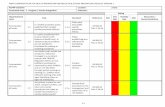
Table 4. Implementation Survey Questions Regarding Youth Screening Process
Question Minimum Maximum Mean Standard
Deviation
Total
Responses
I was able to conduct a program of
youth screening in local schools.
1 4 2.42 1.00 12
The county Suicide Coalition was
helpful in establishing contact with
the schools.
1 5 3.08 1.44 12
The schools were receptive to
youth suicide screening.
1 5 2.58 1.08 12
Data from the screenings was
collected and sent to evaluator.
1 5 1.92 1.38 12
My agency met the target number
of screens.
1 5 3.17 1.53 12
1=To a very great extent; 2=To a great extent; 3=Somewhat; 4=To a small extent; 5=Not at all

23
As can be seen, agencies reported that schools were reasonably receptive, screens were conducted and
data was sent. The presence of coalitions was not sufficient to smooth the process of implementing
youth screening in counties where it had not previously been done. The dispersion in reporting on
meeting targets reflects that agencies knew if they had not met the target: this was a bi-modal
distributions, with 5 agencies saying that they had met it “to a very great extent” or “to a great extent”,
and 6 agencies saying that they had met it “to a small extent” or “not at all.”
Table 5. Implementation Survey Facilitators and Barriers
Question Minimum Maximum Mean Standard
Deviation
Total
Responses
Schools were interested in
providing sufficient time to
conduct screenings.
1
2 1.75 0.45 12
How to explain the screening
procedure was clear.
1 3 1.75 0.62 12
How to conduct screenings and
follow-ups was clear.
1 4 2.17 1.03 12
Sufficient staff were available to
participate in the screening.
1 5 2.17 1.27 12
Knowing what I know now, I would
agree to do screenings again.
1 3 1.75 0.62 12
1=Strongly agree; 2=Agree; 3=Unsure; 4=Disagree; 5=Strongly Disagree
Agencies overall reported that they had learned a great deal about the process by doing it, which is
nearly always the case with implementing a new program. Perhaps the single most telling
information is found in responses to the last question: most agencies indicate that they would agree to
conduct youth screenings again based on their experiences this past year.
Qualitative Responses
Participants were asked to indicate “For your site, what would help make screenings more
successful?”
Some of the implementation issues identified in the quantitative responses were elaborated here. For
example, “poor community readiness”, “having more time to conduct the screens/clinical interviews”,
and “starting earlier in the year” were mentioned as things that would help. Additionally, clarification
of the process, from beginning to end, was mentioned:
“clearer instructions and timelines”, “more clarification on the consent process is needed”, “having
clear cut guidelines on what data points are to be collected”, and “please walk through a screen online
and on paper from beginning to end” indicate the need for more targeted technical assistance to
support the process. However, one participant indicated that the technical assistance received, for both
the screening process and the data collection, was “very helpful”.

24
Results from Gatekeeper Training: At-Risk for High School Educators (Kognito)
Expansion into high-risk counties is shown on the maps on pages 16 and 18; a listing of high-risk
counties where Kognito training is proceeding, as well as those in which both Kognito and youth
screening are conducted, is on pages 17 and 19.
In order to participate in the on-line training, gatekeepers must complete a pre-test of five items
addressing:
1) Identifying behaviors associated with students’ psychological distress
2) Approaching students exhibiting signs of psychological distress
3) Motivating students exhibiting signs of psychological distress to seek help
4) Referring students exhibiting signs of psychological distress
5) Feeling confident to help a suicidal student seek help.
At the conclusion of the training, participants are asked to respond to these same questions, as well as
to items asking about usefulness of the training, whether they would recommend the training to others,
and to comment on the construction of the training. Charts below display the pre and post-training
assessments completed by the gatekeepers. As can be seen, there is a shift from less prepared to more
prepared, and a greater propensity to act to refer students, from the pre- to the post-training
assessments.
Figure 11. Recognize when a student's behavior or appearance is an indicator of psychological distress such
as depression, anxiety or thoughts of suicide

25
5.77
48.08
36.54
9.62
2.22
53.33
44.44
020
40
60
Low Medium High Very high Low Medium High Very high
Pre Post
Pe
rcent
Graphs by source
Figure 12. Approach students exhibiting signs of psychological distress to discuss your concerns
11.54
46.15
30.77
11.54
4.44
57.78
37.78
020
40
60
Low Medium High Very high Low Medium High Very high
Pre Post
Pe
rcent
Graphs by source
Figure 13. Recognize when a student's behavior is a sign of psychological distress.

26
0.22
6.74
52.94
34.07
6.03
0.36
15.35
61.03
23.27
020
40
60
Very Low Low Medium High Very high Very Low Low Medium High Very high
Pre Post
Pe
rcent
Graphs by source
Figure 14. Recognize when a student's physical appearance is a sign of psychological distress
0.14
9.76
49.75
35.61
4.74
0.50
16.63
60.03
22.84
020
40
60
Very Low Low Medium High Very high Very Low Low Medium High Very high
Pre Post
Pe
rcent
Graphs by source
Figure 15. Discuss with a student your concern about the signs of psychological distress they are exhibiting

27
0.72
20.82
42.50
28.43
7.54
0.64
19.41
55.25
24.70
020
40
60
Very Low Low Medium High Very high Very Low Low Medium High Very high
Pre Post
Pe
rcent
Graphs by source
Figure 16. Motivate students exhibiting signs of psychological stress to seek help
0.21
13.37
44.21
33.19
9.01
0.62
16.18
58.58
24.62
020
40
60
Very Low Low Medium High Very high Very Low Low Medium High Very high
Pre Post
Pe
rcent
Graphs by source
Figure 17. Recommend mental health support services (such as guidance counselor, social worker, school
psychologist) to a student exhibiting signs of psychological distress

28
0.21
10.82
35.16
38.21
15.60
0.43
14.20
54.32
31.05
020
40
60
Very Low Low Medium High Very high Very Low Low Medium High Very high
Pre Post
Pe
rcent
Graphs by source
Figure 18. How likely are you to discuss your concerns with a student exhibiting signs of psychological
distress
2.16
12.31
49.46
36.07
0.642.00
50.61
46.75
010
20
30
40
50
Very Unlikely
Somew
hat U
nlikely
Somew
hat L
ikely
Very Like
ly
Very Unlikely
Somew
hat U
nlikely
Somew
hat L
ikely
Very Like
ly
Pre Post
Pe
rcent
Graphs by source
Figure 19. I feel confident in my ability to conduct challenging conversations with students about concerns I
have regarding their classroom behavior

29
3.85
65.38
30.77
71.11
28.89
020
40
60
80
Disagree Agree Strongly agree Disagree Agree Strongly agree
Pre Post
Pe
rcent
Graphs by source
Figure 20. I feel confident in my ability to help a suicidal student seek help
21.15
59.62
19.23
2.22
68.89
28.89
020
40
60
80
Disagree Agree Strongly agree Disagree Agree Strongly agree
Pre Post
Pe
rcent
Graphs by source
Figure 21. I feel confident in my ability to discuss my concern with a student exhibiting signs of
psychological stress

30
2.23
19.78
61.29
16.69
0.573.21
66.81
29.41
020
40
60
80
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Pre Post
Pe
rcen
t
Graphs by source
Figure 22. I feel confident in my ability to recommend mental health support services to a student
exhibiting signs psychological distress
1.65
15.89
60.24
22.21
0.502.36
61.88
35.26
020
40
60
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Pre Post
Pe
rcent
Graphs by source
Figure 24. I feel confident that I know where to refer a student for mental health support

31
1.58
19.29
57.16
21.96
0.412.42
59.13
38.04
020
40
60
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Pre Post
Pe
rcent
Graphs by source
Figure 25. Part of the role of educators is to connect students experiencing psychological distress with
mental health support services
0.83
4.31
59.25
35.61
0.43 1.00
56.46
42.11
020
40
60
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Strong
ly d
isag
ree
Disag
ree
Agree
Strong
ly a
gree
Pre Post
Pe
rcent
Graphs by source
Figure 26. How likely are you to approach and, if necessary, refer a student exhibiting signs of psychological
stress

32
1.92
23.08
28.85
46.15
2.22 2.22
40.00
55.56
020
40
60
Not
like
ly
Somew
hat likel
y
Like
ly
Very lik
ely
Not
like
ly
Somew
hat likel
y
Like
ly
Very lik
ely
Pre Post
Pe
rcent
Graphs by source
In Ohio, the Kognito gatekeeper program At-Risk for High School Educators is being
implemented as part of the Ohio’s Campaign for Hope Youth Suicide Prevention Initiative,
funded by SAMHSA. The Ohio Suicide Prevention Foundation has purchased a state license
so that every school in Ohio can participate in the training. A subsample of gatekeepers who have
participated in the training has been analyzed ; the results appear below.
Participants
303 gatekeepers completed the training. They work at 38 schools throughout Ohio, including
schools in all 5 regions of the state and a mix of urban, suburban and rural schools. Most of the
gatekeepers are teachers, administrators, and support staff (bus drivers, lunch aides, administrative
aides, N=247); about 18% work in mental health related positions (school psychologists, guidance
counselors, intervention specialists, N=55). The vast majority (N=287) are white and female (about
2/3). Nationally, 58% of high school teachers are female. In Ohio, 91% of teachers are white/non-
Hispanic, 6% are African American, and 2% are Hispanic. Though not ethnically diverse, the race
and gender of participants mirrors the make-up of school personnel in Ohio and nationally. About half
of the participants had been in their jobs 10 years or less, and about half of the participants were 46
years of age and older.
Before entering the training, each participant was shown a screen describing the
research, its voluntary nature, and a full consent procedure as required by the university’s
Institutional Review Board, which approved the study. The university has received Federal
assurance that, as a registered IRB, its procedures are in accord with the ethical standards of
the Helsinki Declaration of 1975, as revised in 2008.
Procedures
Gatekeeper Training Program
Kognito At-Risk for High School Educators is a computer-based training

33
Program (www.kognito.com). A gatekeeper logs onto a computer of his or her choice
using a system ID that has been assigned to the school; he or she then creates a unique
password. Creating the training file allows gatekeepers to access materials again after the
training as needed. Lasting about an hour, the training is composed of three role play
vignettes; the gatekeeper views emotionally interactive avatars as they enact situations
drawn from real life examples and deliver scripts written about those examples. The vignettes depict
one student and one teacher discussing behavior that has been observed and is troubling. In each
vignette, there are a series of choice points: gatekeepers are asked to select from three possible
responses the one that best addresses the need of the student. A school psychologist avatar comments
on the choices. If a gatekeeper makes a choice that is not likely to facilitate a student’s seeking help
for suicidal behavior, the psychologist explains that there is a better choice. The gatekeeper is then
directed back to the situation, encouraged to make the better response, and can then see how the
situation improves. In this way, gatekeepers role play making a series of helpful decisions to facilitate
referring students to appropriate people for additional support.
Gatekeepers complete a 5-point Likert type scale that measures preparedness and
likelihood to recognize, discuss, motivate and refer a student who exhibits psychological
distress or signs of suicide. The questions are completed prior to the training (pre-test) and
after completion of the training (post-test). Items assessing utility of the training are completed
at post-test only.
Measures
As described in Albright et al. (2011) three levels of assessment, measuring Reaction
(participants’ opinion of the training), Learning (knowledge and skills gained from the
training), and Behavior (whether participants are likely to apply learned skills and knowledge
in real life) are administered to participants.
Reaction. Questions assessed participants’ reaction to the training program; specifically,
overall rating of the course (on a 4-point Likert scale) and likelihood of recommending it to
colleagues at school. Mean-efficacy questions about how useful and how easy to use they
found the training were rated on a 5-point Likert scale.
Learning criteria. Questions assessed three areas: (1) Preparedness to recognize students’
behavior that could indicate propensity to suicidal behavior; (2) preparedness to approach
students who exhibit such behavior and encourage them to seek help from appropriate school
and community supports; and (3) self-efficacy, or how confident the participant feels to refer
students to appropriate mental health or school personnel.
Behavioral criteria. Questions assessed likelihood to approach students whose behavior could
indicate suicide potential.
Results
All of the pre-training and post-training assessment questions resulted in highly
statistically significant differences: gatekeepers reported that they were more likely to

34
approach, discuss, refer and feel confident in their interactions with students exhibiting
at-risk behavior. Paired sample t-tests were performed in order to compare a given
participant’s pre-training assessment with that person’s post-training responses. Paired
sample t-tests were selected to test the differences between pre-training and post-training
assessments for each individual. Statistical analyses were performed using Stata 12.
The maximum number of participants who responded to assessment questions was 303, and the
minimum number of participants responding to a question was 45. Individual questions results
of interest include: How likely are you to recognize when a student’s behavior is a sign of
psychological distress? (M Pre-training= 1.06, M Post=training=2.17, df= 250, t =-13.62,
p<.0001); How likely are you to approach a student showing signs of psychological distress?
(M Pre-training=0.89, M Post-training=2.49, df= 45, t =--10.69, p<.001); How likely are you to
discuss with a student your concern about signs of psychological distress? (M Pre-training=0.88, M
Post-training=2.13, df=250, t =-15.84, p<.0001); How likely are you to recommend mental health
services to a student showing signs of psychological distress? (M Pre-training=0.86, M Post-
training=2.25,df=257, t=-19.46, p<.0001); and I feel confident in my ability to recommend mental
health support services to a student showing signs of psychological distress (M Pre-training= 1.65, M
Post-training=2.40,df =251,t=-14.10, p<.0001). These results are displayed in Table 1. Confidence
Intervals are included to support the significance of differences.
Table 6
Paired Sample t-tests Comparing Pre-and Post-Training Assessments for Kognito Gatekeeper
Training Participants (N=303)
Question Pre-training(sd) Post-training(sd) df CI (95%) t
________________________________________________________________________
How prepared are you to:
Recognize (#6) 1.08 (0.96) 2.17 (0.61) 250 -1.25/-0.93 -13.62****
Discuss (#8) 0.88 (0.95) 2.13 (0.66) 250 -1.40/-1.09 -15.84****
Motivate (#9) 0.96 (0.94) 2.15 (0.62) 301 -1.33/-1.06 -17.20****
Recommend (#10) 0.86 (0.89) 2.25 (0.65) 257 -1.53/-1.25 -19.46****
Feel confident (#16) 1.65 (0.87) 2.40 (0.51) 251 -0.85/-0.64 -14.10****
****p<.0001
Consistent with the results reported by Albright et al.(2012) gatekeepers reported pre-post
increases in knowledge, motivation, and confidence to recommend mental health support
services to a student. As noted in Cross et al. (2011), confidence is an important predictor of
behavior. Thus, the present study replicates previous findings to include increased confidence
among gatekeepers who participated in the training. Examples of questions that address

35
gatekeeper confidence include:
N13: I feel confident in my ability to conduct challenging conversations with students;
N14: I feel confident in my ability to help a student who is suicidal seek help;
N15: I feel confident in my ability to discuss my concerns with a student exhibiting
suicidal behavior;
N16: I feel confident in my ability to recommend mental health support services to a student; and
N17: I feel confident that I know where to refer a student for mental health support.
Because Cross et al. (2011) found differences between mental health trained gatekeepers and
other gatekeepers, comparisons between mental health and non-mental health trained gatekeepers were
performed. Using the same questions reported above, all pre-post training differences for both mental
health and non-mental health trained gatekeepers were highly statistically significant (see Table 2).
Table 7
Paired-Sample t-tests Comparing Pre- and Post-Training Assessments for Mental Health
and Other Gatekeepers for Kognito Training (N=303)
Question Pre-training Post-training df t
Recognize (#4) Mental Health 0.67 2.48 45 -4.25**
Non-Mental Health 1.18 2.11 204 -10.68****
Discuss (#8) Mental Health 0.56 2.54 45 -12.86****
Non-Mental Health 0.95 2.04 202 -12.72****
Motivate (#9) Mental Health 0.83 2.46 53 -10.68****
Non-Mental Health 0.89 2.18 208 -16.13****
Recommend (#10) Mental Health 0.70 2.57 46 -13.24****
Non-Mental Health 0.89 2.18 208 -16.13****
Feel confident (#16) Mental Health 1.98 2.63 45 -5.21****
Non-Mental Health 1.58 2.34 203 -13.03****

36
****p<.0001
** p<.01
Cross et al. (2011) attributed the lack of change in mental health professionals’ ratings of knowledge
from pre-test to post-test to the significantly greater number of suicide prevention trainings they had
taken. No similar data were collected for the present study, preventing a direct
comparison.
At the conclusion of the training, gatekeepers reported on their satisfaction with
the structure of the training; whether they thought it provided useful information; and
whether they were likely to recommend the training to others. These results are also extremely
positive. For example, over 84% rated the course as either Excellent or Very Good, and over 96% of
participants would recommend the course to colleagues. Over 79% indicated that the course is likely
to help them in assisting a troubled student. Additional results on items measuring means efficacy, or
the participant’s belief that the training is effective, are presented in Table 3. Interestingly, the means
efficacy distribution in the current sample compares closely to that reported by Albright et al. (2012).
Table 8
Means Efficacy Reported by Gatekeepers Taking Kognito Training
Item Not at all A little Some Great Extent Very Great Extent
To what extent is/does the At-Risk Course
A useful tool 0.99% 0.66% 18.81% 54.13% 25.41%
Well constructed 0.66% 1.98% 10.23% 53.14% 33.99%
Easy to use 0.33% 1.66% 10.6% 51.11% 24.44%
Help with troubled 1.18% 2.35% 17.25% 52.55% 26.67%
students
Based on scenarios that 0.66% 1.99% 18.54% 44.37% 34.44%
are relevant to you and
your students
Aid you in getting timely 0.78% 3.52% 19.92% 50% 25.78%
help to your students
Discussion
A sub-sample of gatekeepers’ responses were summarized : 303 persons at 38 schools.
Almost all are Caucasian (N=287); about 2/3 are female. The gatekeepers include people employed in
mental health professional jobs (school psychologist, social worker, guidance counselor,

37
N= 55) as well as non-mental health jobs (teacher, school administrator, aide, N= 247).
Paired sample t-tests compared pre- and post- training responses to questions addressing
ability to recognize signs of suicidal behavior; likelihood to approach, discuss, and refer a
student; and confidence in that knowledge. All pre-post differences were highly statistically
significant. Following the training, gatekeepers responded to questions about the structure of the
training. Most indicated that it is useful, well constructed, easy to use, and provides information
needed to help students who may be wrestling with thoughts of suicide.
The study produced extremely positive results, indicating that dissemination of the program
can be done with the same positive effects on the knowledge of gatekeepers as were found in the
initial program trials. All items found highly significant pre-post differences.
The present study included a large sample of gatekeepers. The fact that mental health
professionals as well as other gatekeepers reported increased knowledge as a result of the training
speaks to the robust nature of the training. The program proved to be easily delivered, since it does
not take any time from the school day, but can be done at the convenience of the individual
gatekeeper. The technology requirements are modest and instructions facilitate participation. Schools
are ramping up technology to keep pace with the interests/needs of students, so training is ecologically
valid for both gatekeepers and the students in schools.
Training for Mental Health Professionals: Assessing and Managing Suicidal Risk (AMSR)
The Assessing and Managing Suicidal Risk (AMSR) program, a best practices day long training with
accompanying study materials, has been conducted four times during the first year of the grant. A
total of 280 mental health professionals have participated in the training; data reported are from the
149 trainees who completed on-line evaluations.
AMSR Training Data Feedback from Aggregate Participants Table 9. Physical environment of the workshop: Aggregate Response Percent Response
Count Very satisfied 62.1% 82
Somewhat satisfied 27.3% 36
Somewhat dissatisfied 6.1% 8
Very dissatisfied 4.5% 6

38
Table 11. Participant manual and other materials: Aggregate
ate
Response Percent Response Count
Very satisfied 90.6% 135
Somewhat satisfied 8.7% 13
Somewhat dissatisfied 0.7% 1
Very dissatisfied 0.0% 0
Table 13. Presentation skills of the trainer: Aggregate Response Percent Response
Very satisfied 69.8% 104
Somewhat satisfied 26.2% 39
Somewhat dissatisfied 3.4% 5
Very dissatisfied 0.7% 1
Table 14. Managing one's own reactions to suicide: Aggregate
Response Percent Response
Count
Increased knowledge very much 45.6% 68
Increased knowledge somewhat 47.0% 70
Knowledge remained the same 7.4% 11
Not sure 0.0% 0
Table 10. We would like to follow-up with a sample of
workshop participants to learn how this workshop has impacted
clinical practice. May we contact you for this purpose?:
Aggregate
Response Percent
Response Count
(N=149)
Yes 74.5% 111
No 25.5% 38
Table 12. Expertise of the trainer: Aggregate Response Percent Response
Very satisfied 85.2% 127
Somewhat satisfied 14.8% 22
Somewhat dissatisfied 0.0% 0
Very dissatisfied 0.0% 0

39
Table 15. Reconciling the difference (and potential conflict) between
the clinician's goal to prevent suicide and the client's goal to
eliminate psychological pain via suicidal behavior: Aggregate
Response Percent Response
Count
Increased knowledge very much 53.7% 80
Increased knowledge somewhat 36.9% 55
Knowledge remained the same 8.7% 13
Not sure 0.7% 1
Table 16. Maintaining a collaborative, non-adversarial stance:
Aggregate Response Percent Response Count
Increased knowledge very much 43.0% 64
Increased knowledge somewhat 41.6% 62
Knowledge remained the same 15.4% 23
Not sure 0.0% 0
Table 17. Eliciting suicide ideation, behavior, plans and intent:
Aggregate Response Percent Response
Count
Increased knowledge very much 49.0% 73
Increased knowledge somewhat 38.3% 57
Knowledge remained the same 12.8% 19
Not sure 0.0% 0
Table 18. Making a clinical judgment of the risk that a client will
attempt or complete suicide in the short and long term:
Aggregate
Response Percent Response Count
Increased knowledge very much 38.9% 58
Increased knowledge somewhat 50.3% 75
Knowledge remained the same 10.1% 15
Not sure 0.7% 1
Table 19. Collaboratively developing a crisis response plan:
Aggregate Response Percent Response
Count
Increased knowledge very much 42.3% 63
Increased knowledge somewhat 45.0% 67
Knowledge remained the same 12.8% 19
Not sure 0.0% 0

40
Table 20. Developing a written treatment and services plan that
addresses the client's immediate, acute, and continuing suicide
ideation and risk for suicide behaviors: Aggregate
Response Percent Response
Count
Increased knowledge very much 39.6% 59
Increased knowledge somewhat 45.0% 67
Knowledge remained the same 14.1% 21
Not sure 1.3% 2
Table 21. Developing policies and procedures for following
clients closely, including taking reasonable steps to be
proactive: Aggregate
Response Percent Response
Count
Increased knowledge very much 34.9% 52
Increased knowledge somewhat 45.6% 68
Knowledge remained the same 16.8% 25
Not sure 2.7% 4
YRBSS OSPF Report 2013 (Year 2)
Table 22. To what degree did the workshop affect your confidence in
managing clients at risk for suicide?: Aggregate Response Percent Response Count
Increased confidence very much 28.9% 43
Increased confidence somewhat 53.0% 79
Confidence remained the same 16.1% 24
Decreased confidence somewhat 0.0% 0
Decreased confidence very much 0.0% 0
Not sure 2.0% 3
Table 23. Overall, how much did you learn in this workshop?:
Aggregate Response Percent Response Count
A great deal 42.3% 63
A good bit 37.6% 56
Some 14.8% 22
Little 3.4% 5
Very little 2.0 3

41
A goal of the Year One Local Evaluation was to obtain YRBSS data from Ohio disaggregated by
county. Through discussion with the local evaluators (Case Western Reserve University Department
of Family Medicine), we learned that Cuyahoga County data is disaggregated. However, discussion
with the Ohio Department of Health and then with the CDC led us to conclude that Ohio’s YRBSS
data is not submitted in a way that allows it to be disaggregated to county. The CDC did send us the
complete data file (in SPSS) together with the codebook. This allows us to do two things in addition
to our reporting of the YRBSS last year:
1) The complete data file contains additional items related to suicidal ideation and behavior that
were not reported on in the previous report.
Q27: During the past 12 months, how many times did you actually attempt suicide?
Number of attempts Number of students % of students
0 1,099 90.9
1 77 5.5
2 or 3 32 2.2
4 or 5 8 0.6
6 or more 11 0.7
Missing 215
Q90: During the past 12 months, how many times did you do something to purposely hurt
yourself without wanting to die, such as cutting or burning yourself on purpose?
Bullying
The data file also contains information about youth reports of experiences with bullying which will be
included as a target activity of the OSPF grant in the third year. Charts relating to bullying items in
Ohio’s 2011 YRBSS data are displayed below.
Q22: During the past 12 months, have you ever been bullied on school property?
Ever been bullied Number of students % of students
Yes 313 9.0
No 1,115 91.0
Missing 104
Number of times Number of students % of students
0 1,193 83.5
1 92 5.9
2 or 3 70 4.5
4 or 5 20 1.4
6 or more times 60 4.7
Missing 7

42
Q23: During the past 12 months, have you ever been electronically bullied?
Ever been bullied Number of students % of students
Yes 199 14.7
No 1,226 85.3
Missing 17
Q91: During the past 12 months, have you ever been bullied away from school property?
Ever been bullied Number of students % of students
Yes 196 14.3
No 1,233 85.7
Missing 13
Smoking A new study (Baek, Eisner & Nierenberg, 2013) reports on the link between smoking and suicidal
ideation in a community sample of 5,695 adults with Major Depressive Disorder (MDD). The study
indicates that current and former smokers have an increased risk of suicidal ideation (current smokers:
odds ratio 1.62, 95% CI 1.42-1.86; former smokers: odds ratio 1.37, 95% CI 1.13-1.66). With that in
mind, YRBSS information on smoking from Ohio’s 2011 data are reported.
Q29: Have you ever tried cigarette smoking, even one or two puffs?
Ever tried cigarettes Number of Students %
Yes 654 51.5
No 685 48.5
Missing 103
Q30: How old were you when you smoked a whole cigarette for the first time?
Age Number of students %
Never 866 59.8
8 years or younger 59 4.7
9 or 10 years 45 3.4
11 or 12 years 74 6.1
13 or 14 years 138 11.2
15 or 16 years 125 11.8
17 years or older 34 2.9
Missing 101
Q31: During the past 30 days, on how many days did you smoke cigarettes?

43
Q32: During the past 30 days, on the days you smoked, how many cigarettes did you smoke
per day?
Q33: During the past 30 days, how did you usually get your own cigarettes?
Method of procurement Number of students %
Did not smoke 1,095 78.9%
Bought at a store 58 5.3%
Bought from a vending machine 3 0.2%
Gave someone else money to buy them for me 56 5.2%
Bummed from someone else 55 5.3%
Someone 18 or older gave them to me 17 1.4%
Took from a store or family member 12 1.0%
Some other way 32 2.7%
Missing 114
Q34: During the past 30 days, on how many days did you smoke cigarettes on school
Number of days smoked Number of students %
0 days 1,101 78.9
1 or 2 days 51 4.5
3 to 5 days 32 3.0
6 to 9 days 18 1.7
10 to 19 days 26 2.5
20 to 29 days 21 1.8
All 30 days 85 7.6
Missing 108
Number smoked per day Number of students %
None 1,097 79%
Less than 1 cigarette 46 4.1%
1 cigarette 42 3.9%
2-5 cigarettes 78 7.1%
6-10 cigarettes 35 3.1%
11-20 cigarettes 20 2.2%
>20 cigarettes 10 0.6%
Missing 114

44
property?
Days smoked on school property Number of students %
0 days 1,317 94.3%
1 or 2 days 20 1.4
3 to 5 days 13 1.0
6 to 9 days 8 0.7
10 to 19 days 6 0.4
20 to 29 days 5 0.4
All 30 days 20 1.8
Missing 53
Q35: Have you ever smoked cigarettes daily, that is, at least one cigarette every day for
30 days?
Ever smoked daily Number of students %
Yes 153 13.1
No 1,201 86.9
Missing 88
Q36: During the past 12 months, did you ever try to quit smoking cigarettes?
Tried to quit Number of students %
Did not smoke in past 12 months 1,000 71.5
Yes 171 15.3
No 159 13.2
Missing
Q39: During the past 30 days, on how many days did you smoke cigars, cigarillos, or little
cigars?
Number of days smoked cigars Number of students %
0 days 1,240 86.3
1 or 2 days 92 6.6
3 to 5 days 37 2.5
6 to 9 days 15 1.2
10 to 19 days 18 1.2
20 to 29 days 7 0.5
All 30 days 27 1.6
Missing 6

45
National Violent
Death Reporting
System (NVDRS) Selected Ohio counties in 2010 included Butler, Cuyahoga, Franklin, Hamilton, Lorain, Lucas, Mahoning, Montgomery, Stark, Summit, Trumbull and Union counties. Source: Ohio Violent Death Reporting System – Selected Counties: Annual Report, 2010. Violence and Injury Prevention Program, Ohio Department of Health, Columbus, Ohio, 2013.
Table 23: County-specific Suicides Rates for Selected Ohio Counties, 2010
County of Residence Deaths Population Rate
Butler 51 363,230 14.0
Cuyahoga 135 1,269,455 10.6
Franklin 141 1,159,947 12.2
Hamilton 88 855,340 10.3
Lorain 38 305,097 12.5
Lucas 54 461,792 11.7
Mahoning 23 234,532 9.8
Montgomery 92 532,181 17.3
Stark 64 377,793 16.9
Summit 59 541,360 10.9
Trumbull 37 208,119 17.8
Union 7 49,165 *
Total 789 6,358,011 12.4
Rates are suppressed for counts less than 10. Rates are expressed per 100,000 persons. Selected Ohio counties in 2010 included Butler, Cuyahoga, Franklin, Hamilton, Lorain, Lucas, Mahoning, Montgomery, Stark, Summit, Trumbull and Union counties. Source: Ohio Violent Death Reporting System – Selected Counties: Annual Report, 2010. Violence and Injury Prevention Program, Ohio Department of Health, Columbus, Ohio, 2013.

46
Table 24: Circumstances of Suicide Victims by Sex for Selected Ohio Counties, 2010
1
Male Female Total
Circumstance Number Percent Number Percent Number Percent
Alcohol Problem 107 18.6 20 12.2 127 17.2
Crisis 153 26.7 38 23.2 191 25.9
Depression 240 41.8 65 39.6 305 41.3
Health Problem 94 16.4 20 12.2 114 15.5
History of Mental Issues 180 31.4 86 52.4 266 36.0
Intimate Partner Problem 183 31.9 41 25.0 224 30.4
Job Problem 84 14.6 16 9.76 100 13.6
Financial Problem 77 13.4 12 7.32 89 12.1
Current Mental Problem 281 49.0 111 67.7 392 53.1
Other Argument 77 13.4 25 15.2 102 13.8
Left a Suicide Note 209 36.4 69 42.7 278 37.7
Substance Use 110 19.2 38 23.2 148 20.1
Suicide Attempt History 106 18.5 54 32.9 160 21.7
Suicide Intent 188 32.8 39 23.8 227 30.8
Currently Receiving Treatment 153 26.7 79 48.2 232 31.4 Rates are suppressed for counts less than 10. Rates are expressed per 100,000 persons. Selected Ohio counties in 2010 included Butler, Cuyahoga, Franklin, Hamilton, Lorain, Lucas, Mahoning, Montgomery, Stark, Summit, Trumbull and Union counties. 1Source: Ohio Violent Death Reporting System – Selected Counties: Annual Report, 2010. Violence and Injury Prevention
Program, Ohio Department of Health, Columbus, Ohio, 2013.

47
Next Steps:
In the coming year, additional goals include:
(1) Continuing expanded school-based youth screening, using the uniform data collection file,
allowing individual level tracking of referral and follow-up for all youth screened.
(2) In addition to other grant activities, begin use of the StandUp Bullying Prevention Program,
described below, in selected schools.
(3) The opportunity to focus on the LGBTQ youth, youth in foster care, youth in juvenile justice
and the adults serving these special population of youth by expanding the online Kognito
Gatekeeper training into settings where adults serving these youth work.
(4) OSPF, as a result of feedback from local educational partners, has purchased a statewide
license for the Kognito online Gatekeeper Training for Ohio Middle Schools. OSPF is also
responding to the passage of the Jason Flatt Act being implemented in Ohio for this
school year 2013-2014 which requires all adults working with children in grades k-12 to get a
least one hour of suicide prevention training. By providing the Kognito online training to our
local educational partners, one more group of Ohioans can recognize the role they play in
suicide prevention, which aligns with Ohio's Suicide Prevention Plan for 2013-2016.
StandUp Bullying Prevention Program
The StandUp program is delivered to each student individually, using a secure cyber platform. Over
the course of four months, students whose parents signed a consent form are asked to come to a
designated location at their school, either before or after school. They are given a system-assigned
individual user id and password and asked to login to a computer. Each student then interacts with the
program, StandUp, by progressing through the online session.
Measures: Bullying. A 24-item measure, adapted from a peer abuse measure developed and validated
in prior research on dating and peer abuse (Levesque, 2011), assessed four types of bullying
experienced and perpetrated during the past year. In the current sample, alphas for the 8 scales ranged
from .68 to .92.
Stage of Change for Using Health Skills to Prevent Bullying. Adapted from the University of Rhode
Island Stage Assessment–Healthy Relationship Skills (URICA–HRS), the measure assessed readiness
to use six healthy skills Teens in the early stages reported perpetrating more peer and dating abuse
than teens in the later stages (Levesque, 2011) .
StandUp: A Program to Prevent Bullying is a newly developed 3 session computer-administered bullying prevention programbased on the Transtheoretical Model of Change (TTM). The
Transtheoretical Model of Change (TTM) provides an empirically validated framework for matching
interventions to readiness along the continuum of change. Research on the TTM over the last 35 years
has found that behavior change involves progress through a series of stages: Precontemplation (not
ready), Contemplation (getting ready), Preparation (ready), Action (making behavioral changes), and
Maintenance (maintaining changes) (Prochaska & DiClemente, 1985). The model includes additional
dimensions central to change:

48
• Decisional balance—the pros and cons related to a behavior’s consequence (Janis
& Mann, 1977).
• Self-efficacy—confidence to make and sustain changes in difficult situations, and
temptation to slip back into old patterns (Bandura, 1977).
• Process of change—10 cognitive, affective, and behavioral activities that facilitate
progress through the stages of change (Prochaska & DiClemente, 1985).
TTM stage-matched interventions have been effective across dozens of populations. For high school
students, interventions matched to readiness to change have the potential to increase efficiency in the
use of scarce intervention resources and improve program effectiveness.
The newly developed StandUp program for bullying prevention and intervention delivers
assessments and individualized feedback on students’:
• Use of skills for relating to others in healthy ways, including videos demonstrating the
skills the student is using the least
• Stage of change for using skills for relating to others in healthy ways
• Other Transtheoretical Model dimensions shown in research to facilitate progress in each
stage of change:
o The Pros (benefits) of using healthy skills
o Stage-matched strategies for change
o Confidence to use healthy skills in a variety of difficult situations
• Behaviors and experiences, including four types of bullying victimization and
perpetration in the past year: verbal abuse, physical violence, sexual coercion and cyberbullying
• Help giving if the student knows someone who is a victim or perpetrator of bullying
• Help seeking if student is a victim or perpetrator of bullying
Results: 115 high school students participated in the first StandUp session; 88 of these
students participated in all three sessions.
Demographics: Students can be described as follows:
� Age range is from 14-18 years
� Grade levels represented are 9 through 12; almost half are 9th graders,
with fewer 12th
graders

49
� Race: over half are white, 38% are black, few Asians and very few Hispanics.
� Almost all parents attended college and most students are not on Free or Reduced
Lunch.
� Gender is almost evenly split between Male and Female.
� About 17% of students report having a physical disability, learning disability, and/or a
psychiatric diagnosis.
� 16 of the youth report being LGBTQ.
Conclusions:
A focus of the StandUp program is the help youth increase readiness to use 6 healthy relationship
skills. Over the course of the three program sessions, youth did significantly increase readiness to use
5 of the 6 healthy relationship skills.
• Understanding and respecting others’ feelings and needs, F=4.77, df=2, p=.01
• Using calm, nonviolent ways to deal with disagreements, F=6.46, df=2, p=.002
• Respecting others’ boundaries, ns
• Communicating feelings and needs clearly and respectfully, F=6.07, df=2, p=.003
• Making decisions that are right for you in social situations, F=6.62, df=2, p.002
• Taking a stand to stop bullying when you see it F=17.08, df=2, p<.001
• Total skills, F=16.04, df=2, p<.001
Changes in readiness to use 5 of 6 healthy relationship skills and total skills over time are
encouraging and indicate StandUp is a promising program to address bullying.

50
References
Albright GA, Goldman R, Shockley KM, et al. (2011). Using an avatar-based simulation to
train families to motivate veterans with Post-Deployment Stress to seek help at the VA.
Games for Health 2011; 1:9-16.
Albright G, Eastgard S, Goldman R, et al. (2012). At-Risk for High School Educators
on-line interactive gatekeeper training simulation for identification and referral of
students exhibiting signs of psychological distress. New York, NY; Kognito
International.
Baek, J.J., Eisner, L.R., & Neirenberg, A.A. (2013). Smoking and suicidality in subjects
with major depressive disorder: Results from the National Epidemiologic Survey on Alcohol
and Related Conditions (NESARC). Journal of Affective Disorders, 150, 1158-1166.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change.
Psychological Review, 84, 191-185.
Cross W, Seaburn D, Gibbs D, et al. (2011). Does practice make perfect? A randomized
control trial of behavioral rehearsal on suicide prevention gatekeeper skills. Journal of
Primary Prevention, 32, 195-211.
Janis, I. L., & Mann, L. (1977). Decision making: A psychological analysis of conflict, choice
and commitment. New York: Free Press.
Levesque, D.A., Van Marter, D.F., Greene, R.N., Prochaska, J.M., Castle, P.H., & Prochaska,
J.O. (2011). Assessing adolescents’ readiness to use health relationship skills for dating
violence prevention: Measure development and validation. Family & Intimate Partner
Quarterly, 3, 319-343.
Ohio Violent Death Reporting System – Selected Counties: Annual Report, 2010. Violence and Injury Prevention Program, Ohio Department of Health, Columbus, Ohio, 2013.
Prochaska, J. O., & DiClemente, C. C. (1985). Common processes of self-change in smoking,
weight-control, and psychological distress. In S. Shiffman & T. Wills (Eds.), Coping and
substance abuse: A conceptual framework (pp. 345-363). New York: Academic Press.


















