Ocular Parasitic Diseases: A Review on Toxocariasis … · Ocular Parasitic Diseases: A Review on...
9
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX Review Article From Centro de Cirugía Oftalmológica (RTC, GR, LC), Caracas, Venezuela; and Princess Margaret Hospital (GPG), University of Toronto, Toronto, Ontario, Canada. Originally submitted January 4, 2010. Accepted for publication May 3, 2010. The authors have no financial or proprietary interest in the materials presented herein. Address correspondence to Gian Paolo Giuliari, MD, 77 Elm Street, Apt. 903, Toronto, Ontario M5G H14, Canada. E-mail: [email protected] doi: 10.3928/01913913-20100719-02 Ocular Parasitic Diseases: A Review on Toxocariasis and Diffuse Unilateral Subacute Neuroretinitis Rafael T. Cortez, MD; Gema Ramirez, MD; Lucienne Collet, MD; Gian Paolo Giuliari, MD ABSTRACT Parasitic infections may damage various ocular tissues, thereby causing visual dysfunction. In 1950, Wilder de- scribed the first case in which larval forms of nematodal intestinal roundworms (Ascaridoidea: Ascaris, Toxocara, Ancylostoma, Necator, and Strongyloides) were impli- cated as a cause of intraocular disease. This review fo- cuses on two disorders associated with parasitic infec- tions: ocular toxocariasis and diffuse unilateral subacute neuroretinitis. [J Pediatr Ophthalmol Strabismus 20XX;XX:XX-XX.] INTRODUCTION Parasitic infections may produce severe dam- age to various ocular tissues, thereby causing visual dysfunction. In this review, we will focus on two of these infections, ocular toxocariasis and diffuse uni- lateral subacute neuroretinitis (DUSN). Although these diseases are not widely distributed worldwide, we believe it is of great value to the general ophthal- mologist to be familiar with their different presenta- tions, due to the poor visual prognosis they carry. OCULAR TOXOCARIASIS Human infection by Toxocara, a common roundworm that infects dogs and cats, may take one of two forms: visceral larva migrans and ocular toxo- cariasis. 1-5 The characteristics of the infection will depend on the number of parasites, site of infection, migratory behavior, and the host immunological re- sponse. 6,7 Visceral larva migrans is characterized by gen- eralized systemic involvement due to the migration capabilities of the second stage larvae of Toxocara canis. It typically presents in children from the ages of 6 months to 5 years. The disease is usually self- limited and subclinical; however, fever, pulmonary manifestations, hepatomegaly, eosinophilia, pallor, irritability, anorexia, and malaise can occur. 6,7 On the other hand, ocular toxocariasis appears in older patients, with an average age of 7.5 to 8.6 years. 7-9 Several studies have revealed Toxocara and other visceral larvae migrans to be the cause of intra- ocular inflammation in 9.4% of pediatric uveitis. 10,11 Rarely does a patient present with both visceral larva migrans and ocular toxoplasmosis at the same time or even at separate intervals. 3,6,12 Epidemiology and Life Cycle of T. canis The adult dog usually acquires the T. canis parasite by ingesting the parasite’s eggs or second stage larvae found in contaminated soil, infected meat, and feces. The larvae form cysts and reactivation of the larvae during gestation can infect the fetal puppies in the uterus. Following birth, the larvae migrate to the pup- pies’ lungs and then travel up the respiratory tract to the pharynx, where they are swallowed. They then ma- ture to become egg-laying adult worms in the gastroin- testinal tract. Approximately 4 weeks after their birth,
-
Upload
vuongthien -
Category
Documents
-
view
221 -
download
2
Transcript of Ocular Parasitic Diseases: A Review on Toxocariasis … · Ocular Parasitic Diseases: A Review on...
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX �
Review Article
From Centro de Cirugía Oftalmológica (RTC, GR, LC), Caracas, Venezuela; and Princess Margaret Hospital (GPG), University of Toronto, Toronto, Ontario, Canada.
Originally submitted January 4, 2010. Accepted for publication May 3, 2010.The authors have no financial or proprietary interest in the materials presented herein. Address correspondence to Gian Paolo Giuliari, MD, 77 Elm Street, Apt. 903, Toronto, Ontario M5G H14, Canada. E-mail: [email protected]: 10.3928/01913913-20100719-02
Ocular Parasitic Diseases: A Review on Toxocariasis and Diffuse Unilateral Subacute Neuroretinitis
Rafael T. Cortez, MD; Gema Ramirez, MD; Lucienne Collet, MD; Gian Paolo Giuliari, MD
ABSTRACTParasitic infections may damage various ocular tissues, thereby causing visual dysfunction. In 1950, Wilder de-scribed the first case in which larval forms of nematodal intestinal roundworms (Ascaridoidea: Ascaris, Toxocara, Ancylostoma, Necator, and Strongyloides) were impli-cated as a cause of intraocular disease. This review fo-cuses on two disorders associated with parasitic infec-tions: ocular toxocariasis and diffuse unilateral subacute neuroretinitis. [J Pediatr Ophthalmol Strabismus 20XX;XX:XX-XX.]
INTRODUCTIONParasitic infections may produce severe dam-
age to various ocular tissues, thereby causing visual dysfunction. In this review, we will focus on two of these infections, ocular toxocariasis and diffuse uni-lateral subacute neuroretinitis (DUSN). Although these diseases are not widely distributed worldwide, we believe it is of great value to the general ophthal-mologist to be familiar with their different presenta-tions, due to the poor visual prognosis they carry.
OCULAR TOXOCARIASISHuman infection by Toxocara, a common
roundworm that infects dogs and cats, may take one of two forms: visceral larva migrans and ocular toxo-cariasis.1-5 The characteristics of the infection will depend on the number of parasites, site of infection,
migratory behavior, and the host immunological re-sponse.6,7
Visceral larva migrans is characterized by gen-eralized systemic involvement due to the migration capabilities of the second stage larvae of Toxocara canis. It typically presents in children from the ages of 6 months to 5 years. The disease is usually self-limited and subclinical; however, fever, pulmonary manifestations, hepatomegaly, eosinophilia, pallor, irritability, anorexia, and malaise can occur.6,7
On the other hand, ocular toxocariasis appears in older patients, with an average age of 7.5 to 8.6 years.7-9 Several studies have revealed Toxocara and other visceral larvae migrans to be the cause of intra-ocular inflammation in 9.4% of pediatric uveitis.10,11 Rarely does a patient present with both visceral larva migrans and ocular toxoplasmosis at the same time or even at separate intervals.3,6,12
Epidemiology and Life Cycle of T. canisThe adult dog usually acquires the T. canis parasite
by ingesting the parasite’s eggs or second stage larvae found in contaminated soil, infected meat, and feces. The larvae form cysts and reactivation of the larvae during gestation can infect the fetal puppies in the uterus. Following birth, the larvae migrate to the pup-pies’ lungs and then travel up the respiratory tract to the pharynx, where they are swallowed. They then ma-ture to become egg-laying adult worms in the gastroin-testinal tract. Approximately 4 weeks after their birth,
� Copyright © SLACK Incorporated
worms begin laying eggs. Older dogs can harbor adult worms that do not lay eggs.13 Toxocara eggs are found in the soil throughout tropical and temperate climate regions. In the United States and Western Europe, soil from parks and public areas has been found to carry a contamination rate of 10% to 30%.14 In Venezuela, a 33% contamination rate was found in a metropolitan area.
Humans are primarily infected through the in-gestion of soil and food contaminated with Toxocara larvae. After the eggs are ingested, they develop into second stage larvae in the small intestine. They then enter the portal circulation, following hematog-enous and lymphatic routes to form cysts in tissue structures.15 The parasites reach the eye through the retinal, ciliary, and choroidal circulation. Humans are not natural hosts of Toxocara, and the parasite cannot mature into an adult worm in the intes-tine.13
Clinical PresentationOcular toxocariasis is typically unilateral. Pa-
tients present with unilateral decrease in visual acu-ity, strabismus, or leukocoria.14,16 Cases with bilateral involvement are extremely rare.17 Younger children generally do not report visual changes, even if visual acuity is profoundly decreased, and it is common that parents may seek medical attention only when the signs become striking. As such, diminished visu-al acuity is frequently detected in routine examina-tion.14,16 Impairment of visual acuity and leukocoria are the most common presenting manifestations.
Several ocular presentations have been recognized, the most common of which is granulomatous inflam-mation in the posterior pole or periphery.14,18-20 Some patients may present with a more marked chronic in-flammation in the retina and the vitreous known as nematode endophthalmitis.5,14
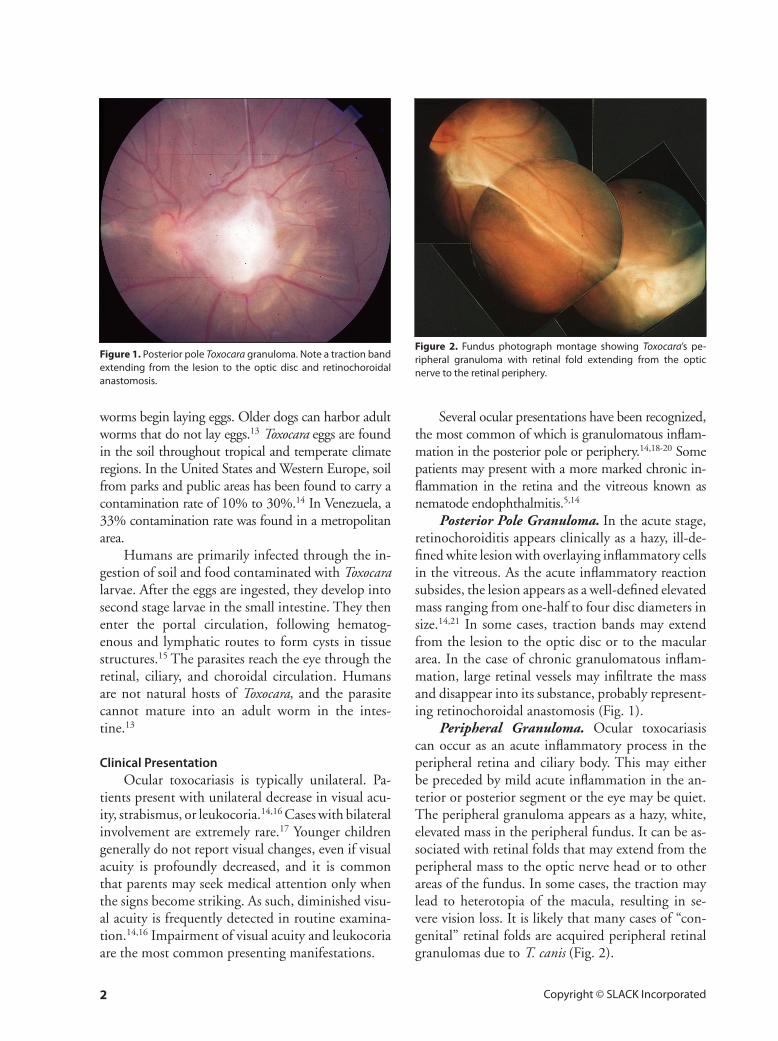
Posterior Pole Granuloma. In the acute stage, retinochoroiditis appears clinically as a hazy, ill-de-fined white lesion with overlaying inflammatory cells in the vitreous. As the acute inflammatory reaction subsides, the lesion appears as a well-defined elevated mass ranging from one-half to four disc diameters in size.14,21 In some cases, traction bands may extend from the lesion to the optic disc or to the macular area. In the case of chronic granulomatous inflam-mation, large retinal vessels may infiltrate the mass and disappear into its substance, probably represent-ing retinochoroidal anastomosis (Fig. 1).
Peripheral Granuloma. Ocular toxocariasis can occur as an acute inflammatory process in the peripheral retina and ciliary body. This may either be preceded by mild acute inflammation in the an-terior or posterior segment or the eye may be quiet. The peripheral granuloma appears as a hazy, white, elevated mass in the peripheral fundus. It can be as-sociated with retinal folds that may extend from the peripheral mass to the optic nerve head or to other areas of the fundus. In some cases, the traction may lead to heterotopia of the macula, resulting in se-vere vision loss. It is likely that many cases of “con-genital” retinal folds are acquired peripheral retinal granulomas due to T. canis (Fig. 2).
Figure �. Posterior pole Toxocara granuloma. Note a traction band extending from the lesion to the optic disc and retinochoroidal anastomosis.
Figure �. Fundus photograph montage showing Toxocara’s pe-ripheral granuloma with retinal fold extending from the optic nerve to the retinal periphery.
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX �
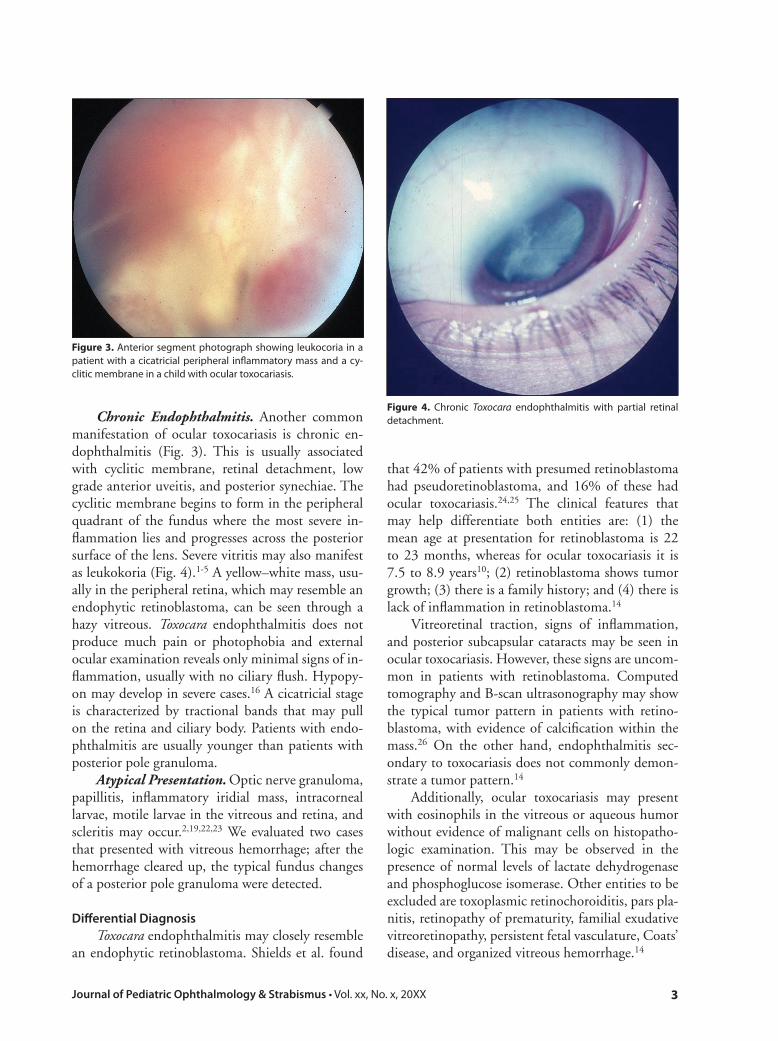
Chronic Endophthalmitis. Another common manifestation of ocular toxocariasis is chronic en-dophthalmitis (Fig. 3). This is usually associated with cyclitic membrane, retinal detachment, low grade anterior uveitis, and posterior synechiae. The cyclitic membrane begins to form in the peripheral quadrant of the fundus where the most severe in-flammation lies and progresses across the posterior surface of the lens. Severe vitritis may also manifest as leukokoria (Fig. 4).1-5 A yellow–white mass, usu-ally in the peripheral retina, which may resemble an endophytic retinoblastoma, can be seen through a hazy vitreous. Toxocara endophthalmitis does not produce much pain or photophobia and external ocular examination reveals only minimal signs of in-flammation, usually with no ciliary flush. Hypopy-on may develop in severe cases.16 A cicatricial stage is characterized by tractional bands that may pull on the retina and ciliary body. Patients with endo-phthalmitis are usually younger than patients with posterior pole granuloma.
Atypical Presentation. Optic nerve granuloma, papillitis, inflammatory iridial mass, intracorneal larvae, motile larvae in the vitreous and retina, and scleritis may occur.2,19,22,23 We evaluated two cases that presented with vitreous hemorrhage; after the hemorrhage cleared up, the typical fundus changes of a posterior pole granuloma were detected.
Differential DiagnosisToxocara endophthalmitis may closely resemble
an endophytic retinoblastoma. Shields et al. found
that 42% of patients with presumed retinoblastoma had pseudoretinoblastoma, and 16% of these had ocular toxocariasis.24,25 The clinical features that may help differentiate both entities are: (1) the mean age at presentation for retinoblastoma is 22 to 23 months, whereas for ocular toxocariasis it is 7.5 to 8.9 years10; (2) retinoblastoma shows tumor growth; (3) there is a family history; and (4) there is lack of inflammation in retinoblastoma.14
Vitreoretinal traction, signs of inflammation, and posterior subcapsular cataracts may be seen in ocular toxocariasis. However, these signs are uncom-mon in patients with retinoblastoma. Computed tomography and B-scan ultrasonography may show the typical tumor pattern in patients with retino-blastoma, with evidence of calcification within the mass.26 On the other hand, endophthalmitis sec-ondary to toxocariasis does not commonly demon-strate a tumor pattern.14
Additionally, ocular toxocariasis may present with eosinophils in the vitreous or aqueous humor without evidence of malignant cells on histopatho-logic examination. This may be observed in the presence of normal levels of lactate dehydrogenase and phosphoglucose isomerase. Other entities to be excluded are toxoplasmic retinochoroiditis, pars pla-nitis, retinopathy of prematurity, familial exudative vitreoretinopathy, persistent fetal vasculature, Coats’ disease, and organized vitreous hemorrhage.14
Figure �. Anterior segment photograph showing leukocoria in a patient with a cicatricial peripheral inflammatory mass and a cy-clitic membrane in a child with ocular toxocariasis.
Figure 4. Chronic Toxocara endophthalmitis with partial retinal detachment.

4 Copyright © SLACK Incorporated
DiagnosisThe current gold standard to test for systemic or
ocular infection with T. canis is the enzyme-linked immunosorbent assay (ELISA), which carries both a sensitivity and specificity rate of approximately 90%.14 Although the Centers for Disease Control and Prevention considers serum ELISA titers of less than 1:32 to be insignificant for the diagnosis of systemic toxocariasis, other institutions have stated that a serum titer of 1:8, or even lower, is sufficient to support the diagnosis if the patient has signs and symptoms compatible with the disease.14,18,27 How-ever, a positive serum titer cannot be used to defini-tively confirm the diagnosis of ocular toxocariasis, although the absence of serologic evidence of Toxo-cara presence could reduce the odds of this organ-ism being the cause of ocular disease.14,18 Authors have found that 31.8% of affected children without signs of ocular toxocariasis exhibited a serum titer of 1:16 or greater.14,18 ELISA testing of intraocular fluids has been demonstrated to be of great value in diagnosing ocular toxocariasis.10,14,18,19,28
TreatmentThe treatment of ocular toxocariasis depends pri-
marily on the extent of inflammation at presentation and the secondary structural changes in the vitreous and retina that are associated with the disease.14 In most cases of severe nematode endophthalmitis, nu-merous complications ensue that frequently result in total blindness in the involved eye. Therefore, prompt treatment is justified in such cases.14
Medical Treatment. With ocular toxocariasis, the objective of treatment is to reduce inflamma-tion to prevent the formation of membranes that can consequently affect intraocular structures. Periocular and systemic steroids (0.5 to 1 mg/kg prednisone daily) are the mainstays of therapy for eyes with active vitritis. Cycloplegic agents should be employed when signs of anterior segment in-volvement are present.14 There have been reports of clinical improvements of ocular toxocariasis treated with antihelmintic agents thiabendazole (25 mg/kg twice daily for 5 days with a maximum of 3 g per day), albendazole (800 mg twice daily for 6 days), or mebendazole (100 to 200 mg twice daily for 5 days).14,29 Although it has been proposed that an-tihelmintic treatment may initiate an intraocular inflammation due to a hypersensitivity response to dead larvae, clinical and experimental evidence in-
dicate that this is not the case.20,30-32 The ultimate utility of antihelmintic therapy remains equivocal.
Surgical Treatment. Surgery is reserved for post-inflammatory complications such as persis-tent vitreous opacification, retinal detachment, and epiretinal membrane formation with vitreomacular or optic nerve traction (Fig. 5).The most common indication for surgical intervention in ocular toxo-cariasis is retinal detachment.27,30,31,33 Retinal reat-tachment has been performed in 71% to 88% of ocular toxocariasis cases, with visual improvement in most patients.27,30,31,33
DIFFUSE UNILATERAL SUBACUTE NEURORETINITIS
DUSN was first described by Gass et al.34 and Gass and Scelfo35 in 1978. They described 29 patients between the ages of 5 and 22 years with severe visual loss in one eye, vitritis, mild papillitis, and recurrent crops of evanescent, gray–white lesions affecting the outer retina and pigment epithelium. These lesions are usually followed by progressive loss of visual field, optic atrophy, narrowing of the major retinal vessels, diffuse and focal depigmentation of retinal pigment epithelium throughout the fundus, and a moderate to marked reduction of the b-wave amplitude on mul-tifocal electroretinogram. Previously, this condition was termed “unilateral wipe-out syndrome.”34,35
DUSN is most prevalent in the southeastern United States and the Caribbean, although some cases have been reported in many sections of the United States, Canada, the northern part of South America, Europe, and China.36-41
In the United States, DUSN is probably caused by at least two different nematodes. The smaller one, Ancylostoma caninum, measures between 400 and 1,000 µm in length and has a diameter of ap-proximately one-twentieth of its length.36-39 It is mainly found in the southeastern United States, the Caribbean, and the northern part of South Amer-ica.36-39 A larger nematode, Baylisascaris procyonis, 1,500 to 2,000 µm long, is responsible for DUSN in the northern-midwestern United States and in some parts of Brazil.34,38,42,43
Clinical ManifestationsOcular findings in DUSN have been well de-
scribed by Gass et al.34-39 Most patients are young and healthy, with ages ranging from 11 to 65 years (the mean age being 24 years) at the time of the ini-
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX �
tial presentation.39 For the most part, it is a unilat-eral condition; although uncommon, bilateral cases have been described.37,39,40
Many patients, particularly children, may be asymptomatic and visual loss is usually discovered on routine eye examination. Other patients may present with acute onset of multiple, and rapidly changing, central or paracentral scotomata, pho-topsias, or unilateral vision loss.34,35,44-46 In the
early stages, inflammation in the anterior segment is uncommon, although keratic precipitates and hypopyon were observed and reported in one pa-tient.34,35 Visual acuity may be reduced moderately if the condition is detected early, but it is usually markedly decreased at the time of presentation. The fundus changes, which are the most promi-nent feature of this syndrome, have been divided into early and late.34,35
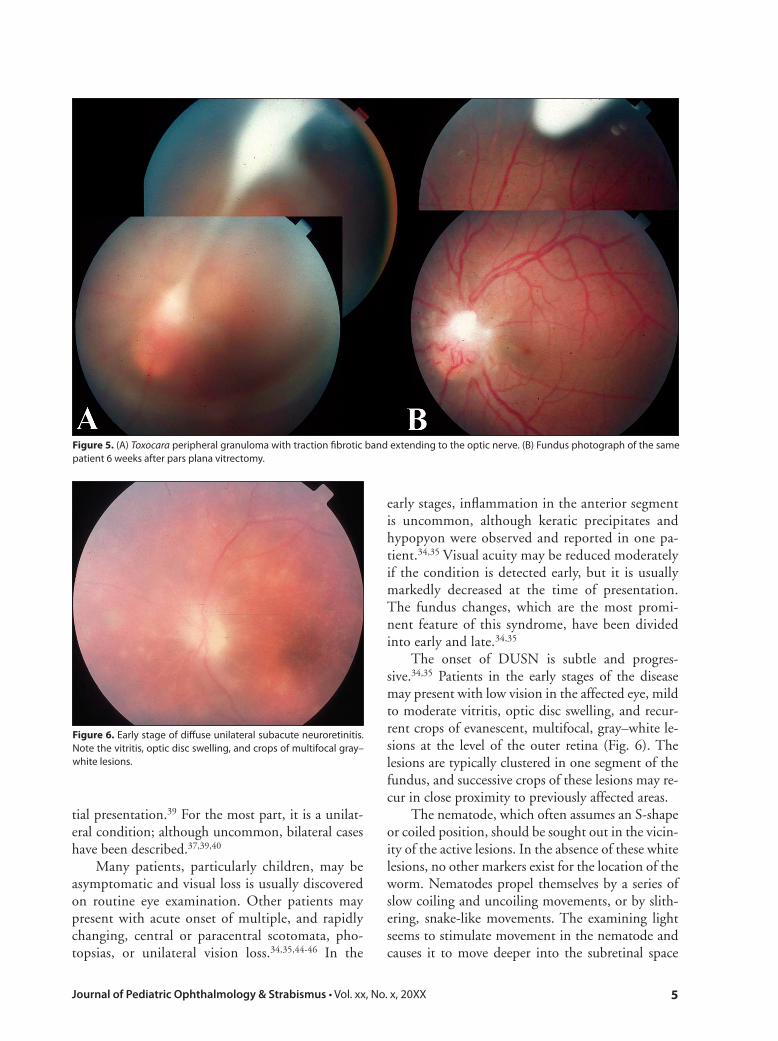
The onset of DUSN is subtle and progres-sive.34,35 Patients in the early stages of the disease may present with low vision in the affected eye, mild to moderate vitritis, optic disc swelling, and recur-rent crops of evanescent, multifocal, gray–white le-sions at the level of the outer retina (Fig. 6). The lesions are typically clustered in one segment of the fundus, and successive crops of these lesions may re-cur in close proximity to previously affected areas.
The nematode, which often assumes an S-shape or coiled position, should be sought out in the vicin-ity of the active lesions. In the absence of these white lesions, no other markers exist for the location of the worm. Nematodes propel themselves by a series of slow coiling and uncoiling movements, or by slith-ering, snake-like movements. The examining light seems to stimulate movement in the nematode and causes it to move deeper into the subretinal space
Figure �. (A) Toxocara peripheral granuloma with traction fibrotic band extending to the optic nerve. (B) Fundus photograph of the same patient 6 weeks after pars plana vitrectomy.
Figure 6. Early stage of diffuse unilateral subacute neuroretinitis. Note the vitritis, optic disc swelling, and crops of multifocal gray–white lesions.
6 Copyright © SLACK Incorporated
where the clinician may lose the opportunity to identify it. In such cases, the light stimulus should be discontinued for the organism to reemerge from the deeper structures.34-36,43,47
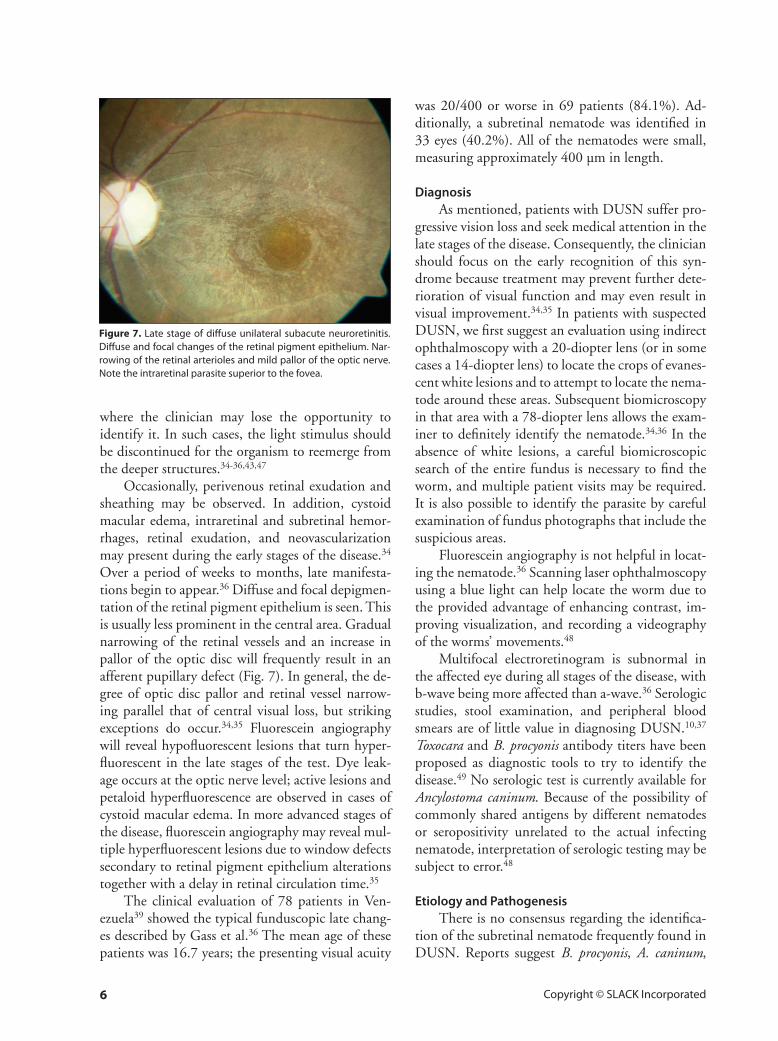
Occasionally, perivenous retinal exudation and sheathing may be observed. In addition, cystoid macular edema, intraretinal and subretinal hemor-rhages, retinal exudation, and neovascularization may present during the early stages of the disease.34 Over a period of weeks to months, late manifesta-tions begin to appear.36 Diffuse and focal depigmen-tation of the retinal pigment epithelium is seen. This is usually less prominent in the central area. Gradual narrowing of the retinal vessels and an increase in pallor of the optic disc will frequently result in an afferent pupillary defect (Fig. 7). In general, the de-gree of optic disc pallor and retinal vessel narrow-ing parallel that of central visual loss, but striking exceptions do occur.34,35 Fluorescein angiography will reveal hypofluorescent lesions that turn hyper-fluorescent in the late stages of the test. Dye leak-age occurs at the optic nerve level; active lesions and petaloid hyperfluorescence are observed in cases of cystoid macular edema. In more advanced stages of the disease, fluorescein angiography may reveal mul-tiple hyperfluorescent lesions due to window defects secondary to retinal pigment epithelium alterations together with a delay in retinal circulation time.35
The clinical evaluation of 78 patients in Ven-ezuela39 showed the typical funduscopic late chang-es described by Gass et al.36 The mean age of these patients was 16.7 years; the presenting visual acuity
was 20/400 or worse in 69 patients (84.1%). Ad-ditionally, a subretinal nematode was identified in 33 eyes (40.2%). All of the nematodes were small, measuring approximately 400 µm in length.
DiagnosisAs mentioned, patients with DUSN suffer pro-
gressive vision loss and seek medical attention in the late stages of the disease. Consequently, the clinician should focus on the early recognition of this syn-drome because treatment may prevent further dete-rioration of visual function and may even result in visual improvement.34,35 In patients with suspected DUSN, we first suggest an evaluation using indirect ophthalmoscopy with a 20-diopter lens (or in some cases a 14-diopter lens) to locate the crops of evanes-cent white lesions and to attempt to locate the nema-tode around these areas. Subsequent biomicroscopy in that area with a 78-diopter lens allows the exam-iner to definitely identify the nematode.34,36 In the absence of white lesions, a careful biomicroscopic search of the entire fundus is necessary to find the worm, and multiple patient visits may be required. It is also possible to identify the parasite by careful examination of fundus photographs that include the suspicious areas.
Fluorescein angiography is not helpful in locat-ing the nematode.36 Scanning laser ophthalmoscopy using a blue light can help locate the worm due to the provided advantage of enhancing contrast, im-proving visualization, and recording a videography of the worms’ movements.48
Multifocal electroretinogram is subnormal in the affected eye during all stages of the disease, with b-wave being more affected than a-wave.36 Serologic studies, stool examination, and peripheral blood smears are of little value in diagnosing DUSN.10,37 Toxocara and B. procyonis antibody titers have been proposed as diagnostic tools to try to identify the disease.49 No serologic test is currently available for Ancylostoma caninum. Because of the possibility of commonly shared antigens by different nematodes or seropositivity unrelated to the actual infecting nematode, interpretation of serologic testing may be subject to error.48
Etiology and PathogenesisThere is no consensus regarding the identifica-
tion of the subretinal nematode frequently found in DUSN. Reports suggest B. procyonis, A. caninum,
Figure 7. Late stage of diffuse unilateral subacute neuroretinitis. Diffuse and focal changes of the retinal pigment epithelium. Nar-rowing of the retinal arterioles and mild pallor of the optic nerve. Note the intraretinal parasite superior to the fovea.
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX 7
Dirofilaria, and a larval form of T. canis as possible infectious agents involved in DUSN.50 However, the larval form of T. canis is smaller than the worm that causes DUSN and there is a lack of serologic evidence to support the mentioned reports. In addi-tion, funduscopic manifestations are different than those associated with other forms of ocular toxoca-riasis and the high prevalence of T. canis does not correlate with the scant number of DUSN cases re-ported.36
A. caninum, which is a common nematode para-site that infects dogs, is suspected of causing DUSN because it frequently results in cutaneous larval mi-grans that may later manifest signs of DUSN. The worm can survive for months and even years with-out changing form and its infective larva measures approximately 650 µm. This better corresponds to the entity described in DUSN.34,35 Scanning elec-tron microscopy of a nematode excised from a case of DUSN by means of an eye wall biopsy was com-patible with, but not diagnostic for, A. caninum.
B. procyonis is an intestinal nematode that in-fects raccoons and skunks. The larva measures be-tween 300 and 2,000 µm, and it has been proposed as the larger nematode responsible for DUSN.49,50 Nevertheless, infrequent exposure to raccoons or skunks and the absence of central nervous system involvement make B. procyonis a highly unlikely pathogen in DUSN.
The pathogenesis of DUSN appears to involve a mechanical, inflammatory, and toxic assault on the outer retina. A local toxic effect in the outer retina
is caused by products left in the worm’s wake, and a more diffuse toxic reaction affecting both the inner and outer retinal tissues ensues.36 Histopathologic study of an eye believed to be affected by DUSN revealed nongranulomatous vitritis and retinitis. It also showed retinal and optic nerve perivasculitis, extensive degeneration of the posterior retina, mild optic atrophy, mild degenerative changes in the reti-nal pigment epithelium, and a low-grade, patchy, non-granulomatous choroiditis.34,35
Differential DiagnosisThe condition most likely to be mistaken for
DUSN is multiple evanescent white-dot syndrome (MEWDS), although in the early stages DUSN may resemble toxoplasmosis, cytomegalovirus, and bacterial abscesses. MEWDS can be distinguished from DUSN by an accompanying history of flu-like symptoms, photophobia, wreath-like hyperfluores-cent dots on fluorescein angiography, blind spot enlargement, multiple gray or whitish outer retinal lesions, and decreased electroretinogram record-ings.51,52 Visual acuity may even return to normal levels in some cases after several weeks or months. On fluorescein angiography, the white lesions in DUSN block the fluorescence in the early phase, whereas in MEWDS the lesions are hyperfluores-cent in the early stages of the angiogram. Rarely, one can mistake DUSN for sarcoidosis, presumed ocular histoplasmosis syndrome, and multifocal choroidi-tis due to the appearance of focal chorioretinal scars scattered throughout the fundus.53 The absence of
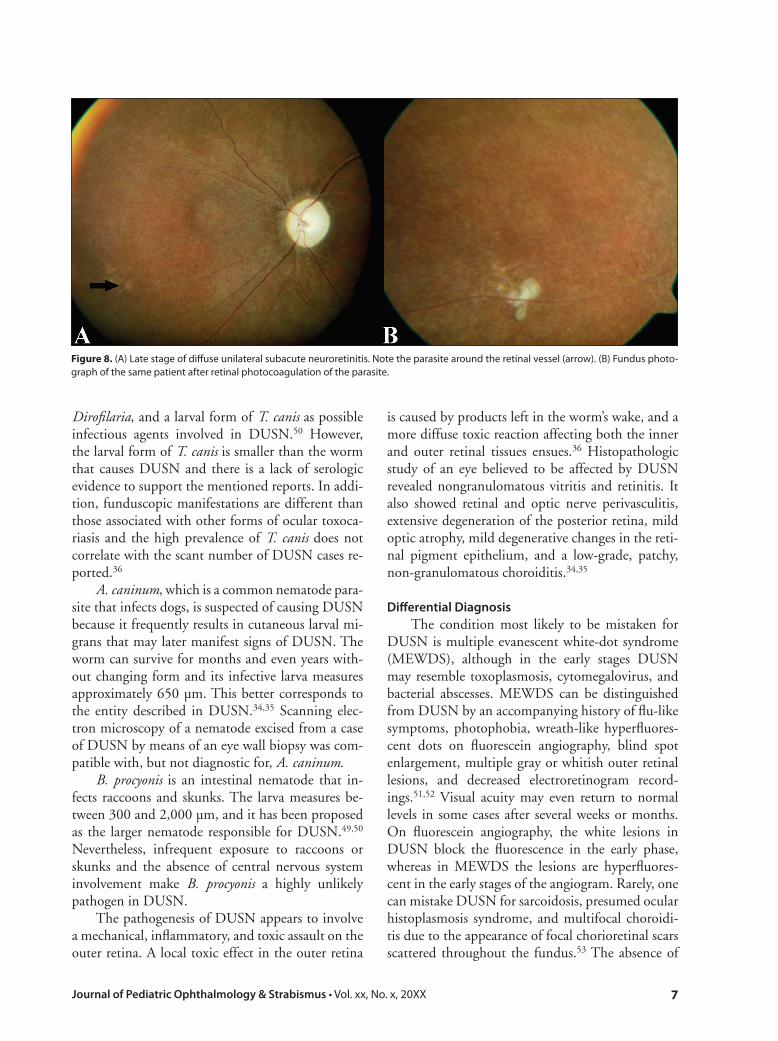
Figure 8. (A) Late stage of diffuse unilateral subacute neuroretinitis. Note the parasite around the retinal vessel (arrow). (B) Fundus photo-graph of the same patient after retinal photocoagulation of the parasite.

8 Copyright © SLACK Incorporated
optic atrophy, vitritis, vessel attenuation, and the presence of normal-looking retinal pigment epithe-lium between punched out lesions is more likely to be encountered in DUSN. Eyes with central retinal artery occlusion may show some characteristics that look like DUSN. Also, the late stages of DUSN may be confused with retinitis pigmentosa, secondary bone-spicules migration, and posterior subcapsular opacification, but unilaterality is characteristically a feature of DUSN.34,35 Trauma may exhibit some DUSN characteristics such as retinal pigment epi-thelial changes and optic atrophy.34,35
TreatmentPhotocoagulation of the parasite when visible,
using 200 to 500 µm, 0.2 to 0.5 second of thermal laser application, is the treatment of choice36,43,47 (Fig. 8), although visual acuity does not significantly improve unless the worm is killed soon after onset of visual loss.54,55 Photocoagulation does not cause exacerbation of inflammation and results in prompt and permanent inactivation of the disease; however, the search for the nematode can become a time-con-suming and frustrating task.36,43,47
Several oral antihelmintic medications, such as thiabendazole and dietylcarbavazine, have been used in an effort to treat this disease.36,56,57 However, most of the studies reported that only the subretinal worms were killed, probably due to inadequate ocu-lar penetration of the drugs. Hence, it has been sug-gested that if the worm cannot be found in a patient with a high suspicion of DUSN, a scatter pattern of laser burns in the vicinity of the multifocal active lesions can be performed to alter the blood–retinal barrier prior to administration of the oral medica-tion.29,47
Recently, several studies have demonstrated al-bendazole as a safe and beneficial treatment modal-ity for these patients.39,58 Our group published the results of the use of oral albendazole in 6 patients with DUSN, following a 10-day regimen at 200 mg orally 3 times daily.39 The nematode was killed and was slowly reabsorbed in three cases. Adverse effects of short-term albendazole treatment were rare.
Findings such as bilateral DUSN and the pres-ence of a nematode in a patient who had undergone successful photocoagulation have been described.37 In light of such reports, we recommend a course of systemic therapy for all patients with DUSN.39
CONCLUSIONOcular toxocariasis and DUSN may produce se-
vere damage to the intraocular structures, causing sig-nificant visual impairment. Although these diseases are not well distributed worldwide due to their poor visual prognosis, it is of great importance that physi-cians be aware of the variety of clinical forms in an effort to achieve an early diagnosis and treatment.
REFERENCES 1. Beaver PC, Snyder CH, Carrera GM, Dent JH, Lafferty JW.
Chronic eosinophilia due to visceral larva migrans; report of three cases. Pediatrics. 1952;9:7-19.
2. Baldone JA, Clark WB, Jung RC. Nematode ophthalmitis: report of two cases. Am J Ophthalmol. 1964;57:763-766.
3. Nichols RL. The etiology of visceral larva migrans: I. Diagnostic morphology of infective second-stage Toxocara larvae. J Parasitol. 1956;42(4 Section 1):349-362.
4. Gillespie SH. Cutaneous larva migrans. Curr Infect Dis Rep. 2004;6:50-53.
5. Wilder HC. Nematode endophthalmitis. Trans Am Acad Ophthal-mol Otolaryngol. 1950;55:99-109.
6. Huntley CC, Costas MC, Lyerly A. Visceral larva migrans syn-drome: clinical characteristics and immunologic studies in 51 pa-tients. Pediatrics. 1965;36:523-536.
7. Schantz PM, Glickman LT. Toxocaral visceral larva migrans. N Engl J Med. 1978;298:436-439.
8. Schantz PM, Stehr-Green JK. Toxocaral larva migrans. J Am Vet Med Assoc. 1988;192:28-32.
9. Schantz PM, Weis PE, Pollard ZF, White MC. Risk factors for toxocaral ocular larva migrans: a case-control study. Am J Public Health. 1980;70:1269-1272.
10. Schantz PM, Meyer D, Glickman LT. Clinical, serologic, and epi-demiologic characteristics of ocular toxocariasis. Am J Trop Med Hyg. 1979;28:24-28.
11. Benezra D, Cohen E, Maftzir G. Patterns of intraocular inflam-mation in children. Bull Soc Belge Ophtalmol. 2001;279:35-38.
12. Paul M, Stefaniak J, Twardosz-Pawlik H, Pecold K. The co-occur-rence of Toxocara ocular and visceral larva migrans syndrome: a case series. Cases J. 2009;2:6881.
13. Vaughn J, Jordan R. Intestinal nematodes in well-cared for dogs. Am J Trop Med Hyg. 1960;9:29-31.
14. Shields JA. Ocular toxocariasis: a review. Surv Ophthalmol. 1984;28:361-381.
15. Sprent JF. The life cycles of nematodes in the family Ascarididae Blanchard 1896. J Parasitol. 1954;40(5, Part 1):608-617.
16. Smith PH, Greer CH. Unusual presentation of ocular Toxocara infestation. Br J Ophthalmol. 1971;55:317-320.
17. Benitez del Castillo JM, Herreros G, Guillen JL, Fenoy S, Banares A, Garcia J. Bilateral ocular toxocariasis demonstrated by aqueous humor enzyme-linked immunosorbent assay. Am J Ophthalmol. 1995;119:514-516.
18. Ellis GS Jr, Pakalnis VA, Worley G, et al. Toxocara canis infesta-tion: clinical and epidemiological associations with seropositivity in kindergarten children. Ophthalmology. 1986;93:1032-1037.
19. Gillespie SH, Dinning WJ, Voller A, Crowcroft NS. The spec-trum of ocular toxocariasis. Eye (Lond). 1993;7:415-418.
20. Watzke RC, Oaks JA, Folk JC. Toxocara canis infection of the eye: correlation of clinical observations with developing pathology in the primate model. Arch Ophthalmol. 1984;102:282-291.
21. Ashton N. Larval granulomatosis of the retina due to Toxocara. Br J Ophthalmol. 1960;44:129-148.
22. Bird AC, Smith JL, Curtin VT. Nematode optic neuritis. Am J Ophthalmol. 1970;69:72-77.
23. Byers B, Kimura SJ. Uveitis after death of a larva in the vitreous cavity. Am J Ophthalmol. 1974;77:63-66.
24. Shields JA, Parsons HM, Shields CL, Shah P. Lesions simulating reti-noblastoma. J Pediatr Ophthalmol Strabismus. 1991;28:338-340.
Journal of Pediatric Ophthalmology & Strabismus • Vol. xx, No. x, 20XX �
25. Shields JA, Shields CL, Parsons HM. Differential diagnosis of retinoblastoma. Retina. 1991;11:232-243.
26. Shields JA, Leonard BC, Michelson JB, Sarin LK. B-scan ultra-sonography in the diagnosis of atypical retinoblastomas. Can J Ophthalmol. 1976;11:42-51.
27. Hagler WS, Pollard ZF, Jarrett WH, Donnelly EH. Results of surgery for ocular Toxocara canis. Ophthalmology. 1981;88:1081-1086.
28. Biglan AW, Glickman LT, Lobes LA Jr. Serum and vitreous Toxo-cara antibody in nematode endophthalmitis. Am J Ophthalmol. 1979;88:898-901.
29. Maguire AM, Zarbin MA, Connor TB, Justin J. Ocular penetra-tion of thiabendazole. Arch Ophthalmol. 1990;108:1675.
30. Belmont JB, Irvine A, Benson W, O’Connor GR. Vitrectomy in ocular toxocariasis. Arch Ophthalmol. 1982;100:1912-1915.
31. Amin HI, McDonald HR, Han DP, et al. Vitrectomy update for macular traction in ocular toxocariasis. Retina. 2000;20:80-85.
32. Benson WE, Belmont JB, Irvine AR, O’Connor GR, Fischer DH. Vitrectomy for complications of ocular toxocariasis. Trans Pa Acad Ophthalmol Otolaryngol. 1983;36:25-30.
33. Small KW, McCuen BW 2nd, de Juan E Jr, Machemer R. Surgi-cal management of retinal traction caused by toxocariasis. Am J Ophthalmol. 1989;108:10-14.
34. Gass JD, Gilbert WR Jr, Guerry RK, Scelfo R. Diffuse unilateral subacute neuroretinitis. Ophthalmology. 1978;85:521-545.
35. Gass JD, Scelfo R. Diffuse unilateral subacute neuroretinitis. J R Soc Med. 1978;71:95-111.
36. Gass JD, Braunstein RA. Further observations concerning the dif-fuse unilateral subacute neuroretinitis syndrome. Arch Ophthal-mol. 1983;101:1689-1697.
37. de Souza EC, Abujamra S, Nakashima Y, Gass JD. Diffuse bilat-eral subacute neuroretinitis: first patient with documented nema-todes in both eyes. Arch Ophthalmol. 1999;117:1349-1351.
38. de Souza EC, da Cunha SL, Gass JD. Diffuse unilateral sub-acute neuroretinitis in South America. Arch Ophthalmol. 1992;110:1261-1263.
39. Cortez R, Denny JP, Muci-Mendoza R, Ramirez G, Fuenmayor D, Jaffe GJ. Diffuse unilateral subacute neuroretinitis in Venezu-ela. Ophthalmology. 2005;112:2110-2114.
40. Harto MA, Rodriguez-Salvador V, Avino JA, Duch-Samper AM, Menezo JL. Diffuse unilateral subacute neuroretinitis in Europe. Eur J Ophthalmol. 1999;9:58-62.
41. Oueghlani E, O’Sullivan E, Pavesio CE. Diffuse unilateral sub-acute neuroretinitis in the United Kingdom. Int Ophthalmol. 2010 Mar 25. [Epub ahead of print]
42. Cialdini AP, de Souza EC, Avila MP. The first South American case of diffuse unilateral subacute neuroretinitis caused by a large nematode. Arch Ophthalmol. 1999;117:1431-1432.
43. Gass JD. Subretinal migration of a nematode in a patient with diffuse unilateral subacute neuroretinitis. Arch Ophthalmol.
1996;114:1526-1527. 44. Carney MD, Combs JL. Diffuse unilateral subacute neuroretini-
tis. Br J Ophthalmol. 1991;75:633-635. 45. Byrne S, Beatty S. Diffuse unilateral subacute neuroretinitis. Ir J
Med Sci. 2003;172:90-91. 46. Audo I, Webster AR, Bird AC, Holder GE, Kidd MN. Progressive
retinal dysfunction in diffuse unilateral subacute neuroretinitis. Br J Ophthalmol. 2006;90:793-794.
47. Gass JD, Callanan DG, Bowman CB. Successful oral therapy for diffuse unilateral subacute neuroretinitis. Trans Am Ophthalmol Soc. 1991;89:97-112.
48. Moraes LR, Cialdini AP, Avila MP, Elsner AE. Identifying live nematodes in diffuse unilateral subacute neuroretinitis by us-ing the scanning laser ophthalmoscope. Arch Ophthalmol. 2002;120:135-138.
49. Kazacos KR, Raymond LA, Kazacos EA, Vestre WA. The raccoon ascarid: a probable cause of human ocular larva migrans. Ophthal-mology. 1985;92:1735-1744.
50. Kazacos KR, Vestre WA, Kazacos EA, Raymond LA. Diffuse uni-lateral subacute neuroretinitis syndrome: probable cause. Arch Ophthalmol. 1984;102:967-968.
51. Hangai M, Fujimoto M, Yoshimura N. Features and function of multiple evanescent white dot syndrome. Arch Ophthalmol. 2009;127:1307-1313.
52. Schaal S, Schiff WM, Kaplan HJ, Tezel TH. Simultaneous ap-pearance of multiple evanescent white dot syndrome and mul-tifocal choroiditis indicate a common causal relationship. Ocul Immunol Inflamm. 2009;17:325-327.
53. Sinha R, Raju S, Garg SP, Venkatesh P, Talwar D. Presumed ocu-lar histoplasmosis syndrome in India. Ocul Immunol Inflamm. 2007;15:315-317.
54. Garcia CA, Gomes AH, Garcia Filho CA, Vianna RN. Early-stage diffuse unilateral subacute neuroretinitis: improvement of vision after photocoagulation of the worm. Eye (Lond). 2004;18:624-627.
55. Garcia CA, Gomes AH, Vianna RN, Souza Filho JP, Garcia Filho CA, Orefice F. Late-stage diffuse unilateral subacute neuroretini-tis: photocoagulation of the worm does not improve the visual acuity of affected patients. Int Ophthalmol. 2005;26:39-42.
56. Gass JD, Callanan DG, Bowman CB. Oral therapy in diffuse uni-lateral subacute neuroretinitis. Arch Ophthalmol. 1992;110:675-680.
57. Casella AM, Farah ME, Belfort R Jr. Antihelminthic drugs in diffuse unilateral subacute neuroretinitis. Am J Ophthalmol. 1998;125:109-111.
58. Souza EC, Casella AM, Nakashima Y, Monteiro ML. Clinical fea-tures and outcomes of patients with diffuse unilateral subacute neuroretinitis treated with oral albendazole. Am J Ophthalmol. 2005;140:437-445.


















