
Ocular Surface Disorder Allergic Conjunctivitis– A Revie · to a different category of allergic...
7
www. dosonline.org l 41 Ocular Surface Disorder Bithi Chaudhary MS, FRCS Bithi Chowdhury MS, FRCS NDMC Medical College and Hindu Rao Hospital, Delhi Allergic Conjunctivitis– A Review Ocular Surface Disorder O cular allergy is one of the most common ocular conditions encountered in clinical practice. Ocular allergy is estimated to affect 5 – 22% of the population depending on the geographical setting and the age of the population 1 . It is also often under diagnosed and undertreated. Definitive etiology is not known but genetic predisposition, air pollution in urban area and exposure to pets have been associated. Besides causing irritating symptoms, visual loss in severe cases, its effect on the quality of life and economic burden on the patient is profound. This article broadly outlines the clinical features, diagnosis, investigation and treatment of allergic conjunctivitis. Types of allergic conjunctivitis Seasonal allergic conjunctivitis (SAC) and perineal allergic conjunctivitis (PAC) are the most commonly seen allergic conjunctivitis. Atopic keratoconjunctivitis (AKC), vernal keratoconjunctivitis (VKC), giant papillary conjunctivitis (GPC) and contact dermatitis conjunctivitis (CDC) represents the other spectrum of the disorder. GPC is caused by micro trauma especially with the use of extended wear soft contact lens. Those with history of allergy have high risk of having GPC. CDC belongs to a different category of allergic reaction as it is not IgE mediated. Seasonal Allergic Conjunctivitis and Perineal Allergic Conjunctivitis SAC is the most common form of all ocular allergic diseases and is triggered by exposure to pollen. It usually occurs in spring. PAC is induced by exposure to dust mites fungi, animal epithelial and/or occupational allergens. The affected patients can show symptoms throughout the year with acute seasonal exacerbations. Pathophysiology The response to allergen in allergic conjunctivitis is due to its interaction with prostaglandins and leukotrienes. It is a type I hypersensitivity reaction and the early response lasts clinically for 20 -30 minutes. The late phase reaction is due to the presence of inflammatory cells in the conjunctival mucosa. This is brought about by activation of vascular endothelial cells, which in turn expresses chemokines, adhesion molecules such as such as intercellular adhesion molecule (ICAM) and vascular cell adhesion molecule (VCAM). Other chemokines secreted include regulated upon activation normal T cell expressed and secreted (RANTES) chemokines, monocyte chemo attractant protein (MCP), interleukin (IL)-8, eotaxin and macrophage inflammatory protein (MIP)-1 alpha. Clinical features The clinical presentation in both the conditions is similar. Patients complains of bilateral itching, tearing and burning sensation. Blurred vision and photophobia may be due to an alteration in the composition and instability of the tear film. PAC affects young adults between 20-40 years of age with no gender predilection while SAC has no age or gender predilection. Both are frequently associated with allergic rhinitis and other allergic disorder (slightly more with SAC). On examination, mild to moderate conjunctival hyperemia with an edematous conjunctival surface is seen. The palpebral conjunctiva appears pale pink in color with diffuse areas of slightly hypertrophic papillae predominantly located in the upper tarsal conjunctiva (Figure-1a,b). The cornea is rarely affected. Diagnosis: Diagnostic features of SAC and PAC consist of itching, redness, and swelling of the conjunctiva. However other criterias that help in the diagnosis are a family
-
Upload
nguyenthien -
Category
Documents
-
view
227 -
download
2
Transcript of Ocular Surface Disorder Allergic Conjunctivitis– A Revie · to a different category of allergic...

www. dosonline.org l 41
Ocular Surface Disorder
Bithi ChaudharyMS, FRCS
Bithi Chowdhury MS, FRCS
NDMC Medical College and Hindu Rao Hospital, Delhi
Allergic Conjunctivitis– A Review
Ocular Surface Disorder
Ocular allergy is one of the most common ocular conditions encountered in clinical practice. Ocular
allergy is estimated to affect 5 – 22% of the population depending on the geographical setting and the age of the population1. It is also often under diagnosed and undertreated. Definitive etiology is not known but genetic predisposition, air pollution in urban area and exposure to pets have been associated. Besides causing irritating symptoms, visual loss in severe cases, its effect on the quality of life and economic burden on the patient is profound. This article broadly outlines the clinical features, diagnosis, investigation and treatment of allergic conjunctivitis.
Types of allergic conjunctivitisSeasonal allergic conjunctivitis (SAC) and perineal allergic conjunctivitis (PAC) are the most commonly seen allergic conjunctivitis. Atopic keratoconjunctivitis (AKC), vernal keratoconjunctivitis (VKC), giant papillary conjunctivitis (GPC) and contact dermatitis conjunctivitis (CDC) represents the other spectrum of the disorder.
GPC is caused by micro trauma especially with the use of extended wear soft contact lens. Those with history of allergy have high risk of having GPC. CDC belongs to a different category of allergic reaction as it is not IgE mediated.
Seasonal Allergic Conjunctivitis and Perineal Allergic ConjunctivitisSAC is the most common form of all ocular allergic diseases and is triggered by exposure to pollen. It usually occurs in spring. PAC is induced by exposure to dust mites fungi, animal epithelial and/or occupational allergens. The affected patients can show symptoms throughout the year with acute seasonal exacerbations.
Pathophysiology
The response to allergen in allergic conjunctivitis is due to its interaction with prostaglandins and leukotrienes. It is a type I hypersensitivity reaction and the early response lasts clinically for 20 -30 minutes. The late phase reaction is due to the presence of inflammatory cells in the conjunctival mucosa. This is brought about by activation of vascular endothelial cells, which in turn expresses chemokines, adhesion molecules such as such as intercellular adhesion molecule (ICAM) and vascular cell adhesion molecule (VCAM). Other chemokines secreted include regulated upon activation normal T cell expressed and secreted (RANTES) chemokines, monocyte chemo attractant protein (MCP), interleukin (IL)-8, eotaxin and macrophage inflammatory protein (MIP)-1 alpha.
Clinical features
The clinical presentation in both the conditions is similar. Patients complains of bilateral itching, tearing and burning sensation. Blurred vision and photophobia may be due to an alteration in the composition and instability of the tear film. PAC affects young adults between 20-40 years of age with no gender predilection while SAC has no age or gender predilection. Both are frequently associated with allergic rhinitis and other allergic disorder (slightly more with SAC). On examination, mild to moderate conjunctival hyperemia with an edematous conjunctival surface is seen. The palpebral conjunctiva appears pale pink in color with diffuse areas of slightly hypertrophic papillae predominantly located in the upper tarsal conjunctiva (Figure-1a,b). The cornea is rarely affected.
Diagnosis: Diagnostic features of SAC and PAC consist of itching, redness, and swelling of the conjunctiva. However other criterias that help in the diagnosis are a family

42 l DOS Times - Vol. 19, No. 4 October, 2013
Ocular Surface Disorder
or personal history of atopy and skin test, response to antiallergic treatment, serum IgE elevation (found in 78% of all patients with SAC–69% being specific of pollen), lacrimal IgE elevation (in 96% of the patients), increased mast cell infiltration of the conjunctiva (in 61% of the cases) and increase in type T mast cells with tryptase release in tears.
Vernal keratoconjunctivitisVKC is a self-limiting, bilateral chronic inflammation that leaves sequelae or permanent alterations in visual acuity in about 5-6% of the patients. It is more frequent in young males with an increased incidence between 11-13 years of age. VKC is rare in adults.
Pathophysiology is not precisely known, though two hypersensitivity mechanisms seem to be involved (type I and type IV). Accordingly, in the presence of an antigen, lymphocyte activation (predominantly of the
Th2 subpopulation) would take place. There is abundant mucosal secretion in these individuals due to increased presence of goblet cells in the conjunctiva.
Clinical features
The disease presents with itching, redness, photophobia and watering. The symptoms may be seasonal or perennial with exacerbations in heat, dust, wind, bright light. Two forms of conjunctival involvement is known: palpebral, with giant subtarsal papillae (>1 mm in diameter) showing a typical cobblestone pattern with profuse mucus secretion (Figure 2) and limbal with Horner-Trantas dots that appear as small gelatinous nodules at limbus and are typical of the active phase of the disease (Figure 3).
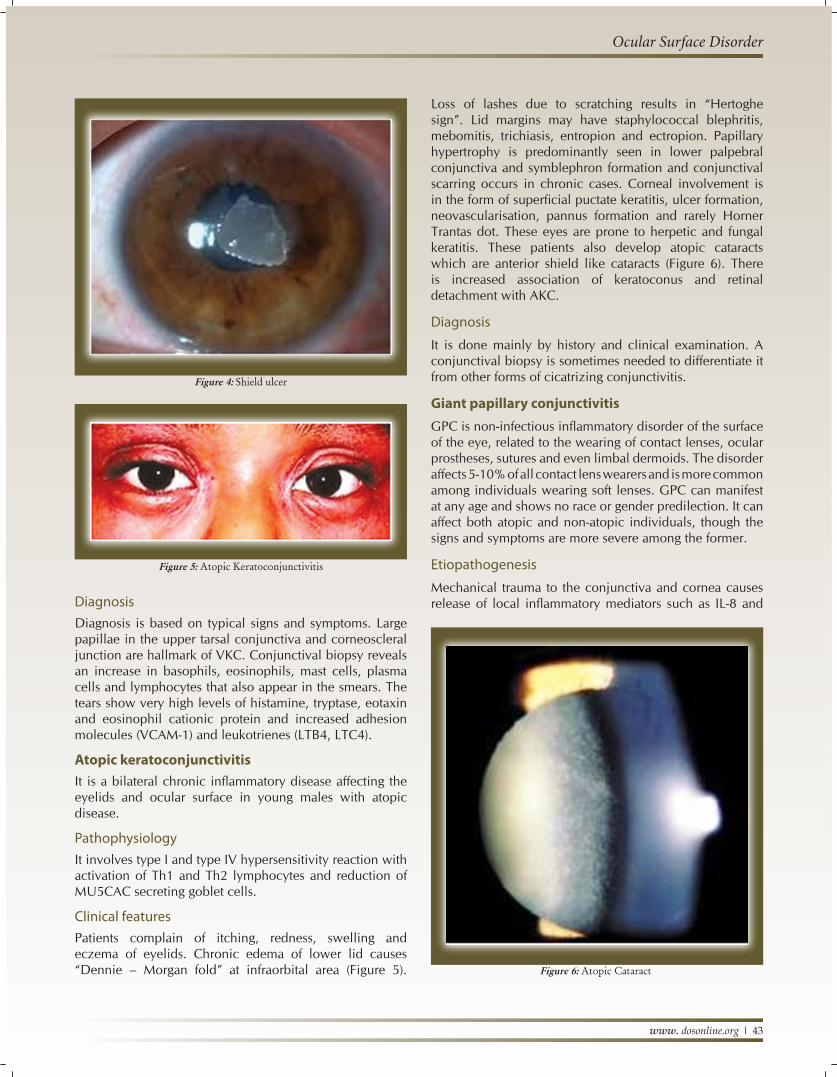
Corneal involvement can manifest as a micropannus superficial punctate keratopathy (normally located in the upper half of the cornea), corneal macro erosions and shield ulcerations (occurs in 3%-11% of cases) covered with mucus and fibrin plaques (Figure 4), subepithelial scarring and pseudogerontoxon. VKC is strongly associated with keratoconus, hydrops and may cause dry eye.
Figure 1a: Conjunctival hyperemia and edema
Figure 1(b): Papillary hypertrophy
Figure 2: Giant papillary hypertrophy
Figure 3: Horner Trantas dots
www. dosonline.org l 43
Ocular Surface Disorder
DiagnosisDiagnosis is based on typical signs and symptoms. Large papillae in the upper tarsal conjunctiva and corneoscleral junction are hallmark of VKC. Conjunctival biopsy reveals an increase in basophils, eosinophils, mast cells, plasma cells and lymphocytes that also appear in the smears. The tears show very high levels of histamine, tryptase, eotaxin and eosinophil cationic protein and increased adhesion molecules (VCAM-1) and leukotrienes (LTB4, LTC4).
Atopic keratoconjunctivitisIt is a bilateral chronic inflammatory disease affecting the eyelids and ocular surface in young males with atopic disease.
PathophysiologyIt involves type I and type IV hypersensitivity reaction with activation of Th1 and Th2 lymphocytes and reduction of MU5CAC secreting goblet cells.
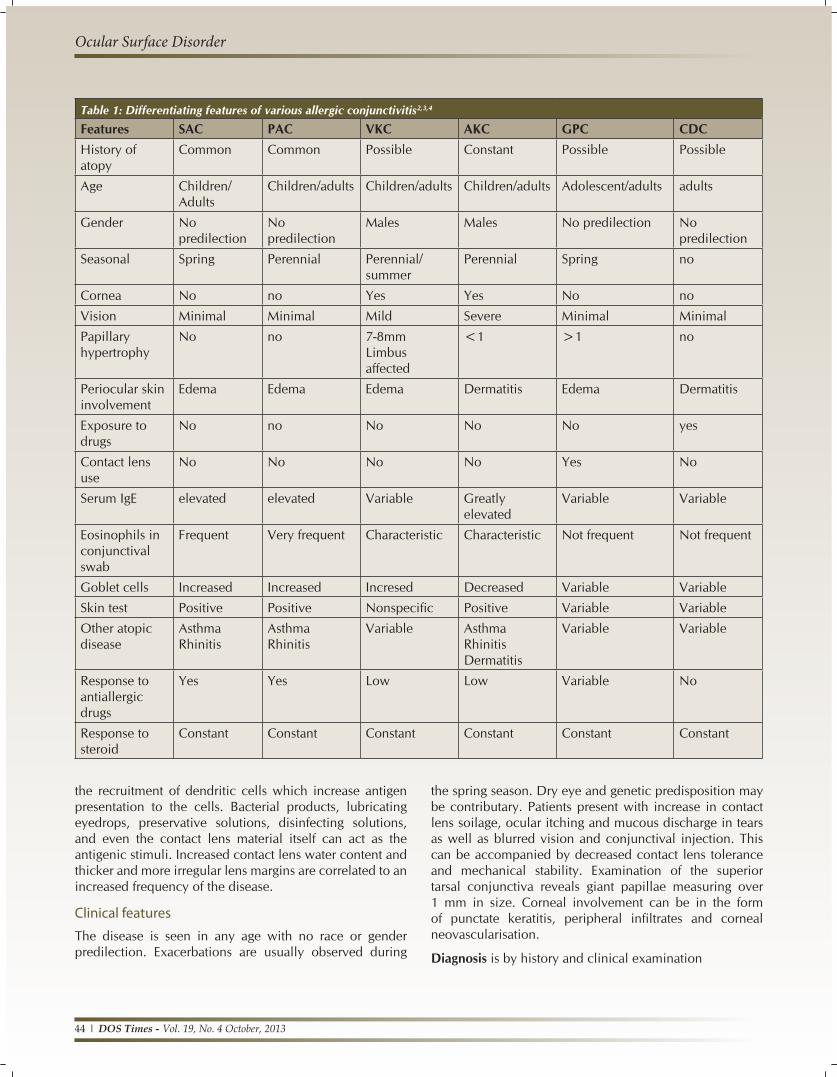
Clinical featuresPatients complain of itching, redness, swelling and eczema of eyelids. Chronic edema of lower lid causes “Dennie – Morgan fold” at infraorbital area (Figure 5).
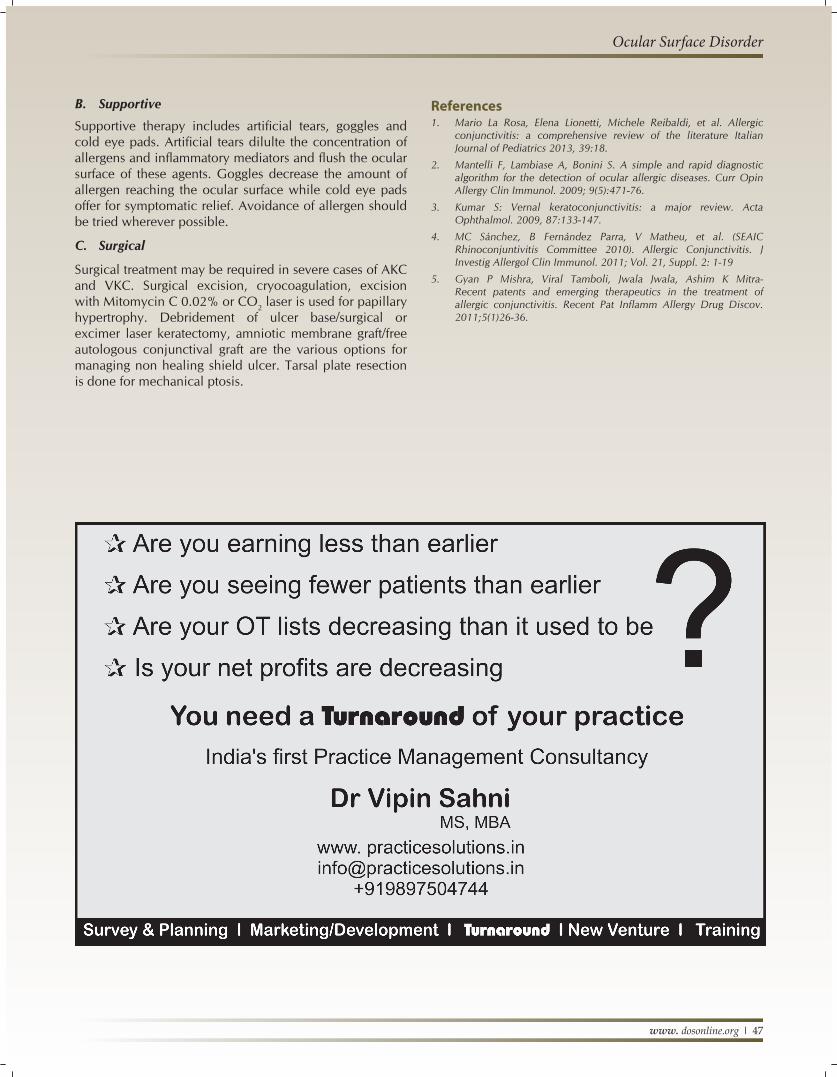
Loss of lashes due to scratching results in “Hertoghe sign”. Lid margins may have staphylococcal blephritis, mebomitis, trichiasis, entropion and ectropion. Papillary hypertrophy is predominantly seen in lower palpebral conjunctiva and symblephron formation and conjunctival scarring occurs in chronic cases. Corneal involvement is in the form of superficial puctate keratitis, ulcer formation, neovascularisation, pannus formation and rarely Horner Trantas dot. These eyes are prone to herpetic and fungal keratitis. These patients also develop atopic cataracts which are anterior shield like cataracts (Figure 6). There is increased association of keratoconus and retinal detachment with AKC.
Diagnosis
It is done mainly by history and clinical examination. A conjunctival biopsy is sometimes needed to differentiate it from other forms of cicatrizing conjunctivitis.
Giant papillary conjunctivitisGPC is non-infectious inflammatory disorder of the surface of the eye, related to the wearing of contact lenses, ocular prostheses, sutures and even limbal dermoids. The disorder affects 5-10% of all contact lens wearers and is more common among individuals wearing soft lenses. GPC can manifest at any age and shows no race or gender predilection. It can affect both atopic and non-atopic individuals, though the signs and symptoms are more severe among the former.
Etiopathogenesis
Mechanical trauma to the conjunctiva and cornea causes release of local inflammatory mediators such as IL-8 and
Figure 4: Shield ulcer
Figure 5: Atopic Keratoconjunctivitis
Figure 6: Atopic Cataract
44 l DOS Times - Vol. 19, No. 4 October, 2013
Ocular Surface Disorder
Table 1: Differentiating features of various allergic conjunctivitis2,3,4
Features SAC PAC VKC AKC GPC CDCHistory of atopy
Common Common Possible Constant Possible Possible
Age Children/Adults
Children/adults Children/adults Children/adults Adolescent/adults adults
Gender No predilection
No predilection
Males Males No predilection No predilection
Seasonal Spring Perennial Perennial/summer
Perennial Spring no
Cornea No no Yes Yes No no
Vision Minimal Minimal Mild Severe Minimal Minimal
Papillary hypertrophy
No no 7-8mmLimbus affected
<1 >1 no
Periocular skin involvement
Edema Edema Edema Dermatitis Edema Dermatitis
Exposure to drugs
No no No No No yes
Contact lens use
No No No No Yes No
Serum IgE elevated elevated Variable Greatly elevated
Variable Variable
Eosinophils in conjunctival swab
Frequent Very frequent Characteristic Characteristic Not frequent Not frequent
Goblet cells Increased Increased Incresed Decreased Variable Variable
Skin test Positive Positive Nonspecific Positive Variable Variable
Other atopic disease
Asthma Rhinitis
Asthma Rhinitis
Variable Asthma Rhinitis Dermatitis
Variable Variable
Response to antiallergic drugs
Yes Yes Low Low Variable No
Response to steroid
Constant Constant Constant Constant Constant Constant
the recruitment of dendritic cells which increase antigen presentation to the cells. Bacterial products, lubricating eyedrops, preservative solutions, disinfecting solutions, and even the contact lens material itself can act as the antigenic stimuli. Increased contact lens water content and thicker and more irregular lens margins are correlated to an increased frequency of the disease.
Clinical features
The disease is seen in any age with no race or gender predilection. Exacerbations are usually observed during
the spring season. Dry eye and genetic predisposition may be contributary. Patients present with increase in contact lens soilage, ocular itching and mucous discharge in tears as well as blurred vision and conjunctival injection. This can be accompanied by decreased contact lens tolerance and mechanical stability. Examination of the superior tarsal conjunctiva reveals giant papillae measuring over 1 mm in size. Corneal involvement can be in the form of punctate keratitis, peripheral infiltrates and corneal neovascularisation.
Diagnosis is by history and clinical examination

www. dosonline.org l 45
Ocular Surface Disorder
Table 2: Drugs used in allergic diseases of the eye
Name Mode of action Effect Examples Indication Dosage Adverse effectAntihistamines Blocks the action
of histamine by blocking the histamine receptors
Relieves itching and redness
Antazoline, Pheniramine, Levocabastine (0.5%)
PAC, SAC Tds to qid
Irritation especially on prolonged use
Vasoconstrictor Constricts blood vessels
Decongestion Oxymetazoline, Naphazoline, Tetrahy-drozoline, Phenylephrine
PAC, SAC Tds Burning, stinging, mydriasis, rebound hyperemia conjunctivitis medicamentosa with chronic use
Mast cell stabiliser
Influx of calcium into mast cell decreases degranulation which decrease the release of histamine and chemotactic factors
Used for prophylaxis
Sodium cromoglycate, Lodoxamine
PAC, SAC Tds Require loading period before exposure to antigen hence requires very good compliance
Multiple action drugs
Exert multiple pharmacological effects such as histamine receptor antagonist action, stabilization of mast cell degranulation and suppression of activation and infiltration of eosinophils
Relieves itching, redness, edema with immediate effect
Olopatadine (0.1%) Ketotifen (0.025%),Nedocromil,Azelastine,Epinastine (0.05%)
PAC, SAC, VKC, AKC,
Bd Blurred vision, burning and stinging
NSAID (non steroidal anti inflammatory drugs)
Block cyclooxygenese pathway, reduces prostaglandin and thromboxane synthesis
Reduce the conjunctival hyperemia and the pruritus caused by lukotrienes and prostaglandins
Ketorolac (0.5%), Pranoprofen, Fluribuprofen,Diclofenac (0.1%)
SAC, VKC Tds Burning and stinging
Corticosteroids Interfere with intracellular protein synthesis and block phospholipase A2. They also inhibit cytokine production and inflammatory cell migration
Used in severe and chronic forms, relieves all signs and symptoms.
Medroxy-progesterone, Fluormetholone, Dexamethasone (0.1%),Prednisolone (1%),Clobetasone, Rimexolone, Loteprednol, (.02% & .05%), Subtenons injection of triamcinalone acetonide
Severe forms of all allergic conjunc-tivitis for short duration
Tds Cataract, glaucoma, infections, delayed wound healing
contd...

46 l DOS Times - Vol. 19, No. 4 October, 2013
Ocular Surface Disorder
Contact dermatitis allergyIt is a type IV mediated hypersensitivity response that involves interaction of antigen with Th1 and Th2 cells resulting in release of cytokines.
Pathophysiology
Typically, it consists of two phases: sensitization and inflammatory response. In the sensitization phase antigen presenting cells processed antigen - MHC class II complex interacts with T-lymphocytes, resulting in the differentiation of CD4+ T-lymphocyte into memory T-lymphocyte. In the second phase, the interaction between the antigen-MHC-II complex and memory T-cells stimulates the proliferation of T-cells. The memory T-lymphocytes during proliferation release cytokines. In sensitized individuals, the immune response takes 48-72 hours to develop. Some of the products that can act as antigens are: mydriatic drugs (atropine, homatropine, tropicamide, phenyephrine); antiglaucoma drugs (Brimonidine, apraclonidine dorzolamide); preservatives (thiomersal, benzalkoniumchloride, chlorhexidine EDTA); antibiotics (aminoglycosides, sulfamides, polymyxin); antiviral drugs (idoxuridine, trifuridine, viderabine); anaesthetic agents (procaine, tetracaine); cosmetics, soaps and detergents.
Clinical features
The lower palpebral conjunctiva is involved first followed by rest of the conjunctiva. The eyelids may show blephritis, eczematous dermatitis which later resulting in folds, crusts, fissures, and skin thickening (Figure 7). The conjunctiva shows follicles, papillae, psedopemphigoid lesions. Corneal involvement may be in the form of superficial punctuate keratitis, marginal infiltrate, ulcer and stromal edema.
Diagnosis is by history and clinical examination
Differentiating features of various types of allergic conjunctivitis in the form of epidemiology, history, clinical features and response to treatment are summarised in (Table 1) (adapted from Mantelli et al.)
Treatment of allergic conjunctivitisA. Medical5
The mainstay of treatment is anti allergic drugs. These include antihistamine, vasoconstrictors, mast cell stabilisers, dual mode action drugs, corticosteroids and immunosuppressives. The regimen that is usually followed is as follows: In mild cases, antihistamines or vasoconstrictors suffice. In moderate cases, NSAID is added along with dual action drugs. In severe cases, steroid drop are given for a short duration of upto 2 weeks followed by dual action drugs. Duration of treatment depends on patients response and the nature of the allergy. Mast cell stabilisers are given prior to the onset of symptoms in susceptible cases. Cyclosporins and tacrolimus is used in severe cases of VKC and AKC. Allergen-specific immunotherapy is an effective treatment for patients with allergic rhinoconjunctivitis. The drugs, their mechanism of action, dosage and adverse effects used in various allergic conjunctivitis are summarised in table 2
Figure 7: Contact Dermatitis Conjunctivitis
Name Mode of action Effect Examples Indication Dosage Adverse effectImmuno-supressives
Cyclosporine inhibits eosinophil infiltration by affecting type IV hypersensitivity reaction. Tacrolimus acts by inhibiting the action of T-cells.
Decreases steroid dosage and tacrolimus is useful in steroid resistant cases
Cyclosporins (1%; 2%), Tacrolimus (0.003%)
AKC, VKC Tds Burning, ocular pain
Oral antihistamines
These block H1 receptors some have anti-inflammatory properties by inhibiting ICAM1 and PGF.
Reduces itching,edema vasodilatation in severe allergic conjunctivitis.
Cetirizine, Loratadine, Ebastine, Levocetirizine, Fexofenadine
Severe allergic conditions
Od;bd Dry eye especially with second generation antihistamines.
Od: Once a day; Bd: two time a day; Tds: Three time a day; qid: four time a day
www. dosonline.org l 47
Ocular Surface Disorder
B. Supportive
Supportive therapy includes artificial tears, goggles and cold eye pads. Artificial tears dilulte the concentration of allergens and inflammatory mediators and flush the ocular surface of these agents. Goggles decrease the amount of allergen reaching the ocular surface while cold eye pads offer for symptomatic relief. Avoidance of allergen should be tried wherever possible.
C. Surgical
Surgical treatment may be required in severe cases of AKC and VKC. Surgical excision, cryocoagulation, excision with Mitomycin C 0.02% or CO2 laser is used for papillary hypertrophy. Debridement of ulcer base/surgical or excimer laser keratectomy, amniotic membrane graft/free autologous conjunctival graft are the various options for managing non healing shield ulcer. Tarsal plate resection is done for mechanical ptosis.
References1. Mario La Rosa, Elena Lionetti, Michele Reibaldi, et al. Allergic
conjunctivitis: a comprehensive review of the literature Italian Journal of Pediatrics 2013, 39:18.
2. Mantelli F, Lambiase A, Bonini S. A simple and rapid diagnostic algorithm for the detection of ocular allergic diseases. Curr Opin Allergy Clin Immunol. 2009; 9(5):471-76.
3. Kumar S: Vernal keratoconjunctivitis: a major review. Acta Ophthalmol. 2009, 87:133-147.
4. MC Sánchez, B Fernández Parra, V Matheu, et al. (SEAIC Rhinoconjuntivitis Committee 2010). Allergic Conjunctivitis. J Investig Allergol Clin Immunol. 2011; Vol. 21, Suppl. 2: 1-19
5. Gyan P Mishra, Viral Tamboli, Jwala Jwala, Ashim K Mitra- Recent patents and emerging therapeutics in the treatment of allergic conjunctivitis. Recent Pat Inflamm Allergy Drug Discov.2011;5(1)26-36.


















