Obstetric Colour Doppler Study
63
OBSTETRIC COLOUR DOPPLER
-
Upload
sandeep-awal -
Category
Health & Medicine
-
view
159 -
download
2
Transcript of Obstetric Colour Doppler Study

OBSTETRIC COLOUR DOPPLER

DOPPLER HISTORY
• First use of doppler
ultrasonography to study flow velocity
in fetal umbilical artery was
reported in 1977.

DOPPLER WAVEFORM ANALYSIS
• Doppler ultrasound waveforms reflect blood velocity.
• Doppler waveforms however, also provide information on
various aspect of blood flow in circulation,including the
presence and direction of flow,velocity profile and
impedence to the flow.
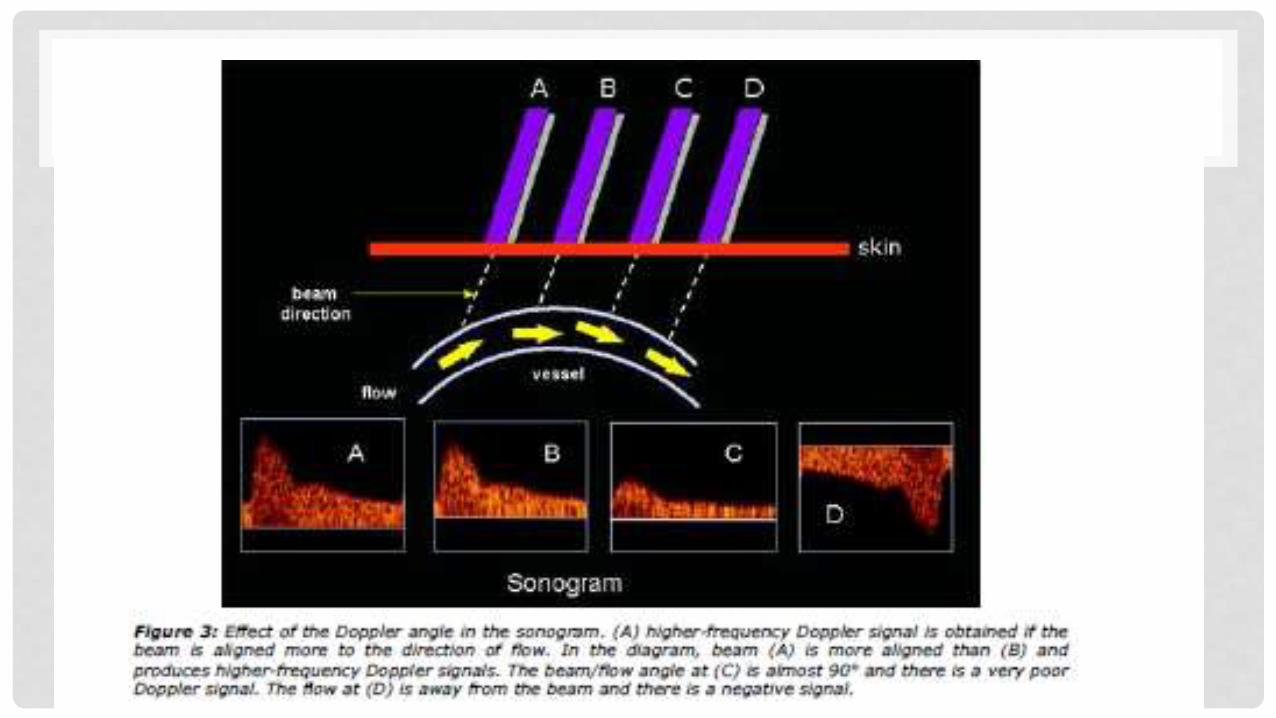
• The angle of insonation: the Doppler frequency increases as the Doppler ultrasound beam becomes more aligned to the flow direction (the angle between the beam and the direction of flow becomes smaller).
•
• This is of the utmost importance in the use of Doppler ultrasound.
• The essential condition for the assessment of true velocity depends on the
angle between the ultrasound beam and the direction of the blood flow, which
needs to be as close as possible to 0 degrees.
• As the incident angle increases ,blood velocity is progressively
underestimated; therefore the angle-independent indices are used.
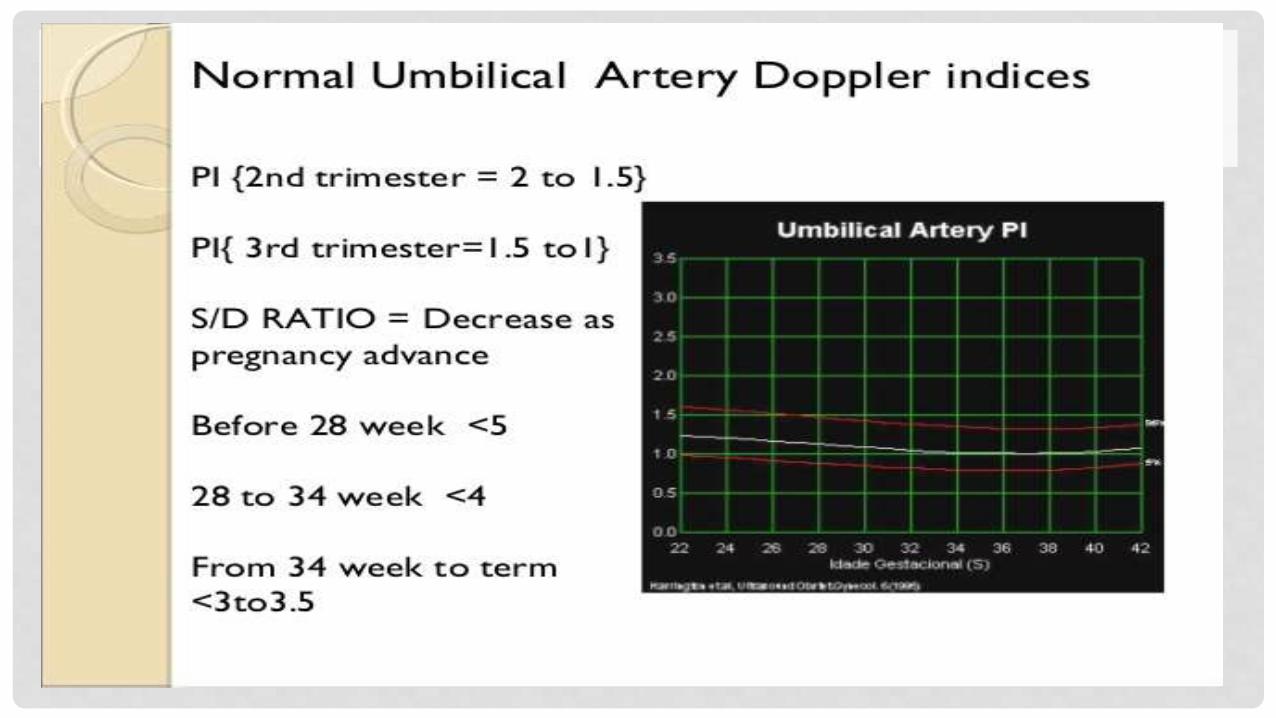
• 1. Systolic-to-diastolic (S/D) ratio = Peak systolic velocity/End diastolic
velocity (PSV/EDV)
• 2. Resistive index (RI) = (PSV - EDV)/PSV
• 3. Pulsatility index (PI) = (PSV - EDV)/Mean velocity
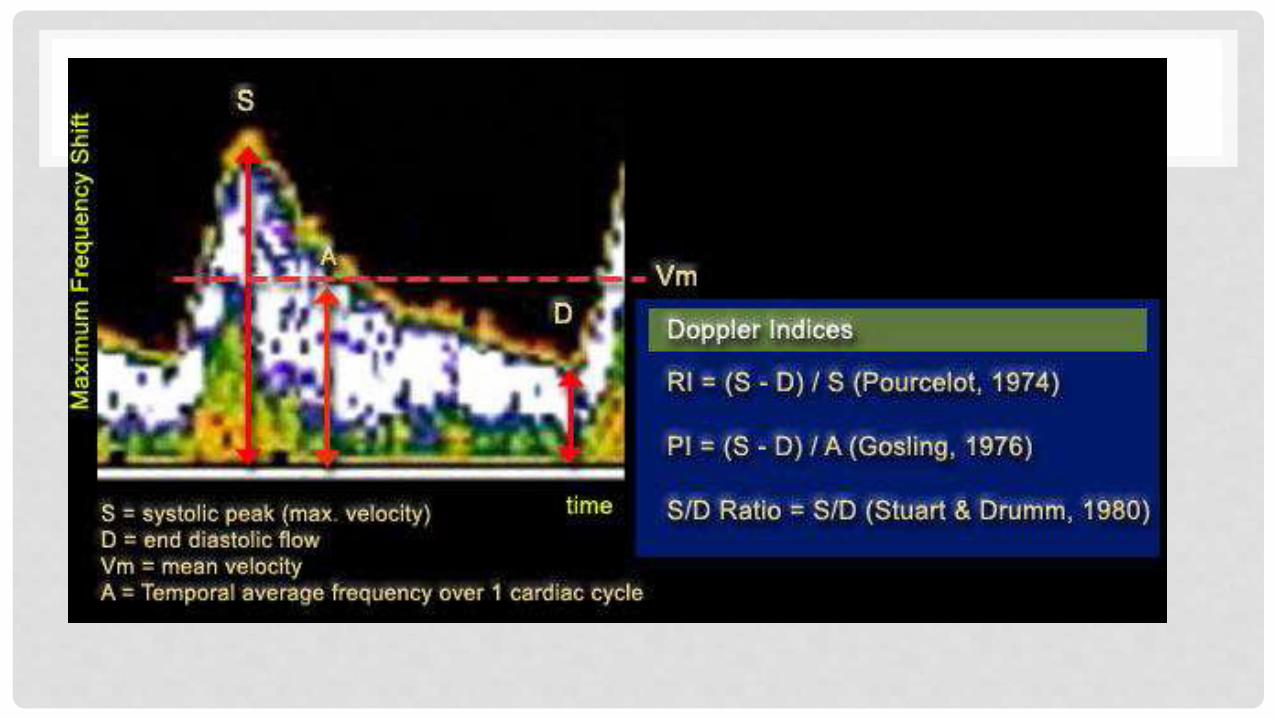

• These three indices provide information on vascular impedance, which is
not the same as vascular resistance.
• In fact, impedance has a more extensive meaning than resistance, because it
depends on vascular resistance,preload, heart rate, and cardiac contractility.
• By calculating one of these indices and therefore estimating the vascular
resistance, we can obtain information on the amount of blood flow.

• For example,if we assess the PI(or the RI or S/D ratio) at the level of the
MCA in fetuses appropriate for gestational age (AGA) and in growth
restricted fetuses at the same gestational age, the IUGR fetuses will have
a lower PI value at the MCA than the AGA fetuses.
•
• Our interpretation is that in IUGR fetuses,there is a lower vascular
resistance at the MCA than in AGA fetuses. This suggests an increased
blood flow to the brain.

PULSATILE AND CONTINUOUS FLOW
• Blood flow velocity of the fetal vascular system can be either pulsatile or
continuous.
• The arteries always have a pulsatile pattern, whereas the veins have either a
pulsatile or a continuous pattern

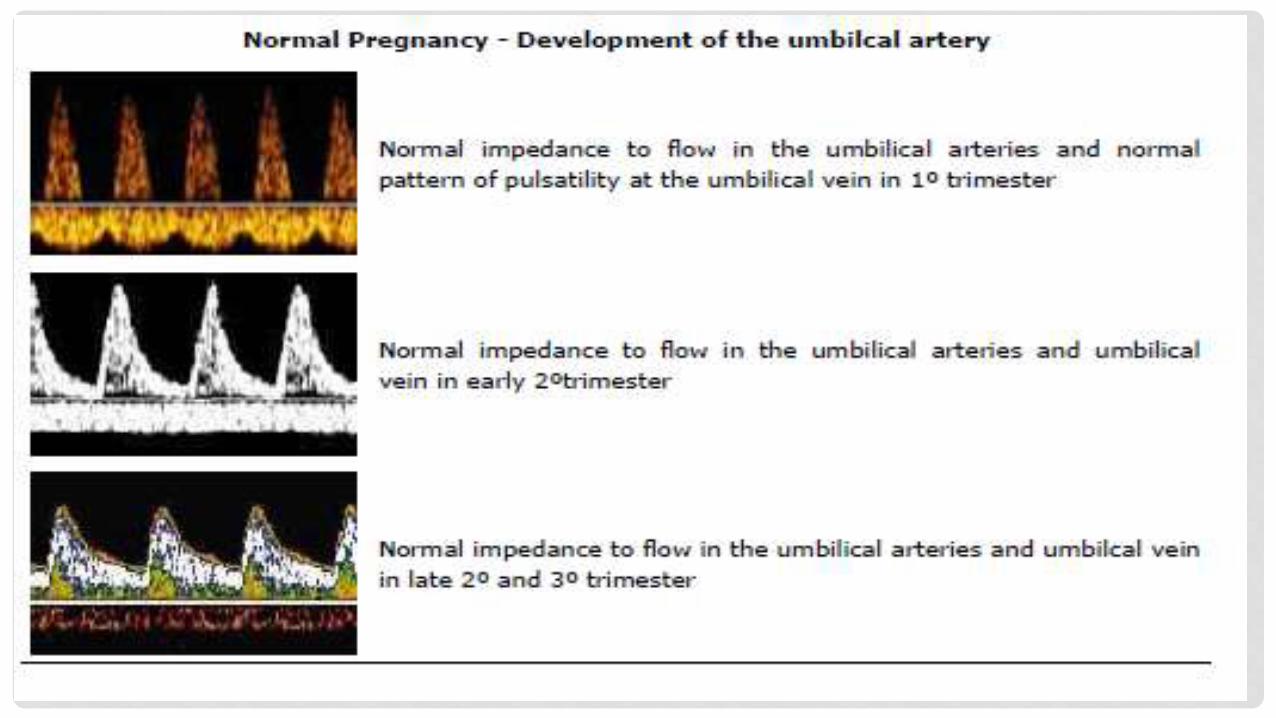
Umbilical artery and umbilical vein.
The umbilical vein has a constant velocity, whereas the umbilical artery
(UA) is pulsatile because it reflects the systole and diastole of the cardiac
cycle. In this case, the umbilical artery blood was directed away from the transducer and
therefore arterial flow is represented below the baseline.

NORMAL ARTERIAL WAVEFORM IN THE SAME PATIENT

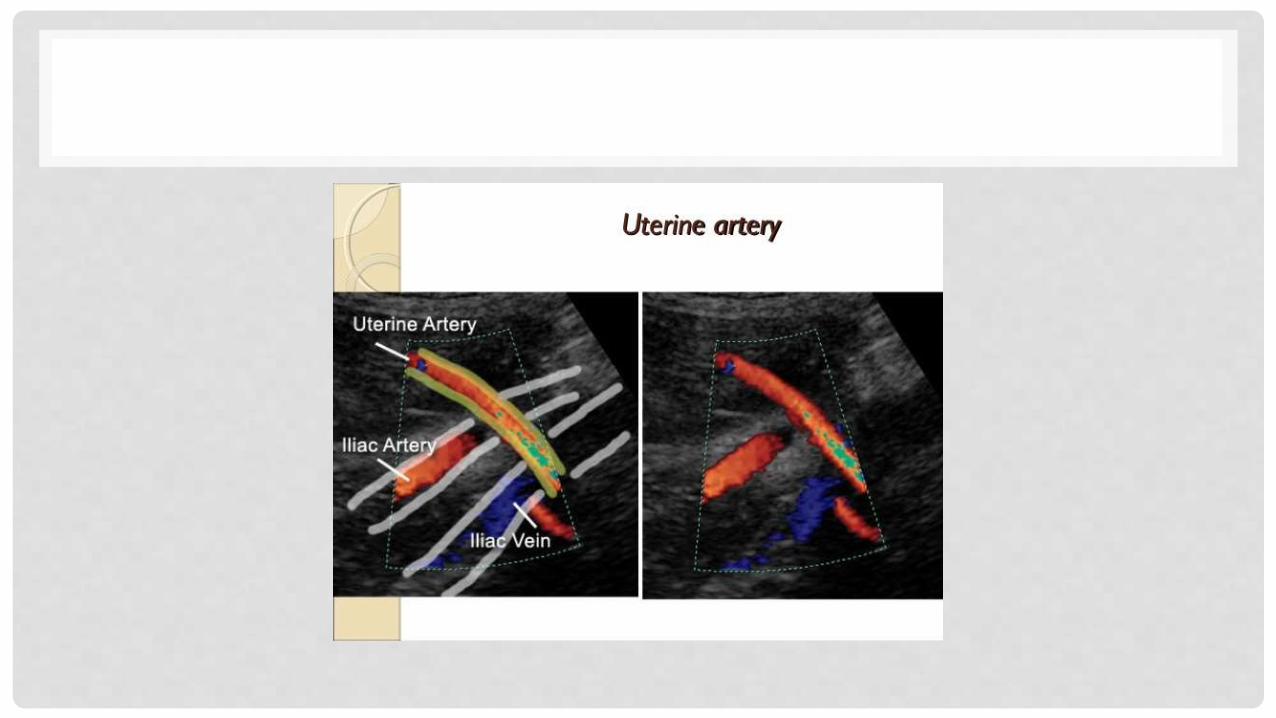
UTEROPLACENTAL CIRCULATION-ANATOMY
• The blood supply to the uterus comes mainly from the uterine arteries, with a small contribution from the ovarian arteries.
•
• These vessels give rise to arcuate arteries that run circumferentially round the uterus.
• The radial arteries arise from the arcuate vessels and penetrate into the outer third of the myometrium.
• Radial vessels then give rise to the basal and spiral arteries, which nourish the myometrium and decidua during pregnancy.
•
• Spiral arteries are responsible for 10-12 fold increase in
blood flow during pregnancy.


VESSELS NEED TO BE EXAMINED
• Umbilical artery
• Middle cerebral artery
• Uterine artery
• Ductus venosus
• IVC
• Umbilical vein

UMBILICAL ARTERY
• The umbilical artery was the first fetal vessel to be evaluated by Doppler velocimetry.
• Placental blood is assessed by studying the umbilical artery.
• Flow velocity waveforms from the umbilical cord have a characteristic saw-tooth appearance of arterial flow in one direction and continuous umbilical venous blood flow in the other.

• UA waveforms are slightly different at the fetal abdominal wall and at the
placental insertion,with indices higher at the wall than the insertion.
• However, the difference is minimal, so it is not important to obtain the
waveforms always at the same level.
• The transducer, is placed on the mother’s abdomen overlying the fetus and is systematically manipulated to obtain the characteristic waveforms from the umbilical artery.
• In practice, the UA is best examined in a segment of free floating umbilical
cord.


• The middle cerebral artery is the vessel of choice to assess the fetal cerebral
circulation because it is easy to identify, is highly reproducible, and provides
information on the brain-sparing effect.
• MCA can be studied easily with an angle of 0 degrees between the
ultrasound beam and the direction of blood flow providing information on the
true velocity of the blood flow.
•
• The MCA should be sampled soon after its origin from the ICA.





BRAIN SPARING EFFECT
• IUGR is associated with increased blood flow to the fetal brain.
This increase in blood flow during diastole can be demonstrated by Doppler
ultrasound of the MCA.
• This effect is termed the brain-sparing effect and is demonstrated by a
lower value of the MCA PI .



• The uterine arterial blood flow in non pregnant women is 50 mL per minute
and increases to over 700 ml per minute in the third trimester of pregnancy.
• Each uterine artery should be sampled soon after the crossing of the iliac
vessels.
•

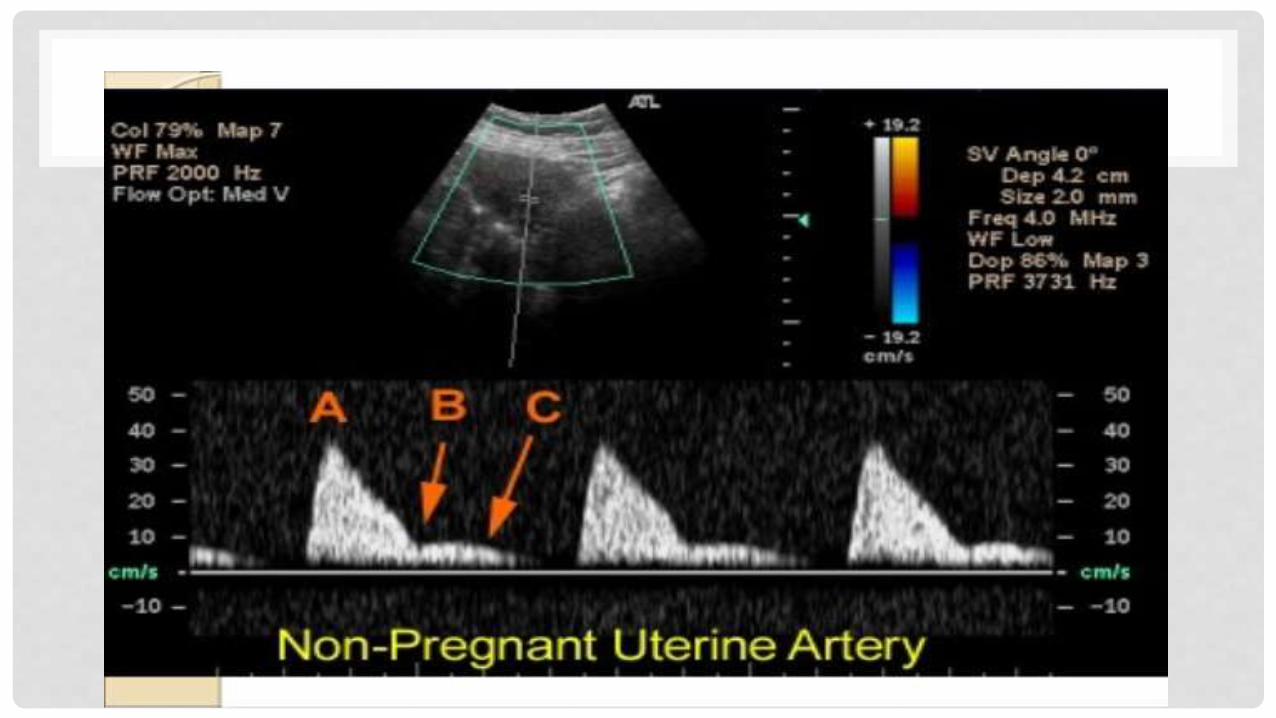
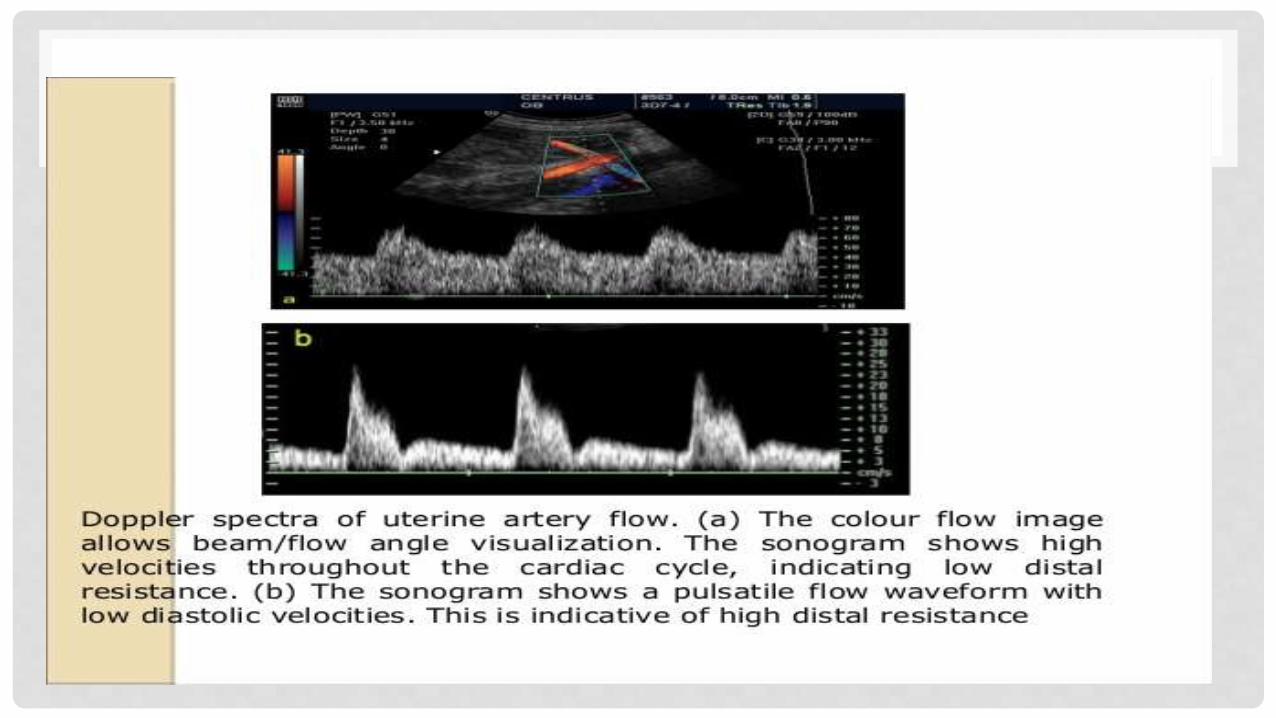
• The uterine artery waveform by the mid–second trimester is characterized by
high end diastolic velocities (EDVs) with continuous forward blood flow
throughout diastole.
• With advancing gestation,the degree of end diastolic flow typically increases.
• Thus the diastolic component of uterine artery Doppler waveform is
transformed during normal pregnancy from one of low peak flow velocity and
an early diastolic notch, to one of high flow velocity and an early diastolic
notch.
• If the end diastolic flow does not increase throughout pregnancy, or if a small
notch is detected at the beginning of diastole, the fetus is at high risk for
developing IUGR.
• Diastolic blood flow may be absent or even reversed with extreme degrees of
placental dysfunction.




• The ductus venosus originates from the umbilical vein
•
• The diameter of the ductus venosus measure approximately one-third of that of the umbilical vein.
•
• It courses posteriorly and in a cephalad direction, with increasing steepness in the same sagittal plane as the original direction of the umbilical vein,and enters the inferior vena cava just below the diaphragm.

• The ductus venosus can be visualized in its full length in a mid-sagittal longitudinal section of the fetal trunk.
•
• In an oblique transverse section through the upper abdomen, its origin from the umbilical vein can be found where color Doppler indicates high velocities compared to the umbilical vein.
• The blood flow velocity accelerates due to the narrow lumen of the ductus venosus, the maximum inner width of the narrowest portion being 2 mm


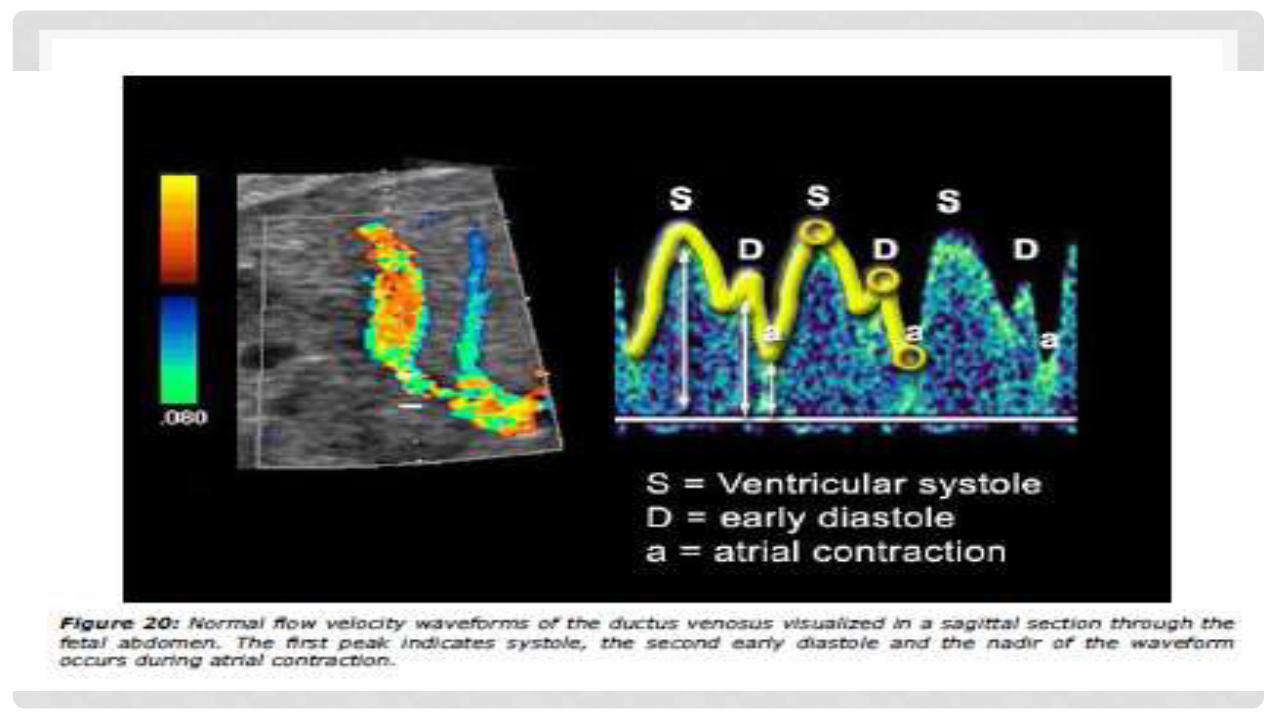
• The DV waveform has a biphasic pattern characterized by two peaks: the
“S”, or peak systolic velocity (PSV), which corresponds to the highest velocity
of the blood in systole.
• It is followed by a period of decreased velocity called isovolumetric relaxation
(IRV); and the “D”, which corresponds to the rapid filling of the ventricles that
is followed by the “A wave,” which corresponds to atrial contraction.
• In AGA fetuses,there is forward flow at the DV, and the PI for veins ([S - D]/A)
decreases with advancing gestation.
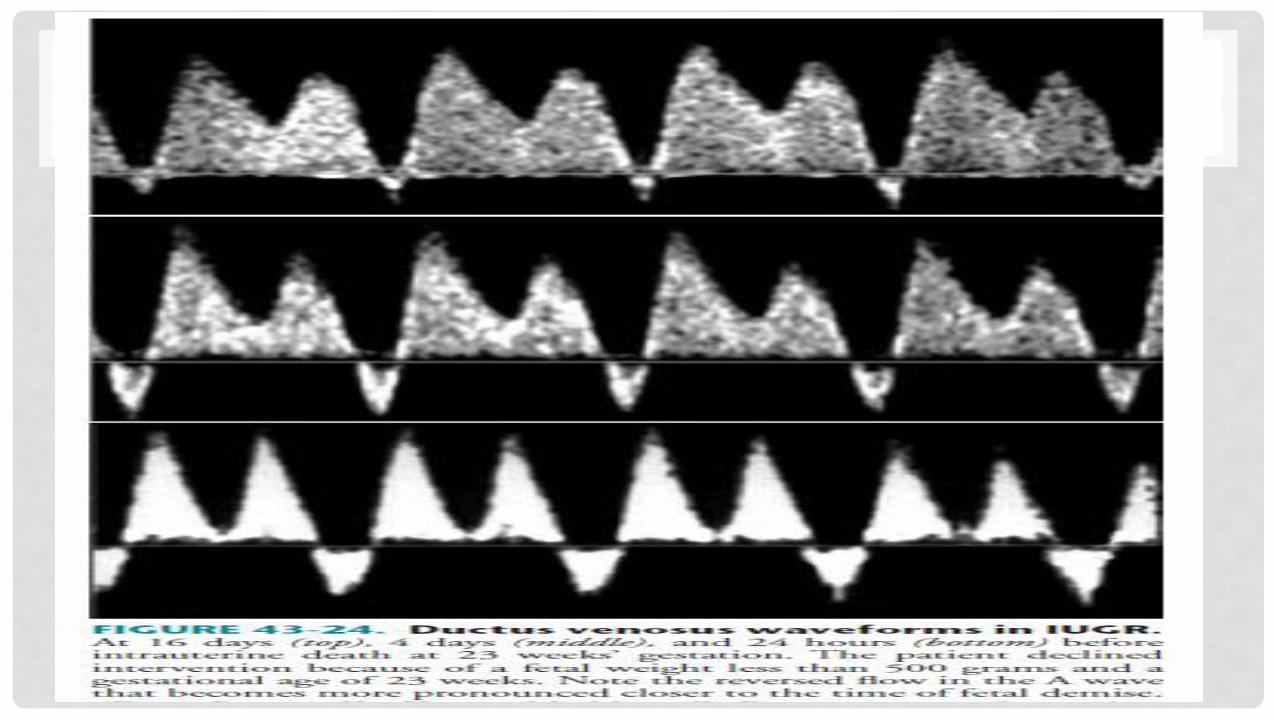
• In growth-restricted fetuses, the PI increases in the DV, and in the most
severe cases, there is A wave of reversed flow.




• The IVC, before its entrance into the right atrium, has a triphasic pulsatile
pattern.
• The first forward wave begins to increase with atrial relaxation,reaches a
peak during ventricular systole, and then falls at the end of ventricular
systole.
• The second forward wave occurs during early diastole, and the third wave,
characterized by reversed flow, is present in late diastole with atrial
contraction.
• In healthy fetuses, a significant decrease of the reversed flow during atrial
contraction is present with advancing gestation.
• In IUGR fetuses the IVC is characterized by an increase in reversed flow
during atrial contraction.
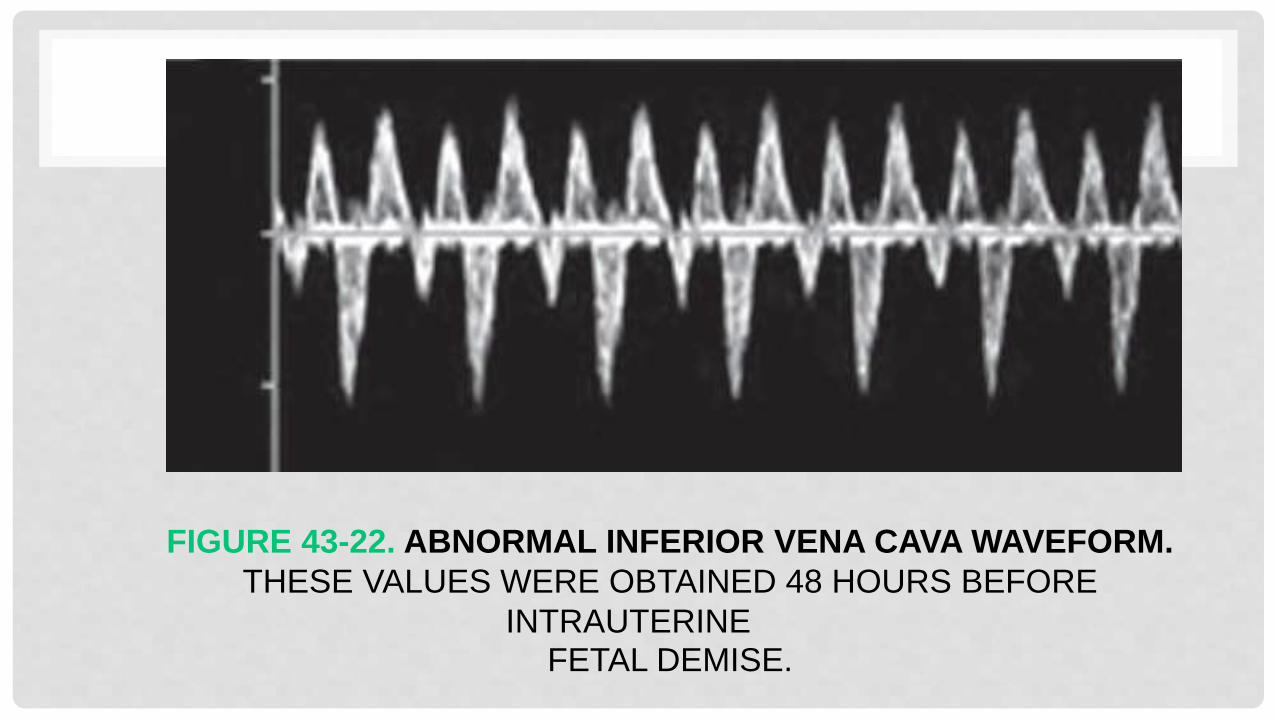
FIGURE 43-22. ABNORMAL INFERIOR VENA CAVA WAVEFORM.
THESE VALUES WERE OBTAINED 48 HOURS BEFORE
INTRAUTERINEFETAL DEMISE.

UMBILICAL VEIN

• Normal flow in the free-floating umbilical vein is monophasic.
• Fetuses with pulsation in the umbilical vein in the second and third trimesters
have a higher morbidity and mortality, even in the setting of normal UA blood
flow.

FIGURE 43-19. ABNORMAL UMBILICAL VEIN WAVEFORMS. A, SINGLE PULSATION. B, DOUBLE
PULSATION. WAVEFORMS OBTAINED CLOSE TO THE ORIGIN OF THE DUCTUS VENOSUS 48
HOURS BEFORE FETAL DEMISE. C, DOUBLE PULSATION; SAME CASE AS B. WAVEFORMS
OBTAINED BETWEEN THE
ORIGIN OF THE DUCTUS VENOSUS AND THE UMBILICUS. D, REVERSED FLOW. FETUS DIED WITHIN 24 HOURS OF THIS FINDING.