천골 골절 (Sacral Fractures) · 2013-02-05 · 천골 골절 373 Fig. 1. Classification of...
11
371 대한골절학회지 제 24 권, 제 4 호, 2011년 10월 ■ 종 설 ■ Journal of the Korean Fracture Society Vol. 24, No. 4, October, 2011 통신저자:변 영 수 대구시 동구 신암동 576-31 대구파티마병원 정형외과 Tel:053-940-7320ㆍFax:053-954-7417 E-mail:[email protected] Address reprint requests to:Young-Soo Byun, M.D. Department of Orthopedic Surgery, Daegu Fatima Hospital, 576-31, Sinam-dong, Dong-gu, Daegu 701-600, Korea Tel:82-53-940-7320ㆍFax:82-53-954-7417 E-mail:[email protected] 천골 골절 (Sacral Fractures) 변 영 수ㆍ장 세 앙 대구파티마병원 정형외과 서 론 천골은 축성 골격의 역학적인 중심에 위치해 있으며, 골 반환의 쐐기돌 (keystone)로써의 역할을 할 뿐만 아니라 척추의 기초 (base)로써의 역할을 한다 43,44) . 이러한 역학적 인 중요성에도 불구하고 천골은 척추와 골반의 이행 부위 에 위치해 있으므로 척추 외과의나 외상 외과의들로부터 비교적 도외시되어 왔다 44) . 천골 골절은 보통 교통사고나 추락과 같은 고 에너지 손 상으로 인하여 발생하므로 대부분 다발성 손상을 받게 된 다. 천골 골절은 다양한 형태로 나타나며, 골반환이 불안정 하게 되거나 척추와 골반 사이가 불안정하게 될 수 있고, 신경 손상이 높은 빈도로 동반된다 3,16,44) . 천골 골절은 골반 골절의 40∼50%에서 발생하며 3,13,22) , 천골에 대한 요천추 신경총의 위치 때문에 천골 골절의 25%에서 신경 손상이 동반된다 3,16,44) . 이러한 역학적 그리고 임상적 중요성에도 불구하고 천골 골절은 일반적으로 전형적인 임상 징후가 없고, 단순 방사선의 판독이 어렵고, 다발성 손상으로 인해 대부분 신경 손상이 항상 명확하게 나타나는 것이 아니므 로 초기 진단 시 자주 간과되기가 쉬우며 43,44,47) , 천골 골절 의 30% 정도가 진단이 늦게 된다 3,16) . 천골 골절의 부적절한 진단과 치료로 인해 동통을 동반 한 변형이 발생할 수 있고 신경 손상이 점진적으로 악화될 수 있다 32,43,44,48) . 이렇게 변형된 천골을 늦게 수술하는 것 은 매우 까다롭고 조기 수술에 비하여 결과 또한 좋지 못 하므로 천골 골절에 대한 일관된 진단적 접근과 치료 방법 이 결정되어야 한다. 천골의 해부학 천골은 양측의 골반과 척추를 연결하는 삼각형의 골로써 5개의 유합된 천골로 구성되어 있으며, 0∼90도의 시상각 을 가진 후만 구조의 형태로 평균 47도 전방으로 기울어져 있다 22,43,44) . 제1천골부터 제3천골까지 상부 3개 천골의 외 측면은 신장 모양의 관절면을 형성하고 있으며, 제1천골의 추체는 중앙선에서 천골 갑각 (sacral promontory)을 형성 하며, 외측으로는 천골익이 후상방에서 전하방으로 경사져 있다 43,44) . 천골의 후면은 피질골이 얇고 거칠며, 얇은 다열 근 (multifidus muscle)과 요천추 근막으로 덮여 있어 둔상 (blunt trauma)에 잘 견딜 수 있다 44) . 또한 천골에 부착된 여러 강한 인대들에 의하여 골반의 안정성이 유지되므로 천골은 인대의 부착 부위를 제공하는 중요한 역할을 한다. 천골의 전면은 약한 전방천장인대에 의해 장골의 전면과 연결되어 있으며, 후면에는 강한 후방천장골간인대가 골반 의 후방을 안정시키는 주요한 구조물로써 역할을 한다. 장 요인대는 장골능의 후면과 제5요추의 횡돌기를 연결하고, 반면 요천추인대는 천골익과 제5요추의 횡돌기를 연결한 다. 그래서 제5요추 횡돌기의 전위된 골절은 후방 골반환이 불안정하다는 것을 암시한다 16,43,44) . 골반저 (pelvic floor)의 주 구조물은 천극인대와 천결절인대로써 이 인대들은 천골 의 전방 회전을 제한하므로 골반의 안정화에 기여한다 43) . 천골의 척추관은 넓어서 마미 (cauda equine)의 크기보 다 더 크며, 천골의 전면에는 두 줄의 천골공이 양측에 각 각 4개씩 있고 이를 통하여 제1천골에서 제4천골까지 전방 운동 신경근이 나온다. 제1천골 신경근은 제4요추 및 제5 요추 신경근과 결합하고 제2천골부터 제4천골 신경근은 좌 골신경과 결합한다. 제2천골에서 제5천골까지 신경근의 전
Transcript of 천골 골절 (Sacral Fractures) · 2013-02-05 · 천골 골절 373 Fig. 1. Classification of...

371
대한골절학회지 제 24 권 제 4 호 2011년 10월985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103 종 설 Journal of the Korean Fracture SocietyVol 24 No 4 October 2011
통신저자변 영 수대구시 동구 신암동 576-31대구파티마병원 정형외과Tel053-940-7320ㆍFax053-954-7417E-mailfatimaosunitelcokr
Address reprint requests toYoung-Soo Byun MDDepartment of Orthopedic Surgery Daegu Fatima Hospital 576-31 Sinam-dong Dong-gu Daegu 701-600 KoreaTel82-53-940-7320ㆍFax82-53-954-7417E-mailfatimaosunitelcokr
천골 골절
(Sacral Fractures)
변 영 수ㆍ장 세 앙
대구파티마병원 정형외과
서 론
천골은 축성 골격의 역학적인 중심에 위치해 있으며 골
반환의 쐐기돌 (keystone)로써의 역할을 할 뿐만 아니라
척추의 기초 (base)로써의 역할을 한다4344)
이러한 역학적
인 중요성에도 불구하고 천골은 척추와 골반의 이행 부위
에 위치해 있으므로 척추 외과의나 외상 외과의들로부터
비교적 도외시되어 왔다44)
천골 골절은 보통 교통사고나 추락과 같은 고 에너지 손
상으로 인하여 발생하므로 대부분 다발성 손상을 받게 된
다 천골 골절은 다양한 형태로 나타나며 골반환이 불안정
하게 되거나 척추와 골반 사이가 불안정하게 될 수 있고
신경 손상이 높은 빈도로 동반된다31644) 천골 골절은 골반
골절의 40sim50에서 발생하며31322)
천골에 대한 요천추
신경총의 위치 때문에 천골 골절의 25에서 신경 손상이
동반된다31644) 이러한 역학적 그리고 임상적 중요성에도
불구하고 천골 골절은 일반적으로 전형적인 임상 징후가
없고 단순 방사선의 판독이 어렵고 다발성 손상으로 인해
대부분 신경 손상이 항상 명확하게 나타나는 것이 아니므
로 초기 진단 시 자주 간과되기가 쉬우며434447)
천골 골절
의 30 정도가 진단이 늦게 된다316)
천골 골절의 부적절한 진단과 치료로 인해 동통을 동반
한 변형이 발생할 수 있고 신경 손상이 점진적으로 악화될
수 있다32434448)
이렇게 변형된 천골을 늦게 수술하는 것
은 매우 까다롭고 조기 수술에 비하여 결과 또한 좋지 못
하므로 천골 골절에 대한 일관된 진단적 접근과 치료 방법
이 결정되어야 한다
천골의 해부학
천골은 양측의 골반과 척추를 연결하는 삼각형의 골로써
5개의 유합된 천골로 구성되어 있으며 0sim90도의 시상각
을 가진 후만 구조의 형태로 평균 47도 전방으로 기울어져
있다224344)
제1천골부터 제3천골까지 상부 3개 천골의 외
측면은 신장 모양의 관절면을 형성하고 있으며 제1천골의
추체는 중앙선에서 천골 갑각 (sacral promontory)을 형성
하며 외측으로는 천골익이 후상방에서 전하방으로 경사져
있다4344) 천골의 후면은 피질골이 얇고 거칠며 얇은 다열
근 (multifidus muscle)과 요천추 근막으로 덮여 있어 둔상
(blunt trauma)에 잘 견딜 수 있다44)
또한 천골에 부착된
여러 강한 인대들에 의하여 골반의 안정성이 유지되므로
천골은 인대의 부착 부위를 제공하는 중요한 역할을 한다
천골의 전면은 약한 전방천장인대에 의해 장골의 전면과
연결되어 있으며 후면에는 강한 후방천장골간인대가 골반
의 후방을 안정시키는 주요한 구조물로써 역할을 한다 장
요인대는 장골능의 후면과 제5요추의 횡돌기를 연결하고
반면 요천추인대는 천골익과 제5요추의 횡돌기를 연결한
다 그래서 제5요추 횡돌기의 전위된 골절은 후방 골반환이
불안정하다는 것을 암시한다164344)
골반저 (pelvic floor)의
주 구조물은 천극인대와 천결절인대로써 이 인대들은 천골
의 전방 회전을 제한하므로 골반의 안정화에 기여한다43)
천골의 척추관은 넓어서 마미 (cauda equine)의 크기보
다 더 크며 천골의 전면에는 두 줄의 천골공이 양측에 각
각 4개씩 있고 이를 통하여 제1천골에서 제4천골까지 전방
운동 신경근이 나온다 제1천골 신경근은 제4요추 및 제5
요추 신경근과 결합하고 제2천골부터 제4천골 신경근은 좌
골신경과 결합한다 제2천골에서 제5천골까지 신경근의 전
372 변 수 장세앙
방 분지들은 방광과 직장에 부교감신경을 분포하여 방광과
직장의 불수의 괄약근의 운동을 조절하며 또한 성기능에
도 기여한다1644)
제1천골 신경근은 천골공의 약 13을 차
지하며 하위 신경근은 상대적으로 보다 더 넓은 천골공의
공간을 가지게 되어 제4천골 신경근은 천골공의 단지 16만
을 차지한다 그러므로 골절이 천골공을 통하여 발생하는 경
우에는 상부의 제1천골과 제2천골 신경근이 하부의 제3천골
과 제4천골 신경근보다 손상을 더 잘 받는다31622354344) 그
리고 천골의 체부와 천골익 사이의 천골공 부위가 특히 제
1천골과 제2천골에서 약하여 천골 골절의 상당히 많은 수
가 신경공을 통하여 발생하며 골절이 발생할 때에 신경근
을 둘러싸고 있는 막이 내측에 유지되어 있어 골절이 전위
되면 천골 신경근이 장력을 받아 손상을 입는다43)
손상 기전
천골 골절을 일으키는 주된 손상의 형태는 교통사고나
추락과 같은 고 에너지 손상이며 단지 천골의 횡 골절만
은 보통 단순히 넘어져 발생한다 골반환의 골절에서는 손
상 기전과 골반 골절의 심한 정도는 상당한 연관성이 있으
나 천골의 골절에서는 천골 골절의 형태와 손상 기전과는
서로 관련이 없다43)
천골 골절은 주로 두 가지 손상 기전에 의하여 발생한
다47) 가장 흔하게는 골반환을 통하여 천골로 전달되는 힘
에 의해서 발생하는 골절이다 이러한 손상 기전으로는 측
방 압박력에 의해 일어나는 천골 골절이 가장 많으며 이
러한 손상은 천골익의 작은 골절이나 천골의 수직 감입 골
절과 같은 안정성이 있는 골절을 일으킨다 그러나 보다
심한 불안정한 Denis zone II의 천골 골절을 일으킬 수도
있다 수직 전단력에 의한 천골 골절은 골반환의 전후방이
모두 손상을 받아 근위부로 전위되는 수직 골절이 발생하
게 된다 전후방 압박력에 의해서는 천골 골절이 잘 일어
나지 않으며 다발성 손상에서는 자주 측방 및 전후방 압
박력이 함께 가해져 천골 골절이 발생하는 경우가 많다
훨씬 덜 흔하게는 천골에 가해지는 직접적인 힘에 의해
발생하는 골절이며 추락으로 인해 둔부로 착지가 되어 발
생하게 된다 이러한 천골 골절은 횡 골절로써 전체 천골
골절의 약 5sim10 정도를 차지하고 있다13)
높은 곳에서
추락하여 발생하는 천골의 근위부 골절 즉 suicidal jump-
errsquos fracture는 대부분은 착지 시에 몸을 보호하기 위하여
자발적으로 요추의 후만 자세를 취하게 되고 천골의 근위
골편은 수평 위치로 되고 원위 골편의 후방으로 전위되며
일부는 착지 시에 뛰어내릴 때의 자세인 양측 고관절의 신
전과 함께 요추의 전만 자세를 취하게 되고 천골의 근위
골편은 원위 골편의 전방으로 전위된다29)
진 단
1 이학적 검사
천골 골절의 약 30는 진단이 늦게 되며 이로 인하여
장기적으로 좋지 못한 결과를 초래할 수 있어 철저한 임상
평가를 통하여 조기 진단을 하여야 한다32228) 환자가 골반
주위에 동통을 호소하면 천골 골절을 의심하고 시진과 촉
진 그리고 이학적 검사들을 하여야 한다 골반 주위에 외
상의 징후가 있거나 특히 천골 골절을 의심하게 하는 천골
의 후방 돌출이나 큰 피하 혈종 (Morel-Lavalle lesion) 등
이 있으면 철저히 진단을 하여야 한다1216)
손상을 입은 환
자에서 직장 검사는 기본적으로 시행하여야 하며 괄약근
의 수축 감각 이상 반사 반응 등 천골 신경근에 대한 기
능적인 평가를 하여야 한다3544)
여성 환자에서는 질 검사
를 통하여 개방성 골반 골절을 놓치지 말아야 한다1643)
2 영상 진단
골반환 손상이 의심되면 골반의 전후면 방사선 영상뿐만
아니라 입구상 (inlet view) 및 출구상 (outlet view)을 함
께 촬영하여야 한다1628)
골반의 입구상에서는 천골의 척추
관과 제1천골의 상부를 명확하게 볼 수 있으며 출구상에
서는 천골의 정확한 전후면 영상을 볼 수 있다 측면상은
전위된 횡 골절을 평가하기 위하여 그리고 suicidal jumperrsquos fracture에서는 시상면에서의 전위 정도를 평가하기 위하여
필요하다 방사선 사진에서 천골 골절의 가능성을 나타내
는 중요한 소견으로는 제5요추 횡돌기 골절 천골의 궁형
선 (arcuate line)의 단절 전방 천골공의 단절을 나타내는
stepladder sign 천극인대나 천결절인대의 견열 골절 등이
있다511161822)
전산화 단층 촬영은 천골의 작은 손상까지
도 정확하게 진단할 수 있게 해주며 복잡한 천골 골절의
진단에 특히 유용하다15222448)
전산화 단층 촬영으로 골절
의 형태를 상세하게 분석할 수 있고 신경 손상을 일으키
는 골편을 확인할 수 있으며 골절의 위치를 정확하게 파
악할 수 있다 또한 골절의 위치와 골편의 크기 등을 분석
하여 내고정을 위한 술전 계획을 철저하게 세울 수 있다
3 전기 생리학적 진단
신경 손상이나 의식장애가 있는 천골 골절 환자는 여러
가지 전기적 진단 (electrodiagnosis)으로 신경 손상을 효과
적으로 평가할 수 있다 항문 주위의 체성 감각 유발 전위
(somatosensory evoked potential)와 항문 괄약근의 근전도
검사는 천골 골절과 관련한 신경 손상을 평가하는데 유용
천골 골 373
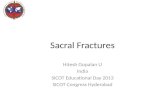
Fig 1 Classification of sacral fractures according to Denis et al Zone I is lateral to the neuroforamina (transalar fracture) Zone II involves the neuroforamina but does not involve the spinal canal (transforaminal fracture) Zone III extends into the spinal canal with primary or associated fracture lines (central fracture)
Fig 2 Subclassification of Denis zone III sacral fractures as described by Roy-Camille et al and modified by Strange-Vognsen and Lebech (A) Type 1 flexion fracture with an anterior simple bending of the upper fragment (B) Type 2 flexion fracture with a posterior displacement of the upper fragment (C) Type 3 extension fracture with an anterior displacement of the upper fragment more and less vertical (D) Type 4 neutral position fracture with marked comminution and nondisplacement of the upper fragment
하고 또한 수술 중에 신경의 상태를 감시하는데 유용하다44)
또한 전기적 진단은 상 운동 신경원 (upper motor neuron)
손상과의 감별에 사용할 수 있으며35)
방광 괄약근 근전도
검사와 함께 시행되는 배뇨 후 잔뇨 측정과 방광 내압 측
정술은 신경원성 방광을 가진 환자의 추적 조사에 이용될
수 있다44)
골절의 분류
천골 골절은 골반환을 침범하지 않은 척추 손상인 횡 골
절 골반환을 침범하고 적어도 어느 정도는 골반환의 불안
정성을 나타내는 종 골절 그리고 횡 골절과 종 골절의 형
태를 모두 가지고 있어 척추-골반 해리 (spino-pelvic dis-
sociation)로 정의되는 복합 골절의 형태로 분류될 수 있다43)
일반적으로 천골 골절은 골반환 골절의 한 부분이며 따
라서 Muumlller AO 분류에 의하면 미골과 제2천골 하방의 횡
골절은 A형 골절로 편측이나 양측의 전후방 압박 골절이
나 측면 압박 골절은 B형 골절로 편측이나 양측의 불안정
한 종 골절은 C형 골절로 분류된다43)
Denis 등3)은 천골을 세 zone으로 나누어 골절을 분류하
였으며 천골 골절에 널리 사용되고 있다 zone I은 천골
의 외측 부위 (transalar fracture) zone II는 천골공 부위
(transforaminal fracture) zone III는 천골공의 내측 부위
(central fracture)를 의미한다 (Fig 1) Denis 등3)의 결과
에 따르면 zone I의 골절이 가장 많아 50를 차지하였고
신경 손상은 59에서 동반되었으며 zone II의 골절은
34를 차지하였고 신경 손상은 284에서 동반되었으며
zone III의 골절은 가장 적어 단지 16를 차지하였으나 신경
손상은 567에서 동반되었다 Roy-Camille 등29)
은 Denis
zone III의 횡 골절을 손상 기전과 전위 정도에 따라 type
1은 천골의 근위 골편이 단순히 전방으로 굽은 굴곡 골절
type 2는 천골의 근위 골편이 후방으로 전위된 굴곡 골절
type 3는 천골의 근위 골편이 전방으로 전위된 신전 골절
로 재분류하였으며 Strange-Vognsen과 Lebech41)
가 이를
수정하여 type 4 천골의 근위 골편은 심하게 분쇄되었으나
374 변 수 장세앙
Fig 3 Complex Denis zone III sacral fractures can be classified descriptively by the letter of the alphabet (A) U-type fracture (B) H-type fracture (C) λ-type (or Y-type) fracture (D) T-type fracture
원위 골편은 전위되지 않은 골절을 추가하였다 (Fig 2)
Roy-Camille 등29)
은 횡 골절과 함께 동반된 양측 종 골
절에서 횡 골절 부분만을 강조하였다 그러나 Denis zone
III 골절 중에서 횡 골절과는 달리 횡 골절과 함께 양측 종
골절이 동반되는 U-형의 천골 골절 즉 척추-골반 해리가
드물게 발생한다 이러한 골절은 형태학적으로 알파벳의
모양대로 U-형 H-형 λ-형 (또는 Y-형) T-형으로 분류되
며 요천추 신경총 손상의 빈도가 높다 (Fig 3)21822293748)
수술적 치료 술기
천골 골절의 수술적 치료 목적은 골편을 정복하여 적절
하게 고정하고 신경조직을 보호하고 손상된 신경은 최대
한 회복될 수 있도록 기회를 제공하는 것이다42sim44)
수술
시기는 치료의 목적 환자의 전신 상태 그리고 수술 술기
의 침습 정도에 기초하여 결정되어야 한다44) 조기에 과감
한 수술은 수술 중에 예기치 못한 출혈이나 술후 연부조직
의 합병증과 감염 등을 일으킬 수 있으며1244)
반면에 신경
의 감압술이 2주 이상 지연되면 신경의 회복에 나쁜 영향
을 줄 수 있다33544)
그러므로 치료 방법이 결정되면 장단
점을 신중하게 고려하여 판단하여야 한다
1 천골 신경근의 감압술
천골 골절에 동반되는 신경 손상은 불완전한 단일 신경
근병증 (monoradiculopathy)에서부터 완전 마미 증후군
(cauda equina syndrome)까지 다양하며 천골 신경근의 좌
상 압박 또는 견인 손상 등은 회복의 가능성이 있으나 신
경근이 절단되거나 견열 (avulsion)된 경우에는 회복의 가
능성이 없다164448)
감압술은 내고정과 함께 시행하며 천
골 신경근에 손상을 주는 골편들을 제거하고 골절의 정복
에 의한 간접적인 방법이나 추궁판 절제술 또는 추공 절단
술 (foraminotomy)에 의한 직접적인 방법으로 감압술을 시
행한다 찢어진 경막은 봉합하여 가성 척수막 공동 (pseudo-
meningocele)이 발생하지 않도록 하여야 한다44)
신경의
회복은 치료 방법과는 상관 없이 전체적으로 약 80에서
호전을 보인다고 하며 수술적 감압술이 보존적 치료보다
좋다고 하기는 어렵지만 수술적 치료 후에 보다 좋은 결과
를 보고한 저자들이 있다378) 신경 손상을 받은 환자에서
감압 수술의 시기는 다소 논란이 있다 신경생리학적 견지
에서 보면 손상을 받은 신경은 손상 후 24시간에서 72시간
내에 조기에 감압술을 시행하는 것이 좋으나 조기에 감압
술을 시행하면 출혈 창상과 관련된 합병증 뇌척수액의 누
출과 같은 합병증이 발생할 수 있으므로 이를 고려하여 수
술 시기와 치료 방법을 신중하게 결정하여야 한다2835)
2 천골 골절의 내고정
불안정한 골반환 손상에서는 후방의 천골 골절에 대한
술식을 하기 전에 골반환의 전방 손상에 대한 술식을 먼저
고려하여야 한다 골반환의 전방 손상은 정복 후 금속판
고정43) 외고정2123) 또는 역행성 치골 나사 고정1726) 등의
방법으로 고정할 수 있으며 전방 고정은 천골 골절을 정
복하는데 도움이 될 수 있으며 복와위에서 후방 술식을
하는 동안 골반환을 보호하는데 도움이 될 수 있다44)
천골 골절은 경피적 방법이나 관혈적 방법으로 정복하여
고정할 수 있으며 두 방법의 장단점을 고려하여 적절한
선택을 하여야 한다 관혈적 방법은 골편을 직접 정복하므
로 해부학적 정복이 가능하며 손상을 받은 신경근을 직접
보고 감압술을 시행할 수 있는 장점이 있다 경피적 방법
천골 골 375
Fig 4 Percutaneous fixation of the iliosacral screw (A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop) (B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet A-P and outlet views of the pelvis
은 앙와위에서 시행할 수 있고 출혈이나 연부조직 합병증
이 거의 없으며 간접 정복으로 만족스러운 정복을 얻을
수 있는 장점이 있다39)
불안정한 천골 골절을 고정하는
방법으로는 장천 나사 고정615162628434446)
경천골 금속판
또는 국소 금속판 고정20) 인장대 금속판 고정16384243) 장
천 지지대 고정 (iliosacral bar)463640)
그리고 척추경 나사
와 장골 나사를 이용한 삼각 내고정과 척추-골반 고정
(spino-pelvic fixation)23031333448) 등이 있으며 장천 지지
대 고정은 최근에는 잘 사용되지 않고 있다
1) 경피적 장천 나사 고정
경피적 장천 나사 고정은 천장관절의 손상뿐만 아니라
여러 천골 골절의 고정에 사용될 수 있다15252743)
장천 나
사는 환자를 앙와위나 복와위에서 경피적으로 삽입할 수
있으며 C-arm을 이용하여 측면상 전후면상 입구상과 출
구상을 보면서 제1천골 체부의 안전한 지역에 조심스럽게
나사를 삽입하여야 한다151643)
나사는 측면상에서는 장골
의 피질골 음영 아래에 위치하여야 하고 천골익의 중심에
삽입하여야 하며 입구상에서는 제1천골의 전방 피질골과
후방 피질골 사이의 체부에 정확하게 삽입하여야 하며
출구상에서는 천골공 바로 위에 놓이도록 하여야 한다
(Fig 4)1543)
최근에는 제한적이지만 3D C-arm을 사용하여
장천 나사를 보다 정확한 위치에 안전하게 삽입하므로 신
경혈관 손상 등의 위험을 줄일 수 있다 장천 나사는 천골
골절 중에서 비관혈적으로 정복이 되는 Denis zone I II
골절과 zone III 골절 중에 type 1 골절에서 경피적으로
삽입할 수 있으며 천골 이형성증 (dysplastic sacrum)이 있
거나 천골 골절이 비관혈적으로 정복이 되지 않을 경우에
는 경피적 장천 나사 고정의 적응이 되지 못한다164344) 분
쇄가 있는 zone II의 천골 골절을 압박 나사로 고정하게
되면 천골공의 지나친 압박으로 인하여 신경의 포착이 발
생할 수 있으므로 완전 나선형의 나사 (fully threaded screw)
로 정적 고정을 하여야 한다1844)
2) 국소 금속판 고정 (local plate osteosynthesis)
작은 금속판을 이용한 국소 금속판 고정법은 천골의 중
376 변 수 장세앙
Fig 5 Methods of surgical stabilization (A) Local plate osteosynthesis (B) Posterior transiliac plate fixation (C) Spino-pelvic fixation (D) Plate stabilization for the low transverse fracture
앙을 가로지르지 않고 천골의 편측에 직접 고정하게 되며
이 때에는 두 개의 금속판을 사용하여 하나는 제1천골에
그리고 다른 하나는 제2천골이나 제3천골에 고정하여 천골
의 회전 불안정성을 방지하도록 하여야 한다 (Fig 5A)20)
금속판의 외측 나사는 천골공의 외측에서 천장관절에 평행
한 방향으로 향하게 하여 천골공이나 척추관을 관통하지
않고 안전하게 삽입할 수 있다 내측 나사는 제1천골에서
는 제5요추-제1천추 후방관절 (facet joint) 바로 아래에서
삽입하게 되며 zone I 골절에서는 천골의 후방 추궁판
(posterior sacral lamina)에 수직으로 그리고 상방 추궁판
(cranial sacral lamina)에 평행하게 삽입하고 zone II 골절
에서는 동일한 위치에서 외측으로 20도 기울여서 삽입하
며 제2천골에서 제4천골까지는 두 천골공 사이의 중간에
서 후방 추궁판에 수직으로 삽입한다2043) 국소 금속판 고
정은 장천 지지대 고정만큼 강하고 천장관절을 고정하지
않고 천골에만 고정하는 장점이 있다20)
3) 후방 경장골 금속판 고정 (transiliac plating)
후방 경장골 금속판 고정은 후방 연부조직 손상이 심하
지 않은 천골의 분쇄 골절에 대하여 적응이 된다 (Fig
5B)144243) 금속판의 삽입을 위해 후상 장골극에서 약 2
cm 외측에서 종절개를 양측에 가하고 대둔근을 기시부에
서 분리하여 골절 부위를 노출시킨다 천골 신경근이 손상
되지 않도록 주의하여 견인과 기구를 이용하여 정복하고
술전 영상 소견상 신경근의 압박이 있으면 감압술을 시행
한다 미리 윤곽 형성한 45-mm 또는 35-mm 금속판을
두 종절개를 통하여 후상 장골극 하방에 위치시키고 양측
장골익에 나사로 고정하며 이 금속판은 인장대 금속판으
로써의 역할을 한다 (Fig 6)1442)
4) 삼각 내고정법 (triangular osteosynthesis)
종축의 요천추 고정과 횡축의 장천골 고정의 조합인 삼
각 내고정법은 불안정한 천골 골절에 효과적인 내고정 방
법이나 내고정의 술기가 복잡하고 내고정물의 제거를 위한
이차 수술이 필요하므로 천골 골절의 분쇄가 심하여 장천
나사 고정으로 견고한 고정을 얻을 수 없는 경우에 사용하
는 것이 좋다30313334)
환자를 복와위로 하여 제4요추부터
천골의 중간까지 중앙 절개를 가하고 정중 측방 접근법
(paramedian approach)으로 제5요추의 척추경 나사 삽입
부위와 장골 나사의 삽입 부위인 후상 장골극 부위와 함께
천골 골절 부위를 포함하여 후방 피질골과 천골공을 노출
시킨다 수술 전에 이학적 및 영상 소견상 신경근의 압박
소견이 있으면 신경근의 감압술로 추궁판 부분 절제술과
함께 신경근을 압박하는 골편을 제거한다 천골 골절은 견
인과 겸자를 사용하여 정복하며 척추-골반 고정을 위하여
삽입한 장골 나사를 joystick으로 사용하여 골절을 정복하
는데 이용할 수 있다 골절은 우선 장천 나사로 고정을 하
고 척추-골반 고정을 하게 된다 척추-골반 고정을 위해 제
5요추에 척추경 나사를 삽입하는데 제5요추의 척추경에
골절이 있거나 제5요추의 전만증이 심하거나 요천추의 이
상 형태 (dysmorphism)가 있으면 제4요추의 척추경에 나사
를 삽입하여야 한다 장골 나사의 삽입 부위는 후상 장골
극 바로 전하방이며 이 고정 자체가 커서 피하조직에 자
극을 주므로 천골과 후상 장골극의 후방 피질골 사이의 틈
에 삽입하는 것이 중요하다 삽입 방향은 전방 측방 하방
으로 향하도록 하여야 하며 삽입 후 나사는 골반의 외측
및 내측 피질골 사이에 그리고 좌골 지지대 (sciatic but-
tress) 바로 위에 놓여야 한다 정확한 나사의 위치가 내측
및 외측 사면 영상에서 확인이 되면 rod와 적절한 clamp
로 장골 나사와 척추경 나사를 연결한다3031)
천골 골 377
Fig 6 This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident (A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum (B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma (C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures
5) 척추-골반 고정 (spino-pelvic fixation)
요천추 고정은 후방 중앙 접근법으로 요추의 횡돌기 천
골익과 후상 장골극 부위를 노출시키고 신경근의 압박 소
견이 있으면 직접적인 방법으로 신경근을 압박하는 골편의
제거와 추궁판 절제술을 시행하고 간접적인 방법으로 골절
의 정복에 의한 신경근의 감압술을 시행한다 골절은 견인
과 Schanz screw를 이용한 joystick 방법이나 겸자 등으로
천골의 길이 복구와 함께 골절을 정복하고 고정은 삼각
내고정법에서와 같은 방법으로 양측에 각각 제45요추에
척추경 나사와 후상 장골극 부위에 장골 나사를 삽입하여
rod와 적절한 clamp로 고정하고 양측의 rod는 서로
cross-connector나 transverse bar로 연결하여 압박한다
(Fig 5C)3248)
수술의 적응증과 골절 형태에 따른 치료
수술적 치료의 적응증은 골반의 불안정성 정도 골절의
전위 정도 그리고 부가적으로 천골 골절에 동반된 신경 손
상에 의해서 결정된다1643)
그러나 환자의 전신상태가 매우
불량하거나 골반골의 골다공증이 심한 경우에는 수술적 치
료의 적응이 되지 못한다
1 전위된 천골의 횡 골절
제2천골 아래의 횡 골절은 보통은 전위가 일어나지 않으
므로 주로 보존적 치료를 한다 그러나 드물지만 골편의
심한 전위로 인하여 직장이나 항문의 기능 장애를 일으키
거나 하위 천골 신경근의 손상이 있을 때에는 수술의 적응
이 되며 신경근의 감압술로 추궁판 절제술을 시행하고 금
속판으로 골편을 고정하여야 한다 (Fig 5D)43)
2 회전 불안정성 천골 골절
회전 불안정성 천골 골절의 대부분은 전위가 거의 일어
나지 않아 안정하므로 특별한 고정이 요하지 않으며 보존
적 치료로 좋은 결과를 얻을 수 있다 천골의 전후방 압박
골절은 매우 드물며 zone II에서 보통 발생한다 전방 손
상은 대부분 치골 결합부의 손상으로 치골 결합부가 25
378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

372 변 수 장세앙
방 분지들은 방광과 직장에 부교감신경을 분포하여 방광과
직장의 불수의 괄약근의 운동을 조절하며 또한 성기능에
도 기여한다1644)
제1천골 신경근은 천골공의 약 13을 차
지하며 하위 신경근은 상대적으로 보다 더 넓은 천골공의
공간을 가지게 되어 제4천골 신경근은 천골공의 단지 16만
을 차지한다 그러므로 골절이 천골공을 통하여 발생하는 경
우에는 상부의 제1천골과 제2천골 신경근이 하부의 제3천골
과 제4천골 신경근보다 손상을 더 잘 받는다31622354344) 그
리고 천골의 체부와 천골익 사이의 천골공 부위가 특히 제
1천골과 제2천골에서 약하여 천골 골절의 상당히 많은 수
가 신경공을 통하여 발생하며 골절이 발생할 때에 신경근
을 둘러싸고 있는 막이 내측에 유지되어 있어 골절이 전위
되면 천골 신경근이 장력을 받아 손상을 입는다43)
손상 기전
천골 골절을 일으키는 주된 손상의 형태는 교통사고나
추락과 같은 고 에너지 손상이며 단지 천골의 횡 골절만
은 보통 단순히 넘어져 발생한다 골반환의 골절에서는 손
상 기전과 골반 골절의 심한 정도는 상당한 연관성이 있으
나 천골의 골절에서는 천골 골절의 형태와 손상 기전과는
서로 관련이 없다43)
천골 골절은 주로 두 가지 손상 기전에 의하여 발생한
다47) 가장 흔하게는 골반환을 통하여 천골로 전달되는 힘
에 의해서 발생하는 골절이다 이러한 손상 기전으로는 측
방 압박력에 의해 일어나는 천골 골절이 가장 많으며 이
러한 손상은 천골익의 작은 골절이나 천골의 수직 감입 골
절과 같은 안정성이 있는 골절을 일으킨다 그러나 보다
심한 불안정한 Denis zone II의 천골 골절을 일으킬 수도
있다 수직 전단력에 의한 천골 골절은 골반환의 전후방이
모두 손상을 받아 근위부로 전위되는 수직 골절이 발생하
게 된다 전후방 압박력에 의해서는 천골 골절이 잘 일어
나지 않으며 다발성 손상에서는 자주 측방 및 전후방 압
박력이 함께 가해져 천골 골절이 발생하는 경우가 많다
훨씬 덜 흔하게는 천골에 가해지는 직접적인 힘에 의해
발생하는 골절이며 추락으로 인해 둔부로 착지가 되어 발
생하게 된다 이러한 천골 골절은 횡 골절로써 전체 천골
골절의 약 5sim10 정도를 차지하고 있다13)
높은 곳에서
추락하여 발생하는 천골의 근위부 골절 즉 suicidal jump-
errsquos fracture는 대부분은 착지 시에 몸을 보호하기 위하여
자발적으로 요추의 후만 자세를 취하게 되고 천골의 근위
골편은 수평 위치로 되고 원위 골편의 후방으로 전위되며
일부는 착지 시에 뛰어내릴 때의 자세인 양측 고관절의 신
전과 함께 요추의 전만 자세를 취하게 되고 천골의 근위
골편은 원위 골편의 전방으로 전위된다29)
진 단
1 이학적 검사
천골 골절의 약 30는 진단이 늦게 되며 이로 인하여
장기적으로 좋지 못한 결과를 초래할 수 있어 철저한 임상
평가를 통하여 조기 진단을 하여야 한다32228) 환자가 골반
주위에 동통을 호소하면 천골 골절을 의심하고 시진과 촉
진 그리고 이학적 검사들을 하여야 한다 골반 주위에 외
상의 징후가 있거나 특히 천골 골절을 의심하게 하는 천골
의 후방 돌출이나 큰 피하 혈종 (Morel-Lavalle lesion) 등
이 있으면 철저히 진단을 하여야 한다1216)
손상을 입은 환
자에서 직장 검사는 기본적으로 시행하여야 하며 괄약근
의 수축 감각 이상 반사 반응 등 천골 신경근에 대한 기
능적인 평가를 하여야 한다3544)
여성 환자에서는 질 검사
를 통하여 개방성 골반 골절을 놓치지 말아야 한다1643)
2 영상 진단
골반환 손상이 의심되면 골반의 전후면 방사선 영상뿐만
아니라 입구상 (inlet view) 및 출구상 (outlet view)을 함
께 촬영하여야 한다1628)
골반의 입구상에서는 천골의 척추
관과 제1천골의 상부를 명확하게 볼 수 있으며 출구상에
서는 천골의 정확한 전후면 영상을 볼 수 있다 측면상은
전위된 횡 골절을 평가하기 위하여 그리고 suicidal jumperrsquos fracture에서는 시상면에서의 전위 정도를 평가하기 위하여
필요하다 방사선 사진에서 천골 골절의 가능성을 나타내
는 중요한 소견으로는 제5요추 횡돌기 골절 천골의 궁형
선 (arcuate line)의 단절 전방 천골공의 단절을 나타내는
stepladder sign 천극인대나 천결절인대의 견열 골절 등이
있다511161822)
전산화 단층 촬영은 천골의 작은 손상까지
도 정확하게 진단할 수 있게 해주며 복잡한 천골 골절의
진단에 특히 유용하다15222448)
전산화 단층 촬영으로 골절
의 형태를 상세하게 분석할 수 있고 신경 손상을 일으키
는 골편을 확인할 수 있으며 골절의 위치를 정확하게 파
악할 수 있다 또한 골절의 위치와 골편의 크기 등을 분석
하여 내고정을 위한 술전 계획을 철저하게 세울 수 있다
3 전기 생리학적 진단
신경 손상이나 의식장애가 있는 천골 골절 환자는 여러
가지 전기적 진단 (electrodiagnosis)으로 신경 손상을 효과
적으로 평가할 수 있다 항문 주위의 체성 감각 유발 전위
(somatosensory evoked potential)와 항문 괄약근의 근전도
검사는 천골 골절과 관련한 신경 손상을 평가하는데 유용
천골 골 373
Fig 1 Classification of sacral fractures according to Denis et al Zone I is lateral to the neuroforamina (transalar fracture) Zone II involves the neuroforamina but does not involve the spinal canal (transforaminal fracture) Zone III extends into the spinal canal with primary or associated fracture lines (central fracture)
Fig 2 Subclassification of Denis zone III sacral fractures as described by Roy-Camille et al and modified by Strange-Vognsen and Lebech (A) Type 1 flexion fracture with an anterior simple bending of the upper fragment (B) Type 2 flexion fracture with a posterior displacement of the upper fragment (C) Type 3 extension fracture with an anterior displacement of the upper fragment more and less vertical (D) Type 4 neutral position fracture with marked comminution and nondisplacement of the upper fragment
하고 또한 수술 중에 신경의 상태를 감시하는데 유용하다44)
또한 전기적 진단은 상 운동 신경원 (upper motor neuron)
손상과의 감별에 사용할 수 있으며35)
방광 괄약근 근전도
검사와 함께 시행되는 배뇨 후 잔뇨 측정과 방광 내압 측
정술은 신경원성 방광을 가진 환자의 추적 조사에 이용될
수 있다44)
골절의 분류
천골 골절은 골반환을 침범하지 않은 척추 손상인 횡 골
절 골반환을 침범하고 적어도 어느 정도는 골반환의 불안
정성을 나타내는 종 골절 그리고 횡 골절과 종 골절의 형
태를 모두 가지고 있어 척추-골반 해리 (spino-pelvic dis-
sociation)로 정의되는 복합 골절의 형태로 분류될 수 있다43)
일반적으로 천골 골절은 골반환 골절의 한 부분이며 따
라서 Muumlller AO 분류에 의하면 미골과 제2천골 하방의 횡
골절은 A형 골절로 편측이나 양측의 전후방 압박 골절이
나 측면 압박 골절은 B형 골절로 편측이나 양측의 불안정
한 종 골절은 C형 골절로 분류된다43)
Denis 등3)은 천골을 세 zone으로 나누어 골절을 분류하
였으며 천골 골절에 널리 사용되고 있다 zone I은 천골
의 외측 부위 (transalar fracture) zone II는 천골공 부위
(transforaminal fracture) zone III는 천골공의 내측 부위
(central fracture)를 의미한다 (Fig 1) Denis 등3)의 결과
에 따르면 zone I의 골절이 가장 많아 50를 차지하였고
신경 손상은 59에서 동반되었으며 zone II의 골절은
34를 차지하였고 신경 손상은 284에서 동반되었으며
zone III의 골절은 가장 적어 단지 16를 차지하였으나 신경
손상은 567에서 동반되었다 Roy-Camille 등29)
은 Denis
zone III의 횡 골절을 손상 기전과 전위 정도에 따라 type
1은 천골의 근위 골편이 단순히 전방으로 굽은 굴곡 골절
type 2는 천골의 근위 골편이 후방으로 전위된 굴곡 골절
type 3는 천골의 근위 골편이 전방으로 전위된 신전 골절
로 재분류하였으며 Strange-Vognsen과 Lebech41)
가 이를
수정하여 type 4 천골의 근위 골편은 심하게 분쇄되었으나
374 변 수 장세앙
Fig 3 Complex Denis zone III sacral fractures can be classified descriptively by the letter of the alphabet (A) U-type fracture (B) H-type fracture (C) λ-type (or Y-type) fracture (D) T-type fracture
원위 골편은 전위되지 않은 골절을 추가하였다 (Fig 2)
Roy-Camille 등29)
은 횡 골절과 함께 동반된 양측 종 골
절에서 횡 골절 부분만을 강조하였다 그러나 Denis zone
III 골절 중에서 횡 골절과는 달리 횡 골절과 함께 양측 종
골절이 동반되는 U-형의 천골 골절 즉 척추-골반 해리가
드물게 발생한다 이러한 골절은 형태학적으로 알파벳의
모양대로 U-형 H-형 λ-형 (또는 Y-형) T-형으로 분류되
며 요천추 신경총 손상의 빈도가 높다 (Fig 3)21822293748)
수술적 치료 술기
천골 골절의 수술적 치료 목적은 골편을 정복하여 적절
하게 고정하고 신경조직을 보호하고 손상된 신경은 최대
한 회복될 수 있도록 기회를 제공하는 것이다42sim44)
수술
시기는 치료의 목적 환자의 전신 상태 그리고 수술 술기
의 침습 정도에 기초하여 결정되어야 한다44) 조기에 과감
한 수술은 수술 중에 예기치 못한 출혈이나 술후 연부조직
의 합병증과 감염 등을 일으킬 수 있으며1244)
반면에 신경
의 감압술이 2주 이상 지연되면 신경의 회복에 나쁜 영향
을 줄 수 있다33544)
그러므로 치료 방법이 결정되면 장단
점을 신중하게 고려하여 판단하여야 한다
1 천골 신경근의 감압술
천골 골절에 동반되는 신경 손상은 불완전한 단일 신경
근병증 (monoradiculopathy)에서부터 완전 마미 증후군
(cauda equina syndrome)까지 다양하며 천골 신경근의 좌
상 압박 또는 견인 손상 등은 회복의 가능성이 있으나 신
경근이 절단되거나 견열 (avulsion)된 경우에는 회복의 가
능성이 없다164448)
감압술은 내고정과 함께 시행하며 천
골 신경근에 손상을 주는 골편들을 제거하고 골절의 정복
에 의한 간접적인 방법이나 추궁판 절제술 또는 추공 절단
술 (foraminotomy)에 의한 직접적인 방법으로 감압술을 시
행한다 찢어진 경막은 봉합하여 가성 척수막 공동 (pseudo-
meningocele)이 발생하지 않도록 하여야 한다44)
신경의
회복은 치료 방법과는 상관 없이 전체적으로 약 80에서
호전을 보인다고 하며 수술적 감압술이 보존적 치료보다
좋다고 하기는 어렵지만 수술적 치료 후에 보다 좋은 결과
를 보고한 저자들이 있다378) 신경 손상을 받은 환자에서
감압 수술의 시기는 다소 논란이 있다 신경생리학적 견지
에서 보면 손상을 받은 신경은 손상 후 24시간에서 72시간
내에 조기에 감압술을 시행하는 것이 좋으나 조기에 감압
술을 시행하면 출혈 창상과 관련된 합병증 뇌척수액의 누
출과 같은 합병증이 발생할 수 있으므로 이를 고려하여 수
술 시기와 치료 방법을 신중하게 결정하여야 한다2835)
2 천골 골절의 내고정
불안정한 골반환 손상에서는 후방의 천골 골절에 대한
술식을 하기 전에 골반환의 전방 손상에 대한 술식을 먼저
고려하여야 한다 골반환의 전방 손상은 정복 후 금속판
고정43) 외고정2123) 또는 역행성 치골 나사 고정1726) 등의
방법으로 고정할 수 있으며 전방 고정은 천골 골절을 정
복하는데 도움이 될 수 있으며 복와위에서 후방 술식을
하는 동안 골반환을 보호하는데 도움이 될 수 있다44)
천골 골절은 경피적 방법이나 관혈적 방법으로 정복하여
고정할 수 있으며 두 방법의 장단점을 고려하여 적절한
선택을 하여야 한다 관혈적 방법은 골편을 직접 정복하므
로 해부학적 정복이 가능하며 손상을 받은 신경근을 직접
보고 감압술을 시행할 수 있는 장점이 있다 경피적 방법
천골 골 375
Fig 4 Percutaneous fixation of the iliosacral screw (A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop) (B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet A-P and outlet views of the pelvis
은 앙와위에서 시행할 수 있고 출혈이나 연부조직 합병증
이 거의 없으며 간접 정복으로 만족스러운 정복을 얻을
수 있는 장점이 있다39)
불안정한 천골 골절을 고정하는
방법으로는 장천 나사 고정615162628434446)
경천골 금속판
또는 국소 금속판 고정20) 인장대 금속판 고정16384243) 장
천 지지대 고정 (iliosacral bar)463640)
그리고 척추경 나사
와 장골 나사를 이용한 삼각 내고정과 척추-골반 고정
(spino-pelvic fixation)23031333448) 등이 있으며 장천 지지
대 고정은 최근에는 잘 사용되지 않고 있다
1) 경피적 장천 나사 고정
경피적 장천 나사 고정은 천장관절의 손상뿐만 아니라
여러 천골 골절의 고정에 사용될 수 있다15252743)
장천 나
사는 환자를 앙와위나 복와위에서 경피적으로 삽입할 수
있으며 C-arm을 이용하여 측면상 전후면상 입구상과 출
구상을 보면서 제1천골 체부의 안전한 지역에 조심스럽게
나사를 삽입하여야 한다151643)
나사는 측면상에서는 장골
의 피질골 음영 아래에 위치하여야 하고 천골익의 중심에
삽입하여야 하며 입구상에서는 제1천골의 전방 피질골과
후방 피질골 사이의 체부에 정확하게 삽입하여야 하며
출구상에서는 천골공 바로 위에 놓이도록 하여야 한다
(Fig 4)1543)
최근에는 제한적이지만 3D C-arm을 사용하여
장천 나사를 보다 정확한 위치에 안전하게 삽입하므로 신
경혈관 손상 등의 위험을 줄일 수 있다 장천 나사는 천골
골절 중에서 비관혈적으로 정복이 되는 Denis zone I II
골절과 zone III 골절 중에 type 1 골절에서 경피적으로
삽입할 수 있으며 천골 이형성증 (dysplastic sacrum)이 있
거나 천골 골절이 비관혈적으로 정복이 되지 않을 경우에
는 경피적 장천 나사 고정의 적응이 되지 못한다164344) 분
쇄가 있는 zone II의 천골 골절을 압박 나사로 고정하게
되면 천골공의 지나친 압박으로 인하여 신경의 포착이 발
생할 수 있으므로 완전 나선형의 나사 (fully threaded screw)
로 정적 고정을 하여야 한다1844)
2) 국소 금속판 고정 (local plate osteosynthesis)
작은 금속판을 이용한 국소 금속판 고정법은 천골의 중
376 변 수 장세앙
Fig 5 Methods of surgical stabilization (A) Local plate osteosynthesis (B) Posterior transiliac plate fixation (C) Spino-pelvic fixation (D) Plate stabilization for the low transverse fracture
앙을 가로지르지 않고 천골의 편측에 직접 고정하게 되며
이 때에는 두 개의 금속판을 사용하여 하나는 제1천골에
그리고 다른 하나는 제2천골이나 제3천골에 고정하여 천골
의 회전 불안정성을 방지하도록 하여야 한다 (Fig 5A)20)
금속판의 외측 나사는 천골공의 외측에서 천장관절에 평행
한 방향으로 향하게 하여 천골공이나 척추관을 관통하지
않고 안전하게 삽입할 수 있다 내측 나사는 제1천골에서
는 제5요추-제1천추 후방관절 (facet joint) 바로 아래에서
삽입하게 되며 zone I 골절에서는 천골의 후방 추궁판
(posterior sacral lamina)에 수직으로 그리고 상방 추궁판
(cranial sacral lamina)에 평행하게 삽입하고 zone II 골절
에서는 동일한 위치에서 외측으로 20도 기울여서 삽입하
며 제2천골에서 제4천골까지는 두 천골공 사이의 중간에
서 후방 추궁판에 수직으로 삽입한다2043) 국소 금속판 고
정은 장천 지지대 고정만큼 강하고 천장관절을 고정하지
않고 천골에만 고정하는 장점이 있다20)
3) 후방 경장골 금속판 고정 (transiliac plating)
후방 경장골 금속판 고정은 후방 연부조직 손상이 심하
지 않은 천골의 분쇄 골절에 대하여 적응이 된다 (Fig
5B)144243) 금속판의 삽입을 위해 후상 장골극에서 약 2
cm 외측에서 종절개를 양측에 가하고 대둔근을 기시부에
서 분리하여 골절 부위를 노출시킨다 천골 신경근이 손상
되지 않도록 주의하여 견인과 기구를 이용하여 정복하고
술전 영상 소견상 신경근의 압박이 있으면 감압술을 시행
한다 미리 윤곽 형성한 45-mm 또는 35-mm 금속판을
두 종절개를 통하여 후상 장골극 하방에 위치시키고 양측
장골익에 나사로 고정하며 이 금속판은 인장대 금속판으
로써의 역할을 한다 (Fig 6)1442)
4) 삼각 내고정법 (triangular osteosynthesis)
종축의 요천추 고정과 횡축의 장천골 고정의 조합인 삼
각 내고정법은 불안정한 천골 골절에 효과적인 내고정 방
법이나 내고정의 술기가 복잡하고 내고정물의 제거를 위한
이차 수술이 필요하므로 천골 골절의 분쇄가 심하여 장천
나사 고정으로 견고한 고정을 얻을 수 없는 경우에 사용하
는 것이 좋다30313334)
환자를 복와위로 하여 제4요추부터
천골의 중간까지 중앙 절개를 가하고 정중 측방 접근법
(paramedian approach)으로 제5요추의 척추경 나사 삽입
부위와 장골 나사의 삽입 부위인 후상 장골극 부위와 함께
천골 골절 부위를 포함하여 후방 피질골과 천골공을 노출
시킨다 수술 전에 이학적 및 영상 소견상 신경근의 압박
소견이 있으면 신경근의 감압술로 추궁판 부분 절제술과
함께 신경근을 압박하는 골편을 제거한다 천골 골절은 견
인과 겸자를 사용하여 정복하며 척추-골반 고정을 위하여
삽입한 장골 나사를 joystick으로 사용하여 골절을 정복하
는데 이용할 수 있다 골절은 우선 장천 나사로 고정을 하
고 척추-골반 고정을 하게 된다 척추-골반 고정을 위해 제
5요추에 척추경 나사를 삽입하는데 제5요추의 척추경에
골절이 있거나 제5요추의 전만증이 심하거나 요천추의 이
상 형태 (dysmorphism)가 있으면 제4요추의 척추경에 나사
를 삽입하여야 한다 장골 나사의 삽입 부위는 후상 장골
극 바로 전하방이며 이 고정 자체가 커서 피하조직에 자
극을 주므로 천골과 후상 장골극의 후방 피질골 사이의 틈
에 삽입하는 것이 중요하다 삽입 방향은 전방 측방 하방
으로 향하도록 하여야 하며 삽입 후 나사는 골반의 외측
및 내측 피질골 사이에 그리고 좌골 지지대 (sciatic but-
tress) 바로 위에 놓여야 한다 정확한 나사의 위치가 내측
및 외측 사면 영상에서 확인이 되면 rod와 적절한 clamp
로 장골 나사와 척추경 나사를 연결한다3031)
천골 골 377
Fig 6 This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident (A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum (B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma (C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures
5) 척추-골반 고정 (spino-pelvic fixation)
요천추 고정은 후방 중앙 접근법으로 요추의 횡돌기 천
골익과 후상 장골극 부위를 노출시키고 신경근의 압박 소
견이 있으면 직접적인 방법으로 신경근을 압박하는 골편의
제거와 추궁판 절제술을 시행하고 간접적인 방법으로 골절
의 정복에 의한 신경근의 감압술을 시행한다 골절은 견인
과 Schanz screw를 이용한 joystick 방법이나 겸자 등으로
천골의 길이 복구와 함께 골절을 정복하고 고정은 삼각
내고정법에서와 같은 방법으로 양측에 각각 제45요추에
척추경 나사와 후상 장골극 부위에 장골 나사를 삽입하여
rod와 적절한 clamp로 고정하고 양측의 rod는 서로
cross-connector나 transverse bar로 연결하여 압박한다
(Fig 5C)3248)
수술의 적응증과 골절 형태에 따른 치료
수술적 치료의 적응증은 골반의 불안정성 정도 골절의
전위 정도 그리고 부가적으로 천골 골절에 동반된 신경 손
상에 의해서 결정된다1643)
그러나 환자의 전신상태가 매우
불량하거나 골반골의 골다공증이 심한 경우에는 수술적 치
료의 적응이 되지 못한다
1 전위된 천골의 횡 골절
제2천골 아래의 횡 골절은 보통은 전위가 일어나지 않으
므로 주로 보존적 치료를 한다 그러나 드물지만 골편의
심한 전위로 인하여 직장이나 항문의 기능 장애를 일으키
거나 하위 천골 신경근의 손상이 있을 때에는 수술의 적응
이 되며 신경근의 감압술로 추궁판 절제술을 시행하고 금
속판으로 골편을 고정하여야 한다 (Fig 5D)43)
2 회전 불안정성 천골 골절
회전 불안정성 천골 골절의 대부분은 전위가 거의 일어
나지 않아 안정하므로 특별한 고정이 요하지 않으며 보존
적 치료로 좋은 결과를 얻을 수 있다 천골의 전후방 압박
골절은 매우 드물며 zone II에서 보통 발생한다 전방 손
상은 대부분 치골 결합부의 손상으로 치골 결합부가 25
378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

천골 골 373
Fig 1 Classification of sacral fractures according to Denis et al Zone I is lateral to the neuroforamina (transalar fracture) Zone II involves the neuroforamina but does not involve the spinal canal (transforaminal fracture) Zone III extends into the spinal canal with primary or associated fracture lines (central fracture)
Fig 2 Subclassification of Denis zone III sacral fractures as described by Roy-Camille et al and modified by Strange-Vognsen and Lebech (A) Type 1 flexion fracture with an anterior simple bending of the upper fragment (B) Type 2 flexion fracture with a posterior displacement of the upper fragment (C) Type 3 extension fracture with an anterior displacement of the upper fragment more and less vertical (D) Type 4 neutral position fracture with marked comminution and nondisplacement of the upper fragment
하고 또한 수술 중에 신경의 상태를 감시하는데 유용하다44)
또한 전기적 진단은 상 운동 신경원 (upper motor neuron)
손상과의 감별에 사용할 수 있으며35)
방광 괄약근 근전도
검사와 함께 시행되는 배뇨 후 잔뇨 측정과 방광 내압 측
정술은 신경원성 방광을 가진 환자의 추적 조사에 이용될
수 있다44)
골절의 분류
천골 골절은 골반환을 침범하지 않은 척추 손상인 횡 골
절 골반환을 침범하고 적어도 어느 정도는 골반환의 불안
정성을 나타내는 종 골절 그리고 횡 골절과 종 골절의 형
태를 모두 가지고 있어 척추-골반 해리 (spino-pelvic dis-
sociation)로 정의되는 복합 골절의 형태로 분류될 수 있다43)
일반적으로 천골 골절은 골반환 골절의 한 부분이며 따
라서 Muumlller AO 분류에 의하면 미골과 제2천골 하방의 횡
골절은 A형 골절로 편측이나 양측의 전후방 압박 골절이
나 측면 압박 골절은 B형 골절로 편측이나 양측의 불안정
한 종 골절은 C형 골절로 분류된다43)
Denis 등3)은 천골을 세 zone으로 나누어 골절을 분류하
였으며 천골 골절에 널리 사용되고 있다 zone I은 천골
의 외측 부위 (transalar fracture) zone II는 천골공 부위
(transforaminal fracture) zone III는 천골공의 내측 부위
(central fracture)를 의미한다 (Fig 1) Denis 등3)의 결과
에 따르면 zone I의 골절이 가장 많아 50를 차지하였고
신경 손상은 59에서 동반되었으며 zone II의 골절은
34를 차지하였고 신경 손상은 284에서 동반되었으며
zone III의 골절은 가장 적어 단지 16를 차지하였으나 신경
손상은 567에서 동반되었다 Roy-Camille 등29)
은 Denis
zone III의 횡 골절을 손상 기전과 전위 정도에 따라 type
1은 천골의 근위 골편이 단순히 전방으로 굽은 굴곡 골절
type 2는 천골의 근위 골편이 후방으로 전위된 굴곡 골절
type 3는 천골의 근위 골편이 전방으로 전위된 신전 골절
로 재분류하였으며 Strange-Vognsen과 Lebech41)
가 이를
수정하여 type 4 천골의 근위 골편은 심하게 분쇄되었으나
374 변 수 장세앙
Fig 3 Complex Denis zone III sacral fractures can be classified descriptively by the letter of the alphabet (A) U-type fracture (B) H-type fracture (C) λ-type (or Y-type) fracture (D) T-type fracture
원위 골편은 전위되지 않은 골절을 추가하였다 (Fig 2)
Roy-Camille 등29)
은 횡 골절과 함께 동반된 양측 종 골
절에서 횡 골절 부분만을 강조하였다 그러나 Denis zone
III 골절 중에서 횡 골절과는 달리 횡 골절과 함께 양측 종
골절이 동반되는 U-형의 천골 골절 즉 척추-골반 해리가
드물게 발생한다 이러한 골절은 형태학적으로 알파벳의
모양대로 U-형 H-형 λ-형 (또는 Y-형) T-형으로 분류되
며 요천추 신경총 손상의 빈도가 높다 (Fig 3)21822293748)
수술적 치료 술기
천골 골절의 수술적 치료 목적은 골편을 정복하여 적절
하게 고정하고 신경조직을 보호하고 손상된 신경은 최대
한 회복될 수 있도록 기회를 제공하는 것이다42sim44)
수술
시기는 치료의 목적 환자의 전신 상태 그리고 수술 술기
의 침습 정도에 기초하여 결정되어야 한다44) 조기에 과감
한 수술은 수술 중에 예기치 못한 출혈이나 술후 연부조직
의 합병증과 감염 등을 일으킬 수 있으며1244)
반면에 신경
의 감압술이 2주 이상 지연되면 신경의 회복에 나쁜 영향
을 줄 수 있다33544)
그러므로 치료 방법이 결정되면 장단
점을 신중하게 고려하여 판단하여야 한다
1 천골 신경근의 감압술
천골 골절에 동반되는 신경 손상은 불완전한 단일 신경
근병증 (monoradiculopathy)에서부터 완전 마미 증후군
(cauda equina syndrome)까지 다양하며 천골 신경근의 좌
상 압박 또는 견인 손상 등은 회복의 가능성이 있으나 신
경근이 절단되거나 견열 (avulsion)된 경우에는 회복의 가
능성이 없다164448)
감압술은 내고정과 함께 시행하며 천
골 신경근에 손상을 주는 골편들을 제거하고 골절의 정복
에 의한 간접적인 방법이나 추궁판 절제술 또는 추공 절단
술 (foraminotomy)에 의한 직접적인 방법으로 감압술을 시
행한다 찢어진 경막은 봉합하여 가성 척수막 공동 (pseudo-
meningocele)이 발생하지 않도록 하여야 한다44)
신경의
회복은 치료 방법과는 상관 없이 전체적으로 약 80에서
호전을 보인다고 하며 수술적 감압술이 보존적 치료보다
좋다고 하기는 어렵지만 수술적 치료 후에 보다 좋은 결과
를 보고한 저자들이 있다378) 신경 손상을 받은 환자에서
감압 수술의 시기는 다소 논란이 있다 신경생리학적 견지
에서 보면 손상을 받은 신경은 손상 후 24시간에서 72시간
내에 조기에 감압술을 시행하는 것이 좋으나 조기에 감압
술을 시행하면 출혈 창상과 관련된 합병증 뇌척수액의 누
출과 같은 합병증이 발생할 수 있으므로 이를 고려하여 수
술 시기와 치료 방법을 신중하게 결정하여야 한다2835)
2 천골 골절의 내고정
불안정한 골반환 손상에서는 후방의 천골 골절에 대한
술식을 하기 전에 골반환의 전방 손상에 대한 술식을 먼저
고려하여야 한다 골반환의 전방 손상은 정복 후 금속판
고정43) 외고정2123) 또는 역행성 치골 나사 고정1726) 등의
방법으로 고정할 수 있으며 전방 고정은 천골 골절을 정
복하는데 도움이 될 수 있으며 복와위에서 후방 술식을
하는 동안 골반환을 보호하는데 도움이 될 수 있다44)
천골 골절은 경피적 방법이나 관혈적 방법으로 정복하여
고정할 수 있으며 두 방법의 장단점을 고려하여 적절한
선택을 하여야 한다 관혈적 방법은 골편을 직접 정복하므
로 해부학적 정복이 가능하며 손상을 받은 신경근을 직접
보고 감압술을 시행할 수 있는 장점이 있다 경피적 방법
천골 골 375
Fig 4 Percutaneous fixation of the iliosacral screw (A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop) (B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet A-P and outlet views of the pelvis
은 앙와위에서 시행할 수 있고 출혈이나 연부조직 합병증
이 거의 없으며 간접 정복으로 만족스러운 정복을 얻을
수 있는 장점이 있다39)
불안정한 천골 골절을 고정하는
방법으로는 장천 나사 고정615162628434446)
경천골 금속판
또는 국소 금속판 고정20) 인장대 금속판 고정16384243) 장
천 지지대 고정 (iliosacral bar)463640)
그리고 척추경 나사
와 장골 나사를 이용한 삼각 내고정과 척추-골반 고정
(spino-pelvic fixation)23031333448) 등이 있으며 장천 지지
대 고정은 최근에는 잘 사용되지 않고 있다
1) 경피적 장천 나사 고정
경피적 장천 나사 고정은 천장관절의 손상뿐만 아니라
여러 천골 골절의 고정에 사용될 수 있다15252743)
장천 나
사는 환자를 앙와위나 복와위에서 경피적으로 삽입할 수
있으며 C-arm을 이용하여 측면상 전후면상 입구상과 출
구상을 보면서 제1천골 체부의 안전한 지역에 조심스럽게
나사를 삽입하여야 한다151643)
나사는 측면상에서는 장골
의 피질골 음영 아래에 위치하여야 하고 천골익의 중심에
삽입하여야 하며 입구상에서는 제1천골의 전방 피질골과
후방 피질골 사이의 체부에 정확하게 삽입하여야 하며
출구상에서는 천골공 바로 위에 놓이도록 하여야 한다
(Fig 4)1543)
최근에는 제한적이지만 3D C-arm을 사용하여
장천 나사를 보다 정확한 위치에 안전하게 삽입하므로 신
경혈관 손상 등의 위험을 줄일 수 있다 장천 나사는 천골
골절 중에서 비관혈적으로 정복이 되는 Denis zone I II
골절과 zone III 골절 중에 type 1 골절에서 경피적으로
삽입할 수 있으며 천골 이형성증 (dysplastic sacrum)이 있
거나 천골 골절이 비관혈적으로 정복이 되지 않을 경우에
는 경피적 장천 나사 고정의 적응이 되지 못한다164344) 분
쇄가 있는 zone II의 천골 골절을 압박 나사로 고정하게
되면 천골공의 지나친 압박으로 인하여 신경의 포착이 발
생할 수 있으므로 완전 나선형의 나사 (fully threaded screw)
로 정적 고정을 하여야 한다1844)
2) 국소 금속판 고정 (local plate osteosynthesis)
작은 금속판을 이용한 국소 금속판 고정법은 천골의 중
376 변 수 장세앙
Fig 5 Methods of surgical stabilization (A) Local plate osteosynthesis (B) Posterior transiliac plate fixation (C) Spino-pelvic fixation (D) Plate stabilization for the low transverse fracture
앙을 가로지르지 않고 천골의 편측에 직접 고정하게 되며
이 때에는 두 개의 금속판을 사용하여 하나는 제1천골에
그리고 다른 하나는 제2천골이나 제3천골에 고정하여 천골
의 회전 불안정성을 방지하도록 하여야 한다 (Fig 5A)20)
금속판의 외측 나사는 천골공의 외측에서 천장관절에 평행
한 방향으로 향하게 하여 천골공이나 척추관을 관통하지
않고 안전하게 삽입할 수 있다 내측 나사는 제1천골에서
는 제5요추-제1천추 후방관절 (facet joint) 바로 아래에서
삽입하게 되며 zone I 골절에서는 천골의 후방 추궁판
(posterior sacral lamina)에 수직으로 그리고 상방 추궁판
(cranial sacral lamina)에 평행하게 삽입하고 zone II 골절
에서는 동일한 위치에서 외측으로 20도 기울여서 삽입하
며 제2천골에서 제4천골까지는 두 천골공 사이의 중간에
서 후방 추궁판에 수직으로 삽입한다2043) 국소 금속판 고
정은 장천 지지대 고정만큼 강하고 천장관절을 고정하지
않고 천골에만 고정하는 장점이 있다20)
3) 후방 경장골 금속판 고정 (transiliac plating)
후방 경장골 금속판 고정은 후방 연부조직 손상이 심하
지 않은 천골의 분쇄 골절에 대하여 적응이 된다 (Fig
5B)144243) 금속판의 삽입을 위해 후상 장골극에서 약 2
cm 외측에서 종절개를 양측에 가하고 대둔근을 기시부에
서 분리하여 골절 부위를 노출시킨다 천골 신경근이 손상
되지 않도록 주의하여 견인과 기구를 이용하여 정복하고
술전 영상 소견상 신경근의 압박이 있으면 감압술을 시행
한다 미리 윤곽 형성한 45-mm 또는 35-mm 금속판을
두 종절개를 통하여 후상 장골극 하방에 위치시키고 양측
장골익에 나사로 고정하며 이 금속판은 인장대 금속판으
로써의 역할을 한다 (Fig 6)1442)
4) 삼각 내고정법 (triangular osteosynthesis)
종축의 요천추 고정과 횡축의 장천골 고정의 조합인 삼
각 내고정법은 불안정한 천골 골절에 효과적인 내고정 방
법이나 내고정의 술기가 복잡하고 내고정물의 제거를 위한
이차 수술이 필요하므로 천골 골절의 분쇄가 심하여 장천
나사 고정으로 견고한 고정을 얻을 수 없는 경우에 사용하
는 것이 좋다30313334)
환자를 복와위로 하여 제4요추부터
천골의 중간까지 중앙 절개를 가하고 정중 측방 접근법
(paramedian approach)으로 제5요추의 척추경 나사 삽입
부위와 장골 나사의 삽입 부위인 후상 장골극 부위와 함께
천골 골절 부위를 포함하여 후방 피질골과 천골공을 노출
시킨다 수술 전에 이학적 및 영상 소견상 신경근의 압박
소견이 있으면 신경근의 감압술로 추궁판 부분 절제술과
함께 신경근을 압박하는 골편을 제거한다 천골 골절은 견
인과 겸자를 사용하여 정복하며 척추-골반 고정을 위하여
삽입한 장골 나사를 joystick으로 사용하여 골절을 정복하
는데 이용할 수 있다 골절은 우선 장천 나사로 고정을 하
고 척추-골반 고정을 하게 된다 척추-골반 고정을 위해 제
5요추에 척추경 나사를 삽입하는데 제5요추의 척추경에
골절이 있거나 제5요추의 전만증이 심하거나 요천추의 이
상 형태 (dysmorphism)가 있으면 제4요추의 척추경에 나사
를 삽입하여야 한다 장골 나사의 삽입 부위는 후상 장골
극 바로 전하방이며 이 고정 자체가 커서 피하조직에 자
극을 주므로 천골과 후상 장골극의 후방 피질골 사이의 틈
에 삽입하는 것이 중요하다 삽입 방향은 전방 측방 하방
으로 향하도록 하여야 하며 삽입 후 나사는 골반의 외측
및 내측 피질골 사이에 그리고 좌골 지지대 (sciatic but-
tress) 바로 위에 놓여야 한다 정확한 나사의 위치가 내측
및 외측 사면 영상에서 확인이 되면 rod와 적절한 clamp
로 장골 나사와 척추경 나사를 연결한다3031)
천골 골 377
Fig 6 This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident (A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum (B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma (C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures
5) 척추-골반 고정 (spino-pelvic fixation)
요천추 고정은 후방 중앙 접근법으로 요추의 횡돌기 천
골익과 후상 장골극 부위를 노출시키고 신경근의 압박 소
견이 있으면 직접적인 방법으로 신경근을 압박하는 골편의
제거와 추궁판 절제술을 시행하고 간접적인 방법으로 골절
의 정복에 의한 신경근의 감압술을 시행한다 골절은 견인
과 Schanz screw를 이용한 joystick 방법이나 겸자 등으로
천골의 길이 복구와 함께 골절을 정복하고 고정은 삼각
내고정법에서와 같은 방법으로 양측에 각각 제45요추에
척추경 나사와 후상 장골극 부위에 장골 나사를 삽입하여
rod와 적절한 clamp로 고정하고 양측의 rod는 서로
cross-connector나 transverse bar로 연결하여 압박한다
(Fig 5C)3248)
수술의 적응증과 골절 형태에 따른 치료
수술적 치료의 적응증은 골반의 불안정성 정도 골절의
전위 정도 그리고 부가적으로 천골 골절에 동반된 신경 손
상에 의해서 결정된다1643)
그러나 환자의 전신상태가 매우
불량하거나 골반골의 골다공증이 심한 경우에는 수술적 치
료의 적응이 되지 못한다
1 전위된 천골의 횡 골절
제2천골 아래의 횡 골절은 보통은 전위가 일어나지 않으
므로 주로 보존적 치료를 한다 그러나 드물지만 골편의
심한 전위로 인하여 직장이나 항문의 기능 장애를 일으키
거나 하위 천골 신경근의 손상이 있을 때에는 수술의 적응
이 되며 신경근의 감압술로 추궁판 절제술을 시행하고 금
속판으로 골편을 고정하여야 한다 (Fig 5D)43)
2 회전 불안정성 천골 골절
회전 불안정성 천골 골절의 대부분은 전위가 거의 일어
나지 않아 안정하므로 특별한 고정이 요하지 않으며 보존
적 치료로 좋은 결과를 얻을 수 있다 천골의 전후방 압박
골절은 매우 드물며 zone II에서 보통 발생한다 전방 손
상은 대부분 치골 결합부의 손상으로 치골 결합부가 25
378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

374 변 수 장세앙
Fig 3 Complex Denis zone III sacral fractures can be classified descriptively by the letter of the alphabet (A) U-type fracture (B) H-type fracture (C) λ-type (or Y-type) fracture (D) T-type fracture
원위 골편은 전위되지 않은 골절을 추가하였다 (Fig 2)
Roy-Camille 등29)
은 횡 골절과 함께 동반된 양측 종 골
절에서 횡 골절 부분만을 강조하였다 그러나 Denis zone
III 골절 중에서 횡 골절과는 달리 횡 골절과 함께 양측 종
골절이 동반되는 U-형의 천골 골절 즉 척추-골반 해리가
드물게 발생한다 이러한 골절은 형태학적으로 알파벳의
모양대로 U-형 H-형 λ-형 (또는 Y-형) T-형으로 분류되
며 요천추 신경총 손상의 빈도가 높다 (Fig 3)21822293748)
수술적 치료 술기
천골 골절의 수술적 치료 목적은 골편을 정복하여 적절
하게 고정하고 신경조직을 보호하고 손상된 신경은 최대
한 회복될 수 있도록 기회를 제공하는 것이다42sim44)
수술
시기는 치료의 목적 환자의 전신 상태 그리고 수술 술기
의 침습 정도에 기초하여 결정되어야 한다44) 조기에 과감
한 수술은 수술 중에 예기치 못한 출혈이나 술후 연부조직
의 합병증과 감염 등을 일으킬 수 있으며1244)
반면에 신경
의 감압술이 2주 이상 지연되면 신경의 회복에 나쁜 영향
을 줄 수 있다33544)
그러므로 치료 방법이 결정되면 장단
점을 신중하게 고려하여 판단하여야 한다
1 천골 신경근의 감압술
천골 골절에 동반되는 신경 손상은 불완전한 단일 신경
근병증 (monoradiculopathy)에서부터 완전 마미 증후군
(cauda equina syndrome)까지 다양하며 천골 신경근의 좌
상 압박 또는 견인 손상 등은 회복의 가능성이 있으나 신
경근이 절단되거나 견열 (avulsion)된 경우에는 회복의 가
능성이 없다164448)
감압술은 내고정과 함께 시행하며 천
골 신경근에 손상을 주는 골편들을 제거하고 골절의 정복
에 의한 간접적인 방법이나 추궁판 절제술 또는 추공 절단
술 (foraminotomy)에 의한 직접적인 방법으로 감압술을 시
행한다 찢어진 경막은 봉합하여 가성 척수막 공동 (pseudo-
meningocele)이 발생하지 않도록 하여야 한다44)
신경의
회복은 치료 방법과는 상관 없이 전체적으로 약 80에서
호전을 보인다고 하며 수술적 감압술이 보존적 치료보다
좋다고 하기는 어렵지만 수술적 치료 후에 보다 좋은 결과
를 보고한 저자들이 있다378) 신경 손상을 받은 환자에서
감압 수술의 시기는 다소 논란이 있다 신경생리학적 견지
에서 보면 손상을 받은 신경은 손상 후 24시간에서 72시간
내에 조기에 감압술을 시행하는 것이 좋으나 조기에 감압
술을 시행하면 출혈 창상과 관련된 합병증 뇌척수액의 누
출과 같은 합병증이 발생할 수 있으므로 이를 고려하여 수
술 시기와 치료 방법을 신중하게 결정하여야 한다2835)
2 천골 골절의 내고정
불안정한 골반환 손상에서는 후방의 천골 골절에 대한
술식을 하기 전에 골반환의 전방 손상에 대한 술식을 먼저
고려하여야 한다 골반환의 전방 손상은 정복 후 금속판
고정43) 외고정2123) 또는 역행성 치골 나사 고정1726) 등의
방법으로 고정할 수 있으며 전방 고정은 천골 골절을 정
복하는데 도움이 될 수 있으며 복와위에서 후방 술식을
하는 동안 골반환을 보호하는데 도움이 될 수 있다44)
천골 골절은 경피적 방법이나 관혈적 방법으로 정복하여
고정할 수 있으며 두 방법의 장단점을 고려하여 적절한
선택을 하여야 한다 관혈적 방법은 골편을 직접 정복하므
로 해부학적 정복이 가능하며 손상을 받은 신경근을 직접
보고 감압술을 시행할 수 있는 장점이 있다 경피적 방법
천골 골 375
Fig 4 Percutaneous fixation of the iliosacral screw (A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop) (B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet A-P and outlet views of the pelvis
은 앙와위에서 시행할 수 있고 출혈이나 연부조직 합병증
이 거의 없으며 간접 정복으로 만족스러운 정복을 얻을
수 있는 장점이 있다39)
불안정한 천골 골절을 고정하는
방법으로는 장천 나사 고정615162628434446)
경천골 금속판
또는 국소 금속판 고정20) 인장대 금속판 고정16384243) 장
천 지지대 고정 (iliosacral bar)463640)
그리고 척추경 나사
와 장골 나사를 이용한 삼각 내고정과 척추-골반 고정
(spino-pelvic fixation)23031333448) 등이 있으며 장천 지지
대 고정은 최근에는 잘 사용되지 않고 있다
1) 경피적 장천 나사 고정
경피적 장천 나사 고정은 천장관절의 손상뿐만 아니라
여러 천골 골절의 고정에 사용될 수 있다15252743)
장천 나
사는 환자를 앙와위나 복와위에서 경피적으로 삽입할 수
있으며 C-arm을 이용하여 측면상 전후면상 입구상과 출
구상을 보면서 제1천골 체부의 안전한 지역에 조심스럽게
나사를 삽입하여야 한다151643)
나사는 측면상에서는 장골
의 피질골 음영 아래에 위치하여야 하고 천골익의 중심에
삽입하여야 하며 입구상에서는 제1천골의 전방 피질골과
후방 피질골 사이의 체부에 정확하게 삽입하여야 하며
출구상에서는 천골공 바로 위에 놓이도록 하여야 한다
(Fig 4)1543)
최근에는 제한적이지만 3D C-arm을 사용하여
장천 나사를 보다 정확한 위치에 안전하게 삽입하므로 신
경혈관 손상 등의 위험을 줄일 수 있다 장천 나사는 천골
골절 중에서 비관혈적으로 정복이 되는 Denis zone I II
골절과 zone III 골절 중에 type 1 골절에서 경피적으로
삽입할 수 있으며 천골 이형성증 (dysplastic sacrum)이 있
거나 천골 골절이 비관혈적으로 정복이 되지 않을 경우에
는 경피적 장천 나사 고정의 적응이 되지 못한다164344) 분
쇄가 있는 zone II의 천골 골절을 압박 나사로 고정하게
되면 천골공의 지나친 압박으로 인하여 신경의 포착이 발
생할 수 있으므로 완전 나선형의 나사 (fully threaded screw)
로 정적 고정을 하여야 한다1844)
2) 국소 금속판 고정 (local plate osteosynthesis)
작은 금속판을 이용한 국소 금속판 고정법은 천골의 중
376 변 수 장세앙
Fig 5 Methods of surgical stabilization (A) Local plate osteosynthesis (B) Posterior transiliac plate fixation (C) Spino-pelvic fixation (D) Plate stabilization for the low transverse fracture
앙을 가로지르지 않고 천골의 편측에 직접 고정하게 되며
이 때에는 두 개의 금속판을 사용하여 하나는 제1천골에
그리고 다른 하나는 제2천골이나 제3천골에 고정하여 천골
의 회전 불안정성을 방지하도록 하여야 한다 (Fig 5A)20)
금속판의 외측 나사는 천골공의 외측에서 천장관절에 평행
한 방향으로 향하게 하여 천골공이나 척추관을 관통하지
않고 안전하게 삽입할 수 있다 내측 나사는 제1천골에서
는 제5요추-제1천추 후방관절 (facet joint) 바로 아래에서
삽입하게 되며 zone I 골절에서는 천골의 후방 추궁판
(posterior sacral lamina)에 수직으로 그리고 상방 추궁판
(cranial sacral lamina)에 평행하게 삽입하고 zone II 골절
에서는 동일한 위치에서 외측으로 20도 기울여서 삽입하
며 제2천골에서 제4천골까지는 두 천골공 사이의 중간에
서 후방 추궁판에 수직으로 삽입한다2043) 국소 금속판 고
정은 장천 지지대 고정만큼 강하고 천장관절을 고정하지
않고 천골에만 고정하는 장점이 있다20)
3) 후방 경장골 금속판 고정 (transiliac plating)
후방 경장골 금속판 고정은 후방 연부조직 손상이 심하
지 않은 천골의 분쇄 골절에 대하여 적응이 된다 (Fig
5B)144243) 금속판의 삽입을 위해 후상 장골극에서 약 2
cm 외측에서 종절개를 양측에 가하고 대둔근을 기시부에
서 분리하여 골절 부위를 노출시킨다 천골 신경근이 손상
되지 않도록 주의하여 견인과 기구를 이용하여 정복하고
술전 영상 소견상 신경근의 압박이 있으면 감압술을 시행
한다 미리 윤곽 형성한 45-mm 또는 35-mm 금속판을
두 종절개를 통하여 후상 장골극 하방에 위치시키고 양측
장골익에 나사로 고정하며 이 금속판은 인장대 금속판으
로써의 역할을 한다 (Fig 6)1442)
4) 삼각 내고정법 (triangular osteosynthesis)
종축의 요천추 고정과 횡축의 장천골 고정의 조합인 삼
각 내고정법은 불안정한 천골 골절에 효과적인 내고정 방
법이나 내고정의 술기가 복잡하고 내고정물의 제거를 위한
이차 수술이 필요하므로 천골 골절의 분쇄가 심하여 장천
나사 고정으로 견고한 고정을 얻을 수 없는 경우에 사용하
는 것이 좋다30313334)
환자를 복와위로 하여 제4요추부터
천골의 중간까지 중앙 절개를 가하고 정중 측방 접근법
(paramedian approach)으로 제5요추의 척추경 나사 삽입
부위와 장골 나사의 삽입 부위인 후상 장골극 부위와 함께
천골 골절 부위를 포함하여 후방 피질골과 천골공을 노출
시킨다 수술 전에 이학적 및 영상 소견상 신경근의 압박
소견이 있으면 신경근의 감압술로 추궁판 부분 절제술과
함께 신경근을 압박하는 골편을 제거한다 천골 골절은 견
인과 겸자를 사용하여 정복하며 척추-골반 고정을 위하여
삽입한 장골 나사를 joystick으로 사용하여 골절을 정복하
는데 이용할 수 있다 골절은 우선 장천 나사로 고정을 하
고 척추-골반 고정을 하게 된다 척추-골반 고정을 위해 제
5요추에 척추경 나사를 삽입하는데 제5요추의 척추경에
골절이 있거나 제5요추의 전만증이 심하거나 요천추의 이
상 형태 (dysmorphism)가 있으면 제4요추의 척추경에 나사
를 삽입하여야 한다 장골 나사의 삽입 부위는 후상 장골
극 바로 전하방이며 이 고정 자체가 커서 피하조직에 자
극을 주므로 천골과 후상 장골극의 후방 피질골 사이의 틈
에 삽입하는 것이 중요하다 삽입 방향은 전방 측방 하방
으로 향하도록 하여야 하며 삽입 후 나사는 골반의 외측
및 내측 피질골 사이에 그리고 좌골 지지대 (sciatic but-
tress) 바로 위에 놓여야 한다 정확한 나사의 위치가 내측
및 외측 사면 영상에서 확인이 되면 rod와 적절한 clamp
로 장골 나사와 척추경 나사를 연결한다3031)
천골 골 377
Fig 6 This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident (A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum (B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma (C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures
5) 척추-골반 고정 (spino-pelvic fixation)
요천추 고정은 후방 중앙 접근법으로 요추의 횡돌기 천
골익과 후상 장골극 부위를 노출시키고 신경근의 압박 소
견이 있으면 직접적인 방법으로 신경근을 압박하는 골편의
제거와 추궁판 절제술을 시행하고 간접적인 방법으로 골절
의 정복에 의한 신경근의 감압술을 시행한다 골절은 견인
과 Schanz screw를 이용한 joystick 방법이나 겸자 등으로
천골의 길이 복구와 함께 골절을 정복하고 고정은 삼각
내고정법에서와 같은 방법으로 양측에 각각 제45요추에
척추경 나사와 후상 장골극 부위에 장골 나사를 삽입하여
rod와 적절한 clamp로 고정하고 양측의 rod는 서로
cross-connector나 transverse bar로 연결하여 압박한다
(Fig 5C)3248)
수술의 적응증과 골절 형태에 따른 치료
수술적 치료의 적응증은 골반의 불안정성 정도 골절의
전위 정도 그리고 부가적으로 천골 골절에 동반된 신경 손
상에 의해서 결정된다1643)
그러나 환자의 전신상태가 매우
불량하거나 골반골의 골다공증이 심한 경우에는 수술적 치
료의 적응이 되지 못한다
1 전위된 천골의 횡 골절
제2천골 아래의 횡 골절은 보통은 전위가 일어나지 않으
므로 주로 보존적 치료를 한다 그러나 드물지만 골편의
심한 전위로 인하여 직장이나 항문의 기능 장애를 일으키
거나 하위 천골 신경근의 손상이 있을 때에는 수술의 적응
이 되며 신경근의 감압술로 추궁판 절제술을 시행하고 금
속판으로 골편을 고정하여야 한다 (Fig 5D)43)
2 회전 불안정성 천골 골절
회전 불안정성 천골 골절의 대부분은 전위가 거의 일어
나지 않아 안정하므로 특별한 고정이 요하지 않으며 보존
적 치료로 좋은 결과를 얻을 수 있다 천골의 전후방 압박
골절은 매우 드물며 zone II에서 보통 발생한다 전방 손
상은 대부분 치골 결합부의 손상으로 치골 결합부가 25
378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

천골 골 375
Fig 4 Percutaneous fixation of the iliosacral screw (A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop) (B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet A-P and outlet views of the pelvis
은 앙와위에서 시행할 수 있고 출혈이나 연부조직 합병증
이 거의 없으며 간접 정복으로 만족스러운 정복을 얻을
수 있는 장점이 있다39)
불안정한 천골 골절을 고정하는
방법으로는 장천 나사 고정615162628434446)
경천골 금속판
또는 국소 금속판 고정20) 인장대 금속판 고정16384243) 장
천 지지대 고정 (iliosacral bar)463640)
그리고 척추경 나사
와 장골 나사를 이용한 삼각 내고정과 척추-골반 고정
(spino-pelvic fixation)23031333448) 등이 있으며 장천 지지
대 고정은 최근에는 잘 사용되지 않고 있다
1) 경피적 장천 나사 고정
경피적 장천 나사 고정은 천장관절의 손상뿐만 아니라
여러 천골 골절의 고정에 사용될 수 있다15252743)
장천 나
사는 환자를 앙와위나 복와위에서 경피적으로 삽입할 수
있으며 C-arm을 이용하여 측면상 전후면상 입구상과 출
구상을 보면서 제1천골 체부의 안전한 지역에 조심스럽게
나사를 삽입하여야 한다151643)
나사는 측면상에서는 장골
의 피질골 음영 아래에 위치하여야 하고 천골익의 중심에
삽입하여야 하며 입구상에서는 제1천골의 전방 피질골과
후방 피질골 사이의 체부에 정확하게 삽입하여야 하며
출구상에서는 천골공 바로 위에 놓이도록 하여야 한다
(Fig 4)1543)
최근에는 제한적이지만 3D C-arm을 사용하여
장천 나사를 보다 정확한 위치에 안전하게 삽입하므로 신
경혈관 손상 등의 위험을 줄일 수 있다 장천 나사는 천골
골절 중에서 비관혈적으로 정복이 되는 Denis zone I II
골절과 zone III 골절 중에 type 1 골절에서 경피적으로
삽입할 수 있으며 천골 이형성증 (dysplastic sacrum)이 있
거나 천골 골절이 비관혈적으로 정복이 되지 않을 경우에
는 경피적 장천 나사 고정의 적응이 되지 못한다164344) 분
쇄가 있는 zone II의 천골 골절을 압박 나사로 고정하게
되면 천골공의 지나친 압박으로 인하여 신경의 포착이 발
생할 수 있으므로 완전 나선형의 나사 (fully threaded screw)
로 정적 고정을 하여야 한다1844)
2) 국소 금속판 고정 (local plate osteosynthesis)
작은 금속판을 이용한 국소 금속판 고정법은 천골의 중
376 변 수 장세앙
Fig 5 Methods of surgical stabilization (A) Local plate osteosynthesis (B) Posterior transiliac plate fixation (C) Spino-pelvic fixation (D) Plate stabilization for the low transverse fracture
앙을 가로지르지 않고 천골의 편측에 직접 고정하게 되며
이 때에는 두 개의 금속판을 사용하여 하나는 제1천골에
그리고 다른 하나는 제2천골이나 제3천골에 고정하여 천골
의 회전 불안정성을 방지하도록 하여야 한다 (Fig 5A)20)
금속판의 외측 나사는 천골공의 외측에서 천장관절에 평행
한 방향으로 향하게 하여 천골공이나 척추관을 관통하지
않고 안전하게 삽입할 수 있다 내측 나사는 제1천골에서
는 제5요추-제1천추 후방관절 (facet joint) 바로 아래에서
삽입하게 되며 zone I 골절에서는 천골의 후방 추궁판
(posterior sacral lamina)에 수직으로 그리고 상방 추궁판
(cranial sacral lamina)에 평행하게 삽입하고 zone II 골절
에서는 동일한 위치에서 외측으로 20도 기울여서 삽입하
며 제2천골에서 제4천골까지는 두 천골공 사이의 중간에
서 후방 추궁판에 수직으로 삽입한다2043) 국소 금속판 고
정은 장천 지지대 고정만큼 강하고 천장관절을 고정하지
않고 천골에만 고정하는 장점이 있다20)
3) 후방 경장골 금속판 고정 (transiliac plating)
후방 경장골 금속판 고정은 후방 연부조직 손상이 심하
지 않은 천골의 분쇄 골절에 대하여 적응이 된다 (Fig
5B)144243) 금속판의 삽입을 위해 후상 장골극에서 약 2
cm 외측에서 종절개를 양측에 가하고 대둔근을 기시부에
서 분리하여 골절 부위를 노출시킨다 천골 신경근이 손상
되지 않도록 주의하여 견인과 기구를 이용하여 정복하고
술전 영상 소견상 신경근의 압박이 있으면 감압술을 시행
한다 미리 윤곽 형성한 45-mm 또는 35-mm 금속판을
두 종절개를 통하여 후상 장골극 하방에 위치시키고 양측
장골익에 나사로 고정하며 이 금속판은 인장대 금속판으
로써의 역할을 한다 (Fig 6)1442)
4) 삼각 내고정법 (triangular osteosynthesis)
종축의 요천추 고정과 횡축의 장천골 고정의 조합인 삼
각 내고정법은 불안정한 천골 골절에 효과적인 내고정 방
법이나 내고정의 술기가 복잡하고 내고정물의 제거를 위한
이차 수술이 필요하므로 천골 골절의 분쇄가 심하여 장천
나사 고정으로 견고한 고정을 얻을 수 없는 경우에 사용하
는 것이 좋다30313334)
환자를 복와위로 하여 제4요추부터
천골의 중간까지 중앙 절개를 가하고 정중 측방 접근법
(paramedian approach)으로 제5요추의 척추경 나사 삽입
부위와 장골 나사의 삽입 부위인 후상 장골극 부위와 함께
천골 골절 부위를 포함하여 후방 피질골과 천골공을 노출
시킨다 수술 전에 이학적 및 영상 소견상 신경근의 압박
소견이 있으면 신경근의 감압술로 추궁판 부분 절제술과
함께 신경근을 압박하는 골편을 제거한다 천골 골절은 견
인과 겸자를 사용하여 정복하며 척추-골반 고정을 위하여
삽입한 장골 나사를 joystick으로 사용하여 골절을 정복하
는데 이용할 수 있다 골절은 우선 장천 나사로 고정을 하
고 척추-골반 고정을 하게 된다 척추-골반 고정을 위해 제
5요추에 척추경 나사를 삽입하는데 제5요추의 척추경에
골절이 있거나 제5요추의 전만증이 심하거나 요천추의 이
상 형태 (dysmorphism)가 있으면 제4요추의 척추경에 나사
를 삽입하여야 한다 장골 나사의 삽입 부위는 후상 장골
극 바로 전하방이며 이 고정 자체가 커서 피하조직에 자
극을 주므로 천골과 후상 장골극의 후방 피질골 사이의 틈
에 삽입하는 것이 중요하다 삽입 방향은 전방 측방 하방
으로 향하도록 하여야 하며 삽입 후 나사는 골반의 외측
및 내측 피질골 사이에 그리고 좌골 지지대 (sciatic but-
tress) 바로 위에 놓여야 한다 정확한 나사의 위치가 내측
및 외측 사면 영상에서 확인이 되면 rod와 적절한 clamp
로 장골 나사와 척추경 나사를 연결한다3031)
천골 골 377
Fig 6 This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident (A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum (B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma (C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures
5) 척추-골반 고정 (spino-pelvic fixation)
요천추 고정은 후방 중앙 접근법으로 요추의 횡돌기 천
골익과 후상 장골극 부위를 노출시키고 신경근의 압박 소
견이 있으면 직접적인 방법으로 신경근을 압박하는 골편의
제거와 추궁판 절제술을 시행하고 간접적인 방법으로 골절
의 정복에 의한 신경근의 감압술을 시행한다 골절은 견인
과 Schanz screw를 이용한 joystick 방법이나 겸자 등으로
천골의 길이 복구와 함께 골절을 정복하고 고정은 삼각
내고정법에서와 같은 방법으로 양측에 각각 제45요추에
척추경 나사와 후상 장골극 부위에 장골 나사를 삽입하여
rod와 적절한 clamp로 고정하고 양측의 rod는 서로
cross-connector나 transverse bar로 연결하여 압박한다
(Fig 5C)3248)
수술의 적응증과 골절 형태에 따른 치료
수술적 치료의 적응증은 골반의 불안정성 정도 골절의
전위 정도 그리고 부가적으로 천골 골절에 동반된 신경 손
상에 의해서 결정된다1643)
그러나 환자의 전신상태가 매우
불량하거나 골반골의 골다공증이 심한 경우에는 수술적 치
료의 적응이 되지 못한다
1 전위된 천골의 횡 골절
제2천골 아래의 횡 골절은 보통은 전위가 일어나지 않으
므로 주로 보존적 치료를 한다 그러나 드물지만 골편의
심한 전위로 인하여 직장이나 항문의 기능 장애를 일으키
거나 하위 천골 신경근의 손상이 있을 때에는 수술의 적응
이 되며 신경근의 감압술로 추궁판 절제술을 시행하고 금
속판으로 골편을 고정하여야 한다 (Fig 5D)43)
2 회전 불안정성 천골 골절
회전 불안정성 천골 골절의 대부분은 전위가 거의 일어
나지 않아 안정하므로 특별한 고정이 요하지 않으며 보존
적 치료로 좋은 결과를 얻을 수 있다 천골의 전후방 압박
골절은 매우 드물며 zone II에서 보통 발생한다 전방 손
상은 대부분 치골 결합부의 손상으로 치골 결합부가 25
378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

376 변 수 장세앙
Fig 5 Methods of surgical stabilization (A) Local plate osteosynthesis (B) Posterior transiliac plate fixation (C) Spino-pelvic fixation (D) Plate stabilization for the low transverse fracture
앙을 가로지르지 않고 천골의 편측에 직접 고정하게 되며
이 때에는 두 개의 금속판을 사용하여 하나는 제1천골에
그리고 다른 하나는 제2천골이나 제3천골에 고정하여 천골
의 회전 불안정성을 방지하도록 하여야 한다 (Fig 5A)20)
금속판의 외측 나사는 천골공의 외측에서 천장관절에 평행
한 방향으로 향하게 하여 천골공이나 척추관을 관통하지
않고 안전하게 삽입할 수 있다 내측 나사는 제1천골에서
는 제5요추-제1천추 후방관절 (facet joint) 바로 아래에서
삽입하게 되며 zone I 골절에서는 천골의 후방 추궁판
(posterior sacral lamina)에 수직으로 그리고 상방 추궁판
(cranial sacral lamina)에 평행하게 삽입하고 zone II 골절
에서는 동일한 위치에서 외측으로 20도 기울여서 삽입하
며 제2천골에서 제4천골까지는 두 천골공 사이의 중간에
서 후방 추궁판에 수직으로 삽입한다2043) 국소 금속판 고
정은 장천 지지대 고정만큼 강하고 천장관절을 고정하지
않고 천골에만 고정하는 장점이 있다20)
3) 후방 경장골 금속판 고정 (transiliac plating)
후방 경장골 금속판 고정은 후방 연부조직 손상이 심하
지 않은 천골의 분쇄 골절에 대하여 적응이 된다 (Fig
5B)144243) 금속판의 삽입을 위해 후상 장골극에서 약 2
cm 외측에서 종절개를 양측에 가하고 대둔근을 기시부에
서 분리하여 골절 부위를 노출시킨다 천골 신경근이 손상
되지 않도록 주의하여 견인과 기구를 이용하여 정복하고
술전 영상 소견상 신경근의 압박이 있으면 감압술을 시행
한다 미리 윤곽 형성한 45-mm 또는 35-mm 금속판을
두 종절개를 통하여 후상 장골극 하방에 위치시키고 양측
장골익에 나사로 고정하며 이 금속판은 인장대 금속판으
로써의 역할을 한다 (Fig 6)1442)
4) 삼각 내고정법 (triangular osteosynthesis)
종축의 요천추 고정과 횡축의 장천골 고정의 조합인 삼
각 내고정법은 불안정한 천골 골절에 효과적인 내고정 방
법이나 내고정의 술기가 복잡하고 내고정물의 제거를 위한
이차 수술이 필요하므로 천골 골절의 분쇄가 심하여 장천
나사 고정으로 견고한 고정을 얻을 수 없는 경우에 사용하
는 것이 좋다30313334)
환자를 복와위로 하여 제4요추부터
천골의 중간까지 중앙 절개를 가하고 정중 측방 접근법
(paramedian approach)으로 제5요추의 척추경 나사 삽입
부위와 장골 나사의 삽입 부위인 후상 장골극 부위와 함께
천골 골절 부위를 포함하여 후방 피질골과 천골공을 노출
시킨다 수술 전에 이학적 및 영상 소견상 신경근의 압박
소견이 있으면 신경근의 감압술로 추궁판 부분 절제술과
함께 신경근을 압박하는 골편을 제거한다 천골 골절은 견
인과 겸자를 사용하여 정복하며 척추-골반 고정을 위하여
삽입한 장골 나사를 joystick으로 사용하여 골절을 정복하
는데 이용할 수 있다 골절은 우선 장천 나사로 고정을 하
고 척추-골반 고정을 하게 된다 척추-골반 고정을 위해 제
5요추에 척추경 나사를 삽입하는데 제5요추의 척추경에
골절이 있거나 제5요추의 전만증이 심하거나 요천추의 이
상 형태 (dysmorphism)가 있으면 제4요추의 척추경에 나사
를 삽입하여야 한다 장골 나사의 삽입 부위는 후상 장골
극 바로 전하방이며 이 고정 자체가 커서 피하조직에 자
극을 주므로 천골과 후상 장골극의 후방 피질골 사이의 틈
에 삽입하는 것이 중요하다 삽입 방향은 전방 측방 하방
으로 향하도록 하여야 하며 삽입 후 나사는 골반의 외측
및 내측 피질골 사이에 그리고 좌골 지지대 (sciatic but-
tress) 바로 위에 놓여야 한다 정확한 나사의 위치가 내측
및 외측 사면 영상에서 확인이 되면 rod와 적절한 clamp
로 장골 나사와 척추경 나사를 연결한다3031)
천골 골 377
Fig 6 This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident (A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum (B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma (C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures
5) 척추-골반 고정 (spino-pelvic fixation)
요천추 고정은 후방 중앙 접근법으로 요추의 횡돌기 천
골익과 후상 장골극 부위를 노출시키고 신경근의 압박 소
견이 있으면 직접적인 방법으로 신경근을 압박하는 골편의
제거와 추궁판 절제술을 시행하고 간접적인 방법으로 골절
의 정복에 의한 신경근의 감압술을 시행한다 골절은 견인
과 Schanz screw를 이용한 joystick 방법이나 겸자 등으로
천골의 길이 복구와 함께 골절을 정복하고 고정은 삼각
내고정법에서와 같은 방법으로 양측에 각각 제45요추에
척추경 나사와 후상 장골극 부위에 장골 나사를 삽입하여
rod와 적절한 clamp로 고정하고 양측의 rod는 서로
cross-connector나 transverse bar로 연결하여 압박한다
(Fig 5C)3248)
수술의 적응증과 골절 형태에 따른 치료
수술적 치료의 적응증은 골반의 불안정성 정도 골절의
전위 정도 그리고 부가적으로 천골 골절에 동반된 신경 손
상에 의해서 결정된다1643)
그러나 환자의 전신상태가 매우
불량하거나 골반골의 골다공증이 심한 경우에는 수술적 치
료의 적응이 되지 못한다
1 전위된 천골의 횡 골절
제2천골 아래의 횡 골절은 보통은 전위가 일어나지 않으
므로 주로 보존적 치료를 한다 그러나 드물지만 골편의
심한 전위로 인하여 직장이나 항문의 기능 장애를 일으키
거나 하위 천골 신경근의 손상이 있을 때에는 수술의 적응
이 되며 신경근의 감압술로 추궁판 절제술을 시행하고 금
속판으로 골편을 고정하여야 한다 (Fig 5D)43)
2 회전 불안정성 천골 골절
회전 불안정성 천골 골절의 대부분은 전위가 거의 일어
나지 않아 안정하므로 특별한 고정이 요하지 않으며 보존
적 치료로 좋은 결과를 얻을 수 있다 천골의 전후방 압박
골절은 매우 드물며 zone II에서 보통 발생한다 전방 손
상은 대부분 치골 결합부의 손상으로 치골 결합부가 25
378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

천골 골 377
Fig 6 This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident (A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum (B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma (C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures
5) 척추-골반 고정 (spino-pelvic fixation)
요천추 고정은 후방 중앙 접근법으로 요추의 횡돌기 천
골익과 후상 장골극 부위를 노출시키고 신경근의 압박 소
견이 있으면 직접적인 방법으로 신경근을 압박하는 골편의
제거와 추궁판 절제술을 시행하고 간접적인 방법으로 골절
의 정복에 의한 신경근의 감압술을 시행한다 골절은 견인
과 Schanz screw를 이용한 joystick 방법이나 겸자 등으로
천골의 길이 복구와 함께 골절을 정복하고 고정은 삼각
내고정법에서와 같은 방법으로 양측에 각각 제45요추에
척추경 나사와 후상 장골극 부위에 장골 나사를 삽입하여
rod와 적절한 clamp로 고정하고 양측의 rod는 서로
cross-connector나 transverse bar로 연결하여 압박한다
(Fig 5C)3248)
수술의 적응증과 골절 형태에 따른 치료
수술적 치료의 적응증은 골반의 불안정성 정도 골절의
전위 정도 그리고 부가적으로 천골 골절에 동반된 신경 손
상에 의해서 결정된다1643)
그러나 환자의 전신상태가 매우
불량하거나 골반골의 골다공증이 심한 경우에는 수술적 치
료의 적응이 되지 못한다
1 전위된 천골의 횡 골절
제2천골 아래의 횡 골절은 보통은 전위가 일어나지 않으
므로 주로 보존적 치료를 한다 그러나 드물지만 골편의
심한 전위로 인하여 직장이나 항문의 기능 장애를 일으키
거나 하위 천골 신경근의 손상이 있을 때에는 수술의 적응
이 되며 신경근의 감압술로 추궁판 절제술을 시행하고 금
속판으로 골편을 고정하여야 한다 (Fig 5D)43)
2 회전 불안정성 천골 골절
회전 불안정성 천골 골절의 대부분은 전위가 거의 일어
나지 않아 안정하므로 특별한 고정이 요하지 않으며 보존
적 치료로 좋은 결과를 얻을 수 있다 천골의 전후방 압박
골절은 매우 드물며 zone II에서 보통 발생한다 전방 손
상은 대부분 치골 결합부의 손상으로 치골 결합부가 25
378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

378 변 수 장세앙
Fig 7 This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb (A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type) (B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a recons-truction plate anteriorly and an iliosacral screw posteriorly Note The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw
cm 이상 넓어진 경우에는 골반저의 파열이 동반되어 있어
전방 고정이 요하며 천골 골절은 완전 골절인 경우에 후
방 고정이 필요하고 보통 경피적 장천 나사로 고정한다43)
천골의 외측 압박 골절은 zone I 또는 zone II에 종 골절
의 형태로 발생한다 전방 손상은 보통 치골지의 종 골절
로 골절의 부정 정렬이 있으면 골절을 정복하고 고정하여
야 하며 천골 골절은 신경 손상이 동반되어 있고 골편이
신경을 압박할 때에만 수술적 치료가 필요하다 신경을 압
박하는 골편에 대해서는 감압술이 요하며 천골 골절은 보
통 경피적 장천 나사로 고정한다 (Fig 7)1943)
3 완전 불안정성 편측 천골 골절
완전 불안정성 편측 천골 골절은 대부분 종 골절로써
zone II에서 가장 흔히 발생하며 경미하게 전위된 골절도
보존적 치료로는 이차적으로 전위될 위험이 크므로 내고정
을 하여야 한다 전방 손상은 치골 결합부나 편측 또는 양
측 치골지 골절 등 다양하게 나타나며 후방의 천골 골절
을 고정하기 전에 전방 고정을 고려하여야 한다 천골 골
절의 전위가 경미하고 신경 손상이 없으면 경피적 장천 나
사 고정으로 충분하다 천골 골절이 상당히 전위되어 있으
나 신경 손상이 없으면 비관혈적 또는 관혈적 정복 후 경
피적 장천 나사 고정으로 치료될 수 있다 이 경우에 전방
손상의 해부학적 정복과 고정으로 자주 만족스러운 후방
정복을 얻을 수 있다 천골 골절이 상당히 전위되어 있고
신경 손상이 동반되어 있는 경우에는 천골 골절의 관혈적
정복 천골 신경근의 감압술 및 견고한 고정이 요구된다
관혈적 정복이 선택되면 창상의 합병증을 피하기 위해 연
부조직의 상태를 고려여야 하며 Morel-Lavalle lesion과 같
은 심한 연부조직 손상이 있으면 수술 접근법을 바꾸어야
한다 이러한 천골 골절은 장천 나사 고정 후방 국소 금
속판 고정 인장대 금속판 고정 또는 삼각 내고정법으로
고정할 수 있다2027344243)
4 척추-골반 해리 (spino-pelvic dissociation)
신경 손상이 없고 경미하게 전위된 안전성 천골 골절인
경우에만 보존적 치료가 가능하다30)
그러나 장기간의 안
정은 특히 다발성 손상 환자에서 좋지 않으며 다발성 손
상 환자에서 수술적 치료로 골반환을 고정하면 조기 운동
이 가능하고 조기 사망률을 감소시키며 장기 결과가 향상
된다고 한다910183245) 천골 신경근이 골편의 전위나 각형
성으로 좌상 압박 또는 견인 등의 손상을 받은 경우에는
신경의 회복 가능성이 있으므로 골절의 정복에 의한 간접
적인 방법과 추궁판 절제술이나 추공 절단술에 의한 직접
적인 방법으로 감압술을 시행하여야 하며 신경근에 손상
을 줄 수 있는 골편은 제거하여야 한다16324344)
골절은 견
인과 Schanz screw를 이용한 joystick 방법이나 겸자 등으
로 정복하며 내고정하기 전에 C-arm으로 정복의 상태를
확인하여야 한다3245)
분쇄가 없고 전위가 거의 되지 않은
U-형의 천골 골절은 경피적 장천 나사로 고정할 수 있으
나 고도로 불안정한 척추-골반 해리는 척추-골반 고정
(spino-pelvic fixation)이나 삼각 내고정 방법으로 고정하는
것이 좋다 (Fig 8)4448)
천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

천골 골 379
Fig 8 This 23-year-old male patient sustained polytrauma including a suicidal jumperrsquos fracture by a fall from the 5th story (A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture (B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures (C) Definitive treatment was performed 11 days after trauma Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation
요 약
천골 골절에 대한 진단과 치료 방법들은 상당히 발전되
어 왔으나 부적절한 진단과 치료로 장기적으로 좋지 못한
결과를 초래하는 경우가 자주 있다 그러므로 일관된 진단
적 접근으로 조기에 정확한 진단을 하고 적절한 치료를 하
여 동통을 동반한 변형과 신경 손상의 악화를 방지하도록
하여야 한다 수술적 치료가 결정되면 수술 시기는 치료의
목적 환자의 전신 상태 그리고 수술 술기의 침습 정도에
기초하여 결정하여야 하며 수술 방법은 조기 감압술 내고
정 조기 운동 등의 장점과 함께 출혈 감염 창상 합병증
또는 마취와 관련된 합병증과 같은 위험 요소들을 고려하
여 개별적으로 결정하여야 한다
참 고 문 헌
1) Albert MJ Miller ME MacNaughton M Hutton WC
Posterior pelvic fixation using a transiliac 45-mm re-
construction plate a clinical and biomechanical study J
Orthop Trauma 7 226-232 1993
2) Bents RT France JC Glover JM Kaylor KL
Traumatic spondylopelvic dissociation A case report and
literature review Spine (Phila Pa 1976) 21 1814-1819
1996
3) Denis F Davis S Comfort T Sacral fractures an im-
portant problem Retrospective analysis of 236 cases Clin
Orthop Relat Res 227 67-81 1988
4) Ebraheim NA Coombs R Hoeflinger MJ Zeman C
Jackson WT Anatomical and radiological considerations
in compressive bar technique for posterior pelvic disrup-
tions J Orthop Trauma 5 434-438 1991
5) Edeiken-Monroe BS Browner BD Jackson H The role
of standard roentgenograms in the evaluation of instability
of pelvic ring disruption Clin Orthop Relat Res (240)
63-76 1989
6) Failinger MS McGanity PL Unstable fractures of the
pelvic ring J Bone Joint Surg Am 74 781-791 1992
7) Fountain SS Hamilton RD Jameson RM Transverse
fractures of the sacrum A report of six cases J Bone
Joint Surg Am 59 486-489 1977
8) Gibbons KJ Soloniuk DS Razack N Neurological in-
jury and patterns of sacral fractures J Neurosurg 72
889-893 1990
9) Gribnau AJ van Hensbroek PB Haverlag R Ponsen
KJ Been HD Goslings JC U-shaped sacral fractures
surgical treatment and quality of life Injury 40
1040-1048 2009
10) Hunt N Jennings A Smith M Current management of
U-shaped sacral fractures or spino-pelvic dissociation
Injury 33 123-126 2002
11) Jackson H Kam J Harris JH Jr Harle TS The sacral
arcuate lines in upper sacral fractures Radiology 145
35-39 1982
380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

380 변 수 장세앙
12) Kellam JF McMurtry RY Paley D Tile M The un-
stable pelvic fracture Operative treatment Orthop Clin
North Am 18 25-41 1987
13) Kim MY Reidy DP Nolan PC Finkelstein JA
Transverse sacral fractures case series and literature
review Can J Surg 44 359-363 2001
14) Krappinger D Larndorfer R Struve P Rosenberger
R Arora R Blauth M Minimally invasive transiliac
plate osteosynthesis for type C injuries of the pelvic ring
a clinical and radiological follow-up J Orthop Trauma
21 595-602 2007
15) Matta JM Saucedo T Internal fixation of pelvic ring
fractures Clin Orthop Relat Res (242) 83-97 1989
16) Mehta S Auerbach JD Born CT Chin KR Sacral
fractures J Am Acad Orthop Surg 14 656-665 2006
17) Mosheiff R Liebergall M Maneuvering the retrograde
medullary screw in pubic ramus fractures J Orthop
Trauma 16 594-596 2002
18) Nork SE Jones CB Harding SP Mirza SK Routt ML
Jr Percutaneous stabilization of U-shaped sacral fractures
using iliosacral screws technique and early results J
Orthop Trauma 15 238-246 2001
19) Osterhoff G Ossendorf C Wanner GA Simmen HP
Werner CM Posterior screw fixation in rotationally un-
stable pelvic ring injuries Injury 42 992-996 2011
20) Pohlemann T Angst M Schneider E Ganz R
Tscherne H Fixation of transforaminal sacrum fractures
a biomechanical study J Orthop Trauma 7 107-117
1993
21) Riemer BL Butterfield SL Diamond DL et al Acute
mortality associated with injuries to the pelvic ring the
role of early patient mobilization and external fixation J
Trauma 35 671-675 1993
22) Robles LA Transverse sacral fractures Spine J 9 60-69
2009
23) Rommens PM Hessmann MH Staged reconstruction of
pelvic ring disruption differences in morbidity mortality
radiologic results and functional outcomes between B1
B2B3 and C-type lesions J Orthop Trauma 16 92-98
2002
24) Rommens PM Vanderschot PM Broos PL
Conventional radiography and CT examination of pelvic
ring fractures A comparative study of 90 patients
Unfallchirurg 95 387-392 1992
25) Routt MLC Jr Meier MC Kregor PJ et al
Percutaneous iliosacral screws with the patient supine Op
Tech Orthop 7 35-45 1993
26) Routt MLC Jr Simonian PT Grujic L The retrograde
medullary superior pubic ramus screw for the treatment of
anterior pelvic ring disruptions a new technique J Orthop
Trauma 9 35-44 1995
27) Routt MLC Jr Simonian PT Mills WJ Iliosacral
screw fixation early complications of the percutaneous
technique J Orthop Trauma 11 584-589 1997
28) Routt MLC Jr Simonian PT Swiontkowski MF
Stabilization of pelvic ring disruptions Orthop Clin North
Am 28 369-388 1997
29) Roy-Camille R Saillant G Gagna G Mazel C
Transverse fracture of the upper sacrum Suicidal jumpers
fracture Spine (Phila Pa 1976) 10 838-845 1985
30) Sagi HC Technical aspects and recommended treatment
algorithms in triangular osteosynthesis and spinopelvic fix-
ation for vertical shear transforaminal sacral fractures J
Orthop Trauma 23 354-360 2009
31) Sagi HC Militano U Caron T Lindvall E A compre-
hensive analysis with minimum 1-year follow-up of verti-
cally unstable transforaminal sacral fractures treated with
triangular osteosynthesis J Orthop Trauma 23 313-319
2009
32) Schildhauer TA Bellabarba C Nork SE Barei DP
Routt ML Jr Chapman JR Decompression and lumbo-
pelvic fixation for sacral fracture-dislocations with spi-
no-pelvic dissociation J Orthop Trauma 20 447-457
2006
33) Schildhauer TA Josten C Muhr G Triangular osteo-
synthesis of vertically unstable sacrum fractures a new
concept allowing early weight-bearing J Orthop Trauma
12 307-314 1998
34) Schildhauer TA Ledoux WR Chapman JR Henley
MB Tencer AF Routt ML Jr Triangular osteosynthesis
and iliosacral screw fixation for unstable sacral fractures
a cadaveric and biomechanical evaluation under cyclic
loads J Orthop Trauma 17 22-31 2003
35) Schmidek HH Smith DA Kristiansen TK Sacral
fractures Neurosurgery 15 735-746 1984
36) Shaw JA Mino DE Werner FW Murray DG
Posterior stabilization of pelvic fractures by use of thread-
ed compression rods Case reports and mechanical testing
Clin Orthop Relat Res (192) 240-254 1985
37) Siebler JC Hasley BP Mormino MA Functional out-
천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011

천골 골 381
comes of Denis zone III sacral fractures treated
nonoperatively J Orthop Trauma 24 297-302 2010
38) Simonian PT Routt ML Jr Biomechanics of pelvic
fixation Orthop Clin North Am 28 351-367 1997
39) Starr AJ Malekzadeh Fractures of the pelvic ring In
Bucholz RW Heckman JD Court-Brown C eds Rockwood
and Greenrsquos Fractures in adults 6th ed Philadelphia
Lippincott Williams amp Wilkins 1585-1664 2006
40) Stocks GW Gabel GT Noble PC Hanson GW Tullos
HS Anterior and posterior internal fixation of vertical
shear fractures of the pelvis J Orthop Res 9 237-245
1991
41) Strange-Vognsen HH Lebech A An unusual type of
fracture in the upper sacrum J Orthop Trauma 5
200-203 1991
42) Suzuki T Hak DJ Ziran BH et al Outcome and com-
plications of posterior transiliac plating for vertically un-
stable sacral fractures Injury 40 405-409 2009
43) Tile M Helfet DL Kellam JF Fractures of the pelvis
and acetabulum 3rd ed Philadelphia USA Lippincott
Williams and Wilkins 203-322 2003
44) Vaccaro AR Kim DH Brodke DS et al Diagnosis and
management of sacral spine fractures Instr Course Lect
53 375-385 2004
45) Vresilovic EJ Mehta S Placide R Milam RA 4th
Traumatic spondylopelvic dissociation A report of two
cases J Bone Joint Surg Am 87 1098-1103 2005
46) Ward EF Tomasin J Vander Griend RA Open reduc-
tion and internal fixation of vertical shear pelvic fractures
J Trauma 27 291-295 1987
47) White JH Hague C Nicolaou S Gee R Marchinkow
LO Munk PL Imaging of sacral fractures Clin Radiol
58 914-921 2003
48) Yi C Hak DJ Traumatic spinopelvic dissociation or
U-shaped sacral fracture a review of the literature Injury
In press 2011