
of acceleration dependent aberration - BMJ
9
Br Heart J 1992;67:16-24 REVIEWS Vagaries of acceleration dependent aberration Charles Fisch, Suzanne B Knoebel Krannert Institute of Cardiology, Department of Medicine, Indiana University School of Medicine, Indianapolis, Indiana, USA C Fisch S B Knoebel Correspondence to Dr Charles Fisch, Krannert Institute of Cardiology, 1111 West Tenth Street, Indianapolis, IN 46202, USA. The earliest electrocardiogram illustrating bizarre intraventricular conduction of supraventricular impulses was published by Sir Thomas Lewis in 1910.' In a subsequent communication Lewis labelled this form of abnormal conduction "aberration" and the ventricular complexes as "aberrant beats."2 In that same paper he also proposed a mechanism for the aberration, namely ". . . disturbances of conduction in the smaller branches of this system and it is held that definite branches are affected in this man- ner, though these branches cannot be iden- tified at the present time". The underlying milieu for aberration proposed by Lewis stood the tests of further observation and experi- mentation. Altered, asynchronous conduction has been demonstrated for all segments of the His-Purkinje system as well as the Purkinje- myocardial junctional areas and, rarely, as a result of preferential atrioventricular and, per- haps, His bundle conduction. The mechan- isms responsible for initiating the conduction alterations are, however, even more complex as attested to by the vast number of published reports, both basic and clinical, on aberrancy that has been generated since Lewis' initial observations. In 1983, on the occasion of the 75th anniversary of Sir Thomas Lewis' description of aberration, Dr Dennis Krikler, Editor of the British Heart Journal, invited an editorial on that subject.3 As our contribution to this Festschrift issue of the British Heart Journal honouring Dr Krikler, we have elected to continue that discussion and focus on the vagaries of acceleration dependent aberration. The subject is particularly well suited to Dr Krikler's long time interest in the history of cardiology and, in particular, in tracing the development of concepts in electrophysiology. We have collated scattered reports on eccentric forms of acceleration dependent aberration and on mechanisms that could explain the vagaries proposed in the hope that further interest in the mechanisms underlying aberration will be stimulated. The material comes from our files and our earlier publications. - II- - A ..4. . Lwr__m-- ILL f.±XL'..17 - t Fig 18. I * _ _ * _ _......... lx Fig. 19. Fig. 18. Curves taken from the three leadls in a case of aortic disease during a febrile attack. They show xlefective condtuction along the right division of the auriculo-ventricular bundle (see Fig. 16). Fig. 19. Curves fromn the same patient, taken a day later and during the subsidence of the fever. The ventricular portions of the curves have changed p,rofoundly; there is now no evidence of bundle defect, but of prepondlerance of the left ventricle. Figure 1 Earliest example of acceleration dependent aberration. (Reproducedfrom Lewis T. The mechanism and graphic registration of the heart beat. London: Shaw and Sons, 1920:125.) Background and observations In 1913, Lewis published two electrocardio- grams illustrating the disappearance of bundle branch block with slowing of the heart rate (fig 1).4 Although the tracings were recorded on different days, they probably are the earliest example of acceleration dependent aberration. The classic manifestation of acceleration dependent aberration is the appearance of aberration at a critical cycle length reached in the course of an increase in heart rate, and normalisation of conduction with slowing of the heart rate to the point that the RR cycle is again longer than that at which aberration was initiated (fig 2).5 While the predictability of the relation between rate and aberrancy is characteristic for acceleration dependent aberration, there are exceptions to this heart rate dependency that we will refer to as vagaries or eccentric forms of acceleration dependent aberration, an example of which also was first reported by Lewis.6 The vagaries will be divided into two groups: Group 1-unexpected normalisation of conduction when aberration would be expected to continue-and Group 2-un- expected appearance or persistence of aberra- tion under conditions in which it would not be expected. Examples under each group are presented and discussed below. IM 16 on March 19, 2022 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Downloaded from
Transcript of of acceleration dependent aberration - BMJ
Br Heart J 1992;67:16-24
REVIEWS
Vagaries of acceleration dependent aberration
Charles Fisch, Suzanne B Knoebel
Krannert Instituteof Cardiology,Department ofMedicine, IndianaUniversity Schoolof Medicine,Indianapolis, Indiana,USAC FischS B KnoebelCorrespondence toDr Charles Fisch,Krannert Institute ofCardiology, 1111 WestTenth Street, Indianapolis,IN 46202, USA.
The earliest electrocardiogram illustratingbizarre intraventricular conduction ofsupraventricular impulses was published bySir Thomas Lewis in 1910.' In a subsequentcommunication Lewis labelled this form ofabnormal conduction "aberration" and theventricular complexes as "aberrant beats."2In that same paper he also proposed amechanism for the aberration, namely". . . disturbances of conduction in thesmaller branches of this system and it is heldthat definite branches are affected in this man-ner, though these branches cannot be iden-tified at the present time". The underlyingmilieu for aberration proposed by Lewis stoodthe tests of further observation and experi-mentation. Altered, asynchronous conductionhas been demonstrated for all segments of theHis-Purkinje system as well as the Purkinje-myocardial junctional areas and, rarely, as aresult of preferential atrioventricular and, per-haps, His bundle conduction. The mechan-isms responsible for initiating the conductionalterations are, however, even more complexas attested to by the vast number of published
reports, both basic and clinical, on aberrancythat has been generated since Lewis' initialobservations.
In 1983, on the occasion of the 75thanniversary of Sir Thomas Lewis' descriptionof aberration, Dr Dennis Krikler, Editor ofthe British Heart Journal, invited an editorialon that subject.3 As our contribution to thisFestschrift issue of the British Heart Journalhonouring Dr Krikler, we have elected tocontinue that discussion and focus on thevagaries of acceleration dependent aberration.The subject is particularly well suited to DrKrikler's long time interest in the history ofcardiology and, in particular, in tracing thedevelopment of concepts in electrophysiology.We have collated scattered reports on
eccentric forms of acceleration dependentaberration and on mechanisms that couldexplain the vagaries proposed in the hope thatfurther interest in the mechanisms underlyingaberration will be stimulated. The materialcomes from our files and our earlierpublications.
- II-- A
..4. . Lwr__m--ILL f.±XL'..17
- t
Fig 18.
I *
_ _ *
__.........
lx
Fig. 19.
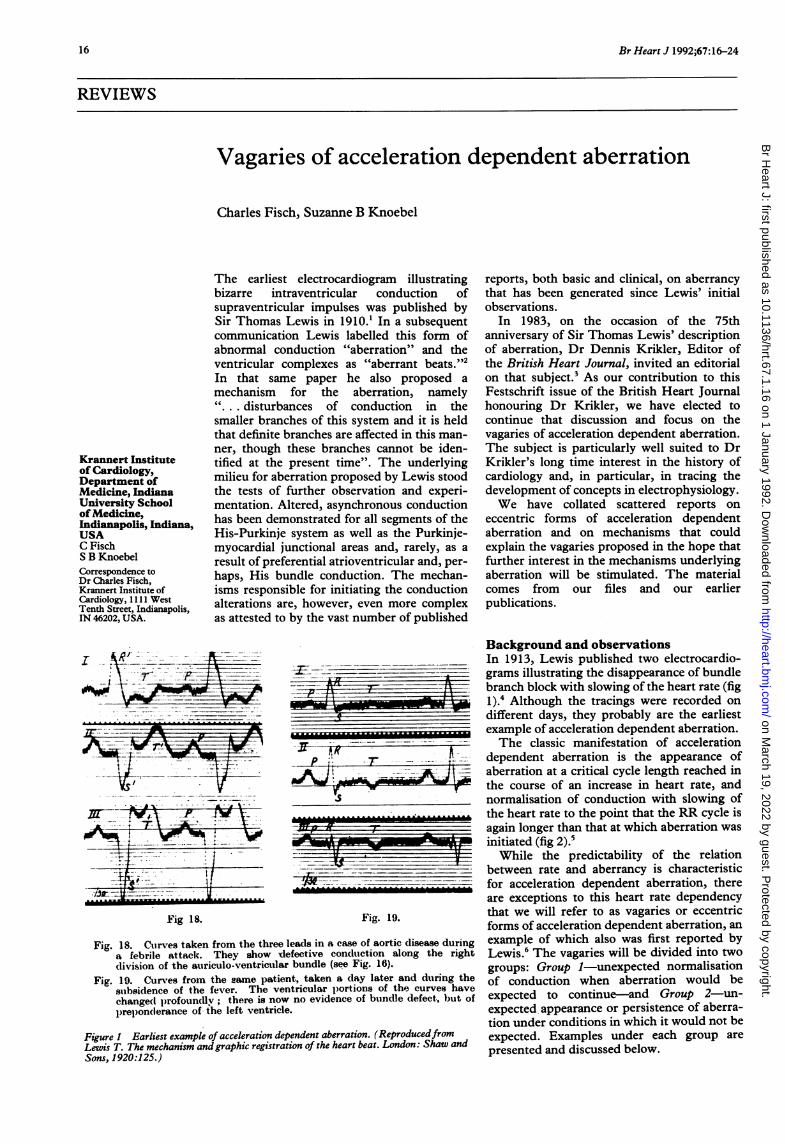
Fig. 18. Curves taken from the three leadls in a case of aortic disease duringa febrile attack. They show xlefective condtuction along the rightdivision of the auriculo-ventricular bundle (see Fig. 16).
Fig. 19. Curves fromn the same patient, taken a day later and during the
subsidence of the fever. The ventricular portions of the curves have
changed p,rofoundly; there is now no evidence of bundle defect, but of
prepondlerance of the left ventricle.
Figure 1 Earliest example of acceleration dependent aberration. (ReproducedfromLewis T. The mechanism and graphic registration of the heart beat. London: Shaw and
Sons, 1920:125.)
Background and observationsIn 1913, Lewis published two electrocardio-grams illustrating the disappearance of bundlebranch block with slowing of the heart rate (fig1).4 Although the tracings were recorded ondifferent days, they probably are the earliestexample of acceleration dependent aberration.The classic manifestation of acceleration
dependent aberration is the appearance ofaberration at a critical cycle length reached inthe course of an increase in heart rate, andnormalisation of conduction with slowing ofthe heart rate to the point that the RR cycle isagain longer than that at which aberration wasinitiated (fig 2).5While the predictability of the relation
between rate and aberrancy is characteristicfor acceleration dependent aberration, thereare exceptions to this heart rate dependencythat we will refer to as vagaries or eccentricforms of acceleration dependent aberration, anexample of which also was first reported byLewis.6 The vagaries will be divided into twogroups: Group 1-unexpected normalisationof conduction when aberration would beexpected to continue-and Group 2-un-expected appearance or persistence of aberra-tion under conditions in which it would not beexpected. Examples under each group are
presented and discussed below.
IM
16
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from
Vagaries of acceleration dependent aberration
LII- .1 V~ ~~~~~~~~~~~~~~..Li....t'I{tf4 tii1-iS10iii1
11001 70061[.... . ... .. ........4i
......
SiWES 1- i
1. UT
ii tit 1-tE11i'0'I!IjII1tt'''..~~~ AI.... IL-*.@..* 1 t'*,.. . ..}.
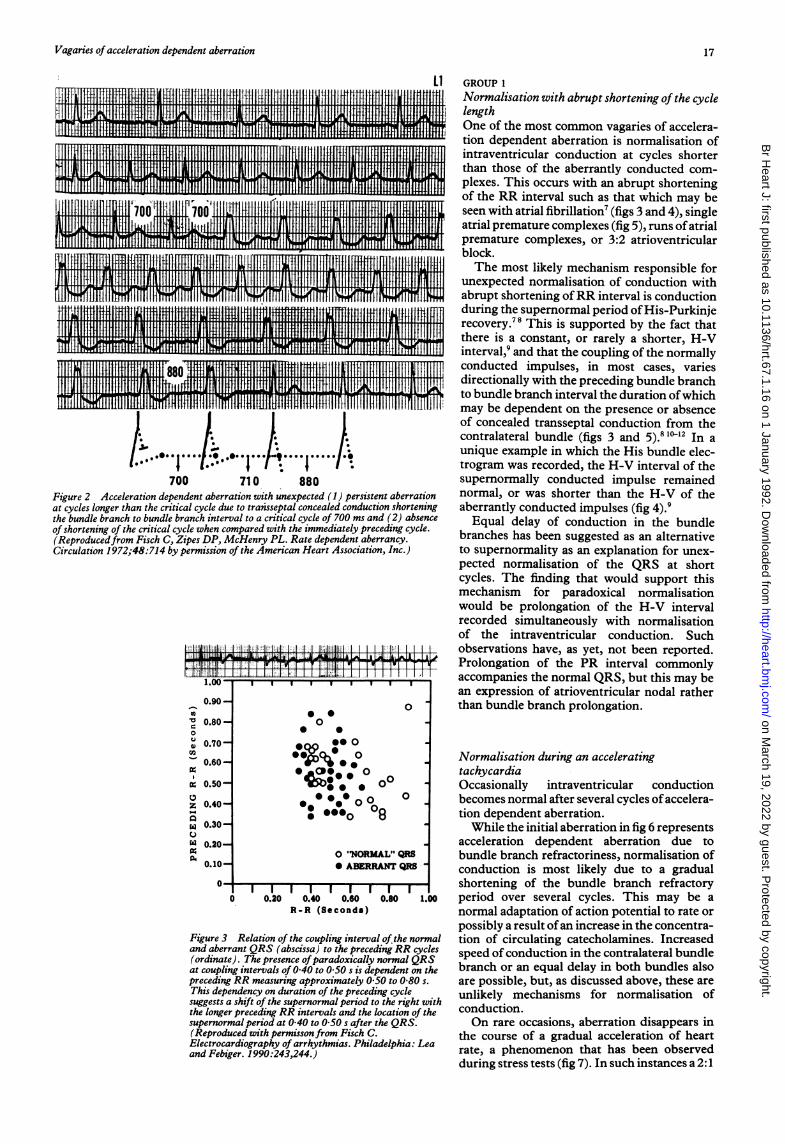
700 710 880Figure 2 Acceleration dependent aberration with unexpected (1) persistent aberrationat cycles longer than the critical cycle due to transseptal concealed conduction shorteningthe bundle branch to bundle branch interval to a critical cycle of 700 ms and (2) absenceof shortening of the critical cycle when compared with the immediately preceding cycle.(Reproducedfrom Fisch C, Zipes DP, McHenry PL. Rate dependent aberrancy.Circulation 1972;48:714 by permission of the American Heart Association, Inc.)
-0.90-
'X 0.80-0
0.70-
0.60-
; 0.500
Z 0.40-
X 0.30-
w 0.20-
0.10-
0
0
0
* 0
'
°*
00 0
0
0 "NORMAL" QRS* ABERRANT QRS
0 0.20 0.40 0.60 0.80 1.00R-R (Seconds)
Figure 3 Relation of the coupling interval of the normaland aberrant QRS (abscissa) to the preceding RR cycles(ordinate). The presence ofparadoxically normal QRSat coupling intervals of 0 40 to 0 50 s is dependent on thepreceding RR measuring approximately 0S50 to 0 80 s.This dependency on duration of the preceding cyclesuggests a shift of the supernormal period to the right withthe longer preceding RR intervals and the location of thesupernormal period at 0 40 to 0 50 s after the QRS.(Reproduced with permissonfrom Fisch C.Electrocardiography of arrhythmias. Philadelphia: Leaand Febiger. 1990:243,244.)
GROUP 1Normalisation with abrupt shortening of the cyclelengthOne of the most common vagaries of accelera-tion dependent aberration is normalisation ofintraventricular conduction at cycles shorterthan those of the aberrantly conducted com-plexes. This occurs with an abrupt shorteningof the RR interval such as that which may beseen with atrial fibrillation7 (figs 3 and 4), singleatrial premature complexes (fig 5), runs ofatrialpremature complexes, or 3:2 atrioventricularblock.The most likely mechanism responsible for
unexpected normalisation of conduction withabrupt shortening ofRR interval is conductionduring the supernormal period ofHis-Purkinjerecovery.78 This is supported by the fact thatthere is a constant, or rarely a shorter, H-Vinterval,9 and that the coupling of the normallyconducted impulses, in most cases, variesdirectionally with the preceding bundle branchto bundle branch interval the duration ofwhichmay be dependent on the presence or absenceof concealed transseptal conduction from thecontralateral bundle (figs 3 and 5).8 1012 In aunique example in which the His bundle elec-trogram was recorded, the H-V interval of thesupernormally conducted impulse remainednormal, or was shorter than the H-V of theaberrantly conducted impulses (fig 4).9Equal delay of conduction in the bundle
branches has been suggested as an alternativeto supernormality as an explanation for unex-pected normalisation of the QRS at shortcycles. The finding that would support thismechanism for paradoxical normalisationwould be prolongation of the H-V intervalrecorded simultaneously with normalisationof the intraventricular conduction. Suchobservations have, as yet, not been reported.Prolongation of the PR interval commonlyaccompanies the normal QRS, but this may bean expression of atrioventricular nodal ratherthan bundle branch prolongation.
Normalisation during an acceleratingtachycardiaOccasionally intraventricular conductionbecomes normal after several cycles ofaccelera-tion dependent aberration.While the initial aberration in fig 6 represents
acceleration dependent aberration due tobundle branch refractoriness, normalisation ofconduction is most likely due to a gradualshortening of the bundle branch refractoryperiod over several cycles. This may be anormal adaptation of action potential to rate orpossibly a result ofan increase in the concentra-tion of circulating catecholamines. Increasedspeed ofconduction in the contralateral bundlebranch or an equal delay in both bundles alsoare possible, but, as discussed above, these areunlikely mechanisms for normalisation ofconduction.On rare occasions, aberration disappears in
the course of a gradual acceleration of heartrate, a phenomenon that has been observedduring stress tests (fig 7). In such instances a 2:1
114i II Ml ti-11 RH LL-1-1-1 1-11 II HI 11-1-11 III III . III II ITMM I rli 114 If 11-1 IIII ff III I FI I ifl-l I fli II H I t If III
11 I 11 i .. F IUNIon II 1. .11
ti, i Li I 1+1 11-1I4I 4FI41 I Hl i P{^-
17
:;,liol; II;7;; .!:m
I'' "t-7!L J TT-T-FF
I I I I
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from
Fisch, Knoebel
fUEl II LI ~~~~~~IIII11 111II, IIII +
II 1 1 * *1 1%
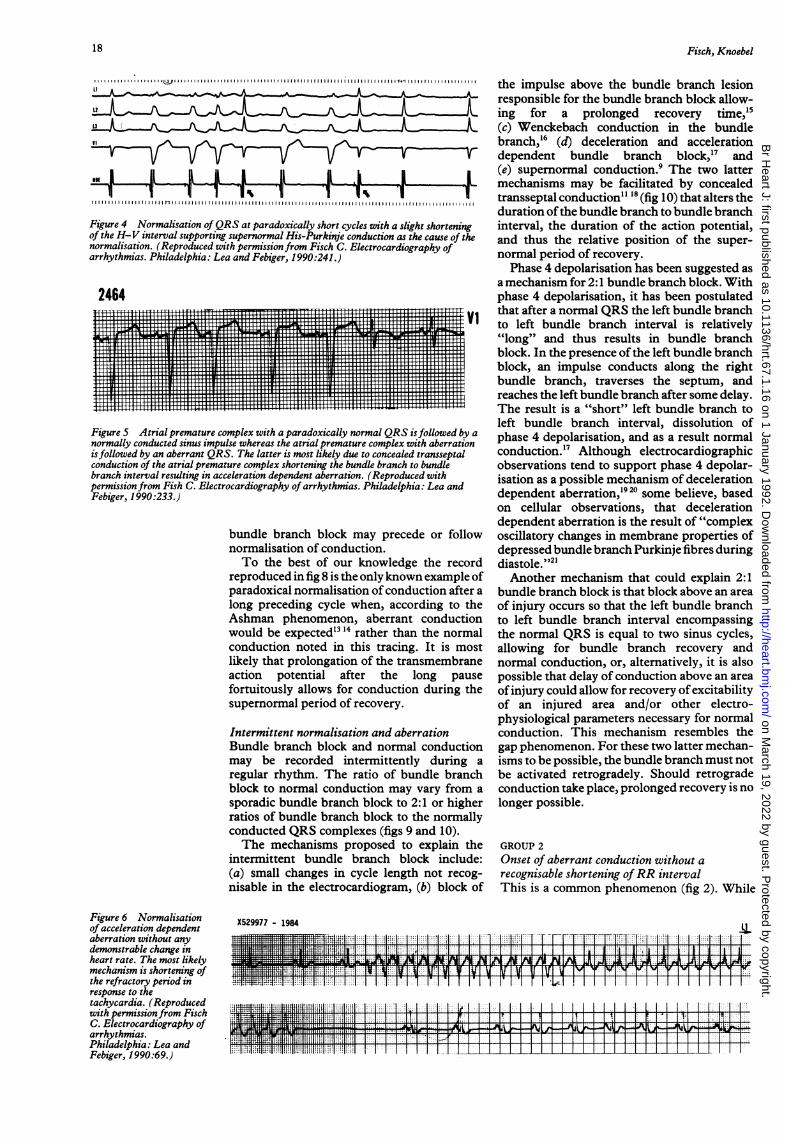
Figure 4 Normalisation ofQRS at paradoxically short cycles with a slight shortenin,of the H-V interval supporting supernormal His-Purkinje conduction as the cause of t,normalisation. (Reproduced with permission from Fisch C. Electrocardiography ofarrhythmias. Philadelphia: Lea and Febiger, 1990:241.)
2464
~~~~~~~~~~~~~~~~~~~~~..i!I.,P.X:F: : : T tI.FT F.,
.F__ri tFi.. 1_F|| ||||| ll§|| |||||X
Figure S Atrial premature complex with a paradoxically normal QRS isfollowed bDnormally conducted sinus impulse whereas the atrial premature complex with aberratiiisfollowed by an aberrant QRS. The latter is most likely due to concealed transseptalconduction of the atrial premature complex shortening the bundle branch to bundlebranch interval resulting in acceleration dependent aberration. (Reproduced withpermission from Fish C. Electrocardiography of arrhythmias. Philadelphia: Lea andFebiger, 1990:233.)
bundle branch block may precede or follnormalisation of conduction.To the best of our knowledge the rec(
reproduced in fig 8 is the only known exampl4paradoxical normalisation ofconduction aftclong preceding cycle when, according to iAshman phenomenon, aberrant conductiwould be expected" 4 rather than the norrconduction noted in this tracing. It is mlikely that prolongation of the transmembrEaction potential after the long paifortuitously allows for conduction duringsupernormal period of recovery.
Intermittent normalisation and aberrationBundle branch block and normal conductmay be recorded intermittently duringregular rhythm. The ratio of bundle brarblock to normal conduction may vary fronsporadic bundle branch block to 2:1 or hig]ratios of bundle branch block to the normaconducted QRS complexes (figs 9 and 10).The mechanisms proposed to explain
intermittent bundle branch block inclu(a) small changes in cycle length not rec4
nisable in the electrocardiogram, (b) block
"" the impulse above the bundle branch lesionresponsible for the bundle branch block allow-ing for a prolonged recovery time,"5(c) Wenckebach conduction in the bundlebranch,'6 (d) deceleration and accelerationdependent bundle branch block,'7 and(e) supernormal conduction.9 The two lattermechanisms may be facilitated by concealedtransseptal conduction" " (fig180) that alters theduration ofthe bundle branch to bundle branchinterval, the duration of the action potential,
he and thus the relative position of the super-normal period of recovery.
Phase 4 depolarisation has been suggested asa mechanism for 2:1 bundle branch block. Withphase 4 depolarisation, it has been postulated
vi that after a normal QRS the left bundle branchto left bundle branch interval is relatively"long" and thus results in bundle branchblock. In the presence of the left bundle branchblock, an impulse conducts along the rightbundle branch, traverses the septum, andreaches the left bundle branch after some delay.The result is a "short" left bundle branch toleft bundle branch interval, dissolution of
y a phase 4 depolarisation, and as a result normalconduction.'7 Although electrocardiographicobservations tend to support phase 4 depolar-isation as a possible mechanism of decelerationdependent aberration,1920 some believe, basedon cellular observations, that decelerationdependent aberration is the result of "complex
low oscillatory changes in membrane properties ofdepressed bundle branch Purkinje fibres during
ord diastole."'2'eof Another mechanism that could explain 2:1er a bundle branch block is that block above an area
the of injury occurs so that the left bundle branchion to left bundle branch interval encompassingnal the normal QRS is equal to two sinus cycles,lost allowing for bundle branch recovery andane normal conduction, or, altematively, it is alsouse possible that delay of conduction above an areathe ofinjury could allow for recovery ofexcitability
of an injured area and/or other electro-physiological parameters necessary for normalconduction. This mechanism resembles the
ion gap phenomenon. For these two latter mechan-a isms to be possible, the bundle branch must not
ich be activated retrogradely. Should retrograden a conduction take place, prolonged recovery is noher longer possible.ally
the GROUP 2Lde: Onset of aberrant conduction without a
og- recognisable shortening ofRR intervalof This is a common phenomenon (fig 2). While
Figure 6 Normalisationof acceleration dependentaberration without anydemonstrable change inheart rate. The most likelymechanism is shortening ofthe refractory period inresponse to thetachycardia. (Reproducedwith permissionfrom FischC. Electrocardiography ofarrhythmias.Philadelphia: Lea andFebiger, 1990:69.)
X529977 - 1984
..
.1'0ji,. l, . .............;: .|......-||-||-||:||.
18
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from
Vagaries of acceleration dependent aberration
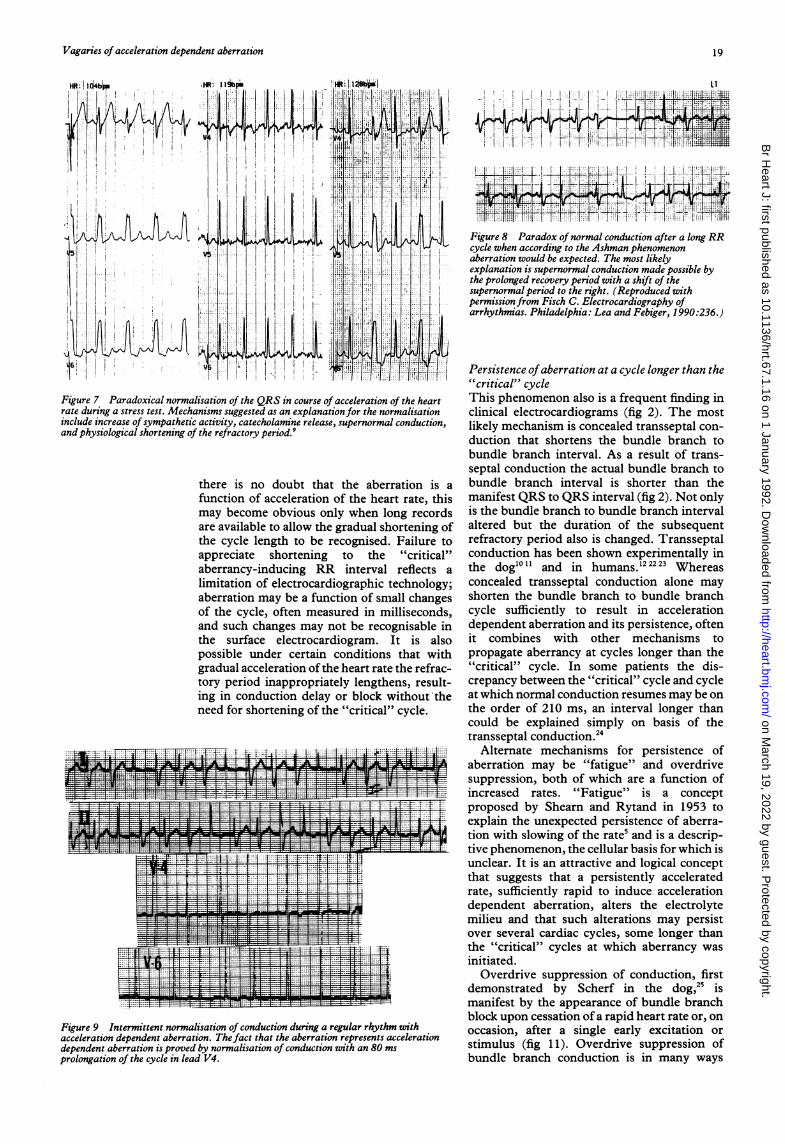
Figure 7 Paradoxical normalisation of the QRS in course of acceleration of the heartrate during a stress test. Mechanisms suggested as an explanation for the normalisationinclude increase of sympathetic activity, catecholamine release, supernormal conduction,and physiological shortening of the refractory period.9
there is no doubt that the aberration is a
function of acceleration of the heart rate, thismay become obvious only when long recordsare available to allow the gradual shortening ofthe cycle length to be recognised. Failure toappreciate shortening to the "critical"aberrancy-inducing RR interval reflects a
limitation of electrocardiographic technology;aberration may be a function of small changesof the cycle, often measured in milliseconds,and such changes may not be recognisable inthe surface electrocardiogram. It is alsopossible under certain conditions that withgradual acceleration of the heart rate the refrac-tory period inappropriately lengthens, result-ing in conduction delay or block without theneed for shortening of the "critical" cycle.
Figure 9 Intermittent normalisation of conduction during a regular rhythm withacceleration dependent aberration. Thefact that the aberration represents accelerationdependent aberration is proved by normalisation of conduction with an 80 ms
prolongation of the cycle in lead V4.
'I!
_...._ _tLi L Li P+ j___' 4 i'
Y ., S1- . U-t |s IL1
Figure 8 Paradox of normal conduction after a long RRcycle when according to the Ashman phenomenonaberration would be expected. The most likelyexplanation is supernormal conduction made possible bythe prolonged recovery period with a shift of thesupernormal period to the right. (Reproduced withpermission from Fisch C. Electrocardiography ofarrhythmias. Philadelphia: Lea and Febiger, 1990:236.)
Persistence ofaberration at a cycle longer than the"critical" cycleThis phenomenon also is a frequent finding inclinical electrocardiograms (fig 2). The mostlikely mechanism is concealed transseptal con-duction that shortens the bundle branch tobundle branch interval. As a result of trans-septal conduction the actual bundle branch tobundle branch interval is shorter than themanifest QRS to QRS interval (fig 2). Not onlyis the bundle branch to bundle branch intervalaltered but the duration of the subsequentrefractory period also is changed. Transseptalconduction has been shown experimentally inthe dog'01' and in humans.'22223 Whereasconcealed transseptal conduction alone mayshorten the bundle branch to bundle branchcycle sufficiently to result in accelerationdependent aberration and its persistence, oftenit combines with other mechanisms topropagate aberrancy at cycles longer than the"critical" cycle. In some patients the dis-crepancy between the "critical" cycle and cycleat which normal conduction resumes may be onthe order of 210 ms, an interval longer thancould be explained simply on basis of thetransseptal conduction.24
Alternate mechanisms for persistence ofaberration may be "fatigue" and overdrivesuppression, both of which are a function ofincreased rates. "Fatigue" is a conceptproposed by Shearn and Rytand in 1953 toexplain the unexpected persistence of aberra-tion with slowing of the rate5 and is a descrip-tive phenomenon, the cellular basis for which isunclear. It is an attractive and logical conceptthat suggests that a persistently acceleratedrate, sufficiently rapid to induce accelerationdependent aberration, alters the electrolytemilieu and that such alterations may persistover several cardiac cycles, some longer thanthe "critical" cycles at which aberrancy wasinitiated.
Overdrive suppression of conduction, firstdemonstrated by Scherf in the dog,25 ismanifest by the appearance of bundle branchblock upon cessation of a rapid heart rate or, onoccasion, after a single early excitation orstimulus (fig 1 1). Overdrive suppression ofbundle branch conduction is in many ways
19
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from
Fisch, Knoebel
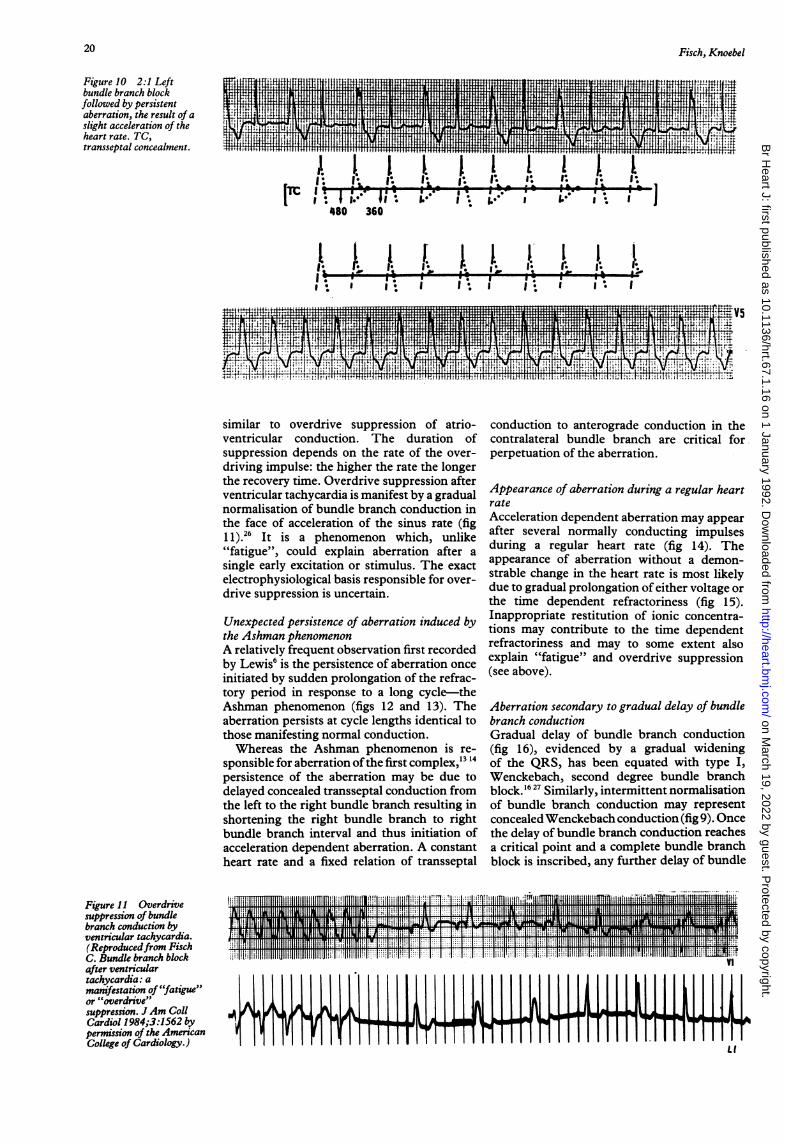
Figure 10 2:1 Leftbundle branch blockfollowed by persistentaberration, the result of aslight acceleration of theheart rate. TC,transseptal concealment. 1w'~~~~~~~~~~~~~~~~~~~~~~~~1 11tt
TM~~~~~~~~~~~~~~~~t}i.I
480 360 *
i 4~ ~ 9. ...........~I
V541' A lsl
tg>0tft4. f.X :.+..# L 1 WjX1:Itih jn .j E2E .l t' U:j.!fL1.1.LMES w mSW.,..s
similar to overdrive suppression of atrio-ventricular conduction. The duration ofsuppression depends on the rate of the over-driving impulse: the higher the rate the longerthe recovery time. Overdrive suppression afterventricular tachycardia is manifest by a gradualnormalisation of bundle branch conduction inthe face of acceleration of the sinus rate (fig1l).26 It is a phenomenon which, unlike"fatigue", could explain aberration after asingle early excitation or stimulus. The exactelectrophysiological basis responsible for over-drive suppression is uncertain.
Unexpected persistence of aberration induced bythe Ashman phenomenonA relatively frequent observation first recordedby Lewis6 is the persistence of aberration onceinitiated by sudden prolongation of the refrac-tory period in response to a long cycle-theAshman phenomenon (figs 12 and 13). Theaberration persists at cycle lengths identical tothose manifesting normal conduction.Whereas the Ashman phenomenon is re-
sponsible for aberration ofthe first complex,13 14persistence of the aberration may be due todelayed concealed transseptal conduction fromthe left to the right bundle branch resulting inshortening the right bundle branch to rightbundle branch interval and thus initiation ofacceleration dependent aberration. A constantheart rate and a fixed relation of transseptal
conduction to anterograde conduction in thecontralateral bundle branch are critical forperpetuation of the aberration.
Appearance of aberration during a regular heartrateAcceleration dependent aberration may appearafter several normally conducting impulsesduring a regular heart rate (fig 14). Theappearance of aberration without a demon-strable change in the heart rate is most likelydue to gradual prolongation of either voltage orthe time dependent refractoriness (fig 15).Inappropriate restitution of ionic concentra-tions may contribute to the time dependentrefractoriness and may to some extent alsoexplain "fatigue" and overdrive suppression(see above).
Aberration secondary to gradual delay of bundlebranch conductionGradual delay of bundle branch conduction(fig 16), evidenced by a gradual wideningof the QRS, has been equated with type I,Wenckebach, second degree bundle branchblock.1627 Similarly, intermittent normalisationof bundle branch conduction may representconcealedWenckebach conduction (fig 9). Oncethe delay of bundle branch conduction reachesa critical point and a complete bundle branchblock is inscribed, any further delay of bundle
Figure 11 Overdrivesuppression of bundlebranch conduction byventricular tachycardia.(Reproducedfrom FischC. Bundle branch blockafter ventriculartachycardia: amanifestation of "fatigue"or "overdrive"suppression. J Am CollCardiol 1984;3:1562 bypermission of the AmericanCollege of Cardiology.) Li
20
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from
Vagaries of acceleration dependent aberration
1t.1.1 I~J. U. ,~I , L.*6.1. **1. V
,%. ft .e e @
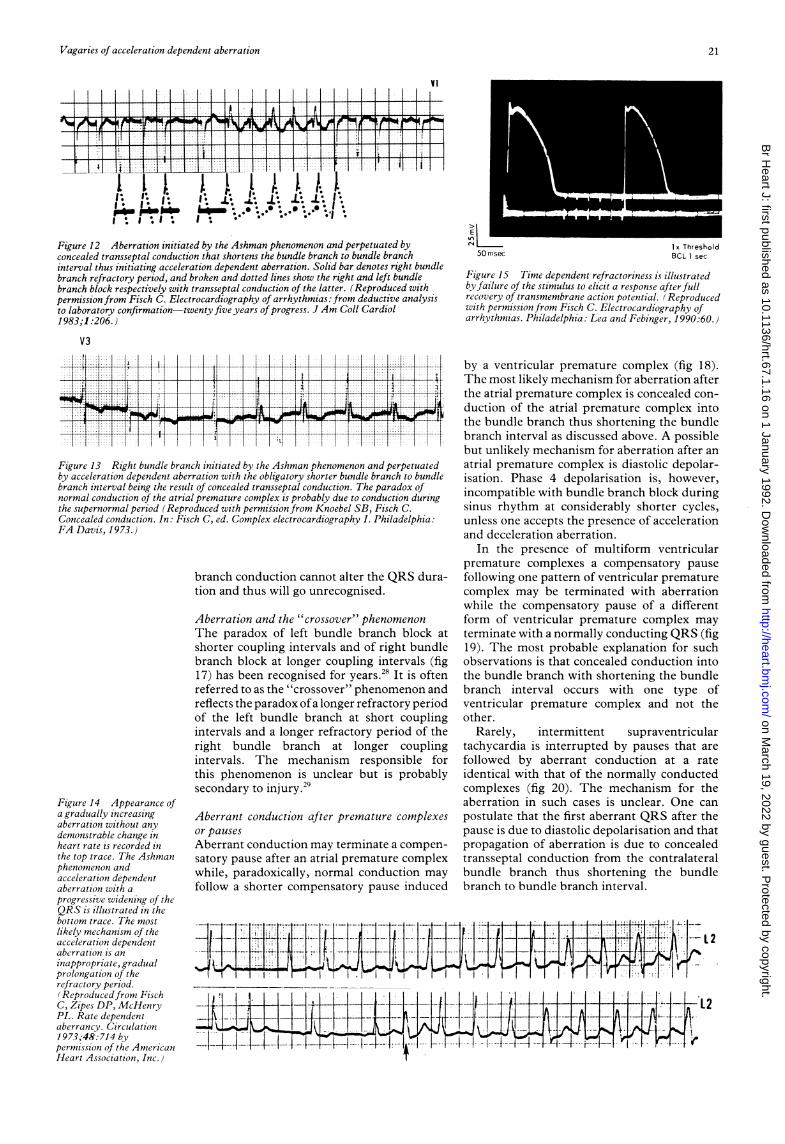
Figure 12 Aberration initiated by the Ashman phenomenon and perpetuated byconcealed transseptal conduction that shortens the bundle branch to bundle branchinterval thus initiating acceleration dependent aberration. Solid bar denotes right bundlebranch refractory period, and broken and dotted lines show the right and left bundlebranch block respectively with transseptal conduction of the latter. (Reproduced withpermission from Fisch C. Electrocardiography of arrhythmias: from deductive analysisto laboratory confirmation-twenty five years of progress. J Am Coll Cardiol1983;1 :206.)
V3:I: tt.::'l:: :1 :: 1 1 1 ' I I I I 11: 1 1 1 :1: 1 1 -I I I 1 1 : 1 . 1-- 1 i i -:1., +, . .,, .... , , . ., , I , , .................... , , ,, , , , , , , , , , S + + * t - § f t.... , , , , , , , , , , , ,, , , , ., ., , #., ., , ...... , , , , , ,-:: 1+::.1 :::s:. :1: 1: :1 113 :: 11: :1: :X1: ::t *-X1 :1. :::I: :l ::t _ l-l i _ i_ 1_ t1
L11+1 11+:1111-1 T;l1 1:1-10:1:1 It1 1:S 101 1:T4ild'3,F1,-1S;... , , , , . i .. ... . . ... . . . . . . . . ............... . .:: 1. :t::::1 ::1:: t :: J 1: ::1 :1 :::1 ::t :1 1:Il I I § Nl § § § { l l I f § I § | § § I .I
I I'.1'-1- 1 1 '
Figure 13 Right bundle branch initiated by the Ashman phenomenon and perpetuatedby acceleration dependent aberration with the obligatory shorter bundle branch to bundlebranch interval being the result of concealed transseptal conduction. The paradox ofnormal conduction of the atrial premature complex is probably due to conduction duringthe supernormal period (Reproduced with permis-sion from Knoebel SB, Fisch C.Concealed conduction. In: Fisch C, ed. Complex electrocardiography I. Philadelphia:FA Davis, 1973.)
branch conduction cannot alter the QRS dura-tion and thus will go unrecognised.
Figure 14 Appearance ofa gradually increasingaberration without anydemonstrable change inheart rate is recorded inthe top trace. The Ashmanphenomenon andacceleration dependentaberration with aprogressive widening of theQRS is illustrated in thebottom trace. The mostlikely mechanism of theacceleration dependentaberration is aninappropriate, gradualprolongation of therefractory period.(Reproducedfrom FischC, Zipes DP, McHenryPL. Rate dependentaberrancy. Circulation1973;48.:714 bypermnission of the AmericanHeart Association, Inc.)
Aberration and the "crossover" phenomenonThe paradox of left bundle branch block atshorter coupling intervals and of right bundlebranch block at longer coupling intervals (fig17) has been recognised for years.28 It is oftenreferred to as the "crossover" phenomenon andreflects the paradox ofa longer refractory periodof the left bundle branch at short couplingintervals and a longer refractory period of theright bundle branch at longer couplingintervals. The mechanism responsible forthis phenomenon is unclear but is probablysecondary to injury.29
Aberrant conduction after premature complexesor pausesAberrant conduction may terminate a compen-satory pause after an atrial premature complexwhile, paradoxically, normal conduction mayfollow a shorter compensatory pause induced
IN.1 1LL
UII
EOs50 msec
lx ThresholdBCL 1 sec
Figure 15 Time dependent refractoriness is illustratedby failure of the stimulus to elicit a response after fullrecovery of transmembrane action potential. (Reproducedwith permission from Fisch C. Electrocardiography ofarrhythmias. Philadelphia: Lea and Febinger, 1990:60.)
by a ventricular premature complex (fig 18).The most likely mechanism for aberration afterthe atrial premature complex is concealed con-duction of the atrial premature complex intothe bundle branch thus shortening the bundlebranch interval as discussed above. A possiblebut unlikely mechanism for aberration after anatrial premature complex is diastolic depolar-isation. Phase 4 depolarisation is, however,incompatible with bundle branch block duringsinus rhythm at considerably shorter cycles,unless one accepts the presence of accelerationand deceleration aberration.
In the presence of multiform ventricularpremature complexes a compensatory pausefollowing one pattern of ventricular prematurecomplex may be terminated with aberrationwhile the compensatory pause of a differentform of ventricular premature complex mayterminate with a normally conducting QRS (fig19). The most probable explanation for suchobservations is that concealed conduction intothe bundle branch with shortening the bundlebranch interval occurs with one type ofventricular premature complex and not theother.
Rarely, intermittent supraventriculartachycardia is interrupted by pauses that arefollowed by aberrant conduction at a rateidentical with that of the normally conductedcomplexes (fig 20). The mechanism for theaberration in such cases is unclear. One canpostulate that the first aberrant QRS after thepause is due to diastolic depolarisation and thatpropagation of aberration is due to concealedtransseptal conduction from the contralateralbundle branch thus shortening the bundlebranch to bundle branch interval.
K.fI
L11,-I
I I I'1 I*I 11'1 IA 1 Al I ln
II ±FL2vs-L- 1
8I 'JKU5''-ti
--.I-
--r-
I
I
21
.:] .:, .'i :, :1 t:, t '.:...I .' 1. -i .l 'I 1: .'.
I1
III.] ..
I.
I.1i--
I1L.
L2
oo
-11 --'-i--- .I
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from
Fisch, Knoebel
:::7
l!
I. ... .... .....
11 ;ifM. ll II III HIIIztllU.M! If z ll,lN III III IItt R III II II II tIIII II I1 III ItII III!Id III 111 IIIJIa 11IiilI II III
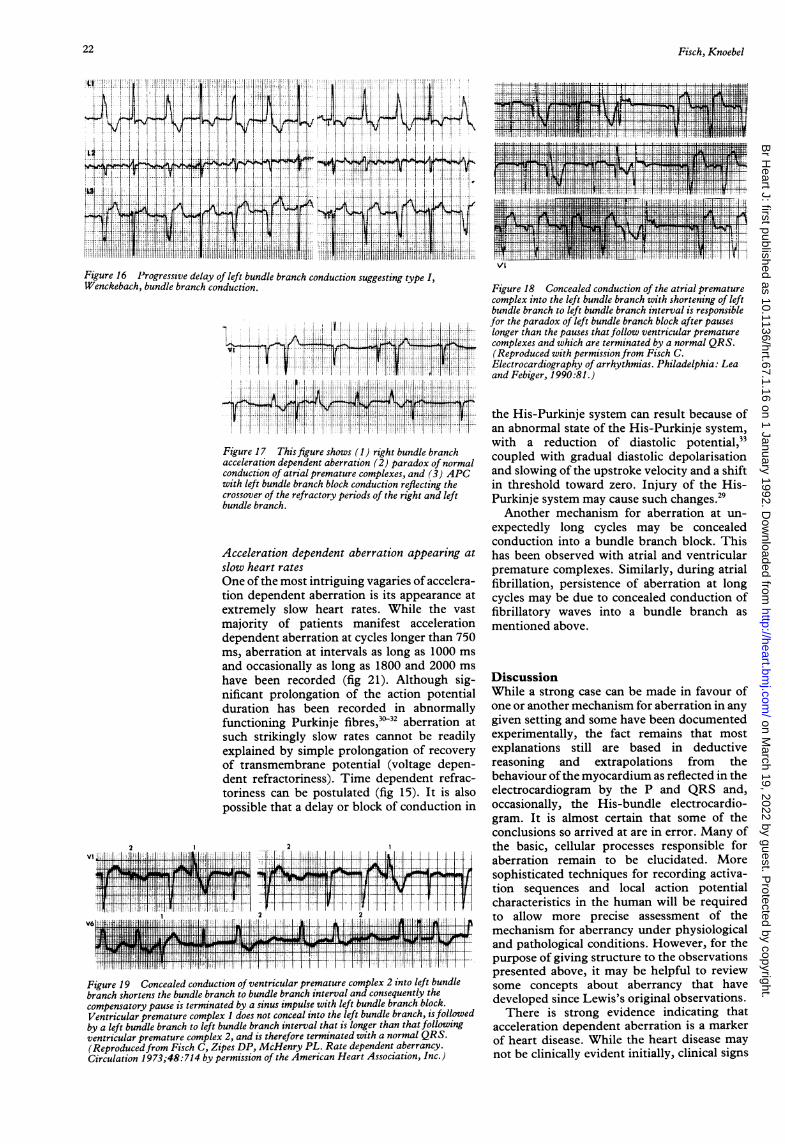
Figure 16 Progressive delay of left bundle branch conduction suggesting type I,Wenckebach, bundle branch conduction.
170.[ ,, 1 1 l 1 .,,I,l llillll t; 1 l'
ll
1.!.
I -"L .-L:~L:~
Figure 18 Concealed conduction of the atrial prematurecomplex into the left bundle branch with shortening of leftbundle branch to left bundle branch interval is responsiblefor the paradox of left bundle branch block after pauseslonger than the pauses that follow ventricular prematurecomplexes and which are terminated by a normal QRS.(Reproduced with permission from Fisch C.Electrocardiography of arrhythmias. Philadelphia: Leaand Febiger, 1990:81.)
Figure 17 Thisfigure shows (1) right bundle branchacceleration dependent aberration (2) paradox of normalconduction of atrial premature complexes, and (3) APCwith left bundle branch block conduction reflecting thecrossover of the refractory periods of the right and leftbundle branch.
Acceleration dependent aberration appearing atslow heart ratesOne of the most intriguing vagaries of accelera-tion dependent aberration is its appearance atextremely slow heart rates. While the vastmajority of patients manifest accelerationdependent aberration at cycles longer than 750ms, aberration at intervals as long as 1000 msand occasionally as long as 1800 and 2000 ms
have been recorded (fig 21). Although sig-nificant prolongation of the action potentialduration has been recorded in abnormallyfunctioning Purkinje fibres,3032 aberration atsuch strikingly slow rates cannot be readilyexplained by simple prolongation of recoveryof transmembrane potential (voltage depen-dent refractoriness). Time dependent refrac-toriness can be postulated (fig 15). It is alsopossible that a delay or block of conduction in
Figure 19 Concealed conduction of ventricular premature complex 2 into left bundlebranch shortens the bundle branch to bundle branch interval and consequently thecompensatory pause is terminated by a sinus impulse with left bundle branch block.Ventricular premature complex 1 does not conceal into the left bundle branch, isfollowedby a left bundle branch to left bundle branch interval that is longer than that followingventricular premature complex 2, and is therefore terminated with a normal QRS.(Reproducedfrom Fisch C, Zipes DP, McHenry PL. Rate dependent aberrancy.Circulation 1973;48:714 by permission of the American Heart Association, Inc.)
the His-Purkinje system can result because ofan abnormal state of the His-Purkinje system,with a reduction of diastolic potential,"coupled with gradual diastolic depolarisationand slowing of the upstroke velocity and a shiftin threshold toward zero. Injury of the His-Purkinje system may cause such changes.29Another mechanism for aberration at un-
expectedly long cycles may be concealedconduction into a bundle branch block. Thishas been observed with atrial and ventricularpremature complexes. Similarly, during atrialfibrillation, persistence of aberration at longcycles may be due to concealed conduction offibrillatory waves into a bundle branch asmentioned above.
DiscussionWhile a strong case can be made in favour ofone or another mechanism for aberration in anygiven setting and some have been documentedexperimentally, the fact remains that mostexplanations still are based in deductivereasoning and extrapolations from thebehaviour of the myocardium as reflected in theelectrocardiogram by the P and QRS and,occasionally, the His-bundle electrocardio-gram. It is almost certain that some of theconclusions so arrived at are in error. Many ofthe basic, cellular processes responsible foraberration remain to be elucidated. Moresophisticated techniques for recording activa-tion sequences and local action potentialcharacteristics in the human will be requiredto allow more precise assessment of themechanism for aberrancy under physiologicaland pathological conditions. However, for thepurpose of giving structure to the observationspresented above, it may be helpful to reviewsome concepts about aberrancy that havedeveloped since Lewis's original observations.There is strong evidence indicating that
acceleration dependent aberration is a markerof heart disease. While the heart disease maynot be clinically evident initially, clinical signs
22
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from
Vagaries of acceleration dependent aberration
/I1.1
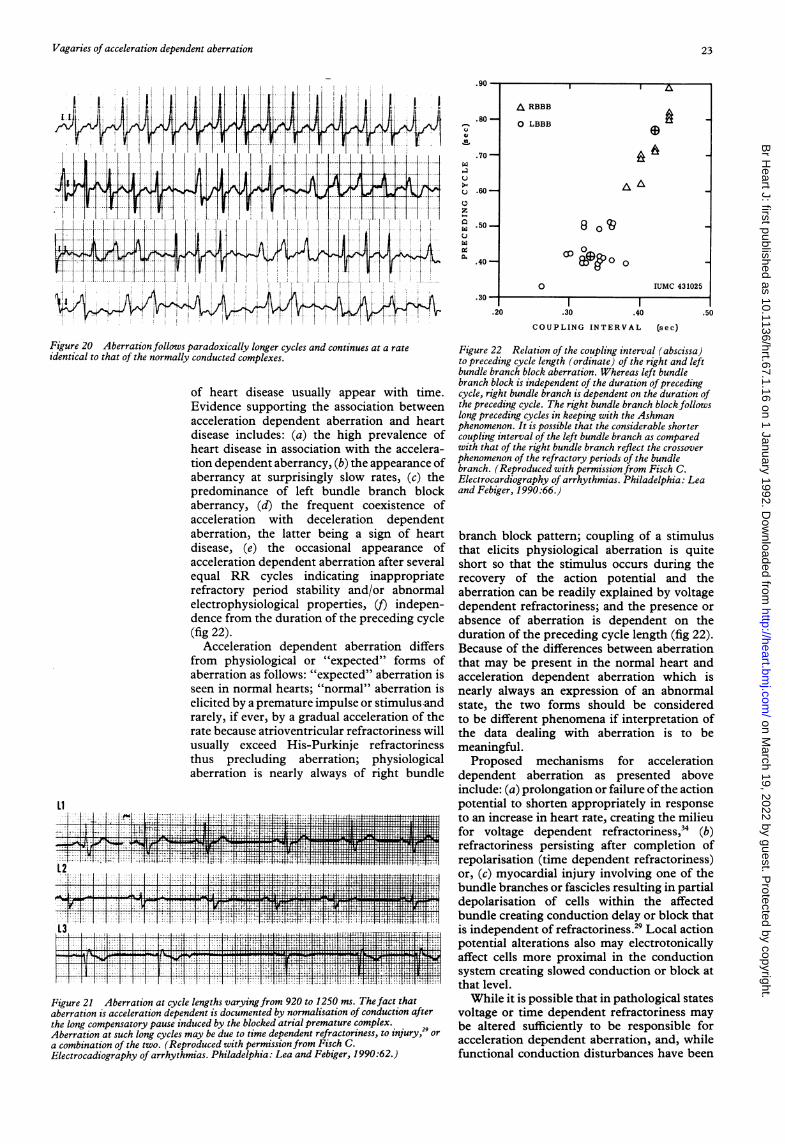
Figure 20 Aberration follows paradoxically longer cycles and continues at a rate
identical to that of the normally conducted complexes.
of heart disease usually appear with time.Evidence supporting the association betweenacceleration dependent aberration and heartdisease includes: (a) the high prevalence ofheart disease in association with the accelera-tion dependent aberrancy, (b) the appearance ofaberrancy at surprisingly slow rates, (c) thepredominance of left bundle branch blockaberrancy, (d) the frequent coexistence ofacceleration with deceleration dependentaberration, the latter being a sign of heartdisease, (e) the occasional appearance ofacceleration dependent aberration after severalequal RR cycles indicating inappropriaterefractory period stability and/or abnormalelectrophysiological properties, (t) indepen-dence from the duration of the preceding cycle(fig 22).
Acceleration dependent aberration differsfrom physiological or "expected" forms ofaberration as follows: "expected" aberration isseen in normal hearts; "normal" aberration iselicited by a premature impulse or stimulus andrarely, if ever, by a gradual acceleration of therate because atrioventricular refractoriness willusually exceed His-Purkinje refractorinessthus precluding aberration; physiologicalaberration is nearly always of right bundle
LI
Figure 21 Aberration at cycle lengths varyingfrom 920 to 1250 ms. The fact thataberration is acceleration dependent is documented by normalisation of conduction afterthe long compensatory pause induced by the blocked atrial premature complex.Aberration at such long cycles may be due to time dependent refractoriness, to injury,29 ora combination of the two. (Reproduced with permission from Fisch C.Electrocadiography of arrhythmias. Philadelphia: Lea and Febiger, 1990:62.)
.80 -
1-0
.70-
c .60-
Z
a .50
.
.40-
.20 .30 .40 .50
COUPLING INTERVAL (sec)
Figure 22 Relation of the coupling interval (abscissa)to preceding cycle length (ordinate) of the right and leftbundle branch block aberration. Whereas left bundlebranch block is independent of the duration ofprecedingcycle, right bundle branch is dependent on the duration ofthe preceding cycle. The right bundle branch block followslong preceding cycles in keeping with the Ashmanphenomenon. It is possible that the considerable shortercoupling interval of the left bundle branch as comparedwith that of the right bundle branch reflect the crossover
phenomenon of the refractory periods of the bundlebranch. (Reproduced with permission from Fisch C.Electrocardiography of arrhythmias. Philadelphia: Leaand Febiger, 1990:66.)
branch block pattern; coupling of a stimulusthat elicits physiological aberration is quiteshort so that the stimulus occurs during therecovery of the action potential and theaberration can be readily explained by voltagedependent refractoriness; and the presence or
absence of aberration is dependent on theduration of the preceding cycle length (fig 22).Because of the differences between aberrationthat may be present in the normal heart andacceleration dependent aberration which isnearly always an expression of an abnormalstate, the two forms should be consideredto be different phenomena if interpretation ofthe data dealing with aberration is to bemeaningful.
Proposed mechanisms for accelerationdependent aberration as presented aboveinclude: (a) prolongation or failure ofthe actionpotential to shorten appropriately in responseto an increase in heart rate, creating the milieufor voltage dependent refractoriness,34 (b)refractoriness persisting after completion ofrepolarisation (time dependent refractoriness)or, (c) myocardial injury involving one of thebundle branches or fascicles resulting in partialdepolarisation of cells within the affectedbundle creating conduction delay or block thatis independent of refractoriness.29 Local actionpotential alterations also may electrotonicallyaffect cells more proximal in the conductionsystem creating slowed conduction or block atthat level.While it is possible that in pathological states
voltage or time dependent refractoriness maybe altered sufficiently to be responsible foracceleration dependent aberration, and, whilefunctional conduction disturbances have been
I~~~~~~IA
A RBBB
0 LBBB a)6
A
00
040 3102
O IUMC 431025
23
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from

Fisch, Knoebel
shown to be favoured at low basic heart rates,"5it is unlikely that either could account foraberration at cycle lengths of 1000 ms or longer,a not infrequent finding in accelerationdependent aberration. In such instances, dis-turbances of conduction are more likely to besecondary to alterations in action potentialcharacteristics such as phase 4 depolarisation,slowing of the upstroke ofphase 0, or reductionof threshold potential due to electropathology.A unifying concept could, therefore, be thatinjury to the conduction tissue, at diverselevels, is the basic defect that underliesacceleration dependent aberration.When the vagaries of acceleration dependent
aberration are under consideration still othermechanisms or combinations of mechanismsneed to be invoked. Examples of these are
presented above and include: (a) shortening ofthe bundle branch to bundle branch cyclewithout change in the manifest QRS to QRScycle secondary to concealed transseptalconduction" " or concealment of atrial andventricular premature complexes into thebundle branches, (b) local injury enhanced byacceleration of the heart rate and a resultantdepression or block of conduction manifestingas fatigue,5 or overdrive suppression,25 26
(c) conduction during the supernormal periodof recovery,9 (d) block above the area ofinjury allowing for bundle branch recovery,(e) "crossover" of the refractory period dura-tion of right and left bundles,2836 (f) equalprolongation of bundle branch conduction,(g) diastolic (phase 4) depolarisation,1733 or,(h) Wenckebach block in a bundle branch.'6 27
Aberration under normal physiological con-
ditions, acceleration dependent aberration andits vagaries, and the similarities and differencesbetween the various "normal" and "abnormal"forms of aberrancy provide a model for under-standing electrophysiological functioning thatis unequalled by any other concept. Even ifbasic cellular and intracellular mechanims forelectrophysiological alteration are eventuallytotally understood there will continue to be theneed for an integrated approach to the conduct-ing system and its functional vagaries.Knowledge of ion channel functioning under a
wide variety of intervention and injury, actionpotential characteristics in response to suchchanges, the effects on refractoriness, cell-to-cell communications, and the effects of all ofthese on conduction patterns is essential if we
are to be able to delineate mechanisms for
aberrancy with more precision that has been
possible to date. There is a large body of
experimental data about the cellular electro-
physiological properties underlying aberra-
tion. A systems approach is needed to make
these observations applicable to the human.
1 Lewis T. Paroxysmal tachycardia, the result of ectopic
impulse formation. Heart 1910;1:262-82.2 Lewis T. Observations upon disorders of the heart's action.
Heart 1911/1912;3:279-309.3 Fisch C. Aberration: seventy five years after Sir Thomas
Lewis. Br Heart J 1983;40:297-302.
4 Lewis T. Certain physical signs of myocardial involvment.BMJ 1913;1:484-9.
5 ShearnHA, Rytand DA. Intermittent bundle branch block.Observations with special reference to the critical heartrate. Arch Intern Med 1953;91:448-63.
6 Lewis T. The mechanism andgraphic registration of the heartbeat. 2nd ed. London: Shaw and Sons, 1920:251.
7 Wellens HJJ. Unusual occurrence of nonaberrant conduc-tion in patientswith atrial fibrillationand aberrant conduc-tion. Am Heart J 1969;77:158-66.
8 Levi RJ, Salerno JA, Nau GJ, Elizari MV, RosenbaumMB.A reappraisal of supernormal conduction. In: RosenbaumMB, Elizari MV, eds. Frontiers of cardiac electro-physiology. Boston: Martinus Nijhoff, 1983:427-56.
9 Fisch C. Electrocardiography of arrhythmias. Philadelphia:Lea & Febiger, 1990:241.
10 Glassman RD, Zipes DP. Site of antegrade and retrogradefunctional right bundle branch in the intact canine heart.Circulation 1981;64:1277-86.
11 Moe GK, Mendez C, Han J. Aberrant A-V impulsepropagation in the dog heart: a study of functional bundlebranch block. Circ Res 1965;16:261-86.
12 Spurrell RAJ, Krikler DM, Sowton E. retrograde invasionof the bundle branches producing aberration of the QRScomplex during supraventricular tachycardia studied byprogrammed electrical stimulation. Circulation 1974;50:487-95.
13 Ashman R, Byer E. Aberration in the conduction ofpremature ventricular impulses. JLa State Univ Sch Med1946;8:62-5.
14 GouauxJL, Ashman R. Auricularfibrillation withaberrationsimulating ventricular paroxysmal tachycardia. Am HeartJ 1947;34:366-73.
15 NauGJ, ElizariMV, RosenbaumMB. The different varietiesof 2:1 bundle branch block. In: Rosenbaum MB, ElizariMV, eds. Frontiers of cardiac electrophysiology. Boston:Martinus Nijhoff, 1983:487-500.
16 Friedberg HD, Schamroth L. The Wenckebach phenome-non in left bundle branch block. Am J Cardiol 1969;24:591-3.
17 Cohen HC, D'Cruz I, Arbel ER, Langendorf R, Pick A.Tachycardia and bradycardia-dependent bundle branchblock alternans. Clinical observations. Circulation1977;55:242-6.
18 Denes P, Wu D, Dhingra R, Pietras RJ, Rosen KM. Theeffects ofcycle length on cardiac refractory periods in man.Circulation 1974;49:32-41.
19 Elizari MV, Nau GJ, Levi RJ, Lazarri JO, Halpern MS,RosenbaumMB. Experimental production ofrate-depen-dent bundle branch block in the canine heart. Circ Res1974;34:730-42.
20 Dressler W. Transient bundle branch block occurringduring slowing of the heart beat and following gagging.Am Heart J 1959;58:760-4.
21 Jalife J, Antzelevitch C, Lamanna V, Moe GK. The cellularmechanism of bradycardia-dependent bundle block [abs-tract]. Circulation 1980;62(suppl III):55.
22 Katz A, Pick A. The transseptal conduction time in thehuman heart. Circulation 1963;27:1061-70.
23 Wellens HJJ, Durrer D. Supraventricular tachycardia withleft aberrant conduction due to retrograde invasion intothe left bundle branch. Circulation 1968;38:474-9.
24 Fisch C, Zipes DP, McHenry PL. Rate dependentaberrancy. Circulation 1973;48:714-24.
25 Scherf D. Experimentelle und klinische Untersuchungenuber interventrikulare Leitungsstorungen. Wein Arch InnMed 1927;14:443-62.
26 Fisch C. Bundle branch block after ventricular tachycardia: a
manifestation of "fatigue" or "overdrive suppression." JAm Coll Cardiol 1984;3:1562-4.
27 Izumi K. Direct Wenckebach periods in left bundle branchduring bradycardia dependent left bundle branch block ina patient with sick sinus syndrome. J Cardiol 1980;13(3):291-6.
28 Burchell HB. Sino-auricular block, interference dissocia-tion, and different recovery ratesofexcitation in thebundlebranches. Br Heart J 1949;11:230-6.
29 Jalife J, Antzelevitch C, Lamanna V, Moe GK. Rate-depen-dent changes in excitability of depressed cardiac Purkinjefibers as a mechanism ofintermittent bundle branch block.Circulation 1983;67:912-22.
30 Friedman PL,Wit AL, Hoffman BF. Experimental myocar-dial infarction: alterations in electrophysiological proper-ties of surviving cells [abstract]. Bull NY Acad Med1972;48:1037.
31 Cranefield PF, Klein HO, Hoffnan BF. Conduction of thecardiac impulse. I. Delay, block and one-way block indepressed Purkinje fibers. Circ Res 1971;28:199-219.
32 Mendez C, Mueller WF, Merideth J, Moe G. Interaction oftransmembrane potentials in canine Purkinje fibers and at
Purkinje fiber-muscle junctions. Circ Res 1969;24:361-72.33 Singer DH, Lazzara R, Hoffman BF. Interrelationships
between automaticity and conduction in Purkinje fibers.Circ Res 1967;21:537-58.
34 Janse MJ, van der Steeen ABM, van Dam RT, Durrer D.Refractory period ofdogs ventricular myocardium follow-ing sudden changes in frequency. Circ Res 1969;24:251-62.
35 Schuilenburg RM, Durrer D. Rate dependency of func-tional block in the human His bundle and bundle branchPurkinje system. Circulation 1973;48:526-40.
36 Chilson DA, Zipes DP, Heger JJ, Browne KF, PrystowskyEN. Functional bundle branch block: discordant responseof right and left bundle branches to changes in heart rate.Am J Cardiol 1984;54:313-6.
24
on March 19, 2022 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.67.1.16 on 1 January 1992. Dow
nloaded from


















