Ohio State's 2016 ASH Review - ASH Review 2015Acute Leukemias and MDS
53
ASH Review 2015 Acute Leukemias and MDS Alice Mims, MD, MSCR January 22, 2016
-
Upload
osuccc-james -
Category
Healthcare
-
view
853 -
download
1
Transcript of Ohio State's 2016 ASH Review - ASH Review 2015Acute Leukemias and MDS

ASH Review 2015 Acute Leukemias and
MDS
Alice Mims, MD, MSCR January 22, 2016
Presenter
Presentation Notes
Hi everyone, thank you so much for coming today. I am going to address the ASH updates and new findings on the topics of acute leukemia and MDS.
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Objectives
Acute Myeloid Leukemia Novel targeted therapeutics
Acute Lymphocytic Leukemia Updates on Immunotherapies
Myelodysplastic Sydrome Improvement of cytopenias with new treatments in
low-risk disease
2
Presenter
Presentation Notes
The topics that I am going to cover include AML in which we will discuss exciting findings with novel targeted therapeutics – updates in FLT inhibition and also discuss IDH inhibitors. For ALL, we will discuss updates with the addition of immunotherapies to standard treatment as well as stand-alone therapy. Lastly, will discuss with MDS, early findings with novel therapeutics that have improved cytopenias in low-risks disease.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Acute Myeloid Leukemia

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Cytogenetic and Molecular Subsets in Younger AML patients
4
Grimwade, et al. Blood 2016;127: 29-41
Presenter
Presentation Notes
Before we delve into the abstracts, I wanted to show this piechart as an example of the complexity and heterogeneity of AML that is being discovered with NGS and other newer techniques. This figure was recently published in Blood which depicts just in younger AML patient population, the cytogenetic and molecular subsets which is continuously being updated. There are many challenges that are ongoing in regards to prognostication, determining dominant clones, disease monitoring – Minimal Residual Disease, and most importantly, personalizing treatment. At ASH there were many presentations in regards to MRD and clonality in AML, however as these findings are still early and not practice changing, I am going to focus on upcoming novel therapeutics. However, I’m encouraged by the progress we are making in regards to AML, hopefully the treatment landscape in 10 years will be much different than the limited options standard 7+3, hypomethylating agents, and supportive care.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
A Phase III Randomized Double-blinded Study Of Chemotherapy +/- Midostaurin (PKC412)
In Newly Diagnosed Adults age 18-60 with FLT3 Mutated Acute Myeloid Leukemia (AML)
Participants: AMLSG, SAL, OSHO, CALGB/ALLIANCE, GIMEMA, SWOG, EGOG, PETHEMA, CETLAM, EORTC, NCIC
CTEP sponsored, Novartis provided drug and sponsored outside North America, and Alliance (formerly CALGB) chaired study, collected data and performed analysis
Richard M. Stone, Sumithra Mandrekar, Ben L Sanford, Susan Geyer, Clara D. Bloomfield, Konstanze Dohner, Christian Thiede, Guido Marcucci, Francesco Lo Coco, Rebecca B. Klisovic, Andrew Wei, Jorge Sierra, Miguel A. Sanz, Joseph M. Brandwein, Theo de Witte, Dietger Niederwieser, Frederic R. Appelbaum, Bruno C. Medeiros, Martin S Tallman, Jurgen Krauter, Richard F. Schlenk, Arnold Ganser, Hubert Serve, Gerhard Ehninger, Sergio Amadori, Richard A. Larson, and Hartmut Dohner
Plenary Abstract # 6
Presenter
Presentation Notes
The first being exciting data in regards to FLT3 inhibition as prior studies have not been as encouraging- which may be due to improvements as newer agents are being developed, which are more specific in their targets. This abstract, “A Phase II Randomized Double Blind Study of Chemotherapy +/- Midostaurin in newly diagnosed adults ages 18-60 with FLT3 mutated AML” was presented at the plenary session by Dr. Rich Stone and was run through the Alliance with intergroup and international participation. The study used the MKI midostaurin or PKC412 versus placebo added to standard of care and followed by maintenance.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
FLT3 Structure and Activating Mutations
5-10%
Litzow MR. Blood. 2005;106:3331-3332.
Presenter
Presentation Notes
FLT3 mutations occur in 25-30% of patients with the standards that are being tested for routinely being Internal Tandem Duplication that result in ligand-dependent activation of FLT3 receptor and a proliferative signal and Tyrosine Kinase Domain point mutations may result in tyrosine kinase activation in 5-10% of patients. ITD mutations are known to have a high risk of relapse (2 year PFS of 20%) and overall poor prognosis (4 year OS of 20%). With TKD, these mutations do not seem to convey same overall poor prognosis.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
RATIFY: Study Design
7
Double-blind, placebo-controlled, randomized phase III study
– Primary endpoint: OS (not censored for SCT)
– Secondary endpoint: EFS
18-60 yrs of age with
FLT3-mutated (non-APL)
AML (N = 717)
Daunorubicin 60 mg/m2 IVP D1-3 +
Cytarabine 200 mg/m2/d IVCI D1-7 +
Midostaurin 50 mg PO BID D8-21
(n= 360)
Daunorubicin 60 mg/m2 IVP D1-3 +
Cytarabine 200 mg/m2/d IVCI D1-7 +
Placebo D8-21
(n = 357)
Cytarabine 3 g/m2 over 3h q12h
D1,3,5 + Midostaurin
50 mg PO BID D8-21 (n = 231)
Cytarabine 3 g/m2 over 3h q12h
D1,3,5 + Placebo
D8-21 (n = 210)
Midostaurin 50 mg PO BID D1-28
(n = 120)
Placebo D1-28
(n = 85)
Stratified by ITD/TKD;
randomized
Induction* (1-2 cycles)
Consolidation (up to 4 cycles)
Maintenance (12 cycles)
CR
CR
*Hydroxyurea allowed for ≤ 5 days prior to induction therapy.
Presenter
Presentation Notes
This study was performed in patients with both types of FLT3 mutations – stratified by either ITD or TKD, Ages 18-60, normal end-organ function who were candidates for intensive chemotherapy. FLT3 mutation was documented prior to enrollment, and centrally determined at 7 academic labs around the globe and showed the ability to be able to perform trials such as this as results were able to return within 48 hours. Up to 5 days of hydroxyurea allowed prior to start of treatment while awaiting results of mutation analysis The study was activated in May 2008 with completed accrual in Oct 2011. There were 3,279 patients screened and 27% of those screened were enrolled at 717 patients. This was a double-blind, placebo controlled randomized Phase III study with the primary endpt assessing OS (not censored for SCT) and secondary endpoint of EFS. Patients were treated with standard induction chemotherapy with daunorubicin at 60mg/m2 and cytarabine 200mg/m2 with midostaurin 50mg po bid or placebo given orally on Days 8-21. Patients could undergo second induction if necessary to achieve CR and those that did, went on to 4 cycles of high-dose cytarabine consolidation with midostaurin vs placebo on Days 8-21 again. These was then followed by maintenance of midostaurin or placebo Days 1-28 for 12 cycles. As you can see, the numbers greatly decreased over time which had a lot to do with the numbers who went on to receive stem cell transplant.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Patient Characteristics
MIDO
(N=360) PBO
(N=357) p value
Age (years), median (range) 47.1
(19.0-100.2) 48.6
(18.0-60.9) 0.27
Gender 0.045 Female 187 (51.9%) 212 (59.4%) Male 173 (48.1%) 145 (40.6%) FLT3 Stratification Group 0.995 FLT3 TKD (No ITD) 81 (22.5%) 81 (22.7%) ITD Allelic ratio <0.7 (+/- FLT3 TKD) 171 (47.5%) 170 (47.6%)
ITD Allelic ratio ≥0.7 (+/- FLT3 TKD) 108 (30.0%) 106 (29.7%)
Presenter
Presentation Notes
As you can see with the patient characteristics, there no clear differences in regards to age or FLT3 mutational group stratification. There were lightly more females in the placebo group versus males in the midostaurin group. For the ITD patients, those with an allelic ration > or equal to 0.7 were considered high expressers versus those with ratios <0.7 that were considered low expressers.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
RATIFY: Safety
Grade 3/4 Nonhematologic AEs (≥ 10% Pts), % Midostaurin
+ Chemo (n = 360)
Placebo + Chemo (n = 357)
P Value
Febrile neutropenia 81 82 .92 Infection 40 38 .49 Diarrhea 15 16 1.00 Hypokalemia 13 17 .17 Pain 13 13 .91 Rash/desquamation 13 8 .02 ALT/SGPT 12 9 .23 Fatigue (asthenia, lethargy, malaise) 9 11 .53
Deaths: 5% (18/360) in midostaurin arm vs 5.3% (19/357) in placebo; leading causes: infection (4 midostaurin, 7 placebo), pneumonitis (3 midostaurin, 0 placebo), hemorrhage, CNS (1 midostaurin, 2 placebo)
Presenter
Presentation Notes
In regards to safety, Grade ¾ non-heme toxicities were same in the midostaurin versus placebo group except a few more rashes were seen in the midostaurin group at 13 versus 8. The death rate was similar in both groups with causes that would be expected in this patient population.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
RATIFY: Efficacy
Characteristic Midostaurin +
Chemo (n = 360)
Placebo + Chemo
(n = 357) P Value
Median OS, mos (range) 74.7 (31.7-NE) 25.6 (18.6-42.9)
4-yr OS, % (95% CI) Uncensored* Censored for SCT†
51.4 (46.0-57.0) 63.8 (56.0-71.0)
44.2 (39.0-50.0) 55.7 (47.0-63.0)
.0074
.04
SCT, n (%) Any time CR1 only
212 (59) 100 (28)
196 (55) 79 (22)
.28 .08
CR, n (%) By Day 60 In induction/consolidation
212 (59) 239 (66)
191 (53) 211 (59)
.15
.045
Median EFS, mos (range) By day 60 In induction/consolidation
8.0 (5.1-10.6) 11.3 (8.4-15.1)
3.0 (1.9-5.9) 6.1 (4.7-7.5)
.0025 .0002
DFS, mos (range) 25.9 (19.4-NE) 14.4 (11.0-22.2) .002
*HR: 0.77. †HR: 0.75.
Presenter
Presentation Notes
In regards to outcomes, the midostaurin group showed significant improvements in OS, EFS and DFS with increased 4 year OS in both uncensored population and for those censored for transplant; median OS was 74.7 months vs 25.6 months in the placebo group. CR rates appears to be similar in both groups looking at a cutoff of Day 60. Ability to undergo SCT at anytime during treatment or CR1 was similar across both groups.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
RATIFY: Outcomes by FLT3 Status
Longer OS shown in midostaurin arm in all FLT3 cohorts FLT3-ITD high, HR: 0.80 (95% CI: 0.57-1.12; P = .09) FLT3-ITD low, HR: 0.80 (95% CI, 0.59-1.10; P = .08) FLT3-TKD, HR: 0.65 (95% CI: 0.39-1.08; P = .05)
4-yr EFS rate was 28% with midostaurin vs 20% in placebo, regardless of FLT3 status
Presenter
Presentation Notes
Longer OS shown in the midostaurin arm in all 3 FLT3 cohorts regardless if high or low expressor of ITD or ITD vs TKD. The 4 year EFS rate was 28% with midostaurin vs 20% in the placebo group regardless of the FLT3 status.
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
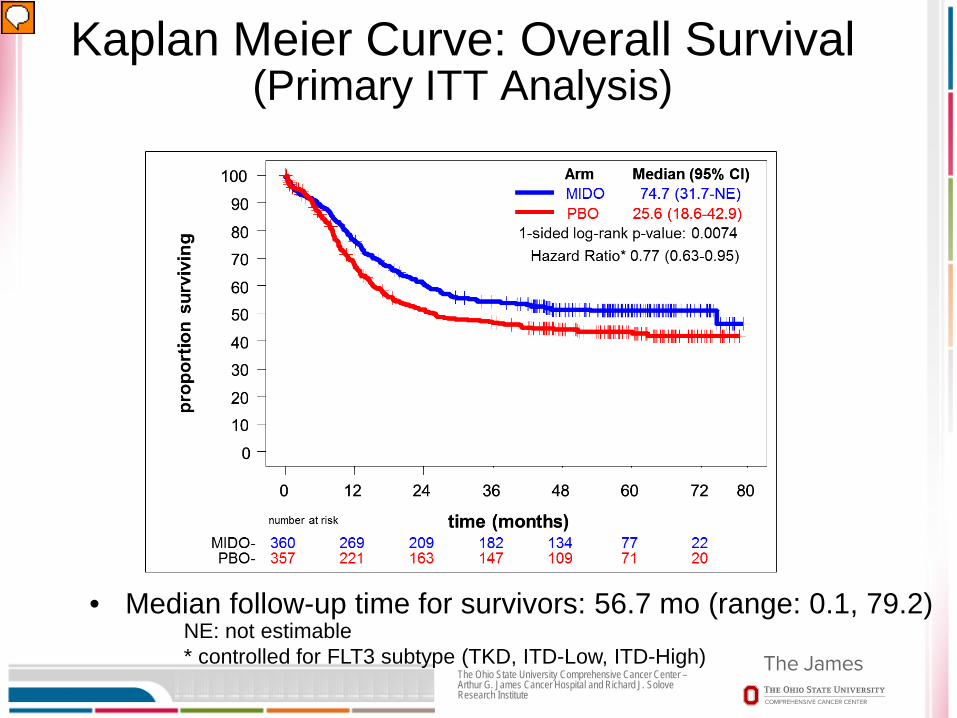
Kaplan Meier Curve: Overall Survival (Primary ITT Analysis)
• Median follow-up time for survivors: 56.7 mo (range: 0.1, 79.2) NE: not estimable * controlled for FLT3 subtype (TKD, ITD-Low, ITD-High)
Presenter
Presentation Notes
This Kaplan Meier Curve is a better visual representation that shows the primary intention to treat analysis in regards to OS and as you can see shows much improvement for the midostaurin group with a median OS 74.7 months versus 25.6 months with a very significant p value with median follow-up time for survivors of 56.7 months.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Kaplan Meier Curve: Overall Survival Censored at time of transplant
NE: not estimable * controlled for FLT3 subtype (TKD, ITD-Low, ITD-High)
Presenter
Presentation Notes
480 or 57% of patients underwent transplant during some point in their course of therapy (quite a high number). This Kaplan Meier Curve shows that if patients were censored at time of transplant – the OS rates are still improved in the midostaurin group with 5 year OS rate of 63.8% vs 55.7% in the placebo group.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
KM survival Curves for Overall Survival post-transplant
All Transplants SCT in/outside of CR1
NE: not estimable
Presenter
Presentation Notes
Looking at just the patients who underwent transplant – those in the midostaurin group had a better OS. However, in subgroup analysis – showed those not transplanedt in 1st remission had similar outcomes regardless if received midostaurin or placebo and did worse all together than those transplanted in CR1. If transplanted in CR1 – patients did better if on midostaurin arm better than the placebo arm.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
CALGB 10603: Conclusions
An International academic-industry collaborative AML study based on genotype at dx is feasible
Grade 3-5 adverse events were similar in each arm Midostaurin, a multi-targeted kinase inhibitor improves
OS and EFS when added to standard chemo with one year maintenance in newly diagnosed pts aged 18-60 with ITD and TKD FLT3 mutant AML
There was a high SCT rate but OS and EFS benefit was consistent in uncensored as well as censored analyses
Study investigators suggest midostaurin addition to current standard chemo with 1-yr subsequent maintenance as a new standard of care for these pts

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Safety and Efficacy of AG-221, a Potent Inhibitor of Mutant IDH2 That Promotes Differentiation of Myeloid
Cells in Patients with Advanced Hematologic Malignancies: Results of a Phase I/II Trial
16
Eytan M. Stein, Courtney DiNardo, Jessica K. Altman, Robert Collins, Daniel J. DeAngelo, Hagop M. Kantarjian, Mikkael A. Sekeres, Amir T. Fathi,
Ian W. Flinn, Arthur E. Frankel, Ross L. Levine, Bruno C. Medeiros, Manish R. Patel, Daniel Pollyea, Gail J. Roboz, Richard M. Stone, Ronan T. Swords,
Martin S. Tallman, Katharine Yen, Eyal C. Attar, Qiang Xu, Alessandra Tosolini, Jay M. Mei, Anjan Thakurta, Robert D. Knight, and Stéphane De Botton
Oral Abstract # 323
Presenter
Presentation Notes
Now I would like to move on to an update on the IDH2 inhibitor, AG-221 Phase I/II trial results as presented by Dr. Stein from MSK.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
IDH is an enzyme of the citric acid cycle
Mutant IDH2 produces 2-hydroxyglutarate (2-HG), which alters DNA methylation and leads to a block in cellular differentiation
AG-221 (CC-90007) is a selective, oral, potent inhibitor of the mutant IDH2 (mIDH2) enzyme
Isocitrate Dehydrogenase (IDH) Mutations as a Target in AML
Tumor Cell
Presenter
Presentation Notes
IDH is an enzyme of the citric acid cycle and when muated produces oncoprotein 2-hydroxyglutarate as opposed to alpha-ketoglutarate. There are two types of mutations: IDH1 and IDH2 names based on the locations with IDH1 occurring in the cytoplasm and IDH2 in the mitochondria. IDH1 mutations typically affect arginine 123 or arginine 172 or 140 in IDH2. IDH1 mutations occur at a frequency of 15% and IDH2 mutations 20% approximately. There are inhibitors to both enzymes with AG-120 targeting IDH1 and AG-221 (what is presented here) for IDH2 mutations – they are both selective, oral, potent inhibitors and seem to be having similar results in regards to response rates and length of responses with early data in patients with these mutations

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Phase 1/2 Study Design
18
Key Endpoints: • Safety, tolerability, MTD, DLTs • Response rates as assessed by local investigator per IWG criteria • Assessment of clinical activity
AG-221 100 mg PO QD
RR-AML (N ≈ 125)
Phase 2 Ongoing
Advanced heme malignancies with IDH2 mutation Continuous 28 day cycles Cumulative daily doses of 50-650 mg
Dose Escalation Completed
RR-AML age ≥60, or any age if relapsed post-BMT
RR-AML age <60, excluding pts relapsed post-BMT
Untreated AML pts age ≥60 who decline standard of care
Any hematologic malignancy ineligible for other arms
Expansion Phase I completed (n=25 pts per arm)
Presenter
Presentation Notes
For the Phase I/II study design for IDH2 inhibitor AG-221 – there was a dose escalation phase in patients with advanced heme malignancies with IDH2 mutations with continuous dosing with cumulative daily doses ranging from 50-650mg. This was followed by a dose expansion in Phase I with 4 subgroups (as above). Followed by a Phase 2 dosing at 100mg po daily in RR-AML with a current number of 125 patients. The key endpoints are safety, tolerability, MTD and DLTs.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute 19
Most Frequent Treatment Emergent Adverse Events (≥15% of patients)
Any Grade Grade ≥3 Preferred Term % Nausea 32 2 Diarrhea 28 3 Fatigue 28 6 Hyperbilirubinemia 27 10 Decreased appetite 27 3 Febrile neutropenia 27 26 Dyspnea 23 5 Pyrexia 23 4 Cough 22 0 Vomiting 20 1 Constipation 19 <1 Anemia 18 12 Peripheral edema 18 2 Thrombocytopenia 16 12
Presenter
Presentation Notes
Most frequent treatment emergent adverse event happening in > or= to 15% of patients, were GI in nature or those expected in AML patients – fever, anemia, thrombocytopenia. The hyperbilirubinemia appears to be transient and without actual resultant hepatotoxicity therefore at this time, these patients are monitored closely without dose de-escalation.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Dose-escalation and Serious Adverse Events
Dose-escalation Highest daily AG-221 dose: 650 mg Dose-escalation ended; MTD not reached Treatment Related Serious Adverse Events 23% of patients had treatment-related SAEs; most frequent were
differentiation syndrome (4%), leukocytosis (4%), and nausea (2%) Drug-related grade 5 SAEs:
atrial flutter (1) cardiac tamponade (1) pericardial effusion (1) respiratory failure (1)
20
Presenter
Presentation Notes
In dose escalation, the MTD was not reached but based on response felt 100mg po daily was an adequate dose to move forward with. 23% of patients had treatment-related SAEs – differentiation syndrome, leukocytosis and nausea. There were 4 grade 5 SAEs due to atrial flutter, cardiac tamponade, pericardial effusion and respiratory failure.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Differentiation Syndrome 21
• 21 days of AG-221 at 100 mg daily • Fever, oxygen requirement • Normal BAL
Courtesy Dr. Stephane De Botton
• Dexamethasone 10 mg BID for 15 days • Resolution of clinical symptoms • Patient achieves a complete remission
Presenter
Presentation Notes
Interestingly in a small subset of patients, there has been a differentiation syndrome that appears consistent with what we would typically see in APL patients. This typically happens close to the initiation of therapy over the first few weeks with increase in neutrophils or blast percentage and patients – some patients have been symptomatic with this and have responded well to steroids with resolution without recurrence after discontinuation of steroids after counts stabilization. This also shows that a rise in blast percentage does not necessarily mean that patients are progressing and should be kept on treatment if possible to see if this is an initial response to therapy.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Response 22
RR-AML (n = 159)
Untreated AML
(n = 24) MDS
(n = 14) All
(N = 209)
Overall Response (CR, CRp, CRi, mCR, PR)
59 (37%) [95%CI: 30%, 45%]
10 (42%) [22%, 63%]
7 (50%) [23%, 77%]
79 (38%) [31%, 45%]
CR 29 (18%) [95%CI: 13%, 25%]
4 (17%) [5%, 37%]
3 (21%) [5%, 51%]
37 (18%) [13%, 24%]
CRp 1 (1%) 1 (4%) 1 (7%) 3 (1%)
CRi 3 (2%) 0 0 3 (1%)
mCR 9 (6%) 1 (4%) 3 (21%) 14 (7%)
PR 17 (11%) 4 (17%) 0 22 (11%)
SD 72 (45%) 9 (38%) 6 (43%) 96 (46%)
PD 10 (6%) 1 (4%) 0 11 (5%)
Not evaluable 18 (11%) 4 (17%) 1 (7%) 23 (11%)
• Overall response by IDH mutation type: R140Q 36% / R172K 42% CR, complete response; CRp, CR with incomplete platelet recovery; CRi, CR with incomplete hematologic recovery; mCR, marrow CR; PR, partial response; SD, stable disease; PD, progressive disease
Presenter
Presentation Notes
ORR response rates were approximately 40% in all-comers with a 37% ORR in RR-AML, 42% in untreated Aml and 50% in MDS. CR rates were approximately 20% in all groups, PR 11% in all-comers and SD is approximately 40-45% of different groups and 46% in all0comers.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Duration of Response: RR-AML 23
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 2 4 6 8 10 12 14 16Time (months)
Sur
viva
l Pro
babi
lity
Censored
Median response duration: 6.9 months (95%CI 4.9, 9.7)
Responders: n=59 Median Tx duration: 6.8 months
(range: 1.8-18.0)
Presenter
Presentation Notes
The median duration of response in RR-AML groups was 6.9 months with 59 responders total with a median treatment duration of 6.8 months
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute 24
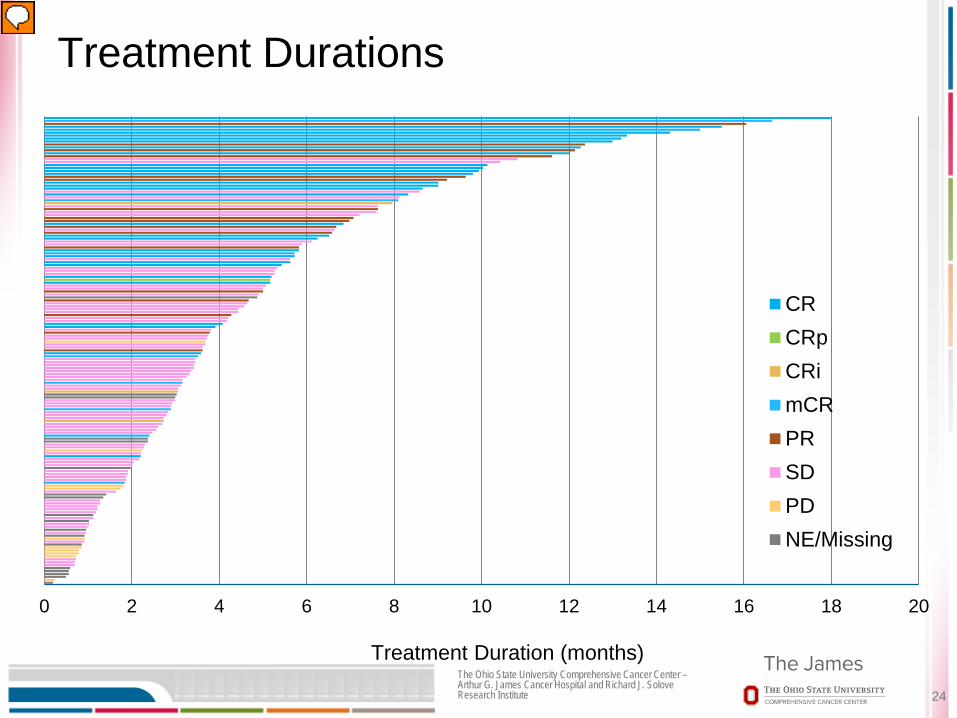
Treatment Durations
0 2 4 6 8 10 12 14 16 18 20
CRCRpCRimCRPRSDPDNE/Missing
Treatment Duration (months)
Presenter
Presentation Notes
As you can see the majority of patients who achieved CR are those who have been on therapy for a longer duration – showing the longer the patient can remain on drug, the more likely they are to obtain a complete CR.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Hematologic Improvement in a Subset of Patients with Stable Disease
25
RR-AML (N=159)
Overall Response 37% (n=59)
Stable Disease 45% (n=72)
ANC Increase >1K* 42% (30/72)
Platelet Increase >25K* 63% (19/30)
Platelet Increase >50K* 30% (9/30)
*Absolute increase regardless of baseline counts for ANC and platelets
Presenter
Presentation Notes
Also very interestingly is that in a subset of patients with stable disease (meaning no improvement or worsening of blast counts, they experienced improvements in the cytopenias. In 72 patients with SD, 30 patients had ANC increase to greater than 1000 and in these patients, 19 experienced a platelet increase >25,000 and 9 had a platelet increase greater than 50,000. This shows that patients even without clinical remission may be deriving clinical benefit with improvement of transfusion requirements. Patients have been allowed to stay on study if they are deriving clinical benefit.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Conclusions
AG-221 is generally well-tolerated Most frequent TEAEs were gastrointestinal events <10% of patients discontinued due to an adverse event Differentiation syndrome observed in a small subset of patients;
appears to be easily managed with steroids
Induces durable responses in patients with RR-AML: Overall response rate 37% Median duration of response to-date 6.9 months
Improvement in ANC and platelets was observed in a subset of RR-AML patients with stable disease
Randomized phase 3 study of AG-221 vs conventional care regimens initiated (IDHENTIFY trial; NCT02577406)
26

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
OSU 14169: Pacritinib and Induction chemotherapy in newly diagnosed AML with FLT3 mutations or pacritinib with decitabine with newly diagnosed unfit or relapsed/refractory AML PI: Dr. Tina Bhatnagar
OSU 14239: AG-120 (IDH1 inhibitor) PI: Dr. Alice Mims
OSU 14143: AG-221 (IDH2 inhibitor) in relapsed/refractory AML PI: Dr. Alice Mims
Upcoming: AG-120 or AG-221 combined with Induction in Newly diagnosed AML
Ongoing clinical trials at OSU
27

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Acute Lymphocytic Leukemia
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
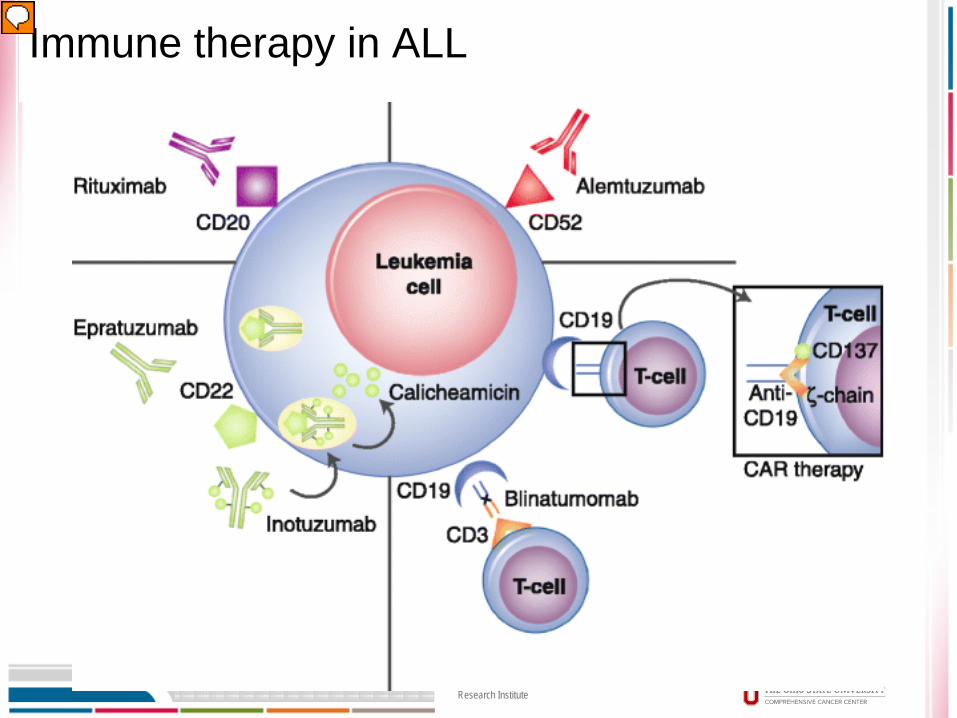
Immune therapy in ALL
Presenter
Presentation Notes
Currently, there is a lot of interest in immunomodulation or targeting B cells in B cell ALL with therapies such as monoclonal antibodies such as rituximab targeting CD20, alemtuzumab targeting CD52 or antibody-drug conjugates such as inotuzumab or bispecific T cell engagers such as blinatumomab and the exciting CAR T cell therapy. I am going to focus new findings with rituximab added to the SOC and blinatumomab though there are many on-going studies with these varying therapeutics.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Addition of Rituximab Improves the Outcome of Adult Patients with CD20-Positive, Ph-Negative, B-Cell
Precursor Acute Lymphoblastic Leukemia (BCP-ALL): Results of the Randomized Graall-R 2005 Study
Sébastien Maury, Sylvie Chevret, Xavier Thomas, Dominik Heim, Thibaut Leguay,
Françoise Huguet, Patrice Chevallier, Mathilde Hunault, Nicolas Boissel, Martine Escoffre-Barbe, Urs Hess, Norbert Vey, Thorsten Braun, Jean-Pierre Marolleau,
Yves Chalandon, Véronique Lhéritier, Kheira Beldjord, Marie-Christine Béné, Norbert Ifrah, and Hervé Dombret
Plenary Abstract # 1
Presenter
Presentation Notes
The Group for Research in Adult Acute lymphoblastic lymphoma (GRAALL) a cooperative group from France and Switzerland presented as a plenary abstract the addition of rituximab to SOC for adult patients with CD20 positive Ph- precursor B cell ALL.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
GRAALL-R: Study Design
Multicenter, randomized, phase III study from 2005-2014
CD20 expressed in 30% to 40% of B-cell precursor ALL pts, associated with worse outcomes
Allogeneic SCT offered in first CR to pts with ≥ 1 high-risk criteria Primary endpoint: EFS Secondary endpoints: relapse/death in first CR, safety, EFS after censoring pts given
allogeneic SCT in first CR 209 pts in mITT analysis (n = 11 excluded for noneligibility criteria)
CD20+ Ph- tx-naïve BCP-ALL pts
18-59 yrs of age with ≥ 20% CD20+ blasts and no other current/recent malignancies
(N = 220)
Standard Chemo + Rituximab IV 375 mg/m2 16-18 infusions
(n = 105)
Standard Chemo w/out Rituximab (n = 104)
Presenter
Presentation Notes
This was a multi-center randomized phase III trial initiated in 2005 and ending in 2014 examining targeting CD20 as this is expressed in 30-40% of pre-B cell ALL and has been associated with worse outcomes. Patients were ages 18-59 with greater or equal to 20% CD20+ with newly diagnosed ALL. They were randomized to standard chemotherapy with or without rituximab with a total of 220 patients. The chemotherapy, I will not go into detail about but is similar multi-agent therapy, that is given in a variety of ways for an extended period of time. The rituximab was given on Days 1 and 7 of induction (reinduction if needed), consolidation blocks with 6 infusions, late intensification Days 1 and 7 and 6 infusions during first year of maintenance for a total of 16-18 infusions. The primary endpt was EFS and secondary endpts were relapse/death in CR1, safety, and EFS after censoring pts who underwent allogeneic SCT in CR1. 209 patients were in the modified ITT analysis with 11 excluded for noneligibility criteria.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
GRAALL-R: Baseline Characteristics
Characteristic All (N = 209)
Rituximab (n = 105)
No Rituximab (n = 104)
P Value
Median age, yrs 40.2 39.9 41.5 .90 ECOG PS ≥ 2, n (%) 27 (13) 9 (9) 18 (18) .06 WBC ≥ 30 x 109/L, n (%) 44 (21) 21 (20) 23 (22) .74 CNS involvement, n (%) 13 (6) 7 (7) 6 (6) .99 Poor PB blast clearance, n (%) 34 (16) 20 (19) 14 (13) .27 Poor BM blast clearance, n (%) 87 (42) 46 (44) 41 (39) .58 High-risk ALL, n (%) 140 (67) 73 (70) 67 (64) .46 Allogeneic SCT in CR1, n (%) 57 (27) 36 (34) 21 (20) .03 Median CD20 positivity, % (range) 66 (0-100) 61 (0-100) 69 (1-100) .24
Presenter
Presentation Notes
Patient baseline characteristics appeared to be similar with the only difference were more patients in the rituximab group underwent allgeneic SCT in CR1 with 34 vs 20 but only about 27% of patients underwent transplant at all.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
GRAALL-R: Response Rates
Response, n (%) Rituximab (n = 105)
No Rituximab (n = 104) P Value
CR in 1 induction course 95 (91) 91 (88) .52
CR 97 (92) 94 (90) .63
Resistant disease 1 (1) 1 (1) .99
Induction deaths 7 (7) 9 (9) .61
Postinduction MRD < 10-4 32/49 (65) 22/36 (61) .82
Postconsolidation MRD < 10-4 42/46 (91) 28/34 (82) .31
Presenter
Presentation Notes
CR rates were similar between groups as well as number of induction deaths and postinduction and consolidation MRD.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
GRAALL-R: Efficacy
Rituximab vs No Rituximab Outcome Probability, % HR (95% CI) Adjusted HR* (95% CI) EFS (2 year)
65 vs 52 0.66 (0.45-0.98) P = .038
0.59 (0.37-0.93) P = .021
OS (2 year)
71 vs 64 0.70 (0.46-1.07) P = .095
0.55 (0.34-0.91) P = .018
Cumulative Incidence of Relapse
18 vs 32 0.52 (0.31-0.89) P = .017
0.49 (0.27-0.89) P = .018
Presenter
Presentation Notes
However, 2 year EFS and OS were significantly higher in the rituximab group with 2 year EFS 65 vs 52% and OS 71 vs 64%. The 2 year cumulative incidence of relapse also was better in the rituximab group at 18 vs 32%. EFS was also impacted by age, CNS involvement, WBC at diagnosis. The data was censored for patients who underwent allogeneic SCT in CR1.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
GRAALL-R: Conclusions
Rituximab added to chemotherapy demonstrated clinical benefit vs chemotherapy alone in adult pts with CD20+, Ph- BCP-ALL Improved EFS (P = .038) Prolonged OS in pts not receiving SCT during CR1 (P = .018) Well-tolerated safety profile in the rituximab group vs standard
chemo alone
The investigators conclude that adding rituximab to standard chemotherapy should become a standard of care for patients with CD20+, Ph- BCP-ALL They note that further study required to determine optimal
rituximab dosing

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Complete Molecular and Hematologic Response in Adult Patients with Relapsed/Refractory Philadelphia
Chromosome-Positive B-Precursor Acute Lymphoblastic Leukemia Following Treatment with Blinatumomab: Results from a Phase 2 Single-Arm,
Multi-Center Study
36
Giovanni Martinelli, Hervé Dombret, Patrice Chevallier, Oliver G. Ottmann, Nicola Goekburger, Max S. Topp, Adele K. Fielding, Lulu Ren Sterling, Jonathan Benjamin,
and Anthony Selwyn Stein
Oral Abstract # 679
Presenter
Presentation Notes
Briefly, I want to mention that it appears that patients with Ph+ ALL are also deriving clinical benefit from blinatumomab as presented by Dr. Martinelli – international multiistitutional study.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
ALCANTARA: Background
Blinatumomab, a bispecific T-cell engaging antibody construct, has shown antileukemic activity in Ph- ALL 43% of pts achieved CR/CRh in first 2 cycles of
blinatumomab monotherapy
Pts with R/R Ph+ ALL have a poor overall prognosis despite improved outcomes from TKI therapy
ALCANTARA evaluated efficacy and safety of blinatumomab in pts with R/R Ph+ ALL resistant to TKI
Presenter
Presentation Notes
Blinatumomab as mentioned prior is a bispecific T cell engaging antibody construct that has shows a CR/CRh (complete remission with partial hematological recovery) response in 43% of Ph-ALL patients in first 2 cycles of therapy. This is FDA approved for the R/R Ph-ALL group but not for Ph+. Ph+ patients with R/R disease have an overall poor prognosis despite the use of Tki therapy. 25% of patients with pre-B ALL have Ph+. This study was designed to evaluate the efficacy and safety of blinatumomab iin patients with Ph+ R/R disease that is resistant to TKIs.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
ALCANTARA: Study Design
Phase II single arm study
Primary endpoint: CR/CRh during first 2 cycles Secondary endpoints: best CR, MRD, RFS, OS, allogeneic HSCT rate,
and safety
Adults with R/R Ph+ B-precursor ALL; ECOG PS 0-2; > 5% BM
blasts; failed TKI (N = 45)
Blinatumomab IV 9 µg/day x 1wk
28 µg/day x 3 wks (cycle 1) 28 µg/day x 4 wks (cycle 2)
(4 wks on, 2 wks off)
Consolidation: Blinatumomab IV 28 µg/day x 4 wks
≤ 3 cycles (4 wks on, 2 wks off)
Follow-up at 30 days and
≤ 18 mos
Primary Endpoint Assessed During First 2 Cycles
Presenter
Presentation Notes
Phase II single arm open label study with 45 patients with R/R Ph+ pre-B ALL adults with >5% BM blasts. Given blinatumomab as standardly given Ph- FDFA approved dosing. Primary enpoint was CR/CRh during first 2 cycles with secondary endpoints of MRD, RFS, OS, allo SCT rate and safety. Included 4 patients with T315I disease

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
ALCANTARA: Efficacy
Median RFS: 6.7 mos (95% CI: 4.4-NE) Median OS: 7.1 mos (95% CI: 5.6-NE)
Parameter Response, % Primary endpoint CR/CRh (first 2 cycles) T315l mutation ≥ 2 prior 2+ gen TKI Prior ponatinib treatment
36 40 41 35
Secondary endpoints Best response (first 2 cycles) CR CRh CRi (not including CRh)
31 4 4
Complete MRD response*
MRD response in pts with ABL-kinase mutations 88
100 Proceeded to allogeneic HSCT 25
Presenter
Presentation Notes
Neurologic events: any grade, n = 21 (47%); grade 3, n = 3 (7%); no grade 4.�Cytokine release syndrome: any grade, n = 4 (9%); no grade 3 or 4. Responses – CR/CRh rate of 36% including patients with T315I mutations, prior ponatinib treatment and greater or equal to 2 prior second generation groups – high risk disease. 25% of patients were able to proceed to allogeneic stem cell transplant. Median RFS 6.7 months and median OS of 7.1 months

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
ALCANTARA: Conclusions
Blinatumomab achieved antileukemic activity in Ph+ R/R ALL pts with poor prognosis and previous failure of TKI therapy CR/CRh rate: 36% Response to therapy was independent of T315l mutation
100% of responders with ABL-kinase domain mutations had complete MRD response
Median OS: 7.1 mos
Safety profile consistent with blinatumomab treatment of pts with Ph- R/R ALL

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
ECOG E1910: Randomized Trial Incorporating Blinatumomab in Upfront Therapy for Ph- B Adult ALL (Ages 30-70) PI: Dr. Rebecca Klisovic
SWOG S1318: Upfront Therapy Blinatumomab with
POMP for Ph- Adult ALL or Blinatumomab with Dasatinib/Prednisone for Ph+ Adult ALL (Ages ≥ 65) PI: Dr. Rebecca Klisovic
Ongoing clinical trials at OSU
41

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Myelodysplastic Syndrome

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Eltrombopag for the Treatment of Thrombocytopenia of Low and Intermediate-1 IPSS Risk Myelodysplastic Syndromes: Interim Results on Efficacy, Safety, and
Quality of Life of an International, Multicenter Prospective, Randomized, Trial
43
Esther Natalie Olivia, Valeria Santini, Caterina Alanti, Antonella Poloni, Alfredo Molteni, Pasquale Niscola, Grazia Sanpaolo, Flavia Salvi, Giuseppe A. Palumbo, Enrico Balleari, Stefana Impera, Agostino Cortelezzi, Anna Marina Liberati, Paolo Avanzini, Paolo Di Bartolomeo, Christian Rose, Odile Beyne-Rauzy, Francesco
Buccisano, Monica Bocchia, Fortunato Morabito, Aspasia Stamatoullas, Francesca Ronco, Gina Zini, Maria Grazia D’Errigo, Natale Ranieri, Patrizia Cufari, Irene
Santacanterina, Pierre Fenaux, and Roberto Latagliata
Oral Abstract # 91
Presenter
Presentation Notes
For MDS, I am quickly go to discuss this interesting abstract where reponses in low and intermediate-1 risk IPSS MDS were found with eltrombopag.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
EQoL-MDS: Background Severe thrombocytopenia occurs in approximately 10% of lower-risk
pts with MDS
PLT transfusions given for lower IPSS risk pts with bleeding (occurs in ~ 25% pts with low, int-1 risk MDS)
Thrombopoetin receptor agonists in MDS Romiplostim: ↑ PLT responses and ↓ PLT transfusion events vs placebo in
pts with low/int-1 risk MDS, but ↑ peripheral blast cell counts led to study closure
OS and AML-free survival similar to placebo
Eltrombopag: thrombopoetin receptor agonist Antiproliferative effects against many AML cell lines but not against
normal cells Reduces intracellular iron and induction of differentiation
Presenter
Presentation Notes
Severe thrombocytopenia occurs in 10% of patients with lower risk MDS and approximately 25% of low and int-1 risk MDS require plt transfusion due to bleeding. The first study looking at thrombopoetin receptor agonists in low and intermediate-1 risk MDS did not go wel as there was an increase in platelet responses and decreased platelet transfusion vs placebos but increase in peripheral blast count led to study closure and no difference seen in groups in regards to AML-free survival and OS. Eltrombopag has been shown in pre-clinical studies to show antiproliferative effects againt AML cell lines but not against normal cells and also has been to show reduction in intracellular iron and induction of differentiation.
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
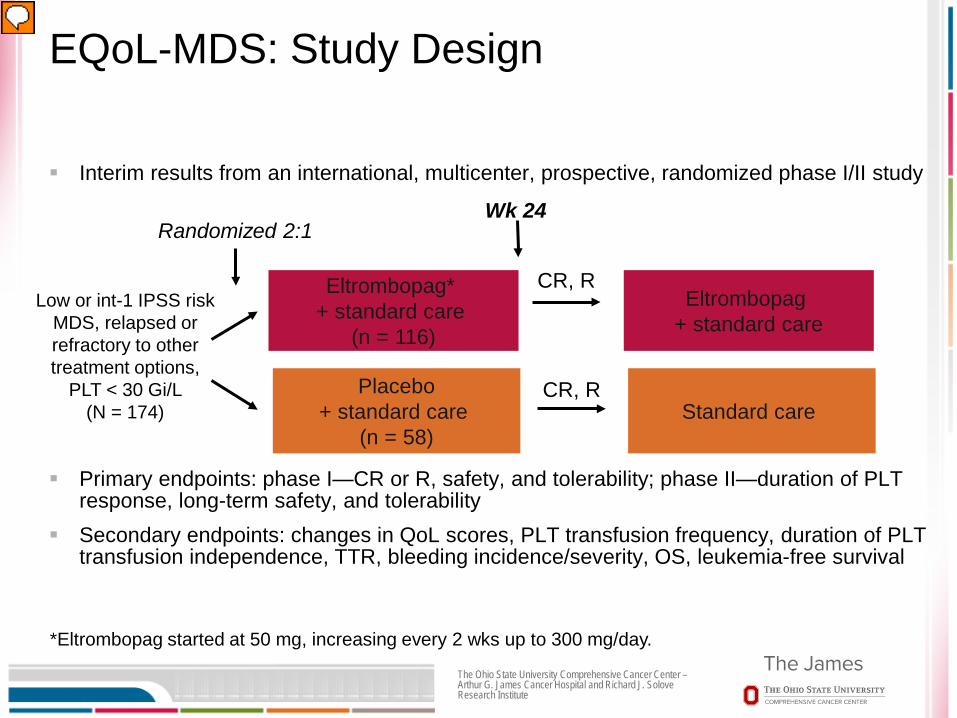
EQoL-MDS: Study Design
Interim results from an international, multicenter, prospective, randomized phase I/II study
Primary endpoints: phase I—CR or R, safety, and tolerability; phase II—duration of PLT response, long-term safety, and tolerability
Secondary endpoints: changes in QoL scores, PLT transfusion frequency, duration of PLT transfusion independence, TTR, bleeding incidence/severity, OS, leukemia-free survival
Low or int-1 IPSS risk MDS, relapsed or refractory to other treatment options,
PLT < 30 Gi/L (N = 174)
Eltrombopag* + standard care
(n = 116)
Placebo + standard care
(n = 58)
Randomized 2:1 Wk 24
CR, R
CR, R
*Eltrombopag started at 50 mg, increasing every 2 wks up to 300 mg/day.
Eltrombopag + standard care
Standard care
Presenter
Presentation Notes
These are interim results from the international , multicenter randomized phase I/II trial. 174 pts with low or int-1 risk with r/r disease and platelets <30,000 and no prior exposure to Thrombopoietin receptor agonist were randomized in a 2:1 fashion to eltrombopag + SOC vs placebo + SOC. Eltrombopag was started at 50mg daily and increased every two weeks up to 300mg/day to target platelets 100,000. At week 24 they were assessed for response and if CR (>100,000 and absence of bleeding or response (defined as baseline plt >20,000: absence of bleeding and increase of plt at least 30,000 from baseline or baseline plt <20,000 and platelets increase >20,000 and at least by 100% not due to plt transfusion. and if response in treatment group allowed to continue. Placebo group not allowed to crossover. Primary endpoint Phase I – CR or reponse, safety and tolerability. For phase II –duration of platelet response, long-term safety and tolerability.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
EQoL-MDS: Baseline Characteristics
Characteristic Eltrombopag (n = 46*) Placebo (n = 24*)
Mean age, yrs (SD) 69 (11) 66 (16)
Female, % 41 54 Median MDS duration, mos (IQR) 9 (2-39) 9 (2-18)
IPSS risk, % Low Int-1
26 74
42 58
WHO bleeding score ≥ 2, % 11 12
PLT transfusion dependent, n (%) 33 33
Mean PLT, x 109 (SD) 17.4 (8.1) 16.3 (8.6) RBC transfusion dependent, % 33 37
Mean Hb, g/dL (SD) 9.9 (2.6) 11 (2.2) Cytogenetics normal, n del20q
36 6
16 3
*Of 70 pts randomized, 24 remain in eltrombopag arm (1 death, 3 each persistent, AML evolution, MDS progression) and 11 in placebo arm (1 each of AML evolution, MDS progression); 1 pt ongoing in each arm.
Presenter
Presentation Notes
70 patients total have been randomized thus far with 46 on eltrombopag and 24 on placebo. Mean age is 68.3. Mean platelet count was 17,100 with mean haemoglobin level of 10.8 gdL. A 1/3 of patients in each group were platelet-transfusion dependent or RBC transfusion dependent

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
EQoL-MDS: Response
8 Wks 24 Wks
Response, n Eltrombopag (n = 41)
Placebo (n = 17)
Eltrombopag (n = 24)
Placebo (n = 11)
Total responses 21 0 13 3
R 12 0 5 3
CR 9 0 8 0
NR 20 17 11 8
WHO bleeding grade ≥ 2, events 1 2 3 1
Presenter
Presentation Notes
23 cases in the eltrombopag (50%) patients have responded versus 2 (8%) in placebo arm. 33 patients have completed at least 24 weeks of study with TTR of 14 days at a median daily dose of 75.

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
50,000
EQoL-MDS: Mean Change in PLT Counts
8 wks 250,000
200,000
150,000
100,000
0
P < .0001 P < .004
24 wks
50,000
250,000
200,000
150,000
100,000
0 Placebo Eltrombopag Placebo Eltrombopag
26
69 25
Presenter
Presentation Notes
IQR, interquartile range; PLT, platelet. 8-wk median PLT counts increased from 18 Gi/L (IQR: 10-25) to 44 Gi/L (IQR: 18-70) with eltrombopag treatment vs no significant change at 8 wks with placebo Platelet count was increased by a mean of 53.2 vs No signicant change in placebo by week 24.
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
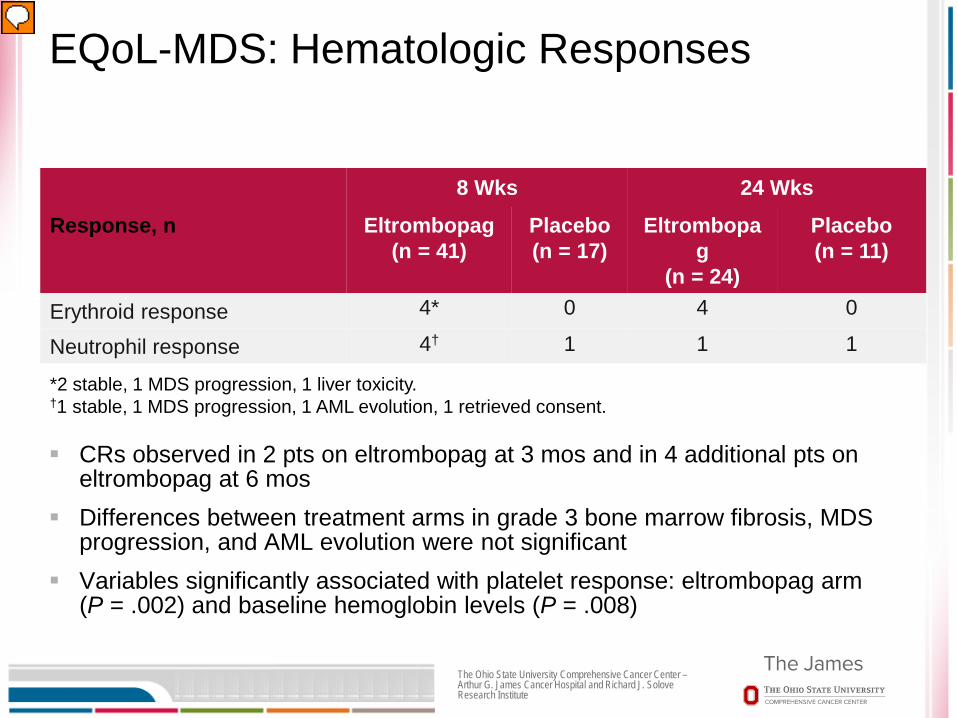
EQoL-MDS: Hematologic Responses
CRs observed in 2 pts on eltrombopag at 3 mos and in 4 additional pts on eltrombopag at 6 mos
Differences between treatment arms in grade 3 bone marrow fibrosis, MDS progression, and AML evolution were not significant
Variables significantly associated with platelet response: eltrombopag arm (P = .002) and baseline hemoglobin levels (P = .008)
8 Wks 24 Wks
Response, n Eltrombopag (n = 41)
Placebo (n = 17)
Eltrombopag
(n = 24)
Placebo (n = 11)
Erythroid response 4* 0 4 0
Neutrophil response 4† 1 1 1
*2 stable, 1 MDS progression, 1 liver toxicity. †1 stable, 1 MDS progression, 1 AML evolution, 1 retrieved consent.
Presenter
Presentation Notes
Study related Grade ¾ AEs – n/v 6 and liver toxicity increased transaminitis/bilirubin 4

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
EQoL-MDS: Conclusions
Eltrombopag in pts with low/intermediate-1 risk MDS and severe thrombocytopenia: Interim results reveal increased platelet counts, durable PLT
responses vs placebo May induce hematological remission in some pts
Associated with manageable toxicity No association with MDS progression or AML evolution Pts who responded to eltrombopag reported improved QoL
from baseline
Trial will continue to evaluate long-term safety, impact on survival
Presenter
Presentation Notes
AML, acute myeloid leukemia; MDS, myelodysplastic syndrome; PLT, platelet; QoL, quality of life.
The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Key Points AML
FLT3 inhibition with midostaurin plus standard induction will likely become the standard of care for newly diagnosed younger adult AML patients with FLT3 mutated disease
Small molecular inhibitors that target recurrent molecular mutations in AML appear to show clinical response and may allow some patients with relapsed/refractory disease to bridge to transplantation
ALL The role of immunotherapy in ALL continues to evolve and will
likely soon become part of the standard of care in both upfront and the relapsed/refractory setting
MDS Targeting the thrombopoietin receptor with eltrombopag in
low/int-1 risk disease appears to improve clinically significant thrombocytopenia without increasing risk of disease progression with early findings
51

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Acknowledgements
Thanks to Drs. Richard Stone (midostaurin) and Eytan Stein (AG-221) for providing me with their ASH presentation slides for this ASH review. I have modified some of the slides due to our time
constraints. This material is unpublished and these slides should not be reproduced without the consent of the authors.
52

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Questions?
53