Ocular Manifestations of Rheumatoid Diseases … Manifestations of Rheumatoid Diseases Update ......
113
Ocular Manifestations of Rheumatoid Diseases Update March 2017 Julie A. Tyler, OD, FAAO Nova Southeastern University
-
Upload
nguyennguyet -
Category
Documents
-
view
224 -
download
2
Transcript of Ocular Manifestations of Rheumatoid Diseases … Manifestations of Rheumatoid Diseases Update ......
Ocular Manifestations of Rheumatoid Diseases Update
March 2017Julie A. Tyler, OD, FAAO
Nova Southeastern University
Ocular Manifestations of Rheumatoid Diseases Update
• No Disclosures
• Thank you in advance for invitation to present.
Ocular Manifestations of Rheumatoid Diseases Update - Definitions
Autoimmune diseases-Characterized: tissues of the body mistakenly
attacking an individual’s own cellsMay result in significant ocular complications.
Examples of Autoimmune diseases : Rheumatoid Arthritis (RA), Systemic Lupus Erythematosus (SLE), Graves’ disease, Multiple Sclerosis (MS), and Giant cell arteritis (GCA)

Ocular Manifestations of Rheumatoid Diseases Update
Rheumatoid diseases-Characterized: Inflammation and loss of function of one or more connecting or supporting structures of the body– Joints, tendons, muscles,
ligaments and bones - typically affected with extra-articular manifestations
– Common sx: Pain, swelling & stiffness
Ocular Manifestations of Rheumatoid Diseases Update
There are over 100 rheumatic diseases, many with ocular manifestations…

Rheumatic Diseases with Ocular Considerations
1. Rheumatoid arthritis (RA)2. Systemic lupus erythematosus (SLE)3. Juvenile rheumatoid arthritis (JRA)4. Spondylo- (verteb) arthro- (joint) pathies (disease) –
a. Ankylosing spondylitisb. Reactive Arthritis (Reiter’s syndrome) –seronegative spondyloarthropathy
• 5. Others include Scleroderma (systemic sclerosis), gout, polychondritis….
Scleroderma

But before we get into the details of rheumatologic disease…..
HOW are optometrists going to know about these conditions and why do we care…..?

Ocular Manifestations of Rheumatoid Diseases– Many presentations
• Blepharitis• Conjunctivitis• Episcleritis/Scleritis• Keratitis
– Dry eye – Infiltrative disease
• Uveitis• Retinal disease
– Retinitis– Vasculitits
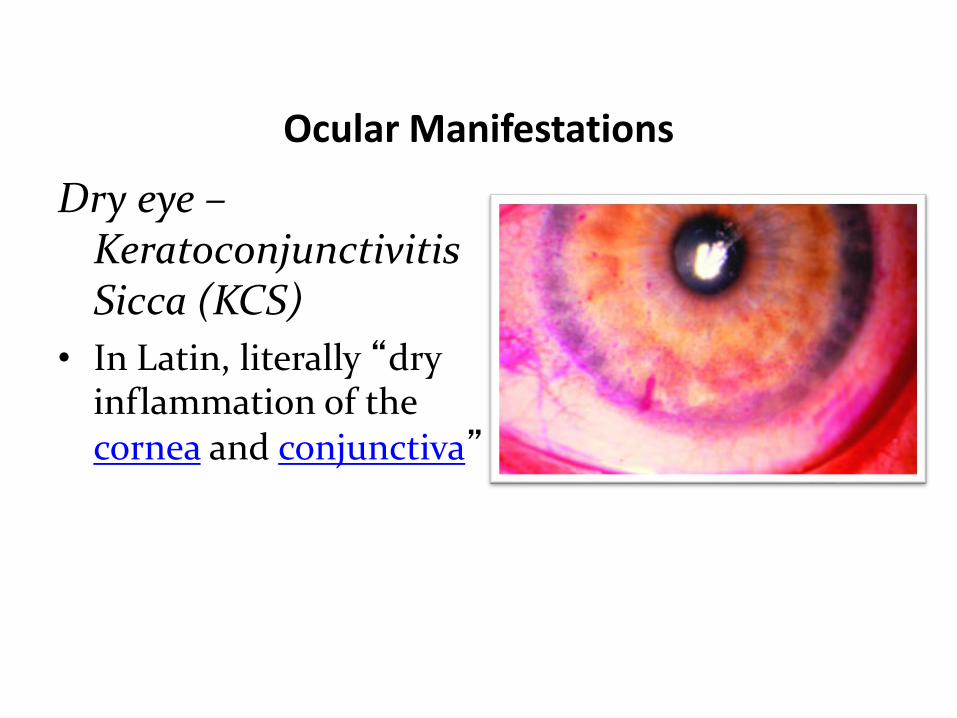
Ocular Manifestations
Dry eye –Keratoconjunctivitis Sicca (KCS)
• In Latin, literally “dry inflammation of the cornea and conjunctiva”
Ocular Manifestations
Dry eye – Keratoconjunctivitis Sicca (KCS)• Systemic conditions - Rheumatologic:
– Rheumatoid arthritis (RA), SLE
• Systemic conditions - Others/Differential Dx:– Auto-immune diseases – Hashimoto’s
thyroiditis– Allergy & atopic disease– Dermatologic disease – Acne rosacea– Other – Age related/hormonal changes
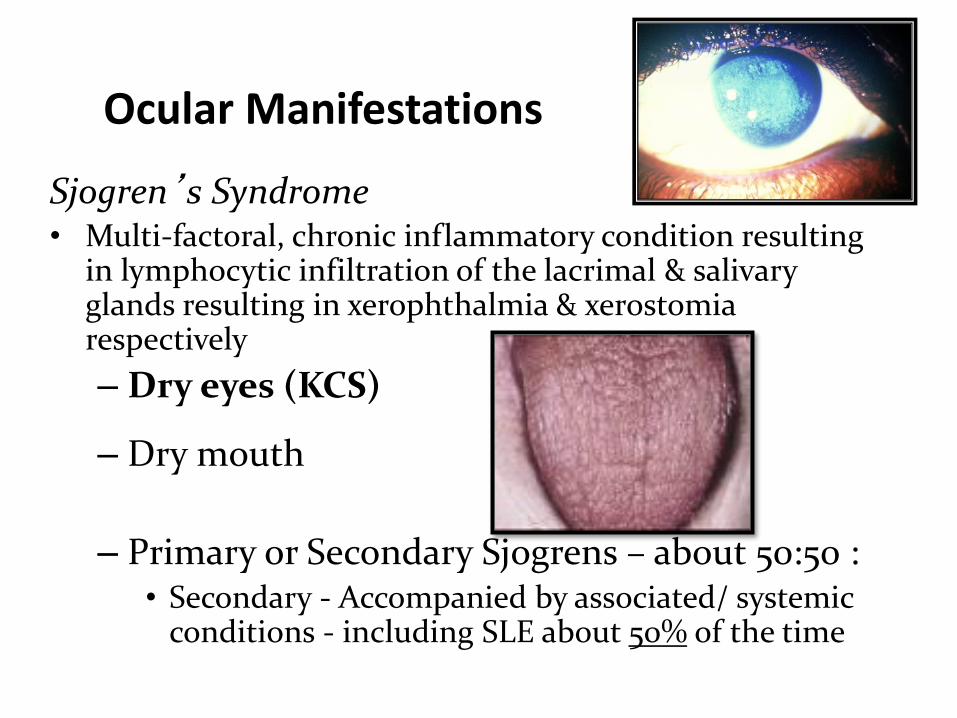
Ocular Manifestations
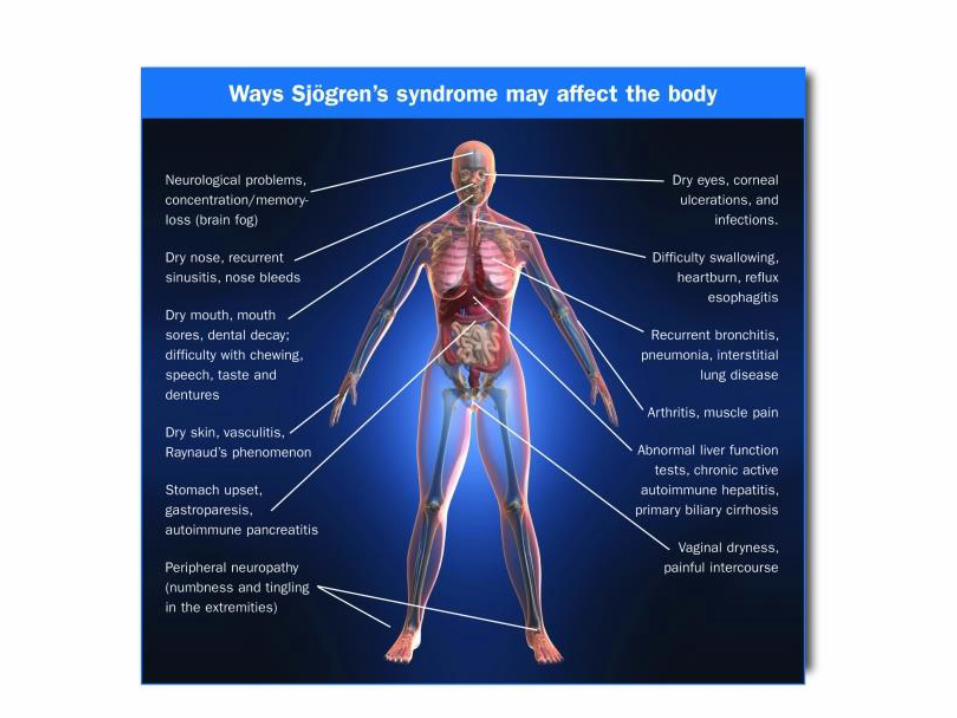
Sjogren’s Syndrome• Multi-factoral, chronic inflammatory condition resulting
in lymphocytic infiltration of the lacrimal & salivary glands resulting in xerophthalmia & xerostomia respectively – Dry eyes (KCS)
– Dry mouth
– Primary or Secondary Sjogrens – about 50:50 :• Secondary - Accompanied by associated/ systemic
conditions - including SLE about 50% of the time

Ocular Manifestations of Rheumatoid Diseases
Dry eye –Sjogren’s Syndrome• Other symptoms
– Debilitating fatigue– Joint pain– Periods of flares & remission– Dysfunction of other organs:
• Æ Pancreas, kidneys, lungs, liver, GI and CNS
• Other considerations– Increased risk of lymphoma
Ocular Manifestations of Rheumatoid Diseases
Dry eye –Sjogren’s Syndrome
• Up to 4 million American’s w/ Sjogren’s syndrome– 9 out of 10 = women
• Testing options….
Ocular Manifestations of Rheumatoid Diseases
Dry eye –Sjogren’s Syndrome• Serology
– ELISA, “LIPS: Luciferase ImmunoPrecipitation Systems”
– Article: Rapid serological detection of autoantibodies associated with Sjögren's syndrome• J Transl Med. 2009; 7: 83. Published online 2009
September 24. doi: 10.1186/1479-5876-7-83• Quick version of LIPS (QLIPS): 10 min incubation, btwn
49-70% detection of antibodies (100% specificity)
Ocular Manifestations of Rheumatoid Diseases
Dry eye –Sjogren’s Syndrome• Often is overlooked…..
– Early diagnosis & treatment important—• May prevent serious complications • Greatly improve a patient’s quality of life• On average, nearly seven years to receive diagnosis (~6.5
yrs)– No single test to confirm diagnosis– Conduct a SERIES of tests and ask about symptoms
• Æ Rheumatologists have primary responsibility for diagnosing/managing Sjögren’s

Ocular Manifestations of Rheumatoid Diseases
• Sept 2011: Venus Williams withdraws from U.S. Open after revealing she has “incurable” immune system disease– Star set for break from tennis to
treat illness
• Has returned to the court …complicated diagnosis and management
Ocular Manifestations of Rheumatoid Diseases
Dry eye –Sjogren’s Syndrome• Treat aggressively – including anti-
inflammatory management in addition to tear supplementation
• Dry eye treatment:– International Dry Eye Workshop (DEWS)
• 2007: Update of the disease– Stage Dry Eye & determine etiology if possible
• Management and therapy of dry eye disease: report of the Management and Therapy Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007 Apr;5(2):163-78
– As advanced….Pulse steroid with Restasis
Dry Eye Treatment Considerations
Staging of Dry eye first….o Early Æ Supportive treatment & environmental
modificationso Artificial tears
o Lacrimal/ “tear”o Emoillant/ “oil”
o Lid hygiene if indicatedo Increase hydration in general Æ Drink H2Oo Decreasing caffeine & anti-histamine intake
o Homeopathic/Nutritional optionso Flax seedo Omega balance (3&6)

Dry Eye Treatment Considerations - continued
o Moderate ÆoMaintain artificial tears & supportive measureso Pulse dose of mild steroid w/ concurrent start of
cyclosporine A
o Severe Æo Remove filamentsoOral medications
o Salagen (Pilocarpine)
Dry Eye Treatment Considerations - continued
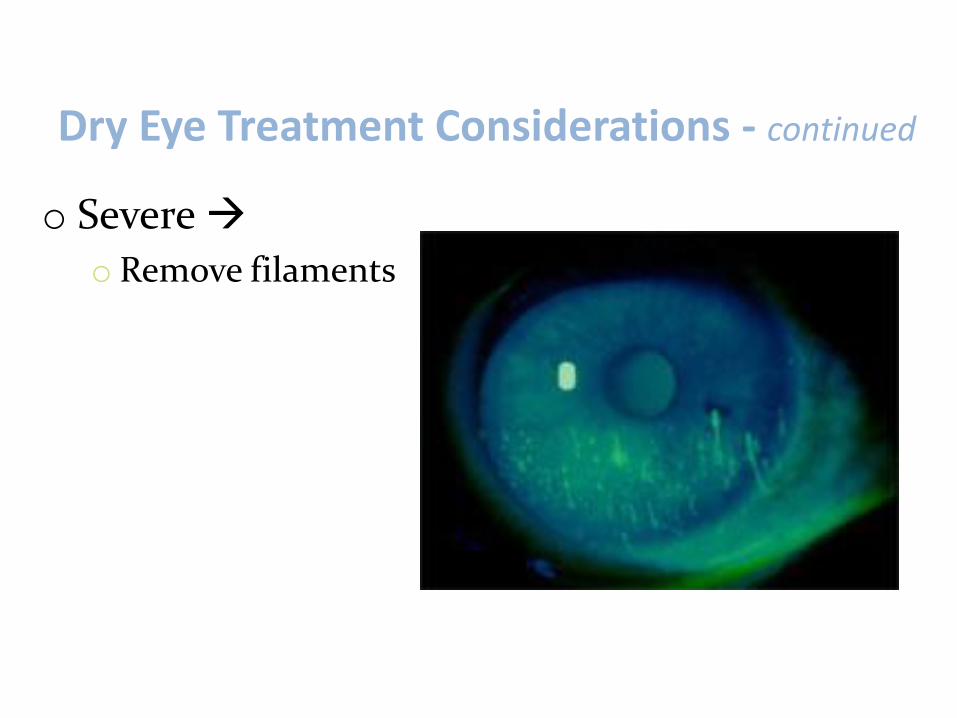
o Severe Æo Remove filaments
Dry Eye Treatment Considerations - continued
o Severe Æ Oral medications: Salagen (Pilocarpine)oAffects the nervous systemo Increases saliva secretion in mouth
o Two 12 week randomized, double-blind, placebo-controlled studiesÆ 629 pts: To measure the ability of
Salagen® tablets to stimulate saliva production
o Varying doses of Salagen® Tablets (2.5-7.5 mg)
o Rate of saliva production was plotted Æ Increased after first dose
• Read more at http://www.drugs.com/mtm/salagen.html#6sugAVj4AyVHRoSs.99
Dry Eye Treatment Considerations - continued
o Role of Lacrisert?o Lacrisert® (hydroxypropyl
cellulose ophthalmic insert)o Efficacy of hydroxypropyl cellulose
ophthalmic inserts (LACRISERT) in subsets of patients with dry eye syndrome: findings from a patient registry. Luchs JI, Nelinson DS, Macy JI; LAC-07-01 Study Group. Cornea. 2010 Dec;29(12):1417-27.
o Benefit for: Subsets of pts with MOD to SEVERE dry eye and comorbid conditions,o Improve the symptoms of DESo Ability to perform ADLso Quality of life

Dry Eye Treatment Considerations - continued
o Lid management/Demodex and Blepharitiso Increased number of OTC and prescription lid
hygiene options that include various products to assist with lid diseaseo i lid/AvenovaÆ hypochlorous acid has shown to be
fast-acting against bacteria, biofilm and toxinsoBlephadexÆ Cleanser for blepharitis and demodexoCliradexÆ essential oils, most specifically tea tree
oil, scruboOral medication consideration
Generalized Uveitis
o Categorized by Æ Location, Type, Course, Etiology
• Location • Anterior uveitis• Keratouveitis• Trabeculitis• Intermediate uveitis-“Pars planitis”
• Panuveitis
• Type • Granulomatous• Non-granulomatous
• Course• Acute• Chronic• Recurrent
• Etiology• Systemic• Primary Ocular
Ocular Manifestations of Rheumatoid Diseases
Uveitis: When to consider work-up?
• Bilateral disease• Granulomatous KP Æ
– Most rheumatoid disease non-granulomatous
• Recurrent• Intermediate and posterior uveitis• Acute anterior, unilateral if SEVERE or if
history/examination is suspicious
Differentiating systemic conditions work-up based on anterior uveitis
Bilateral:• Idiopathic• Juvenile rheumatoid arthritis
(JRA)• Inflammatory bowel disease• Sarcoid• Behcet’s (generally)• Others: Coccidioidmycosis
Unilateral:yIdiopathicyAnkylosing Spondylitis (AS) yReiter’s/ Reactive arthritisyInflammatory bowel diseaseyVaricella-zosteryHerpes SimplexyPosner-Schlossman syndrome (PSS/GCC)yHLA-B27 associated uveitisyFuch’s Heterochomia Iridocyclitis
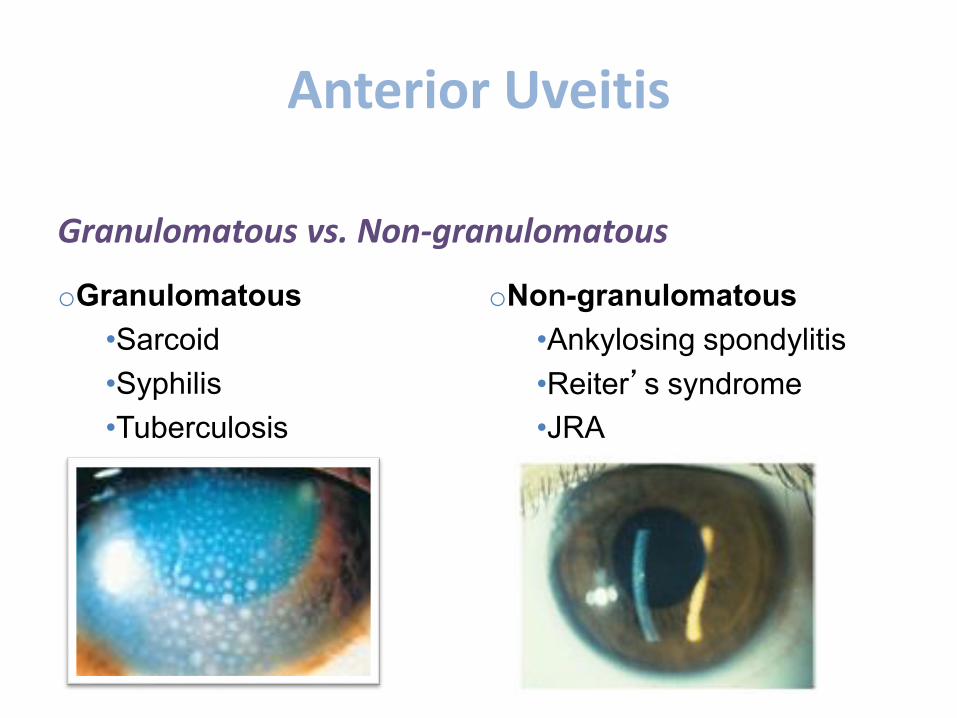
Anterior Uveitis
Granulomatous vs. Non-granulomatous
oGranulomatous•Sarcoid•Syphilis•Tuberculosis
oNon-granulomatous•Ankylosing spondylitis•Reiter’s syndrome•JRA
Additional TestingSystemic considerations o Labs should be tailored to the history and
physical examinationExamples: • 45 year old black female with a cough….• 25 year old white male with pain on urination…

General Lab tests to accompany specifics…
Blood work considerations – General lab tests
1. CBC with differential (CBC) & Erythrocyte sedimentation rate (ESR)– ESR measures inflammation• Elevated ESR indicates the presence of an inflammatory
disorder, including Sjögren’s
2. Challenging cases (esp, uveitis): HLA-B27Human lymphocyte antigen – B27

Rheumatoid disease suspected…Serology– General lab tests1. Rheumatoid Factor (RF) – Antibody test most often performed for the
diagnosis of rheumatoid arthritis (RA) – Positive in many rheumatic diseases– 60-70% Sjogren’s are positive
2. Anti-Nuclear Antibody (ANA)– Group of antibodies that react against normal
components of a cell nucleus– 70% of Sjögren’s patients

Rheumatoid disease suspected…Serology– General lab tests3. To rule out (or in…) Sjogren’s: SS-A (or Ro) and SS-B
(or La)– Marker antibodies for Sjögren's– 70% of Sjögren’s patients are positive for SS-A– 40% are positive for SS-B Æ Also with SLE
4. IGs (Immunoglobulins)– Normal blood proteins– Participate in immune reactions
5. ACPA = anti-citrullinated protein antibody
Anterior Segment– Serology & Radio. testing
Grouping tests for rheumatologic disease:y Rheumatoid Arthritis
y CBC = often has Normochromic-normocytic anemiay ESR & C-reactive protein (CRP)y RF
o SLE• ANA
o JRA (need all tests to categorize)• Knee X-ray• Rheumatoid Factor (RF)• ANA• HLA-B27
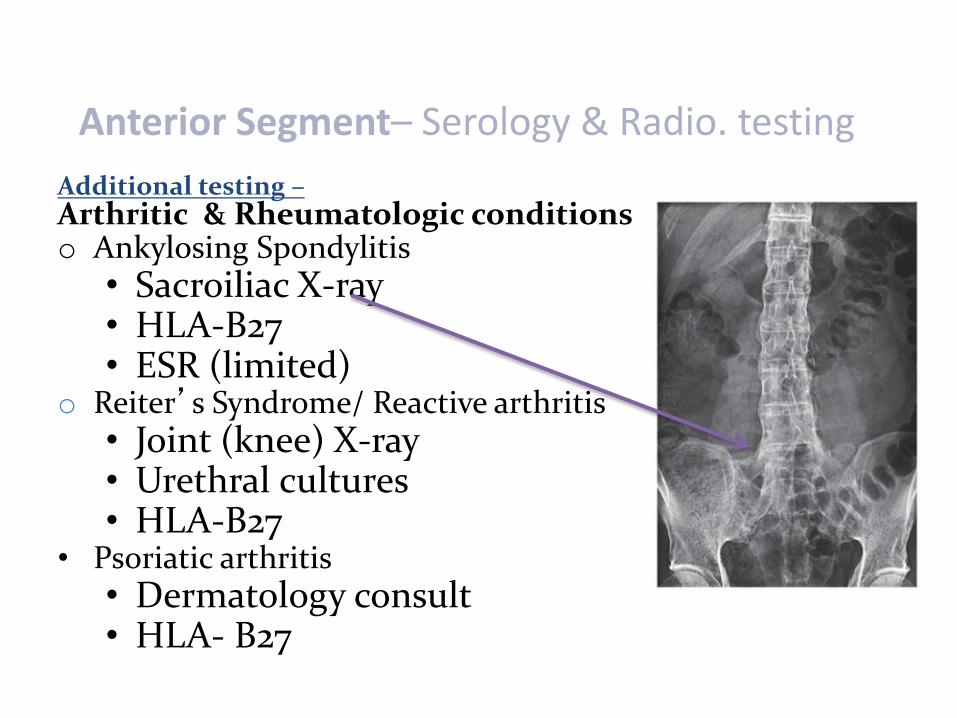
Anterior Segment– Serology & Radio. testing Additional testing –Arthritic & Rheumatologic conditionso Ankylosing Spondylitis
• Sacroiliac X-ray• HLA-B27• ESR (limited)
o Reiter’s Syndrome/ Reactive arthritis• Joint (knee) X-ray• Urethral cultures• HLA-B27
• Psoriatic arthritis• Dermatology consult• HLA- B27
o Chief Complaints
o Questions to Ask¾ History¾ Rashes¾ Aches and Pains
o Findings ¾ Slit lamp¾ Dermatologic¾ Fundus evaluation
o Plans and Follow-up
o Referrals
Rheumatoid Diseases –Overall Case Considerations
Rheumatoid ArthritisChronic, progressive inflammatory disease
w/several ocular associations Æ pain, stiffness, swelling, & limitation in the motion
• Qualities of Rheumatoid arthritis– Periods of exacerbations and remissions– Differs from Juvenile form
Rheumatoid Arthritis• Incidence
– In the US, RA is found in ~ 1% of the adult population• 2010 estimation of 1.3 million Americans
– Peak incidence between the fourth and sixth decades• Can be at any age however…
– Women (2.5x) >> Men– Higher prevalence = Native americans
Rheumatoid Arthritis Update** 2010 RA reclassification:
Gillian Hawker, et al. 2010 Rheumatoid Arthritis Classification Criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative initiative. Arthritis & Rheumatism; August 9, 2010
Revised classification criteria for RA:• Allow the study of treatments for RA at much earlier
stages of the diseaseÆ before joint damage• Originally not designed for diagnosis in CLINICAL
Practice….– Previous criteria 1987 = Barrier to study of RA
• Æ New therapies emerged that prevent joint damage
Rheumatoid Arthritis Update** 2010 RA reclassification:• Modern therapy = Goal of treatment to
prevent people from reaching the point of chronic joint damage
• Many pts did not fulfill 1987 arthritis classification criteria until their disease was well-advanced & in many cases-joint damage had already occurred– Limited researchers from studying early phase RA

Rheumatoid Arthritis Update** 2010 RA reclassification:• For development
– Phase I: Reviewed existing data for characteristics of high risk for progression to persistent, erosive RA
– Phase II: Consensus amongst practicing rheumatologist to determine factors most important in understanding a person’s likelihood of developing the chronic joint damage that is hallmark of RA
– Phase III: Integrate parts of Phase I and Phase II to develop a SCORING system
Rheumatoid Arthritis UpdateConfirmed research criteria:• Presence of joint swelling, indicating synovitis-
the inflammation of the synovial membrane –without another possible co-morbidity (eg, SLE, gout)– Definite ‘rheumatoid arthritis,’
• Æ Score of six or greater (out of a possible 10)• The scoring system :
– Number and site/size of involved joints– Laboratory tests of inflammation and auto-immunity– Symptom duration

Rheumatoid ArthritisEtiology• Specific etiology of RA is unidentified• Current theory:
– Genetic predisposition involving multiple genes– Initiated by an unknown trigger(s)
• Association w/female sex hormones has been postulated due to:– Increased prevalence in women– RA remission during pregnancy– Increased risk of RA onset postpartum
Rheumatoid ArthritisFamilial risksy Monozygotic twin studies have found a
concordance rate of 15-30%
y Familial aggregation reported is less frequent than other autoimmune diseases such as SLE and MS
Differentialy Unlike osteoarthritis, which is mechanical in
etiology, RA is an inflammatory condition
Rheumatoid Arthritis
Disease Process• Onset usually insidious: over weeks to months• Primary (but not solitary) target of the abnormal immune
response is the synovial membranes & articular structures• RA progresses:
– From swelling of the synovial lining to synovial thickeningand finally deformity of the joints
• Common extra-articular manifestations:– Rheumatoid nodules, ocular disease, Sjögren’s syndrome,
rheumatoid vasculitis and neurologic disease

Rheumatoid Arthritis
Common symptoms – Symmetrical stiffness in multiple joints– Morning stiffness greater in duration than 1 hour– Generalized fatigue
Clinical Signs– Joint swelling– Tenderness

Rheumatoid Arthritis
Ocular Manifestations - ~ 25% of patients with RA– Keratoconjunctivitis sicca (KCS)
• Combination of inflammation of the lacrimal gland and meibomian gland dysfunction
• Conjunctival staining, punctate epithelial keratitis (PEK), diminished tear meniscus and decreased TBUT
– Episcleritis– Scleritis– Keratitis - Peripheral corneal ulceration

Rheumatoid Arthritis – Making Dx
– Historically, the 1987 criteria for the classification of RA was the presence of at least four of seven criteria
– Based on medical history, physical examination, serology, and imaging studies
• New guidelines: Identifying pts with RA “earlier”
– Target population (Who should be tested?): • Pts who have at least 1 joint with definite clinical synovitis
(swelling)*
• Pts with the synovitis not better explained by another disease†
Rheumatoid Arthritis - Serologyy Complete blood count (CBC)
y Normochromic-normocytic anemia in 80% of cases
y Erythrocyte sedimentation rate (ESR) & C-reactive protein (CRP)y Both measure inflammation
y CRP has a more immediate response during both the increase and decrease of inflammation
y ESR elevated in 90% of cases
y Rheumatoid factor (RF) Æ (+) in 70% of cases with RA
y ACPA = anti-citrullinated protein abÆ New criteria
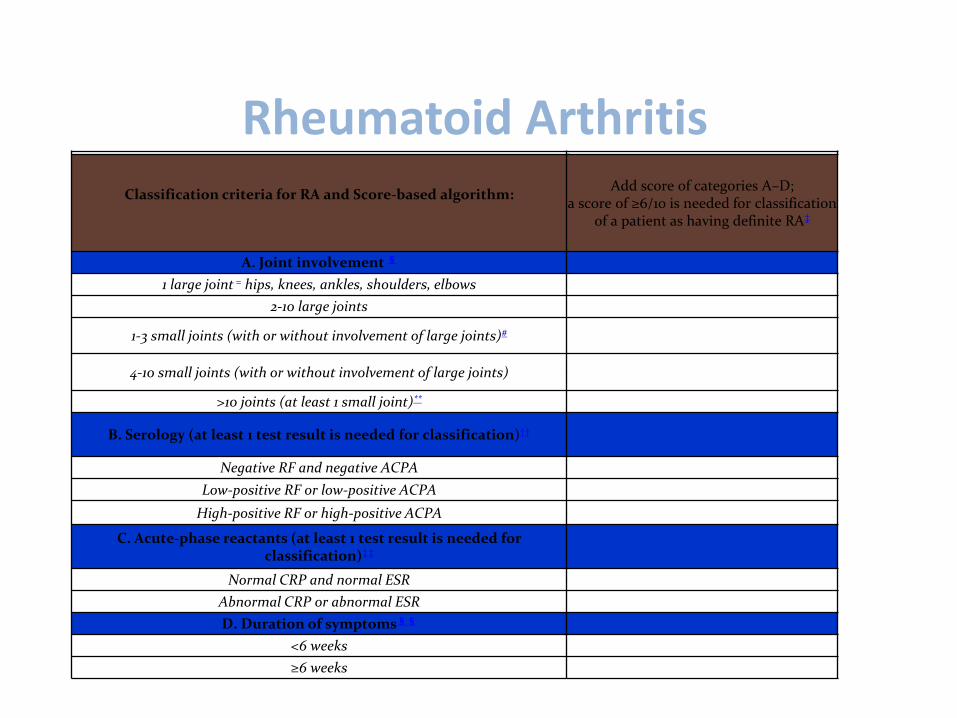
Rheumatoid ArthritisScore
Classification criteria for RA and Score-based algorithm: Add score of categories A–D;a score of ≥6/10 is needed for classification
of a patient as having definite RA‡
A. Joint involvement §
1 large joint = hips, knees, ankles, shoulders, elbows 0
2-10 large joints 1
1-3 small joints (with or without involvement of large joints)# 2
4-10 small joints (with or without involvement of large joints) 3
>10 joints (at least 1 small joint)** 5
B. Serology (at least 1 test result is needed for classification)††
Negative RF and negative ACPA 0
Low-positive RF or low-positive ACPA 2
High-positive RF or high-positive ACPA 3
C. Acute-phase reactants (at least 1 test result is needed for classification)‡‡
Normal CRP and normal ESR 0
Abnormal CRP or abnormal ESR 1
D. Duration of symptoms§§
<6 weeks 0
≥6 weeks 1
Rheumatoid Arthritis
• Permanent damage can occur in first two years of infliction– Aggressive treatment philosophy!!!– Goal: Reduce inflammation
• With the 1987 Criteria, # 1 through 4 must have been present for at least six weeks
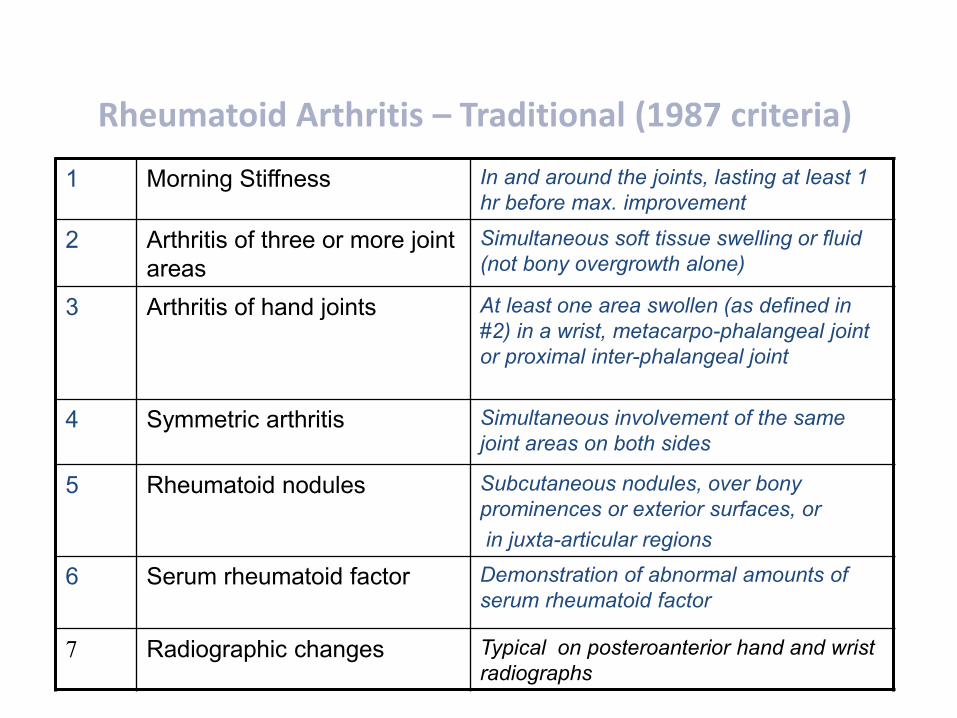
Rheumatoid Arthritis – Traditional (1987 criteria)
1 Morning Stiffness In and around the joints, lasting at least 1 hr before max. improvement
2 Arthritis of three or more joint areas
Simultaneous soft tissue swelling or fluid (not bony overgrowth alone)
3 Arthritis of hand joints At least one area swollen (as defined in #2) in a wrist, metacarpo-phalangeal joint or proximal inter-phalangeal joint
4 Symmetric arthritis Simultaneous involvement of the same joint areas on both sides
5 Rheumatoid nodules Subcutaneous nodules, over bony prominences or exterior surfaces, orin juxta-articular regions
6 Serum rheumatoid factor Demonstration of abnormal amounts of serum rheumatoid factor
7 Radiographic changes Typical on posteroanterior hand and wrist radiographs

Rheumatoid ArthritisRequires timely management• Dependent on individual & severity• Multifaceted approach to management
– Patient education– Balance of rest and exercise– Medications
• Neutraceuticals - be aware….• eg, Rheumatol ÆMannose, Galactose, Fucose, Glucose Xylose, N-
acetylneuramic acid, N-acetylgalactosamine, N-acetylglucosamine
– Joint protection– Surgery
One bottle option = $67 for 60 pills

Rheumatoid ArthritisMedications• First-line medications, NSAIDS and
corticosteroids• Second-line medications Æ
– DMARDs (Disease-modifying anti-rheumatic drugs)• Suppress immune system & inhibit loss of cartilage and
bone– BRMs (Biologic response modifiers)
• Influence the activity of cytokines • Agents carefully designed to block actions of natural
substances that are part of the immune response– tumor necrosis factor or interleukin-1
Rheumatoid Arthritis
Treatment -
• Disease-modifying anti-rheumatic drugs (DMARDs)– Hydroxychloroquine Æ Plaquenil– Methotrexate ÆRheumatrex– Cyclosporin Æ Neoral– Azathioprine Æ Imuran
Rheumatoid ArthritisBiologic response modifiers (BRMs) • “New” specific area of drug development = anti-TNF (tumor
necrosis factor blocker)- inhibit abnormal B cell activity
– AdalimumabÆHumira– EtanerceptÆEnbrel (1st)– InfliximabÆRemicade
• Rituxan® (rituximab) in combination with methotrexate– Approved 1st line therapy for RA
• Myocophenolate MofetilÆ Cellcept immunosuppressor with questionable results – may not be superior than other medications (also tested for muscular dystrophy with variable results)
Approved 1st line therapy for RA
Plaquenil – what’s “old”?Considerations:• Common drug used in treatment of
of RA and SLE• MOA: Unclear• Considerations: Known to BIND to melanin in all
pigmented cells• Complications: Light exposure of the drug,
releases TOXIC by-products– IN the RETINA Æ Leads to “Bull’s Eye”
because of central blocked pigment

Plaquenil – what’s “old”?Considerations:• Potential for retinal complications and toxicity
– Toxicity is RARE when prescribed correctly (<1 %)– Toxicity is RARE with low accumulative dose (<5 yrs)– BUT, when it occurs there is an incidence of IRREVERSIBLE
retinal toxicity near the central vision
Plaquenil – what’s NEW?Considerations:
• Identified RISK FACTORS:– Duration of use > 5 years– Cumulative dose >1000g– Daily dose >6.5mg/kg (<136 lbs for standard
400mg) Æ ** Pts should be 137 “lean” lbs– Elderly age group– Kidney or liver disease– Pre-existing outer retinal disease (eg, drusen)
• * Chloroquine & Hydroxychloroquine preferably bind to cells that contain melanin

Plaquenil – what’s new?New Guidelines for management – At year ONE:
1. BASELINE exam within 1st year of use to document baseline retinal changes– Fundus exam with photos
2. White 10-2 threshhold visual fields3. One of the following:– SD-OCT – Fundus autofluorescence (FAF)– Multifocal ERG (mfERG)

Plaquenil – what’s new?Scheduling management:
� Annual exams starting FIVE years after initiation of tx�EARLIER screening if RISK factors
�Detection PRIOR to Bull’s eye changes�Largely irreversible (poor clearance of med?)
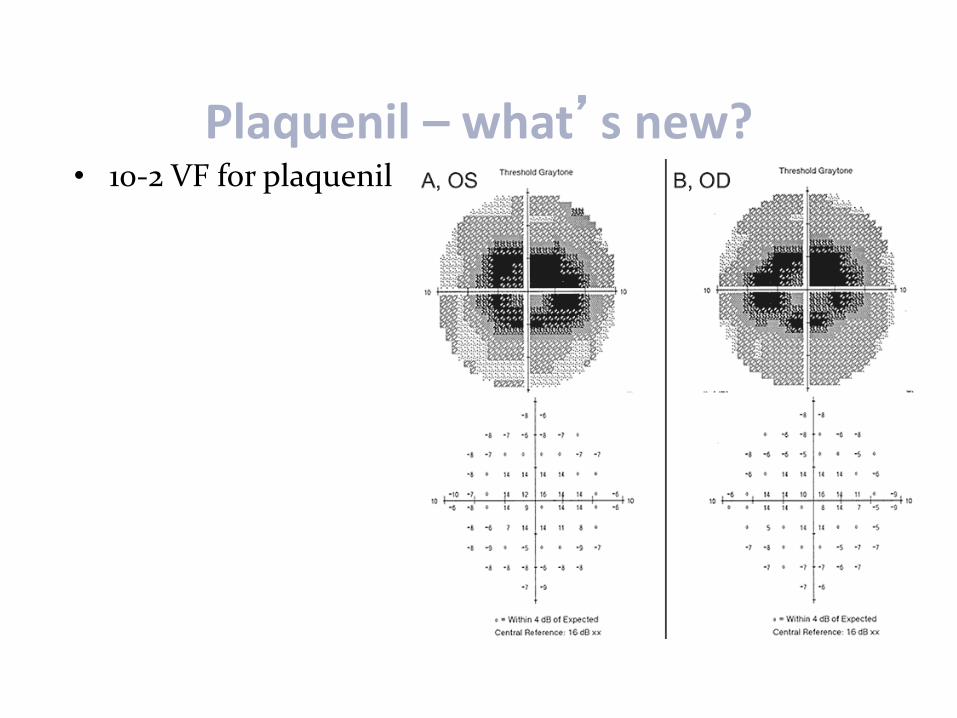
Plaquenil – what’s new?• 10-2 VF for plaquenil
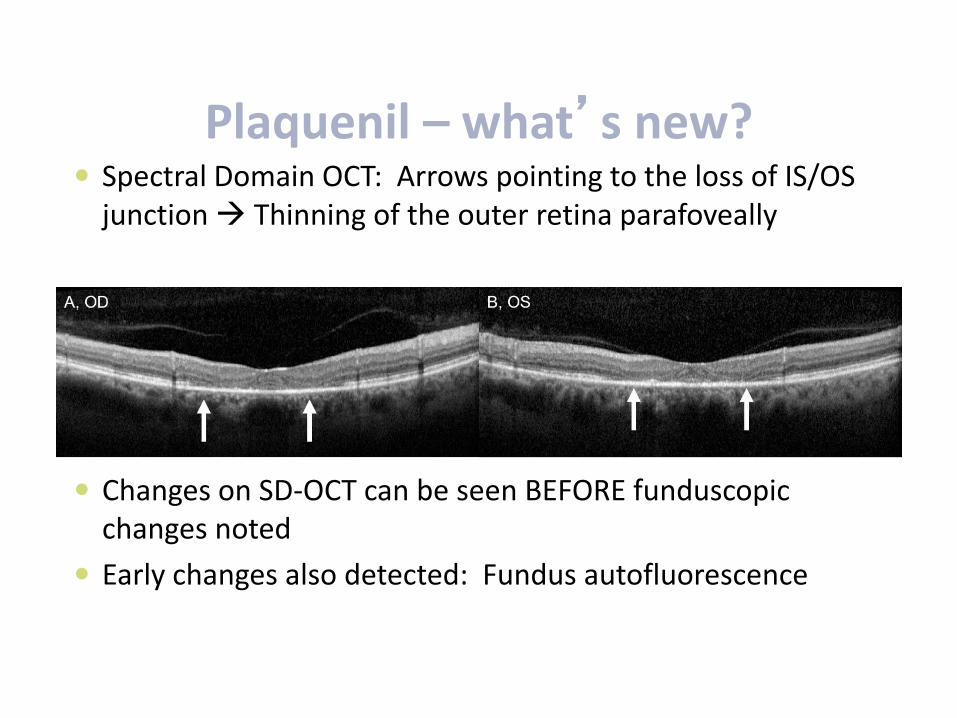
Plaquenil – what’s new?y Spectral Domain OCT: Arrows pointing to the loss of IS/OS
junction Æ Thinning of the outer retina parafoveally
y Changes on SD-OCT can be seen BEFORE funduscopicchanges noted
y Early changes also detected: Fundus autofluorescence
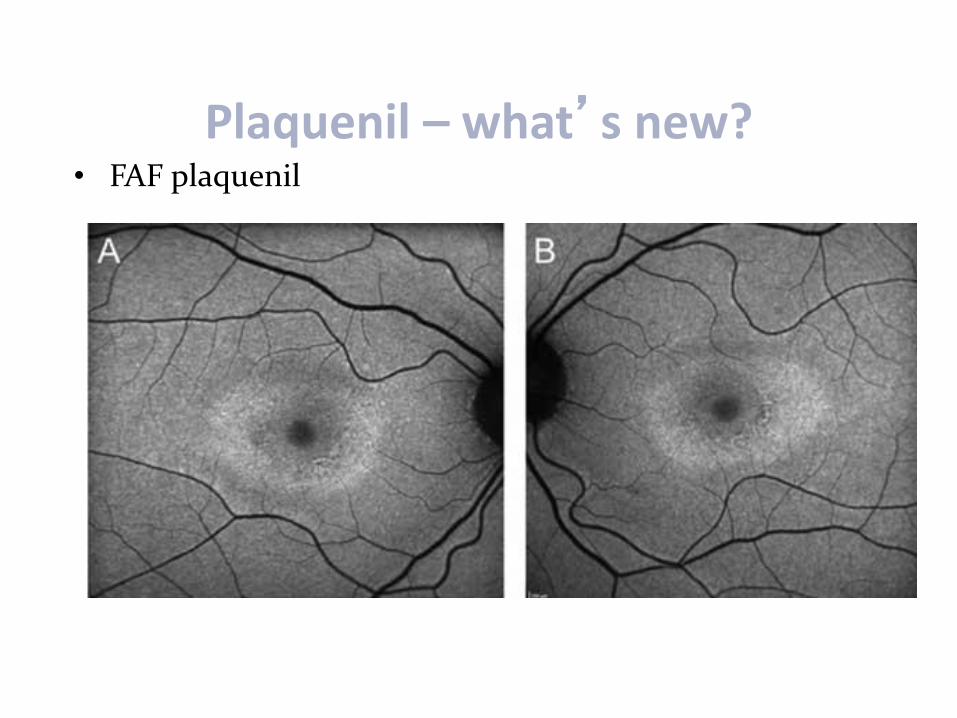
Plaquenil – what’s new?• FAF plaquenil
Plaquenil – what’s new?What is FAF (Fundus Autofluorescence)
Imaging?• RPE & Lipofuscin (LF)
– Lipofuscin = in all RPE cells Æ accumulates within aging cells that are metabolically active • Made of at least 10 different “Fluorophores” : excited with short
wavelength light– Build-up of LF in RPE mainly caused by incomplete degradation
of photoreceptor outer segment discs• Maximum autofluorescence is in the parafoveal region and decreases
peripherally– IF RPE missing or blocked Æ appears dark (disc, under BV)
• Decreased FAF @ fovea center due to luteal pigment
Plaquenil – what’s new?Reduced Autofluorescence?y Normal central macular luteal pigmenty Where no RPE is found (the ONH)y Where RPE is blocked (vessels)
y Æ Intraretinal or subretinal hemes, exudatey RPE loss or atrophy
y Æ Hereditary retinal dystrophies
y Media opacities

Plaquenil – what’s new?Increased Autofluorescence?• Excessive RPE LF accumulation
–ÆMac degeneration, Stargardts, Best’s Disease, Vitelliform Dystrophies
• Drusen within the RPE• Optic disc drusen• Macrophages containing LF in subretinal
space–Æ Overlying a choroidal tumor
Systemic Lupus Erythematosus (SLE)
SLE Qualities• Considered an “imitator”
– Symptoms & clinical course vary widely– Mimics other conditions
• Chronic autoimmune/ inflammatory - can affect:– Skin– Kidneys– Joints– Nervous system– Blood, eyes and other organs

Systemic Lupus Erythematosus (SLE)
Incidence and Prevalence• In the U.S., SLE prevalence is ~ 1 in 2,000
– An estimated 1.5 million Americans have a type of SLE
• Frequency varies by ethnicity• 2 to 3 X more prevalent in non-whites:
– Blacks, Asians, Hispanics & Native Americans
• According to the Lupus Society of America:– Peak incidence: 80% develop SLE between ages 15-
45– Predominant among females (90% are female)

Systemic Lupus Erythematosus (SLE)
SLE and Mortality [1]• Five-year survival rate of patients has increased
from 50% in the 1950s to between 91% to 97% today
• Mortality rates are higher among SLE pts with– Infectious complications– Seizures– Lupus nephritis and renal failure
• [1] Gill JM, Quisel AM, Rocca PV, et al. Diagnosis of systemic lupus erythematosus. American Family Physician 2003; 68(11) : 2179-86
Systemic Lupus Erythematosus (SLE)
Etiologyy Complex disease: Unknown etiology - a combination of
genetic, environmental and hormonal factors Æ Likely initiated by a trigger
y Trigger may be bacterial infectiony Trigger may be viral infection
y Flares associated with periods of significant hormonal changes:y Pregnancyy Initiation of hormone replacement therapy
Systemic Lupus Erythematosus (SLE)
Pathophysiology
y In SLE, autoantibody production is directed at molecules on the cell surface, molecules in the cytoplasm and in the nucleus, coagulation factors, and IgG.[2]
y This leads to immune complex formation
[2] Mok CC, Lau CS. Pathogenesis of systemic lupus erythematosus. J ClinPathol 2003;56:481-90

Systemic Lupus Erythematosus (SLE)
Disease Process • Initially = flu-like syndrome:
– Fatigue, fever, weight loss, and muscle & joint pain
• Pathology of SLE Æ Vascular abnormalities & inflammation– Leads to immune complex deposition Æ
occlusive vasculopathy Æ vasculitis
Systemic Lupus Erythematosus (SLE)
Disease Process • As SLE progresses, complications become more
diverse and severe

Systemic Lupus Erythematosus (SLE)
Disease Process – what causes it?
• While a female predilection is clear, endogenous sex hormones have an unknown role in disease predisposition and activity.
• The concordance rate of the disease is 2-9% in dizygotic twins and 24-65% in monozygotic twins.[3]
[3] Sullivan KE. Genetics of systemic lupus erythematosus: clinical implications. Rheum Dis Clin North Am 2000;26:229-56.
Systemic Lupus Erythematosus (SLE)
Triggers
y Ultraviolet lighty Pregnancy/ HRT initiationy Infectionsy Medications
y hydralazine- Apresolineanti-hypertensive
y procainamide-Procan anti-
arrhythmic
y Cough Remedies
y Stress/Overworky Acute emotionsy Injuriesy Surgeriesy Skin allergiesy Immunizationsy Laxativesy Stopping Meds
Systemic Lupus Erythematosus (SLE)
Ocular Manifestationsy Occur in ~ 15% of patients with SLE
y Occur more frequently in pts who have concurrent systemic disease
y Ocular complications variable
y Children with SLE may have a higher risk (~35%) of ocular manifestations
Systemic Lupus Erythematosus (SLE)
Common symptoms – Initial flu-like syndrome…
• Fatigue, Fever• Weight loss• Muscle and joint pain
Clinical Signs– Malar Rash, Hives– Sores on the skin and in mouth – Alopecia– Blood in Urine
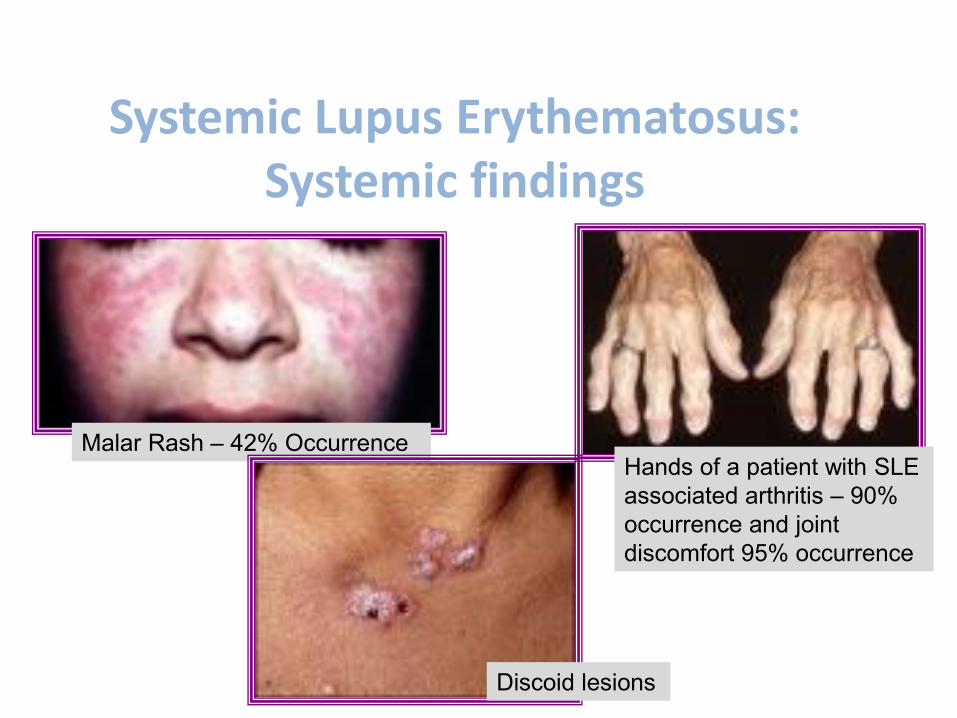
Systemic Lupus Erythematosus: Systemic findings
Hands of a patient with SLE associated arthritis – 90% occurrence and joint discomfort 95% occurrence
Malar Rash – 42% Occurrence
Discoid lesions

Systemic Lupus Erythematosus: Systemic findings
Malar Rash
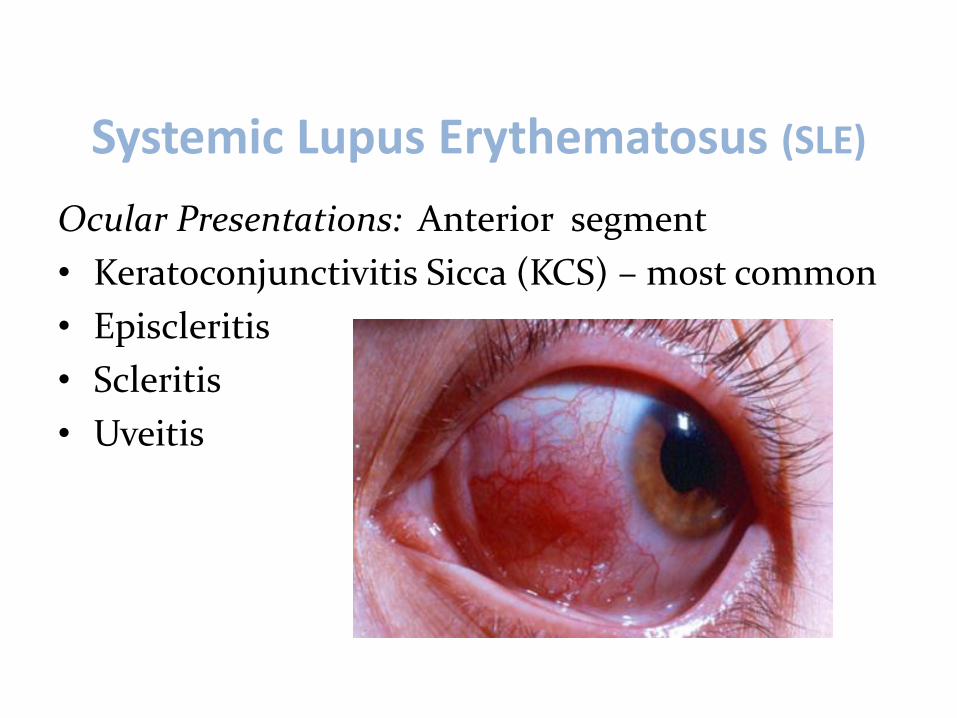
Systemic Lupus Erythematosus (SLE)
Ocular Presentations: Anterior segment• Keratoconjunctivitis Sicca (KCS) – most common• Episcleritis• Scleritis• Uveitis
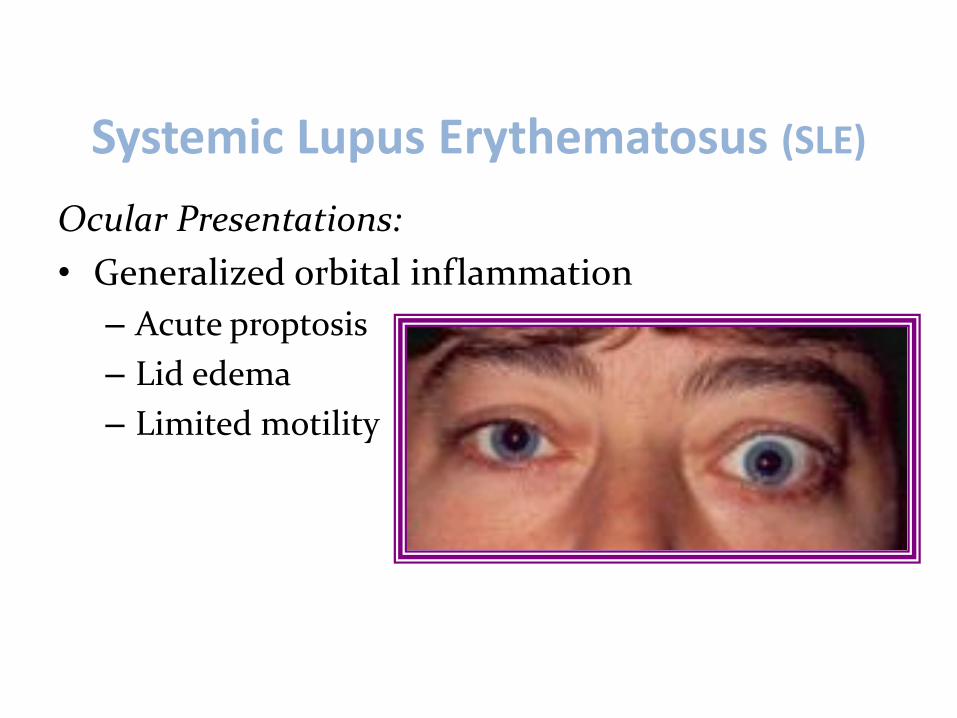
Systemic Lupus Erythematosus (SLE)
Ocular Presentations:• Generalized orbital inflammation
– Acute proptosis– Lid edema– Limited motility
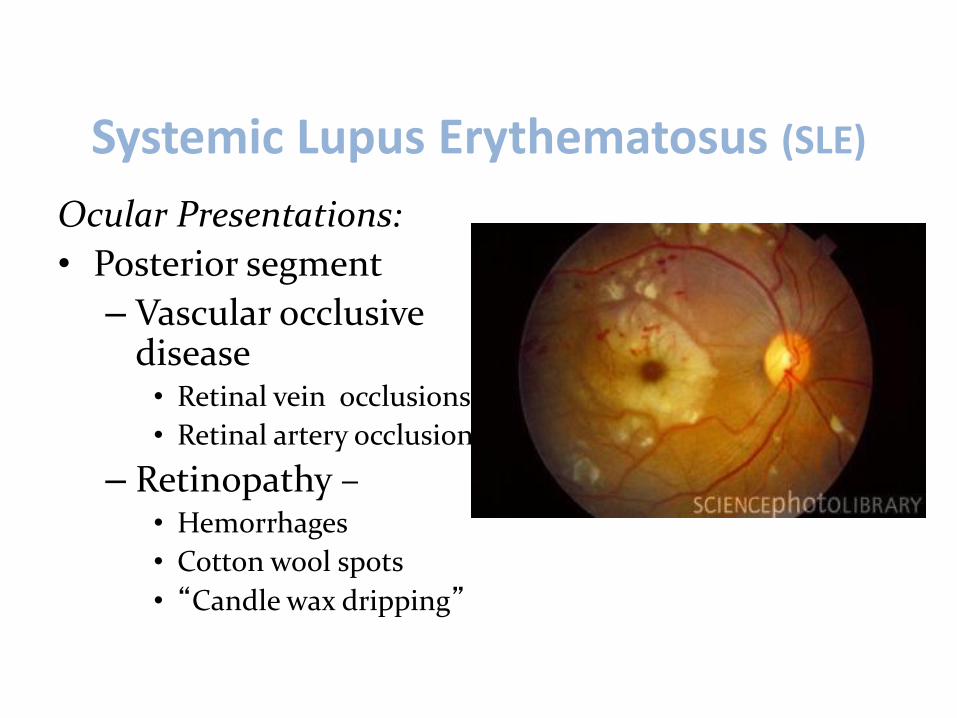
Systemic Lupus Erythematosus (SLE)
Ocular Presentations:• Posterior segment
– Vascular occlusive disease• Retinal vein occlusions• Retinal artery occlusion
– Retinopathy –• Hemorrhages• Cotton wool spots• “Candle wax dripping”
Systemic Lupus Erythematosus (SLE)
Making the Diagnosis
y Based on presence of at least four of eleven diagnostic criteria established by the American College of Rheumatologyy Symptoms DO NOT need to be concurrent
y Serologic testing (ANA) may be beneficial y Æ Not necessary for Dx
y Lab tests may help in diagnosis & management (monitored)

SLE: Diagnosis - Table One
1 Malar Rash –“Butterfly” rash
Flat or raised rash across cheeks & nose –persistent
2 Discoid Rash Raised red patches noted on the skin with associated scaling; atrophic scarring may arise
3 Photosensitivity Abnormal sensitivity to light, resulting in development of a skin rash or an increase in dermatologic response
4 Ulcers Noted in mouth or nasal passage
5 Arthritis Requires two or more peripheral joints being involved; non-erosive to bone but characterized by tenderness and swelling
6 Serositis Inflammation of the lining of the lungs or heart
(1-6 out of 11)

SLE: Diagnosis - Table One
7 Renal Disorder Protein in urine and/or abnormal elements in the urine
8 Neurologic Disorder Psychosis and/or seizures in the absence of metabolic conditions or drugs that might be causative
9 Hematologic Disorder Noted on two or more occasions: Leukopenia or lymphopenia. Also, hemolytic anemia or thrombocytopenia in the absence of causative drugs.
10 Immunologic Disorder False positive on syphilis test (VDRL); positive anti-double stranded anti-DNA test, anti-Sm test, lupus anti-coagulant or antiphospholipid antibody
11 Antinuclear Antibody (ANA)(hydralazine, isoniazid, procainamide, and some anticonvulsants)
Positive test for ANA in the absence of drugs known to cause a positive response
(7-11 out of 11)
SLE: Diagnosis – About ANA
Antinuclear antibody (ANA):• Screener Æmost useful to rule out SLE
•Due to high sensitivity and low specificity
•Antinuclear antibodies present in > 95% of SLE pts at some point
To monitor the status of condition:•CBC, C3, C4, (complement 3&4), Anti-nDNA and Urinalysis are primarily used
•Creatine clearance monitored for status of kidney disease
Systemic Lupus Erythematosus (SLE)
Treatment• There currently is no cure for SLE so goal of
therapy is:– Alleviate symptoms– Prolong remissions– Reverse immune dysregulatoin– Prevent organ damage
Systemic Lupus Erythematosus (SLE)
Treatment• First-line drugs include NSAIDs &
corticosteroids– Have long been used for controlling symptoms
• Second-line drugs – Disease-modifying anti-rheumatic drugs
(DMARDs):• Suppress immune system
– Biologic response modifiers (BRMs):• Influence activity of cytokines
Systemic Lupus Erythematosus (SLE)
New Medical Options – initially off label for SLE• “New” area of drugs anti-TNF (tumor necrosis factor
blocker)- inhibit abnormal B cell activity – AdalimumabÆHumira– EtanerceptÆEnbrel– InfliximabÆRemicade
• Approved 1st line therapy for RA and off label for SLE
• Several forms of treatments for autoimmune conditions involve reducing the number of a patient’s B cellsÆrituximab (Rituxan®, developed by Genentech) – Approved 1st line therapy for RA, used in non-Hodgkins
lymphoma and has been in trials for Lupus
Juvenile Rheumatoid Arthritis (JRA)
Rheumatologic disease - Incidence & Risks• Also called Juvenile Idiopathic Arthritis
– 50,000 US Kids– Different than adult RA
• Types, associated serology/testing and presentations
• Psoriatic arthritis and undifferentiated may also fall into this general category
• Typical signs Æ Soreness of joints/swelling, High fevers (spike @ night) & resolve, rashes that appear & disappear on body
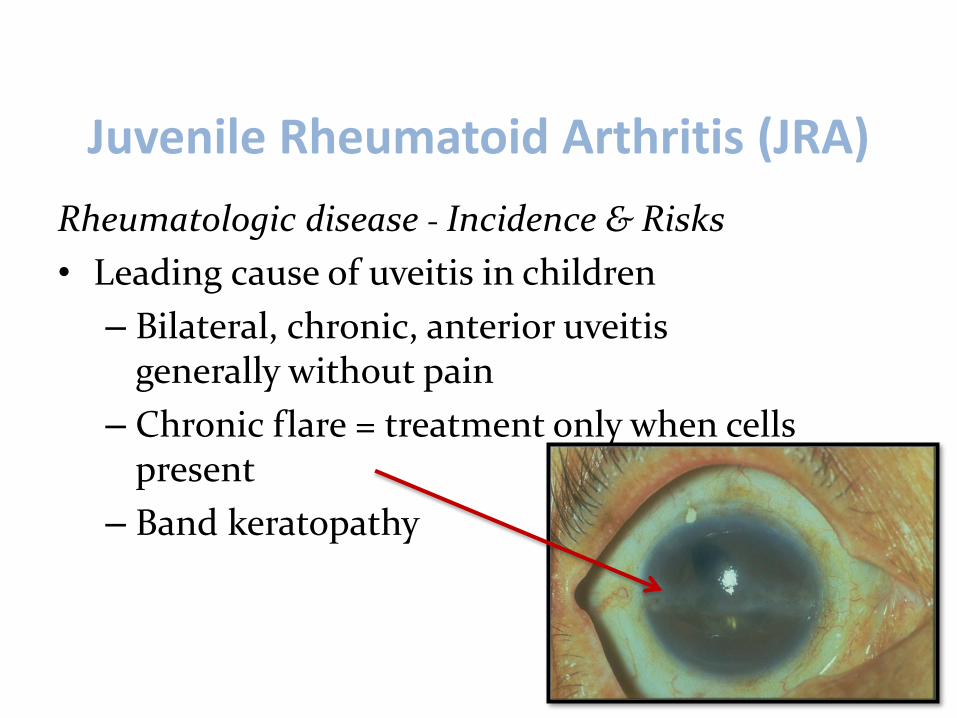
Juvenile Rheumatoid Arthritis (JRA)
Rheumatologic disease - Incidence & Risks• Leading cause of uveitis in children
– Bilateral, chronic, anterior uveitis generally without pain
– Chronic flare = treatment only when cells present
– Band keratopathy
Juvenile Rheumatoid Arthritis (JRA)Rheumatologic disease - Incidence & Risks
• High risk– Females, Pauciarticular (4 or less joints
involved), (+) ANA, Chronic asymptomatic iridocyclitis
• “Better pattern”– Males, Polyarticular (5 or more joints
involved), (+) HLA-B27, Acute recurrent uveitis
JRA is actually a group of diseases that have chronic joint inflammation in common
Juvenile Rheumatoid Arthritis (JRA)
JRA Different types:• Type I
– Pauciarticular, (-)RF, (+)ANA, female (4:1), without sacroilitis & onset by age 4
• Type II (~50% of patients with JRA)
– Pauciarticular, (-)RF, (-)ANA, (+)HLA-B27, slight male, sacroilitis common, onset by 8
• Type III– “Childhood” spondyloarthropathy Æ acute,
unilateral, self-limited ant. uveitis in males > than 12yo; (+)HLA-B27
Juvenile Rheumatoid Arthritis (JRA)
JRA - Variant: Still’s Disease
• 20% of all JRA patients
• Systemic onset– Fever, Rash, Lymphadenopathy– Can affect Heart, Spleen and Liver
• RARE to have uveitis
Juvenile Rheumatoid Arthritis (JRA)
Etiology Considerations
Common Signs and Symptoms• Pain & discomfort of the joints – young person• Disfigurement of joints• Some will complain with ocular findings
– Eye pain– Others will have uveitis but minimal discomfort

Juvenile Rheumatoid Arthritis (JRA)
Common Signs and Symptoms
Juvenile Rheumatoid Arthritis (JRA)Ocular Manifestations• Common findings
– UveitisWith age:– Band keratopathy– Cataracts/PSC– Glaucoma
• High risk for complications– Posterior synechiae– Often end up with VA 20/200 or worse
Juvenile Rheumatoid Arthritis (JRA)
JRA – Uveitis treatment• Topical steroid/mydriatics first• Periocular injections• Oral steroids last choice
Making the diagnosis• Need all tests to categorize
– Rheumatoid Factor (RF)– Knee X-ray– ANA– HLA-B27

Juvenile Rheumatoid Arthritis (JRA)
JRA – Treatment• Main goal:
– Help patient live as normal a life as possible– Must address all aspects of the disease
• medical problems and complications• physical functioning• school performance• social and emotional adjustment
• First line, NSAIDS (takes ~ 4 weeks to get affect)– Secondary complications – stomach upset, etc– NO ASPIRIN

Juvenile Rheumatoid Arthritis (JRA)
JRA – Treatment• Cox-2 inhibitors (Vioxx) was approved by FDA
– Less stomach upset but…. Recall due to heart issues
• DMARDs – interfere with immune processes that cause inflammation– Do not work for all patients with JRA– May take several months to reach full effect
• May be “bridged” with anti-inflammatory
• BRMs - Newer, specialized type of immunosuppressive

Juvenile Rheumatoid Arthritis (JRA)
JRA – Treatments inhibit inflammatory cascade…• Methotrexate
– Given as an Injectable or oral preparation– Used at night and the usual recommended starting dose is 7.5 - 10
mg per week and increasing dose versus response to 15 mg / week– The drug takes approximately 4-6 weeks for a response – Often concurrent use of Folic Acid
• Luflunomide (Arava)– Works in a similar fashion to methotrexate and is similar in both
response, and potential side effect
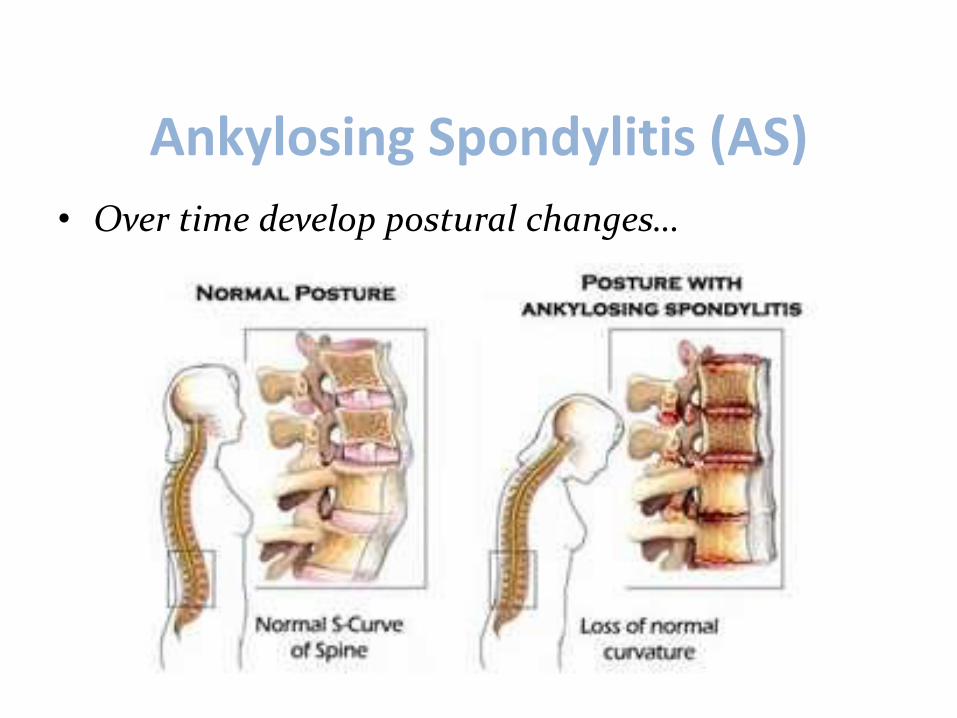
Ankylosing Spondylitis (AS)Rheumatologic disease - AS qualities• What does ankylosing spondylitis mean?
– Type of arthritis with chronic inflammation of the spine & sacroiliac joints
– Over time, chronic spinal inflammation (spondylitis) can lead to a complete “cementing together” (fusion) of the vertebrae, a process called ankylosis.
– Ankylosis causes total loss of mobility of the spine
• Differences in this condition versus arthritis
Ankylosing Spondylitis (AS)Rheumatologic disease - Incidence & Risks• Peak incidence: Between ages 20 and 30 years
• Predominant among Males 3x > Female
• Anterior uveitis– 1/3 of patients, 4/10 have recurrence– Eye pain, red and watery eyes, blurred vision
• Inflammation/pain along spine, ribs, shoulder blades, hips and thighs
Ankylosing Spondylitis (AS)
Etiology/ Common signs and symptoms• Joint stiffness that IMPROVES with activity
Worse first thing in am and after rest…– Males = lower back– Females = hip or shoulder aches
Ankylosing Spondylitis (AS)
• Over time develop postural changes…
Ankylosing Spondylitis (AS)
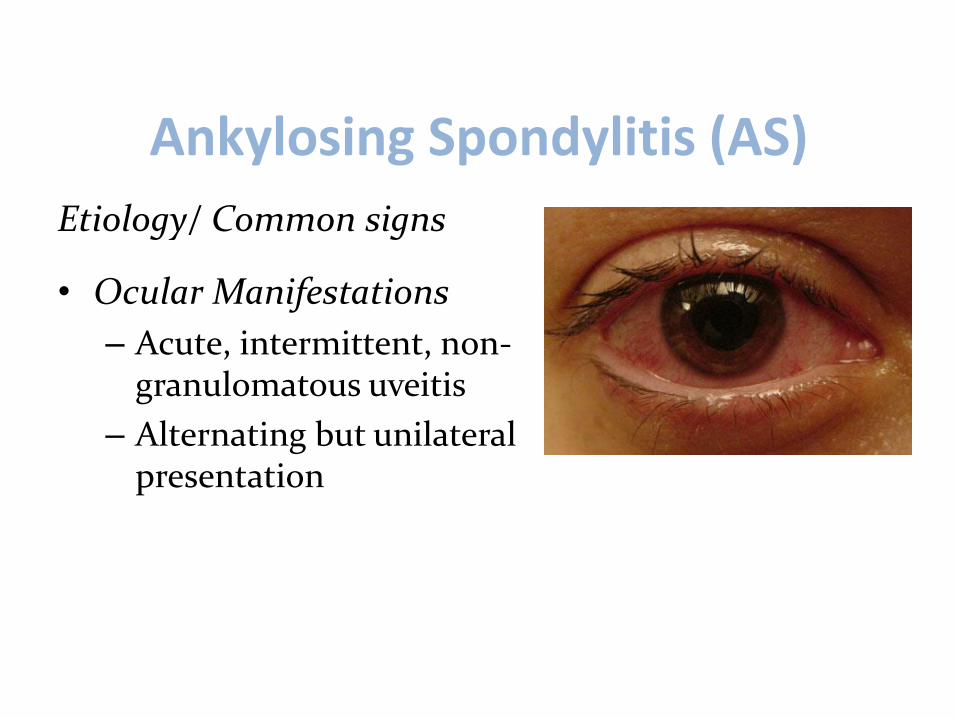
Etiology/ Common signs
• Ocular Manifestations– Acute, intermittent, non-
granulomatous uveitis– Alternating but unilateral
presentation

Ankylosing Spondylitis (AS)Making the diagnosis• Check family history• X-ray - Sacroiliac joint “blurred” initially; then sclerosis• HLA- B27 = ~88 to 93% (versus 6% of gen. pop.)• ESR (limited)
TreatmentNonsteroidal Anti-inflammatory Drugs (NSAIDs)• Including diclofenac (Cataflam, Voltaren), ibuprofen (Advil, Motrin),
ketoprofen (Orudis), naproxen (Aleve, Naprosyn), piroxicam (Felden), etodolac (Lodine), Indomethacin (Indocin), Oxaprozin (Daypro), nabumetone (Relafen), and meloxicam (Mobic)

Ankylosing Spondylitis (AS)TreatmentCOX-2 inhibitors (Celebrex, Arcoxia)• Less risky to GI than regular NSAIDS • Pulled by FDA (Vioxx and Bextra)
DMARDs• Clinical trials of sulfasalazine (Azulfidine) have shown benefits• Methotrexate is useful in some patients
– The remaining DMARDs have not been well studied in ankylosing spondylitis
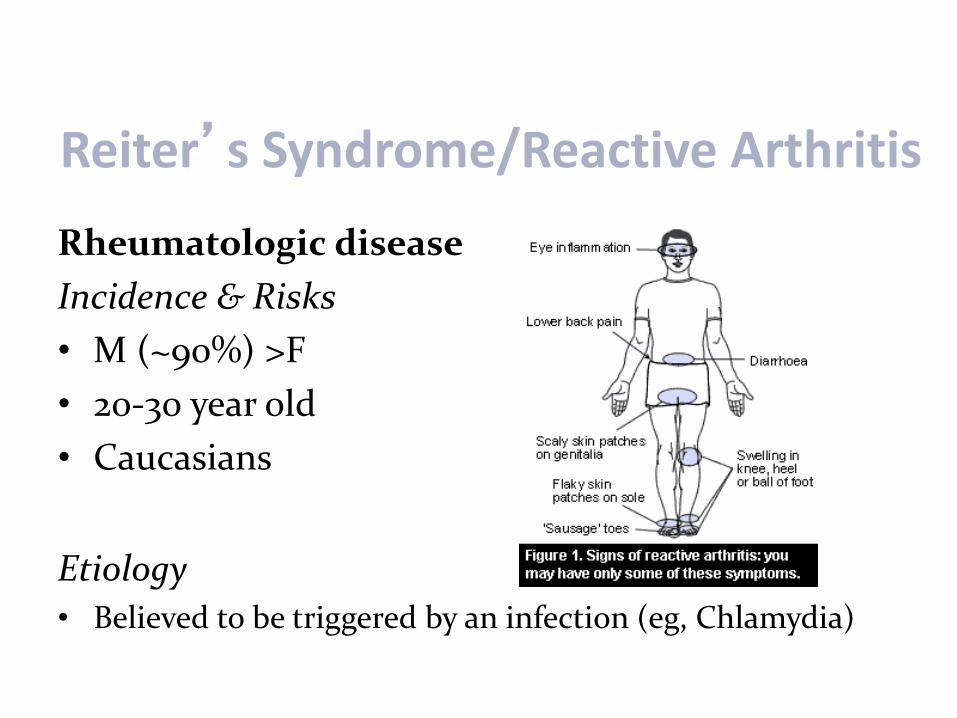
Reiter’s Syndrome/Reactive Arthritis
Rheumatologic disease Incidence & Risks• M (~90%) >F• 20-30 year old• Caucasians
Etiology• Believed to be triggered by an infection (eg, Chlamydia)

Reiter’s Syndrome/Reactive Arthritis
Common Signs and Symptoms• Triad -generally not all seen at same time:
– Urethritis – Polyarthritis: ~80 to 94%– Conjunctivitis – mucopurulent
• More common than anterior uveitis
• PLUS, a variety of other symptoms…
Reiter’s Syndrome/Reactive Arthritis
Common Signs and Symptoms• A variety of associated findings:
– Arthritis –inflammation of large, weight bearing joints (ankles/knees)
– Tendonitis - especially heel– Skin and mucous membrane complications –
rash– Rash on toes/feet

Reiter’s Syndrome/Reactive Arthritis
Ocular Manifestations• Conjunctivitis – mucopurulent
– More common than anterior uveitis
• Acute, intermittent, non-granulomatous iritis– Mild iridocyclitis

Reiter’s Syndrome/Reactive Arthritis
Making the diagnosis1. Joint (knee) X-ray2. Urethral cultures3. (+) HLA-B27 = 50 to 80% seropositive
Treatment• Traditionally self-limiting, 3 to 12 month
– >50% may have relapsing or chronic disease