
Ohio State's 2016 ASH Review Blood and Marrow Trasplantation (with Turning Point)
29
Ohio State’s 2016 ASH Review Blood and Marrow Transplantation Basem M. William, MD, MRCP(UK), FACP Assistant Professor of Internal Medicine Blood and Marrow Transplant Program
-
Upload
osuccc-james -
Category
Healthcare
-
view
345 -
download
0
Transcript of Ohio State's 2016 ASH Review Blood and Marrow Trasplantation (with Turning Point)
Ohio State’s 2016 ASH Review Blood and Marrow Transplantation
Basem M. William, MD, MRCP(UK), FACP Assistant Professor of Internal Medicine Blood and Marrow Transplant Program

What is the upper age limit for marrow or peripheral blood stem cell transplant?
A. 60 B. 70 C. 75 D. 90 E. Probably not 90, but I don’t
know!
A. B. C. D. E.
0% 0% 0%0%0%
In 2016, how many % patients in the U.S. would have an available donor for allogeneic stem cell transplant?
A. 30% B. 40% C. 50% D. 70% E. >80%
A. B. C. D. E.
0% 0% 0%0%0%

Patients with myeloma should be referred to transplant:
A. Upon diagnosis B. Upon progression C. Upon diagnosis and
progression D. Only if ≤ 65 years
old E. After starting
treatment A. B. C. D. E.
0% 0% 0%0%0%

Current Challenges in Hematopoietic Stem Cell Transplantation (HCT) • Intensity/Toxicity of the conditioning regimen • Donor availability • Selection of suitable candidates for transplant
• Patient characteristics (age, functional status, co-morbid conditions) • Disease characteristics (chemoresistance, sensitivity to GVL) • Timing of transplant (in the era of “novel” agents)
• Relapse after HCT (prevention, monitoring, treatment) • Infections after HCT (prevention, monitoring, treatment) • Graft vs Host Disease (prevention, monitoring, treatment) • Access and financial burden of transplant

Conditioning Regimen Intensity
Gyurkocza1 B and Sandmaier BM. Blood: 124 (3): 344 - 353
Tumor killing + Buying time for
GVL = Less Relapse
Toxicity + GVHD = Higher
Non-relapse mortality
GVL sensitivity vs
Host fitness
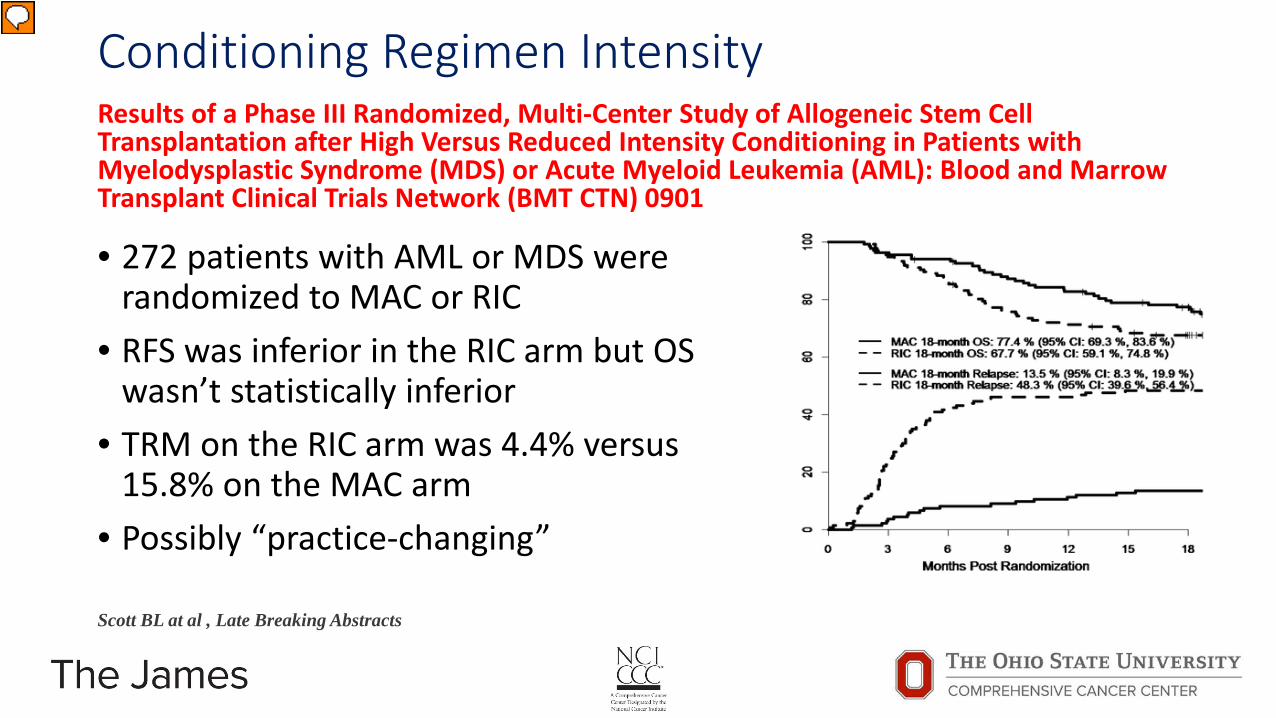
Conditioning Regimen Intensity Results of a Phase III Randomized, Multi-Center Study of Allogeneic Stem Cell Transplantation after High Versus Reduced Intensity Conditioning in Patients with Myelodysplastic Syndrome (MDS) or Acute Myeloid Leukemia (AML): Blood and Marrow Transplant Clinical Trials Network (BMT CTN) 0901
• 272 patients with AML or MDS were randomized to MAC or RIC
• RFS was inferior in the RIC arm but OS wasn’t statistically inferior
• TRM on the RIC arm was 4.4% versus 15.8% on the MAC arm
• Possibly “practice-changing”
Scott BL at al , Late Breaking Abstracts
Presenter
Presentation Notes
Although reduced intensity conditioning (RIC) has a lower toxicity profile and lower treatment related mortality (TRM), retrospective analyses have shown higher relapse rates and similar overall survival (OS) when compared to myeloablative (MAC) regimens in patients with myeloid malignancies. The BMT CTN performed a phase III randomized trial to compare outcomes by conditioning intensity in patients with MDS (N=54) or AML (N=218) (18-65 years, HCT-specific comorbidity index score ≤ 4) who had < 5% marrow myeloblasts by morphology at time of pre-transplant assessment. The primary endpoint of the study was 18 month post-randomization overall survival (OS). Secondary endpoints included: relapse free survival (RFS), relapse rates, TRM, graft-versus-host disease (GVHD), and quality of life (QOL). The RIC regimens were fludarabine (120-180 mg/m2) with busulfan (≤ 8 mg/kg oral or IV equivalent) (Flu/Bu, N=110) or melphalan (< 150 mg/m2) (FM, N=27). The MAC regimens were busulfan (16 mg/kg oral or 12.8 mg/kg IV) with cyclophosphamide (120 mg/kg) (Bu/Cy, N=40); or fludarabine (120-180 mg/m2) (Bu/Flu, N=87); or, cyclophosphamide (120 mg/kg) and total body irradiation (1200-1420cGy) (CyTBI, N=8). The planned enrollment was 356 patients; however, accrual was stopped early due to a presumed benefit of MAC as assessed by an independent DSMB safety review. Among 272 patients enrolled, 135 received MAC and 137 received RIC regimens. Seven enrolled patients did not receive a transplant (RIC N=4, MAC N=3) mainly due to relapse. Most (80.3%) patients randomized to RIC received a busulfan-based regimen. At 18 months, OS for patients on the RIC arm was 67.7% (95%CI 59.1-74.8%) versus 77.4% (95%CI 69.3-83.6%) on the MAC arm, based on intention-to-treat analysis. Although survival was higher with MAC, the difference was not statistically significant (difference of 9.7%, 95% CI -0.9-20.3%, p=0.07). Grade II-IV acute GVHD through 100 days was 31.6% on the RIC arm versus 44.7% on the MAC arm, p=0.024. TRM on the RIC arm was 4.4% (95%CI 1.8-8.9%) versus 15.8% (95%CI 10.2-22.6%) on the MAC arm, p=0.02. Relapse on the RIC arm was 48.3% (95%CI 39.6-56.4%) versus 13.5% (95%CI 8.3-19.9%) on the MAC arm, p<0.01. RFS for patients on the RIC arm was 47.3% (95%CI 38.7-55.4%) versus 67.7% (95%CI 59.0-74.9%) on the MAC arm and the difference was statistically significant (difference of 20.4%, 95%CI 8.8-31.9%, p<0.01). Among patients randomized to RIC, 44 died; relapse was the primary cause of death (86.4%). Among patients randomized to MAC, 31 died; GVHD was the primary cause of death (51.6%) followed by relapse (32.2%). QOL was assessed as a secondary endpoint in this trial using FACT and SF36 tools. Better QOL was observed at day 100 and one year with RIC, particularly regarding physical components with fewer differences in mental and social components. This trial confirms that RIC results in higher relapse rates and lower TRM compared to MAC, with a statistically significant advantage in RFS for patients receiving MAC. The appropriate choice of conditioning intensity remains challenging with a necessity to balance the risk of relapse with TRM in individual patients; however the data from this trial support MAC as the standard of care for patients able to receive it. For patients who are not candidates for MAC, novel regimens, which incorporate enhanced anti-leukemia activity without increasing toxicity, are needed.

Disease characteristics Double Expressing (MYC/BCL2) and Double-Hit Diffuse Large B-Cell Lymphomas Have Inferior Survival Following Autologous Stem Cell Transplantation a522
• Retrospective comparison of 201 pts with rel/ref DLBCL DFCI/COH
• Archival tissue examined by FISH and IHC; myc ≥ 40% bcl-2 ≥ 50%
• 185 patients with complete IHC data, 38% were DEL: 4y PFS and OS in DEL vs. non-DEL 37% v 52% (p=0.001), and 51% v 69% (p=0.005)
• Remission status by PET-CT didn’t change poor outcome of DEL/DHI in multi-variate analysis
Herrera AF et al. Abstract 522
Presenter
Presentation Notes
Background: Double-hit lymphomas (DHL) are a subset of diffuse large B-cell lymphoma (DLBCL) with concurrent chromosomal rearrangements involving the MYC and BCL2 or BCL6 genes, and are associated with dismal outcomes with standard upfront therapy. Double expressing lymphomas (DEL) are a subset of DLBCL with co-expression of MYC and BCL2 by immunohistochemistry (IHC), and also have a poor prognosis with standard therapy. While DHL status may be associated with inferior outcomes in patients with relapsed or refractory (rel/ref) disease (Cuccuini, Blood, 2012), little is known about the outcome of DHL patients with rel/ref disease who proceed to autologous stem cell transplantation (ASCT), and no study to date has examined the outcome of patients with DEL following ASCT. We evaluated the prognostic impact of DHL and DEL status in patients with rel/ref DLBCL who underwent ASCT at 2 centers. Methods: We retrospectively studied patients with rel/ref DLBCL, including transformed indolent lymphoma (TIL), who underwent ASCT at Brigham and Women's Hospital/Dana-Farber Cancer Institute (DFCI) and City of Hope (COH) between 1/2000 and 7/2013. The most recent biopsy prior to ASCT was used for testing when possible. IHC for MYC and BCL2 were performed using the Ventana (MYC: DFCI) and Leica BOND III (MYC: COH; BCL2: DFCI, COH) platforms according to standard protocols. For DEL, IHC cutoffs of ≥ 40% MYC-positive and ≥ 50% BCL2-positive cells were used (Johnson, JCO, 2012). Fluorescence in situ hybridization (FISH) for MYC was performed using LSIMYC dual-color break-apart probes (Abbott Molecular, Des Plaines, IL). MYC-rearranged cases had FISH for BCL2and BCL6 performed using LSI BCL2 and BCL6 dual-color break-apart probes. DHL was defined as > 20% nuclei with break-apart signals for MYC and BCL-2 and/or BCL-6. Results: 201 patients with available archival tissue and clinical data were included. The median age was 60 (range 30-77) years; 60% were male; 26% had TIL; the median number of prior lines of therapy was 2 (range 2-5); 99% had prior rituximab; 53% had primary refractory disease or early (< 6 mo) relapse; 60% were in CR by PET at ASCT; and conditioning regimens were: 66% CBV v 16% BEAM v 10% rituximab and/or ibritumomab tiuxetan-BEAM v 8% other. Overall, the 4y progression-free survival (PFS) and overall survival (OS) were 44% and 61%, respectively. Among 185 patients with complete IHC data, 38% were DEL. The 4y PFS and OS in patients with DEL compared to non-DEL patients were 37% v 52% (p=0.001), and 51% v 69% (p=0.005), respectively [Figure 1]. Results were similar using other reported IHC cutoffs for DEL (e.g. MYC ≥ 40%/BCL2 ≥ 70%, Green, JCO, 2012). Among 93 patients with complete FISH and IHC data available, 13% had MYC rearrangement: 4% were MYC/BCL2 DHL, 3% were MYC/BCL6DHL, and 2% had rearrangements of all 3 loci. The 4y PFS and OS in DHL v non-DHL were 30% v 42% (p=0.042), and 40% v 57% (p=0.026), respectively. Patients with DEL (excluding DHL) and patients with DHL had similar PFS, which was inferior to non-DEL/non-DHL patients (4y PFS 35% v 30% v 45%, respectively, p=0.026) [Figure 2]. In multivariable models testing pre-ASCT variables, including PET response to salvage, DEL (HR 2.1, p=0.0002), TIL histology (HR 1.8, p=0.009), and SD/PD at ASCT (HR 2.9, p=0.025) were associated with poorer PFS, while DEL (HR 2.0, p=0.004) and SD/PD (HR 3.1, p=0.021) were associated with poorer OS. Neither MYC (≥ 40%) nor BCL2 (≥ 50%) expression alone was independently associated with PFS or OS. When analysis was restricted to the subset of patients with complete IHC and FISH data, DEL (HR 1.9, p=0.023), DHL (HR 2.4, p=0.048), and SD/PD at ASCT (HR 7.6, p=0.009) were associated with inferior PFS. No center effect was observed. Conclusions: DEL and DHL status are both associated with inferior PFS in patients with rel/ref DLBCL who undergo ASCT, regardless of remission status. Although ASCT remains a potentially curative approach, these patients should be targeted for study of pre- or post-ASCT relapse risk reduction strategies.

Disease characteristics vs Regimen Intensity Double Epigenetic Modulation of High-Dose Chemotherapy (HDC) with Autologous Stem-Cell Transplant (ASCT) for Patients with Refractory or Poor-Risk Relapsed Lymphoma a1992
• MDACC Gem-Bu-Mel regimen + Azacitidine and vorinostat
• 60 patients were enrolled: 25 DLBCL (10 double hit), 21 HL, 8 T-NHL (3 PTCL, 2 ALCL, 1 AITL, 1 NK/T, 1 panniculitis-like), 4 follicular NHL and 2 mantle cell
• Mucositis is the main toxicity (40%) and 1 death from RSV
• ASCT effective in chemorefractory lymphomas
Nieto Y et al. Abstract 1992
ORR CR % EFS % OS
DLBCL 78% 44% 68% 86%
HL 86% 86% 81% 100%
T-NHL 100% 100% 87.5% 87.5%
Presenter
Presentation Notes
More active high-dose regimens are needed for refractory or poor-risk relapsed non-Hodgkin's (NHL) and Hodgkin's lymphomas (HL), where standard BEAM offers unsatisfactory results. We previously developed a regimen of infusional gemcitabine with busulfan and melphalan (Gem/Bu/Mel), pursuing the inhibition by gemcitabine of DNA damage repair (Nieto et al, BBMT 2012). Since vorinostat induces chromatin relaxation and facilitates access of chemotherapy to DNA, we combined it with Gem/Bu/Mel, which resulted in a safe and markedly synergistic regimen (Nieto et al, BBMT 2015). Still, the addition of vorinostat to GemBuMel induced upregulation of DNAmethyltransferase (DNMT) in lymphoma cells, which could be abrogated preclinically by azacitidine, further increasing tumor-cell kill (Valdez et al, Exp Hematol 2012). These observations led us to study the clinical combination of azacitidine with vorinostat/Gem/Bu/Mel. METHODS: Patients ages 12-65 with refractory or poor-risk relapsed lymphomas and adequate end-organ function were eligible. Azacitidine was given on days -8 to -3 at 15-35 mg/m2/day IV (levels 1-3), followed by vorinostat (1,000 mg PO daily, days -8 to -3), gemcitabine (loading dose of 75 mg/m2 followed by infusion at 10 mg/m2/min over 4.5 hours, days -8 and -3), busulfan (target daily AUC of 4,000, days -8 to -5) and melphalan (60 mg/m2/day, days -3 and -2). ASCT was on day 0. Patients with CD20+ tumors received rituximab (375 mg/m2) on day -9. Dose limiting toxicities (DLT) were defined as any G4-5 nonhematological organ toxicity, or as G3 skin or G3 mucositis lasting >3 days at peak severity. Dose escalation of azacitidine followed a Bayesian design targeting a maximal DLT probability of 25%. We assessed DNMT-3B levels by Western blot in peripheral blood mononuclear cells drawn at baseline and days -5 and -1 in 8 patients treated at the MTD. RESULTS: Between 11/13 and 6/15, 60 patients were enrolled: 25 DLBCL (10 double hit), 21 HL, 8 T-NHL (3 PTCL, 2 ALCL, 1 AITL, 1 NK/T, 1 panniculitis-like), 4 follicular NHL and 2 mantle cell (Table 1). Table 1. Patient population. Median age (range) 41 (16-65) Primary induction failure / high-risk/refractory relapse 28% / 62% Bulky lesions at relapse/PD 58% Secondary IPI (DLBCL): 0-1 / >1 44% / 56% LDH at relapse/PD (DLBCL): High / Normal 50% / 50% Median # prior chemotherapy lines (range) 3 (2-7) Prior xRT 17% PET+ at HDC 32% Status at HDC: 68% CR, 25% PR, 7% unresponsive Patients were treated at levels 1-3, with the MTD of azacitidine established at level 1 (15 mg/m2/day). The DLT was mucositis, observed at the following frequencies: level 1 (N=37): 16%, level 2 (N=18): 28%, level 3 (N=5): 40%. One patient died from early RSV pneumonia at level 3. The toxicity profile at the MTD was manageable: mucositis (40% G2, 32% G3), self-limited transaminitis (16% G2, 16% G3), self-limited elevation of bilirubin not associated with VOD (19% G2, 22% G3) and dermatitis (13% G2). There were no cardiac, pulmonary, renal or CNS toxicities. Neutrophils and platelets engrafted promptly at median days +9 (7-11) and +12 (8-64), respectively. This toxicity profile is identical to the one seen with Gem/Bu/Mel and vorinostat/Gem/Bu/Mel. DNMT-3B levels in PBMNC decreased from baseline to day -1 by a median 58% (19-80%) in 7/8 pts. Response assessment and patient outcomes at median follow-up of 11 months (2-21) at are shown on Table 2 and Figures
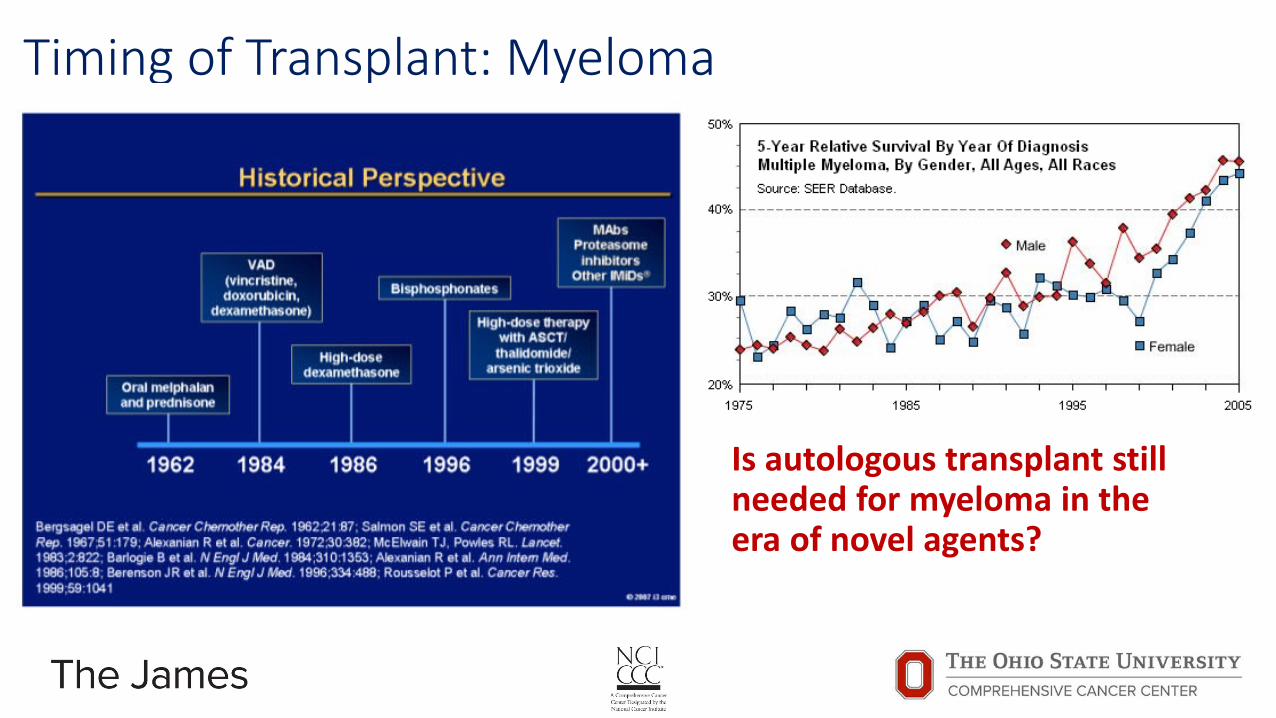
Timing of Transplant: Myeloma
Is autologous transplant still needed for myeloma in the era of novel agents?
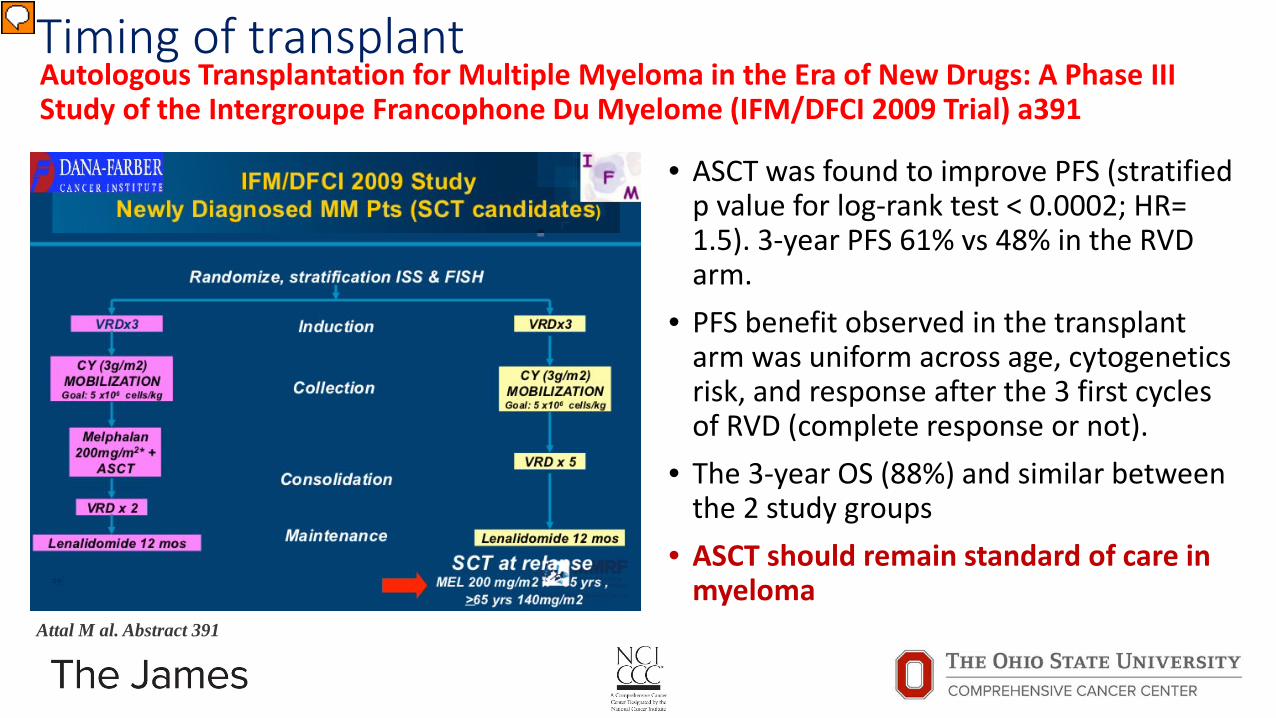
Timing of transplant Autologous Transplantation for Multiple Myeloma in the Era of New Drugs: A Phase III Study of the Intergroupe Francophone Du Myelome (IFM/DFCI 2009 Trial) a391
• ASCT was found to improve PFS (stratified p value for log-rank test < 0.0002; HR= 1.5). 3-year PFS 61% vs 48% in the RVD arm.
• PFS benefit observed in the transplant arm was uniform across age, cytogenetics risk, and response after the 3 first cycles of RVD (complete response or not).
• The 3-year OS (88%) and similar between the 2 study groups
• ASCT should remain standard of care in myeloma
Attal M al. Abstract 391
Presenter
Presentation Notes
High dose chemotherapy plus autologous transplantation (ASCT) is considered a standard of care for newly diagnosed myeloma patients younger than 65 years of age. The high complete response rate (CR) achieved with the triplet combination of immunomodulatory drugs + proteasome inhibitors + dexamethasone has led investigators to propose this strategy upfront without immediate ASCT. The aim of this study was to determine if, in the era of new drugs, ASCT was still required in the initial management of young patients.We conducted a randomized trial comparing conventional dose treatment (RVD arm= 8 cycles of Lenalidomide, Bortezomib and Dexamethasone, plus stem cell mobilization after 3 cycles of RVD utilizing high dose cyclophosphamide and G-CSF) to RVD with ASCT (Transplant arm= 3 induction cycles of RVD, followed by stem cell collection, and then ASCT conditioned with Melphalan 200 mg/m2, followed by 2 cycles of RVD as consolidation). Maintenance treatment with Lenalidomide (10 to 15 mg/d) was used in both arms for one year. In the RVD arm, ASCT was planned at time of relapse. From November 2010 to November 2012, 700 previously untreated French and Belgian patients were equally randomized between arms. Randomization was stratified according to ISS stage (I vs II vs III) and FISH analysis (standard vs high risk = del 17p or t(4;14) or t(14;16)). The primary study end point was progression-free survival (PFS). Two pre-specified interim analysis were to be performed at 33% and 69% of the estimated total number of events. The second interim analysis was performed in June 2015 (346 events= 197 in the RVD arm, 149 in the transplant arm). These results were submitted to an independent data management and safety committee, who recommended completing the trial, and continuing follow-up (without cross over before progression), since the difference in PFS between the 2 groups had reached the pre-specified level of significance for stopping the study. As of June 8, 2015, median follow up was 39 months. All patients had discontinued treatment (completion of planned therapy= 66%, disease progression= 16%, adverse events= 10%). Patient characteristics of each group were similar and no significant differences were found with regard to age (median=58 years), ISS stage (I=233, II=341, III=126), Ig isotype, beta-2-microglobulin (median=3.5 mg/L), and cytogenetics (high risk=90 patients). In the transplant arm, 93% of patients underwent ASCT and 5 toxic deaths occurred during mobilization or in the actual transplant phase (1.4%). ASCT was found to improve PFS (stratified p value for log-rank test < 0.0002; HR= 1.5, 95% CI= 1.2-1.9). The 3-year post-randomization PFS rate was 61% in the transplant arm versus 48% in the RVD arm. The PFS benefit observed in the transplant arm was uniform across all the following subgroups: age (≤ or > 60 years), sex, Ig isotype (IgG or others), ISS stage (I or II or III), cytogenetics (standard or high risk), and response after the 3 first cycles of RVD (complete response or not). The 3-year post randomization rate of overall survival was extremely high (88%) and similar between the 2 study groups (stratified p value for log rank test=0.25). The complete response rate was significantly higher in the transplant arm compared to the RVD arm: 58% versus 46%, respectively (p<0.01). Forty-one second primary malignancies among 39 patients were recorded (Transplant arm=23, RVD arm=18). In conclusion, these results demonstrate that ASCT should remain a standard of care for young patients with de novo myeloma, and suggest that RVD plus ASCT could be a future reference strategy in this setting. Further follow-up is needed, as the number of deaths is still low in both arms. The parallel US trial, which uses a similar design but importantly administers maintenance Lenalidomide continuously until progression in both arms, is ongoing.

Timing of transplant A Salvage Autologous Stem Cell Transplant (ASCT2) Induces Superior Overall Survival Following Bortezomib-Containing Re-Induction Therapy for Relapsed Multiple Myeloma (MM): Results from the Myeloma X (Intensive) Trial a394
• PFS benefit observed in the ASCT arm; 67 m vs 31/39 m • OS benefit at 4y: 69 vs 50% • A second ASCT should be considered early in patients
with myeloma relapsing after first ASCT Cook G al. Abstract 394
Relapsed myeloma after ASCT
Bortezomib-Doxorubicin-Dex (4 cycles)
Response (SD or better)
PBSC mobilization CY + G-CSF
Randomization=174
ASCT CY weekly x 12 cycles
Presenter
Presentation Notes
Introduction: Autologous transplantation (ASCT) in myeloma (MM) is standard consolidative therapy in first line therapy in eligible patients. We have shown definitely that a salvage ASCT in relapse setting can induce superior durability of responses (time-to-progression; TTP) over non-transplant consolidation with oral cyclophosphamide after a proteasome inhibitor-based re-induction schedule (ISRCTN601231201). The secondary end point of this multi-centre phase III randomised controlled trial was to evaluate the impact of salvage ASCT on the overall survival (OS_ of patients relapsing after a prior ASCT and delineate patient subgroups that may benefit the most. Patients and Methods: Eligible patients with MM relapsing after a prior ASCT were enrolled. All patients were re-induced with Bortezomib, Doxorubicin and Dexamethasone (PAD) therapy delivered in 2-4 21-day cycles before 1:1 randomization to either a second ASCT (melphalan 200mg/m2 iv; ASCT2 supported by either stored or remobilized stem cells) or low dose consolidation with weekly cyclophosphamide 400mg/m2 PO for 12 weeks (Non-TransplantConsolidation; NTC). Response was assessed (by IMWG criteria) after re-induction and 100 days post-randomization with TTP being determined as the primary end-point. Patients were stratified by β2microglobulin (β2M) at trial entry, ASCT1 TTP and response to re-induction, analyzed according to cytogenetic abnormalities by iFISH (unfavorable:t(4;14), t(14;16) and del17p) with OS was a key secondary endpoint. Results: 297 patients were entered into the study and 174 randomized from April 2008 to November 2012: ASCT2 n=89, NTC n=85. Median age was 61 (range 38-75) with 73.6% of patients relapsing more than 24 months from first ASCT. ORR to re-induction therapy was 79.4% with a 16.0% sCR/CR rate. Post-randomization, sCR/CR was significantly higher after ASCT2 (39.3% [95% CI 29.1,50.3] vs 22.4% [95% CI 14.0,32.7]; p=0á012). The median follow-up is 52 months (IQR range 41, 62) and the up-dated TTP demonstrates continued advantage in ASCT2 cohort compared to NTC (19 months [95% CI 16,26] vs 11 months [95% CI 9,12]; Log Rank p<0.0001). 75 patients (43.1%) have died since randomization, primarily from disease progression (59.4%). The median survival was 67 months (95% CI 55, °) in the ASCT2 cohort compared with 52 months (95% CI 42,60) in the NTC cohort (Log Rank p=0.022). Cox proportional hazards regression (adjusted for stratification factors including whether PBSC was remobilized) showed a reduced hazard of death in the ASCT2 group compared to NTC (HR=0.56, 95%CI [0.35, 0.90], p=0.0169). CR/sCR to re-induction therapy (HR 0.14, p=0.032), ASCT1 TTP > 24m (HR0.60, p=0.089), β2M level <3.5mg/L (HR 0.35, p=0.039) and the absence of high risk iFISH (HR 0.36, p=0.007) were associated with improved OS in favour of ASCT2 (Fig. 1A). To-date, following progression on protocol, 88.7% in the ASCT2 and 84% in the NTC cohorts have received 3rd line therapy, primarily consisting of a lenalidomide based combination (88.9% in the ASCT2 and 81% in the NTC cohorts). 20 patients (26.7%) in the NTC cohort underwent salvage ASCT in 3rd/4thline (NTC/ASCT2), with 1 patient in each cohorts proceeding to allogeneic SCT. The PFS2 was significantly better in the ASCT2 compared with both NTC/ASCT2 and NTC cohorts (ASCT2: 67m, [95%CI 52,°] vs NTC/ASCT2: 31m, [95%CI 23,42] vs NTC 39m, [95%CI 32,47]; p<0.0001). Consequently, the 4-year OS demonstrated a superiority of asalvage ASCT in second line over 3rd line or not (ASCT2: 69% [95%CI 58,79] vs NTC/ASCT2: 61% [95%CI 52,69] vsNTC 50% [95%CI 36,64]) where the OS in NTC groups split by 3rd line ASCT were not significantly different (p= 0.139, Fig. 1b). Conclusion: This long-term follow-up analysis demonstrates a clear advantage in terms of OS when salvage ASCT consolidates bortezomib-based re-induction therapy in patients with MM at first relapse. The delay of salvage ASCT to third line, though being suggestive of benefit over no salvage ASCT, does not confer the same degree of OS advantage as shown with a salvage transplant in second line. This data is key for patient-centered clinical decision-making.
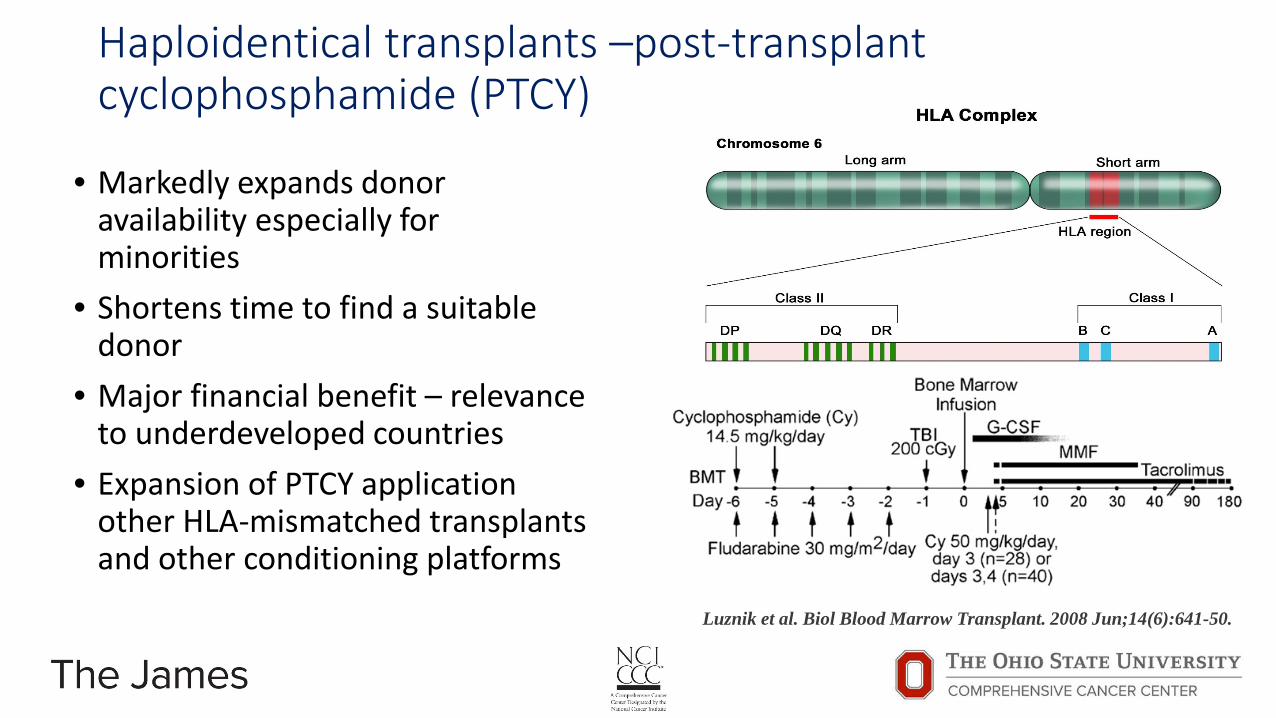
Haploidentical transplants –post-transplant cyclophosphamide (PTCY)
• Markedly expands donor availability especially for minorities
• Shortens time to find a suitable donor
• Major financial benefit – relevance to underdeveloped countries
• Expansion of PTCY application other HLA-mismatched transplants and other conditioning platforms Luznik et al. Biol Blood Marrow Transplant. 2008 Jun;14(6):641-50.

Haploidentical transplants –post-transplant cyclophosphamide (PTCY)
• Two recent large CIBMTR analysis show similar outcomes to HLA matched donors
• Uniformly lower incidence chronic GVHD with haplo-HCT • For AML, 3y OS was 45/46% haplo-HCT vs 50/44% MUD (MA/RIC) • For lymphomas, 3y OS was 61% vs. 62% MRD (with RIC) • No difference in PFS or cumulative incidence of relapse with Haplo-HCT • No difference in TRM with Haplo-HCT
Ciurea et al. Blood. 2015 Aug 20;126(8):1033-40
Ghosh et al Reduced-intensity transplantation for lymphomas using haploidentical related donors versus HLA-matched sibling donors (2016) in press
Presenter
Presentation Notes
AML: We studied adults with acute myeloid leukemia (AML) after haploidentical (n=192) and 8/8 HLA-matched unrelated donor (n=1982), transplantation. Data were obtained from the Center for International Blood and Marrow Transplant Research. Haploidentical recipients received calcineurin inhibitor (CNI), mycophenolate and post-transplant cyclophosphamide for graft-versus-host disease (GVHD) prophylaxis; 104 patients received myeloablative and 88, reduced intensity conditioning regimens. Matched unrelated donor transplant recipients received CNI with mycophenolate or methotrexate for GVHD prophylaxis; 1245 patients received myeloablative and 737, reduced intensity conditioning regimens. In the myeloablative setting, day-30 neutrophil recovery was lower after haploidentical compared to matched unrelated donor transplants (90% versus 97%, p=0.02). Corresponding rates after reduced intensity conditioning transplants were 93% and 96%, (p=0.25). In the myeloablative setting, 3-month acute grade 2-4 (16% versus 33%, p<0.0001) and 3-year chronic GVHD (30% versus 53%, p<0.0001) were lower after haploidentical compared to matched unrelated donor transplants. Similar differences were observed after reduced intensity conditioning transplants, 19% versus 28%, (p=0.05) and 34% versus 52%, (p=0.002). Among patients receiving myeloablative regimens, 3-year probabilities of overall survival were 45% (95% CI 36-54) and 50% (95% CI 47-53) after haploidentical and matched unrelated donor transplants (p=0.38). Corresponding rates after reduced intensity conditioning transplants were 46% (95% CI 35-56) and 44% (95% CI 0.40-47) (p=0.71). Although statistical power is limited, these data suggests that survival for patients with AML after haploidentical transplantation with posttransplant cyclophosphamide is comparable with matched unrelated donor transplantation. Lymphoma: Background: Related donor haploidentical hematopoietic cell transplantation (Haplo-HCT) using post transplantation cylophosphamide (PT-Cy) is increasingly used in patients lacking HLA-matched sibling donors (MSD). We compared outcomes after Haplo-HCT using PT-Cy with MSD-HCT in patients with lymphoma. Methods: We evaluated 987 adult patients undergoing either Haplo-HCT (n=180) or MSD-HCT (n=807) following reduced-intensity conditioning regimens. The haploidentical group received graft-versus-host disease (GVHD) prophylaxis with PT-Cy ± a calcineurin inhibitor (CNI) and mycophenolate. The MSD group received CNI-based GVHD prophylaxis. Results: Median follow-up of survivors was 3-years. The 28-day neutrophil recovery was similar in the two groups (95% vs. 97%; p=0.31). The 28-day platelet recovery was delayed in the haploidentical group compared to the MSD group (63% vs. 91%, p=0.001). Cumulative incidence of grade II-IV acute GVHD at day 100 was similar between the two groups (27% vs. 25%; p=0.84). Cumulative incidence of chronic GVHD at 1-year was significantly lower after Haplo-HCT (12% vs. 45%; p<0.001) and this benefit was confirmed on multivariate analysis (RR=0.21, 95%CI 0.14-0.31; p<0.0001). For Haplo-HCT vs. MSD-HCT, 3-year rates of non-relapse mortality (15% vs. 13%; p=0.41), relapse/progression (37 vs. 40%; p=0.51), progression-free survival (48% vs. 48%; p=0.96) and overall survival (61 vs. 62%; p=0.82) were similar. Multivariate analysis showed no significant difference between haplo-HCT and MSD-HCT in terms of non-relapse mortality (p=0.06), progression/relapse (p=0.10), progression-free survival (p=0.83) and overall survival (p=0.34). Conclusion: Haplo-HCT provides survival outcomes comparable to MSD-HCT, with a significantly lower risk of chronic GVHD.

Haploidentical transplants –PTCY Survival after T-Cell Replete Haploidentical Related Donor Transplant Using Post-Transplant Cyclophosphamide Compared with Matched Unrelated Donor (MUD) Transplant for Lymphoid Malignancies a194
• Retrospective comparison of 917 adult pts with HL/NHL from CIBMTR
• cGVHD rates were 13% vs 51/33% for MUD -/+ ATG (p<0.001)
• 3 y OS was 60%, 62% and 50% • No difference in relapse rate, PFS,
or NRM
Mussetti A et al. Abstract 194
Presenter
Presentation Notes
Background: The use of haploidentical hematopoietic cell transplantation (HCT) using post- transplant cyclophosphamide (PT-Cy), calcineurin inhibitors (CNI) and mycophenolate as graft-versus-host disease (GVHD) prophylaxis is rapidly increasing in patients (pts) lacking suitable HLA-matched donors. Herein we compare outcomes of haploidentical HCT using this GVHD prophylaxis with 8/8 allele-level MUD HCT. Methods: Included are 917 adult (>18) lymphoma pts who underwent allogeneic HCT between 2008 and 2013. All pts received non-myeloablative or reduced-intensity conditioning regimens. The study cohort was divided into 3 groups; haploidentical (n=185), MUD without (w/o) antithymocyte globulin (ATG; n=491) and MUD with (w/) ATG (n=291). The primary end-point was overall survival (OS). Secondary endpoints included cumulative incidence (Cum-Inc) of acute GVHD, chronic GVHD, non-relapse mortality (NRM), relapse/progression (rel/prog) and progression-free survival (PFS). The study had an 83% power to detect an 11% difference in OS. Results: The baseline characteristics are shown in Table 1. Pts in the haploidentical group received conditioning with Flu/CY/2Gy TBI and PT-Cy + CNI and mycophenolate as GVHD prophylaxis, while the two MUD cohorts received fludarabine-based (+ an alkylator or 2GyTBI) conditioning and CNI-based GVHD prophylaxis. Graft source was bone marrow in 93% of the haploidentical pts and peripheral blood in 94% and 91% of MUD w/o ATG and MUD w/ ATG pts, respectively. The 28-day neutrophil recovery and platelet recovery were 94%, 97%, 97% (p=0.32) and 63%, 89%, 84% (p<0.001) in the haploidentical, MUD w/o ATG and MUD w/ ATG groups respectively. Cum-Inc of grade II-IV acute GVHD at day100 and chronic GVHD at 1 year was 27%, 40% and 49% (p=0.07) and 13%, 51% and 33% (p<0.001) in the haploidentical, MUD w/o ATG and MUD w/ ATG groups, respectively. On multivariate analysis (MVA) higher risk of chronic GVHD was seen in MUD w/o ATG (RR=5.85, 95%CI 3.96-8.64; p<0.0001) and MUD w/ ATG (RR=3.64, 95%CI 2.37-5.59; p<0.0001) groups relative to the haploidentical cohort. The 3 year NRM was 17%, 22% and 26% in the haploidentical, MUD w/o ATG and MUD w/ ATG groups (p=0.08), respectively. On MVA a trend towards higher NRM was noted in MUD w/ ATG cohort, RR 1.54 (95%CI 0.98 - 2.41, p=0.06), relative to the haploidentical group. Among the haploidentical, MUD w/o ATG and MUD w/ ATG cohorts the 3 year Cum-Inc of rel/prog was 36% vs. 28% vs. 36%, PFS was 47% vs. 49% vs. 38% and OS was 60%, 62% and 50% (Figure), respectively. MVA demonstrated no significant difference between the three groups in terms of rel/prog (p=0.27) and PFS (p=0.07). Compared to the haploidentical group, the two MUD groups did not have a significantly different mortality risk (inverse of OS; p>0.05), but compared to MUD w/ ATG, the MUD w/o ATG pts had a reduced mortality risk (RR=0.67; p=0.001). We tested for a transplant center effect on survival and found none. Conclusion: With lower-intensity conditioning regimens the early (up to 3 years) survival outcomes are comparable between conventional MUD transplants (w/ or w/o ATG) and haploidentical HCT with PT-Cy approach. Chronic GVHD was significantly lower with haploidentical HCT. Prospective, randomized confirmation of these findings is necessary before wide spread adoption of haploidentical HCT over MUD transplants in lymphomas.
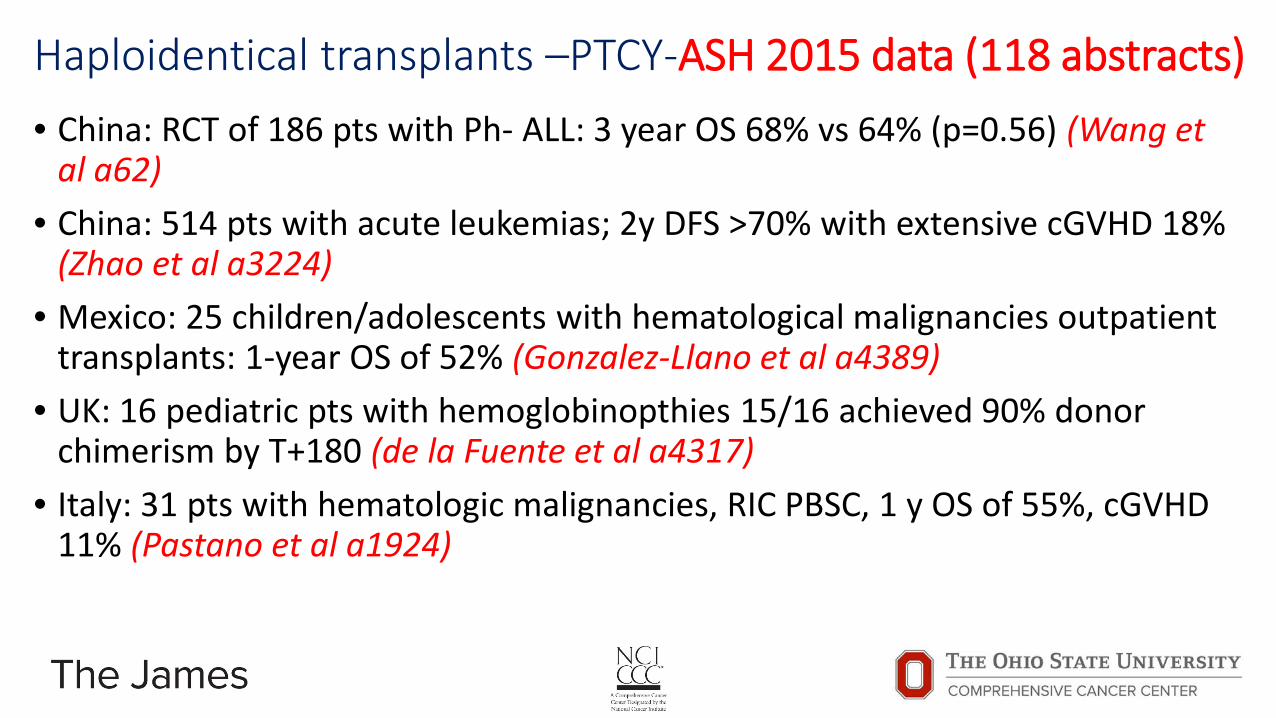
Haploidentical transplants –PTCY-ASH 2015 data (118 abstracts) • China: RCT of 186 pts with Ph- ALL: 3 year OS 68% vs 64% (p=0.56) (Wang et
al a62) • China: 514 pts with acute leukemias; 2y DFS >70% with extensive cGVHD 18%
(Zhao et al a3224) • Mexico: 25 children/adolescents with hematological malignancies outpatient
transplants: 1-year OS of 52% (Gonzalez-Llano et al a4389) • UK: 16 pediatric pts with hemoglobinopthies 15/16 achieved 90% donor
chimerism by T+180 (de la Fuente et al a4317) • Italy: 31 pts with hematologic malignancies, RIC PBSC, 1 y OS of 55%, cGVHD
11% (Pastano et al a1924)

PTCY- Beyond Haploidentical transplants Results of a Two-Arm Phase II Clinical Trial Using Post-Transplantation Cyclophosphamide for Prevention of Graft-Versus-Host Disease in Haploidentical and Mismatched Unrelated Donors Hematopoietic Stem-Cell Transplantation a152
Gaballa S et al. Abstract 152
Presenter
Presentation Notes
Allogeneic stem cell transplantation offers curative therapy for many patients (pts) with high-risk hematologic malignancies. Donor availability remains a major limitation for many pts. The introduction of high-dose post-transplant cyclophosphamide (PTCy) has significantly improved the outcomes of pts undergoing haploidentical (HAPLO) stem cell transplants. The choice between a HAPLO or a one-antigen HLA mismatched unrelated donor (9/10 MUD) for pts lacking an HLA-matched donor remains unclear. Methods: We conducted a prospective non-randomized phase 2 clinical trial with two parallel arms, HAPLO (n=60) and 9/10 MUD (n=46) transplants, for pts with advanced hematologic malignancies or aplastic anemia who lacked an HLA-matched unrelated donor type at 10 loci (HLA-A, -B, -C, -DRB1, and -DQB1) using a MEL-based reduced-intensity conditioning regimen. The regimen included a single intravenous dose of MEL 140 mg/m2 (day -7), thiotepa 5 mg/kg (day -6), and four daily IV doses of fludarabine 40 mg/m2 (day -5 to day -2) (FM140). Thiotepa was intermittently available and was replaced by total body irradiation at a dose of 2 Gy on day -1. Pts >55 years (yr) old or with significant comorbidities received a lower MEL dose (100 mg/m2) (FM100). All pts with CD20-positive lymphoma received rituximab (375 mg/m2) on days -13, -6, +1 and +8. GVHD prophylaxis consisted of PTCy 50 mg/kg on day +3 and +4, and tacrolimus and mycophenolate for 6 and 3 months (mo), respectively. The stem cell source was unmodified bone marrow for both arms. Results: Patient characteristics are shown in Table 1. The median follow-up duration was 24 mo in the HAPLO arm and 29 mo in the 9/10 MUD arm. The cumulative incidence (CI) of neutrophil (ANC) recovery at day 45 was 95% and 98% in the HAPLO and 9/10 MUD arm, respectively. The median time to ANC recovery was 18 days in both arms; the median time to platelet recovery was 25 days in the HAPLO arm and 28 days in the 9/10 MUD arm. Primary graft failure developed in two pts in the HAPLO arm (one due to anti-donor HLA antibodies) and one patient in the 9/10 MUD arm. One pt in both arms developed mixed donor chimerism at day 100; otherwise, all pts in both arms achieved full (>95%) donor chimerism. Bone marrow was the graft source in all pts except 2 in the HAPLO arm and 8 in the 9/10 MUD arm who received a peripheral blood graft. The 1-yr overall and progression free survival were 70% and 60%, respectively, in the HAPLO arm (Fig. 1A) and 60% and 47%, respectively, in the 9/10 MUD arm (Fig. 1B). Day 100 CI of grade II-IV aGVHD and III-IV aGVHD were 28% and 3%, respectively, in the HAPLO arm versus 33% and 13%, respectively, in the 9/10 MUD arm; the 2-yr CI of chronic extensive GVHD was 13% and 14% in the two groups, respectively. The 1-yr CI of non-relapse mortality was 21% in the HAPLO arm and 31% in the 9/10 MUD arm, while the 1-yr relapse rate was 19% and 25% in the two groups, respectively. Conclusions: This study establishes PTCy, tacrolimus, and mycophenolate as an effective regimen for GVHD prevention in mismatched transplantation using both haploidentical and mismatched unrelated donor sources. Melphalan-based reduced-intensity conditioning is an effective regimen for a broad range of hematologic malignancies. Prospective randomized studies comparing haploidentical and unrelated donor sources are needed.

Haploidentical transplants –expanding donor availability • Historically less than 50% of pts who needed an allogenic transplant
would have an HLA 8/8 fully matched donor • Donor availability/eligibility remains a limitation in haploidentical donors • Body weight limits umbilical blood (UCB) grafts as an option • Report from MSKCC: 15% pts has no UCB graft options and 20% had no
haplo graft options (compromised donor availability was common in minority patients) Ksouri at al. ASH 2015 a2027
• Potential for HLA-mismatched URD with PTCY remains to be explored

PTCY- HLA-mismatched MUDs = Everyone has a donor!! Nonmyeloablative (NMA), HLA-Mismatched Unrelated Donor (mMUD) BMT with High-Dose Posttransplantation Cyclophosphamide (PTCy) Has Outcomes Similar to Matched BMT a2002
Kasamon YL at al. Abstract 2002
Presenter
Presentation Notes
Background: The results of NMA, related HLA-haploidentical (haplo) BMT with PTCy are comparable to matched BMT (Blood 2015;125;3024). However, patients (pts) may lack related donors, often because of familial disease susceptibility or cytotoxic antibodies against donor HLA molecules. Although partially HLA-mMUD BMT could be considered if a MUD is unavailable, mismatches > 1 HLA antigen have historically been associated with unacceptable rates of GVHD, graft failure, and nonrelapse mortality (NRM). We hypothesized that PTCy may overcome this HLA barrier. Methods: We developed a prospective, regimen-finding study of NMA BMT for hematologic malignancies pts without an acceptable matched or first-degree related haplo donor. The objective was to identify a regimen with ≤ 25% severe acute GVHD and ≤ 20% NRM by day 100, using mMUD's or non-first-degree relatives. Results of mMUD BMT with our standard conditioning are presented. Pt eligibility included age 0.5-75 years, no suitable family donor, ECOG PS ≤ 2, LVEF ≥ 35%, FEV1 and FVC ≥ 40% predicted, and adequate hepatic function. The mismatched donor shared ≥ 5/10 HLA alleles (based on molecular typing of HLA-A, -B, -Cw, -DRB1, and -DQB1) with ≥ 1 allele matched for a HLA class I gene and ≥ 1 allele matched for a class II gene. Donors matched at ≥ 1 allele at each locus were prioritized, followed by donors having the fewest number of mismatched loci. All pts received fludarabine (30 mg/m2 IV days -6 to -2), Cy (14.5 mg/kg IV days -6 and -5), TBI (200 cGy day -1) and T-cell replete bone marrow. GVHD prophylaxis consisted of high-dose PTCy (50 mg/kg IV days 3 and 4), mycophenolate mofetil on days 5-35, and either sirolimus (15 pts) or tacrolimus (1 pt) on days 5-180. GCSF was given from day 5 until neutrophil recovery. Safety was continuously monitored. Results: Sixteen pts (median age 57, range 37-66) received mMUD BMT on this study from 7/2011-6/2014 (9 AML cases, 4 MDS or MPN, 1 CML, 2 PTCL). Major reasons for utilizing a mMUD included the absence of an adult haplo first-degree relative and the presence of prohibitive donor-specific anti-HLA antibodies (DSA's). The unrelated grafts had a median of 2 HLA mismatches and included three 7/10 matches, one 6/10 match, and one 5/10 match. HLA-C mismatch was present in 10 grafts (63%) and complete DP mismatch in 6 (38%).By revised Disease Risk Index, 25% of pts were high risk, 69% intermediate risk, and 6% low risk; 69% were in CR at BMT. The median graft doses were 3.36 x 108 total nucleated cells/kg and 3.87 x 107 CD3+ cells/kg. All pts engrafted, and there were no non-relapse deaths or prohibitive toxicities. By competing-risk analysis, the estimated cumulative incidence (CuI) of neutrophil recovery was 100% by day 29, with a median of 20 (range 14-29) days. The CuI of platelet recovery ≥ 20,000/µL was 100% by day 46, with a median of 32 (range 12-46) days. By day 60, 14/15 (93%) evaluable pts achieved full donor chimerism in either CD3+ or unsorted cells. Notably, there were no cases of acute grade 3-4 GVHD. Acute grade ≥ 2 GVHD was limited to 2 cases of skin-only grade 2 GVHD and 1 case of grade 2 skin and ungradable visceral GVHD. By competing-risk analysis, the estimated CuI of acute grade 2 GVHD was 12% at day 100 (90% CI, 0-27%) and 19% at day 180 (90% CI, 2-37%)(Fig A). The CuI of any chronic GVHD at 1 and 2 years was 7% (90% CI, 0-18%)(Fig A). Critical illness prior to relapse was limited to 1 case of sepsis which resolved. With a 3-year median follow-up, the probability of PFS was 56% at 1 year and 50% at 3 years (Fig B). The estimated CuI of relapse was 44% at 1 year. Median OS has not been reached, with an estimated 1 year and 3 year OS of 68% (Fig B). Conclusion: These results suggest that virtually no pt should be denied allogeneic BMT because of lack of an HLA-matched or haplo donor. mMUD searches were successful in pts with DSA's that were too high for desensitization.

Prevention of GVHD Randomized Trial on GvHD Prophylaxis with or without Anti-Human T-Lymphocyte Immunoglobulin ATG-Fresenius (ATG-F) in Allogeneic Hematopoietic Cell Transplantation from Matched Unrelated Donors: Final Long-Term Results after 8.6 Years Median Follow-up a853
• Incidence of extensive chronic GvHD after 8 years was 13.5% in the ATG-F group vs 51.8% in the control group (p<0.0001).
• The 8-year rates: NRM 20.5% vs 34.0% (p=0.15), relapse 35.2% vs 29.9% (p=0.54), relapse mortality 30.8% vs 28.8% (p=0.90), DFS 44.3% vs 36.1% (p=0.60), and OS 48.7% vs 36.8% (p=0.31)
• Support results from a Canadian RCT in 203 pts (13% vs 29% severe cGVHD) (Walker et al. Lancet Oncol Dec 2015)
Finke J at al. Abstract 853
Presenter
Presentation Notes
Abstract Background: Previously, in 201 adult patients with allogeneic hematopoietic cell transplantation from matched unrelated donors, we demonstrated that the addition of ATG-F to standard cyclosporine, methotrexate GvHD prophylaxis (control) significantly reduces acute and chronic GvHD without negatively affecting relapse and survival [1,2,3]. Methods: Now, we present final results after an extended follow-up (median 8.6, Q1 8.0, Q3 9.3 years) with regard to chronic GvHD, non-relapse mortality (NRM), relapse, relapse mortality, disease-free survival (DFS) and overall survival (OS). Additionally, we analyse the effect of ATG-F vs control on the composite endpoint severe GvHD (acute GvHD III-IV, extensive chronic GvHD) and relapse-free survival, and on time under immunosuppressive therapy. Since mortality within the first year after transplantation is usually high, we also analyse conditional survival, i.e. the OS probability after having survived 1 and 2 years after transplantation. Results: The incidence of extensive chronic GvHD after 8 years was 13.5% in the ATG-F group vs 51.8% in the control group (p<0.0001). The 8-year rates with respect to outcome were: NRM 20.5% vs 34.0% (p=0.15), relapse 35.2% vs 29.9% (p=0.54), relapse mortality 30.8% vs 28.8% (p=0.90), DFS 44.3% vs 36.1% (p=0.60), and OS 48.7% vs 36.8% (p=0.31), ATG-F vs control, respectively. ATG-F substantially increased the combined severe GvHD/relapse-free survival rate. The rates were 48.5% vs 20.4% after 1 year and 33.6% vs 13.0% after 8 years (p=0.0003), ATG-F vs control, respectively (see figure). The probability of being alive and free of immunosuppressive therapy was 46.8% in the ATG-F group and 11.2% in the control group at 8 years (p=0.0002). The survival probabilities increased when patients had survived the first year. The conditional 8 years-survival probability increased in the ATG-F group from 48.7% (unconditional) to 70.6% and 80.9% (conditional on having survived 1 and 2 years after transplantation), and in the control group from 36.8% (unconditional) to 58.5% and 71.7% (conditional on having survived 1 and 2 years after transplantation). Conclusion: The long-term follow-up of 8.6 years shows that ATG-F GvHD prophylaxis provides a sustained protective effect without increasing relapse and compromising survival. ATG-F in addition to standard cyclosporine, methotrexate as GvHD prophylaxis results in significantly improved severe GvHD/relapse-free survival. Furthermore, the stable results from our prospective trial after an extended long-term follow-up demonstrate that the choice to use ATG-F in unrelated donor transplantation after myeloablative conditioning substantially increases the probability of surviving free of immunosuppressive therapy, and thus reduces the risk associated with long-term immunosuppression.

Prevention of Relapse after HCT Updated Efficacy and Safety Data from the AETHERA Trial of Consolidation with Brentuximab Vedotin after Autologous Stem Cell Transplant (ASCT) in Hodgkin Lymphoma Patients at High Risk of Relapse a3172
Sweetenham at al. a3172 Moskowitz, at al. Lancet 2015. 385: 1853-62
PFS BV Placebo 2 y 65% 45% 3 y 61% 43%
Presenter
Presentation Notes
Introduction The AETHERA trial is a phase 3, randomized, placebo-controlled trial (ClinicalTrials.gov #NCT01100502), which evaluated whether post-ASCT consolidation treatment with brentuximab vedotin (BV) could prevent disease progression in Hodgkin lymphoma (HL) patients at high risk for relapse. The study met its primary endpoint: significant improvement in progression-free survival (PFS) per independent review with BV versus placebo (hazard ratio [HR]=0.57, P=0.001) (Moskowitz, 2015). The 2 most common adverse events (AEs) in the BV- treatment group were peripheral sensory neuropathy (56%) and neutropenia (35%). We are presenting updated efficacy and safety data after approximately 1 additional year of follow-up after the primary analysis. Methods Patients were randomized to receive BV 1.8 mg/kg q3wk or placebo for 16 cycles (approximately 12 months), 30–45 days after transplantation. Randomization was stratified by response to frontline therapy and by best clinical response to pre-ASCT salvage therapy. Patients whose disease had progressed after salvage treatment were not eligible. Patients received CT scans quarterly for the first year and then at 18 and 24 months during long-term follow-up (LTFU). Clinical lymphoma assessments were performed at each cycle of treatment, quarterly during the first year of LTFU, and every 6 months thereafter. AEs were collected for 30 days after the end of treatment, except for peripheral neuropathies and secondary malignancies, which were followed throughout LTFU. Clinical responses to subsequent BV treatment received after progression were also recorded. Results A total of 329 patients were randomized to the BV- (n=165) or placebo- (n=164) treatment arms. Median PFS per investigator assessment was not reached (95% CI not estimable [NE]–NE) in the BV arm and was 15.8 months (95% CI 8.5–44.0) in the placebo arm (HR=0.52, 95% CI 0.37–0.71). A sustained plateau with substantial separation is evident between both treatment groups, with improved PFS at 3-years post-randomization with BV consolidation versus placebo (Figure). The 3-year PFS rate was 61% (95% CI 52–68) for the BV arm and 43% (95% CI 36-51) for the placebo arm. Six PFS events (2 progressions and 4 deaths) were recorded after the 24-month evaluation period in the BV arm and 3 in the placebo arm (2 progressions and 1 death). The HR for PFS per independent review was 0.58 (95% CI 0.41–0.82). No new secondary malignancies have been observed since the primary analysis. The number of cases were comparable between the 2 treatment arms (n=4 BV, n=2 placebo). Malignancies on the BV arm included bladder cancer, lung cancer, pancreatic cancer, and myelodysplastic syndrome (n=1 each). In the placebo arm, secondary malignancies included mantle cell lymphoma and myelodysplastic syndrome (n=1 each). Among the 112 patients on the BV arm who experienced treatment-emergent peripheral neuropathy based on a Standardised Medical Dictionary for Regulatory Activities (MedDRA) Query (SMQ) analysis, 99 patients (88%) experienced some improvement (23%) or complete resolution (65%) of neuropathy symptoms at the time of analysis. Discontinuation of treatment due to an AE occurred in 54 patients (33%) on the BV arm, most commonly due to peripheral sensory and motor neuropathies (14% and 7%, respectively). Patients who discontinued treatment as a result of an AE received a median of 9.5 cycles (range, 1 to 15) on the BV arm. The 2-year PFS rate in these patients was 69% (95% CI 54–79) versus 82% (95% CI 71–89) for patients who completed all 16 treatment cycles. Conclusions Consolidation treatment with BV in HL patients at high risk of relapse after ASCT showed an improvement in PFS versus placebo, approximately 3 years since the last patient was randomized. Kaplan-Meier analysis of PFS per investigator assessment showed a continued benefit of BV consolidation. No additional secondary malignancies have been observed in either treatment arm and most patients experienced resolution of peripheral neuropathy symptoms. We are currently analyzing clinical responses to BV treatment after disease progression.

Too old for transplant ??-ASH 2015 • CIBMTR analysis: Outcome of patients 65 years and older (n=699) with MDS
receiving Allo-HCT similar to patients 55-64 years of age (n=592) Attalah, at al. a193
• Université de Montréal: 90 pts ≥ 60 y received auto-HCT for lymphoma. Age ≥65 year was not associated with an increase TRM. Estimated 5 y OS is 62% and PFS is 40%. TRM only 1% at 100 days and 2% at 1 y Lemieux, at al. a3171
• Germany: 187 pts with AML/MDS ≥ 60 y. OS at 3 y 35%. NRM and relapse at 1 y were 37% and 22%. Disease status and ECOG PS but not age were predictors of poor outcomes Pohlen at al. a2025
• EBMT: 345 pts had allo-HCT for MDS/sAML. 3y OS 33%. Only Karnofsy PS and CMV positivity influenced survival Heidenreich, at al. a4390
Presenter
Presentation Notes
INTRODUCTION: Despite recent advances in treatment for MDS, allogeneic hematopoietic stem cell transplantation (alloHCT) remains the only curative therapy. Historically, patients (pts) 65 and older with Medicare did not have coverage for HCT. On August 4th 2010, the Centers for Medicare and Medicaid services (CMS) established coverage for HCT for MDS through coverage with evidence development (CED). A Center for International Bone MarrowTransplant Research (CIBMTR) study comparing outcomes of pts 55-64 vs. 65 and older was approved. Herein we report the survival outcomes of the first 688 pts enrolled on the study. RESULTS: From 12/15/2010 to 5/14/2014, 688 pts 65 years and older (65+) underwent alloHCT for MDS compared with 592 pts 55-64 years (55-64). Median follow-up was 12 and 18 months for the 65+ and 55-64 group respectively. Median age was 68 and 61 for the 65+ and 55-64 group respectively. In the 65+ group, 76%, 22% and 2% were ages 65-69, 70-74 and > 74 years old. At the time of diagnosis, 30%, 10%, 42% were diagnosed with RA/RARS/RCMD/RCMDRS/5q-, CMML and RAEB respectively. The IPSS score at diagnosis was Low risk/intermediate-1 and intermediate-2/high risk in 39% and 31% respectively, and 23% had t-MDS. In the 55-64group, 43% and 57% were 55-59 and 60-64 years old respectively. Otherwise, patient and disease characteristics were similar in both groups. More patients in the 55-64 group compared to 65+ group received a myeloablativealloHCT (49% vs. 29%). The donor was an HLA identical sibling in 24% vs. 34% in the 65+ vs. the 55-64 groups. Because of confounding between age and selection of transplant procedures (including preparative regimen intensity, graft source, gvhd prophylaxis) we chose to adjust only for patient and disease characteristics in the multivariate analysis (MVA). Age group 65+ vs. 55-64 had no significant impact on 100-day mortality (HR 1.26; CI 0.91-1.75 p=0.16) or overall survival (HR 1.14; CI 0.98-1.33 p=0.1) in the MVA. The adjusted 100 day survival was 84% vs. 87%, one year survival was 60% vs. 56% and 2 year survival was 42% vs. 46% in the 65+ group vs. 55-64group respectively. As expected, MVA for 100 day mortality identified that poor cytogenetics (HR 1.85; CI 1.28-2.68) compared to good cytogenetics, patients with stable disease/no response to therapy (HR 3.35; CI 1.59-7.07), disease progression/relapsed disease (HR 2.91; CI 1.13-7.51), patients who did not receive any therapy prior to preparative regimen (HR 2.9; CI 1.17-7.21) compared to patients in complete remission and platelet count <50x109/L (H1.68; CI 1.17-2.43) compared to platelet ≥ 50 x 109/L at diagnosis were independently associated with worse outcome. MVA for overall survival identified that, 11-20% blasts in bone marrow at time of preparative regimen (HR 1.58; CI 1.24-2.03) compared to < 5% blasts, poor cytogenetics (HR 1.68; CI 1.4-2.01) compared to good cytogenetics and Sorror comorbidity index ≥ 4 (HR 1.59; CI 1.27-1.99) compared to Sorror comorbidity index 0 were independently associated with worse outcome. CONCLUSION: In patients who are eligible for alloHCT, there was no difference in 100 day mortality or overall survival for patients 55-64 compared to patients 65 years and older. Age alone should not be a determinant for alloHCT eligibility.

“Surveillance imaging” doesn’t improve survival in lymphoma after auto-HCT-ASH 2015 • Retrospective analysis of
194 of DLBCL patients after auto-HCT: radiographic vs clinical relapse PFS/OS 218/643 vs 402/615 d (p=NS) Epperla, at al. a4360
• Retrospective analysis of 148 of HL patients after auto-HCT: radiographic vs clinical relapse PFS/OS 426/1270 vs 318/931 d (p=NS) Kapke, at al. a3169
Presenter
Presentation Notes
INTRODUCTION: Despite recent advances in treatment for MDS, allogeneic hematopoietic stem cell transplantation (alloHCT) remains the only curative therapy. Historically, patients (pts) 65 and older with Medicare did not have coverage for HCT. On August 4th 2010, the Centers for Medicare and Medicaid services (CMS) established coverage for HCT for MDS through coverage with evidence development (CED). A Center for International Bone MarrowTransplant Research (CIBMTR) study comparing outcomes of pts 55-64 vs. 65 and older was approved. Herein we report the survival outcomes of the first 688 pts enrolled on the study. RESULTS: From 12/15/2010 to 5/14/2014, 688 pts 65 years and older (65+) underwent alloHCT for MDS compared with 592 pts 55-64 years (55-64). Median follow-up was 12 and 18 months for the 65+ and 55-64 group respectively. Median age was 68 and 61 for the 65+ and 55-64 group respectively. In the 65+ group, 76%, 22% and 2% were ages 65-69, 70-74 and > 74 years old. At the time of diagnosis, 30%, 10%, 42% were diagnosed with RA/RARS/RCMD/RCMDRS/5q-, CMML and RAEB respectively. The IPSS score at diagnosis was Low risk/intermediate-1 and intermediate-2/high risk in 39% and 31% respectively, and 23% had t-MDS. In the 55-64group, 43% and 57% were 55-59 and 60-64 years old respectively. Otherwise, patient and disease characteristics were similar in both groups. More patients in the 55-64 group compared to 65+ group received a myeloablativealloHCT (49% vs. 29%). The donor was an HLA identical sibling in 24% vs. 34% in the 65+ vs. the 55-64 groups. Because of confounding between age and selection of transplant procedures (including preparative regimen intensity, graft source, gvhd prophylaxis) we chose to adjust only for patient and disease characteristics in the multivariate analysis (MVA). Age group 65+ vs. 55-64 had no significant impact on 100-day mortality (HR 1.26; CI 0.91-1.75 p=0.16) or overall survival (HR 1.14; CI 0.98-1.33 p=0.1) in the MVA. The adjusted 100 day survival was 84% vs. 87%, one year survival was 60% vs. 56% and 2 year survival was 42% vs. 46% in the 65+ group vs. 55-64group respectively. As expected, MVA for 100 day mortality identified that poor cytogenetics (HR 1.85; CI 1.28-2.68) compared to good cytogenetics, patients with stable disease/no response to therapy (HR 3.35; CI 1.59-7.07), disease progression/relapsed disease (HR 2.91; CI 1.13-7.51), patients who did not receive any therapy prior to preparative regimen (HR 2.9; CI 1.17-7.21) compared to patients in complete remission and platelet count <50x109/L (H1.68; CI 1.17-2.43) compared to platelet ≥ 50 x 109/L at diagnosis were independently associated with worse outcome. MVA for overall survival identified that, 11-20% blasts in bone marrow at time of preparative regimen (HR 1.58; CI 1.24-2.03) compared to < 5% blasts, poor cytogenetics (HR 1.68; CI 1.4-2.01) compared to good cytogenetics and Sorror comorbidity index ≥ 4 (HR 1.59; CI 1.27-1.99) compared to Sorror comorbidity index 0 were independently associated with worse outcome. CONCLUSION: In patients who are eligible for alloHCT, there was no difference in 100 day mortality or overall survival for patients 55-64 compared to patients 65 years and older. Age alone should not be a determinant for alloHCT eligibility.

What is the upper age limit for marrow or peripheral blood stem cell transplant?
A. 60 B. 70 C. 75 D. 90 E. Probably not 90, but I don’t
know!
A. B. C. D. E.
0% 0% 0%0%0%

In 2016, how many % patients in the U.S. would have an available donor for allogeneic stem cell transplant?
A. 30% B. 40% C. 50% D. 70% E. >80%
A. B. C. D. E.
0% 0% 0%0%0%

Patients with myeloma should be referred to transplant:
A. Upon diagnosis B. Upon progression C. Upon diagnosis and
progression D. Only if ≤ 65 years
old E. After starting
treatment A. B. C. D. E.
0% 0% 0%0%0%

HCT Take-home messages-ASH 2015 • Autologous stem cell transplantation should be considered in all patients with
myeloma; upfront and on progression • Advanced age is no longer a contraindication for transplant • Allogeneic transplant are becoming safer – less toxic regimens and better
GVHD prophylaxis (evolving role of HaploHCT and PTCY) • More than 80% of patients now has a donor available for allogeneic transplant • Transplant should be considered early in relapsed lymphoma and or high-risk
lymphomas (myc or “double hit”, mantle, peripheral T-cell lymphomas) • Brentuximab maintenance should be considered in relapsed Hodgkin’s
lymphoma after autologous transplant

Appropriate referrals for Transplant • All patients with myeloma upon diagnosis and upon progression • All adult patients with acute leukemias • Patients with myelodysplastic syndrome • Patients with CP-CML failing first line TKI or any advanced phase CML • Patients with MPD/MF • Patients with relapsed/refractory or high-risk lymphomas (myc or “double hit”,
mantle, peripheral T-cell lymphomas) • Patients with CTCL who are needing systemic treatment • Unexplained cytopenias • Relapsed germ-cell tumors • All patients should be considered for transplant regardless of age!

Thank you Questions?


















