
Oculoplastics overview - cdn.auckland.ac.nz · Driving lacrimal pump ... Orbital disorders . 49 ....
70
Oculoplastics overview Dr Ekta Aggarwal
Transcript of Oculoplastics overview - cdn.auckland.ac.nz · Driving lacrimal pump ... Orbital disorders . 49 ....

Oculoplastics overview Dr Ekta Aggarwal

Case Scenario Links Oculoplastics overview • Child with red swelling around one eye (Oph10) • Diplopia (Oph06) • Gradual deterioration in visual acuity over time (Oph07) • Watery eye in an infant (Oph03) • Skin tumours (Derm03)
2

3
EYELIDS

Functions of Eyelids:
Light protection & regulation Keep cornea moist Driving lacrimal pump Mechanical protection of globe
4

EYELIDS (surface anatomy)
Upper lid [UL] covers superior 2mm of cornea (10 – 2’o clock)
Lower Lid [LL] margin JUST touches inferior limbus 5
EYELIDS (surface anatomy)
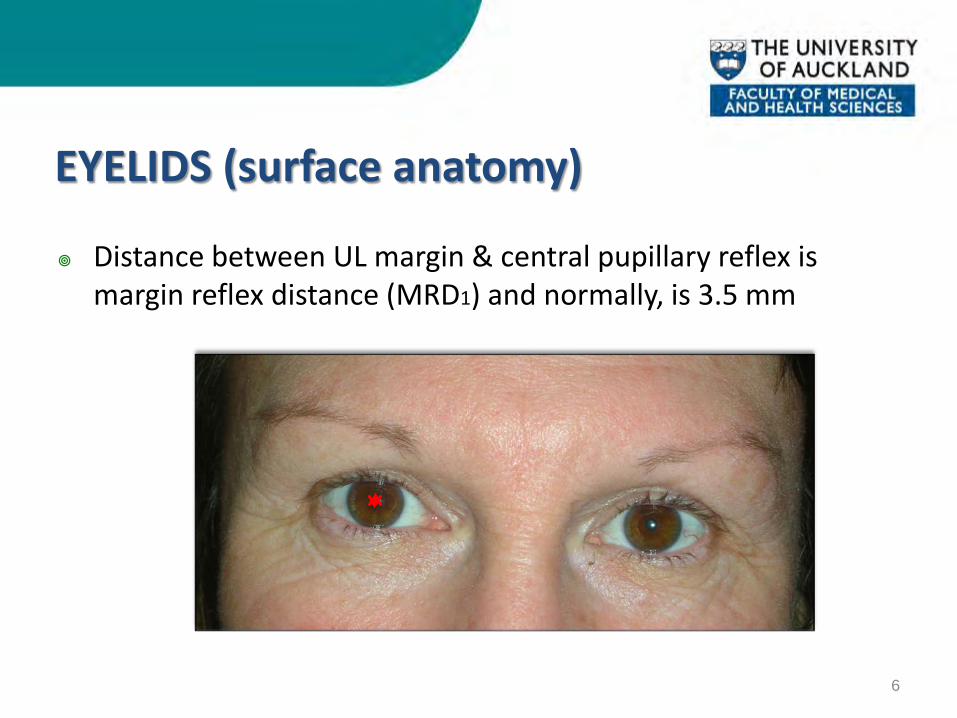
Distance between UL margin & central pupillary reflex is margin reflex distance (MRD1) and normally, is 3.5 mm
6

EYELIDS (surface anatomy)
Space between UL & LL is palpebral fissure height (PFH) and normally, it is 10-12 mm.
7

EYELIDS (surface anatomy)
A puncta (one in each lid) lies in close apposition to globe
8

Levator Palpebrae superioris [LPS]
• LPS action – From extreme down gaze to extreme up gaze, by blocking the Frontalis
• Important while planning surgical management of ptosis
9
Presenter
Presentation Notes
Nearly 50mm long, originates above Annulus of Zinn, stays close to orbital roof. Travels forward and close to superior orbital rim, it changes its antero-posterior direction to vertical and inserts down at various levels close to tarsus. This direction change is marked by Whitnall’s ligament, which marks the end of muscular part and beginning of aponeurotic LPS. Its insertion into lid skin makes lid crease
To summarize- Normal parameters for lid position evaluation:
MRD1 – 3.5 – 4.0 mm PFH – 10 -11mm LPA – <4mm – poor 5-7mm – fair > 7-8mm – good Lid crease height – 10 mm in females 8-10 mm in males Inferior scleral show – Nil Lagophthalmos (inability to close eyes) – Nil Bell’s phenomenon (globe movement on eye closure) – Up and out
10

Eyelid muscular and nervous control
11
Presenter
Presentation Notes
Protractor muscle, i.e. Orbicularis Oculi, closes the eyelid and is supplied by 7th cranial nerve. Retractors of the eyelid are Levator Palpebrae Superioris and Muller’s muscle, supplied by 3rd cranial nerve (parasympathetic) and sympathetic nerves respectively.
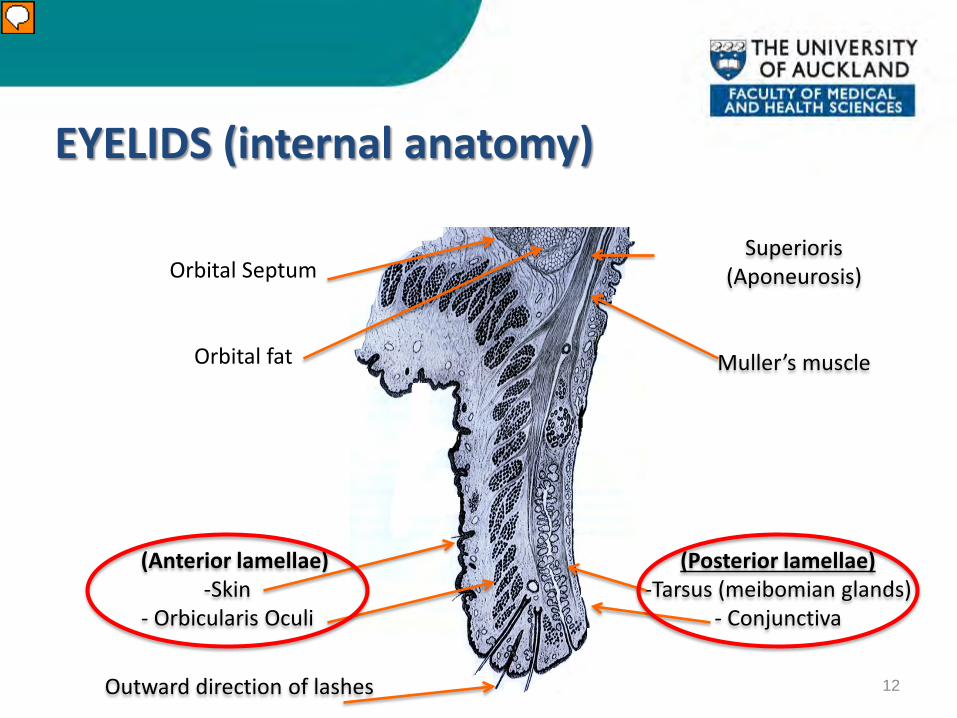
EYELIDS (internal anatomy)
12
(Anterior lamellae) -Skin
- Orbicularis Oculi
(Posterior lamellae) -Tarsus (meibomian glands)
- Conjunctiva
Superioris (Aponeurosis)
Muller’s muscle
Orbital Septum
Orbital fat
Outward direction of lashes
Presenter
Presentation Notes
Basically, eyelid is divided into anterior [consisting of skin & Orbicularis muscle] and posterior layers [tarsus and conjunctiva]. It is easier to understand eyelid pathologies, by having a clear concept of these two layers.

EYELID POSITION ANOMALIES along horizontal axis
PTOSIS (droopy eyelid)
14

Congenital Ptosis FEATURES: - Fair to Poor LPS action - Faint/ Absent lid crease - Lid lag on down gaze
15
If chin elevation & frontalis overaction (s/o visual axis obstruction by ptotic lid), It needs urgent intervention, or else amblyopia develops.
Presenter
Presentation Notes
Chin elevation and frontalis overaction are suggestive of visual field being obstructed by droopy eyelid. A young child is at high risk of amblyopia, if visual axis is covered by ptotic lid, thus warranting immediate surgery.

Acquired Ptosis FEATURES: - Good LPS action - High lid crease - No lid lag on down gaze
16
Presenter
Presentation Notes
Notice chin elevation and frontalis overaction, suggestive of visual field being obstructed by droopy eyelid.

Acquired Ptosis Causes: Involutional Mechanical Myogenic Traumatic Neurogenic
17
Not all acquired cases have classical
features of acquired ptosis

Acquired Ptosis Involutional (Aponeurotic) the most common type of ptosis
18
Frontalis overaction (s/o visual axis obstruction by ptotic lid); but surgery depends upon patient’s comfort level. No risk of amblyopia after the age of
8-10 yrs.

Acquired Ptosis
Myogenic:
Chronic Progressive External Ophthalmoplegia [CPEO] Myasthenia gravis [diurnal variation] Ptosis is one component of these syndromes
19
Presenter
Presentation Notes
CPEO and Myasthenia gravis affect Levator muscle, thus causing droopiness of eyelids.

Acquired Ptosis Neurogenic: - Third Cranial nerve palsy Note: Total ptosis Exotropia Hypotropia Mydriasis
20
Presenter
Presentation Notes
Oculomotor nerve palsy as in brain lesions or trauma or orbital apex syndrome would paralyze Levator muscle, thus causing ptosis. Sympathetic chain lesions would affect Muller’s muscle leading to mild ptosis.
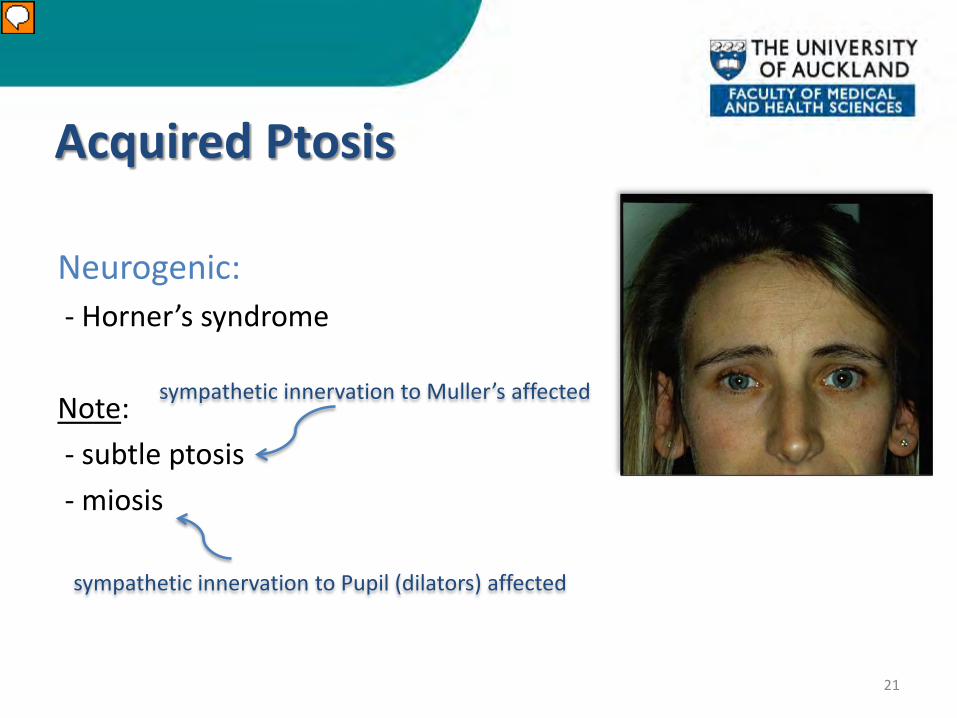
Acquired Ptosis Neurogenic: - Horner’s syndrome Note: - subtle ptosis - miosis
21
sympathetic innervation to Pupil (dilators) affected
sympathetic innervation to Muller’s affected
Presenter
Presentation Notes
Oculomotor nerve palsy as in brain lesions or trauma or orbital apex syndrome would paralyze Levator muscle, thus causing ptosis. Sympathetic chain lesions would affect Muller’s muscle leading to mild ptosis.

Acquired Ptosis Mechanical: UL tumors as Hemangioma Lid edema as post-trauma/ surgery Dermatochalasis (aging skin hanging over UL margin)
22
Presenter
Presentation Notes
Classic clinical features of acquired ptosis can again vary.

Acquired Ptosis Trauma: Blunt or penetrating Long term contact lens wear Iatrogenic
Causes of mechanical/ traumatic ptosis may overlap
23
Presenter
Presentation Notes
Classical features of acquired ptosis may vary.

EYELID POSITION ANOMALIES along horizontal axis
Lid Retraction
24

Lid Retraction Causes: Congenital Acquired - Thyroid Eye Disease - Midbrain lesions - Parinaud’s syndrome
25

EYELID POSITION ANOMALIES along vertical axis
Ectropion
(eyelid margin is away from the globe)
26

ECTROPION Causes: Involutional Cicatricial Paralytic (VII CN palsy) Mechanical
Prolonged ectropion leads to metaplastic changes in exposed conjunctiva
27

ECTROPION Causes:
Involutional Cicatricial Paralytic (VII CN palsy) Mechanical
Due to laxity of canthal tendons (structural support of lids at medial & lateral
ends) with age
28

ECTROPION Causes: Involutional Cicatricial Paralytic (VII CN palsy) Mechanical
Traumatic scar at cheek pulling the lower lid down
29

ECTROPION Causes: Involutional Cicatricial Paralytic (VII CN palsy) Mechanical
Facial nerve supplying Orbicularis Oculi is affected, as in Bell’s palsy, Parotid tumor excision, Acoustic Neuroma
30

ECTROPION Causes: Involutional Cicatricial Paralytic (VII CN palsy) Mechanical
Lower eyelid edema causing mechanical ectropion
31

EYELID POSITION ANOMALIES along vertical axis
Entropion
(eyelid margin rolled in)
32

ENTROPION Causes: Involutional Trauma Cicatricial
Entropion leads to trichiasis (misdirection of lashes), which may cause
punctate epitheliopathy of cornea to frank corneal ulcers.
33
Presenter
Presentation Notes
The main pathology in involutional type is over-riding of pre-septal orbicularis on pre-tarsal orbicularis oculi.

ENTROPION Causes: Involutional Trauma Cicatricial Ocular Cicatricial Pemphigoid Stevens Johnson syndrome Trachoma (developing countries) Chemical injury Contraction and thus, shortening of posterior lamella of the eyelid: which
pulls and rolls in the eyelid margin along with eyelashes.
34
Presenter
Presentation Notes
The main pathology in involutional type is over-riding of pre-septal orbicularis on pre-tarsal orbicularis oculi.

ORBIT

Gener
36
General overview of Orbital bones

37 37
Frontal, Sphenoid

38 38
Zygomatic, Sphenoid

39 39
Zygomatic, Maxilla, Palatine

40 40
Maxilla, Lacrimal, Ethmoid, Sphenoid

41

42

43
•Optic Nerve •Ophthalmic A •Sympathetic N plexus

44
Annulus of Zinn

45
Orbital septum is a white 360° tough barrier between orbit and lid tissues, stretching from distal
tarsus border to orbital rim
Important to differentiate, if inflammation/ infection is limited in front of OS extends behind the orbital septum

46
Skull Sinuses & Orbit
46
Frontal Sinus
Ethmoid Sinus
Maxillary Sinus

Skull Sinuses & Orbit
Function of sinuses: Decrease weight of skull. Increase resonance of voice. Humidify and heat the inhaled air
47

Orbit examination • Visual acuity • Pupils – miosis, mydriasis, RAPD • Visual field • Extra-ocular movements • Exophthalmometer – axial/non-axial, look from above/below • Palpate orbit for masses • Lids – retraction, masses, scleral show • Optic nerve
48
Common Orbital disorders
49

Pre-septal cellulitis Etiology: Trauma, Insect bite, Stye Features: - Inflamed, oedematous lids - Nil/ mild pain on eye movements - Visual acuity good - Intact Optic Nerve function
50

Orbital Cellulitis Aetiology: Sinusitis (commoner in children) Trauma/ Tumor in adjoining sinuses Features: - Proptosis - Inflamed pre-septal tissues - Painful/ limited eye movements - Drop in Visual acuity - Compromised Optic Nerve function
51
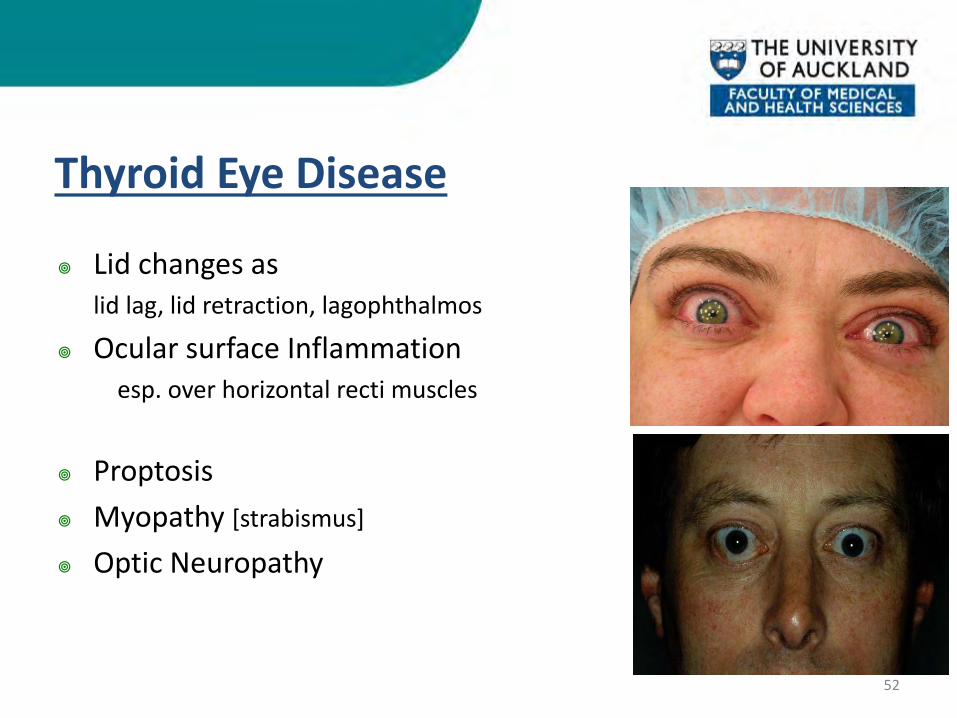
Thyroid Eye Disease
Lid changes as lid lag, lid retraction, lagophthalmos
Ocular surface Inflammation esp. over horizontal recti muscles
Proptosis Myopathy [strabismus]
Optic Neuropathy
52

Thyroid Eye Disease
CT scan features in Thyroid eye disease • Thick extra-ocular (recti) muscles • Maximum diameter of globe beyond lateral orbital rim • Tenting of optic nerve on right side ( )
53

Thyroid Eye Disease
Keep a close watch on: Corneal exposure – treat with lubricants/ taping eyelids shut Optic nerve functions due to its possible compression by
enlarged extra-ocular muscles – might need urgent surgical intervention
54

Orbital Fracture
Classical Signs: Hypotropia Enophthalmos Restricted motility, esp. vertical gaze Infra-orbital anesthesia
55 55

Orbital Fracture
Orbital Floor fracture and prolapse of Inf. Rectus & soft tissues in maxillary sinus
56 56
Common Eyelid Lesions
57

Benign Eyelid Lesions
Chalazion - Chronic, granulomatous inflammation of meibomian glands - Involving posterior eyelid lamellae
Stye - Tender, acute inflammation of sebaceous glands of Zeiss or sweat glands of Moll at the base of eyelashes in anterior eyelid lamellae
58

Benign Eyelid Lesions
Stye Treatment: - Warm compresses, antibiotic ointment - Expression of pus ± lash removal
59
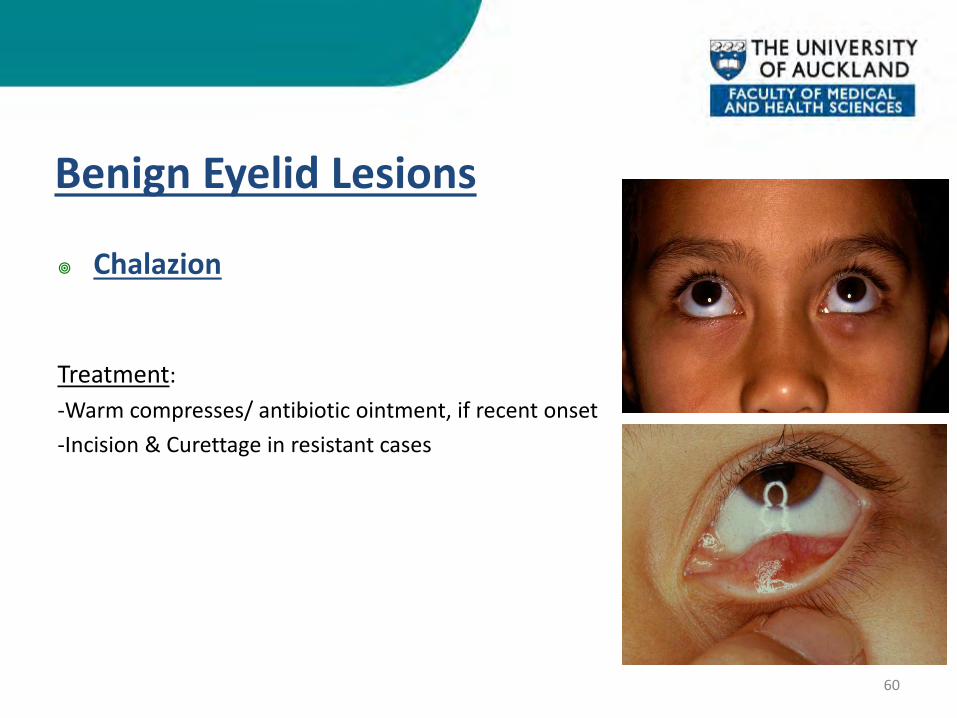
Benign Eyelid Lesions
Chalazion
Treatment: -Warm compresses/ antibiotic ointment, if recent onset -Incision & Curettage in resistant cases
60

Benign Eyelid Lesions
Xanthelasmas - Yellowish, sessile plaques - S/o hypercholesterolaemia
Treatment: - Removal for cosmesis
61

Malignant Eyelid Lesions
Basal cell cancer - Commonest lid malignancy (90%) - Risk factors: Fair skin & UV exposure
Features: - Nodular/ulcerative with rolled edges - Loss of lashes - Telengiectatic blood vessels on surface Treatment: Excision with wide margins ± Cryotherapy
62

Malignant Eyelid Lesions
Squamous cell cancer - Fast growing skin cancer
Features: - Nodular - Hyperkeratotic surface
Treatment: Excision Biopsy with wide margins ± radiotherapy depending upon the depth of involvement
63

Lacrimal Drainage System
64

65
Lacrimal gland produce tears (aqueous part)

66
Lacrimal gland produce tears (aqueous part)
Lacrimal drainage system

Common Lacrimal Disorders
67

Congenital Naso-lacrimal Duct Obstruction
Symptoms start soon after birth - Watering ± discharge
- Fluorescein dye disappearance delayed
68

Congenital Naso-lacrimal Duct Obstruction
Treatment Options in order of preference: a) Conservative [Lacrimal Massage ± Antibiotics] b) Probing & Syringing c) Intubation/ Balloon Dacryoplasty d) Dacryocystorhinostomy
Nearly 95% resolve conservatively by the end of one year of age
69

Acquired Naso-lacrimal Duct Obstruction
• Commoner in females > 40 years of age • Delayed Fluorescein dye disappearance test • Syringing: Complete/ partial regurgitation of fluid Treatment: - Dacryocystorhinostomy [external/ endoscopic] ± silicon intubation
70
The End
All material contained in this presentation is copyright of The University of Auckland, Department of Ophthalmology and should not be reproduced without written permission


















