October 2016 telehealth tuesday 3 three part series
72
Nancy A. Roget, MS Technology-Based Interventions: Extending the Reach of Organizations and Practitioners Help ! Talk with me
-
Upload
mikewilhelm -
Category
Data & Analytics
-
view
565 -
download
1
Transcript of October 2016 telehealth tuesday 3 three part series
PowerPoint Presentation
Nancy A. Roget, MS
Technology-Based Interventions:Extending the Reach of Organizations and PractitionersHelp!Talk with me
1
understand the benefits, ease of use, and clinical application to enhance behavioral services AND This podcast is designed to introduce you to Technology-Based Interventions in order to help participants be aware of the positive and negative factors that impact adoption by practitioners and organizations
This is the goal for this training. Please review the goal with the participants. 2
This training is not about identifying devices and platforms to be used in the delivery of technology-assisted services.
Please make these points in this training workshop. Participants may ask for recommendations for technology platforms or devices and it is important not to give advice as it is outside the scope of this training and most presenters.Technology-assisted treatment and recovery support services can be delivered using a variety of devices and platforms for example, telephone; videoconferencing; text messaging; and cell phone apps just to name a few. This training does not focus on how to choose the right device and/or platform, or reimbursement issues related to providing technology-based services. If you are interested in obtaining this information, contact the National Frontier and Rural Addiction Technology Transfer Center (NFAR ATTC).
Neither the NFAR ATTC nor the trainer presenting today endorse or promote the use of any specific technology application mentioned in this training. All technology applications are discussed as examples of available resources only. The NFAR ATTC does not guarantee that any of the technologies discussed meet federal, state, or local regulations. Please consult with an attorney, your institutions HIPAA compliance officer, and/or your local licensing agency before using any technology for clinical or recovery support purposes.
3
OutlineUse of TechnologyDefinition and Use of Technology-Based InterventionsOrganizational, Staff, and Patient Issues with TBIsModels of TBIsResearch on TBIsInteractive Voice Response (IVR)VideoconferencingAppsTexting
4
Technology has the potential to narrow the access gap to behavioral healthinterventions and reduce health disparities in disadvantaged and hard-to-reach populationsGibbons et al., 2011
In addition, technology can increase access to healthcare services for individuals who traditionally have had difficulty receiving services. This slide starts the discussion on the benefits of technology-based care.
SourceGibbons, M. C., Fleisher, L., Slamon, R. E., Bass, S., Kandadai, V., & Beck, J. R. (2011). Exploring the potential of web 2.0 to address health disparities. Journal of Health Communication, 16(sup1), 77-89, DOI: 10.1080/10810730.2011.5969165
Seven billion people (95% of the global population) live in an area covered by a mobile-cellular network By the end 2016, 3.9 billion people (53% of the worlds population) will not be using the InternetInternational Telecommunications Union, 2016
The point of this slide is to demonstrate the diffusion of cell phone use in the world. Although 95% of the worlds population live in an area covered by a cellular carrier, over half of the are not using the Internet. These technology use data have implications for which technologies may be more accessible for patients. For example, this may explain the popularity of texting interventions.
SourceInternational Telecommunications Union. (2016). ICT Facts and Figures 2016. Retrieved from http://www.itu.int/en/ITU-D/Statistics/Pages/facts/default.aspx6
In a national sample of adults who had smartphones or tablets36% had mHealth apps on their devices Among those with apps, 60% reported the usefulness of mHealth apps in achieving health behavior goals, 35% reported their helpfulness for medical care decision-making38% reported their usefulness in asking their physicians new questions or seeking a second opinionBhuyan et al., 2016
This article discusses a study that was done to determine the use of mobile health applications for health seeking behavior. Over one-third of adults had mhealth apps on their devices, while more than half thought the apps were helpful in meeting their health goals and assisted them in making health care decisions. Finally, roughly 40% thought mhealth apps helped them ask new questions of their doctors, especially when seeking a second opinion.
SourceBhuyan, S., Lu, N., Chandak, A., Kim, H., Wyant, D., Bhatt, J., Kedia, S., & Chang, C. F. (2016). Use of mobile health applications for health-seeking behavior among US adults. Journal of Medical Systems, 40(153). doi: 10.1007/s10916-016-0492-7
7
Technology-based behavioral health interventions, which involve the delivery of evidence-informed practices via computers, web-based applications, mobile phones, wearable sensors, or other technological platforms, are rapidly being developed.Marsch, 2012; Carroll & Rounsaville, 2010DEFINITION
There is extensive literature showing the use and effectiveness of technology-based interventions in other disciplines. Several different terms are used in the literature (e.g., digital health technologies, technology-assisted care, e-health, mhealth, etc.). The term used for this training curriculum will be technology-based interventions.Currently, there are still technology-based interventions that are downloaded as software on individual computers at healthcare sites. However, most computer-based interventions are accessed through a web portal that includes a log-in. Health care providers pay a licensing fee and then give patients access to these interventions while receiving services. Web-based interventions now include different platforms or devices (computers, mobile phone, and tablets). Think of it this way - right now your bank probably offers online banking. How you conduct online banking using whatever tools you have available doesnt matter. The issue is that you can do your banking online.
SourcesCarroll, K. M. & Rounsaville, B. J. (2010). Computer-assisted therapy in psychiatry: Be brave-Its a new world. Current Psychiatry Reports, 12(5), 426-432.Marsch, L. A. (2012). Leveraging technology to enhance addiction treatment and recovery.Journal of Addictive Diseases, 31(3), 313318.8
the application of behavioral and psychological intervention strategies through the use of technology features to address behavioral, cognitive and affective targets that support physical, behavioral and mental healthsBehavioral Intervention Technologies (BITs) Burns & Mohr, 2012
Digital Health Technologies (DHTs) include assessments and interventions delivered via computer, Internet, mobile phone, and wireless or wearable device technologiesMuench, 2015
There are several different terms and definitions for TBIs. This slide includes two examples of terms and definitions. Each field or specialty may have their own and it is important to remind participants of this fact. This curriculum uses the term TBI as many of the substance use disorder researchers use this term.
Ask participants what terms and definitions are used in their fields/disciplines.
SourcesBurns, M. N. & Mohr D. C. (2012). eHealth, Telehealth, and Telemedicine. In M.D. Gellman & J.R. Turner (Eds). Encyclopedia of Behavioral Medicine. New York: Springer.Muench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
9
Technology-Based Interventionsmay consist of text, audio, video, animations, and/or other forms of multimediause information from medical records,physiological data capture devices, or other sourcesmay be interactively customized, or tailored, to an individual users needsAronson, Marsch, & Acosta, 2013
This definition of TBIs helps describe the features and activities included in many of the interventions. An important point to include is that research has found that interventions that provide customized or tailored feedback to individual users needs have a greater impact on behavior.
SourceAronson, I. D., Marsch, L. & Acosta, M. C. (2013). Using findings in multimedia learning to inform technology-based behavioral health interventions. Translational Behavioral Medicine, 3(3), 234-243.10
Technology-based interventions range from simple text-based reminders to complex interactive computer-based counseling interfaces, to smartphones with GPS and biomedical sensors.
Simoni et al., 2015
This slide makes the point that there are a range of TBIs, from sophisticated to simplistic, and all have different purposes. It is important to understand the features of each. New wearable technologies are also in development, including t-shirts and bracelets (biomedical sensors), that provide additional patient information.
SourcesDayer, L., Heldenbrand, S., Anderson, P., Gubbins, P.O., & Martin, B. C. (2003). Smartphone medication adherence apps: Potential benefits to patients and providers. Journal of the American Pharmaceutical Association, 53, 17281.Kurth, A. E., Spielberg, F., Cleland, C. M., Lambdin, B., Bangsberg, D. R., Frick, P. A., et al. (2014). Computerized counseling reduces HIV-1 viral load and sexual transmission risk: Findings from a randomized controlled trial. Journal of Acquired Immune Deficiency Syndrome, 65, 61120. Lester, R. T., Ritvo, P., Mills, E. J., Kariri, A., Karanja, S., Chung, M. H., et al. (2010). Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): A randomised trial. Lancet, 376, 18381845. Simoni, J. M., Kutner, B. A. & Horvath, K. J. (2015). Opportunities and challenges of digital technology for HIV treatment and prevention. Current HIV/AIDS Reports, 12(4), 437-40.11
Jones et al., 2013
The rapid technological advancements and developing evidence base supporting these approaches have effectively positioned technology-based interventions at the forefront of behavioral health care innovation.
The development of new technologies and the publics use and adoption of technology has driven the development of technology-based interventions (TBIs) in many different healthcare fields.
SourceJones, D. J., Forehand, R., Cuellar, J., Kincaid, C., Parent, J., Fenton, N., & Goodrum, N. (2013). Harnessing innovative technologies to advance childrens mental health: Behavioral parent training as an example.Clinical Psychology Review, 33(2), 241-252. 12
To date, more than100 different technology-based interventions have been developed for and behavioral health problems Klein et al., 2012; Moore et al., 2011
Technology-based interventions have been around for some time and used to treat a variety of physical and mental health disorders (e.g., cancer, diabetes, heart disease depression, anxiety, poor nutrition, and sexual risk behaviors) with positive outcomes (Klein, et al., 2012; Moore, et al., 2011). However, the literature for using computer-based interventions to treat substance use disorders is more recent. (See the reference section for full citations).
SourcesKlein, A. A., Slaymaker, V. J., Dugosh, K. L., & McKay, J. R. (2012). Computerized continuing care support for alcohol and drug dependence: A preliminary analysis of usage and outcomes.Journal of Substance Abuse Treatment, 42(1),25-34. doi: 10.1016/j.jsat.2011.07.002Marks, I. M., Cavanagh, K., & Gega, L. (2007). Computer-aided psychotherapy: Revolution or bubble? The British Journal of Psychiatry, 191(6), 471-473.Moore, B. A., Fazzino, T., Garnet, B., Cutter, C. J., & Barry, D. T. (2011). Computer-based interventions for drug use disorders: A systematic review.Journal of Substance Abuse Treatment, 40(3),215-223.13
Technology-Based Interventions have been used to augment care and support forCancer DiabetesHeart DiseaseMood Disorders Depression/AnxietyPoor NutritionSexual Risk Behaviors
The conditions listed here have used technology-based interventions to augment or extend care and support. The citations below show that many of these TBIs have been in use for over ten years. Communicate this point to participants. (See the reference section for full citations)
Cancer - Gustafson, D. H., McTavish, F. M. et al. (2005). Diabetes - Glasgow, R. E., Nutting, P. A. et al. (2005); Williams, G. C., Lynch, M. et al. (2007); Montani, S., Bellazzi, R. et al. (2001). Heart Disease - Verheijden, M., Bakx, J. C. et al. (2004) Mood Disorders - Farvolden, P., Denisoff, E. et al. (2005)Depression/Anxiety - Cavanagh, K., & Shapiro, D. A. (2004); Kaltenthaler, E., Parry, G. et al. (2008); Reger, M. A. & Gahm, G. A. (2009); Spek, V., Cuijpers, P. et al. (2007)Poor Nutrition - Portnoy, D. B., Scott-Sheldon, L. A. J. et al. (2008) Sexual Risk Behaviors - Ybarra, M. L., & Bull, S. S. (2007); Marsch L. A. & Bickel W. K. (2004)
14
Asch et al., 2012, p. 1Even chronically ill patients spend only a few hours per year with a doctor or nurse, leaving at least 5,000 hours per year in which they are engaged in other health-related behaviors
Think about it
The point of this slide is to remind participants how much time patients are on their own to manage their health conditions. This is why support groups are popular with many patients and why technology-based interventions can meet patient needs for support, education, monitoring, etc.
Source Asch, D. A., Muller, R. W., & Volpp, K. G. (2012). Automated hovering in health care: Watching over the 5000 hours. New England Journal of Medicine, 367(1), 1-3.15
That leaves a lot of time for patients toAsch et al. 2012, p. 1take prescribed medications;follow other medical advice;decide what to eat and drink; orwhether to smoke, drink, or take drugs All of these choices can profoundly influence their health
This slide continues the point about patient hovering and that patients spend the majority of their time managing their health on their own (outside of the practitioners office). Medication reminder text messages and online support groups are just two examples of technology-based interventions.
Source Asch, D. A., Muller, R. W., & Volpp, K. G. (2012). Automated hovering in health care: Watching over the 5000 hours. New England Journal of Medicine, 367(1), 1-3.
16
TBIs can address barriers to accessing treatment in both rural and urban areas
Remind participants that travel time to healthcare services is not just an issue for patients living in rural or remote areas. Many patients who reside in urban areas also face travel issues (e.g., traffic jams, delays in public transportation, numerous changes with different buses and trains, etc.). In addition, travel related barriers also include costs and time away from work. For many patients who are unable to drive (e.g., individuals with alcohol use disorders whose license may have been revoked due to legal consequences; epilepsy) may place additional transportation demands on family members or friends. 17
Technology-based interventions also have the ability to lower consumer threshold for initiation of treatmentClarke & Yarborough, 2013
The message here suggests that technology may help patients get their foot in the door meaning that patients can test out treatment or support for their health-related issue without actually entering treatment or seeing a health care practitioner. Many health-related conditions especially behavioral health disorders carry stigma that serves as a barrier to entering treatment.
SourceClarke, G. & Yarborough, B. J. (2013). Evaluating the promise of health IT to enhance/expand the reach of mental health services. General Hospital Psychiatry, 35(4), 339344.18
Allow for on-demand access to therapeutic support outside of formal care settings anytime/anywhereMarsch, 2012
Technology-Based Interventions can provide support to patients during non-clinic hours. This is important as numerous studies have demonstrated that when given the opportunity, patients called phone lines to listen to educational modules on Intervoice Response Systems or accessed online educational modules during non-clinic times.
SourceMarsch, L. A. (2012) Leveraging technology to enhance addiction treatment and recovery. Journal of Addictive Disorders, 31(3), 313-318.
19
TBIs can Enable AnonymityMarsch, 2012
Many technology-based interventions allow patients to join online support groups or take online assessments and remain anonymous. Anonymity can be important to patients as many healthcare conditions are stigmatized, which can hinder help-seeking. Once again, this anonymity may help patients seek initial help, education, feedback on their conditions, thereby leading to receiving treatment or supportive services.
SourceMarsch, L. A. (2012) Leveraging technology to enhance addiction treatment and recovery. Journal of Addictive Disorders, 31, 313-318.
20
Technology-Based Interventionsfor Individuals with low problem severity who perceive barriers TBI may provide the optimal lower dose of treatment to foster service access may instill an enhanced sense of empowerment while still providing evidence-based careClarke &Yarborough, 2013
The main point of this slide reminds participants that TBIs can assist patients with low severity problems by providing a small dose of treatment which may help them enter treatment or provide resolution. Since most TBIs use evidence-based practices, patients may experience an enhanced sense of empowerment related to managing their health conditions or seeking formal assessment or treatment services.
SourceClarke, G. & Yarborough, B. J. (2013). Evaluating the promise of health IT to enhance/expand the reach of mental health services. General Hospital Psychiatry, 35(4), 339344.
21
As Fox (2013) suggests, the clinical value of technology lies not in its computing power but in its ability to connect providers to their patientsMuench, 2015
Finally, use this slide to remind participants that TBIs help practitioners connect with their patients, which carries significant clinical value. Recent studies have demonstrated that engaged patients have better outcomes and TBIs can be used to foster effective relationships.
SourceFox, S. (2013). Mobile health in context: How information is woven into our lives. Symposium at the University of Maryland, Pew Research Center, College Park, MD, October 22, 2013.
22
OrganizationalStaffPatientISSUES with TBIs
This is an introductory slide that identifies the new section - Issues with TBIs.23
3 Diffusion of Innovation Constructs Relative Advantage ComplexityCompatibility
Most relevant constructs to technology adoption researchVan Slyke et al., 2004; Corneille et al., 2014Rogers, 1995Adoption of Technology
The adoption of technology (innovations) has been studied by many researchers, with Everett Rogers work being some of the most well-known, especially in healthcare. While Rogers had five diffusion of innovation constructs, these three are the most relevant to technology adoption research.
SourceCorneille, M., Carter, L., Hall-Byers, N., Clark, T., & Young, S. (2014). Exploring user acceptance of a text-message based health intervention. 47th Hawaii International Conference on System Science.Rogers, E. M. (2003). Diffusion of Innovation. New York: The Free Press.Van Slyke, C., Belanger, F., & Comunale, C. (2004). Factors influencing the adoption of Web-based shopping: The impact of trust. Database for Advances in Information Systems, 35(2), 32-49.
24
Agencies with annual operating budgets of greater than $10 million reported significantly fewer barriersRamsey et al., 2016than those with budgets of $10 million or less
In this recent study conducted by Ramsey and colleagues, 260 care decision makers completed an open-ended question about perceived barriers to using technology at their behavioral health care agency. These care decision makers were employed by Member Agencies of National Council on Behavioral Health. This slide and the next highlight some the findings from this study, which focused on the budget size of the organizations and the number of patients served.Organizations with operating budgets of $10 million or more reported fewer barriers to adopting technology. This may be due in part to these organizations having more resources with which to purchase additional training for staff to assist with technology adoption. In addition, these larger organizations may be more familiar with making system-wide changes.
SourceRamsey, A., Lord, S., Torrey, J., Marsch, L., & Lardiere, M. (2016). Paving the way to successful implementation: Identifying key barriers to the use of technology-based therapeutic tools for behavioral health care. Journal of Behavioral Health Services Research, 43(54). doi:10.1007/s11414-014-9436-5
25
Agencies serving more than 3,000 patients per year reported significantly fewer implementation barriers than those serving less patients annually.Ramsey et al., 2016
This data point comes from that same study by Ramsey and colleagues regarding why some organizations are more likely to adopt technology than others when they provide similar services. Results suggested that organizations serving more than 3,000 patients per year reported fewer implementation barriers than those serving lower numbers of patients. One explanation for this difference could be that organizations serving larger numbers of patients may be more open to technologies that would help them more effectively manage/serve their patient caseloads.
SourceRamsey, A., Lord, S., Torrey, J., Marsch, L., & Lardiere, M. (2016). Paving the way to successful implementation: Identifying key barriers to the use of technology-based therapeutic tools for behavioral health care. Journal of Behavioral Health Services Research, 43(54). doi:10.1007/s11414-014-9436-5
26
How will technologies change how the provider does business?
Muench, 2015
Adoption of technology-based interventions will change how the provider or organization does business on numerous levels. The next slides discuss some the specifics regarding business practice changes.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
27
Most providers will need to re-structure operations to understand how technology will impact clinician workloadaccept e-mails or phone messages on work phonesdevelop on call lists or use peer specialists to manage alerts/requests for help and client check-ins if not automated (Muench, 2015)
The narrative on this slide comes from an excellent article by Frederick Munch. He suggests that when adopting TBIs, organizations will need to restructure operations and examine the impact on clinician workload. For example, an organization adopts a recovery support app for their patients with substance use disorders. This app allows the patient to send alerts to practitioners 24 hours a day, seven days a week. Policies and staffing patterns will need to be adjusted to respond to the services offered by the new technology.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.28
Adoption of New Technologyagencies should focus on integrating new procedures into existing workflowscreate new staff roles (e.g., project managers who will train staff and deal with resistance to or fear of integration)balance a DHTs financial costs against its potential rewardsunderstand how technology shifts certain roles and responsibilitiesMuench, 2015
This slide provides some specific recommendations for organizations that adopt new technology-based interventions for their patients. Review these recommendations and discuss with participants.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
29
Selection of appropriate training to increase staff confidence in navigating potentially foreign technologies is essential
Restructuring services related to the adoption of TBIs will require that the organization offer training to practitioners. To be most effective, training should be an ongoing process rather than a one-time event, and include peer mentors. When possible, videos or podcasts should be produced that staff members can refer to after training events. In addition, repetition is an important learning concept so offer training often.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
30
The most pressing staff concerns usually fall within the realms of level of comfort with the use of technology
Muench, 2015
This slide and the next slide go together. When discussing these slides, it might be helpful to return to Rogers Diffusion of Innovation constructs: relative advantage, complexity, and compatibility. If the technology being proposed for adoption is as easy to use as the current technology, if it produces better results, and its more efficient, then adoption rates will increase. In other words, if it is better, as easy to use, and saves time, practitioners comfort level will increase. Practitioners who are unfamiliar with or resistant to using technology may experience a more difficult time becoming comfortable. Ask participants to give examples of their current comfort level regarding a technology at work. In addition, the time burden can refer to the time it takes to learn a new technology (e.g., training, feedback on skills, new policies and procedures, etc.). This same narrative also appears on the next slide. The trainer can click through this first slide on comfort with technology and then go on to the time burden slide and then highlight both slides.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.31
Campbell et al., 2012
and the time burden
32This slide and the next slide go together. When discussing these slides, it might be helpful to return to Rogers Diffusion of Innovation constructs: relative advantage, complexity, and compatibility. If the technology being proposed for adoption is as easy to use as the current technology, if it produces better results, and its more efficient, then adoption rates will increase. In other words, if it is better, as easy to use, and saves time, practitioners comfort level will increase. Practitioners who are unfamiliar with or resistant to using technology may experience a more difficult time becoming comfortable. Ask participants to give examples of their current comfort level regarding a technology at work. In addition, the time burden can refer to the time it takes to learn a new technology (e.g., training, feedback on skills, new policies and procedures, etc.). This same narrative also appears on the next slide. The trainer can click through this first slide on comfort with technology and then go on to the time burden slide and then highlight both slides.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
a substantial portion of providers reported a lack of basic knowledge about how technologies can be used for behavioral health careRamsey et al., 2016
As the slide states, many practitioners may be unfamiliar with TBIs and how they are used in healthcare and behavioral health care settings. This lack of knowledge will make adoption and implementation efforts more difficult for organizations. In the following slides, this issue is discussed in greater detail regarding staff being worried that TBIs will replace them or that patient care will be compromised.
SourceRamsey, A., Lord, S., Torrey, J., Marsch, L., & Lardiere, M. (2016). Paving the way to successful implementation: Identifying key barriers to the use of technology-based therapeutic tools for behavioral health care. Journal of Behavioral Health Services Research, 43(54). doi:10.1007/s11414-014-9436-533
debunk fears cited by providers regarding the use of technologies compromised client care and job replacementRamsey et al., 2016
Due to lack of knowledge or exposure to TBIs, many practitioners have inaccurate perceptions about TBIs and their role in service delivery. The next slide on the clinician extender model helps address these fears by practitioners. Overall, TBIs enhance the work of practitioners, allowing them to deal with patients experiencing a crisis or higher level treatment-related activities. It is recommended that in TBI training, practitioners concerns are addressed.
SourceRamsey, A., Lord, S., Torrey, J., Marsch, L., & Lardiere, M. (2016). Paving the way to successful implementation: Identifying key barriers to the use of technology-based therapeutic tools for behavioral health care. Journal of Behavioral Health Services Research, 43(54). doi:10.1007/s11414-014-9436-534
In some cases, TBIs may change practitioners roles and work duties. Muench and colleagues (2013) found that although 80% of providers want to be alerted if their client is at risk of relapse, only 8% would want an immediate mobile alert. Muench, 2015
This slide makes the point that adoption and implementation of TBIs may impact the practitioners duties and require new work structures. For example, if an organization chose a TBI that included a patient panic button and, when used, it would contact the practitioner during off hours, so different work strategies/responses would need to be put in place. This particular survey of practitioners found that a majority wanted an alert if a patient was at risk of relapse-not just an immediate alert. Organizations adopting and implementing TBIs will need to address issues like the one raised in this study.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.35
36Clinician ExtendersBickel et al., 2008; Carroll & Rounsaville, 2010; Des Jarlais et al., 1999; Marsch, 2011allow providers to work at their highest level of training and focus on the most high need client issues
Serve as adjuncts to standard treatment; Save clinician time; Extend clinician expertise; Integrate other EBPs to provide additional services to clients with co-morbid conditions; Provide access to computerized smoking cessation programs or other health-related conditionsGiven the difficulty of being trained in every single EBP, computer-based Interventions can help save clinician time and extend their expertise. For example, most addiction treatment providers need to concurrently address clients use of nicotine while in substance abuse treatment. The following data support that point.Many computer-based interventions are designed to serve as an adjunct to treatment services, thereby extending the work of the clinician. For example, a computer-based intervention may be used instead of a group counseling session. The client works on a module, learns about drug refusal skills and practices them through a series of learning experiences rather than attending the group session. This allows the counselor to spend their time with clients who may be dealing with other more pressing problems or issues that require their immediate attention. The term clinician extenders appears in journal articles authored by Lisa Marsch, Warren Bickel, and Kathy Carroll. This is about helping counselors, not replacing them, as well as enhancing treatment services.The anonymity of this approach might be appealing to some individuals when dealing with substance abuse and other risk behaviors. These tools can have a significant public health impact by reaching frontier and rural areas, and may be used in a wide variety of settings such as: Web-based interventions offered in the homeCommunity organizations SchoolsEmergency rooms Health care provider officesMobile devicesSourcesBickel, W.K., Marsch, L.A., Buchhalter, A.R., & Badger, G.J. (2008). Computerized behavior therapy for opioid-dependent patients: A randomized controlled trial.Experimental and Clinical Psychopharmacology, 16(2), 132-143.Carroll, K.M. & Rounsaville, B.J. (2010). Computer-assisted therapy in psychiatry: Be brave-its a new world. Current Psychiatry Reports, 12, 426-432.Des Jarlais, D.C., Paone, D., Miliken, J. et al. (1999). Audio-computer interviewing to measure risk behaviour for HIV among injecting drug users: A quasi-randomised trial. Lancet, 353(9165), 1657-1661.Marsch, L. (2011). Technology-based interventions targeting substance use disorders and related issues: An editorial. Substance Use & Misuse, 46(1), 1-3.36
Patients Acceptability of Technologies
The next set of slides discuss patients acceptability of technologies and TBIs.37
Moore et al., 2011; Muench et al., 2013; Muench, 2015Current evidence demonstrates that patients use and are interested in using technologies as part of their treatment or continuing support
Three different journal articles highlight evidence that patients use technologies and are interested in using technologies as part of their treatment or continuing support. It is important to remind participants that they should not assume patients wouldnt be interested in using technology to receive services.
SourcesMoore, B.A., Fazzino, T., Garnet, B., Cutter, C.J., & Barry, D.T. (2011). Computer-based interventions for drug use disorders: A systematic review.Journal of Substance Abuse Treatment, 40,215-223.Muench, F., Weiss, B., Kuebis, A. & Morgenstern, J. (2013). Developing a theory driven text messaging intervention for addiction care with user driven content, Psychology of Addictive Behaviors, 27(1), 315-21.Muench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
38
Patients Issues Regarding Using Technologies for Treatment and RecoveryMake sure patients understand:technologies that may monitor them and their locationshow to use the technologieswhat to do in the case of emergencies and service problems
Muench, 2015
If an organization adopts and implements TBIs, it is essential that patients are provided training regarding how to use the technologies and what to do in case of emergencies or service problems. This informed consent-related training should include information regarding privacy, security, and confidentiality as many technologies, like mobile apps, may monitor patients and their locations.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
39
Other Technology Issues with ClientsMany clients change phone numbers or experience disruptions in their phone service which interferes with use of technology-based interventions.Approximately 20% of participants had their phone service turned off at least once over the course of a 5-week study as a result of nonpayment.Clients sharing phones with family members/others raises issues with privacy/security and confidentiality.Warn clients about technology failures and that their messages might not go through.Determine the percentage of clients that have access to smart phones before implementing technologyMuench, 2012; 2015
Discuss each bullet point on this slide with participants as there are important implications for practice.Many patients use pay as you go cell phones. However, there are inherent problems with these types of phones. First, there might be disruptions in service, which interferes with use of the technology-based interventions. Muench (2015) discovered that 20% of the participants in his study had their phone service turned off during a 5-week period. Next, at times, patients share phones with family members/others and so privacy, security, and confidentiality may be at risk. Inform patients about what they should do regarding technology failures. Finally, before adopting and implementing TBIs, ensure that a majority of patients have access to the proposed technology (e.g., proposing to use an app that is available on smartphone and tablets only).
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.40
Models of Integration for Technology-Based InterventionsBrief Intervention - particularly in settings where SUD treatment services are limited (e.g., primary care [FQHCs], mental health, etc.)Could improve motivation and/or readiness?Stand alone treatment - comprehensive service (up to 65 modules available) delivered over a structured period of time (e.g., 12 weeks)Clinician extender - administered as an adjunct to treatment whereby clinicians prescribe TBIs (or portions of) to enhance therapeutic intervention
Marsch, 2012
It is important participants understand that TBIs are used in different ways to enhance services or provide additional services. In some settings, TBIs provide additional screening services that practitioners dont have time to implement or possess the knowledge and skill to implement with fidelity to the EBP. For example, Therapeutic Education Services (TES), a web-based TBI, can be used as a stand alone treatment or an enhancement to current services. Examples of these different integration models for TBIs will be discussed in more detail later in this section.
SourceMarsch, L. A. (2012). Leveraging technology to enhance addiction treatment and recovery. Journal of Addictive Disorders, 31(3), 313318.
41
Examples of EBPs Used by TBIsCognitive Behavioral TherapyCommunity Reinforcement ApproachContingency ManagementMotivational EnhancementMotivational InterviewingBrief InterventionScreeningRelapse PreventionAronson, Marsh, & Acosta, 2013; Carroll & Rounsaville, 2010
Most TBIs use evidence-based practices (EBPs) along with a variety of learning and behavioral theories. It is important that practitioners understand which EBPs the TBI uses, especially when implementing a clinician extender model. Practitioners should be aware that many apps, especially those sold in the commercial App stores, typically are not based on EBPs.
SourcesAronson, D., Marsch, L. A., & Acosta, M. C. (2013). Using Findings in multimedia learning to inform technology-based interventions. Translational Behavioral Medicine, 3(3), 234243. Carroll, K. M. & Rounsaville, B. J. (2010). Computer-assisted therapy in psychiatry: Be braveits a new world. Current Psychiatry Reports, 12(5), 426432.
42
Four characteristics that help with implementationproducts ease of use eHealth interventions compatibility with the clinical settingpresence of tools that make it easier for the user to engage in therapeutic activitiesprovision of a feasible therapeutic pathway to growthBaumel & Muench, 2016
Successful implementation of TBIs can be attributed to these four characteristics. Ease of use and compatibility with the clinics setting are two of the most important characteristics. For example, a clinic should be aware of selecting a technology platform that is not user friendly for the staff and patients. This includes being too complex or adding a time burden.
SourceBaumel, A., Muench, F. (2016). Heuristic evaluation of ehealth interventions: Establishing standards that relate to the therapeutic process perspective. JMIR Mental Health, 3(1), e5. DOI:10.2196/mental.4563
43
Potential Benefits of TBIsCan be delivered with low cost or cost savingsAccessible in a wide array of settingsEasily exportableFidelity/replicability is assuredLess threatening in addressing sensitive topicsPermits more rapid diffusionIncrease adoption of science-based interventionsPermits expansion of treatmentMarsch, 2012
What are some potential benefits of using TBIs in substance abuse treatment? Lead as facilitated discussion
Other benefits:Requires active responding Can be readily modified Permits temporal flexibilityTailoring/Customization Readily Accomplished
SourceMarsch, L. A. (2012). Leveraging technology to enhance addiction treatment and recovery. Journal of Addictive Disorders, 31(3), 313-318.
44
Touch Points in Care: Which technologies can you integrate in different points in careIntake (Decision Support/Dashboard)Consent (What you need to know)Waiting Room (Use of video early and late)Early Treatment Enhancing Care Using TBIs (Engagement)Ongoing Care/Addressing Comorbidities Through TBIsPost Treatment
Intake (Decision Support/Dashboard) - During intake, patients can use web-based platforms or IVR devices that provide screening and assessment activities. The practitioner can use these results to augment their in-person screening/assessment activities as well as the patient can receive additional feedback on their condition or issue. Consent (What you need to know) - Instead of practitioners providing information to the patient regarding informed consent issues, a video or podcast audio can be created, followed by the practitioner discussing specific questions that the patient may have.Waiting Room (Use of Video early and late) - In addition, videos or websites may be created to more effectively use the patients time while sitting in the waiting room. Practitioners can provide patients with tablets or other devices if patients do not have access to their own devices.Early Treatment Enhancing Care Using TBIs (Engagement) - Providers can adopt apps or SMS systems that encourage and persuade patients about the benefits of remaining in treatment. These TBIs can help patients get used to tracking their condition and reporting data back to providers.Ongoing Care/Addressing Comorbidities Through TBIs - Since many patients have more than one health problem to address, TBIs could be used to address these other issues. For example, many behavioral health providers have purchased Texting Platforms for tobacco cessation. This helps patients with comorbidities and provides expertise that the provider might not have on staff.Post Treatment-Many apps, SMS texting programs, online support groups are designed to help patients as they transit to less intensive services. Providers could purchase these post treatment systems and integrate them in continuing care to help prevent relapse especially for chronic conditions.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
45
2010 Data*Addiction Provider (N=34)Patient(N=49)Would Use SMS System87%98%Provider Alerts80%78%Specific SMS Alerts8%---When would a system like this be most helpful?When treatment begins 27%34%During course of treatment51%22%After treatment11%44%*
Different Goals
This study compares providers and patients responses regarding use of Short Messages Service (SMS) text messaging technology platform for SUD services. It provides interesting feedback for providers, especially regarding when the patient thinks the TBI would be most helpful. Ask participants to reflect on the data and then facilitate a brief discussion. The important message is that patients in this study stated that TBIs were more important at the beginning and end of treatment rather than during treatment.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.
46
TBIsInteractive Voice Response (IVR)VideoconferencingAppsTexting
This slide represents the TBIs that this training will cover in more detail.47
a telephone-based technology
Rose et al., 2009Interactive voice response (IVR) uses touch-tone phones to enable a caller to interact with a computer using the telephone keypad as the interface
The Interactive Voice Response system uses the telephone to access computer-based interventions. IVR systems have been used in primary care and emergency department settings to conduct screening and brief intervention. Patients use a phone at the medical office or their own phone and call a number where they answer a number of questions by pressing the phones key pad. These systems are easy to use for patients. Many of the IVR systems also afford patients to call during off hours and listen to brief educational modules.
SourceRose, G.L., MacLean, C.D., Skelly, J., Badger, G.J., Ferraro, T.A., & Helzer, J.E. (2010). Interactive voice response technology can deliver alcohol screening and brief intervention in primary care. Journal of General Internal Medicine, 25(4), 340-4.
48
IVR-BI produced greater exposure to needed advice and information 1/3 of calls to IVR-BI were made outside of clinic hours
This study offered SBI to patients in a primary care setting. As part of the study, educational modules were added to the IVR system and available to patients to call-in to listen to. Study results demonstrated that 1/3 of the calls made to the IVR system were made outside of clinic hours (after hours).
SourceHelzer, J. E., Rose, G. L., Badger, G. J., Searles, J. S., Thomas, C. S., Lindberg, S. A. & Guth, S. (2008). Using interactive voice response to enhance brief alcohol intervention in primary care settings. Journal of Studies on Alcohol and Drugs, 69(2), 251258.
49
Recent Study Using IVR with Patients in Methadone Maintenance Program Patients used the system on almost 10 of the 28 days and found the system interesting, helpful, and easy to useRated most modules positively Calls were generally brief (10 minutes), but most patients accessed the majority of the content domainsPatients more likely to report abstinence on days they used IVRMoore et al., 2013
This a brief review of a small feasibility study conducted by Moore and colleagues about adding an automated telephone program, interactive voice response (IVR) to an outpatient methadone maintenance program. While the sample size was small the results showed some positive results. Patients were randomized into two groups over 4 weeks; half of the sample received treatment as usual and the other half received treatment as usual plus access to the recovery line. Patients who used the recovery line were more likely to report abstinence from opiates and cocaine on the days they used the recovery line. Patients used the recovery line on average of 10 days out of 28 even though they were instructed to use the line every day and were prompted to use the line with reminder messages. Patients reaction to the Recovery line was positive and researchers plan to conduct a larger study and to examine patient engagement issues.
SourceMoore, B.A., Fazzino, T., Barry, D.T., Fiellin, D.A., Cutter, C.J., Schottenfeld, R.S. & Ball, S.A. (2013). The Recovery Line: A pilot trial of automated, telephone-based treatment for continued drug use in methadone maintenance. Journal of Substance Abuse Treatment, 45(1), 63-69.
50
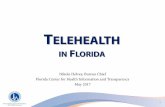
This chart shows how the Recovery Line IVR worked for patients participating in the study. From the chart, you can see the full range of services that were provided with this program including: information about the clinic (services, group times, etc.); daily questions (how are you doing, have you taken your methadone today, and did you use illicit drugs since your last call) assessment; learning modules, which were based on CBT principles; activities; and an encouragement section.
Researchers reported that IVR technologies are easily scalable and it could be an added intervention/support to enhance opioid dependence treatment.
51
Videoconferencing
This is a transition slide that announces the next TBI to be discussed.52
Systematic Review of Videoconferencing PsychotherapyPatients and providers perceived a strong therapeutic alliance over videoconferencing Studies that compared videoconferencing to in-person psychotherapy reported similar satisfaction levels between the conditionsHigh levels of satisfaction and acceptance with telemental health have been consistently demonstrated among patients across a variety of clinical populations and a broad range of services(Backhaus et al., 2012)Backhaus et al., 2012
Backhaus et al. (2012) did a systematic review of 891 articles on videoconferencing of psychotherapy 65 were selected for ; of those, only 47 were rated as empirical studies. Because of the low number of empirical studies, it is hard to determine if the treatment outcome of videoconferencing is the same as face-to-face. Small sample sizes and lack of randomization also impact the ability to assess treatment outcomes. In 45% of the studies people used CBT in videoconferencing, and 60% of the patients were male. In studies with each of the following populations - African-Americans, Hispanic Latino and American Indians - using videoconferencing psychotherapy demonstrated effectiveness.Studies showed strong patient and provider therapeutic alliance over video-conferencing with high levels of satisfaction. SourceBackhaus, A., Agha, Z., Maglione, M.L., Repp, A., Ross, B., Zuest, D., & Rice-Thorp, N.M., Lohr, J., & Thorp, S.R. (2012). Videoconferencing psychotherapy: A systematic review. Psychological Services, Special Issue: Telehealth, Telepsychology, and Technology, 9(2), 111-131.(See also: Bouchard et al., 2000; Ghosh, McLaren, & Watson, 1997; Morgan, Patrick, Magaletta, 2008; Simpson, 2001; Cluver et al., 2005; King et al., 2009; Morgan et al., 2008; Nelson, Barnard, & Cain, 2003; Ruskin et al., 2004)53
Evidence accumulated over six decades showsChakrabarti, 2015Hailey et al., 2008videoconferencing-based assessments are reliable, and clinical telepsychiatric/ telepsychology outcomes are comparable to conventional treatment among diverse patient populations on several measuresnegative attitudes of clinicians and institutions are the most significant barriers affecting telepsychiatric services usevideoconferencing telepsychiatry/psychotherapy is an acceptable and feasible form of providing mental health-care
Although telepsychiatry/psychology has been in existence for over 60 years, its uptake has been slow. Extensive systematic reviews found that telepsychiatry/psychology is as effective as in-person services for the following conditions: depressive disorders; anxiety disorders; PTSD; eating disorders; schizophrenia; and suicide. As videoconferencing equipment became more affordable and portable its uptake has increased. However, its adoption still remains low especially given its effectiveness. Negative attitudes of clinicians and institutions have impacted its adoption as well and is considered the significant barrier according to Hailey and colleagues.
SourceChakrabarti, S. (2015). Usefulness of telepsychiatry: A critical evaluation of videoconferencing-based approaches World Journal of Psychiatry, 5(3), 286-304.Hailey D, Roine R, Ohinmaa A. (2008). The effectiveness of telemental health applications: A review. Canadian Journal of Psychiatry, 53, 769-778.
54
Studies on Videoconferencing in Addiction TreatmentOpioid Treatment-group counseling(King et al., 2009 and King et al., 2014) Alcohol Treatment (Postel et al., 2005)Alcohol Treatment (Frueh et al., 2005)Teleconferencing Supervision (TCS) - MI(Smith et al., 2012)(Backhaus et al., 2012)
Of the 891 articles that have been published on videoconferencing, there are only 3 addressing treating substance use disorders. This is an interesting finding and demonstrates researchers interest in studying other telehealth technologies other than videoconferencing.The last article shown in the slide (Training Substance Abuse Clinicians in Motivational Interviewing Using Live Supervision via Teleconferencing) examined using teleconferencing to provide clinical supervision to counselors regarding adherence to MI.
SourceBackhaus, A., Agha, Z., Maglione, M.L., Repp, A., Ross, B., Zuest, D., & Rice-Thorp, N.M., Lohr, J., & Thorp, S.R. (2012). Videoconferencing psychotherapy: A systematic review. Psychological Services, Special Issue: Telehealth, Telepsychology, and Technology, 9(2), 111-131.55
eGetgoing uses videoconferencing technology to deliver therapy to patients with opioid dependence
(King et al., 2009 and King et al., 2014)
eGetgoing is the name of the videoconferencing platform used by King and colleagues in the two studies using videoconferencing to deliver group counseling to patients with opioid dependence. E-Getgoing patients reported positive feelings and a preference for videoconferencing citing that they liked the convenience the videoconferencing providing.
SourcesKing, V. L., Brooner, R.K., Peirce, J.M., Kolodner, K., Kidorf, M.S. (2014) Randomized trial of Web-based videoconferencing for substance abuse counseling. Journal of Substance Abuse Treatment, 46, 36-42.King, V. L.,Stoller, K.B., Kidorf, M., Kindbom, K., Hursh, S., Brady, T. & Brooner, R.K. (2009). Assessing the effectiveness of an Internet-based videoconferencing platform for delivering intensified substance abuse counseling. Journal of Substance Abuse Treatment, 36(3), 331-338.
56
Smartphones travel with individuals throughout their day, providing instant access to information and inspiration, as well as sources of social support, sponsors, or health professionals when cravings and urges or the fear of a lapse are at their greatest. Savic 2013, p.316
The quote in the article by Savic (2013) continued: In this regard, apps can provide ready access to continuing care and individually chosen support and information as needed. The discreet nature of using apps was also viewed positively and may be particularly important given the stigma surrounding addiction.
SourceSavic, M., Best, D., Rodda, S. & Lubman, D.I. (2013). Exploring the focus and experience of smartphone applications for addiction recovery. Journal of Addictive Diseases, 32(3), 310-319.57
ACHESSMonitoring and alertsRemindersAutonomous motivationAssertive outreachCare coordinationMedication remindersPeer & family supportRelaxationLocations trackingContact with professionalsInformation
This is a list app functions for ACHESS. A clinical trial with 300 subjects indicated that patients randomly assigned to the ACHESS condition had 50% fewer risky drinking days and a higher percent of maintained abstinence than people assigned to post treatment recovery support as usual.
Trainers Note: Sometimes during this presentation participants will share the mobile apps that they or their treatment program uses. It is important to re-emphasize two points: 1.) NFAR is not promoting ACHESS it simply showcasing it as one mobile app that is used for individuals in recovery; and 2.) it meets the criteria that is application is built upon well understood/tested theories and it has undergone clinical trials.
SourceQuanbeck, A., Chih, Ming-Yuan, Isham, A., Johnson, R., & Gustafson, D. (2014). Mobile delivery of treatment for alcohol use disorders: A review of the literature.Alcohol Research,36(1), 111-122.58
AppsSelf-Help Apps - http://www.ptsd.va.gov/PTSD/public/materials/apps/index.asp PTSD Coach learn about/cope with PTSD-symptoms common following traumaPTSD Family Coach supports family members of those with PTSDMindfulness Coach helps person stay grounded in the present to facilitate better coping with unpleasant thoughts and emotionsMY3 app - stay connected when struggling with tough emotions or having thoughts of suicide http://www.suicidepreventionlifeline.org/gethelp/my3-app.aspxSuicide Safe helps providers integrate suicide prevention strategies into their practice and address suicide risk among their patients a free app based on SAMHSA's Suicide Assessment Five-Step Evaluation and Triage(SAFE-T) card
These are examples of apps that were developed by the federal government and/or are free. Review each of the apps and suggest that participants review these apps by following the weblink. Of special note is the Suicide Safe app - SAMHSA's new suicide prevention app for mobile devices and optimized for tablets that helps providers integrate suicide prevention strategies into their practice and address suicide risk among their patients. Suicide Safe is a free app based on SAMHSA's Suicide Assessment Five-Step Evaluation and Triage(SAFE-T) card.
Have participants check out these apps? What do they think about their features? Process reactions.59
Text messaging seems to be a unique hybrid of writing and talking, recently being described as fingered speech McWhorter, 2012First peer-reviewed study of text messaging for health promotion was published in 2002; First RCT in 2005
Neville et al., 2002; Rodgers et al., 2005
The message of this slide is to reinforce that texting messaging for health promotion studies have been going on for over a decade and that texting is a combination of writing and talking and that many people think when they are texting that they are having a synchronous conversation. This belief is helpful when designing supportive texting programs.
SourcesMcWhorter, J. (2012, April 23). Talking with your fingers. The New York Times. Retrieved from http://opinionator.blogs.nytimes.com/2012/04/23/talking-with-your-fingers/?_r=0 Neville, R., Greene, A., McLeod, J., Tracey, A., Surie, J. (2002). Mobile phone text messaging can help young people manage asthma. BMJ, 325(7364), 600.Rodgers, A., Corbett, T., Bramley, D., Riddell, T., Wills, M., Lin, R.B., Jones, M. (2005). Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tobacco Control, 14, 255-261.
60
Research Studies Using Textingweight/obesity (Gerber et al., 2009)diabetes(Franklin et al., 2009)asthma (Neville et al., 2002)tobacco dependence (Rodgers et al., 2005)sexual health (Leach-Lemens, 2009; Lim et al., 2008)
Texting reminders and educational/motivational messages have been found to produce behavior change and better disease management outcomes across many chronic diseases.
In a review of some of these studies, positive behavior change outcomes were observed in 13 of the 14 reviewed studies. The review suggests that texting-delivered interventions have positive short-term behavioral outcomes (Fjeldsoe et al., 2009).
Free et al. (2011; 2012) demonstrated that smoking cessation support delivered via mobile phone text messaging doubles quit rates at 6 months.
61
Examples of TBI StudiesRodgers et al. (2005). Do u smoke after txt? smoking cessation using mobile phone text messagingFranklin et al. (2008). Patients engagement with Sweet Talk text messaging support system for young people with diabetes Woolford et al. (2011). OMG do not say LOL obese adolescents perspectives on the content of text messages to enhance weight loss effortsMalbon et al. (2013). Text in the city implementation of a clinic-based text messaging program to educate and informNorth Carolina (APPCNC). Birds n Bees adolescent pregnancy prevention campaign (www.appcnc.org)
The above (and below) listed references are highlighted to show participants how some researchers/developers are having fun with intervention names. Ask participants to get out their smart phones and google the name of these TBIs. Have them discuss these TBIs in their groups and then report back out to the large group. If the trainer wants to provide more data on the studies, below are excerpts from two of the studies.Text in the City was developed with the goal of providing youth seeking primary care services with a reminder system to improve birth control adherence, and accurate and timely health education.Birds n Bees acts as a state-wide service for sexual health-related questions. Its use has extended beyond the realms of sexual health
SourcesFranklin V.L., Greene, A., Waller, A., Greene, S.A., & Pagliari, C. (2008). Patients engagement with Sweet Talk a text messaging support system for young people with diabetes. Journal of Medical Internet Research, 10(2), e20.Rodgers, A., Corbett, T., Bramley, D., et al., (2005). Do u smoke after txt? Results of a randomized trial of smoking cessation using mobile phone text messaging. Tobacco Control, 14, 255-261.Malbon, K., Clifton Oxnard, S., Linares, L.O. & Nucci-Sack, A. (2012). Text in the city: Implementation of a clinic text messaging program to educate and inform. Journal of Communication in Healthcare, 5(2), 98-101.Woolford, S.J., Barr, K.L., Derry, H.A., Jepson, C.M., Clark, S.J., Strecher, V.J., & Resnicow, K. (2011). OMG do not say LOL: Obese adolescents perspectives on the content of text messages to enhance weight loss efforts. Obesity, 19(12), 23822387.
62
Allows for direct contactAsynchronouscan reach someone at any time; flexibility in timingUsed routinely for reminders in medical settingsincreases attendanceTailored messages can change behaviorTherapeutic reminders can bridge gap between treatment and daily lifeCost effective
Texting benefitsClough & Casey, 2011; Fjeldsoe et al., 2009; Gonzalez et al., 2014
As a reminder, there are many uses of texting that could support interaction between clients in SUD treatment and their counselors. This training is not focused on this type of technology-based counseling, but rather on the use of recovery support technologies that are accessible outside of the counseling frameworktechnologies that provide 24/7 support for long-term recovery. Even in the absence of a counselor who is responding to texts, there are many benefits to using this platform for recovery support. Implementing a mobile texting recovery program offers several advantages over traditional-based approaches currently in place, including:wide population reachpersonalization and targeted engagement, which is important given that personally tailored messages are more effective for health behavior change than untailored messages increased convenience enhanced assessment and monitoringgreater flexibility of service delivery in terms of frequency and timingrequiring minimal financial resources to maintain Additionally, because aftercare services to support recovery are not, mobile technology greatly enhances access to aftercare services, which are not routinely or systematically rendered in the substance use treatment field can help address lack of recovery support participation and drop out by youthrequire minimal time commitments and effort from providers as the majority of service-information can be automatedusers may gain more confidence in themselves for learning to self-manage their addiction behavior and cope with stressorsreminders can be sent outside of usual business hours and clients can read and respond in their own time may facilitate early development of the therapeutic alliance, another strategy often employed to decrease dropoutserve as an appropriate bridge between inpatient treatment and outpatient daily life to help clients maintain and consolidate the gains achieved in treatmentThe potential of texting may be particularly significant among population groups most likely to use mobile telephones as their primary means of communication. The highest level of mobile telephone use is among adolescents, younger adults, socioeconomically disadvantaged populations, less educated young adults, and people who rent or frequently change addresses. Further, a high level of mobile telephone use is associated with lower levels of self-rated health and engaging in health-compromising behaviors. Texting presents a prime delivery channel for health behavior change interventions because it has high penetration in populations oflower sociodemographic position and populations with poorer health.SourcesGonzalez, R., Ang, A., Murphy, D.A., Glik, D.C., & Anglin, M.D. (2014). Substance use recovery outcomes among a cohort of youth participating in a mobile-based texting aftercare pilot program. Journal of Substance Abuse Treatment, 47(1), 20-26.Fjeldsoe, B.S., Marshall, A.L., & Miller, Y.D. (2009). Behavior change interventions delivered by mobile telephone short-message service. American Journal of Preventive Medicine, 36(2), 166-173.Clough, B. A. & Casey, L. M. (2011). Technological adjuncts to increase adherence to therapy: A review. Clinical Psychology Review, 31(5), 697-710.
63
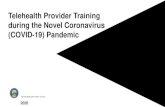
Ingersoll et al., 2014
This image of a therapeutic text messaging program comes from the study by Ingersoll and colleagues (2014). Ask participants their reaction to this image (is it what they imagined; too simplistic to work; shouldnt it be fancier; etc. are all examples of questions that participants may ask). Process reactions with the participants.
Special thanks to Dr. Ingersoll and her colleagues for including this example in their journal article. It is helpful to provide a glimpse of what patients see when involved with a SMS texting program.
SourceIngersol, K., Dillingham, R., Reynolds, G., Hettema, J., Freeman, J., Hosseinbor, S. & Winstead-Derlega, C. (2014). Development of a personalized bidirectional text messaging tool for HIV adherence assessment and intervention among substance abusers. Journal of Substance Abuse Treatment, 46, 66-73.64
Used youth to craft languageDaily self-monitoring texts, a daily wellness recovery tip, and substance abuse education and social support resource information on weekendsCompared with standard aftercare, texting reduced relapse risk and promoted recovery engagementYouth-Focused Texting Case StudyGonzales et al., 2016
One study by Gonzales et al. (2014) sent three types of messages to teens in SUD recovery: daily self-monitoring texts; a daily wellness recovery tip; and substance abuse education and social support resource information on weekends. Youth provided text message suggestions and ratings for various monitoring-feedback areas scenarios.Self-monitoring texts focused on the following core areas associated with youth relapse post-treatment: low confidence; stress; negative mood; not engaging in recovery goal-directed behaviors; and continued substance use. Youth texted back a corresponding number to the monitoring text, which prompted an automated feedback text to be sent back, consisting of positive appraisal messages, motivational/inspirational messages, stress management tips, and coping advice. The wellness daily recovery tips addressed four general areas of health/wellness:personal health, social health, emotional health, and physical health. Lastly, youth were also sent weekend text messages specific to substance abuse education and social support resource information. The texts were tailored to individual participants' primary substances they reported receiving treatment for. Information about social support services and resources were also sent to participants on the weekend and were tailored geographically to the participants' zip-code residence location reported at enrollment to the program.Compared to a standard aftercare control condition this mobile texting aftercare pilot program:demonstrated promise for reducing relapse risk and promoting recovery behavior engagement served as a buffer towards the tendency for youth to continue to relapse in the initial 3 months after treatmentgreatly reduced substance use problem severity
SourceGonzales, R., Hernandez, M., Murphy, D. A. and Ang, A. (2016). Youth recovery outcomes at 6 and 9 months following participation in a mobile texting recovery support aftercare pilot study. American Journal of Addiction, 25, 62-68.
65
Text Messaging Examples How many days in the past week did you feel stressed or have negative emotions (Text 07)? Participant texts back a 3 (Feedback text) Think about 2 good things in your life right nowwrite them down and focus on those. Ignore everything else. Youth were also sent one daily reminder text that provided them with a recovery tip of the day focused on wellness using the following text prompt throughout the 12 weeks: Todays a new day in your recovery, think about the change you are working toward... (wellness tip).Gonzales et al., 2016
This slide shows some of the text messages that adolescents involved in the Gonzales (2016) study. Have participants read these text messaging examples and they ask for comments or questions. The journal article by Gonzales and colleagues provides additional detail on how they created the messages and conducted a focus group with adolescent patients in order to help with the language and authenticity.
SourceGonzales, R., Hernandez, M., Murphy, D. A. and Ang, A. (2016). Youth recovery outcomes at 6 and 9 months following participation in a mobile texting recovery support aftercare pilot study. American Journal of Addiction, 25, 6268.
66
How you could use existing technology to extend the reach or enhance your organizations services
Ask participants to get into groups and discuss how they could use technology to extend the reach or enhance service delivery. This is a brainstorming section so dont expect participants to have all the answers. Some participants may complain that they do not have enough information to have this discussion. However, this is inaccurate. Encourage participants to continue with the brainstorming process. 67
Examples of a Technology-Based Intervention that can extend the reach of clinical staffTreatment Orientation Videouseful and efficient means to orient someone to the treatment process (Zwick & Attkisson, 1985)as effective as in-person orientations for many health and behavior problems improves overall outcomes compared with no-orientation control groups (Walitzer et al. 1999; Zwick & Attkisson, 1985)Help patients put reminders/alerts on their phonesMuench, 2015
One example of a technology-based intervention that extends a practitioners the reach is a treatment orientation video. Organizations that have an extensive informed consent process or provide residential/hospital-based care could produce a video for patients to watch rather than the practitioner spending time repeating the same information again and again for patients. These treatment orientation videos have been studied and found to be as effective as in-person orientations and improving patient outcomes when compared to no-orientation control groups. The orientation video extends the reach of practitioners by using technology to take on a practitioner activity and freeing up time for practitioner to take on more complex tasks.
SourceMuench, F.(2015).The promises and pitfalls of integrating digital health technologies into alcohol treatment.Alcohol Research, Current Reviews, 36(1), 131-142.Walitzer, K.S., Dermen, K.H., & Connors, G.J. (1999). Strategies for preparing clients for treatment: A review. Behavior Modification, 23(1), 129151. PMID: 9926524Zwick, R. & Attkisson, C.C. (1985). Effectiveness of a client pretherapy orientation videotape. Journal of Counseling Psychology, 32(4), 514524.68
Technology-Based Interventions 1. feasible2. patients interested in using them3. initial studies demonstrate positive outcomes
hold great promise for reaching the large number of individuals who may benefit from earlier assessment and treatment but do not access services currently
Use these slides to summarize the benefits of TBIs. 69
Technology-Based Interventions can1. help health care and other settings implement EBPsgreater ability to reach rural and underserved populations, and greater confidentiality, leading to fewer concerns about stigma 2. encourage patients disclose health conditions3. extends the reach of clinicians
After reviewing this second summary slide, ask participants if they have any benefits of TBI to add to this list or if they disagree with any of the stated benefits. Process these comments with the participants.70
SAMHSAs TIP 60 assists clinicians with the implementation of technology-assisted care (TAC)highlights the importance of using technology-based assessments and interventions in behavioral health treatment servicesdiscusses how technology reduces barriers to accessing care
http://store.samhsa.gov/71
SUDTECH.ORG
This website is a great resource for you to become more familiar with technology-based interventions, including videos, literature reviews and demonstrations of various technologies for substance abuse treatment. 72