Oedematous Child
57
1 Group F1 Group F1 THE OEDEMATOUS CHILD THE OEDEMATOUS CHILD
-
Upload
amoak-stephen -
Category
Documents
-
view
32 -
download
1
description
b
Transcript of Oedematous Child

1
Group F1Group F1
THE OEDEMATOUS CHILDTHE OEDEMATOUS CHILD

2
GROUP MEMBERSGROUP MEMBERS
BARBARA OSSEI ANANE-BINFOHBARBARA OSSEI ANANE-BINFOHSAMSON SEIBUSAMSON SEIBUYVONNE DAPAAH-BERKOYVONNE DAPAAH-BERKO
MODERATORS: DR. ADDO-YOBOMODERATORS: DR. ADDO-YOBO DR. ANSONGDR. ANSONG

3
OUTLINEOUTLINE
DEFINITIONDEFINITION FACTORS DETERMINING FLUID FACTORS DETERMINING FLUID
DISTRIBUTIONDISTRIBUTION PATHOPHYSIOLOGYPATHOPHYSIOLOGY EXAMPLES OF DISORDERS WITH OEDEMAEXAMPLES OF DISORDERS WITH OEDEMA CLINICAL RECOGNITIONCLINICAL RECOGNITION MANAGEMENTMANAGEMENT SUMMARY/CONCLUSIONSUMMARY/CONCLUSION CASE STUDYCASE STUDY

4
DEFINITIONDEFINITION
Oedema is the excessive Oedema is the excessive accumulation of interstitial fluid.accumulation of interstitial fluid.
Some specific termsSome specific terms: hydrothorax, : hydrothorax, pericardial effusion, ascites, pericardial effusion, ascites, anarsacaanarsaca..

5
Factors Determining Fluid Factors Determining Fluid DistributionDistribution
Oedema is normally prevented by a proper balance b/n the Oedema is normally prevented by a proper balance b/n the opposing forces that affect the distribution of fluid across opposing forces that affect the distribution of fluid across the capillariesthe capillaries
Starling forces:Starling forces: Into capillaries:Into capillaries: Intra-cap colloid osmotic pressure: this determines plasma Intra-cap colloid osmotic pressure: this determines plasma
oncotic pressure & is dependent on the conc of plasma oncotic pressure & is dependent on the conc of plasma proteins, particularly albumin.proteins, particularly albumin.
Interstitial hydrostatic pressure: the magnitude varies from Interstitial hydrostatic pressure: the magnitude varies from organ to organ.organ to organ.
Out of capillaries:Out of capillaries: Intra-cap hydrostatic pressure: due to circulating blood vol Intra-cap hydrostatic pressure: due to circulating blood vol
& cardiac contractility. Na & water balance is an important & cardiac contractility. Na & water balance is an important determinant of this force. determinant of this force.
Interstitial colloid osmotic pressure.Interstitial colloid osmotic pressure.

6
Factors Determining Fluid Factors Determining Fluid Distribution (cont’d) Distribution (cont’d)
Tissue fluid is a continuously circulating medium, Tissue fluid is a continuously circulating medium, formed from & returned to the vascular systemformed from & returned to the vascular system
Filtration results from a net filtration pressure of Filtration results from a net filtration pressure of 11mmHg at the arteriolar end of the capillary bed11mmHg at the arteriolar end of the capillary bed
Interstitial fluid re-uptake is achieved by a net Interstitial fluid re-uptake is achieved by a net pressure of -9mmHg at the venular end of the pressure of -9mmHg at the venular end of the capillary bed. This change is as a result of a fall in capillary bed. This change is as a result of a fall in the capillary hydrostatic pressurethe capillary hydrostatic pressure
This re-uptake mechanism is said to be responsible This re-uptake mechanism is said to be responsible for the uptake of 85% of filtered fluid. The remaining for the uptake of 85% of filtered fluid. The remaining 15% is returned to the blood by the lymphatics15% is returned to the blood by the lymphatics
Conditions that tip this pressure balance to increase Conditions that tip this pressure balance to increase the net filtration pressure or decrease the re-uptake the net filtration pressure or decrease the re-uptake pressure will result in the accumulation of fluid in pressure will result in the accumulation of fluid in tissues tissues

7
PathophysiologyPathophysiology
Oedema may result from:Oedema may result from: High arterial blood pressure: High arterial blood pressure: increases cap increases cap
pr & causes excessive filtrationpr & causes excessive filtration Venous obstruction:Venous obstruction: produces a congestive produces a congestive
rise in cap pressurerise in cap pressure Leakage of plasma prot into interstitial Leakage of plasma prot into interstitial
fluid: fluid: as in inflamation & allergic rxns (e.g as in inflamation & allergic rxns (e.g angioneurotic oedema)angioneurotic oedema)
Decreased plasma pr conc:Decreased plasma pr conc: Liver Liver dxse,renal dxse & protein-losing dxse,renal dxse & protein-losing enteropathiesenteropathies

8
Pathophysiology cont’dPathophysiology cont’d
Myxoedema: Myxoedema: excessive production of excessive production of some glycoproteins (mucin) in the some glycoproteins (mucin) in the interstitial space in hypothyroidisminterstitial space in hypothyroidism
Obstruction of lymphatic drainage:Obstruction of lymphatic drainage: as as in filariasisin filariasis

9
Examples of Disorders with Examples of Disorders with OedemaOedema
Nephrotic syndromeNephrotic syndrome Nephritic syndromeNephritic syndrome Renal failureRenal failure Protein energy malnutritionProtein energy malnutrition Liver failureLiver failure Congestive heart failureCongestive heart failure Protein –losing enteropathiesProtein –losing enteropathies Angioneurotic oedemaAngioneurotic oedema LymphoedemaLymphoedema Over-hydrationOver-hydration

10
Nephrotic syndrome -1Nephrotic syndrome -1
A syndrome x’terised by:A syndrome x’terised by: Heavy proteinuria (urine pr = 3+ or Heavy proteinuria (urine pr = 3+ or
more)more) Hypoalbuminaemia ( <25g ) Hypoalbuminaemia ( <25g ) Oedema (usually generalised)Oedema (usually generalised) HypercholesterolaemiaHypercholesterolaemia
The primary pathology is the increased The primary pathology is the increased permeability of the GFB to plasma permeability of the GFB to plasma proteins, notably albuminproteins, notably albumin

11
Nephrotic Syndrome cont’dNephrotic Syndrome cont’d
Oedema in NSOedema in NS Oedema is a principal clinical feature of NSOedema is a principal clinical feature of NS Results primarily from decreased plasma Results primarily from decreased plasma
oncotic pressure secondary to oncotic pressure secondary to hypoalbuminaemiahypoalbuminaemia
Stimulation of the ren-ang-ald system as a Stimulation of the ren-ang-ald system as a result of the intravascular vol contraction result of the intravascular vol contraction leading to Na & water retention & thereby leading to Na & water retention & thereby sustaining the oedemasustaining the oedema

12
Nephrotic Syndrome cont’dNephrotic Syndrome cont’d
X’teristically there is:X’teristically there is: Periorbital oedema (esp. on waking)Periorbital oedema (esp. on waking) Scrotal/vulva, leg & ankle oedemaScrotal/vulva, leg & ankle oedema AscitesAscites Pleural effusionPleural effusion

13
Nephritic syndromeNephritic syndrome A clinical syndrome resulting from A clinical syndrome resulting from
glomerulonephritis glomerulonephritis Increased glomerular cellularity as a result Increased glomerular cellularity as a result
of the inflamatory process restricts GBF & of the inflamatory process restricts GBF & therefore GFR is reduced. This leads totherefore GFR is reduced. This leads to
# oliguria# oliguria # hypertension# hypertension # oedema# oedema # haematuria# haematuria # proteinuria (2+ or less on dipstick)# proteinuria (2+ or less on dipstick) # raised BUN# raised BUN

14
Renal FailureRenal Failure
Oedema in RF (esp CRF) is due to fluid Oedema in RF (esp CRF) is due to fluid retention as a result of:retention as a result of:
Decreased GFRDecreased GFR Loss of nephron fxnLoss of nephron fxn Na retentionNa retention

15
PEMPEM Results from dietary Results from dietary
deficiency of protein, deficiency of protein, energy & some energy & some micronutrients like Zn, micronutrients like Zn, vit A & Fevit A & Fe
There are a number of There are a number of forms of classifying forms of classifying PEM:PEM:
# Gomez# Gomez # Waterlow# Waterlow # Wellcome # Wellcome
classificationsclassifications Wellcome Wellcome
classificationclassification
Wt % Wt % of of standarstandardd
edema +edema + edemaedema--
60-80%60-80% kwash- kwash- iorkoriorkor
Under-Under-wtwt
<60%<60% Maras- Maras- mus-mus-kwashkwash
MarasmMarasm- us- us

16
PEMPEM
Oedema in PEMOedema in PEM The oedema results from low plasma albumin The oedema results from low plasma albumin
due to the poor dietary protein intake.due to the poor dietary protein intake. Based on severity and distribution, the Based on severity and distribution, the
oedema is rated as follows:oedema is rated as follows:
+ mild: both feet+ mild: both feet
++ moderate: both feet + lower legs + ++ moderate: both feet + lower legs + hands/lower arms hands/lower arms
+++ severe: generalised (moderate + face)+++ severe: generalised (moderate + face)

17
LIVER FAILURELIVER FAILURE There are two types;There are two types;1.1. ACUTE LIVER FAILURE (ALF)ACUTE LIVER FAILURE (ALF)2.2. CHRONIC LIVER FAILURE (CLF)CHRONIC LIVER FAILURE (CLF) ALF is uncommon in children but has a high ALF is uncommon in children but has a high
mortality rate.mortality rate. Causes of liver failure include;Causes of liver failure include;1.1. INFECTION – viral hepatitis A,B,C, non-A to GINFECTION – viral hepatitis A,B,C, non-A to G2.2. POISON/DRUGS – Paracetamol, isoniazidPOISON/DRUGS – Paracetamol, isoniazid3.3. METABOLIC – Wilson’s diseaseMETABOLIC – Wilson’s disease4.4. AUTOIMMUNE HEPATITISAUTOIMMUNE HEPATITIS5.5. REYE’S SYNDROMEREYE’S SYNDROME6.6. CIRRHOSISCIRRHOSIS

18
LIVER FAILURE cont’dLIVER FAILURE cont’d Plasma oncotic pressure is largely as a result of the Plasma oncotic pressure is largely as a result of the
presence of albumin in the blood. (which is produced presence of albumin in the blood. (which is produced by the liver.by the liver.
In liver failure the production of albumin is In liver failure the production of albumin is decreased a fall in the oncotic pressure.decreased a fall in the oncotic pressure.
Thus the overwhelming effect of the opposing Thus the overwhelming effect of the opposing plasma hydrostatic pressure will cause a net plasma hydrostatic pressure will cause a net movement of fluid from capillaries into the movement of fluid from capillaries into the interstitium.interstitium.
In some cases like cirrhosis, the obstruction to the In some cases like cirrhosis, the obstruction to the flow of blood in the portal system a rise in the flow of blood in the portal system a rise in the portal hydrostatic pressure, coupled with the portal hydrostatic pressure, coupled with the hypoalbuminaemia ascites. hypoalbuminaemia ascites.

19
PROTEIN-LOSING PROTEIN-LOSING ENTEROPATHYENTEROPATHY
Denotes the excessive loss of protein into Denotes the excessive loss of protein into the gut lumen, sufficient to cause the gut lumen, sufficient to cause hypoproteinaemia.hypoproteinaemia.
Less than 10% of plasma protein is Less than 10% of plasma protein is normally lost from the GIT.normally lost from the GIT.
It occurs in many gut disorders but is most It occurs in many gut disorders but is most common in those where ulceration occurs.common in those where ulceration occurs.
In other disorders protein loss results from In other disorders protein loss results from increased mucosal permeability or increased mucosal permeability or obstruction of intestinal lymphatic vessels.obstruction of intestinal lymphatic vessels.

20
Aetiology of Protein-losing Aetiology of Protein-losing enteropathies enteropathies
With mucosal erosion or ulcerationWith mucosal erosion or ulceration1.1. Crohn’s diseaseCrohn’s disease2.2. Ulcerative colitisUlcerative colitis3.3. LymphomaLymphoma
Without mucosal erosions or ulcerationWithout mucosal erosions or ulceration1.1. Bacterial overgrowthBacterial overgrowth2.2. Coeliac diseaseCoeliac disease3.3. Systemic Lupus ErythematosusSystemic Lupus Erythematosus 4.4. Measles enteritis Measles enteritis
With lymphatic obstructionWith lymphatic obstruction1.1. LymphomaLymphoma2.2. Intestinal lymphangiectasiaIntestinal lymphangiectasia3.3. Constrictive pericarditisConstrictive pericarditis

21
CARDIAC FAILURECARDIAC FAILURE
It is said to exist when the pumping It is said to exist when the pumping action of the heart is unable to action of the heart is unable to meet the metabolic demands of the meet the metabolic demands of the body.body.
Causes include;Causes include;
1.1. Biventricular failureBiventricular failure
2.2. Cardiac tamponadeCardiac tamponade
3.3. Constrictive pericarditisConstrictive pericarditis

22
1. CONGESTIVE CARDIAC 1. CONGESTIVE CARDIAC FAILURE (CCF)FAILURE (CCF)
CCF is characterized by the features of CCF is characterized by the features of systemic and systemic and pulmonary congestion.pulmonary congestion.
Systemic congestion (right sided failure);Systemic congestion (right sided failure);
The failure of the right ventricle to pump to the lungs results The failure of the right ventricle to pump to the lungs results in the pooling of blood in the systemic venous system in the pooling of blood in the systemic venous system increased hydrostatic over the opposing normal oncotic increased hydrostatic over the opposing normal oncotic pressure fluid passing into the interstitium.pressure fluid passing into the interstitium.
NB: fluid retention doesn’t show up as dependent edema, NB: fluid retention doesn’t show up as dependent edema, but it rather produces impressive hepatomegaly in but it rather produces impressive hepatomegaly in infants.infants.
Patient may present with abdominal distension due to Patient may present with abdominal distension due to ascites.Ther may be sacral edema in supine patients. ascites.Ther may be sacral edema in supine patients.

23
CARDIAC FAILURE CONT’DCARDIAC FAILURE CONT’D
Pulmonary congestion (left sided Pulmonary congestion (left sided failure)failure)
A failing left ventricle causes pooling of A failing left ventricle causes pooling of blood in the pulmonary system blood in the pulmonary system resulting in an increase in the resulting in an increase in the capillary hydrostatic pressure…………capillary hydrostatic pressure…………
Patient presents with features of Patient presents with features of pulmonary oedema (breathlessness, pulmonary oedema (breathlessness, tachypnoea and restlessness).tachypnoea and restlessness).

24
CARDIAC FAILURE CONT’DCARDIAC FAILURE CONT’DLVFLVF
Passive congestion of pulmonary circulationPassive congestion of pulmonary circulation
Increased hydrostatic pressure in the pulmonary vasculatureIncreased hydrostatic pressure in the pulmonary vasculature
Leakage of fluid into the interstitial tissue and air spacesLeakage of fluid into the interstitial tissue and air spaces
Pulmonary oedemaPulmonary oedema
Increased pulmonary vasculature resistanceIncreased pulmonary vasculature resistance
Right heart failureRight heart failure
Systemic venous congestion and soft tissue oedemaSystemic venous congestion and soft tissue oedema

25
CARDIAC FAILURE CONT’DCARDIAC FAILURE CONT’D
Cardiac tamponade and constrictive Cardiac tamponade and constrictive pericarditis all cause the ineffective pericarditis all cause the ineffective pumping of blood by the heart pumping of blood by the heart leading to pooling of blood in the leading to pooling of blood in the venous system.venous system.
Capillary hydrostatic pressure Capillary hydrostatic pressure increases as a result, over the increases as a result, over the opposing Starling’s forcesopposing Starling’s forces
Fluid moves into the interstitium. Fluid moves into the interstitium.

26
LYMPHOEDEMALYMPHOEDEMA
Obstruction to the flow of lymph in Obstruction to the flow of lymph in lymphatic vessels also lead to lymphatic vessels also lead to movement of fluid into the movement of fluid into the interstitium by the mechanism of interstitium by the mechanism of increased hydrostatic pressure.increased hydrostatic pressure.
Some of the causes include Some of the causes include neoplasm and infection (filarial neoplasm and infection (filarial worm infestation as in worm infestation as in elephantiasis). elephantiasis).

27
OTHER CAUSESOTHER CAUSES
Other causes of oedema in children Other causes of oedema in children are protein malabsorption, are protein malabsorption, angioneurotic oedema, angioneurotic oedema, inflammatory/allergic oedema.inflammatory/allergic oedema.

28
CLINICAL RECOGNITIONCLINICAL RECOGNITION
Oedema is detected clinically by Oedema is detected clinically by pressing on bony prominences in the pressing on bony prominences in the lower limbs and sacrum for between lower limbs and sacrum for between 30 and 60 secs,and examining for 30 and 60 secs,and examining for pitting and depression.on the face pitting and depression.on the face there is noticeable fullness of the there is noticeable fullness of the periorbital area and obvious facial periorbital area and obvious facial flank fullnessflank fullness

29
DIAGNOSISDIAGNOSIS Elements of diagnosis:Elements of diagnosis:
Good history,Good history, Thorough physical examination Thorough physical examination Appropriate laboratory investigations.Appropriate laboratory investigations.
Note:Note: the clinical presentation of oedema appears the clinical presentation of oedema appears
with other associated features which aids in with other associated features which aids in identifying it’s origin.identifying it’s origin.
oedema therefore should not be considered in oedema therefore should not be considered in isolation, because it is usually secondary to a isolation, because it is usually secondary to a disease processdisease process

30
History in relation to the History in relation to the oedematous childoedematous child
NutritionalNutritional CVSCVS RenalRenal hepatichepatic Metabolic (hypothyroidism)Metabolic (hypothyroidism) angioneuroticangioneurotic

31
OEDEMA OF NUTRITIONAL OEDEMA OF NUTRITIONAL ORIGINORIGIN
Emphasis should be laid on the Emphasis should be laid on the nutritional history.nutritional history. Type of food taken, quantity and quality.Type of food taken, quantity and quality. Frequency of food intake per day.Frequency of food intake per day. Duration of exclusive breastfeeding and Duration of exclusive breastfeeding and
the type of weaning foods introduced.the type of weaning foods introduced. Enquiries should also be made about the Enquiries should also be made about the
social history taken into consideration the social history taken into consideration the socioeconomic status of the parents socioeconomic status of the parents (income of the parents versus the (income of the parents versus the number of children)number of children)

32
OEDEMA OF CARDIAC ORIGINOEDEMA OF CARDIAC ORIGIN
History of breathlessness on History of breathlessness on exertion, orthopnoea and paroxsymal exertion, orthopnoea and paroxsymal nocturnal dyspnoeanocturnal dyspnoea
Poor feedingPoor feeding Sweating Sweating History of congenital heart diseaseHistory of congenital heart disease

33
OEDEMA OF RENAL ORIGINOEDEMA OF RENAL ORIGIN
History of decreased urine outputHistory of decreased urine output History of haematuriaHistory of haematuria Preceding history of pharyngitis or Preceding history of pharyngitis or
skin infection (PIGN)skin infection (PIGN) History of early morning facial History of early morning facial
puffinesspuffiness

34
OEDEMA OF HEPATIC ORIGINOEDEMA OF HEPATIC ORIGIN
History of jaundiceHistory of jaundice History of pruritus, dark urineHistory of pruritus, dark urine History of bruising and petechiaeHistory of bruising and petechiae

35
OEDEMA OF METABOLIC OEDEMA OF METABOLIC ORIGIN(MYXOEDEMA)ORIGIN(MYXOEDEMA)
History of cold intoleranceHistory of cold intolerance History of weight gain despite poor History of weight gain despite poor
appetiteappetite

36
ANGIONUEROTIC OEDEMAANGIONUEROTIC OEDEMA
History of insect bite( bee sting)History of insect bite( bee sting) ?drugs?drugs

37
PHYSICAL EXAMINATIONPHYSICAL EXAMINATION ON INSPECTIONON INSPECTION Wasting, dermatosis, silky and sparse Wasting, dermatosis, silky and sparse
hair, eye signs of Vit A deficiency hair, eye signs of Vit A deficiency (NUTRITIONAL)(NUTRITIONAL)
Jaundice, clubbing, spider naevi, caput Jaundice, clubbing, spider naevi, caput medusae (HEPATIC)medusae (HEPATIC)
Small for age, breathless, clubbing, Small for age, breathless, clubbing, raised JVP, cyanosis (CARDIAC)raised JVP, cyanosis (CARDIAC)
Increased BP, multiple scarring on the Increased BP, multiple scarring on the skin (RENAL)skin (RENAL)

38
ON PALPATIONON PALPATION
Is the apex displaced, thrills or Is the apex displaced, thrills or heaves?heaves?
Pulse rate, collapsing?Pulse rate, collapsing? Tender hepatomegally?Tender hepatomegally? Check oedema at the sacral region Check oedema at the sacral region
and the extent of pedal oedema.and the extent of pedal oedema.

39
ON ON PERCUSSION/AUSCULTATIONPERCUSSION/AUSCULTATION
Percuss for ascites and shifting Percuss for ascites and shifting dullness and fluid thrill.dullness and fluid thrill.
Percussion of the chest will be dull Percussion of the chest will be dull (pleural effusion)(pleural effusion)
AND ON AUSCULTATION, crackles AND ON AUSCULTATION, crackles and murmursand murmurs

40
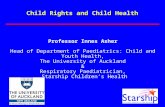
Oedema
History ofDecreased food intakeShort period of EBF or no BFParents being of low socio-economic class
History of•Decreased urinary output•Haematuria•Sore throat/skin rash
History of progressiveJaundice.
History of•Dyspnoea on exertion•Orthopnoea•PND
Signs of•Wasting•Flaky paint•Fluffy hair•Apathy
Examine for•HPT by mea- suringThe BP
Signs of•Jaundice•Hepatomegaly
Examine for•Galllop rhythm•Dyspnoea•Raised JVP•Tender hepatomegaly
Oedema of Nutritional
originOedema of
Renal origin
Oedema ofHepaticOrigin
Oedema ofCardiacOrigin

41
INVESTIGATIONS INVESTIGATIONS
RENALRENAL Low serum albumin and protein (nutritional and renal)Low serum albumin and protein (nutritional and renal) Urinalysis:+3/4 proteinuria or >2g/24hrsUrinalysis:+3/4 proteinuria or >2g/24hrs Hypoalbuminaemia(<25g/l)hypercholeslrolaemia(nephrotic Hypoalbuminaemia(<25g/l)hypercholeslrolaemia(nephrotic
syndrome)syndrome) Casturia and RBCs (nephritic)Casturia and RBCs (nephritic)LIVERLIVER Liver function test: mixed hyperbilirubinaemia, low serum Liver function test: mixed hyperbilirubinaemia, low serum
albuminalbumin Coagulation may be abnormalCoagulation may be abnormalCVSCVS Chest X-ray: cardiomegallyChest X-ray: cardiomegally ECG, echoECG, echoMYXOEDEMAMYXOEDEMAThyroid function test: low T4,TSH may be high or lowThyroid function test: low T4,TSH may be high or low

42
TREATMENTTREATMENT
The mainstay of treatment of the The mainstay of treatment of the oedematous child is to determine and treat oedematous child is to determine and treat the underlying cause. the underlying cause.
Treating the underlying cause often causes Treating the underlying cause often causes the oedema to improve or resolve.the oedema to improve or resolve.
It may be necessary to control severe It may be necessary to control severe symptomatic oedema to assist in recoverysymptomatic oedema to assist in recoverye.g. severe nephritic syndrome, severe e.g. severe nephritic syndrome, severe ascites.ascites.

43
Measure of oedema controlMeasure of oedema control
FLUID RESTRICTIONFLUID RESTRICTION
DIETRY CONTROLDIETRY CONTROL
SALT POOR ALBUMINSALT POOR ALBUMIN
ABDOMINAL PARACENTESISABDOMINAL PARACENTESIS
DIURETICSDIURETICS

44
TREATMENT CONT’DTREATMENT CONT’D FLUID RESTRICTIONFLUID RESTRICTION
Particularly important in oedema of renal origin Particularly important in oedema of renal origin due to intrinsic renal failure. Here fluid must be due to intrinsic renal failure. Here fluid must be restricted to the previous day’s output plus restricted to the previous day’s output plus involuntary loss (500ml/m2 in children)involuntary loss (500ml/m2 in children)
DIETARY CONTROLDIETARY CONTROL Important in oedema due to decreased Important in oedema due to decreased
capillary oncotic pressure from protein loosing capillary oncotic pressure from protein loosing state or salt and water retention .state or salt and water retention .
Patients with oedema of renal origin should be Patients with oedema of renal origin should be advised to restrict or reduce their salt intake.advised to restrict or reduce their salt intake.Those with oedema of nutritional origin or Those with oedema of nutritional origin or nephrotic syndrome due to the proteinuria are nephrotic syndrome due to the proteinuria are advised to increase their protein intakeadvised to increase their protein intake

45
TREATMENT CONT’DTREATMENT CONT’D SALT POOR ALBUMINSALT POOR ALBUMIN
This is particularly useful in intractable oedema due to nephrotic This is particularly useful in intractable oedema due to nephrotic syndrome.It helps to increase the oncotic pressure in the capillary syndrome.It helps to increase the oncotic pressure in the capillary space thereby controlling the oedema. However salt poor albumin space thereby controlling the oedema. However salt poor albumin is not easily obtainable in the tropics so plasma transfusion which is not easily obtainable in the tropics so plasma transfusion which follows the same principle is an alternativefollows the same principle is an alternative
ABDOMINAL PARACENTESISABDOMINAL PARACENTESIS
This is done when there is ascities as a component of the This is done when there is ascities as a component of the generalised oedema and continues to increse despite generalised oedema and continues to increse despite pharmacological measures taken.It is done particularly when the pharmacological measures taken.It is done particularly when the ascities is so great that it causes respiratory ascities is so great that it causes respiratory embarrassment.However it gives only short relief as it soon embarrassment.However it gives only short relief as it soon accumulates again in most cases,peritonitis is also a riskaccumulates again in most cases,peritonitis is also a risk
DIRETICS:They are useful in the mobilization of oedema fluid DIRETICS:They are useful in the mobilization of oedema fluid thereby controlling the oedema.Diuretics should not be used in thereby controlling the oedema.Diuretics should not be used in oedema of nutritional origin and should also be used with caution oedema of nutritional origin and should also be used with caution in plasma depleted nephrotic syndromein plasma depleted nephrotic syndrome

46
Summary/ConclusionSummary/Conclusion
Oedema is defined as excessive accumulation Oedema is defined as excessive accumulation of interstitial fluidof interstitial fluid
It is normally prevented by a proper balance It is normally prevented by a proper balance between opposing forces that affect between opposing forces that affect distribution of fluid across the capillariesdistribution of fluid across the capillaries
It should not be considered in isolation since it It should not be considered in isolation since it is usually secondary to a disease process…….is usually secondary to a disease process…….
A good history, thorough physical examination A good history, thorough physical examination and appropriate investigations aids in arriving and appropriate investigations aids in arriving at a diagnosis of the cause of oedemaat a diagnosis of the cause of oedema

47

48
Case presentationCase presentation
A 5-year old girl.A 5-year old girl.
PC:PC: Suppurative lesion on mandible – 3/52Suppurative lesion on mandible – 3/52 Generalised body swelling -5/7Generalised body swelling -5/7
HPC: HPC: Toothache 3 weeks ago. Toothache 3 weeks ago. Painful jaw swelling a week later (received hospital Painful jaw swelling a week later (received hospital medication??)medication??)
Then suppuration and ulceration plus early morning facial Then suppuration and ulceration plus early morning facial puffiness puffiness
KATH admission for I&D and Blood transfusionKATH admission for I&D and Blood transfusion
Then anasarca 3 days laterThen anasarca 3 days later

49
ODQODQ
Poor feeding- 3 weeksPoor feeding- 3 weeks ? Fever. ? Fever. No urinary symptoms No urinary symptoms No GI symptomsNo GI symptoms Paralysis (since illness)Paralysis (since illness) Poor speech (from jaw lesion)Poor speech (from jaw lesion) No respiratory symptomsNo respiratory symptoms

50
HISTORYHISTORY
Past medical hx : nil of notePast medical hx : nil of note Immunisation hx: completed according to Immunisation hx: completed according to
RTHC . BCG scar not seen.RTHC . BCG scar not seen. Nutritional hx: Nutritional hx:
Apparently good nutrition before illness.Apparently good nutrition before illness.
Drug hx: herbal preparations for swellingDrug hx: herbal preparations for swelling Family & Social Hx:Family & Social Hx:
55thth of 5 children. of 5 children. Mother is 46 & a farmer. Father dead Mother is 46 & a farmer. Father dead (hypertention).(hypertention).

51
O/EO/E Ill-lookingIll-looking
Jaw swelling covered with plasterJaw swelling covered with plaster
Generalised oedema (bilateral pitting Generalised oedema (bilateral pitting pedal oedama), afebrile, pale, anictericpedal oedama), afebrile, pale, anicteric
No clubbingNo clubbing Hair browning along hairlineHair browning along hairline Not wastedNot wasted Extremities warmExtremities warm Weight=20kgs(above the 70th centile)Weight=20kgs(above the 70th centile) Height=106cm(below 50Height=106cm(below 50thth centile) centile)

52
O/EO/E Chest : Chest :
Tachypnoea (RR=60cpm). Tachypnoea (RR=60cpm). Clinically clear. Clinically clear.
CVS: BP=90/70mmHg, CVS: BP=90/70mmHg, HR=140bpm, HS=I+II+0HR=140bpm, HS=I+II+0
Tender Gibbus (Thoracolumbar)Tender Gibbus (Thoracolumbar)
Abdomen: Abdomen: Liver-5cm, Non-tender, firm, smooth. Liver-5cm, Non-tender, firm, smooth. Spleen not palpableSpleen not palpableNo ascites No ascites

53
DIFFERENTIALSDIFFERENTIALS(Why is this child oedematous?)(Why is this child oedematous?)
Post-infection glomerulonephritis Post-infection glomerulonephritis (Nephritic Syndrome)(Nephritic Syndrome)
Nephrotic syndromeNephrotic syndrome MalnutritionMalnutrition ? Renal Insufficiency (?TB, ?Bacteria)? Renal Insufficiency (?TB, ?Bacteria)

54
INVESTIGATIONSINVESTIGATIONS
Urinalysis Urinalysis Serum albumin & proteinSerum albumin & protein Renal function testRenal function test X-ray of the spine, Jaw X-ray of the spine, Jaw
Others:Others: Haematology: Haematology:
Hb, FBC, ESR ASO titre, Hb, FBC, ESR ASO titre, Wound swab for C/SWound swab for C/S Mantoux test Mantoux test

55
RESULTSRESULTS
Hb= 8.0g/dlHb= 8.0g/dl ESR=86mm fall/hrESR=86mm fall/hr
URINALYSISURINALYSIS PROTEIN=TRACEPROTEIN=TRACE BLOOD =+1BLOOD =+1 BILIRUBIN=+1BILIRUBIN=+1 LEUCOCYTES=+1LEUCOCYTES=+1

56
DIAGNOSIS?DIAGNOSIS?
What could be the most probable What could be the most probable diagnosis?diagnosis?

57





![· Web viewYour "Dependent child" includes Your legally adopted child, Your step-child, Your foster child, the child of his or her civil union partner, [and] [, the child of his](https://static.fdocuments.net/doc/165x107/5f0bd4557e708231d4326b13/web-view-your-dependent-child-includes-your-legally-adopted-child-your.jpg)











